Back to Journals » Infection and Drug Resistance » Volume 19
Clinical Characteristics, Antimicrobial Resistance Profiles and Carbapenemases Genotypes of Providencia rettgeri: A 5-Year Retrospective Study in a Tertiary Teaching Hospital in Northern China
Authors Li Y, Wang Y, Chen D, Yang W, Lan H, Ju L ![]() , Min R
, Min R ![]() , Wang P, Cao J
, Wang P, Cao J ![]()
Received 13 March 2026
Accepted for publication 2 June 2026
Published 12 June 2026 Volume 2026:19 605665
DOI https://doi.org/10.2147/IDR.S605665
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Ying Li,1,* Yan Wang,1,* Diandian Chen,1 Wenshuo Yang,1 He Lan,1 Leyang Ju,1 Rong Min,1 Peichang Wang,1,2 Jingrong Cao1,2
1Department of Clinical Laboratory, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 2Department of Clinical Laboratory, Xiongan Xuanwu Hospital, Xiongan New Area, Hebei, 070001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingrong Cao, Department of Clinical Laboratory, Xuanwu Hospital Capital Medical University, No. 45 Changchun Street, Xicheng District, Beijing, 100053, People’s Republic of China, Email [email protected] Peichang Wang, Department of Clinical Laboratory, Xuanwu Hospital Capital Medical University, No. 45 Changchun Street, Xicheng District, Beijing, 100053, People’s Republic of China, Email [email protected]
Background: Providencia rettgeri is an emerging opportunistic pathogen linked with healthcare-associated infections and increasing antimicrobial resistance. This study aimed to characterize the clinical features, antimicrobial resistance profiles and carbapenemase genotypes of P. rettgeri isolates in a tertiary teaching hospital in northern China.
Methods: A 5-year retrospective study (2021– 2025) was conducted at Xuanwu Hospital. Isolates were identified using MALDI-TOF MS, with 16S rRNA sequencing as the gold standard for ambiguous results. Antimicrobial susceptibility testing followed CLSI guidelines, including disk diffusion, broth disk elution assays and Vitek 2 automated systems. Carbapenemases and the genotypes were detected by gold immunochromatography, multiplex fluorescent PCR (mPCR) and whole genome sequencing (WGS).
Results: Twenty-five non-duplicate P. rettgeri isolates were collected, primarily from urine (44.0%, 11/25), followed by drainage and secretions (24.0%, 6/25). Multidrug resistance (MDR) was observed in 88.0% (22/25) of isolates, including 52.0% (13/25) carbapenem-resistant P. rettgeri (CRPR) strains. Ceftazidime-avibactam (CZA) showed no in vitro activity against CRPR isolates, while aztreonam-avibactam (AZA) exhibited activity against 61.5% (8/13) of CRPR isolates. The immunochromatography assay identified NDM-type carbapenemase production and mPCR detected the presence of blaNDM gene in all CRPR isolates. WGS combined with Sanger sequencing validated that all CRPR isolates harbored the blaNDM-1 gene. In addition, 92.3% (12/13) CRPR isolates co-harboring blaOXA-10 and 61.5% (8/13) isolates resistant to aztreonam also harbored blaPER genes.
Conclusion: P. rettgeri isolates in our study exhibited high rates of MDR and carbapenem resistance with the presence of the blaNDM-1 gene. The co-occurrence of blaNDM-1, blaOXA-10 and blaPER in these CRPR isolates might complicate the antimicrobial resistant mechanisms. AZA exhibited the better in vitro activity against CRPR isolates compared to other antimicrobials, though its clinical efficacy remains to be validated. Continuous surveillance and further mechanistic studies are critical to combat this emerging threat.
Keywords: Providencia rettgeri, antimicrobial resistance, carbapenemase, aztreonam-avibactam, whole-genome sequencing
Introduction
Providencia rettgeri, a member of the Enterobacterales order, is an opportunistic pathogen linked with healthcare-associated infections, particularly in immunocompromised patients or those with indwelling devices.1,2 Clinical manifestations include urinary tract infections (UTIs), pneumonia, bacteremia, neonatal sepsis, meningitis, endocarditis and diarrhea.3,4 Unlike other Enterobacterales, Providencia species exhibit intrinsic resistance to multiple antimicrobial classes including ampicillin, first-generation cephalosporins, polymyxins and tigecycline,5 which severely limits treatment options for infections caused by this species. The emergence of multidrug-resistant (MDR) even carbapenem-resistant P. rettgeri (CRPR) has further narrowed therapeutic choices, as carbapenems are often the last line of defense against MDR Enterobacterales.2,6 At present, due to the significantly lower clinical isolation rate of P. rettgeri compared to other Enterobacteriaceae bacteria (such as Escherichia coli and Klebsiella pneumoniae), there is limited international research on the epidemiology and drug resistance profiles of P. rettgeri.7,8 In China, relevant studies are also scarce. Our study represents the first comprehensive analysis of P. rettgeri clinical isolates from a tertiary teaching hospital in northern China, filling an important gap in the regional epidemiological data of P. rettgeri.
Novel β-lactam/β-lactamase inhibitor combinations (BLBLICs), namely ceftazidime-avibactam (CZA) and aztreonam-avibactam (AZA), have shown promise against carbapenemase-producing Enterobacterales (CPE), targeting serine and metallo-β-lactamases (MBLs)-producing isolates, respectively.9,10 However, data on their efficacy against P. rettgeri remains scarce, especially in the Chinese clinical setting. Previous studies have indicated that MBLs (such as NDM, IMP) are the predominant mechanisms of CRPR,6,11 which limited the activity of CZA to conquer CRPR. However, the potential activity of AZA against CRPR remains unclear, particularly in China. This study aims to investigate this issue about P. rettgeri and discuss the underlying resistance mechanisms preliminarily.
