Back to Journals » Journal of Inflammation Research » Volume 18
Clinical Characteristics of CARD14-Associated Papulosquamous Eruption and Evaluation of Therapeutic Efficacy of Secukinumab
Authors Zhao X ![]() , Wang Z, Chen Y
, Wang Z, Chen Y ![]() , Xiang X, Liu Y, Miao C, Xu Z
, Xiang X, Liu Y, Miao C, Xu Z ![]()
Received 18 February 2025
Accepted for publication 23 April 2025
Published 23 May 2025 Volume 2025:18 Pages 6597—6605
DOI https://doi.org/10.2147/JIR.S519554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Xinrong Zhao, Zhaoyang Wang, Yunliu Chen, Xin Xiang, Yuanxiang Liu, Chaoyang Miao, Zigang Xu
Department of Dermatology, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health and KeyLaboratory of Major Diseases in Children, Ministry of Education, Beijing, People’s Republic of China
Correspondence: Zigang Xu, Department of Dermatology, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health and Key Laboratory of Major Diseases in Children, Ministry of Education, Beijing, People’s Republic of China, Tel +8601013370110521, Email [email protected]
Background: CARD14-associated papulosquamous eruption (CAPE) is a spectrum of disease exhibited by patients with CARD14 mutations, which are rare and have a wide variety of clinical manifestations. Patients usually have limited response to traditional therapies.
Methods: We retrospectively analyzed a case series of 8 patients with CAPE in China. Whole-exome sequencing (WES) was performed in all patients to identify the mutation type. Three patients received the treatment of secukinumab with a 52-week follow-up period. They achieved 84.6%, 76.9%, and 68.8% improvement in PASI score, respectively.
Results: The study identified three new variants in CARD14 that had not been previously reported: c.392_397del, c.391_392delinsTT, and c.-280C>T. Three patients with different clinical manifestations showed good response to secukinumab.
Conclusion: The mutation types in CARD14-associated papulosquamous eruption were various. IL-17A inhibitors, such as secukinumab, can be an alternative treatment option for pediatric patients with CAPE.
Keywords: CARD14-associated papulosquamous eruption, CARD14 mutation, biological treatments, secukinumab
Introduction
CARD14 is one of the genes associated with psoriasis susceptibility, and to date, more than 20 variants have been detected in psoriasis patients.1–3 A gain-of-function mutation in CARD14 can activate the NF-kB signaling pathway, resulting in increased production of inflammatory cytokines and chemokines. This cascade promotes the recruitment and differentiation of inflammatory cells, ultimately contributing to skin inflammation.2 Previous studies have showed that patients with CARD14 mutation can present with various conditions, including psoriasis vulgaris (PV), generalized pustular psoriasis (GPP), palmoplantar pustular psoriasis (PPP), psoriasis arthritis (PsA) and pityriasis rubra pilaris (PRP).4 In 2018, the term “CARD14-associated papulosquamous eruption (CAPE)” was proposed to describe this spectrum of disease.5 However, patients with CARD14 mutation typically present with an early age of onset (primarily before 1 year of age), prominent facial involvement (cheeks, chin and ears), a frequent family history of psoriasis or PRP, and a limited response to conventional topical and systemic therapies. These characteristics distinguish them from patients with more common forms of psoriasis and acquired PRP.6 Given the rarity of these diseases and the challenges in treatment, there is a need for further exploration of effective treatment methods. In this study, we report on eight pediatric patients of CAPE from our department and observed the effects of secukinumab in three of these patients over 52 weeks.
Materials and Methods
Patients
This retrospective study included eight patients who were clinically and genetically diagnosed with CAPE by two expert genetic dermatologists at the Department of Dermatology, Beijing Children’s Hospital. We used the Psoriasis Area and Severity Index (PASI) score to assess the severity of the lesions. Three patients were treated with secukinumab and were followed up at week 0, week 12, week 24, and week 52, respectively, to evaluate the therapeutic efficacy and adverse reactions of the treatment.
