Back to Journals » Infection and Drug Resistance » Volume 15
Clinical Characteristics, Microbiology, and Risk Factors for Mortality of Pre-Engraftment and Post-Engraftment Bloodstream Infection in Hematopoietic Stem Cell Transplantation Recipients
Authors Chen W, Zhao Y, Luo Y, Yu J, Fu H, Lai X, Liu L, Ye Y, He J, Sun J, Zheng W, Zhao Y, Wei G, Cai Z, Huang H, Shi J
Received 15 October 2022
Accepted for publication 16 November 2022
Published 28 November 2022 Volume 2022:15 Pages 6893—6905
DOI https://doi.org/10.2147/IDR.S392804
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Weihao Chen,1– 4 Yanmin Zhao,1– 4 Yi Luo,1– 4 Jian Yu,1– 4 Huarui Fu,1– 4 Xiaoyu Lai,1– 4 Lizhen Liu,1– 4 Yishan Ye,1– 4 Jingsong He,1– 4 Jie Sun,1– 4 Weiyan Zheng,1– 4 Yi Zhao,1– 4 Guoqing Wei,1– 4 Zhen Cai,1– 4 He Huang,1– 4 Jimin Shi1– 4
1Bone Marrow Transplantation Center, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2Liangzhu Laboratory, Zhejiang University Medical Center, Hangzhou, 311121, People’s Republic of China; 3Institute of Hematology, Zhejiang University, Hangzhou, People’s Republic of China; 4Zhejiang Province Engineering Laboratory for Stem Cell and Immunity Therapy, Hangzhou, People’s Republic of China
Correspondence: Jimin Shi; He Huang, Bone Marrow Transplantation Center, The First Affiliated Hospital, School of Medicine, Zhejiang University, No. 79 Qingchun Road, Hangzhou, People’s Republic of China, Tel/Fax +86-0571-87236706, Email [email protected]; [email protected]
Background: Bloodstream infection (BSI) is a common and serious complication that may lead to high mortality during the different phases after hematopoietic stem cell transplant (HSCT). We investigated BSI in patients undergoing HSCT to provide an appropriate clinical anti-infection experience and improve the prognosis of recipients with BSI after HSCT.
Methods: A total of 105 patients with BSI after HSCT at our center from January 2015 to June 2020 were included in this retrospective study. We analyzed the clinical and microbiological data, and the risk factors for mortality at 3 months after BSI.
Results: Of the 1141 HSCT recipients, 105 (9.2%) patients presented with 122 episodes of BSI, of which we isolated 85 (65.9%) gram-negative bacteria, 32 (24.8%) gram-positive bacteria and 12 (9.3%) fungi. Multidrug-resistant bacteria (MDR) were more than 70% of all pathogens and carbapenem-resistant organisms (CRO) were 25.6%. There were 55 episodes of BSI in the pre-engraftment phase and 67 episodes in the post-engraftment phase. The mortality of post-engraftment BSI was significantly higher than that of pre-engraftment (56.7% vs 32.7%, p = 0.005). Through multivariate analysis, the independent risk factors for all-cause mortality at 3 months after BSI were higher levels of procalcitonin (PCT), failure to cover appropriate antibiotics timely, and CRO BSI in pre-engraftment period or multidrug-resistant gram-negative bacteria (MDRGNB) BSI in post-engraftment period.
Conclusion: Although the incidence of BSI was lower after HSCT, MDR-dominated BSI had a high mortality rate. Rapid identification of infection or pathogens’ classification with various testing methods and the more sensible and timely antibiotic cover are critical to the outcome of BSI after HSCT.
Keywords: bloodstream infection, hematopoietic stem cell transplantation, multidrug-resistant bacteria, all-cause mortality
Introduction
Hematopoietic stem cell transplantation (HSCT) is currently the most effective treatment for hematological malignancies or non-malignant diseases. As one of the serious and life-threatening complications of HSCT, bloodstream infection (BSI) needs more attention. It has occurred in 12–47% of HSCT recipients according to previous reports.1–4 Based on recipients’ immune reconstitution, their post-transplantation period can be divided into two phases: pre-engraftment and post-engraftment phase. BSI can occur during both two phases.
Previous studies have shown that mucosal damage, central venous catheter-related infections, and neutropenia are the main causes of BSI.1–7 Moreover, many factors in the development of pre-engraftment BSI included transplantation method,3 type of allografts,2,8 human leukocyte antigen (HLA) match,7,9 donor selection,7,10 and conditioning regimen.11 While severe graft-versus-host disease (GVHD),3,9 particularly in the intestinal tract, immunosuppression caused by steroids,3,12 and secondary neutropenia12 increased the risk of BSI during the post-engraftment period.
In the past decades, a downward trend can be observed in the incidence of BSI after HSCT, due to the increasing use of reduced-intensity conditioning (RIC) regimen, the advancement of supportive care measures, and the administration of fluoroquinolone prophylaxis.2,7 Consequently, the gradual emergence of gram-negative bacteria (GNB) as the major pathogens for BSI was reported which contributes to higher mortality than gram-positive bacteria (GPB).13,14 In China, the proportion of GNB was higher than that of GPB in the past 10 years.15 Meanwhile, a mounting number of multidrug-resistant organisms were isolated, including extended-spectrum beta-lactamase-producing bacteria, carbapenem-resistant organisms (CRO), and vancomycin-resistant Enterococcus.13,16 Therefore, our next goal, in this new era of drug-resistant bacteria, is to reduce the mortality of BSI, which can be achieved by studying its risk factors.