Materials and Methods
Isolates Collection and Identification
P. rettgeri isolates were collected from January 2021 to December 2025 at Xuanwu Hospital, a 1500-bed tertiary teaching hospital in Beijing, China. Isolates were identified via MALDI-TOF MS (Bruker Daltonics, Germany), with a score >2.000 considered reliable. For ambiguous results, 16S rRNA gene sequencing was performed as the gold standard.12 Isolates were classified as clinical infection pathogens if they met the following criteria: (1) for urine isolates: >105 CFU/mL growth with >10 WBC/high power field (HPF) on urinalysis and clinical signs of urinary tract infection (fever, dysuria or flank pain); (2) for other sites: growth from a normally sterile site or growth from a non-sterile site with corresponding clinical signs of infection. Colonizing isolates (low colony counts from non-sterile sites without clinical signs of infection) were excluded from the analysis. However, due to the retrospective nature of the study, some misclassification may still have occurred, particularly for urine isolates from catheterized patients. Duplicate isolates from the same source within 10 days were also excluded.
Clinical Data Collection
Clinical data were retrieved from electronic medical records, including patient demographics (age, gender, wards), underlying diseases, infection sites, antimicrobial therapy history and clinical outcomes. The study was approved by the Medical Ethics Committee of Xuanwu Hospital (XA[KS2024] 039–002), and informed consent was waived due to its retrospective nature. The patients data were maintained with confidentiality, and all procedures were performed in accordance with the principles of the Declaration of Helsinki.
Antimicrobial Susceptibility Testing (AST)
Minimum inhibitory concentrations (MICs) were determined using the Vitek 2 Compact system with AST-N334 cards (bioMérieux, France), following Clinical and Laboratory Standards Institute (CLSI) M100 guidelines (36th edition),13 with Escherichia coli ATCC 25922, Pseudomonas aeruginosa ATCC 27853 and Staphylococcus aureus ATCC 29213 as the quality control strains. For CRPR isolates, disk diffusion assays were performed for aztreonam (ATM, 30 μg), ceftazidime-avibactam (CZA, 30/20 μg) and aztreonam-avibactam (AZA, 30/20 μg), with results interpreted using CLSI M100 (36th edition) breakpoints.13 The in vitro effectiveness of CZA in combination with aztreonam on CRPR isoaltes was evaluated through a disk synergy method described previously, with an increase in inhibition zone diameter of ≥5 mm for either drug in the presence of the other considered synergistic.14
Broth disk elution assays were conducted as an alternative method following CLSI:13 5 mL of cation-adjusted Mueller-Hinton broth (CAMHB) was inoculated with antibiotic disks of ATM, CZA, ATM + CZA, and AZA, incubated at 35°C for 30–60 minutes, then inoculated with 0.5 McFarland standard bacterial suspension. Tubes were incubated for 16–20 hours at 35°C, with no growth indicating being susceptible. For broth disk elution assays, E. coli ATCC 25922, Klebsiella pneumoniae ATCC BAA-1705 and K. pneumoniae ATCC BAA-2146 were used as the quality control strains according to CLSI recommendation. Interpretive breakpoints for ATM, CZA and AZA were based on CLSI M100 36th edition breakpoints for Enterobacterales, as species-specific breakpoints for P. rettgeri are not yet available.
Carbapenemase Genotypes Detection
Carbapenemase production was screened using a colloidal gold immunochromatography assay kit (Beijing Gold Mountainriver Technology Co., Ltd. China), targeting KPC, NDM, VIM, IMP, and OXA-48-like carbapenemases.15 A commercial multiplex fluorescent PCR (mPCR) kit (Shanghai BioGerm Medical Technology Co., Ltd. China) targeting common carbapenemase genes including blaKPC, blaNDM, blaIMP, and blaOXA-48 was also used as a preliminary test.16 Shallow whole genome sequencing (WGS) of all CRPR isolates were performed by Shanghai Biozeron Biotechnology Co., Ltd. (China) via next-generation sequencing (NGS) with a mean sequencing depth of 200× (range: 180–250×). NGS was performed using the Illumina HiSeq or MiSeq platform (Illumina, USA). Raw reads were trimmed with TrimGalore (v0.4.5) (https://github.com/FelixKrueger/TrimGalore) and assembled to scaffolds by SPAdes (v3.13.0) (http://bioinf.spbau.ru/spades), without further whole-genome drafts assembly. Genome annotation was performed using GeneMark 4.17 with default parameters for bacterial genomes. For antimicrobial resistance (AMR) gene detection, two complementary databases were employed: Comprehensive Antibiotic Resistance Database (CARD) (https://card.mcmaster.ca/) and NCBI AMRFinder database. Resistance genes were confirmed via BLASTn alignment (≥98% nucleotide identity, ≥90% coverage) against reference sequences.17 All blaNDM alleles detected by WGS were validated by Sanger sequencing using previously described primers.18
Statistical Analysis
Categorical variables were expressed as frequencies and percentages, and continuous variables as median with range or mean ± standard deviation. Comparisons between groups were performed using Fisher’s exact test for categorical variables, and Mann–Whitney U-test for continuous variables, as appropriate. A P value <0.05 was considered statistically significant. All statistical analyses were performed using SPSS software (version 26.0; IBM Corp., Armonk, NY, USA). Clinical demographic variables (age, gender, underlying diseases, outcomes, etc) were analyzed at the patients level (n = 23), while specimen types, resistance phenotypes and genotypes were analyzed at the isolates level (n = 25). For patients with multiple isolates, clinical characteristics were counted once per patient, while isolate-specific characteristics were counted for each isolate. Given the small sample size, all statistical comparisons are exploratory and underpowered to detect significant intergroup differences, and findings should be interpreted cautiously.
