Back to Journals » Psoriasis: Targets and Therapy » Volume 16
Clinical Characteristics, Healthcare Resource Utilization, and Costs of Patients with Generalized Pustular Psoriasis in Taiwan: A National Claims Database Study
Authors Chien HT ![]() , Tseng CY
, Tseng CY ![]() , Lu CW
, Lu CW ![]() , Chung WH
, Chung WH ![]() , Lin FJ
, Lin FJ ![]()
Received 1 March 2026
Accepted for publication 20 June 2026
Published 26 June 2026 Volume 2026:16 606150
DOI https://doi.org/10.2147/PTT.S606150
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tina Bhutani
Hsiu-Ting Chien,1 Chien-Yu Tseng,1 Chun-Wei Lu,2,3 Wen-Hung Chung,2,3 Fang-Ju Lin1,4,5
1Graduate Institute of Clinical Pharmacy, College of Medicine, National Taiwan University, Taipei, Taiwan; 2Department of Dermatology, Drug Hypersensitivity Clinical and Research Center, Chang Gung Memorial Hospital, Taoyuan, Taiwan; 3College of Medicine, Chang Gung University, Taoyuan, Taiwan; 4School of Pharmacy, College of Medicine, National Taiwan University, Taipei, Taiwan; 5Department of Pharmacy, National Taiwan University Cancer Center, Taipei, Taiwan
Correspondence: Fang-Ju Lin, Graduate Institute of Clinical Pharmacy, College of Medicine, National Taiwan University, No. 33, Linsen S. Road, Taipei, Taiwan, 10050, Taiwan, Tel +886-2-3366-8809, Fax +886-2-3366-8780, Email [email protected]
Background: Generalized pustular psoriasis (GPP) is a rare and severe inflammatory disease characterized by widespread pustular eruptions and systemic inflammation.
Objective: To evaluate the clinical characteristics and disease burden of patients with GPP in Taiwan using a national claims database.
Methods: Patients with GPP and no prior diagnosis of psoriasis vulgaris (PV) who experienced an incident flare between January 1, 2017, and September 30, 2020, were identified from Taiwan’s National Health Insurance Database. Clinical characteristics, comorbidities, and treatment patterns were described. Recurrent flare frequency, healthcare resource utilization (HCRU) and costs were compared with those of a propensity score–matched PV cohort at a ratio of up to 1:4. Outpatient-managed flares were classified as moderate, whereas hospitalized flares were classified as severe.
Results: A total of 245 patients with GPP were included (mean age 51.3 years; 49.8% male). During follow-up, 1,156 moderate-to-severe flares were identified. Compared with matched patients with PV, patients with GPP had a higher recurrent flare rate (rate ratio 1.14; 95% CI 1.06– 1.23). Patients with GPP also had greater HCRU, including more outpatient visits (incidence rate ratio [IRR] 1.03 [95% CI 1.01– 1.05]), emergency room visits (IRR 1.33, 95% CI 1.19– 1.49), and hospital admissions (IRR 1.69 [1.50– 1.91]). Median monthly healthcare costs were approximately twice as high among patients with GPP as among matched patients with PV.
Conclusion: Patients with GPP experienced recurrent flares, greater healthcare utilization, and higher healthcare costs than matched patients with PV, underscoring the substantial real-world clinical and economic burden of GPP.
Keywords: disease burden, generalized pustular psoriasis, healthcare costs, national health database, patient characteristics, pustular psoriasis
Introduction
Generalized pustular psoriasis (GPP) is a rare, severe, and potentially life-threatening inflammatory skin disease characterized by widespread erythema, sterile pustules, and systemic inflammation.1,2 Distinct from the more prevalent psoriasis vulgaris (PV), which typically manifests as well-demarcated erythematous scaly plaques, GPP can cause extensive pustular eruptions over large body areas and may require urgent medical attention.3 The abrupt onset and severity of GPP flares pose substantial clinical challenges, and severe episodes may be complicated by secondary infection, sepsis, organ dysfunction, or other life-threatening complications.4
The pathogenesis of GPP is complex and multifactorial, involving interacting genetic, immunological, and environmental factors.5 GPP is characterized by prominent innate immune activation and neutrophil-dominant inflammation, in which dysregulation of the interleukin-36 (IL-36) pathway plays a central role.3,5 Mutations in the interleukin-36 receptor antagonist (IL36RN) gene can lead to uncontrolled IL-36 signaling and represent a key genetic factor.6,7 This dysregulation amplifies downstream cytokine and chemokine networks, including tumor necrosis factor (TNF)-α, IL-1β, IL-17, IL-23, and IL-6, which promote systemic inflammation and neutrophil recruitment. Recruited neutrophils become activated and accumulate within the epidermis, forming the sterile pustules characteristic of GPP.8 Activated neutrophils further amplify inflammation by releasing proteolytic enzymes, reactive oxygen species, and inflammatory mediators, contributing to tissue damage and systemic manifestations.8 In parallel, IL-17/IL-23-related T helper 17 responses and keratinocyte activation contribute to a self-amplifying inflammatory loop that promotes keratinocyte proliferation and sustains cutaneous inflammation.5,9 Environmental and physiological triggers, including infections, medication exposure or withdrawal, pregnancy, and stress, may initiate or exacerbate this inflammatory cascade, thereby precipitating acute GPP flares.4,10
Although GPP is rare, its epidemiologic and clinical burden is substantial. Reported prevalence ranges from 0.18 to 12.23 per 100,000 across countries, with generally higher estimates in some Asian populations.11 A Swedish population-based register study reported an approximately 50% higher mortality rate among patients with GPP than among comparator populations, underscoring its clinical severity.12 Patients with GPP frequently have multiple comorbidities, while recurrent and prolonged flares impose substantial clinical, economic, and quality-of-life burdens,13 including physical discomfort, impaired mobility, psychological distress, social stigmatization, and reduced work productivity.14,15
Despite this growing evidence, population-based real-world evidence on the clinical characteristics, treatment patterns, healthcare resource utilization (HCRU), and costs of GPP remains limited.16 Leveraging a nationwide claims database with nearly complete population coverage, this study had two objectives. The first was to characterize the clinical profile, comorbidities, treatment patterns, flare characteristics, and disease burden among patients experiencing GPP flares. The second was to compare all-cause HCRU and costs between patients with GPP flares and a matched cohort of patients with PV during the 12 weeks following the index flare and over the entire follow-up period.
