Back to Journals » Infection and Drug Resistance » Volume 19
Clinical Characteristics and Risk Factors for Mortality in Candidemia: A Retrospective Single-Center Study in China
Authors Zhou S, Zhang X, Yuan K ![]() , Ling Y
, Ling Y ![]() , Zhang J, Tian B, Zhang X
, Zhang J, Tian B, Zhang X
Received 6 April 2026
Accepted for publication 24 June 2026
Published 30 June 2026 Volume 2026:19 614406
DOI https://doi.org/10.2147/IDR.S614406
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Sihai Zhou1,*, Xin Zhang2,*, Kaixuan Yuan3,*, Yong Ling3, Jiahuan Zhang3, Benshun Tian3, Xiao Zhang1
1Department of Clinical Laboratory, Suzhou Ninth People’s Hospital Affiliated to Soochow University, Suzhou, Jiangsu, 215200, People’s Republic of China; 2Department of Hepatobiliary Surgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China; 3Department of Clinical Laboratory Medicine, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences) Southern Medical University, Guangzhou, Guangdong, 510080, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Benshun Tian, Department of Clinical Laboratory Medicine, Guangdong Provincial People’s Hospital, (Guangdong Academy of Medical Sciences), Southern Medical University, No. 106 Zhongshan 2nd Road, Yuexiu District, Guangzhou, Guangdong, 510080, People’s Republic of China, Tel/Fax +86 19552153915, Email [email protected]; Xiao Zhang, Department of Clinical Laboratory, Suzhou Ninth People’s Hospital Affiliated to Soochow University, No. 2666 Ludang Road, Taihu New Town, Wujiang District, Suzhou, Jiangsu, 215200, People’s Republic of China, Tel/Fax +86 13812711163, Email [email protected]
Purpose: Candidemia is a major cause of hospital-acquired bloodstream infections and is associated with high mortality. This study evaluated clinical characteristics, pathogen distribution, antifungal susceptibility, and factors associated with 28-day outcome in patients with candidemia.
Methods: We retrospectively analyzed 169 patients with confirmed candidemia at Guangdong Provincial People’s Hospital from January 2021 to December 2023. Patients were classified as survivors (n = 81) or non-survivors (n = 88) according to 28-day outcome. Species distribution, time to positivity (TTP), antifungal susceptibility, clinical features, and prognostic factors were compared. Variables significant in univariate analysis were entered into a multivariable logistic regression model.
Results: Most patients were admitted to the intensive care unit (70.41%), and the 28-day mortality rate was 52.07%. The main causative species were Candida albicans (38.46%), Candida parapsilosis (27.22%), Candida glabrata (15.98%), and Candida tropicalis (15.98%). TTP differed significantly among species; C. tropicalis showed the shortest median TTP (18.73 h), whereas C. parapsilosis and C. glabrata showed longer TTPs (38.34 h and 37.15 h, respectively; P < 0.0001). C. tropicalis showed high resistance rates to fluconazole and voriconazole, at 33.33% and 37.04%, respectively. Univariate analysis showed that age, coronary heart disease, respiratory disease, concomitant bacterial bloodstream infections, septic shock, APACHE II score, catheter insertion, mechanical ventilation, glucocorticoid use, antifungal treatment within 48 h, and antifungal therapy duration ≥ 14 days were associated with 28-day mortality. Multivariate logistic regression further demonstrated that only antifungal therapy lasting ≥ 14 days emerged as an independent risk factor for 28-day mortality.
Conclusion: Candidemia entails severe infection and poor prognosis, with C. albicans predominating. Clinicians should maintain vigilant monitoring and interventions targeting identified risks while tracking evolving resistance patterns.