Results
Clinical Characteristics of P. rettgeri Infections
A total of 53 P. rettgeri strains were isolated from patients admitted to our hospital during the period 2021–2025. Finally, 25 clinically relevant P. rettgeri isolates from 23 patients were included. Among these patients, one patient had two P. rettgeri isolates with different antimicrobial phenotypes (from MDR to CRPR) from sputum with a period of more than 10 days, and one patient had isolated two P. rettgeri strains (both CRPR) from urine and blood sources, respectively. The median age of involved patients was 59 years (range: 26–97 years), with a male predominance (87.0%, 20/23). The most common specimen source was urine (44.0%, 11/25), followed by drainage and secretions (24.0%, 6/25), sputum (20.0%, 5/25), blood (8.0%, 2/25), and pleural effusion (4.0%, 1/25). Among patients with urinary isolates, 72.7% (8/11) had indwelling catheters or history of urinary tract surgery (such as renal transplant, nephrostomy). 56.5% (13/23) of patients had concurrent infections, including eight patients with bacterial co-infection with P. rettgeri from the same sources (5 drainage, 2 sputum, 1 urine). Clinical outcomes of P. rettgeri infection patients in this study were comparatively acceptable since cure rate reached 17.4% (4/23) patients, the partial remission rate was 52.2% (12/23), while 30.4% (7/23) of patients got no-progression or deterioration during the hospitalization, including one mortality case attributed to severe bloodstream infection by P. rettgeri. No significant difference was observed between patients from different drug-resistant phenotypes of P. rettgeri isolates in the concerning clinical characteristics (P > 0.05) (Table 1).
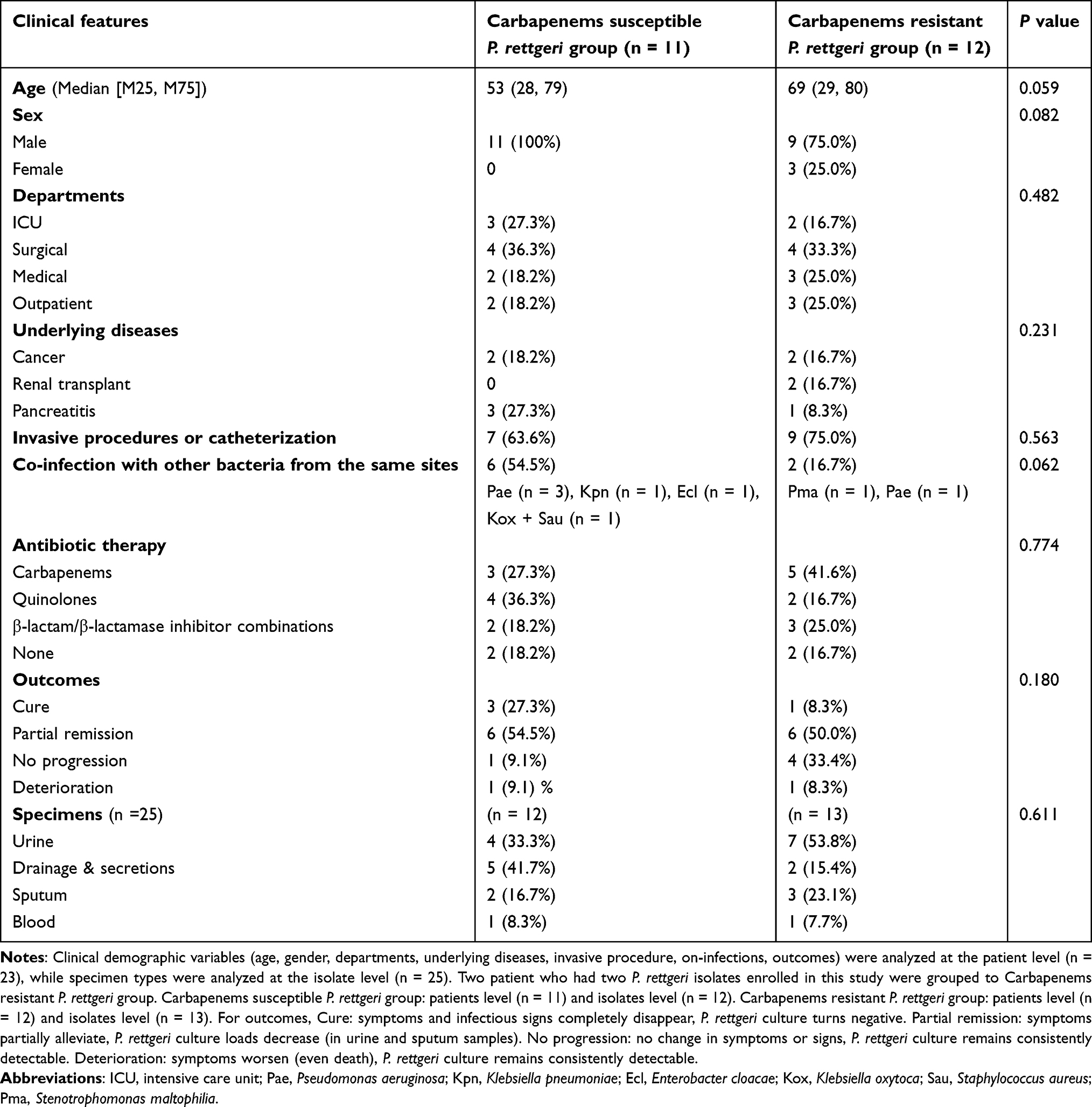 |
Table 1 Clinical characteristics of 23 patients with P. rettgeri isolates |
Antimicrobial Resistance Profiles
Of the 25 P. rettgeri isolates, 88.0% (22/25) were MDR, 52.0% (13/25) were CRPR and 12.0% (3/25) were pan-resistant strains. Amikacin was the most active agent (68.0%, 17/25, susceptibility), followed by cefoxitin (52.0%, 13/25) and ertapenem (48.0%, 12/25). Cefuroxime (88.0%, 22/25) and levofloxacin (84.0%, 21/25) showed the highest rates of resistance (Table 2). Notably, two sequential isolates from one patient demonstrated a transition from MDR to CRPR over 11 days.