Methods
Study Design and Data Source
This nationwide retrospective cohort study utilized the Taiwan National Health Insurance Research Database (NHIRD), which provides comprehensive health data for over 99% of Taiwan’s population. The database contains beneficiary registries, outpatient and inpatient claims, and pharmacy prescription records, offering demographic insights and valuable information on healthcare processes and disease burden.17
The analysis covered data from January 1, 2016, to December 31, 2020. This timeframe was chosen because Taiwan transitioned to the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnostic coding system in 2016, while December 31, 2020, represented the latest available claims data at the time of data extraction. Adoption of ICD-10-CM introduced a specific diagnosis code for GPP (ICD-10-CM: L40.1), which was absent in the previous ICD-9-CM system. The use of this specific diagnosis code for GPP enabled accurate and consistent identification of the study cohort. This study was approved by the Institutional Review Board of the Chang Gung Medical Foundation (No. 202200813B0).
Study Population and Flare Definition
Patients were eligible for inclusion if they met both of the following criteria: (1) had a documented diagnosis of GPP (ICD-10-CM: L40.1) or PV (ICD-10-CM: L40.0) and received systemic treatment between January 1, 2016, and December 31, 2020; and (2) experienced an incident (index) flare during the cohort identification period between January 1, 2017, and September 30, 2020. Patients younger than 18 years of age on the index date or with missing sex information were excluded. For the GPP cohort, patients with a prior PV diagnosis before the initial GPP diagnosis were excluded. Patients diagnosed with GPP exclusively during the third trimester of pregnancy were also excluded to focus on non-pregnancy-associated GPP and reduce clinical heterogeneity, because impetigo herpetiformis is considered a pregnancy-associated pustular psoriasis that occurs most frequently during the last trimester. This exclusion also helped minimize potential confounding by pregnancy-related HCRU.18 For the PV cohort, patients were excluded if they had a prior or concurrent diagnosis of GPP.
Flares were identified using a treatment-based algorithm that reflected intensification (initiation or escalation) of systemic dermatologic treatment. A flare-defining event was defined as the addition of a new systemic therapy, transition from topical to systemic treatment, switching to an alternative systemic agent, resumption of systemic treatment after a treatment gap of at least three months, or dose escalation of existing systemic treatment. The systemic therapies considered were acitretin, adalimumab, brodalumab, cyclosporine, etanercept, guselkumab, ixekizumab, methotrexate, prednisolone, secukinumab, and ustekinumab.
Flare severity was classified based on the healthcare setting in which the flare was managed: flares treated in the outpatient department (OPD) were classified as moderate, whereas flares requiring admissions into the inpatient department (IPD) were classified as severe. Because clinical severity scores, such as the Generalized Pustular Psoriasis Area and Severity Index (GPPASI), Generalized Pustular Psoriasis Physician Global Assessment (GPPGA), and Psoriasis Area and Severity Index (PASI), are unavailable in claims data, healthcare setting was used as a proxy for flare severity. Accordingly, all flares captured in this study were classified as moderate to severe.
The index flare was defined as the first qualifying flare episode during the cohort identification period, with no flare identified in the prior 365-day washout period. The index date was defined as the date of the first healthcare encounter associated with the index flare. Each flare was operationalized as a 12-week episode beginning on the flare start date, with any flare-defining treatment intensification occurring within this period considered part of the same episode. The study timeline and cohort identification process are illustrated in Supplementary Figure S1.
Outcome and Follow-Up
Outcomes assessed after the index date included recurrent flares, all-cause HCRU, and all-cause healthcare costs. Recurrent flares were defined as flare episodes occurring after the index date and were identified using the same treatment-based flare algorithm and 12-week episode definition described above. Costs were defined as total reimbursed claims amounts, encompassing inpatient, outpatient, and pharmacy costs, and were converted from New Taiwan dollar (TWD) to U.S. dollar (USD) using the average 2017–2020 exchange rate rounded to 1 USD = 30 TWD.19 Medication costs were defined as reimbursed costs for prescribed drugs, whereas non-medication costs included all other reimbursed medical costs, such as physician service, procedure, laboratory, diagnostic, and facility-related fees. Outcomes were evaluated over two follow-up windows: (1) the 12 weeks following the index date and (2) the entire follow-up period. Follow-up commenced on the index date and continued until death or the end of the study period (December 31, 2020), whichever occurred first.
Statistical Analysis
Continuous variables are presented as mean ± standard deviation (SD) or median (interquartile range), while categorical variables are presented as counts and percentages.
To reduce confounding in comparative analyses of HCRU and costs, propensity score matching was employed to balance baseline characteristics between the GPP and PV cohorts. Propensity scores were estimated using logistic regression, incorporating the following baseline covariates: age, sex, Charlson Comorbidity Index (CCI), comorbidities, comedications, and index flare severity. A 365-day baseline period preceding the index date was used to collect data on comorbidities and comedication use. The comorbidities assessed were hypertension, hyperlipidemia, hyperuricemia, coronary artery disease, liver disease, asthma, thyroid disease, depression, uveitis, ulcerative colitis, and psoriatic arthritis. Comedications were identified based on medication use prior to the index flare and included antidiabetic agents, antihypertensive agents, lipid-lowering agents, and treatments for chronic obstructive pulmonary disease and asthma. Matching between GPP and PV study cohorts was performed using greedy nearest neighbor matching without replacement at a ratio of up to 1:4, with a caliper width of 0.2 SD of the logit of the propensity scores.
Recurrent flare rates were calculated among patients who experienced at least one recurrence of flares, using the 12-week flare episode definition described above. Conditional Poisson regression was used to compare the HCRU and rate ratios for recurrent flare events between patients with GPP and PV. For cost analysis, a generalized linear model (GLM) with a gamma distribution was applied when the number of zero-cost observations was fewer than 10, with zero replaced by 1×10−10 to allow for log transformation. If more than 10 zero-cost observations were present, a two-stage model was used, consisting of logistic regression followed by a GLM with a gamma distribution to appropriately account for the excess zeros.16 Cost ratios were estimated from generalized linear models with a log link and gamma distribution using model-derived mean costs. 95% confidence intervals (CIs) were estimated for all comparisons. For the two-stage model, the 95% CIs were calculated using 1,000 bootstrap replications.
All statistical analyses were performed using SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Patient Demographic and Baseline Characteristics
A total of 245 patients with GPP were identified based on the study criteria (Figure 1). The mean age at enrollment was 51.3 ± 16.8 years, and 49.8% were male (Table 1). The most common comorbidities were hypertension (27.8%), diabetes (19.2%), dyslipidemia (15.5%), and thyroid disease (18.0%). The mean CCI score was 0.8 ± 1.3. Regarding comedication use, antidiabetic agents were used by 13.5% of patients, antihypertensive agents by 35.5%, and lipid-lowering agents by 15.1%. Severe index flares were observed in 9.0% of patients.