Histopathology
For histopathology analysis, biopsies from affected skin were fixed with 4% formaldehyde overnight, then dehydrated and embedded in paraffin. The tissue sections were stained with hematoxylin and eosin following standard procedures.
DNA Extraction, Sequencing, and Bioinformatic Analysis
Approximately 2 mL peripheral blood (EDTA anticoagulant) was collected from the proband and her parents, and genomic DNA was extracted using QIAamp Blood Midi Kit (QIAGEN, Germany) according to the instructions. For one patient with linear erythematous scales, DNA with extracted from both peripheral blood and the lesion. An Illumina Novaseq 6000 sequencer (Illumina, San Diego, CA, USA)/DNBSEQ (DNBSEQ-T7) (MGI, Shenzhen, China) was used with 150 bp paired-end reads. After sequencing, the raw data were saved in FASTQ format. Quality control (QC) filters were applied to remove reads with low quality. Then, the clean reads were assembled and spliced using the second-generation sequencing analysis platform provided by MyGenostics and the coverage and sequencing quality of the target region were evaluated. Finally, flash analysis platform was used to analyze the pathogenicity of variation, and the possible variation loci were determined. The pathogenicity of variation loci was also analyzed according to ACMG (American College of Medical Genetics and Genomics) genetic variation classification criteria and guidelines. An ABI3730xl sequencer (Applied Biosystems, USA) was used to apply the Sanger sequencing method, and the results were compared to the capture sequencing results.
Results
The clinical characteristics of eight patients with CAPE were exhibited in Table 1.
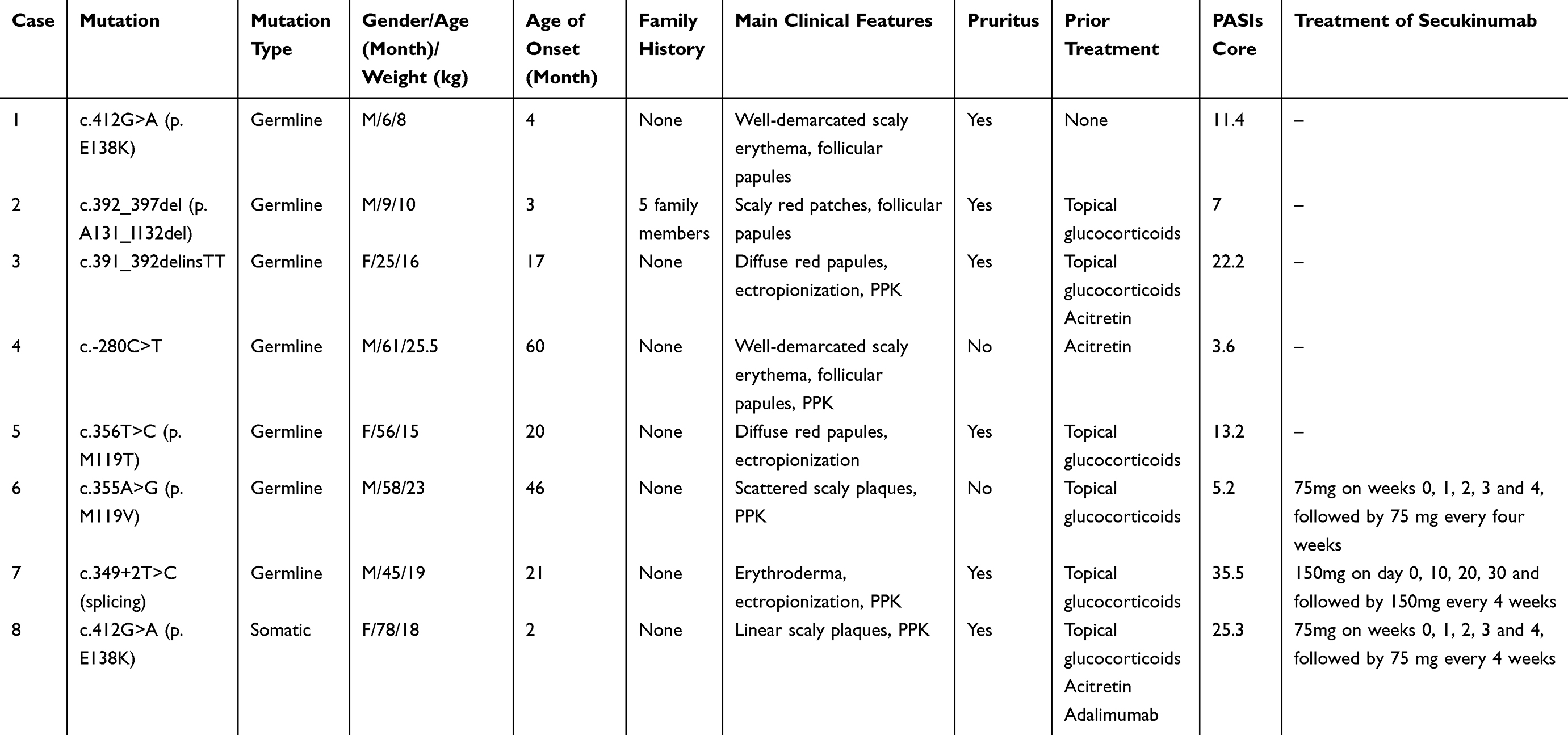 |
Table 1 Clinical Characteristics of 8 Patients with CAPE |
Among the 8 patients, 62.5% (5/8) are male and 37.5% (3/8) are female. The median age of onset is 18.5 months. One patient (patient 2) has a family history and five members of her family, including her mother, maternal uncle, great-grandmother, great-aunt, and her cousin, had similar conditions. In terms of clinical manifestations, among the 8 patients, 75% (6/8) presented with red plaques covered with scales (P1-P6), 12.5% (1/8) presented with erythroderma (P7), and 12.5% (1/8) presented with linear erythema distributed along the Blaschko lines (P8). In addition, 62.5% (5/8) of the patients presented with palmoplantar keratoderma (P3, P4, P6, P7, P8), 37.5% (3/8) had follicular papules (P1, P2, P4), and 37.5% (3/8) had ectropionization (P3, P5, P7). 