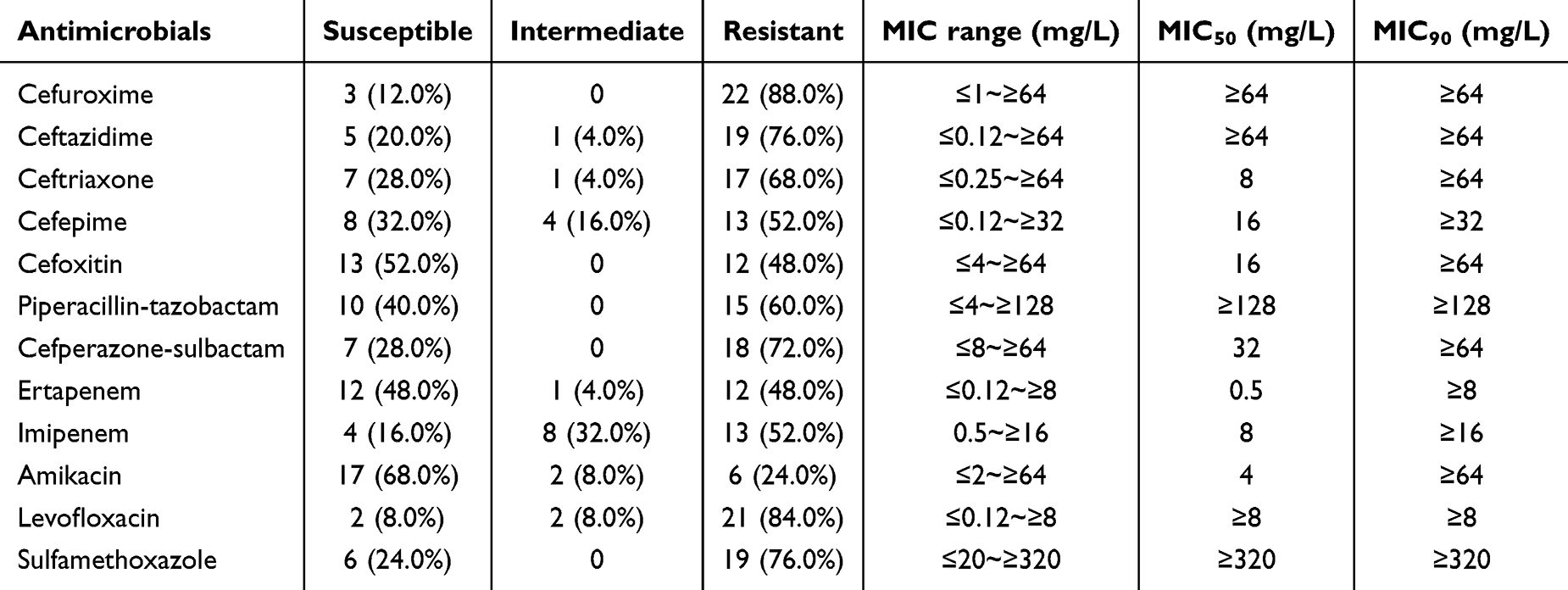 |
Table 2 Antimicrobial susceptibility profiles of 25 P. rettgeri isolates |
Susceptibility to Novel β-Lactam/β-Lactamase Inhibitor Combinations
All 13 CRPR isolates were resistant to CZA (inhibition zones <20 mm), while 61.5% (8/13) CRPR isolates were resistant to ATM. AZA exhibited activity against 61.5% (8/13) of CRPR isolates via both disk diffusion and broth disk elution assay, with a corresponding resistance rate of 38.5% (5/13). Synergy between CZA and ATM was observed in 38.5% (5/13) of CRPR isolates (Table 3, Figure 1).