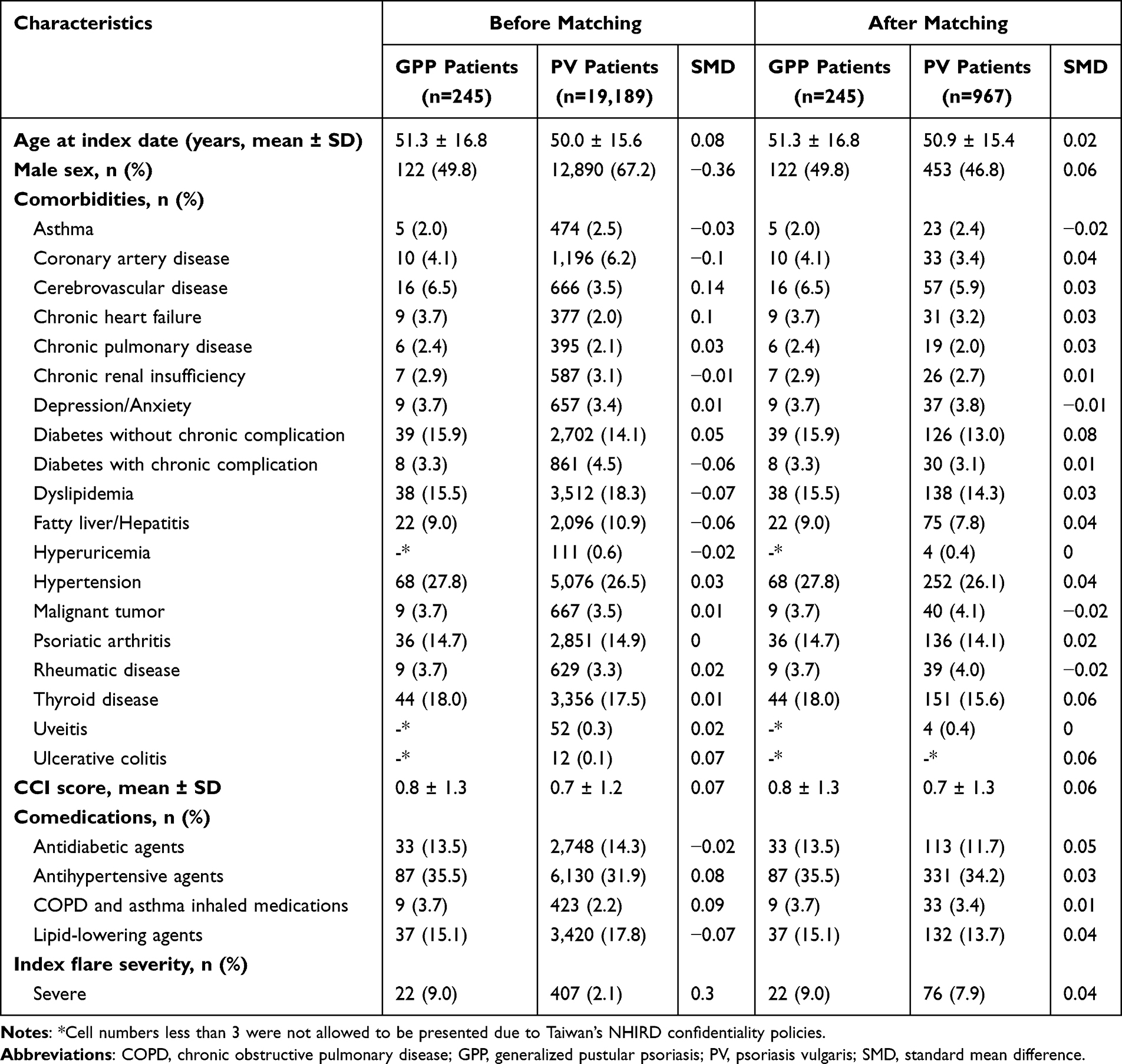 |
Table 1 Patient Baseline Demographic and Clinical Characteristics |
 |
Figure 1 Flowchart of patient selection for GPP and PV cohorts. Abbreviations: GPP, generalized pustular psoriasis; PV, plaque psoriasis. |
Before matching, compared with patients with PV, those with GPP were similar in age and comorbidity profile; however, a lower proportion of GPP patients were male (49.8% vs. 67.2%), and a greater proportion experienced a severe index flare (9.0% vs. 2.1%). After propensity score matching, baseline characteristics were well balanced between the two cohorts (Table 1).
GPP Flare Severity and Treatment
Among the patients with GPP, 1,156 moderate-to-severe flares were recorded during follow-up, of which 93.0% were moderate and 7.0% were severe (Table 2). All flare episodes were treated with systemic therapy, most commonly prednisolone (47.2%), methotrexate (39.3%), acitretin (30.2%), and cyclosporine (26.7%). Biologic therapy was less frequently used, with adalimumab (9.1%) and ustekinumab (7.3%) being the most commonly prescribed biologic agents.