75% (6/8) of the patients experienced itching to varying degrees. Skin biopsies were performed on 87.5% (7/8) patients. Histopathologically, 57.1% (4/7) of the patients showed fused parakeratosis of epidermis, 14.3% (1/7) had focal parakeratosis, and 28.6% (2/7) had alternating parakeratosis and hyperkeratosis, which is the typical manifestation of pityriasis rubra pilaris. All patients had perivascular infiltration of lymphocytes and histiocytes in the superficial dermis. The clinical and pathological images of patient 1, 2, and 4 are shown in Figures 1–3, those of patient 6 in Figure 4a and b, and those of patient 7 in Figure 5a and b.
 |
Figure 1 Well-demarcated thin scaly erythema on lower limbs of patient 1 (a). Psoriasiform epidermal hyperplasia with fused parakeratosis and scattered lymphocyte infiltration in the superficial dermis (b). |
 |
Figure 2 Red plaques distributed on lower limbs of patient 2 (a). Psoriasiform epidermal hyperplasia with fused parakeratosis and a slight infiltration of lymphocytes around small vessels in the superficial dermis (b). |
 |
Figure 3 Follicular papules around the eyes and mouth, trunk, and well-demarcated scaly erythema on elbows of patient 4 (a and b). Alternating hyperkeratosis and parakeratosis and a slight infiltration of lymphocytes around small vessels in the superficial dermis (c). |
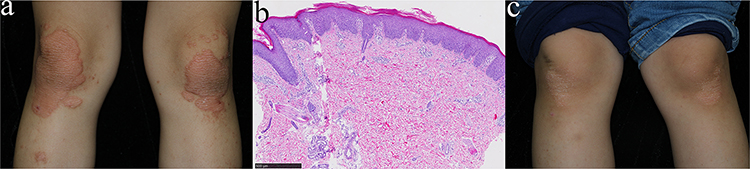 |
Figure 4 Well-demarcated erythematous on the knees of patient 6 (a). Psoriasiform epidermal hyperplasia with fused parakeratosis and a slight infiltration of lymphocytes in the superficial dermis (b). Significant improvement after the treatment of secukinumab for 12 weeks (c). |
 |
Figure 5 Diffuse erythema on the back of patient 7 (a). Acanthosis with fused parakeratosis, normal granular layer, and keratin plug in hair follicle (b). A marked resolution was observed after the treatment of secukinumab for 6 months (c). |
Peripheral blood whole exon sequencing (WES) was performed in all patients and seven gain-of-function variants were detected: CARD14 c.412G>A, c.392_397del, c.391_392delinsTT, c.-280C>T, c.356T>C, c.355A>G, and c.349+2T>C. Patients 1–7 all had germline mutations. A somatic mutation of CARD14 was detected in patient 8 with a variant allele load of 24% in affected skin and 4% in blood because of the symmetrical erythematous plaques with scales following the lines of Blaschko.