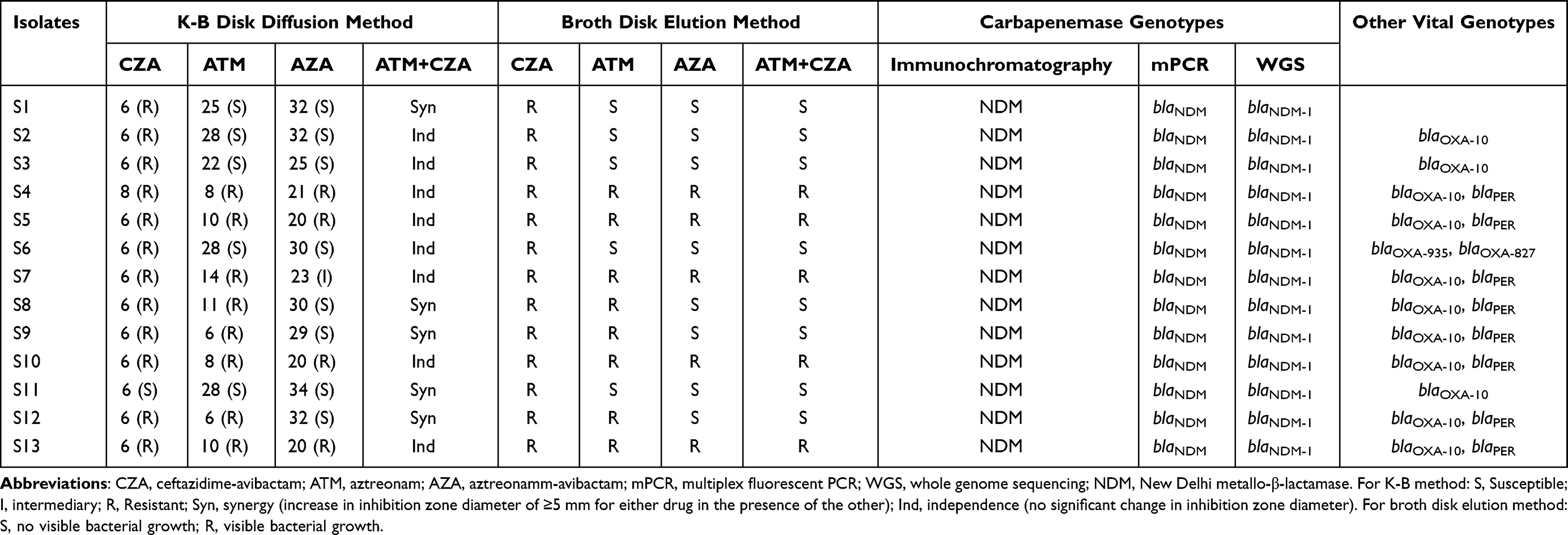 |
Table 3 Susceptibility to ATM, CZA, AZA and carbapenemase genotypes of 13 carbapenem resistant P. rettgeri isolates |
 |
Figure 1 Typical susceptibility testing results of carbapenem resistant P. rettgeri isolates by broth disk elution assay (A1–C1) and disk synergy method (A2–C2). There were five isolates presenting phenotype A, three isolates presenting phenotype B and five isolates presenting phenotype C. Abbreviation: GC, growth control. |
Carbapenemase Genotypes
All CRPR isolates were positive for NDM-type carbapenemase via immunochromatography, while one isolate (S3) was weakly positive for OXA-48 carbapenemase in the initial test, and further confirmed as false positive by mPCR. WGS detected blaNDM-1 (n=5) and blaNDM-23 (n=8) as the predominant carbapenem resistant genes through genome annotation analysis, while after Sanger sequencing validation, all CRPR isolates were positive for blaNDM-1 gene and no occurance of blaNDM-23. Partial blaNDM-1 gene nucleotide sequences of all CRPR isolates were deposited in the GenBank database under the Genbank accession numbers PZ418434 to PZ418446. There were 92.3% (12/13) of CRPR isolates which co-harbored blaOXA-10 gene and its alleles. In addition, the blaPER gene was detected in eight CRPR isolates resistant to ATM (S4, S5, S7, S8, S9, S10, S12, S13) (Table 3, Figure 2).
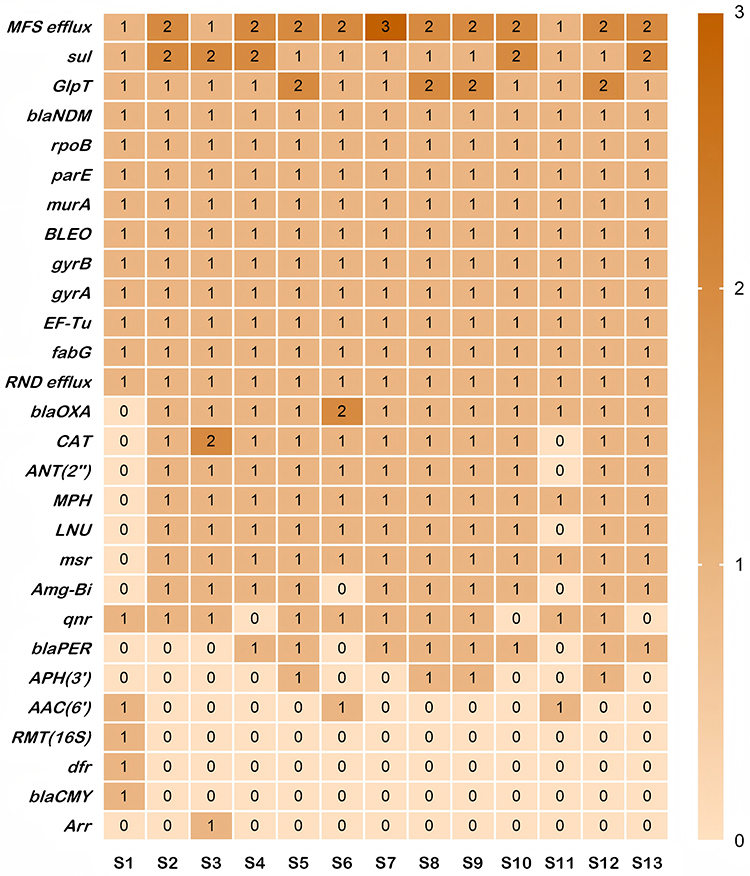 |
Figure 2 Heatmap of antimicrobial resistance (AMR) gene family abundance in 13 carbapenem-resistant P. rettgeri Isolates (S1–S13). The heatmap represents the count of antimicrobial resistance genes per family (scale: 0–3), with color intensity proportional to the number of genes detected. Counts were calculated based on CARD database annotation of WGS assemblies. Notes: β-lactamases resistance: blaNDM, blaOXA, blaPER and blaCMY; Efflux pump: MFS (Major Facilitator Superfamily), RND (Resistance-Nodulation-Cell Division) and msr (msr-type ABC-F protein); Aminoglycoside resistance: ANT(2′′), APH(3′) and AAC(6′); Fluoroquinolone resistance: qnr, gyrA/gyrB and parE; Other resistance genes: sul (sulfonamide), dfr (trimethoprim), CAT (chloramphenicol), Arr (rifampin), MPH (macrolide phosphotransferase), LNU (lincosamide nucleotidyltransferase), GlpT and murA (fosfomycin resistance-related), BLEO (bleomycin), EF-Tu (elfamycin) and fabG (triclosan). |
Discussion
This 5-year retrospective study highlights the high prevalence of MDR and carbapenem resistance in this emerging opportunistic pathogen, P. rettgeri, from a tertiary teaching hospital in northern China. AZA exhibited favorable in vitro activity against CRPR isolates with susceptible rate of 61.5%, while the co-occurrence of blaNDM, blaOXA and blaPER genes in CRPR isolates complicates the resistance mechanisms and underscores the need for enhanced surveillance and infection control measures.