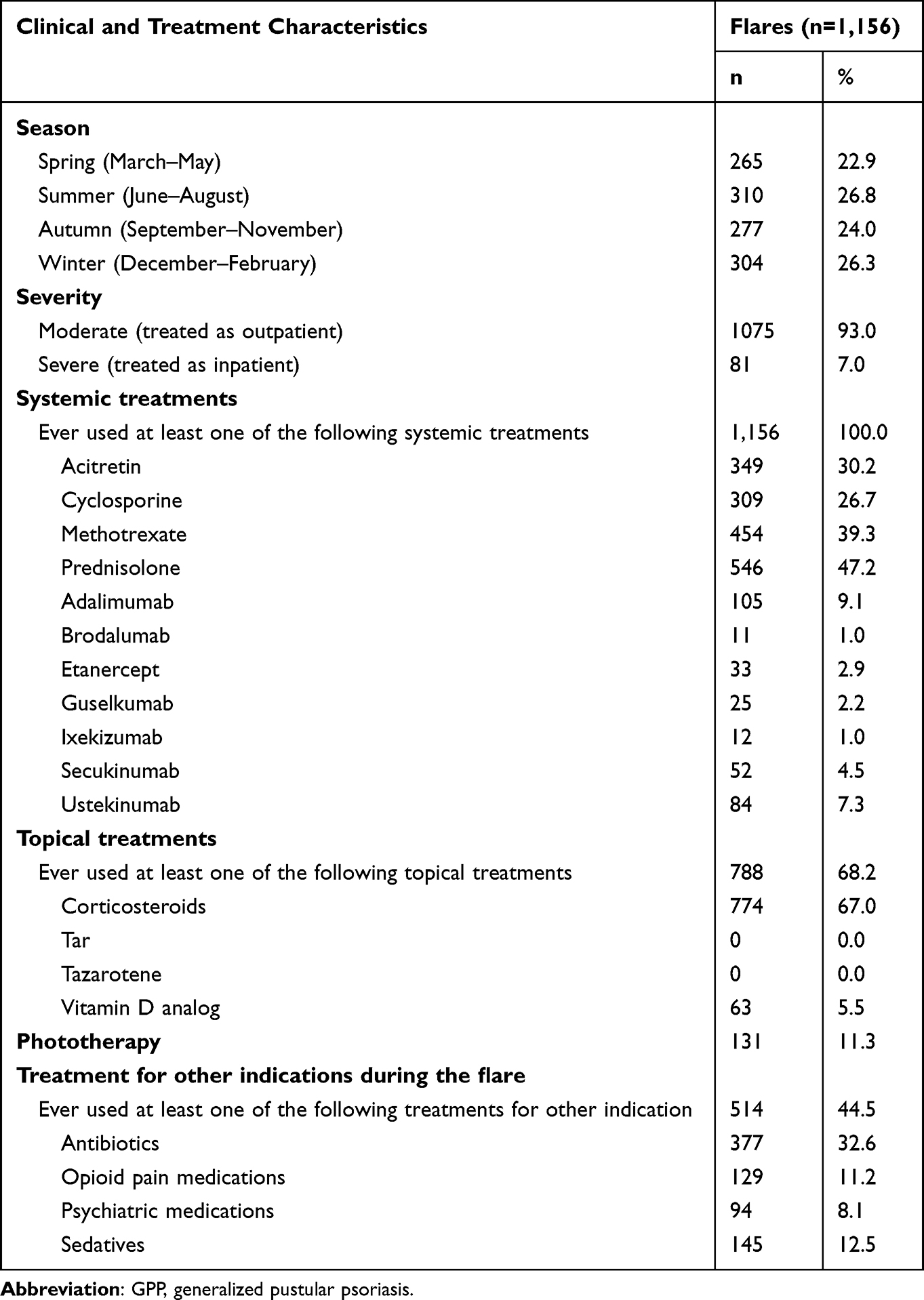 |
Table 2 Clinical and Treatment Characteristics of GPP Flares During Follow-Up |
Topical treatments were used in 68.2% of flares, primarily corticosteroids (67.0%), while phototherapy was administered in 11.3% of cases. Treatments for other indications were also common (44.5%), most commonly antibiotics (32.6%), sedatives (12.5%), opioid analgesics (11.2%), and psychiatric medications (8.1%).
Frequency of Recurrent Flares
In the GPP group, 243 of 245 (99.2%) patients experienced at least one recurrent flare during follow-up (Table 3). Among patients with recurrence, the median follow-up was 2.9 (1.8–3.5) years for GPP and 2.7 (1.7–3.4) years for PV. The overall recurrent flare event rate was 4.0 per 1,000 patient-days (95% CI, 3.7–4.2), with 3.7 per 1,000 patient-days attributable to moderate flares and 0.3 per 1,000 patient-days to severe flares.
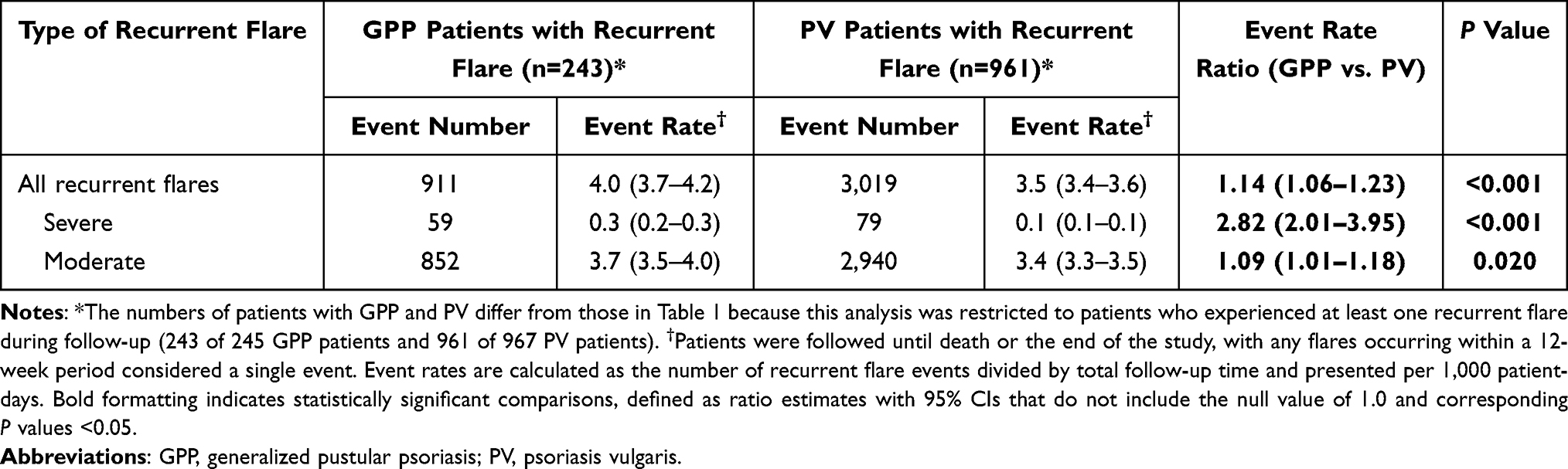 |
Table 3 Comparison of Recurrent Flare Event Rates Between Patients with GPP and PV Who Experienced Recurrence |
Compared with patients with PV, those with GPP exhibited a higher overall recurrent flare event rate (rate ratio, 1.14; 95% CI, 1.06–1.23). When stratified by severity, the rate ratio was 2.82 (95% CI, 2.01–3.95) for severe flares and 1.09 (95% CI, 1.01–1.18) for moderate flares.
HCRU
Table 4 summarizes HCRU among patients with GPP and PV. During the 12-week period following the index flare, patients with GPP had a mean of 0.2 ± 0.6 emergency room (ER) visits, 7.0 ± 4.7 OPD visits, 0.3 ± 0.6 IPD admissions, and 0.0 ± 0.1 ICU stays. Compared with patients with PV, those with GPP showed higher utilization of services in the ER (incidence rate ratios [IRR], 1.43 [95% CI 1.04–1.97]), OPD (1.11 [1.05–1.17]), and IPD (1.92 [1.46–2.51]) during this early post-flare period.