There are relatively more studies on the risk factors of BSI and fewer studies on the risk factors of mortality of BSI after HSCT. Therefore, our research aimed to describe the epidemiology, microbiology, and risk factors of mortality of BSI after HSCT, which desire to provide evidence and ideas for guiding clinical empirical antibiotic treatment.
Methods and Materials
Study Population and Data Collection
The retrospective study was performed on HSCT patients who underwent bloodstream infection from January 2015 to June 2020 at our center. If bloodstream infection occurred before receiving the conditioning regimens, the patients were excluded. The grouping process of patients with BSI after HSCT during this period is shown in Figure 1.
 |
Figure 1 Diagram of patients’ grouping process of BSI after HSCT. |
Through the electronic medical record system of our hospital, we collected the information of enrolled patients, including basic demographics, the underlying disease, clinical characteristics of BSI, infectious or microbiological data, and other relevant information before and after transplantation. The entire study procedure was in accordance with the Declaration of Helsinki and was approved by the Ethics Review Committee of the First Affiliated Hospital of Zhejiang University.
Transplantation Procedure
Transplantation-related procedures followed a previous study at our center.17 Myeloablative conditioning (MAC) regimens of haploidentical transplantation comprised cytarabine (4 g/m2 /d IV on days −10 to −9), busulfan (3.2 mg/kg per day IV on days −8 to −6), cyclophosphamide (1.8 g/m2 per day IV on days −5 to −4) and Me-CCNU (250 mg/m2 orally on days −3). For HLA-identical sibling transplant or unrelated donor transplant, MAC mainly included busulfan (3.2 mg/kg per day IV on days −7 to −4), and cyclophosphamide (60 mg/kg per day IV on days −3 to −2). RIC was a fludarabine-based regimen, including fludarabine (180 mg/m2) and busulfan (6.4 mg/kg IV; or 12.8 mg/kg) for 2–3 days. GVHD prophylaxis consisted of cyclosporin A, methotrexate, low-dose mycophenolate mofetil, and anti-T-lymphocyte globulin for haploidentical transplantation (2.5 mg/kg per day on days −5 to −2, Fresenius, Bad Homburg, Germany) or rabbit anti-thymocyte globulin (ATG) for unrelated donors transplant (4.5–6 mg/kg total dose, Genzyme, Cambridge, MA).
Prophylactic Use of Antimicrobials
All patients were admitted to a separate sterile laminar flow chamber before conditioning. Oral levofloxacin (500 mg/d) was used to clear gut bacteria before infusing stem cells and intravenous piperacillin sodium tazobactam for prophylactic use before neutrophil engraftment. Prophylaxis of fungal infections was used with oral fluconazole or voriconazole, or intravenous echinocandin. Prophylaxis of cytomegalovirus infections was used ganciclovir from days −7 to day 0 and acyclovir from day +1 to days +365. Oral trimethoprim-sulfamethoxazole (160 mg trimethoprim and 800 mg sulfamethoxazole twice a day from days −10 to days +30 or 160 mg trimethoprim and 800 mg sulfamethoxazole twice a week from days +30 to days +180) was administered to prevent for Pneumocystis jirovecii.
Definitions
BSI was defined as the isolation of pathogens from a single blood culture. If coagulase-negative staphylococci (CoNS) or common skin contaminants were isolated, two separate positive blood cultures were required.18 Neutropenia was defined as an absolute neutrophil count (ANC) <500/mm3 in peripheral blood or expected to decrease to <500/mm3 in the next 48 hours.19 Neutrophil engraftment was defined as ANC ≥500/mm3 at least 3 consecutive days after transplantation. The diagnosis of acute intestinal GVHD was defined according to the standard criteria.20 Adequate doses of steroids were considered as the administration of a cumulative dose >1 mg/kg of methylprednisolone or equivalent other steroids for at least 7 consecutive days within the 1 month preceding the development of BSI. Blood culture and procalcitonin (PCT) were performed simultaneously when the oral temperature was ≥38.3°C for a single time, and the oral temperature was ≥38.0°C for persistently more than 1 hour, or other overt clinical symptoms and signs of infection occurred. Pre-engraftment BSI was defined as infection occurring between the onset of the conditioning regimen and neutrophil engraftment. Post-engraftment BSI was considered as the infection occurring after the neutrophil engraftment.
Multidrug-resistant (MDR) bacteria were defined as non-susceptibility to at least one agent in three or more classes of antibiotics.21 According to antimicrobial categories of different organism groups (such as Enterococcus spp., Enterobacteriaceae, Pseudomonas aeruginosa, and Acinetobacter spp.), we identified the isolated bacteria that conform with the standard criteria as MDR.21 All Stenotrophomonas maltophilia strains were considered MDR.21,22 CRO is mainly composed of carbapenem-resistant Enterobacteriaceae (CRE), carbapenem-resistant Pseudomonas aeruginosa, and carbapenem-resistant Acinetobacter baumannii. Timely and appropriate antibiotic coverage was defined as less than 24 hours between the timing of positive blood culture drawn and a sensitive antibiotic administration based on the final microbial susceptibility test.