In this study, urine was the most common source of P. rettgeri isolates (44.0%), and the majority of patients with urinary P. rettgeri infections had a history of urinary tract surgery or indwelling urinary catheterization, which is consistent with previous reports linking this pathogen to healthcare-associated UTIs.1 Middle-aged and elderly males were the predominant population of P. rettgeri infection in this study, which may be attributed to the high incidence of the urolithiasis in this demographic, a key risk factor for UTIs that can cause urinary tract mucosal damage and increase the risk of bacterial colonization and infection. For non-urinary P. rettgeri infections, 66.7% (8/12) cases were complicated with co-infections by other Gram negative bacillus (eg, Klebsiella spp. and Pseudomonas aeruginosa) at the same sites, which may be related to the compromised immune function of the infected patients and the complex microecological environment of the infection sites.
The isolation rates of P. rettgeri in our hospital remained stable during the past 5 years, while the resistance rates, especially the CRPR proportion, have been increased slightly in the last two years than the first three years (63.6% (7/11) vs 42.8% (6/14)). The high resistant rate of CRPR isolates in our study is alarming, significantly higher than the carbapenem resistance rate of other Enterobacterales species in our institution which is about 20%. Our findings are comparable to the recent studies in Europe and Mexico, which reported 42.7% and 48.9% rates of CRPR in the clinical, respectively, demonstrating a severe carbapenem resistance situation of P. rettgeri in multi-regions of the world.7,8 Additionally, the observed phenotype transition of P. rettgeri from MDR to CRPR in one patient over 11 days highlights the dynamic evolution of antimicrobial resistance in clinical settings. These findings emphasize the need for rapid AST and genomic surveillance in patients with persistent P. rettgeri infections, as delayed detection of resistance evolution can lead to inappropriate therapy. Although the isolation rate of CRPR was relatively high, the clinical outcomes of the patients involved in this study, particularly mortality rate, were not poor. Since the majority of patients achieved remission even recovery during hospitalization, which might be attributed not only to appropriate antibiotic therapy but also to other medical interventions (eg, urinary catheter removal), given that urine specimens constituted a substantial proportion of the samples collected in this study. In addition, we must acknowledge that there may be individual cases which P. rettgeri colonization was misinterpreted as infections, since non-sterile specimens (such as urine and sputum) accounted high proportion in this study, while drainage fluid samples often co-existed with other bacteria, so the role of P. rettgeri in these cases requires careful analysis.
In this study, all 13 CRPR isolates were resistant to CZA, and 38.5% (5/13) of the isolates were resistant to AZA, which is an unexpected finding since most clinical CPE isolates are susceptible to at least one of the two new agents.9 A discrepancy was observed that different susceptibility results of AZA between disk diffusion (being intermediate) and broth disk elution assay (being resistance) in one CRPR isolate (S7), warranting further investigation into methodological limitations and biological factors (eg, strain heterogeneity). For clinical practice, broth microdilution method may better predict in vitro and in vivo AZA efficacy against heteroresistant P. rettgeri strains. A pattern could be observed in this study that isolates susceptible to ATM were also susceptible to AZA; whereas isolates resistant to ATM could be resistant to AZA partially, with a small subset of isolates remaining susceptible to AZA. These data implied the resistance mechanisms of CRPR isolates are more complex than those of other CPE, which may be related to the co-expression of multiple carbapenemases and other resistance mechanisms (eg, porin deficiency, efflux pump overexpression) which requires further investigation to confirm.19 A previous study reported the development of AZA resistance in Providencia species during AZA monotherapy, with probable mechanism of mutations in penicillin-binding protein 3 (PBP3) gene, a principal β-lactam target, resulting in reduced affinity for agent ATM and subsequently compromised in vitro AZA activity in Providencia isolates.20 In our study, none of the patients received AZA or CZA exposures during hospitalization, suggesting that the resistance of CRPR isolates to these two agents is an acquired trait rather than induced by antimicrobial pressure.
Previous studies have revealed that numerous carbapenemase producing P. rettgeri isolates mainly carry carbapenemases including IMP-, NDM- and VIM-type MBLs, and NDM appears to be the predominant carbapenemase in CRPR reported worldwide since 2013.11,21,22 In this study, the gold immunochromatography assay, mPCR and WGS analysis revealed the presence of blaNDM gene in all CRPR isolates, and Sanger sequencing validated that blaNDM-1 gene was the unique carbapenemase genotype in our isolates. It should be noted that blaNDM-23, which is an allele of blaNDM-1 having the same antimicrobial resistance abilities with single base difference (301A>C) to blaNDM-1,23 sometimes might be falsely annotated by WGS analysis, and Sanger sequencing still keeps the crucial role in drug-resistant genes analysis and validation, especially for some infrequent genotypes. In addition, 92.3% (12/13) of CRPR isolates in this study co-harbored blaNDM-1 and blaOXA-10 genes, a proportion significantly higher than previous reports of single-strain studies.24–26 It is well known that OXA-10 is a class of narrow-spectrum oxacillinase without carbapenemase activity, while a previous study which suggested that OXA-10 combined with low outer-membrane permeability might promote carbapenem resistance in Enterobacterales.27 Here, it remains unknown whether this finding applies to our P. rettgeri isolates and warrants further research. The co-occurrence of blaNDM-1 and blaPER genes in 61.5% of CRPR isolates further complicates the resistance phenotype and severely limits clinical therapeutic options, as blaNDM-1 could confer resistance to CZA, while blaPER encodes extended-spectrum β-lactamases (ESBLs) that confer resistance to third-generation cephalosporins (eg ceftazidime) and aztreonam,28 the vital components of CZA and AZA. This might partly explain the observed CZA, ATM and AZA triple resistance in some CRPR isolates (38.5%, 5/13), while the underlying mechanisms of three isolates harboring blaNDM-1 and blaPER but being susceptible to AZA needs further research. The co-harboring of multiple resistance genes in P. rettgeri isolates poses a significant threat to hospital infection control, as these resistance determinants can be horizontally transmitted to other bacterial strains or species through the transferable plasmids.29,30 Therefore, strict contact isolation measures and active surveillance should be implemented for CRPR isolates carrying both blaNDM-1, blaOXA-10 and blaPER genes to prevent their spread in healthcare settings.