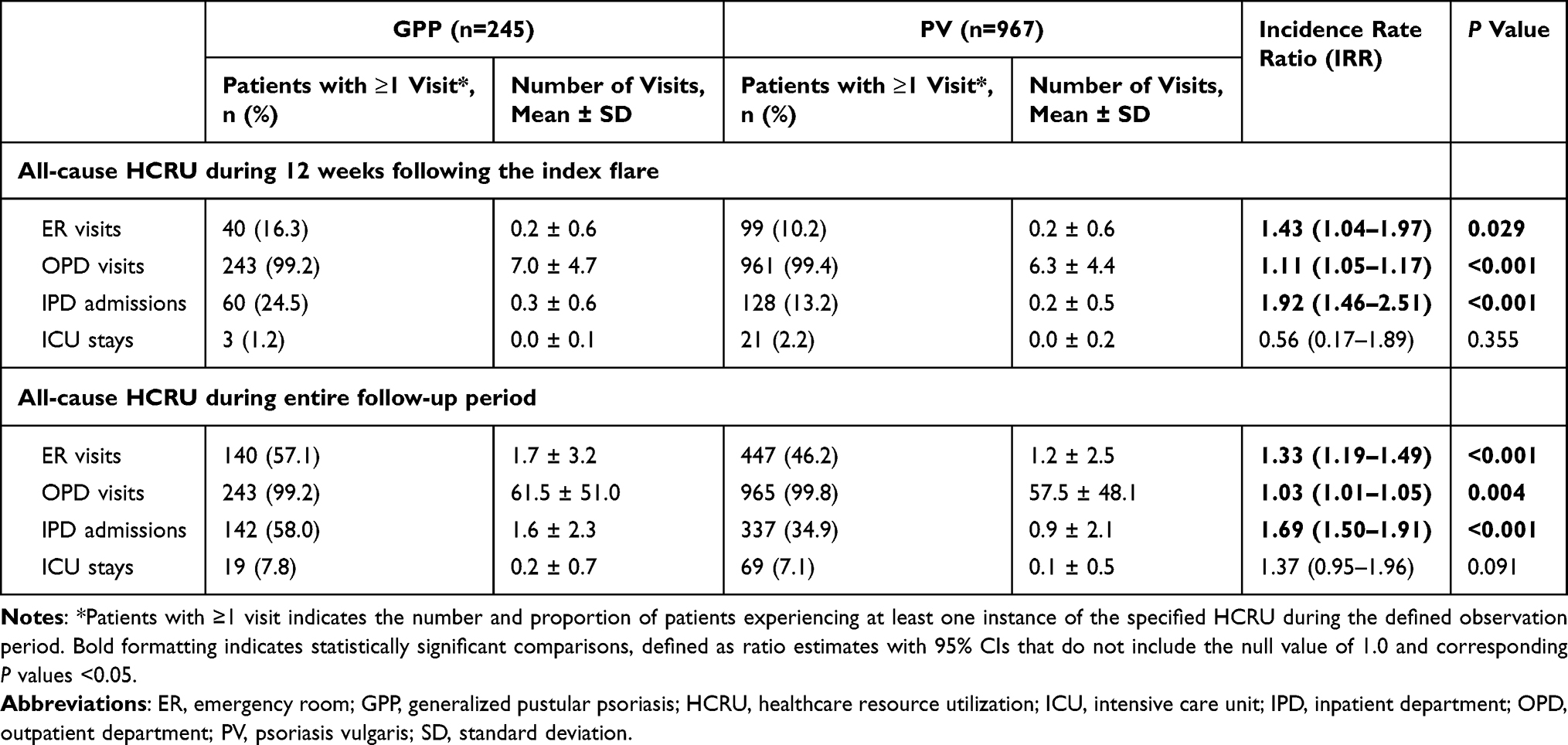 |
Table 4 Comparison of HCRU Between Patients with GPP and PV Following Disease Flares |
The median duration of complete follow-up was 3.1 (2.0–3.7) years for patients with GPP and 3.0 (1.9–3.6) years for patients with PV. Over the entire follow-up period, patients with GPP consistently demonstrated greater HCRU, including more ER visits (1.33 [1.19–1.49]), OPD visits (1.03 [1.01–1.05]), and IPD admissions (1.69 [1.50–1.91]), compared with patients with PV.
Healthcare Costs
During the 12-week period following the index flare, patients with GPP experienced a pronounced economic burden, with a median total healthcare cost of USD 579.70, substantially higher than that observed among patients with PV (USD 274.40) (Table 5). Outpatient care accounted for the largest share of costs in this early post-flare period, and patients with GPP incurred significantly higher outpatient costs than those with PV (cost ratio, 1.40; 95% CI, 1.09–1.80).
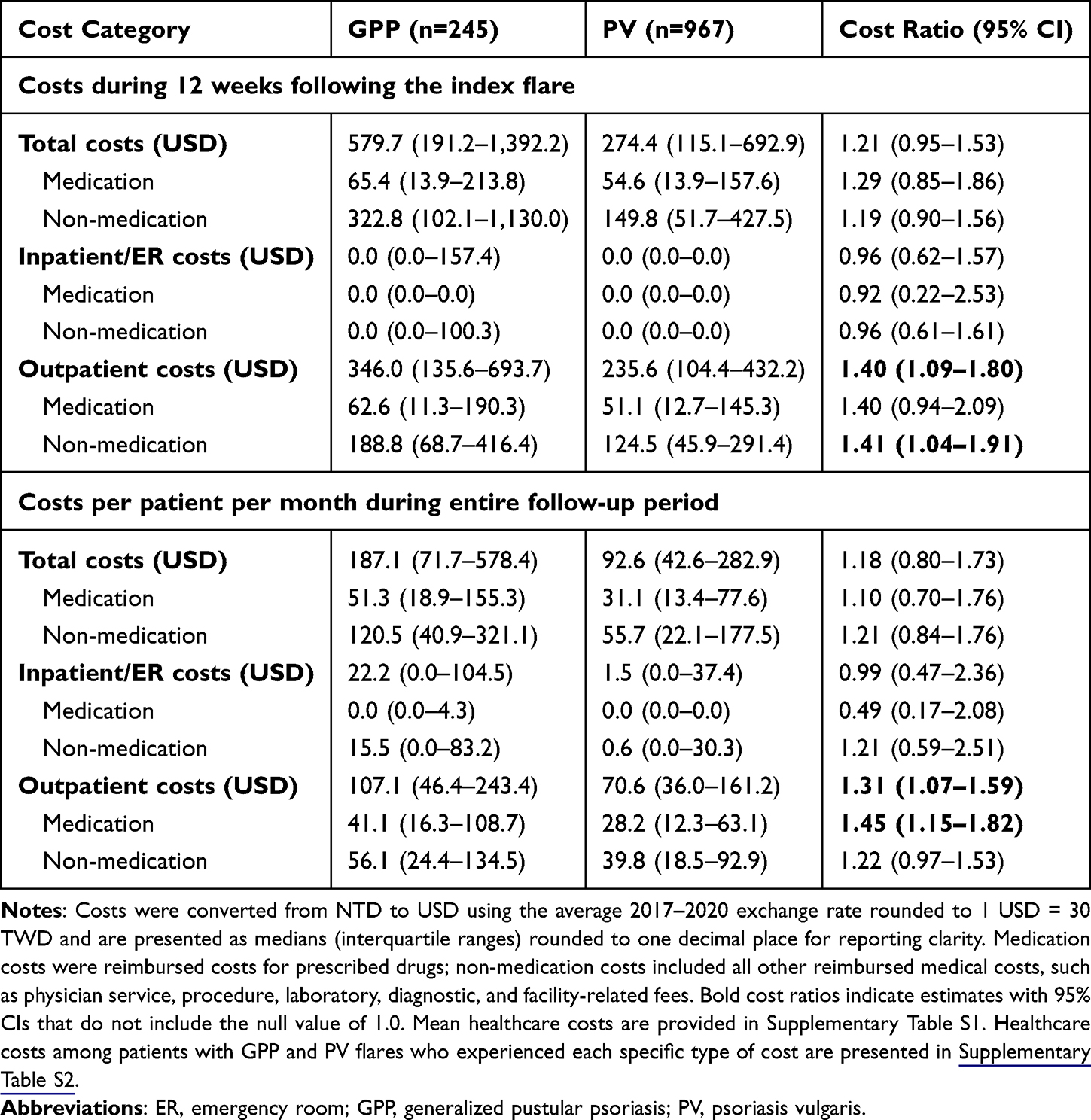 |
Table 5 Healthcare Costs Among Patients with GPP and PV Following Disease Flares |
Over the entire follow-up period, the median total healthcare cost among patients with GPP was USD 187.10 per patient per month, approximately twice that of patients with PV (USD 92.60). Outpatient services remained the dominant contributor to overall costs, with consistently higher outpatient expenditures observed in the GPP group (cost ratio, 1.31; 95% CI, 1.07–1.59). In contrast, differences in IPD and ER costs between groups were not statistically significant across either time horizon. Mean healthcare costs for the corresponding analyses are provided in Supplementary Table S1.
Discussion
This study comprehensively examined the clinical characteristics and disease burden associated with GPP, providing valuable insights into its demographic, clinical, and economic aspects and underscoring its significant impact on patients.
Our analysis showed that patients with GPP in Taiwan had a mean age of approximately 51 years, with a nearly equal distribution between males and females. This finding aligns with previous research indicating that GPP affects a broad age range, with mean or median ages around 50 years.20–22 Interestingly, a multiethnic study reported variations in the age of onset among different ethnic groups, with Chinese patients exhibiting an earlier peak onset (20–39 years) compared with Malay and Indian patients (40–49 years).23 Additionally, the prevalence of GPP varied across ethnicities, with the highest prevalence observed in the Chinese population (271 per million), followed by Malay (186 per million) and Indian (179 per million) populations. This difference may be attributable to a higher prevalence of IL36RN mutations among Chinese patients (27%) compared with Malay (17%) and Indian (0%) patients.24 These findings are consistent with another study which indicated that the prevalence of GPP appears to be higher in Asia,11 highlighting potential ethnic differences and variability in disease manifestation across populations.
Consistent with our findings, studies have reported that GPP affects both sexes relatively equally.20,22 In contrast, a population-based study conducted in Malaysia reported a higher GPP prevalence among females, with a female-to-male ratio of 2:1 ratio and period prevalence rates of 267 and 127 per million in females and males, respectively. In that study, prevalence was consistently higher among females across all age groups, peaking at 40–59 years, while prevalence among males peaked after the age of 60 years.23 The differing sex distributions observed between our study and this prior report warrant further investigation to determine whether they reflect population-specific characteristics or other underlying factors.
