Back to Journals » Infection and Drug Resistance » Volume 19
Clinical Distribution and Antimicrobial Resistance Characteristics of Pseudomonas aeruginosa Infections in Otorhinolaryngology in Eastern China: A Single-Center Retrospective Study
Authors Lin K, Liu Y, Lü P, Zhou J ![]()
Received 24 March 2026
Accepted for publication 23 May 2026
Published 28 May 2026 Volume 2026:19 611494
DOI https://doi.org/10.2147/IDR.S611494
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemant Joshi
Kaichun Lin,1 Yining Liu,1 Pan Lü,2 Jian Zhou3
1Department of Otorhinolaryngology-Head and Neck Surgery, The First People’s Hospital of Yongkang, Jinhua, Zhejiang, People’s Republic of China; 2Clinical Laboratory, The First People’s Hospital of Yongkang, Jinhua, Zhejiang, People’s Republic of China; 3Department of Pediatrics, The First People’s Hospital of Yongkang, Jinhua, Zhejiang, People’s Republic of China
Correspondence: Jian Zhou, Department of Pediatrics, The First People’s Hospital of Yongkang, No. 599 Jinshan West Road, Yongkang, Jinhua, Zhejiang, 321300, People’s Republic of China, Email [email protected]
Background: Pseudomonas aeruginosa is a clinically important opportunistic pathogen in otorhinolaryngology, where chronic inflammation, impaired drainage, postoperative wounds, and device-associated biofilms may complicate treatment. Specialty-specific data linking anatomical distribution, multidrug resistance (MDR), and clinical outcomes remain limited in regional hospitals in China.
Objective: To describe the clinical distribution and antimicrobial susceptibility profile of P. aeruginosa infections in otorhinolaryngology and to identify factors associated with MDR.
Methods: This single-center retrospective cohort study included 112 consecutive patients with clinically adjudicated otorhinolaryngological infection and culture-confirmed P. aeruginosa at The First People’s Hospital of Yongkang, Eastern China, from January to December 2024. MDR was defined as non-susceptibility to at least one agent in three or more antimicrobial categories. Group comparisons and multivariable logistic regression were performed.
Results: The most common sites were the external ear canal/external ear (31.2%), middle ear/mastoid (25.0%), and nasal cavity/paranasal sinuses (21.4%). MDR was identified in 37 patients (33.0%). The highest susceptibility percentages were observed for colistin/polymyxin B (95.5%), amikacin (84.8%), and piperacillin-tazobactam (79.5%), whereas the highest resistance percentages were observed for aztreonam (32.1%), levofloxacin (27.7%), and ceftazidime (24.1%). Recent carbapenem exposure (adjusted odds ratio [aOR] 5.09, 95% confidence interval [CI] 1.22– 21.19), postoperative indwelling devices/drainage (aOR 4.81, 95% CI 1.81– 12.83), and hospital-acquired infection (aOR 2.52, 95% CI 1.02– 6.23) were independently associated with MDR. MDR infections were associated with longer hospitalization, higher C-reactive protein levels, more antimicrobial regimen modifications, and lower clinical success.
Conclusion: This study provides specialty- and region-specific evidence that MDR P. aeruginosa is a substantial concern in otorhinolaryngological infections. In patients with recent carbapenem exposure, postoperative drainage or devices, or hospital-acquired infection, early culture acquisition, source control, and susceptibility-guided therapy are particularly important.
Keywords: Pseudomonas aeruginosa, otorhinolaryngology, antimicrobial susceptibility testing, multidrug resistance, hospital-acquired infection, carbapenems, eastern China
Introduction
Pseudomonas aeruginosa is a Gram-negative opportunistic pathogen with marked environmental adaptability, intrinsic resistance to multiple antimicrobial classes, and the ability to acquire additional resistance under antimicrobial pressure.1–4 In otorhinolaryngology, P. aeruginosa is frequently recovered from chronic suppurative otitis media, otitis externa, postoperative wound infections, and sinonasal infections.5–11 The anatomical characteristics of the external and middle ear, mastoid cavity, nasal cavity, and paranasal sinuses - including relatively limited ventilation, impaired drainage, and the frequent presence of chronic mucosal inflammation - may facilitate persistence of this organism and promote biofilm-associated infection.
Multidrug-resistant (MDR) P. aeruginosa is a major concern because resistance may compromise empirical therapy, delay effective treatment, and increase the need for repeated regimen modification or source-control procedures.12–16 National and regional surveillance studies from China have documented clinically important resistance among P. aeruginosa isolates from diverse specimen sources, particularly respiratory, bloodstream, urinary, and wound specimens.17–21 However, large surveillance datasets usually aggregate isolates across hospital departments and specimen types; they do not adequately address the specific anatomical distribution, specimen-source characteristics, and clinical outcomes of otorhinolaryngological infections. Therefore, the specialty-specific burden of MDR P. aeruginosa in otorhinolaryngology remains insufficiently defined, especially in regional hospitals in Eastern China.
This evidence gap has practical implications. Empirical therapy for otorhinolaryngological infections is often initiated before culture results are available, and the decision to broaden coverage or intensify source control depends on local risk factors, local susceptibility patterns, and the distinction between true infection and colonization.13,14 In addition, most available studies emphasize microbiological susceptibility data alone, whereas fewer studies combine anatomical distribution, MDR versus non-MDR comparisons, clinical exposure variables, and outcome indicators in the same otorhinolaryngology cohort.