Eight patients used different treatment methods, and the treatment effects varied. Patient 1 did not receive any medication treatment and only used emollients, which showed mild relief in a short period. Patient 2 and Patient 5 refused systemic treatment, and topical glucocorticoids showed no significant efficacy. Patient 3 was treated with acitretin at a dosage of 0.3mg/kg/d. After 16 weeks, both the lesions and pruritus improved, with the PASI score decreasing from 22.2 to 10.5. However, at subsequent follow-up visits, there was no further improvement in the lesions. Patient 4 was also treated with acitretin at a dosage of 0.4mg/kg/d. After 14 weeks of treatment, there was improvement in the lesions on face, limbs and trunk, although the palmoplantar keratoderma remained unchanged. Patients 6–8 ultimately received treatment with secukinumab. Patients 6 and 8 received secukinumab treatment according to the standard protocol for moderate-to-severe psoriasis. For Patient 7, who presented with extensive skin lesions involving 100% of the body surface area, we deviated from conventional dosing based on prior clinical experience indicating that such patients are challenging to treat and often require higher doses. To achieve rapid inflammatory control, we administered 150 mg of secukinumab. However, to balance therapeutic efficacy with safety considerations, the intensive dosing interval was extended to 10 days. Patient 6 was treated with secukinumab, receiving a dosage of 75mg on weeks 0, 1, 2, 3, and 4, followed by 75 mg every four weeks. Significant improvement was observed after 12 weeks (Figure 4c). The lesions showed persistent improvement throughout the 52-week treatment period with a PASI score from 5.2 to 0.8 and BSA from 15% to 1% although a mild recurrence occurred at 24 weeks due to an upper respiratory tract infection. Patient 7 was treated with secukinumab, starting with an initial dose of 150mg on days 0, 10, 20, and 30, followed by 150mg every four weeks. Initially, the skin lesions worsened after four weeks of treatment. However, a marked resolution of lesions and reduction in itching were observed after 24 weeks (Figure 5c). The lesions continued to show persistent improvement throughout the 52-week treatment period with a PASI from 35.5 to 8.2 and BSA from 100% to 65%. Patient 8 is a case we reported previously.7 She received treatment with topical medications and acitretin, but no therapeutic effect was observed. Then, the treatment was switched to adalimumab for three months, which only led to mild improvement. However, he demonstrated a positive response to the treatment of secukinumab over the 52-week period with a PASI from 25.3 to 7.9 and BSA from 65% to 43%. The changes of PASI scores following secukinumab treatment in 3 patients were presented in Figure 6.