Our study revealed a high prevalence of comorbid conditions among patients with GPP, consistent with broader observations in psoriasis populations. Cardiovascular and metabolic comorbidities were particularly prevalent, followed by thyroid disease, while approximately 4% of patients had a psychiatric disorder. Similarly, a previous study identified hypertension, hyperlipidemia, and diabetes as common comorbidities of GPP, along with thyroid disorders, depression, and anxiety as frequently observed conditions.25
GPP is characterized by recurrent and prolonged flares that substantially contribute to the overall disease burden. A systematic review by Bhutani et al13 reported that patients typically experience annual flares lasting from two weeks to three months, and that more than 80% of patients experience residual disease following flare resolution. Such episodes can significantly impact daily activities and mental health, often leading to or exacerbating anxiety and depression.13 Prior literature on these interrelationships underscores the importance of a comprehensive, multidisciplinary approach to GPP management that addresses dermatologic manifestations as well as associated systemic and psychological comorbidities.26
HCRU among patients with GPP was high, with a mean of 61.5 OPD visits per patient over a median follow-up time of 3.1 years. IPD and ER visits were more frequent in the GPP group than in the PV group, likely reflecting the acute and systemic nature of GPP flares. Widespread pustular eruptions and epidermal barrier disruption may contribute to pain, fluid loss, secondary infection, sepsis, organ dysfunction, and other complications requiring urgent or intensive medical care. Studies from Japan, Sweden, and the United States have similarly reported higher HCRU among patients with GPP, including longer hospital stays and more frequent healthcare provider visits compared to both the general population and patients with PV or plaque psoriasis.27–29 These findings highlight the substantial disease burden and economic impact of GPP compared with PV.
In our study, patients with GPP exhibited higher recurrence rates, more severe flares, and greater HCRU, translating into higher healthcare costs compared with patients with PV. This finding is consistent with prior studies reporting higher direct healthcare costs and more intensive healthcare needs among patients with GPP than those with PV, plaque psoriasis, or the general population.28,30 For example, Wang et al reported that a higher proportion of patients with GPP required hospitalization than patients with PV (22.0% vs. 7.8%), and that hospital stays were longer among patients with GPP, underscoring the severe and resource-intensive nature of the disease.31
Notably, although we anticipated that costs would be concentrated in the immediate post-flare period, total costs during the 12 weeks following the index flare were not disproportionately higher than those observed over the entire follow-up period. This pattern likely reflects a highly skewed, zero-inflated distribution of inpatient and ER utilization, in which many patients did not require acute care during the initial 12-week window, whereas a small subgroup accounted for the majority of early expenditures. Accordingly, when restricting analyses to patients who incurred any inpatient or ER costs (Supplementary Table S2), 12-week post-flare expenditures were markedly higher than the overall per-patient average, indicating substantial cost concentration among those requiring acute care. In addition, because our estimates represent all-cause rather than GPP-attributable costs, flare-related differences may be attenuated.