The objectives of this study were to (1) describe the anatomical distribution and specimen-source characteristics of P. aeruginosa infections in otorhinolaryngology; (2) analyze antimicrobial susceptibility profiles against commonly used antipseudomonal agents; (3) compare clinical exposure characteristics between MDR and non-MDR infections; and (4) evaluate factors associated with MDR and their clinical outcome correlates. By focusing on a single regional center in Eastern China, the study aimed to provide a pragmatic local evidence base for risk stratification, culture-driven therapy, source control, infection prevention, and antimicrobial stewardship in otorhinolaryngology.
Materials and Methods
Study Design and Ethics Statement
This was a single-center retrospective cohort study conducted in the Department of Otorhinolaryngology-Head and Neck Surgery at The First People’s Hospital of Yongkang, Jinhua, Zhejiang Province, Eastern China. The study protocol was approved by the Institutional Review Board of The First People’s Hospital of Yongkang (approval number: YKSDYRMYYEC2024-KT-HS-013). The requirement for informed consent was waived because the study was retrospective and all data were de-identified before analysis. The study was conducted in accordance with the Declaration of Helsinki and reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.22,23
Study Population and Case Adjudication
The laboratory information system and electronic medical records were reviewed for patients who presented to or were admitted to the otorhinolaryngology department between January 1, 2024 and December 31, 2024 and had P. aeruginosa isolated from an otorhinolaryngological specimen. For patients with more than one positive culture during the same infectious episode, only the first non-duplicate isolate was included. Recurrent infections separated by complete clinical resolution were reviewed, but only the index episode during the study period was analyzed to avoid within-patient clustering.
Eligible patients met all of the following criteria: (1) a clinically diagnosed otorhinolaryngological infection, supported by compatible symptoms and signs such as otalgia, otorrhea, purulent nasal or sinus secretion, fever, postoperative wound inflammation, neck swelling, abscess formation, or endoscopic/imaging evidence of infection; (2) isolation of P. aeruginosa from a clinically relevant specimen, including ear discharge, ear canal swab, nasal or paranasal sinus secretion, pharyngeal swab, surgical site exudate or pus, drainage fluid, abscess aspirate, or postoperative drainage fluid; and (3) available antimicrobial susceptibility results and clinical outcome information.
To reduce misclassification between true infection and colonization, each candidate case was adjudicated on the basis of concordance between clinical manifestations, specimen source, inflammatory markers, imaging or endoscopic findings when available, and the treating physician’s assessment. P. aeruginosa was considered a causative pathogen when it was recovered from purulent material or a clinically involved site and the clinical record supported active infection requiring targeted management. Cases were classified as colonization or contamination and excluded when P. aeruginosa was isolated from a non-sterile superficial site without compatible local or systemic signs of infection, without supportive inflammatory or imaging findings, or without a treatment decision consistent with active infection.
Exclusion criteria were: (1) colonization or contamination without clinical evidence of infection; (2) polymicrobial infection in which P. aeruginosa could not be determined as the principal pathogen from the clinical record; and (3) missing key data on antimicrobial susceptibility or clinical outcome. Because this was a microbiology-based retrospective cohort, the denominator of all patients with suspected otorhinolaryngological infection but negative cultures was not available; this limitation was considered when interpreting generalizability and selection bias.
Data Collection and Variable Definitions
Data were extracted from electronic medical records and the laboratory information system using a standardized data collection form. Demographic variables included age and sex. Clinical exposure variables included diabetes mellitus, immunosuppression or malignancy, hospitalization within the preceding 90 days, intensive care unit admission, postoperative status with indwelling devices or drainage, antimicrobial exposure within the preceding 30 days, carbapenem exposure within the preceding 30 days, and mode of infection acquisition.
Hospital-acquired infection was defined as new evidence of infection occurring 48 hours or more after admission, or infection associated with hospitalization, surgery, invasive procedures, indwelling devices, or postoperative drainage.24 Community-acquired infection was defined as infection present at admission or within the first 48 hours of admission without a healthcare-associated exposure explaining onset.
Outcome variables included length of hospital stay, number of antimicrobial regimen modifications, white blood cell count (WBC), C-reactive protein (CRP), and clinical outcome. Clinical success was defined as cure or improvement at discharge or the last documented evaluation. Cure was defined as resolution of symptoms and signs without need for further anti-infective therapy; improvement was defined as partial but clear clinical response allowing discharge or step-down treatment; relapse was defined as recurrence of infection symptoms requiring renewed medical evaluation after initial improvement; treatment failure was defined as persistent or worsening infection despite treatment; death was recorded when death occurred during hospitalization or the documented treatment episode.
Microbiological Identification and Antimicrobial Susceptibility Testing
Specimens were collected by trained clinicians using routine aseptic procedures appropriate to the anatomical site and were transported promptly to the clinical microbiology laboratory. Isolate identification was performed using an automated microbiological identification system (VITEK 2 Compact; bioMerieux, Marcy-l’Etoile, France) and/or matrix-assisted laser desorption/ionization time-of-flight mass spectrometry when required for confirmation. Testing was performed according to the laboratory’s standard operating procedures and manufacturer instructions.
Antimicrobial susceptibility testing was performed using an automated susceptibility testing system, Kirby-Bauer disk diffusion on Mueller-Hinton agar, and/or broth microdilution in cation-adjusted Mueller-Hinton broth, as appropriate for the agent and according to routine laboratory practice. Final susceptible, intermediate, and resistant categories were harmonized according to Clinical and Laboratory Standards Institute (CLSI) M100 breakpoints (34th edition, 2024).25 When results were potentially discordant or when broth microdilution was required for reliable interpretation, the final categorical result was based on the confirmatory method.