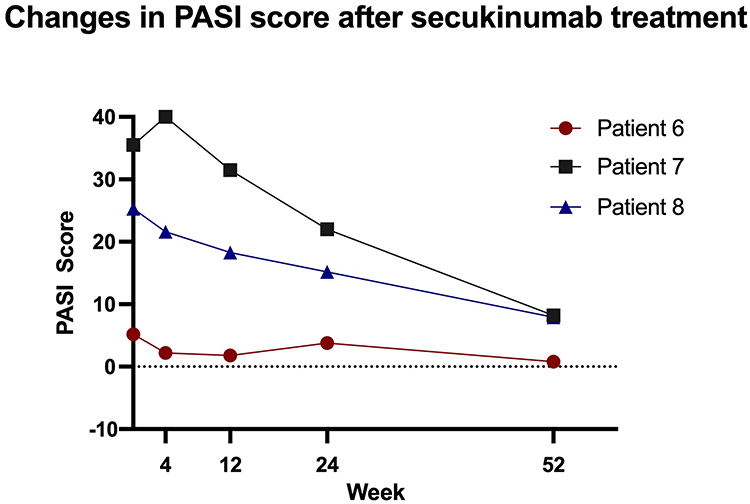 |
Figure 6 The severity changes of the disease in three patients with the treatment of secukinumab. |
Discussion
CAPE was proposed in 2018 to describe the spectrum of disease exhibited by patients with CARD14 mutations, which display characteristics of both psoriasis and PRP. The shared characteristic features of CAPE include early age of onset; prominent involvement of the cheeks, chin, and ears; family history of psoriasis or PRP; minimal response to conventional topical and systemic psoriasis therapies; and improvement with ustekinumab.5 CARD14, located on 17q25, encodes the protein cysteine protease recruitment domain family-14 (also known as the caspase recruitment domain and membrane-associated guanylate kinase-like protein 2, or CARMA2), primarily expressed in keratinocytes.8 CARD14 mutation can activate nuclear factor-κB (NF-κB) signaling pathway, leading to the recruitment and differentiation of inflammatory cells.9 Previous studies have revealed that the skin hyperplasia and inflammation observed in CARD14E138A/+ mice closely resemble human psoriasis at clinical, historical, and transcriptomic levels. Increased expression of critical cytokines, such as IL-17a, IL-23, IL-17c, TNF-α and IL-22, suggests that treatments targeting these cytokines could be effective.10
In this study, we aimed to characterize eight pediatric patients with CARD14 mutation. Six patients experienced onset of symptoms at or before one year of age, while the other two at ages of three and five years. These patients presented with psoriasiform and pityriasis rubra pilaris-like manifestations, such as scaly erythema, follicular papules and palmoplantar keratoderma (PPK). Additionally, we observed that three patients (P3, P5, P7) exhibited ectropionization, a clinical manifestation that has been less frequently reported. A patient with erythroderma has previously been reported to exhibit ectropionization,11 and we suggested that chronic and severe inflammatory stimulation may reduce eyelid tissue elasticity and induce scar contracture. These changes could alter eyelid positioning, ultimately leading to ectropion. In addition to the above clinical manifestations, we found that a recent study reported a case of a Taiwanese female patient carrying the CARD14 c.349 +5G > A mutation, who developed multiple cutaneous malignancies following PUVA and etanercept therapy. This suggests that phototherapy, immunosuppression, and mutation-related NF-κB pathway abnormalities may synergistically promote carcinogenesis.12
We identified three CARD14 variants that had not been previously reported: c.392_397del, c.391_392delinsTT, and c.-280C>T. The mutation of c.392_397del in patient 2 could lead to changes in protein length and was not found in the normal population. Notably, six family members had a history of similar disease, suggesting that this variant is likely pathogenic. The mutation of c.-280C >T in patient 4 suggested that CARD14 mutation in the intron region may also cause disease. The mutation is located in the promoter region (c.-280C>T), which may affect transcription factor binding or promoter activity, thereby regulating CARD14 expression. This mutation has not been observed in population databases, and the patient’s clinical manifestations align with CAPE, suggesting a genotype-phenotype correlation. Based on the above evidence, we suppose that this mutation may be pathogenic. Meanwhile, the mutation of c.349+2T>C has in patient 7 suggested that splicing alteration may cause severe erythroderma. The pathogenic mechanism of c.349+2T>C may involve both splicing alterations and functional domain disruption. Prior studies indicate that c.349+1G>A (intron 3 splice donor site) and the adjacent c.349G>A mutation induce aberrant exon 3 splicing, directly impairing critical functional domains in psoriasis and GPP.3,4 We propose that c.349+2T>C similarly disrupts key domains via analogous splicing defects, thereby driving pathogenesis.