Statistical Analysis
We used Mann–Whitney U-test and t-test to compare continuous variables, and chi-square test to categorical variables. Overall survival (OS) was plotted using the Kaplan–Meier method. For the risk factors of mortality, in univariate analysis, Mann–Whitney U-test and t-test were performed likewise for continuous variables and chi-square test for categorical variables. All variables with P < 0.1 or clinical significance in the univariate analysis were included in the multivariate analysis. Due to the interaction between CRO and CRE, CRE is not included in the multivariate analysis model. Cox proportional hazard regression model was adopted for multivariate analysis. All statistical analysis used SPSS version 21 (Chicago, IL, USA) and R software (version 4.2.0, R Foundation for Statistical Computing, Vienna, Austria). All P values are two-tailed, and P < 0.05 was considered statistically significant.
Results
Patients Characteristics and Clinical Characteristics of BSI
Of the 1141 HSCT recipients, 105 (9.2%) patients developed BSI. Among them, 88 (83.8%) patients had 1 BSI and 17 patients (16.2%) had more than 2 BSI. The characteristics of patients with BSI are summarized in Table 1. The pre-engraftment BSI occurred in 47 patients (44.8%) and post-engraftment BSI occurred in 54 patients (51.4%), and patients with BSI in both two periods were 4 (3.8%). Male comprised 60% of the total (63/105). The most common underlying disease was acute myeloid leukemia. The median age was 35 years (range, 13–66 years). Compared with post-engraftment, the median age was younger in the group of pre-engraftment BSI (31 years vs 44 years).
 |
Table 1 Patient Characteristics |
A total of 122 episodes of BSI in 105 patients were documented after HSCT. There were 55 episodes of BSI in the pre-engraftment phase and 67 episodes in the post-engraftment phase. The median onset of BSI in the pre- and post-engraftment phase were +8 days (−8 to +18 days) and +251 days (+16 to +1462 days), respectively. The former group was more likely to present neutropenia at the onset of BSI than the latter (94.5% vs 74.6%). In the pre-engraftment phase, we did not find patients using adequate doses of steroids before infection, while 25 (37.3%) cases of post-engraftment BSI did. Acute intestinal GVHD was more common in patients with post-engraftment BSI (25.4% vs 7.2%). These clinical characteristics of BSI are shown in Table 2.
 |
Table 2 Clinical Characteristics of BSI |