The antimicrobial agents analyzed were piperacillin-tazobactam, ceftazidime, cefepime, aztreonam, imipenem, meropenem, amikacin, gentamicin, ciprofloxacin, levofloxacin, and colistin/polymyxin B. P. aeruginosa ATCC 27853 was used as the quality-control strain. Quality-control results were required to fall within CLSI-specified acceptable ranges before patient isolate results were released; assays with out-of-range quality-control results were repeated according to laboratory policy.
Definition of Multidrug Resistance
MDR was defined according to the international consensus criteria proposed by Magiorakos et al as acquired non-susceptibility to at least one agent in three or more antimicrobial categories.1 Intermediate and resistant results were both considered non-susceptible for MDR classification. Antimicrobial categories included antipseudomonal penicillin/beta-lactamase inhibitor combinations, antipseudomonal cephalosporins, monobactams, carbapenems, aminoglycosides, fluoroquinolones, and polymyxins.
Statistical Analysis
Statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were assessed for normality using the Shapiro–Wilk test. Normally distributed variables were expressed as mean ± standard deviation and compared using the independent-samples t-test. Non-normally distributed variables were expressed as median and interquartile range (IQR) and compared using the Mann–Whitney U-test. Categorical variables were expressed as counts and percentages and compared using the chi-square test or Fisher’s exact test, as appropriate.
Multivariable logistic regression was performed with MDR status as the dependent variable. Candidate variables included those with P<0.10 in univariable analysis and variables considered clinically relevant a priori. To reduce overfitting given the limited number of MDR events, the number of variables retained in the model was restricted. Multicollinearity was assessed using variance inflation factors and pairwise correlation review; no variable with clinically problematic collinearity was retained in the same model. Model calibration was assessed using the Hosmer-Lemeshow goodness-of-fit test. Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were reported.
Because of the retrospective design and sample size, the regression results were interpreted as factors associated with MDR rather than as a validated prediction model. All tests were two-sided, and P<0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 112 eligible patients with clinically adjudicated P. aeruginosa otorhinolaryngological infection were included. The cohort comprised 61 males (54.5%), and the median age was 44 years (IQR, 34–54 years). Thirty-seven patients (33.0%) were classified as having MDR infection and 75 (67.0%) as having non-MDR infection.
Patients with MDR infection more frequently had postoperative indwelling devices or drainage than those with non-MDR infection (43.2% vs 20.0%, P=0.018). Hospital-acquired infection was also numerically more frequent in the MDR group (45.9% vs 28.0%, P=0.094). Other baseline factors, including sex, age, diabetes mellitus, immunosuppression or malignancy, prior hospitalization, intensive care unit admission, antimicrobial exposure, and carbapenem exposure, did not differ significantly between the groups in univariable comparisons (Table 1).
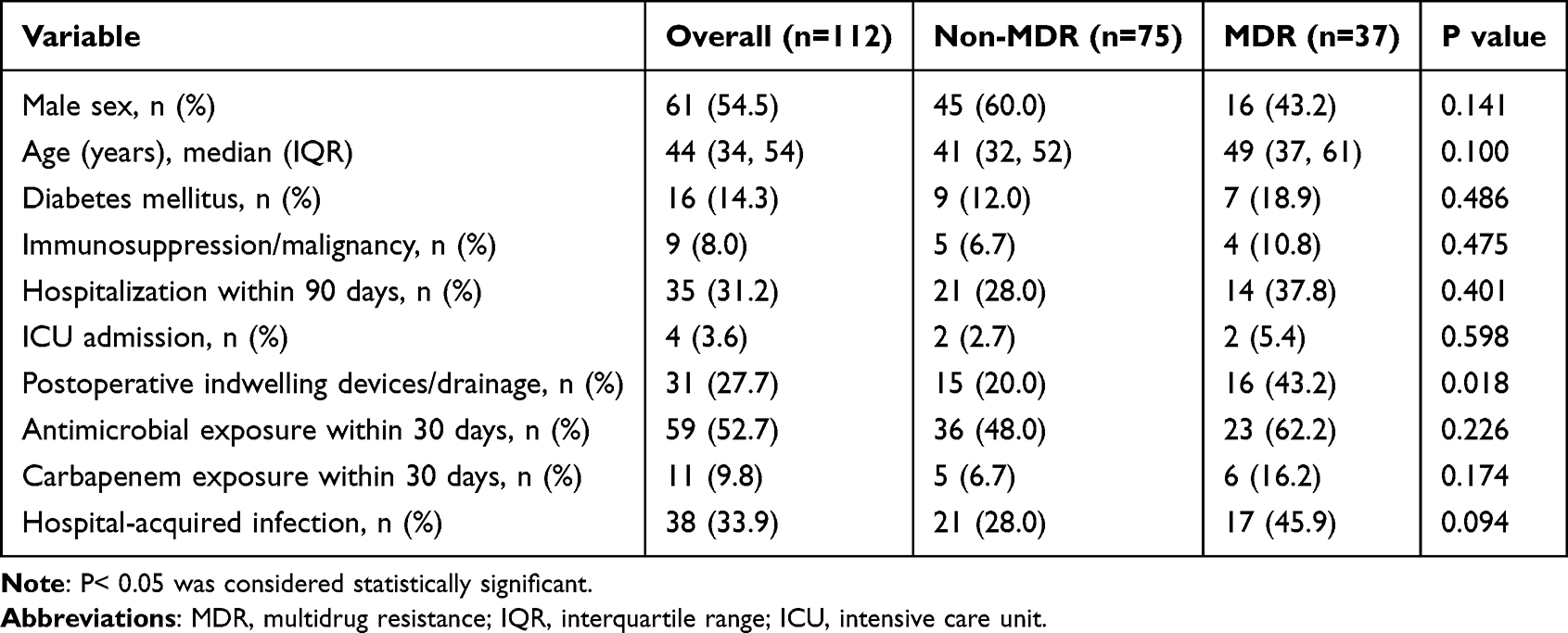 |
Table 1 Baseline Characteristics of Patients with MDR and Non-MDR P. Aeruginosa Infection |
Infection Sites and Specimen Sources
The external ear canal/external ear (31.2%), middle ear/mastoid (25.0%), and nasal cavity/paranasal sinuses (21.4%) were the leading anatomical sites, together accounting for 77.6% of infections. Ear discharge (32.1%) and ear canal swab (19.6%) were the most common specimen types. These findings indicate that ear-related infections represented the major clinical context for P. aeruginosa recovery in this otorhinolaryngology cohort (Figure 1).