Treatment and cost patterns should also be interpreted in the context of the 2016–2020 study period, when no GPP-specific therapy had been approved. Management during this period largely relied on conventional systemic agents, corticosteroids, and biologics approved for plaque psoriasis or psoriatic disease. Spesolimab, an IL-36 receptor antagonist and the first approved treatment for GPP flares, was approved after the observation period. Thus, the treatment patterns, HCRU, and costs observed in this study reflect the pre-GPP-specific therapy era and may differ from current practice, in which targeted IL-36 pathway inhibition is available. In addition, biologic uptake may be limited in routine clinical practice,32,33 and treatment initiation can be delayed by access and reimbursement processes, such that biologic-related costs may accrue beyond the initial 12-week period. Taken together, these findings suggest that the economic impact of GPP arises from both acute flares and sustained care needs over time, underscoring the importance of effective management strategies to reduce flares and mitigate downstream HCRU.
Our study has several strengths. First, it leveraged large-scale national insurance data, providing a comprehensive overview of GPP in Taiwan. Given the rarity of GPP, use of a population-based database is especially valuable for capturing a sufficiently large sample to enable robust analyses of clinical characteristics, disease burden, HCRU, and economic impact. Analysis of real-world claims data offers valuable insights into disease management across diverse patient populations. Second, inclusion of a comparison cohort of patients with PV strengthened the study’s validity by enabling direct comparisons and highlighting unique features to GPP. Third, the detailed examination of treatment patterns further enriched the understanding of GPP management strategies.
Despite its strengths, this study has several limitations. First, because this study relies on administrative claims data, GPP cases were identified based on ICD codes rather than confirmed through chart review, which may have resulted in underestimation of disease burden due to misdiagnosed or undiagnosed cases. Second, clinical severity scores, including GPPASI, GPPGA, and PASI, were unavailable in the claims database. Therefore, flare severity was operationalized using healthcare setting as a proxy. Although this approach reflects clinically meaningful differences in healthcare intensity, it may not fully capture skin involvement, systemic manifestations, or physician-assessed disease severity. Third, key clinical details, such as IL36RN mutation status, are also unavailable in the claims database. In addition, chronic infections were not included in the predefined baseline covariate set, although they may influence subsequent risk profiles, HCRU, and costs. These unmeasured or unaccounted factors may have contributed to residual confounding. Finally, we could not distinguish GPP-specific HCRU and costs from those attributable to other causes. Consequently, our analysis reflects overall HCRU and costs rather than those directly attributable to GPP. Future studies incorporating disease-specific information could improve the accuracy of disease characterization and provide more precise assessments of HCRU and economic burden.
Building on these findings, coordinated multidisciplinary care that addresses cardiometabolic, endocrine, and mental health comorbidities may be warranted. Earlier, proactive control of flares with timely use of biologics or other advanced therapies, when appropriate, may help reduce recurrence, HCRU, and costs. Further research comparing treatment approaches and their cost-effectiveness could help clarify optimal care pathways, alongside investigations into genetic and environmental contributors to support more individualized management. A systematic assessment of psychosocial impact and quality of life could further inform comprehensive patient-centered care.
Conclusion
This study underscores the substantial clinical and economic burden of GPP. Patients with GPP had frequent comorbidities and recurrent flares and, compared with matched patients with PV, they experienced higher HCRU and outpatient costs. These findings highlight the need for comprehensive management strategies to reduce flares, prevent complications, and mitigate downstream HCRU. Continued evaluation of emerging treatment approaches has the potential to further optimize the care and management of patients with GPP.
Data Sharing Statement
The data used in this study are subject to ethical and legal restrictions. The de-identified datasets from Taiwan are regulated by the Ministry of Health and Welfare and cannot be shared publicly. Additional details can be provided by the corresponding author upon a reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Chang Gung Medical Foundation Institutional Review Board (No. 202200813B0), and informed consent was waived due to the use of de-identified data.
Acknowledgments
This study utilized data from the National Health Insurance Research Database, provided by the National Health Insurance Administration under Taiwan’s Ministry of Health and Welfare and managed by the Health and Welfare Data Science Center.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This investigator-initiated study was supported by Boehringer Ingelheim Taiwan. The study design, conduct, analysis, and interpretation were performed entirely by the academic authors. The sponsor had no involvement in the study methodology, data analysis, interpretation of results, or the decision to publish.
Disclosure
FJL received a research grant from Boehringer Ingelheim Taiwan. This support did not constitute a conflict of interest. All other authors declare no conflicts of interest in this work.
References
1. Rivera-Díaz R, Daudén E, Carrascosa JM, Cueva P, Puig L. Generalized Pustular Psoriasis: a Review on Clinical Characteristics, Diagnosis, and Treatment. Dermatol Ther. 2023;13(3):673–12. doi:10.1007/s13555-022-00881-0
2. Löfvendahl S, Norlin JM, Schmitt-Egenolf M. Prevalence and incidence of generalized pustular psoriasis in Sweden: a population-based register study. Br J Dermatol. 2022;186(6):970–976. doi:10.1111/bjd.20966
3. Bachelez H, Barker J, Burden AD, Navarini AA, Krueger JG. Generalized pustular psoriasis is a disease distinct from psoriasis vulgaris: evidence and expert opinion. Expert Rev Clin Immunol. 2022;18(10):1033–1047. doi:10.1080/1744666X.2022.2116003
4. Fujita H, Gooderham M, Romiti R. Diagnosis of Generalized Pustular Psoriasis. Am J Clin Dermatol. 2022;23(Suppl 1):31–38. doi:10.1007/s40257-021-00652-1
5. Bachelez H. Pustular psoriasis and related pustular skin diseases. Br J Dermatol. 2018;178(3):614–618. doi:10.1111/bjd.16232
6. Setta-Kaffetzi N, Navarini AA, Patel VM, et al. Rare Pathogenic Variants in IL36RN Underlie a Spectrum of Psoriasis-Associated Pustular Phenotypes. J Invest Dermatol. 2013;133(5):1366–1369. doi:10.1038/jid.2012.490
7. Akiyama M. Updated genetic background of generalized pustular psoriasis as an autoinflammatory keratinization disease. J Dermatol. 2024. doi:10.1111/1346-8138.17585
8. Menter A, Van Voorhees AS, Hsu S. Pustular Psoriasis: a Narrative Review of Recent Developments in Pathophysiology and Therapeutic Options. Dermatol Ther. 2021;11(6):1917–1929. doi:10.1007/s13555-021-00612-x
9. Hawkes JE, Chan TC, Krueger JG. Psoriasis pathogenesis and the development of novel targeted immune therapies. J Allergy Clin Immunol. 2017;140(3):645–653. doi:10.1016/j.jaci.2017.07.004
10. Choon SE, Lai NM, Mohammad NA, Nanu NM, Tey KE, Chew SF. Clinical profile, morbidity, and outcome of adult-onset generalized pustular psoriasis: analysis of 102 cases seen in a tertiary hospital in Johor, Malaysia. Int J Dermatol. 2014;53(6):676–684. doi:10.1111/ijd.12070
11. Feng JN, Guo JZ, Zhang Q, et al. Higher Prevalence of Generalized Pustular Psoriasis in Asia? A Population-Based Study Using Claim Data in China and a Systematic Review. Dermatology. 2023;239(2):195–205. doi:10.1159/000528850
12. Ericson O, Löfvendahl S, Norlin JM, Gyllensvärd H, Schmitt-Egenolf M. Mortality in generalized pustular psoriasis: a population-based national register study. J Am Acad Dermatol. 2023;89(3):616–619. doi:10.1016/j.jaad.2023.04.066
13. Bhutani T, Farberg AS. Clinical and Disease Burden of Patients with Generalized Pustular Psoriasis: a Review of Real-World Evidence. Dermatol Ther. 2024;14(2):341–360. doi:10.1007/s13555-024-01103-5
14. Feldman SR, Goffe B, Rice G, et al. The Challenge of Managing Psoriasis: unmet Medical Needs and Stakeholder Perspectives. Am Health Drug Benefits. 2016;9(9):504–513.