Microbial Isolates and Antimicrobial Resistance
A total of 129 pathogens were isolated from 122 episodes of BSI, including 85 GNB, 32 GPB, and 12 Fungi (Table 3). The distribution of pathogenic organisms of BSI is presented in Figure 2. Coagulase-negative staphylococci (n = 15) was the most common and accounted for nearly half of the total GPB, followed by Enterococcus faecium (n = 10), while only one strain of Staphylococcus aureus was isolated before neutrophil engraftment. The most frequently isolated GNB were Klebsiella pneumoniae and Escherichia coli, accounting for 36.5% (n = 31) and 27.0% (n = 23) respectively, followed by Pseudomonas aeruginosa (11.8%, n = 10) and Stenotrophomonas maltophilia (11.8%, n = 10). Among the fungi, all were Candida spp., including 11 (91.7%) strains of Candida tropicalis and 1 (8.3%) strain of Candida parapsilosis. Multidrug-resistant bacteria were more than 70% of all pathogens which comprised 26 (20.5%) strains of MDRGPB and 69 (53.5%) strains of MDRGNB. CRO were 33 (25.6%), of which 26 (78.8%) are CRE. There was no significant difference in the distribution of all kinds of pathogens between pre- and post-engraftment BSI.
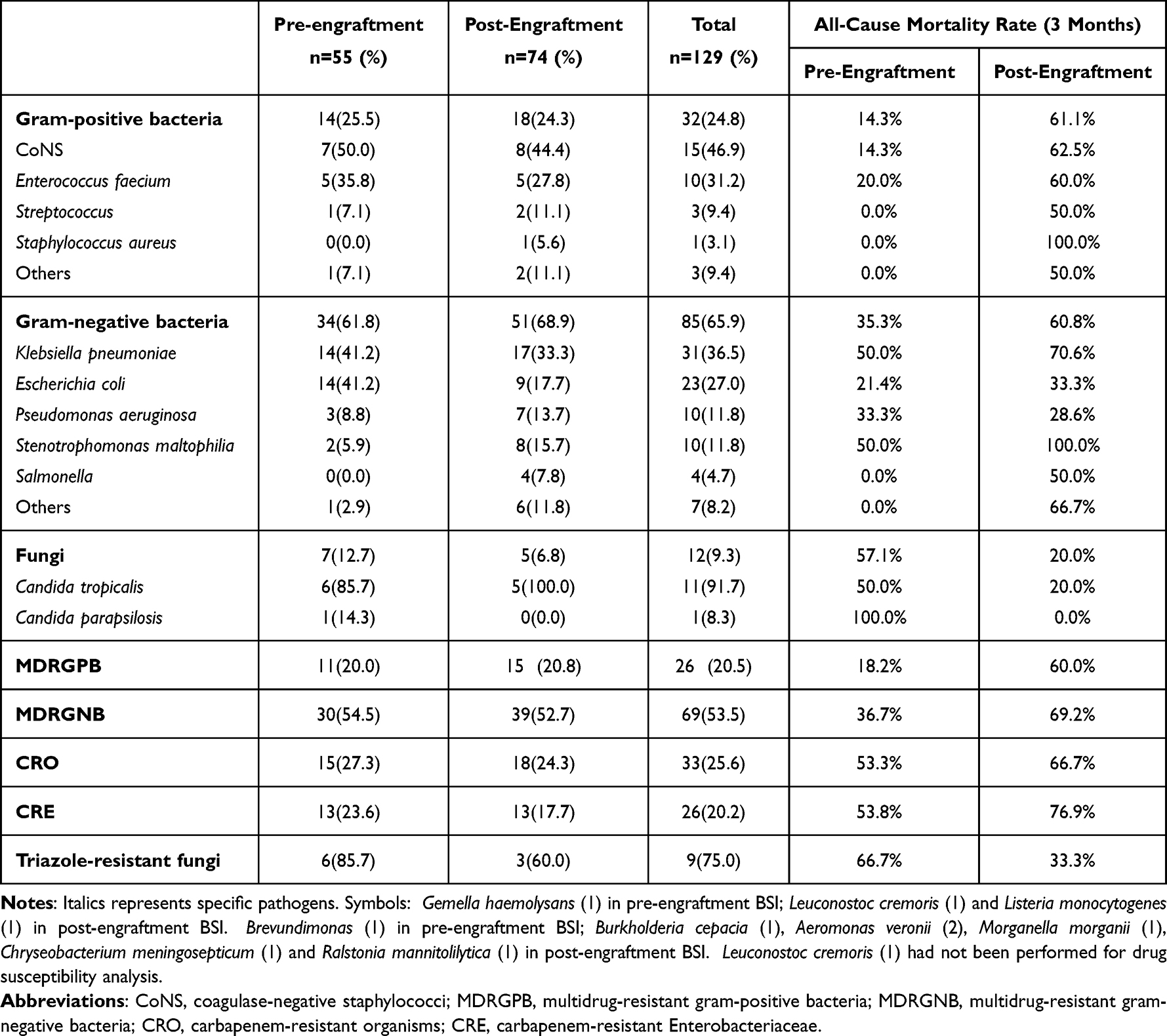 |
Table 3 Microbiological Classification and All-Cause Mortality Rate Caused by Pathogens of BSI |
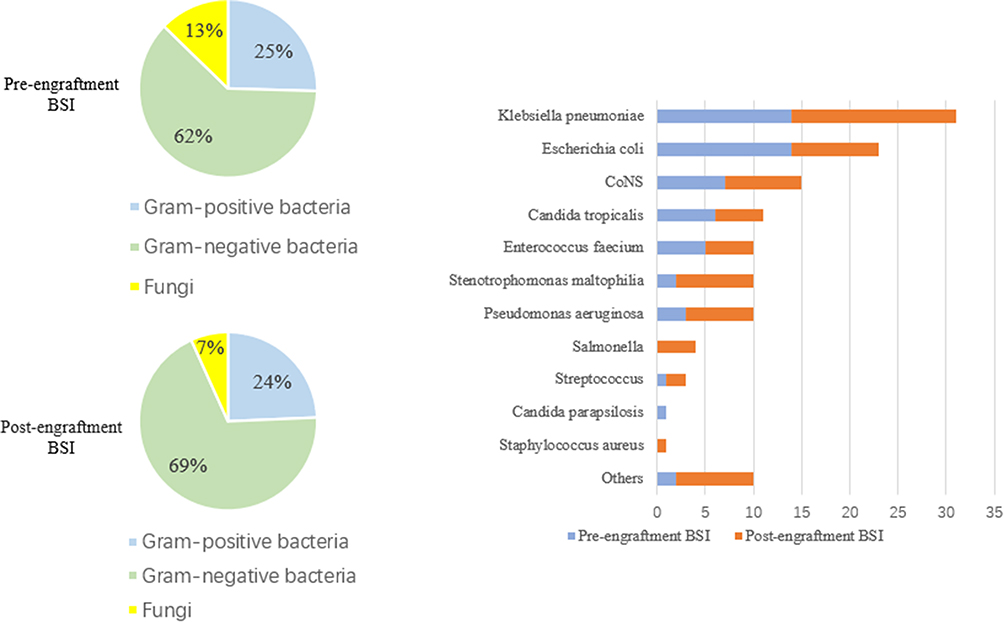 |
Figure 2 Distribution of pathogenic organisms in different periods. |
Outcomes and Risk Factors for Mortality
Of the 122 cases, 56 (45.9%) died ultimately at 3 months after BSI. The mortality of post-engraftment BSI was significantly higher than that of pre-engraftment (56.7% vs 32.7%, p = 0.005, Figure 3). In the pre-engraftment phase, the mortality caused by different organisms were 35.3% (GNB) vs 14.3% (GPB) vs 57.1% (Fungi), while in post-engraftment phase, the mortality caused by different organisms were 60.8% (GNB) vs 61.1% (GPB) vs 20.0% (Fungi) (Table 3).
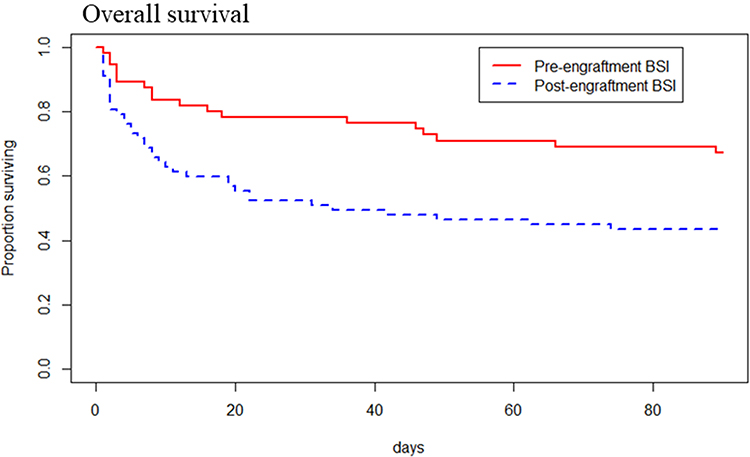 |
Figure 3 OS curve for 3 months after pre-engraftment BSI vs post-engraftment BSI (p=0.005). |
In patients with pre-engraftment BSI, the univariate analysis demonstrated higher levels of PCT, failure to cover appropriate antibiotics timely, and BSI caused by CRO were associated with all-cause mortality at 3 months after BSI (Table 4). According to multivariate analysis, these three variables were significantly associated with higher all-cause mortality at 3 months after pre-engraftment BSI (Table 5).