Keywords: Candidemia, Candida albicans, mortality risk factors, epidemiology, in vitro antifungal susceptibility
Introduction
The widespread use of broad-spectrum antimicrobials, corticosteroids, immunosuppressants, cancer therapies, invasive catheterization, and organ transplantation has substantially increased the immunocompromised population at risk for fungal infections.1,2 Invasive candidiasis (IC) is increasingly prevalent worldwide, representing a significant threat to patient health. Candidemia, the most common manifestation of IC, ranks as the fourth most frequent hospital-acquired bloodstream infection.3 It frequently results in a prolonged hospitalization and poor clinical outcomes, with mortality rates reaching 35% to 70%.4–7 The increase in mortality may be associated with the rise in non-Candida albicans Candida (NCAC) infections.5,8 Current diagnostic challenges for candidemia include non-specific clinical manifestations and the suboptimal performance of blood cultures characterized by low sensitivity and prolonged turnaround times. Compounding these issues, certain Candida species exhibit escalating resistance rates and demonstrate healthcare-associated transmission.6 Notably, the rising prevalence of azole-resistant C. tropicalis strains with significant cross-resistance further complicates both early diagnosis and effective antifungal intervention.7,9–11 Moreover, the species distribution and drug susceptibility profiles of Candida vary by geographic region and over time.12,13
Given these challenges, it is imperative to investigate the species distribution, in vitro antifungal susceptibility profiles, clinical characteristics of candidemia patients, and particularly mortality risk factors. Such insights will provide critical evidence for early targeted therapy and optimized clinical interventions. Accordingly, this single-center retrospective study analyzed clinical data from patients with candidemia at our institution between January 2021 and December 2023. We systematically examined the demographic and clinical characteristics, pathogen distribution patterns, in vitro antifungal susceptibility results, and prognostic determinants. This comprehensive analysis aims to establish evidence-based guidance for improving candidemia management through early diagnosis and precision treatment.
Materials and Methods
Study Population
This study population included 169 patients diagnosed with candidemia at Guangdong Provincial People’s Hospital between January 2021 and December 2023. All patients met the diagnostic criteria for candidemia as outlined in the 2016 IDSA Clinical Practice Guidelines for the Management of Candidiasis. Inclusion criteria were as follows: i) at least one positive blood culture for Candida, with the first positive culture used for patients with multiple positive cultures; ii) exclusion of bacteremia alone, filamentous fungemia, cryptococcal fungemia, missing records of time to positivity (TTP), and duplicated strains; iii) availability of complete clinical data, including symptoms, signs, auxiliary diagnostic results, laboratory tests, and medical records.
Data Collection
Data collected included clinical characteristics, risk factors, in vitro antifungal susceptibility (AFST) results, treatment methods, and prognosis. Based on the 28-day prognosis following the first positive blood culture, patients were categorized into survival and non-survival groups. TTP was defined as the time interval from the start of blood culture incubation to the automated positive signal indicating organism growth. If both aerobic and anaerobic bottles were positive, the shorter TTP was used for analysis. If a patient had persistent candidemia with multiple positive blood cultures, only the TTP of the first positive blood culture episode was recorded. APACHE II scores were assessed at admission date; (1,3)-β-D-glucan (BDG) levels were measured at blood culture date.
Candida Isolation and Identification
Bilateral venous blood was collected aseptically using the BD BACTEC™ Plus Aerobic/F Culture Vials (Becton Dickinson, USA). After inoculation, the blood culture bottles were placed in the BD BACTECTM FX system (Becton Dickinson, USA) for incubation and automatic detection of positivity. Gram staining was performed on positive culture vials. If yeast-like fungi were observed, the cultures were inoculated onto Sabouraud Agar (SDA) and CHROM agar and incubated at 35 °C for 24–48 hours. Species identification was conducted using the VITEK MS (IVD 3.2) mass spectrometer (bioMérieux, France). AFST was performed using the ATB FUNGUS 3 kit (bioMérieux, France), strictly adhering to the manufacturer’s instructions.