This study has several limitations, such as single-center design, the small sample size due to the low isolation rate of P. rettgeri in clinical specimens, the retrospective design introduced selection bias, and no plasmid sequencing which limited the clear elucidation of resistance gene transmission mechanisms. Additionally, no significant correlation was observed between the cabapenemase genotypes and AZA antimicrobial susceptibility profiles of CRPR, likely due to the additional contribution of other mechanisms (eg PBP3 mutations) to AZA resistance. Future multicenter studies with larger sample sizes and in-depth mechanistic investigations including plasmid sequencing and PBP3 gene mutations detection are needed to validate and advance our study.
Conclusion
P. rettgeri is an emerging pathogen with high rate of carbapenem resistance in clinical practice. The co-existence of blaNDM-1, blaOXA-10 and blaPER genes complicates resistance mechanisms and limits therapeutic options. AZA demonstrated in vitro activity against a large proportion of CRPR isolates and may represent a potential candidate for further clinical validation about its clinical efficacy against CRPR. Further multicenter studies, continuous surveillance, in-depth investigation into its resistance mechanisms including plasmid-level genomic analysis are needed to better understand the epidemiology and resistance mechanisms of this emerging pathogen.
Data Sharing Statement
De-identified datasets supporting the findings of this study are available from the corresponding author Jingrong Cao (Email: [email protected]) upon reasonable request.
Ethical Approval
The research protocol was approved by the Medical Ethics Committee of Xuanwu Hospital, Capital Medical University (XA[KS2024] 039-002). All methods were performed in accordance with the relevant guidelines and regulations. All patient data were de-identified and maintained with strict confidentiality to protect patient privacy, and all procedures were performed in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
We thank Xuanwu Hospital for providing isolates, data, and all study participants. We thank the clinical laboratory staff at Xuanwu Hospital for their assistance with sample collection and testing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Hebei Provincial Department of Science and Technology (244X7703D & XA202401102002K), and Beijing Natural Science Foundation (L256081).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Patel G, Bonomo RA. Providencia spp.: an emerging cause of healthcare-associated infections. Clin Microbiol Rev. 2020;33(4):e00015–11.
2. Abdallah M, Balshi A. First literature review of carbapenem-resistant Providencia. New Microbes New Infect. 2018;25:16–23. doi:10.1016/j.nmni.2018.05.009
3. Wie SH. Clinical significance of Providencia bacteremia or bacteriuria. Korean J Intern Med. 2015;30(2):167–169. doi:10.3904/kjim.2015.30.2.167
4. Sharma D, Sharma P, Soni P. First case report of Providencia rettgeri neonatal sepsis. BMC Res Notes. 2017;10(1):536. doi:10.1186/s13104-017-2866-4
5. Stock I, Wiedemann B. Natural antibiotic susceptibility of Providencia stuartii, P. rettgeri, P. alcalifaciens and P. rustigianii strains. J Med Microbiol. 1998;47(7):629–642. doi:10.1099/00222615-47-7-629
6. Iwata S, Tada T, Hishinuma T, et al. Emergence of carbapenem-resistant Providencia rettgeri and Providencia stuartii producing IMP-type metallo-beta-lactamase in Japan. Antimicrob Agents Chemother. 2020;64(11):e00382–20. doi:10.1128/AAC.00382-20
7. Boattini M, Bianco G, Llorente LI, et al. Enterobacterales carrying chromosomal AmpC beta-lactamases in Europe (EuESCPM): epidemiology and antimicrobial resistance burden from a cohort of 27 hospitals, 2020-2022. Int J Antimicrob Agents. 2024;63(5):107115. doi:10.1016/j.ijantimicag.2024.107115
8. Bocanegra-Ibarias P, Duran-Bedolla J, Silva-Sánchez J, et al. Identification of Providencia spp. clinical isolates co-producing carbapenemases IMP-27, OXA-24, and OXA-58 in Mexico. Diagn Microbiol Infect Dis. 2024;109(1):116246. doi:10.1016/j.diagmicrobio.2024.116246
9. Tamma PD, Aitken SL, Bonomo RA, et al. Infectious Diseases Society of America 2022 guidance on the treatment of extended-spectrumβ-lactamase producing Enterobacterales (ESBL-E), Carbapenem-resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with difficult-to-treat resistance (DTR-P. aeruginosa). Clin Infect Dis. 2022;75:187–212. doi:10.1093/cid/ciac268
10. Wong DW. Practical application of aztreonam-avibactam as a treatment strategy for Ambler class B metallo-beta-lactamase producing Enterobacteriaceae. Antibiotics. 2024;13(8):766. doi:10.3390/antibiotics13080766