15. DiBonaventura M, Carvalho AVE, Souza CDS, Squiassi HB, Ferreira CN. The association between psoriasis and health-related quality of life, work productivity, and healthcare resource use in Brazil. An Bras Dermatol. 2018;93(2):197–204. doi:10.1590/abd1806-4841.20186069
16. Prignano F, Atzori L, Bellinato F, et al. Epidemiology, Characteristics of Disease, and Unmet Needs of Patients with Generalized Pustular Psoriasis: a Large Italian Delphi Consensus. Dermatology. 2024;240(3):414–424. doi:10.1159/000538072
17. Hsieh CY, Su CC, Shao SC, et al. Taiwan’s National Health Insurance Research Database: past and future. Clin Epidemiol. 2019;11:349–358. doi:10.2147/clep.S196293
18. Seishima M, Fujii K, Mizutani Y. Generalized Pustular Psoriasis in Pregnancy: current and Future Treatments. Am J Clin Dermatol. 2022;23(5):661–671. doi:10.1007/s40257-022-00698-9
19. Central Bank of the Republic of China (Taiwan). Exchange Rates of the N.T. Dollar Against the U.S. Dollar: interbank Spot Market Closing Rates (Period Average). Available from: https://www.cbc.gov.tw/en/cp-480-1879-66035-2.html.
20. Viguier M, Bentayeb M, Azzi J, et al. Generalized pustular psoriasis: a nationwide population-based study using the National Health Data System in France. J Eur Acad Dermatol Venereol. 2024;38(6):1131–1139. doi:10.1111/jdv.19901
21. Ohata C, Tsuruta N, Yonekura K, et al. Clinical characteristics of Japanese pustular psoriasis: a multicenter observational study. J Dermatol. 2022;49(1):142–150. doi:10.1111/1346-8138.16217
22. Zelickson BD, Muller SA. Generalized pustular psoriasis. A review of 63 cases. Arch Dermatol. 1991;127(9):1339–1345.
23. Choon SE, Wright AK, Griffiths CEM, et al. Incidence and prevalence of generalized pustular psoriasis in multiethnic Johor Bahru, Malaysia: a population-based cohort study using routinely captured electronic health records in the Teleprimary Care (TPC®) clinical information system from 2010 to 2020. Br J Dermatol. 2023;189(4):410–418. doi:10.1093/bjd/ljad158
24. Tsai T-F. Heterogeneity of generalized pustular psoriasis in multiethnic Johor Bahru, Malaysia. Br J Dermatol. 2023;189(4):361–362. doi:10.1093/bjd/ljad197
25. Morita A, Kotowsky N, Gao R, Shimizu R, Okubo Y. Patient characteristics and burden of disease in Japanese patients with generalized pustular psoriasis: results from the Medical Data Vision claims database. J Dermatol. 2021;48(10):1463–1473. doi:10.1111/1346-8138.16022
26. Strober B, Leman J, Mockenhaupt M, et al. Unmet Educational Needs and Clinical Practice Gaps in the Management of Generalized Pustular Psoriasis: global Perspectives from the Front Line. Dermatol Ther. 2022;12(2):381–393. doi:10.1007/s13555-021-00661-2
27. Okubo Y, Kotowsky N, Gao R, Saito K, Morita A. Clinical characteristics and health-care resource utilization in patients with generalized pustular psoriasis using real-world evidence from the Japanese Medical Data Center database. J Dermatol. 2021;48(11):1675–1687. doi:10.1111/1346-8138.16084
28. Löfvendahl S, Norlin JM, Schmitt-Egenolf M. Economic Burden of Generalized Pustular Psoriasis in Sweden: a Population-Based Register Study. Psoriasis. 2022;12:89–98. doi:10.2147/ptt.S359011
29. Crowley J, Golembesky AK, Kotowsky N, et al. Clinical Characteristics and HealthCare Resource Utilization in Patients With Generalized Pustular Psoriasis: real-World Evidence From a Large Claims-Based Dataset. J Psoriasis Psoriatic Arthritis. 2021;6(3):151–158. doi:10.1177/24755303211021786
30. Hanna ML, Singer D, Valdecantos WC. Economic burden of generalized pustular psoriasis and palmoplantar pustulosis in the United States. Curr Med Res Opin. 2021;37(5):735–742. doi:10.1080/03007995.2021.1894108
31. Wang HM, Xu JM, Jin HZ. Characteristics and Burdens of Disease in Patients from Beijing with Generalized Pustular Psoriasis and Palmoplantar Pustulosis: multicenter Retrospective Cohort Study Using a Regional Database. Am J Clin Dermatol. 2023;24(6):991–1002. doi:10.1007/s40257-023-00807-2
32. Strober B, Kwiatkowski H, Lavasani L, et al. Real-world treatment patterns in patients with generalized pustular psoriasis: a US-based claims study. J Am Acad Dermatol. 2026;94(1):104–112. doi:10.1016/j.jaad.2025.08.089
33. Lu CW, Tseng CY, Wang CW, et al. Clinical Characteristics and Disease Burden of Patients with Moderate-to-Severe Generalized Pustular Psoriasis Flares in Taiwan. Dermatol Ther. 2024;14(8):2261–2275. doi:10.1007/s13555-024-01228-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.