 |
Table 4 Univariate Analyses of Risk Factors for All-Cause Mortality at 3 Months After Bloodstream Infection |
 |
Table 5 Multivariate Analyses of Risk Factors for All-Cause Mortality at 3 Months After Bloodstream Infection |
In the group of post-engraftment BSI, univariate analysis revealed six variables (HLA mismatch, the longer interval between the onset of fever and positive blood culture drawn, higher levels of PCT, failure to cover appropriate antibiotic timely, BSI caused by MDRGNB, or CRO) may be associated with post-infection mortality (Table 4). In multivariate analysis, factors that increased the risk of post-engraftment BSI mortality were higher levels of PCT, failure to cover appropriate antibiotics timely, and BSI caused by MDRGNB (Table 5).
The higher levels of PCT, failure to cover appropriate antibiotics timely, and BSI caused by MDRGNB or CRO were the independent risk factors for all-cause mortality at 3 months after BSI by multivariate analysis in all cases.
Discussion
We conducted a retrospective analysis of 122 episodes of bloodstream infections in 105 HSCT recipients at our center from 2015 to June 2020. We observed a relatively lower overall incidence of BSI (9.2%) among HSCT patients compared with other similar studies.3,5,6,12 Additionally, this study demonstrated that higher PCT levels, delayed administration of appropriate antibiotics, and MDRGNB or CRO BSI were associated with an increased risk of all-cause mortality at 3 months after BSI. GNB were the main pathogens of BSI. Moreover, the prevalence of drug-resistant bacteria, especially CRO, was a sticky problem and would hinder the long-term survival of HSCT patients.
By observing the clinical characteristics of BSI, we found that almost all pre-engraftment BSI occurred in the neutropenic phase after the conditioning regimen, while post-engraftment BSI was predisposed to occur in patients with chemotherapy-induced secondary neutropenia after relapse of underlying disease, in patients with acute intestinal GVHD, or in patients who have received adequate doses of steroids before BSI. Although we did not perform an analysis of risk factors for BSI after HSCT, our results are consistent with the risk factors of BSI after HSCT from previous studies.2,3,7,9,12
Like other studies,1,6 the all-cause mortality rate of BSI in the latter phase was higher than that in the former (56.7% vs 32.7%, p = 0.005). In our cohort, the possible explanation for this difference is the frailty state after the underlying disease relapsed and delayed treatment of BSI that occurred out of hospital. Due to the recurrence of the underlying disease, patients who were re-treated with multiple courses of chemotherapy developed severe neutropenia, increased frailty, and repeated exposure to antibiotics. These factors may be responsible for the higher mortality from post-engraftment BSI. Additionally, since the patient can be discharged from the hospital after the hematopoietic system is rebuilt, approximately 30 days, the window time of nosocomial infection for the patient is limited.16 A recent long-term retrospective study has indicated that 39% of BSI occur outside the hospital.13 Therefore, some patients who were under a long-term and constant risk of non-nosocomial infection might delay empiric antibiotic treatment and lead to worse outcomes if they were not vigilant about infection and fail to identify the occurrence of infection early and rapidly.
Our multivariate analysis concluded that PCT levels (>0.5ng/mL) were a predictor of death. PCT released by parenchymal cells under the stimulation of bacterial toxin can be detected after 2–4 hours in serum and peaked at 6 hours.23 The half-life of PCT is approximately 24 hours when the infection is controlled by the host immune system or antibiotic therapy.24,25 Repeat PCT testing is recommended every 1–2 days if PCT levels were >0.5ng/mL, depending on the severity of disease.25 Therefore, PCT can be used to monitor infection continuously, evaluate the effectiveness of empiric antibiotics, and guide antibiotic discontinuation, which is superior to the C-reactive protein, IL-6, and other acute inflammation makers.24,26,27 Notably, PCT is more specific than sensitive and many other factors can exert an impact on PCT, such as trauma and ATG which can raise PCT levels.28
Delayed administration of appropriate antibiotics was considered a vital independent risk factor for high mortality in two phases, which is consistent with other studies.29,30 Among patients with delayed administration of appropriate antibiotics, 72.5% (29/40) received inappropriate antibiotics within 24 hours of blood culture drawn. It is imperative to collect and analyze detailed data about bacterial epidemiology and its drug resistance in the local region or hospital. Based on grasping regional bacterial epidemiology, the risk stratification of suspected infectious patients combined with the patient’s clinical status and history of previous infections may help to select more appropriate antibiotics. Additionally, rapid diagnostic technologies (such as the matrix-assisted laser desorption ionization time-of-flight, multiplex polymerase chain reaction (PCR)31 and metagenomic next-generation sequencing) should be available to identify the classification of pathogens and their resistance mechanisms early, which guide replacement or combination antibiotic therapy and improve the accuracy of antibiotics usage.29
The most common bacteria isolated from both periods in our study were GNB, dominated by Klebsiella pneumoniae and Escherichia coli. CoNS and Enterococcus faecium dominated in GPB and were both sensitive to vancomycin. Compared to other studies which were usually dominated by GPB BSI,13,14,18 possible explanations for the predominance of GNB BSI in our cohort are that the prevalent strains of nosocomial infections are GNB in China15 and that better oral care and catheter care have reduced the transfer of Streptococcus or CoNS to the bloodstream.32,33 Before neutrophil engraftment, GNB BSI was associated with higher mortality than positive bacteria (35.3% vs 14.3%, p = 0.125), in line with previous reports.6,34 Nevertheless, the mortality caused by GNB BSI and GPB BSI is roughly similar (60.8% vs 61.1%) in post-engraftment BSI. This is most likely due to the weakness state of the patient, although GPB, mainly CoNS, are less virulent.12 Candida spp. BSI had a higher rate of resistance to triazole antifungals in our center, 85.7% in the early stage and 60.0% in the late stage, which cause high mortality. This could be explained by a breakthrough infection, even if we were using fluconazole or voriconazole prophylaxis. All fungi were sensitive to amphotericin. For those patients with persistent or recurrent fever 4–7 days after antibiotic administration,19 antifungal therapy should be adjusted to echinocandin, posaconazole, or even amphotericin.