Recent studies on pathogenesis of CAPE have shown that IL-12/23 inhibitors, such as ustekinumab and risankizumab, can be effective treatments.5,12,13 However, such patients require individualized drug administration. For example, higher dosages of ustekinumab (ranging from 0.75mg to 2 mg/kg) or reduced intervals between administrations (from every 12 weeks to every 8 weeks) have been necessary to achieve complete or near-complete resolution of the dermatosis.5,6,14–16 Risankizumab is an IL-23 blocker. Recent studies have shown that two pediatric CAPE patients were successfully treated with risankizumab. However, while some patients experienced rapid initial improvement with risankizumab, most struggled to sustain efficacy over time, potentially requiring higher doses, shorter treatment intervals, or even switching to other biologic therapies.17
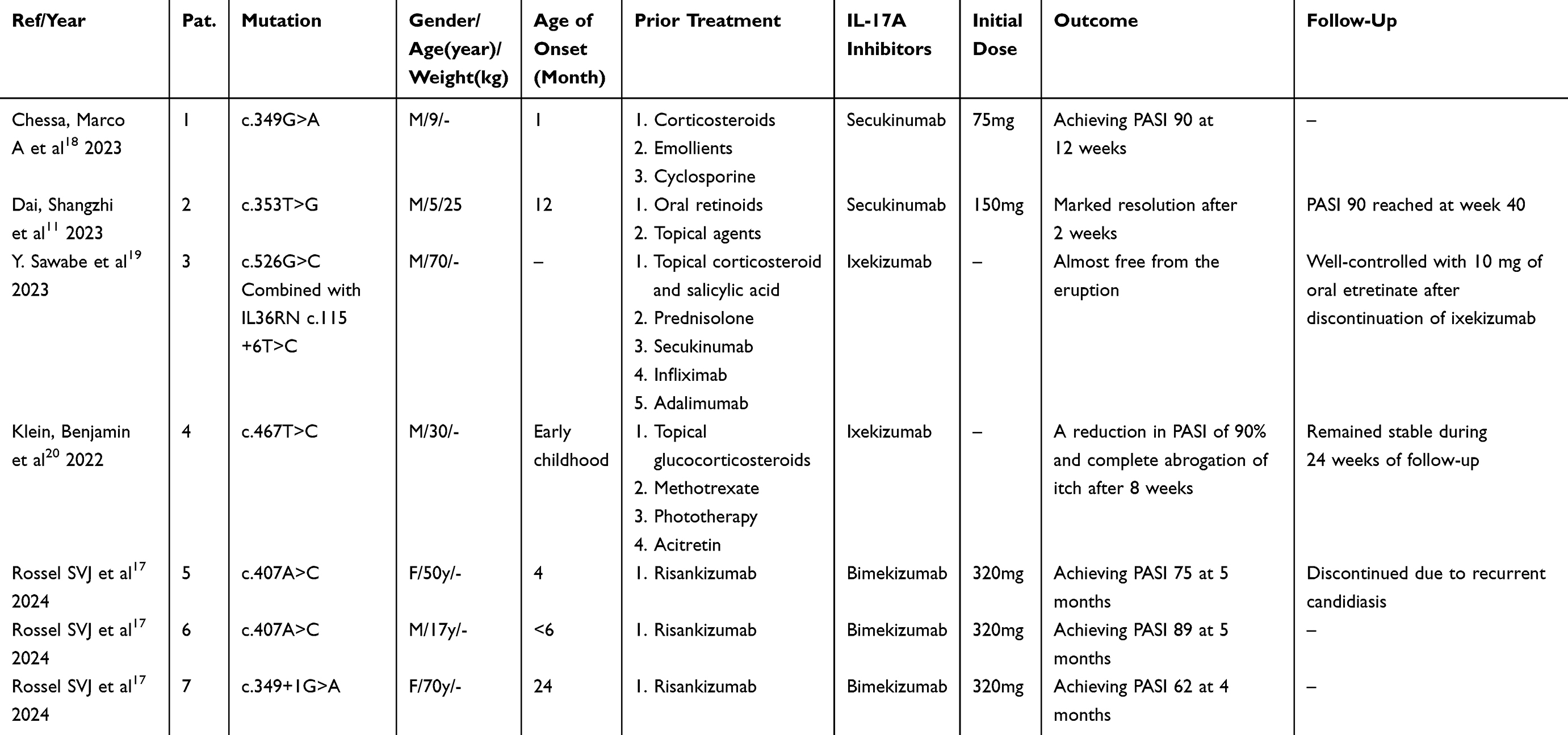 |
Table 2 Summary of the Patients with CAPE Treated with IL-17A Inhibitors in Previous Studies |
The efficacy of anti-IL-17 treatments, particularly in pediatric patients, has been less extensively studied. To date, a total of ten patients have been treated with IL-17 inhibitors (including three from our study), with seven cases reported in previous literatures (Table 2).11,17–20 Among these seven patients, six presented with psoriasis-like scaly plaques, one with GPP, one with PRP-like pink-orange scaly plaques, and two with erythroderma. Eight of these patients reported pruritus. Following the treatment with IL-17A inhibitors (five pediatric patients receiving secukinumab, two adult patients receiving ixekizumab and three adult patients receiving bimekizumab, an IL-17A/F inhibitor), there was significant improvement in skin lesions, and pruritus was alleviated or resolved. Although one patient was treated with secukinumab during treatment and eventually improved with ixekizumab,19 this may have been due to the sudden discontinuation of oral prednisone at the same time as the addition of secukinumab.
Our findings suggest that IL-17A inhibitors can be effective for this disease, addressing multiple clinical manifestations associated with CARD14 mutations and improving both skin lesions and itch in patients. Therefore, IL-17A inhibitors, particularly secukinumab, represent a promising treatment option for these patients, especially those with low body weight. Based on our experience, patients can be treated with secukinumab at a dosage of 75mg on weeks 0, 1, 2, 3, and 4, followed by 75mg every four weeks, or with 150mg on days 0, 10, 20, 30, followed by 150mg every four weeks.
Conclusion