Antifungal Susceptibility Testing
AFST of Candida spp. to antifungal antibiotics were performed on ATB Fungus 3 kit, strictly adhering to the manufacturer’s instructions: i) pick a single isolated colony and suspend it in 0.9% sterile saline to match the 2.0 McFarland standard; ii) add 20 µL to each lyophilized ampoule and vortex well; iii) add 135 µL to each microtiter well. Incubate the plate aerobically at 35 °C ± 2 °C in a humidified incubator for 24 ± 2 hours. Use C. parapsilosis ATCC 22019 as the quality control strain. Minimum inhibitory concentrations (MICs) for all antifungal drugs were recorded after 24 hours of incubation. AFST results were interpreted according to CLSI M59 and CLSI M60 standards.14,15 Based on the recommended clinical breakpoints (CBPs), results were classified as susceptible (S), intermediate (I), susceptible-dose dependent (SDD), or resistant (R). Epidemiological cutoff values (ECVs) were also applied: isolates with MICs ≤ ECVs were classified as wild-type (WT), and those with MICs > ECVs were classified as non-wild-type (NWT). Due to the lack of recommended CBPs and ECVs for 5-fluocytosine, its susceptibility results were not analyzed in this study.
Statistical Analysis
Statistical analysis was performed using SPSS 23.0 software. Normally distributed continuous variables were expressed as mean ± standard deviation and compared using independent samples t-tests. Non-normally distributed variables were expressed as median and interquartile range [M (P25, P75)] and compared using the Mann–Whitney U-test. Categorical variables were expressed as percentages (%) and compared using the chi-square (χ2) test. Variables with statistical significance in univariate analysis were included in a multivariate logistic regression model to calculate odds ratios (OR) and 95% confidence intervals (CI). A P-value < 0.05 was considered statistically significant. Variables with collinearity or clinical overlap were excluded from the multivariable model after model diagnostics.
Results
Pathogen Detection and Related Findings
Among 169 Candida isolates, C. albicans accounted for 38.46% (65/169) while NCAC species represented 61.54% (104/169), demonstrating a statistically significant predominance of NCAC (χ2 = 17.09, P < 0.0001). NCAC distribution comprised: C. parapsilosis (27.22%, 46/169), C. glabrata (15.98%, 27/169), C. tropicalis (15.98%, 27/169), and other species (2.37%, 4/169) (Figure 1A). Most patients originated from intensive care units (70.41%, 119/169), with surgical wards contributing 17.75% (30/169) (Figure 1B). Temporal analysis revealed a significant epidemiological shift: The isolation rate of C. parapsilosis increased progressively from 18.18% (12/66) in 2021 to 28.26% (13/46) in 2022 and further to 36.84% (21/57) in 2023, whereas that of C. albicans declined from 48.48% (32/66) in 2021 to 32.61% (15/46) in 2022 and subsequently to 31.58% (18/57) in 2023. (Figure 1C). The median TTP for all isolates was 31.08 hours (IQR 23.23–45.63), with only 26.03% (44/169) yielding TTPs < 24 hours. Significant interspecies variation was observed (Kruskal–Wallis Z = 35.90, P < 0.0001): C. tropicalis demonstrated the shortest TTP (18.73 hours, IQR 14.70–26.22), followed by C. albicans (28.70 hours, IQR 23.23–47.12), while C. parapsilosis (38.34 hours, IQR 30.04–46.45) and C. glabrata (37.15 hours, IQR 25.65–62.27) exhibited the longest TTP (Figures 1D). Figure 2 shows that C. glabrata and C. tropicalis showed the highest mortality rates, both at 66.67%. C. albicans showed an intermediate mortality rate of 52.31%, whereas C. parapsilosis had the lowest mortality rate, at 36.96% (P < 0.05). This gradient distribution reveals distinct pathogenic differences among strains, notably with C. glabrata and C. tropicalis showing nearly 30 percentage points higher mortality than C. parapsilosis. These findings provide key insights for clinical precision medicine, underscoring an urgent need to strengthen rapid identification of high-risk strains and develop differentiated treatment strategies.