 |
Figure 1 Clinical distribution of Pseudomonas aeruginosa infections in otorhinolaryngology at The First People’s Hospital of Yongkang, Eastern China (n=112). (A) Distribution of infection sites by number of patients. (B) Distribution of specimen types by number of isolates. |
Antimicrobial Susceptibility
Most isolates remained susceptible to several antipseudomonal agents, but resistance was observed across multiple drug classes. The highest susceptibility percentages were found for colistin/polymyxin B (95.5%), amikacin (84.8%), piperacillin-tazobactam (79.5%), gentamicin (77.7%), and meropenem (75.9%). The highest resistance percentages were observed for aztreonam (32.1%), levofloxacin (27.7%), ceftazidime (24.1%), imipenem (22.3%), ciprofloxacin (22.3%), cefepime (21.4%), and meropenem (21.4%) (Figure 2).
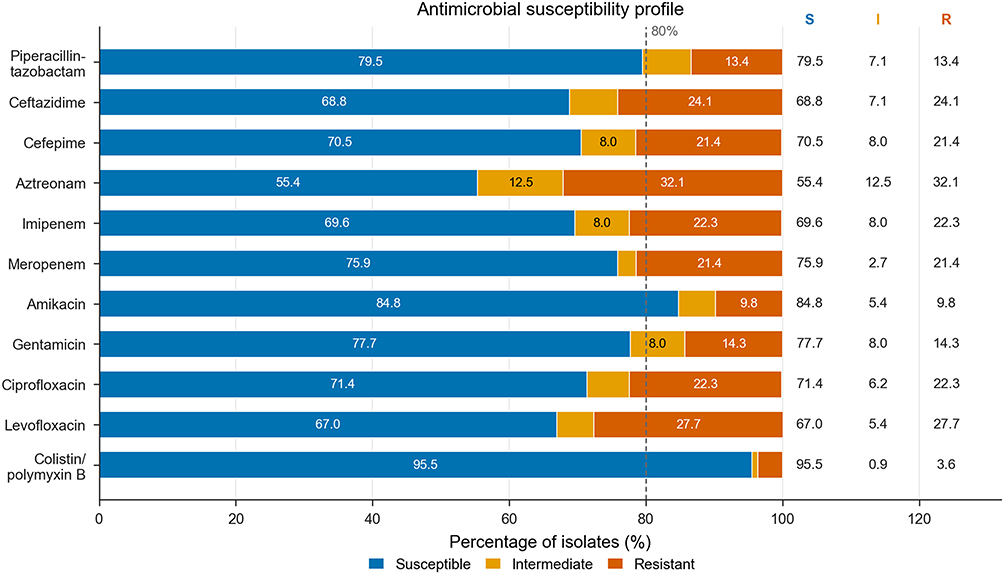 |
Figure 2 Antimicrobial susceptibility profile of 112 P. aeruginosa isolates. Horizontal stacked bars show the percentages of susceptible, intermediate, and resistant isolates for each antimicrobial agent. The dashed vertical line indicates an 80% susceptibility reference threshold for visual comparison only. Exact susceptible/intermediate/resistant percentages are displayed in the right-side columns. Susceptibility results were interpreted according to CLSI M100, 34th edition. |
The distribution of resistance across monobactams, fluoroquinolones, cephalosporins, and carbapenems suggests that empirical therapy based on a single high-resistance class may be unreliable in patients with risk factors for MDR. Conversely, the relatively high susceptibility to amikacin and colistin/polymyxin B should be interpreted in light of toxicity, route of administration, infection severity, and the need for susceptibility-guided rather than purely empirical use.
Factors Associated with Multidrug Resistance
Variables entered into the multivariable model included postoperative indwelling devices/drainage, hospital-acquired infection, carbapenem exposure within 30 days, diabetes mellitus, and age. Multicollinearity assessment did not identify clinically problematic collinearity among retained variables. The Hosmer-Lemeshow test suggested acceptable model calibration (chi-square=3.42, P=0.905).