Furthermore, our cohort demonstrated that MDRGNB was an independent risk factor of mortality in post-engraftment BSI, and the incidence of MDR bacteria was over 70% in both periods. We found that the mortality rates of Klebsiella pneumoniae BSI (19/31) and Stenotrophomonas maltophilia BSI (9/10) were 61.3% and 90%, respectively, which were the most lethal bacteria in the whole period. Of the 19 strains of Klebsiella pneumonia, 18 (94.7%) were MDR and 15 (78.9%) were CRE. Moreover, we should be more vigilant about Stenotrophomonas maltophilia BSI in the post-engraftment period, because it often occurs in immunocompromised patients and is resistant to carbapenems. A retrospective case–control study has demonstrated that the risk of death increases by 8 times when patients develop Stenotrophomonas maltophilia BSI.35
Among GNB, 44.1% were CRO in the former period and 35.3% in the latter period. CRO, as an independent risk factor in pre-engraftment BSI, caused >50% of crude mortality for HSCT patients. The problem with CRO is that CRO can encode various β-lactamases to hydrolyze many antibiotics, resulting in few antibiotics being effective against them.36 While CRE BSI, which occupies a dominant position in CRO BSI, is worthy of more attention. Early identification of intestinal colonization by CRE and its resistance mechanisms is critical for the control and treatment of CRE BSI.37,38 Previous studies at our center have found that increasing the frequency of CRE screening can help detect CRE colonization,39 and subsequent preemptive treatment of CRE-colonized patients with infectious symptoms can reduce the morbidity and mortality of CRE BSI.40 Moreover, several screen methods that rapidly detect carbapenemase genes through rectal swabs have recently been applied, especially Xpert Carba-R.38,41,42 However, the main drawback of these PCR-based methods is the low positive predictive value.
In addition, PCT levels and MDRGNB or CRO BSI, or MDRGNB and CRO that were extracted as risk factors of mortality appeared to confound each other. MDRGNB or CRO infection typically was related to higher PCT levels and CRO may overlap with MDRGNB. Nonetheless, we did not find that severe multicollinearity among these variables was sufficient to affect the stability of the Cox proportional hazards regression model after we tested these variables using the collinearity diagnostics. Therefore, we think these risk factors of mortality were still statistically significant.
There are limitations to our study. Firstly, this is retrospectively single-center research, and most patients with HSCT are the haploidentical transplant. Accordingly, our conclusions may not apply to other centers because of differences in transplantation patterns, regional microbial epidemiology, and drug resistance across centers. Moreover, due to data limitations, we may have overlooked other potential risk factors for mortality of BSI after HSCT, such as virus activation.
Conclusion
We conducted this retrospective study to investigate the clinical and microbiological characteristics of BSI after HSCT. Although the incidence of BSI after transplantation is now low compared to decades ago, the incidence and mortality of BSI caused by multidrug-resistant bacteria, especially MDRGNB or CRO, are gradually increasing. Rapid identification of infection or pathogens’ classification with various testing methods, and more sensible and timely empirical antibiotic use can improve the outcome of BSI after HSCT.
Abbreviations
BSI, bloodstream infection; CR, complete remission; HLA, human leukocyte antigen; MAC, myeloablative conditioning; RIC, reduced-intensity conditioning; NMA, nonmyeloablative conditioning; GVHD, graft-versus-host disease; PCT, procalcitonin; CoNS, coagulase-negative staphylococci; MDRGPB, multidrug-resistant gram-positive bacteria; MDRGNB, multidrug-resistant gram-negative bacteria; CRO, carbapenem-resistant organisms; CRE, carbapenem-resistant Enterobacteriaceae; PCR, polymerase chain reaction; HR, hazard ratio; CI, confidence interval.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, He Huang or Jin-min Shi, upon reasonable request.
Consent for Publication
All authors read and approved the final manuscript.
Ethics Approval
The entire study procedure was in accordance with the Declaration of Helsinki and was approved by the Ethics Review Committee of the First Affiliated Hospital of Zhejiang University (20200313C04). Written informed consent was obtained from each patient or parent/legal representative and all data were processed anonymously.
Acknowledgments
Sincere thanks to all staff, clinicians, and patients who contributed to this study.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors report no conflict of interest.