Our study identifies 4 new variants in CARD14 and demonstrates the potential efficacy of IL-17 inhibitors, such as secukinumab, as an alternative treatment option for pediatric patients with CAPE. These findings provide valuable insight into both the clinical spectrum of the disease and possible therapeutic approaches. We hope that our experience with this group of patients will help identify and successfully treat affected individuals, while expanding our understanding of the range of clinical features associated with CAPE.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics and Consent Statements
Informed consent was obtained from the patient’s guardians for the photographing and medication treatment of the patients. The study complies with the Declaration of Helsinki. This study was approved by the ethics committee of Beijing Children’s Hospital, Capital Medical University (2024-E-139-R).
Funding
The study was funded by the National Key R&D Program of China (2023YFC2508101) and Beijing Hospitals Authority’s Ascent Plan (DFL20241201).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Garber K. Genetics: deep exploration. Nature. 2012;492(7429):S56–7. doi:10.1038/492S56a
2. Jordan CT, Cao L, Roberson EDO, et al. PSORS2 is due to mutations in CARD14. Am J Hum Genet. 2012;90(5):784–795. doi:10.1016/j.ajhg.2012.03.012
3. Jordan CT, Cao L, Roberson EDO, et al. Rare and common variants in CARD14, encoding an epidermal regulator of NF-kappaB, in psoriasis. Am J Hum Genet. 2012;90(5):796–808. doi:10.1016/j.ajhg.2012.03.013
4. Takeichi T, Kobayashi A, Ogawa E, et al. Autosomal dominant familial generalized pustular psoriasis caused by a CARD14 mutation. Br J Dermatol. 2017;177(4):e133–e135. doi:10.1111/bjd.15442
5. Craiglow BG, Boyden LM, Hu R, et al. CARD14-associated papulosquamous eruption: a spectrum including features of psoriasis and pityriasis rubra pilaris. J Am Acad Dermatol. 2018;79(3):487–494. doi:10.1016/j.jaad.2018.02.034
6. Frare CP, Blumstein AJ, Paller AS, et al. CARD14-associated papulosquamous eruption (CAPE) in pediatric patients: three additional cases and review of the literature. Pediatr Dermatol. 2021;38(5):1237–1242. doi:10.1111/pde.14779
7. Zhao X, Miao C, Xiang X, et al. Effect of secukinumab on inflammatory linear verrucous epidermal naevus with a somatic mutation in CARD14. Clin Exp Dermatol. 2024;49(6):631–633. doi:10.1093/ced/llae047
8. Inoue N, Dainichi T, Fujisawa A, Nakano H, Sawamura D, Kabashima K. CARD14 Glu138 mutation in familial pityriasis rubra pilaris does not warrant differentiation from familial psoriasis. J Dermatol. 2016;43(2):187–189. doi:10.1111/1346-8138.13008