Recent carbapenem exposure was independently associated with MDR (aOR 5.09, 95% CI 1.22–21.19, P=0.025). Postoperative indwelling devices or drainage (aOR 4.81, 95% CI 1.81–12.83, P=0.002) and hospital-acquired infection (aOR 2.52, 95% CI 1.02–6.23, P=0.046) were also independently associated with MDR. Age and diabetes mellitus were not statistically significant in the adjusted model (Figure 3). These variables should be regarded as associated factors rather than validated predictors.
 |
Figure 3 Multivariable logistic regression analysis of factors associated with multidrug-resistant P. aeruginosa infection. Squares represent adjusted odds ratios (aORs), and horizontal lines represent 95% confidence intervals (CIs). Blue markers indicate statistically significant associations (P< 0.05), and gray markers indicate non-significant associations. The vertical dashed line indicates aOR=1. Hosmer-Lemeshow test: chi-square=3.42, P=0.905. |
Clinical Outcomes
Overall clinical outcomes were cure in 63 patients (56.3%), improvement in 42 (37.5%), relapse in 5 (4.5%), treatment failure in 1 (0.9%), and death in 1 (0.9%). Compared with the non-MDR group, the MDR group had a longer median hospital stay (13 vs 10 days, P<0.001), more antimicrobial regimen modifications (median 2 vs 1, P=0.013), and higher CRP levels (38 vs 22 mg/L, P=0.003). WBC levels were not significantly different between groups (P=0.171).
Clinical success was lower in the MDR group than in the non-MDR group (86.5% vs 97.3%, P=0.038). Relapse occurred in five non-MDR cases and in no MDR case (6.7% vs 0%, P=0.038). Because the number of relapse events was very small, this finding should be interpreted cautiously and should not be regarded as evidence that MDR is protective against relapse (Figure 4).
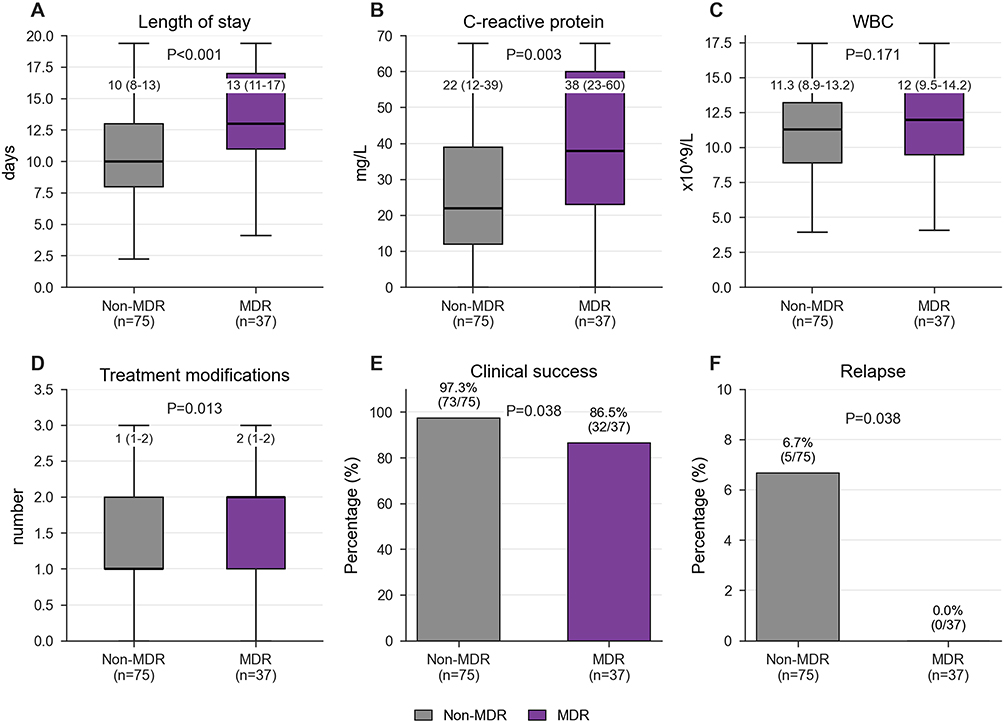 |
Figure 4 Comparison of clinical outcomes between MDR and non-MDR P. aeruginosa infection groups. (A–D) Box-and-whisker plots show reproducible simulated patient-level values for length of stay, C-reactive protein, WBC, and antimicrobial regimen modifications; the simulations were calibrated to the reported medians and interquartile ranges and are intended for visualization only. (E and F) Percentages and event counts are shown for clinical success and relapse. P values for continuous variables were calculated using the Mann–Whitney U-test, and P values for categorical variables were calculated using Fisher’s exact test. |
Discussion
This single-center retrospective cohort study provides specialty- and region-specific data on P. aeruginosa infections in otorhinolaryngology in Eastern China. The principal findings were as follows. First, P. aeruginosa infections were concentrated in the external ear, middle ear/mastoid, and sinonasal region. Second, one-third of clinically adjudicated infections were caused by MDR isolates. Third, resistance was not confined to one antimicrobial class; the highest resistance percentages were observed for aztreonam, levofloxacin, ceftazidime, and carbapenems. Fourth, recent carbapenem exposure, postoperative indwelling devices or drainage, and hospital-acquired infection were independently associated with MDR. Finally, MDR infection was associated with greater treatment complexity, reflected by longer hospitalization, more regimen changes, higher CRP levels, and lower clinical success.
The anatomical distribution observed in this study is clinically plausible. The external ear canal, middle ear, mastoid cavity, and sinonasal tract can provide favorable conditions for P. aeruginosa persistence when local barriers are disrupted by chronic inflammation, moisture, impaired drainage, prior surgery, or repeated antimicrobial exposure.5–11,26 Ear discharge and ear canal swabs accounted for more than half of all specimens, reinforcing the importance of careful otologic specimen collection before empirical escalation. The findings support the need for otorhinolaryngology-specific microbiological surveillance rather than exclusive reliance on hospital-wide or respiratory-dominant surveillance data.