11. Saavedra-Rojas SY, Duarte-Valderrama C, González-de-Arias MN, et al. Emergence of Providencia rettgeri NDM-1 in two departments of Colombia, 2012-2013. Enferm Infecc Microbiol Clin. 2017;35(6):354–358. doi:10.1016/j.eimc.2015.05.011
12. Yang W, Chen J, Yang F, et al. Identification of a novel Providencia species showing multi-drug-resistant in three patients with hospital-acquired infection. Int J Antimicrob Agents. 2024;64(2):107211. doi:10.1016/j.ijantimicag.2024.107211
13. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
14. Romina PE, Lucía A, Leticia C, et al. In vitro effectiveness of ceftazidime-avibactam in combination with aztreonam on carbapenemase-producing Enterobacterales. J Glob Antimicrob Resist. 2023;35:62–66. doi:10.1016/j.jgar.2023.08.010
15. Zhang J, Xu J, Shen S, et al. Comparison of three colloidal gold immunoassays and GeneXpert Carba-R for the detection of Klebsiella pneumoniae bla (KPC-2) variants. J Clin Microbiol. 2024;62(7):e0015424. doi:10.1128/jcm.00154-24
16. Chen D, He L, Yang W, et al. Comparative in vitro activity and clinical outcomes of eravacycline, tigecycline, and omadacycline against carbapenem-resistant Acinetobacter baumannii and Klebsiella pneumoniae. Infect Drug Resist. 2026;19:583973. doi:10.2147/IDR.S583973
17. Zheng H, Blechert O, Mei H, et al. Whole-genome resequencing of Trichophyton rubrum provides insights into population differentiation and drug resistance. Mycopathologia. 2020;185(1):103–112. doi:10.1007/s11046-019-00384-1
18. Nordmann P, Poirel L, Carrër A, et al. How to detect NDM-1 producers. J Clin Microbiol. 2011;49(2):718–721. doi:10.1128/JCM.01773-10
19. Farzana R, Jones LS, Rahman MA, et al. Genomic insights into the mechanism of carbapenem resistance dissemination in Enterobacterales from a tertiary public heath setting in south Asia. Clin Infect Dis. 2023;76(1):119–133. doi:10.1093/cid/ciac287
20. Chew KL, Qiao Y, Lye P, et al. Whole-genome analysis of NDM-producing Providencia hangzhouensis associated with recurrent bacteraemia with rapid development of aztreonam-avibactam resistance. Emerg Microbes Infect. 2025;14(1):2539193. doi:10.1080/22221751.2025.2539193
21. Gefen-Halevi S, Hindiyeh MY, Ben-David D, et al. Isolation of genetically unrelated blaNDM-1-positive Providencia rettgeri strains in Israel. J Clin Microbiol. 2013;51(5):1642–1643. doi:10.1128/JCM.00381-13
22. Piza-Buitrago A, Rincón V, Donato J, et al. Genome-based characterization of two Colombian clinical Providencia rettgeri isolates co-harboring NDM-1, VIM-2, and other β-lactamases. Bmc Microbiol. 2020;20(1):345. doi:10.1186/s12866-020-02030-z
23. García-González N, Beamud B, Fuster B, et al. Tracking the emergence and dissemination of a bla (NDM-23) gene in a multidrug resistance plasmid of Klebsiella pneumoniae. Microbiol Spectr. 2023;11(2):e0258522. doi:10.1128/spectrum.02585-22
24. Shen S, Huang X, Shi Q, et al. Occurrence of NDM-1, VIM-1, and OXA-10 co-producing Providencia rettgeri clinical isolate in China. Front Cell Infect Microbiol. 2022;11:789646. doi:10.3389/fcimb.2021.789646
25. Li Y, Shao K, Cai R, et al. Detection of NDM-1 and OXA-10 co-producing Providencia rettgeri clinical isolate. Infect Drug Resist. 2023;16:5319–5328. doi:10.2147/IDR.S418131
26. Peng J, Xia Z, Zhang T, et al. Identification of tmexC3-tmexD3-toprJ1b in an XDR Providencia rettgeri clinical isolate co-producing NDM-1 and OXA-10 carbapenemases. J Glob Antimicrob Resist. 2023;34:229–233. doi:10.1016/j.jgar.2023.07.018
27. Alonso-García I, Vázquez-Ucha JC, Martínez-Guitián M, et al. Interplay between OXA-10 beta-lactamase production and low outer-membrane permeability in carbapenem resistance in Enterobacterales. Antibiotics. 2023;12(6):999. doi:10.3390/antibiotics12060999
28. Jiang X, Yin Z, Yuan M, et al. Plasmids of novel incompatibility group IncpRBL16 from Pseudomonas species. J Antimicrob Chemother. 2020;75(8):2093–2100. doi:10.1093/jac/dkaa143
29. Elbehiry A, Marzouk E, Abalkhail A. Molecular insights into carbapenem resistance in Klebsiella pneumoniae: from mobile genetic elements to precision diagnostics and infection control. Int J Mol Sci. 2026;27(3):1229. doi:10.3390/ijms27031229
30. Li Y, Zhang H, Wang X, et al. Epidemiological trends of carbapenem-resistant Providencia rettgeri in China, 2015-2022. Antimicrob Resist Infect Control. 2023;12(1):98. doi:10.1186/s13756-023-01300-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Hospital-Based Surveillance of Klebsiella pneumoniae and Other Klebsiella species in Southern Saudi Arabia (2012–2024): Escalating Carbapenem and DTR Resistance with Species-Specific Phenotypes and Genotypes
Shabi Y, Algarni AM, Binkhamis K, Al Bshabshe A, Alazraqi T, Abdullah Mohammed S, Habbash S, Alqahtani AJ, Basheer NA, Alhazmi AH, Patriquin G, Bawazeer AO, Tahtouh EI
Infection and Drug Resistance 2026, 19:554543
Published Date: 4 February 2026