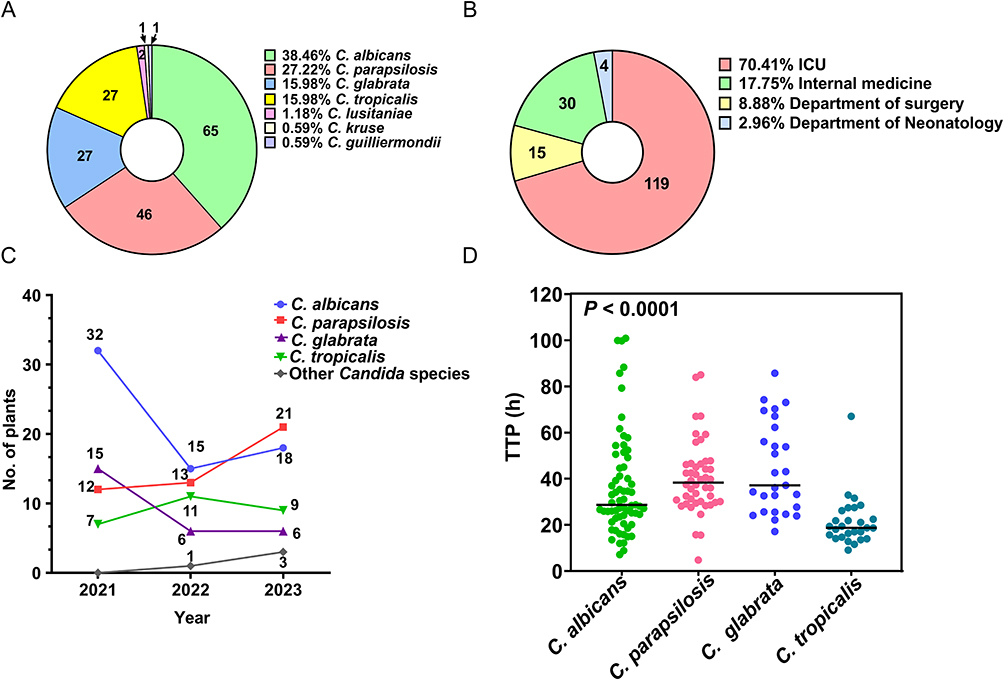 |
Figure 1 Etiological distribution and clinical characteristics of candidemia. (A) Species distribution of Candida isolates (n = 169); (B) distribution across hospital wards; (C) temporal trends in species distribution from 2021 to 2023; (D) comparison of time to positivity among predominant Candida species (P < 0.0001). |
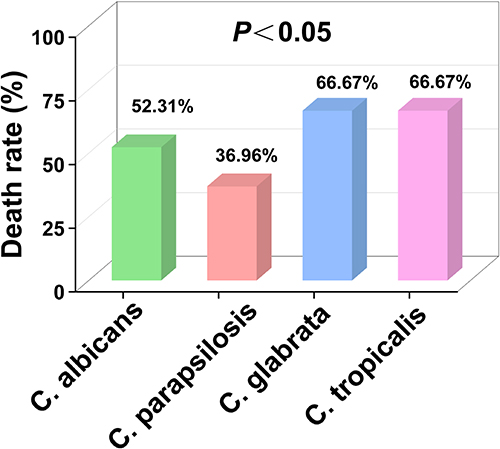 |
Figure 2 Mortality rates among patients infected with different Candida species. |
Morphological Characteristics of Candida Species on Blood Smears and CHROM Agar
All four Candida species exhibited yeast-like blastoconidia with predominantly oval-to-spherical morphology on smears prepared from positive blood culture vials (Figure 3A–D). Distinctive morphological features were observed: C. parapsilosis demonstrated elongated oval blastoconidia (Figure 3C), while C. glabrata displayed significantly smaller cellular dimensions compared to other species (mean diameter 2.1 ± 0.3 μm vs 4.5 ± 0.6 μm in C. albicans, P < 0.001) (Figure 3D). After 24 hours of incubation at 37 °C on CHROM agar, chromogenic differentiation yielded species-specific colony pigmentation: C. albicans formed emerald green colonies; C. tropicalis produced slate-gray colonies with a metallic sheen; C. parapsilosis developed pale pink colonies exhibiting smooth margins; and C. glabrata displayed central purple pigmentation surrounded by a white periphery (representative microscopic and macroscopic appearances are shown in Figure 3E–H, respectively).