The antimicrobial susceptibility profile has direct implications for empirical and step-down treatment decisions and should be interpreted in the context of national and regional surveillance data.13,17–21 Although susceptibility remained relatively high for colistin/polymyxin B, amikacin, and piperacillin-tazobactam, the observed resistance to aztreonam, levofloxacin, ceftazidime, and carbapenems indicates clinically meaningful cross-class resistance. In patients without MDR risk factors and with localized infection, local practice may reasonably emphasize culture acquisition, local treatment when appropriate, and narrow systemic therapy guided by severity and susceptibility results. In contrast, for patients with recent carbapenem exposure, postoperative drainage or devices, or hospital-acquired infection, empirical reliance on aztreonam, fluoroquinolone, or ceftazidime monotherapy may be inappropriate before susceptibility data are available. These patients should undergo early specimen collection, reassessment within 48–72 hours, de-escalation or escalation based on susceptibility results, and evaluation for source control, including drainage, debridement, and device management when clinically indicated.11,13
The association between carbapenem exposure and MDR is consistent with the biological plausibility of antimicrobial selective pressure. In P. aeruginosa, resistance may emerge through overlapping mechanisms, including reduced outer membrane permeability, efflux pump upregulation, AmpC overexpression, target-site changes, and acquisition of beta-lactamases.3,27–30 However, this study did not perform resistance gene detection or whole-genome sequencing; mechanistic explanations should therefore be interpreted as contextual rather than directly demonstrated by the present dataset.
For severe MDR or difficult-to-treat P. aeruginosa infections, newer antipseudomonal agents, including ceftolozane-tazobactam, ceftazidime-avibactam, and cefiderocol, have shown activity in recent in vitro and clinical studies.13,31–33 Nevertheless, these agents should not be extrapolated to uncomplicated localized otorhinolaryngological infections without considering disease severity, source control, local formulary availability, susceptibility results, and antimicrobial stewardship principles.
Postoperative indwelling devices or drainage showed the strongest association with MDR among procedural variables. This likely reflects a combination of biofilm formation, repeated healthcare contact, more severe or complicated disease, and greater cumulative antimicrobial exposure.2,26,34,35 For otorhinolaryngologists, this finding emphasizes that antimicrobial selection alone is insufficient. Clinical management should include early assessment of whether drainage tubes, wound packing, implants, or postoperative cavities are contributing to persistent infection and whether additional source control is required.
The outcome findings suggest that MDR infection increases treatment complexity even when mortality is uncommon, which is consistent with the broader epidemiological profile of resistant P. aeruginosa infections.15,16,19,36 The lower clinical success rate and longer hospitalization in the MDR group indicate that MDR has clinically meaningful consequences in this specialty. The relapse finding requires a more cautious interpretation. All five relapses occurred in the non-MDR group, which is counterintuitive if relapse is considered solely a function of resistance. The low event count makes this comparison unstable In otorhinolaryngology, relapse may be driven by chronic anatomical disease, persistent local inflammation, inadequate drainage, or incomplete source control rather than by antimicrobial resistance alone. Therefore, relapse should be interpreted separately from acute-phase treatment difficulty.
This study adds to existing surveillance literature by focusing on a defined specialty cohort, linking anatomical site and specimen-source information with MDR status and outcome indicators, and providing a local evidence base for risk-stratified management in a regional hospital in Eastern China. Rather than proposing a universal prediction model, the findings should be used pragmatically to identify patients who warrant earlier culture acquisition, closer reassessment, infection-control attention, and susceptibility-guided antimicrobial adjustment.
Several limitations should be acknowledged. First, this was a single-center retrospective study with 112 patients and 37 MDR events. Although consecutive eligible cases were included, the sample size limits precision, and the findings may not be generalizable to other regions or hospital settings. Second, because the study was microbiology-based, the denominator of all suspected otorhinolaryngological infections was unavailable; selection bias cannot be excluded. Third, the number of events per variable in the multivariable model was limited, and the results should be interpreted as associations rather than validated predictors. Fourth, susceptibility testing was performed using routine clinical laboratory methods, and the use of more than one testing approach may introduce variability despite CLSI harmonization and quality-control procedures.25 Fifth, molecular mechanisms of resistance, clonal transmission, topical antimicrobial exposure, detailed surgical procedures, and adequacy of source control were not fully characterized. Sixth, the one-year study period was insufficient for evaluating temporal trends in resistance.
Future studies should use multicenter prospective designs, include predefined screening logs, collect detailed local treatment and source-control variables, and incorporate molecular epidemiology to distinguish clonal spread from independent resistance emergence. Such data would support more robust specialty-specific algorithms for the management of P. aeruginosa infections in otorhinolaryngology.
Conclusions
In this regional single-center cohort from Eastern China, P. aeruginosa otorhinolaryngological infections were mainly distributed in the external ear, middle ear/mastoid, and sinonasal region, and MDR accounted for one-third of cases. Recent carbapenem exposure, postoperative indwelling devices or drainage, and hospital-acquired infection were independently associated with MDR, which was accompanied by longer hospitalization, more treatment modifications, higher CRP levels, and lower clinical success. These findings support early specimen collection, careful differentiation of infection from colonization, risk-stratified empirical therapy, prompt susceptibility-guided adjustment, and source-control assessment in high-risk otorhinolaryngology patients.
Abbreviations
aOR, adjusted odds ratio; CI, confidence interval; CLSI, Clinical and Laboratory Standards Institute; CRP, C-reactive protein; ICU, intensive care unit; IQR, interquartile range; MALDI-TOF MS, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry; MDR, multidrug-resistant or multidrug resistance; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; WBC, white blood cell count.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available because of patient privacy and institutional data governance requirements, but de-identified data may be available from the corresponding author upon reasonable request and with appropriate institutional approval.