References
1. Ustun C, Young J-AH, Papanicolaou GA, et al. Bacterial blood stream infections (BSIs), particularly post-engraftment BSIs, are associated with increased mortality after allogeneic hematopoietic cell transplantation. Bone Marrow Transplant. 2019;54:1254–1265. doi:10.1038/s41409-018-0401-4
2. Busca A, Cavecchia I, Locatelli F, et al. Blood stream infections after allogeneic stem cell transplantation: a single-center experience with the use of levofloxacin prophylaxis. Transpl Infect Dis. 2012;14:40–48. doi:10.1111/j.1399-3062.2011.00650.x
3. Gudiol C, Garcia-Vidal C, Arnan M, et al. Etiology, clinical features and outcomes of pre-engraftment and post-engraftment bloodstream infection in hematopoietic SCT recipients. Bone Marrow Transplant. 2014;49:824–830. doi:10.1038/bmt.2014.37
4. Hong J, Moon SM, Ahn HK, et al. Comparison of characteristics of bacterial bloodstream infection between adult patients with allogeneic and autologous hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2013;19:994–999. doi:10.1016/j.bbmt.2013.03.019
5. Poutsiaka DD, Price LL, Ucuzian A, et al. Blood stream infection after hematopoietic stem cell transplantation is associated with increased mortality. Bone Marrow Transplant. 2007;40:63–70. doi:10.1038/sj.bmt.1705690
6. Mikulska M, Del Bono V, Bruzzi P, et al. Mortality after bloodstream infections in allogeneic haematopoietic stem cell transplant (HSCT) recipients. Infection. 2012;40:271–278. doi:10.1007/s15010-011-0229-y
7. Yan CH, Wang Y, Mo X-D, et al. Incidence, risk factors, microbiology and outcomes of pre-engraftment bloodstream infection after haploidentical hematopoietic stem cell transplantation and comparison with HLA-identical sibling transplantation. Clin Infect Dis. 2018;67:S162–s173. doi:10.1093/cid/ciy658
8. Akinboyo IC, Young RR, Spees LP, et al. Microbiology and risk factors for hospital-associated bloodstream infections among pediatric hematopoietic stem cell transplant recipients. Open Forum Infect Dis. 2020;7:ofaa093. doi:10.1093/ofid/ofaa093
9. Poutsiaka DD, Munson D, Price LL, Chan GW, Snydman DR. Blood stream infection (BSI) and acute GVHD after hematopoietic SCT (HSCT) are associated. Bone Marrow Transplant. 2011;46:300–307. doi:10.1038/bmt.2010.112
10. Meyer E, Beyersmann J, Bertz H, et al. Risk factor analysis of blood stream infection and pneumonia in neutropenic patients after peripheral blood stem-cell transplantation. Bone Marrow Transplant. 2007;39:173–178. doi:10.1038/sj.bmt.1705561
11. Junghanss C, Marr KA, Carter RA, et al. Incidence and outcome of bacterial and fungal infections following nonmyeloablative compared with myeloablative allogeneic hematopoietic stem cell transplantation: a matched control study. Biol Blood Marrow Transplant. 2002;8:512–520. doi:10.1053/bbmt.2002.v8.pm12374456
12. Almyroudis NG, Fuller A, Jakubowski A, et al. Pre- and post-engraftment bloodstream infection rates and associated mortality in allogeneic hematopoietic stem cell transplant recipients. Transpl Infect Dis. 2005;7:11–17. doi:10.1111/j.1399-3062.2005.00088.x
13. Puerta-Alcalde P, Cardozo C, Marco F, et al. Changing epidemiology of bloodstream infection in a 25-years hematopoietic stem cell transplant program: current challenges and pitfalls on empiric antibiotic treatment impacting outcomes. Bone Marrow Transplant. 2020;55:603–612. doi:10.1038/s41409-019-0701-3
14. Weisser M, Theilacker C, Tschudin Sutter S, et al. Secular trends of bloodstream infections during neutropenia in 15 181 haematopoietic stem cell transplants: 13-year results from a European multicentre surveillance study (ONKO-KISS). Clin Microbiol Infect. 2017;23:854–859. doi:10.1016/j.cmi.2017.03.020
15. Hu FP, Guo Y, Zhu D-M, et al. Resistance trends among clinical isolates in China reported from CHINET surveillance of bacterial resistance, 2005–2014. Clin Microbiol Infect. 2016;22(Suppl 1):S9–14. doi:10.1016/j.cmi.2016.01.001
16. Heston SM, Young RR, Hong H, et al. Microbiology of bloodstream infections in children after hematopoietic stem cell transplantation: a single-center experience over two decades (1997–2017). Open Forum Infect Dis. 2020;7:ofaa465. doi:10.1093/ofid/ofaa465
17. Luo Y, Xiao H, Lai X, et al. T-cell-replete haploidentical HSCT with low-dose anti-T-lymphocyte globulin compared with matched sibling HSCT and unrelated HSCT. Blood. 2014;124:2735–2743. doi:10.1182/blood-2014-04-571570
18. Kikuchi M, Akahoshi Y, Nakano H, et al. Risk factors for pre- and post-engraftment bloodstream infections after allogeneic hematopoietic stem cell transplantation. Transpl Infect Dis. 2015;17:56–65. doi:10.1111/tid.12345
19. Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. Clin Infect Dis. 2011;52:e56–93. doi:10.1093/cid/cir073
20. Przepiorka D, Weisdorf D, Martin P, et al. 1994 consensus conference on acute GVHD grading. Bone Marrow Transplant. 1995;15:825–828.
21. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18:268–281. doi:10.1111/j.1469-0691.2011.03570.x
22. Averbuch D, Tridello G, Hoek J, et al. Antimicrobial resistance in gram-negative rods causing bacteremia in hematopoietic stem cell transplant recipients: intercontinental prospective study of the infectious diseases working party of the European Bone Marrow Transplantation Group. Clin Infect Dis. 2017;65:1819–1828. doi:10.1093/cid/cix646
23. Henriquez-Camacho C, Losa J. Biomarkers for sepsis. Biomed Res Int. 2014;2014:547818. doi:10.1155/2014/547818
24. Limper M, de Kruif MD, Duits AJ, Brandjes DP, van Gorp EC. The diagnostic role of procalcitonin and other biomarkers in discriminating infectious from non-infectious fever. J Infect. 2010;60:409–416. doi:10.1016/j.jinf.2010.03.016
25. Schuetz P, Albrich W, Mueller B. Procalcitonin for diagnosis of infection and guide to antibiotic decisions: past, present and future. BMC Med. 2011;9:107. doi:10.1186/1741-7015-9-107
26. Dandona P, Nix D, Wilson MF, et al. Procalcitonin increase after endotoxin injection in normal subjects. J Clin Endocrinol Metab. 1994;79:1605–1608. doi:10.1210/jcem.79.6.7989463
27. Manian FA. Use of procalcitonin to guide duration of antimicrobial therapy in intensive care units: proceed with caution. Clin Infect Dis. 2012;54:578. doi:10.1093/cid/cir888
28. Bruno B, Busca A, Vallero S, et al. Current use and potential role of procalcitonin in the diagnostic work up and follow up of febrile neutropenia in hematological patients. Expert Rev Hematol. 2017;10:543–550. doi:10.1080/17474086.2017.1326813
29. Ji J, Klaus J, Burnham JP, et al. Bloodstream infections and delayed antibiotic coverage are associated with negative hospital outcomes in hematopoietic stem cell transplant recipients. Chest. 2020;158:1385–1396. doi:10.1016/j.chest.2020.06.011
30. Liu VX, Fielding-Singh V, Greene JD, et al. The timing of early antibiotics and hospital mortality in sepsis. Am J Respir Crit Care Med. 2017;196:856–863. doi:10.1164/rccm.201609-1848OC
31. Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an antibiotic stewardship program: guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62:e51–77. doi:10.1093/cid/ciw118
32. Graber CJ, de Almeida K, Atkinson JC, et al. Dental health and viridans streptococcal bacteremia in allogeneic hematopoietic stem cell transplant recipients. Bone Marrow Transplant. 2001;27:537–542. doi:10.1038/sj.bmt.1702818
33. Raad I, Chaftari AM. Advances in prevention and management of central line-associated bloodstream infections in patients with cancer. Clin Infect Dis. 2014;59(Suppl 5):S340–343. doi:10.1093/cid/ciu670
34. Mikulska M, Del Bono V, Raiola AM, et al. Blood stream infections in allogeneic hematopoietic stem cell transplant recipients: reemergence of Gram-negative rods and increasing antibiotic resistance. Biol Blood Marrow Transplant. 2009;15:47–53. doi:10.1016/j.bbmt.2008.10.024
35. Senol E, DesJardin J, Stark PC, Barefoot L, Snydman DR. Attributable mortality of Stenotrophomonas maltophilia bacteremia. Clin Infect Dis. 2002;34:1653–1656. doi:10.1086/340707
36. Nordmann P, Poirel L. Epidemiology and diagnostics of carbapenem resistance in gram-negative bacteria. Clin Infect Dis. 2019;69:S521–s528. doi:10.1093/cid/ciz824
37. Schwaber MJ, Carmeli Y. An ongoing national intervention to contain the spread of carbapenem-resistant Enterobacteriaceae. Clin Infect Dis. 2014;58:697–703. doi:10.1093/cid/cit795
38. Banerjee R, Humphries R. Clinical and laboratory considerations for the rapid detection of carbapenem-resistant Enterobacteriaceae. Virulence. 2017;8:427–439. doi:10.1080/21505594.2016.1185577
39. Yang TT, Luo X-P, Yang Q, et al. Different screening frequencies of carbapenem-resistant Enterobacteriaceae in patients undergoing hematopoietic stem cell transplantation: which one is better? Antimicrob Resist Infect Control. 2020;9:49. doi:10.1186/s13756-020-0706-0
40. Forcina A, Baldan R, Marasco V, et al. Control of infectious mortality due to carbapenemase-producing Klebsiella pneumoniae in hematopoietic stem cell transplantation. Bone Marrow Transplant. 2017;52:114–119. doi:10.1038/bmt.2016.234
41. Josa DF, Bustos G, Torres IC, Esparza SG. Evaluación de tres métodos de tamizaje para detección de Enterobacteriaceae productoras de carbapenemasas en hisopados rectales [Evaluation of three screening methods for detection of carbapenemase-producing Enterobacteriaceae in rectal swabs]. Rev Chilena Infectol. 2018;35:253–261. Spanish. doi:10.4067/s0716-10182018000300253
42. Traczewski MM, Carretto E, Canton R, Moore NM. Multicenter evaluation of the Xpert Carba-R assay for detection of carbapenemase genes in gram-negative isolates. J Clin Microbiol. 2018;56. doi:10.1128/jcm.00272-18
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.