9. Afonina IS, Van Nuffel E, Baudelet G, et al. The paracaspase MALT1 mediates CARD14-induced signaling in keratinocytes. EMBO Rep. 2016;17(6):914–927. doi:10.15252/embr.201642109
10. Li N, Tao J, Zhang J, Liu Z, Yu P. A novel mutation in a CARD14-associated papulosquamous eruption. Pediatr Dermatol. 2023;40(4):706–709. doi:10.1111/pde.15254
11. Dai S, Zhang S, Wang C, et al. CARD14 Missense Variant Underlying CARD14-Associated Papulosquamous Eruption with Beneficial Response to Secukinumab. JID Innov. 2023;3(2):100174. doi:10.1016/j.xjidi.2022.100174
12. Hsu CJ, Tsai TF. Report of a case with CARD14-associated papulosquamous eruptions and multiple skin cancers[J]. Photodermatol Photoimmunol Photomed. 2024;40(3):e12969. doi:10.1111/phpp.12969
13. Kolt-Kaminska M, Osinska A, Kaznowska E, Reich A. Successful Treatment of Pityriasis Rubra Pilaris with Risankizumab in Children. Dermatol Ther. 2023;13(10):2431–2441. doi:10.1007/s13555-023-01005-y
14. Signa S, Campione E, Rusmini M, et al. Whole exome sequencing approach to childhood onset familial erythrodermic psoriasis unravels a novel mutation of CARD14 requiring unusual high doses of ustekinumab. Pediatr Rheumatol Online J. 2019;17(1):38. doi:10.1186/s12969-019-0336-3
15. Nogueira M, Reis J, Abreu M, Coelho A, Reis CF, Machado S. A child with CARD14-associated papulosquamous eruption (CAPE) successfully treated with ustekinumab. Pediatr Dermatol. 2023;40(6):1104–1106. doi:10.1111/pde.15336
16. Niedzwiedz M, Narbutt J, Siekierko A, et al. Case report: successful treatment with biologics in a pediatric patient with a severe inflammatory skin disease and novel CARD14 mutation. Front Med. 2024;11:1360248. doi:10.3389/fmed.2024.1360248
17. Rossel SVJ, Reich A, Baniel A, et al. Exploring shared clinical features and successful therapeutic interventions in CARD14-associated papulosquamous eruption. J Eur Acad Dermatol Venereol. 2024. doi:10.1111/jdv.20420
18. Chessa MA, Rossi AN, Baracca MF, Piraccini BM, Neri I. CARD14-associated papulosquamous eruption flare-up after SARS-CoV-2 infection in a child: secukinumab a safe and effective treatment. Int J Dermatol. 2023;62(10):1304–1306. doi:10.1111/ijd.16790
19. Sawabe Y, Hayashi K, Kamata M, et al. Case of generalized pustular psoriasis with coexisting mutations in IL36RN and CARD14. J Dermatol. 2019;46(10):e368–e370. doi:10.1111/1346-8138.14909
20. Klein B, Treudler R, Dumann K, et al. Clinical response of CARD14-associated papulosquamous eruption to an anti-interleukin-17A antibody. Br J Dermatol. 2022;187(3):419–422. doi:10.1111/bjd.21229
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.