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board of The First People’s Hospital of Yongkang (approval number: YKSDYRMYYEC2024-KT-HS-013). The requirement for informed consent was waived by the Institutional Review Board because this was a retrospective study using de-identified clinical and laboratory data. The study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Public Welfare Science and Technology Project of Jinhua Science and Technology Bureau, Zhejiang Province, China (Grant No. 2024-4-313). The funder had no role in the study design, data collection, data analysis, interpretation of results, manuscript preparation, or the decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–11. doi:10.1111/j.1469-0691.2011.03570.x
2. Alhede M, Bjarnsholt T, Givskov M, Alhede M. Pseudomonas aeruginosa biofilms: mechanisms of immune evasion. Adv Appl Microbiol. 2014;86:1–40. doi:10.1016/B978-0-12-800262-9.00001-9
3. Lister PD, Wolter DJ, Hanson ND. Antibacterial-resistant Pseudomonas aeruginosa: clinical impact and complex regulation of chromosomally encoded resistance mechanisms. Clin Microbiol Rev. 2009;22(4):582–610. doi:10.1128/CMR.00040-09
4. Qin S, Xiao W, Zhou C, et al. Pseudomonas aeruginosa: pathogenesis, virulence factors, antibiotic resistance, interaction with host, technology advances and emerging therapeutics. Signal Transduct Target Ther. 2022;7(1):199. doi:10.1038/s41392-022-01056-1
5. Dohar JE, Hebda PA, Veeh R, et al. Mucosal biofilm formation on middle-ear mucosa in a nonhuman primate model of chronic suppurative otitis media. Laryngoscope. 2005;115(8):1469–1472. doi:10.1097/01.mlg.0000172036.82897.d4
6. Roland PS, Stroman DW. Microbiology of acute otitis externa. Laryngoscope. 2002;112(7):1166–1177. doi:10.1097/00005537-200207000-00005
7. Mansoor T, Musani MA, Khalid G, Kamal M. Pseudomonas aeruginosa in chronic suppurative otitis media: sensitivity spectrum against various antibiotics in Karachi. J Ayub Med Coll Abbottabad. 2009;21(2):120–123.
8. Brook I. Microbiology of chronic rhinosinusitis. Eur J Clin Microbiol Infect Dis. 2016;35(7):1059–1068. doi:10.1007/s10096-016-2640-x
9. Artono A, Purnami N, Handoko E, Widodo ADW, Juniastuti J. Pseudomonas aeruginosa in chronic suppurative otitis media. Infect Chemother. 2025;57(1):63–71. doi:10.3947/ic.2024.0062
10. Kang DW, Lee HJ, Bang JH, et al. Bacteriology and trends of antimicrobial resistance of Pseudomonas aeruginosa and methicillin-resistant Staphylococcus aureus in otitis media: a retrospective data analysis. Clin Otolaryngol. 2023;48(6):872–880. doi:10.1111/coa.14086
11. Bhutta MF, Leach AJ, Brennan-Jones CG. Chronic suppurative otitis media. Lancet. 2024;403(10441):2339–2348. doi:10.1016/S0140-6736(24)00259-9
12. World Health Organization. WHO Bacterial Priority Pathogens List, 2024: Bacterial Pathogens of Public Health Importance to Guide Research, Development and Strategies to Prevent and Control Antimicrobial Resistance. Geneva: World Health Organization; 2024.
13. Tamma PD, Heil EL, Justo JA, Mathers AJ, Satlin MJ, Bonomo RA. Infectious Diseases Society of America 2024 guidance on the treatment of antimicrobial-resistant gram-negative infections. Clin Infect Dis. 2024. doi:10.1093/cid/ciae403
14. Raman G, Avendano EE, Chan J, Merchant S, Puzniak L. Risk factors for hospitalized patients with resistant or multidrug-resistant Pseudomonas aeruginosa infections: a systematic review and meta-analysis. Antimicrob Resist Infect Control. 2018;7:79. doi:10.1186/s13756-018-0370-9
15. Peng Y, Bi J, Shi J, et al. Multidrug-resistant Pseudomonas aeruginosa infections pose growing threat to health care-associated infection control in the hospitals of Southern China: a case-control surveillance study. Am J Infect Control. 2014;42(12):1308–1311. doi:10.1016/j.ajic.2014.08.006
16. Peng Y, Shi J, Bu T, et al. Alarming and increasing prevalence of multidrug-resistant Pseudomonas aeruginosa among healthcare-associated infections in China: a meta-analysis of cross-sectional studies. J Glob Antimicrob Resist. 2015;3(3):155–160. doi:10.1016/j.jgar.2015.04.001
17. Guo Y, Ding L, Han R, et al. Antimicrobial resistance profile of clinical isolates from hospitals across China: CHINET 2024 surveillance report. One Health Adv. 2025;3:23. doi:10.1186/s44280-025-00092-0
18. Lyu J, Chen H, Bao J, et al. Clinical distribution and drug resistance of Pseudomonas aeruginosa in Guangzhou, China from 2017 to 2021. J Clin Med. 2023;12(3):1189. doi:10.3390/jcm12031189
19. Xiao S, Liang X, Han L, Zhao S. Incidence, antimicrobial resistance and mortality of Pseudomonas aeruginosa bloodstream infections among hospitalized patients in China: a retrospective observational multicenter cohort study from 2017 to 2021. Front Public Health. 2024;11:1294141. doi:10.3389/fpubh.2023.1294141
20. Xiao M, Wang Y, Yang QW, et al. Antimicrobial susceptibility of Pseudomonas aeruginosa in China: a review of two multicentre surveillance programmes, and application of revised CLSI susceptibility breakpoints. Int J Antimicrob Agents. 2012;40(5):445–449. doi:10.1016/j.ijantimicag.2012.07.002
21. Narimisa N, Keshtkar A, Dadgar-Zankbar L, Moradali MF, Razavi S, Hashemi A. Prevalence of colistin resistance in clinical isolates of Pseudomonas aeruginosa: a systematic review and meta-analysis. Front Microbiol. 2024;15:1477836. doi:10.3389/fmicb.2024.1477836
22. De Sanctis V, Soliman AT, Daar S, et al. Retrospective observational studies: lights and shadows for medical writers. Acta Biomed. 2022;93(5):e2022319. doi:10.23750/abm.v93i5.13179
23. Von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
24. Ministry of Health of the People’s Republic of China. Diagnostic criteria for nosocomial infections (trial). Zhonghua Yi Xue Za Zhi. 2001;81(5):314–320. Chinese.
25. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. 34th Ed. CLSI Supplement M100. Wayne, PA: Clinical and Laboratory Standards Institute; 2024.
26. de Kievit TR. Quorum sensing in Pseudomonas aeruginosa biofilms. Environ Microbiol. 2009;11(2):279–288. doi:10.1111/j.1462-2920.2008.01792.x
27. Malkocoglu G, Aktas E, Bayraktar B, Otlu B, Bulut ME. VIM-1, VIM-2, and GES-5 carbapenemases among Pseudomonas aeruginosa isolates at a tertiary hospital in Istanbul, Turkey. Microb Drug Resist. 2017;23(3):328–334. doi:10.1089/mdr.2016.0012
28. Terzi HA, Kulah C, Atasoy AR, Ciftci IH. Investigation of OprD porin protein levels in carbapenem-resistant Pseudomonas aeruginosa isolates. Jundishapur J Microbiol. 2015;8(12):e25952. doi:10.5812/jjm.25952
29. Oliver A, Mulet X, Lopez-Causape C, Juan C. The increasing threat of Pseudomonas aeruginosa high-risk clones. Drug Resist Updat. 2015;21-22:41–59. doi:10.1016/j.drup.2015.08.002
30. Elfadadny A, Ragab RF, AlHarbi M, et al. Antimicrobial resistance of Pseudomonas aeruginosa: navigating clinical impacts, current resistance trends, and innovations in breaking therapies. Front Microbiol. 2024;15:1374466. doi:10.3389/fmicb.2024.1374466
31. Weber C, Schultze T, Göttig S, Kessel J, Kempf VAJ, Wichelhaus TA. Antimicrobial activity of ceftolozane-tazobactam, ceftazidime-avibactam, and cefiderocol against multidrug-resistant Pseudomonas aeruginosa recovered at a German university hospital. Microbiol Spectr. 2022;10(5):e01697–22. doi:10.1128/spectrum.01697-22
32. Gill CM, Santini D, Nicolau DP, ERACE-PA Global Study Group. In vitro activity of cefiderocol against a global collection of carbapenem-resistant Pseudomonas aeruginosa with a high level of carbapenemase diversity: the ERACE-PA Global Surveillance Programme. J Antimicrob Chemother. 2024;79(2):412–416. doi:10.1093/jac/dkad396
33. Shields RK, Abbo LM, Ackley R, et al. Effectiveness of ceftazidime-avibactam versus ceftolozane-tazobactam for multidrug-resistant Pseudomonas aeruginosa infections in USA (CACTUS): a multicentre, retrospective, observational study. Lancet Infect Dis. 2025;25(5):574–584. doi:10.1016/S1473-3099(24)00648-0
34. Li QY, Liu B, Liu L. Successfully controlling the incidence of multidrug-resistant Pseudomonas aeruginosa through antibiotic stewardship and infection control programmes at a Chinese university hospital. J Clin Pharm Ther. 2021;46(5):1357–1366. doi:10.1111/jcpt.13446
35. Khedr A, Mathew BM, Mushtaq H, et al. Pseudomonas infection reduction in the ICU: a successful multidisciplinary quality improvement project. Infez Med. 2022;30(4):577–586. doi:10.53854/liim-3004-13
36. Paterson DL. The epidemiological profile of infections with multidrug-resistant Pseudomonas aeruginosa and Acinetobacter species. Clin Infect Dis. 2006;43(Suppl 2):S43–S48. doi:10.1086/504476
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Successful Treatment of Fournier’s Gangrene in Child with Relapsed Acute Lymphoblastic Leukemia: Case Report and Review of the Literature
Kołodziejczyk J, Czarny J, Królak S, Rutkowska S, Moryciński S, Mańkowski P, Bartkowska-Śniatkowska A, Wachowiak J, Derwich K, Zając-Spychała O
Infection and Drug Resistance 2025, 18:1667-1673
Published Date: 1 April 2025
Development and Validation of a Nomogram for Predicting Multidrug-Resistant Pseudomonas Aeruginosa Pneumonia in Hospitalized Patients
Du Z, Yang D, Pan L, Zeng Q, Chen X
Infection and Drug Resistance 2025, 18:3543-3559
Published Date: 16 July 2025
Community-Acquired Severe Pseudomonas Aeruginosa pneumonia: A Case Report and Review of the Literature
Zhang J, Xie M, Ni R, Zhong M
Infection and Drug Resistance 2025, 18:6185-6190
Published Date: 26 November 2025