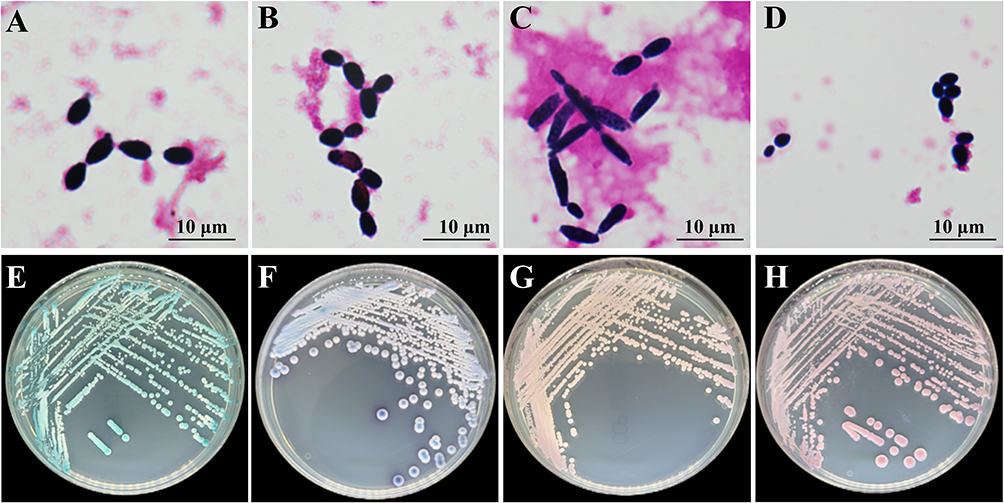 |
Figure 3 Morphological and chromogenic characteristics of predominant Candida species. (A–D) Gram-stained blood culture smears (×1000): (A) C. albicans; (B) C. tropicalis; (C) C. parapsilosis; (D) C. glabrata. (E–H) CHROMagar Candida colonies (37 °C, 24 h): (E) C. albicans (emerald green); (F) C. tropicalis (slate-gray); (G) C. parapsilosis (pale pink); (H) C. glabrata (purple center, white periphery). |
AFST Results for Four Common Candida Species
C. albicans exhibited low resistance rates to fluconazole (4.62%; 3/65) and voriconazole (4.62%; 3/65). Similarly, C. parapsilosis showed low resistance to voriconazole (4.35%; 2/46) and fluconazole (8.70%; 4/46), along with a low NWT rate to itraconazole (4.35%; 2/46). In contrast, C. tropicalis demonstrated high resistance rates to both fluconazole (33.33%; 9/27) and voriconazole (37.04%; 10/27), with an MIC90 of 128 μg/mL and a geometric mean (GM) of 34.48 μg/mL for fluconazole. C. tropicalis also exhibited a high NWT rate to itraconazole (33.33%; 9/27). While C. glabrata had a higher resistance rate to voriconazole (18.52%; 5/27), no resistance or NWT isolates were observed for fluconazole or itraconazole. No NWT strains of amphotericin B were detected. Overall, C. albicans, C. tropicalis, and C. parapsilosis displayed varying degrees of resistance to fluconazole and voriconazole (Table 1).
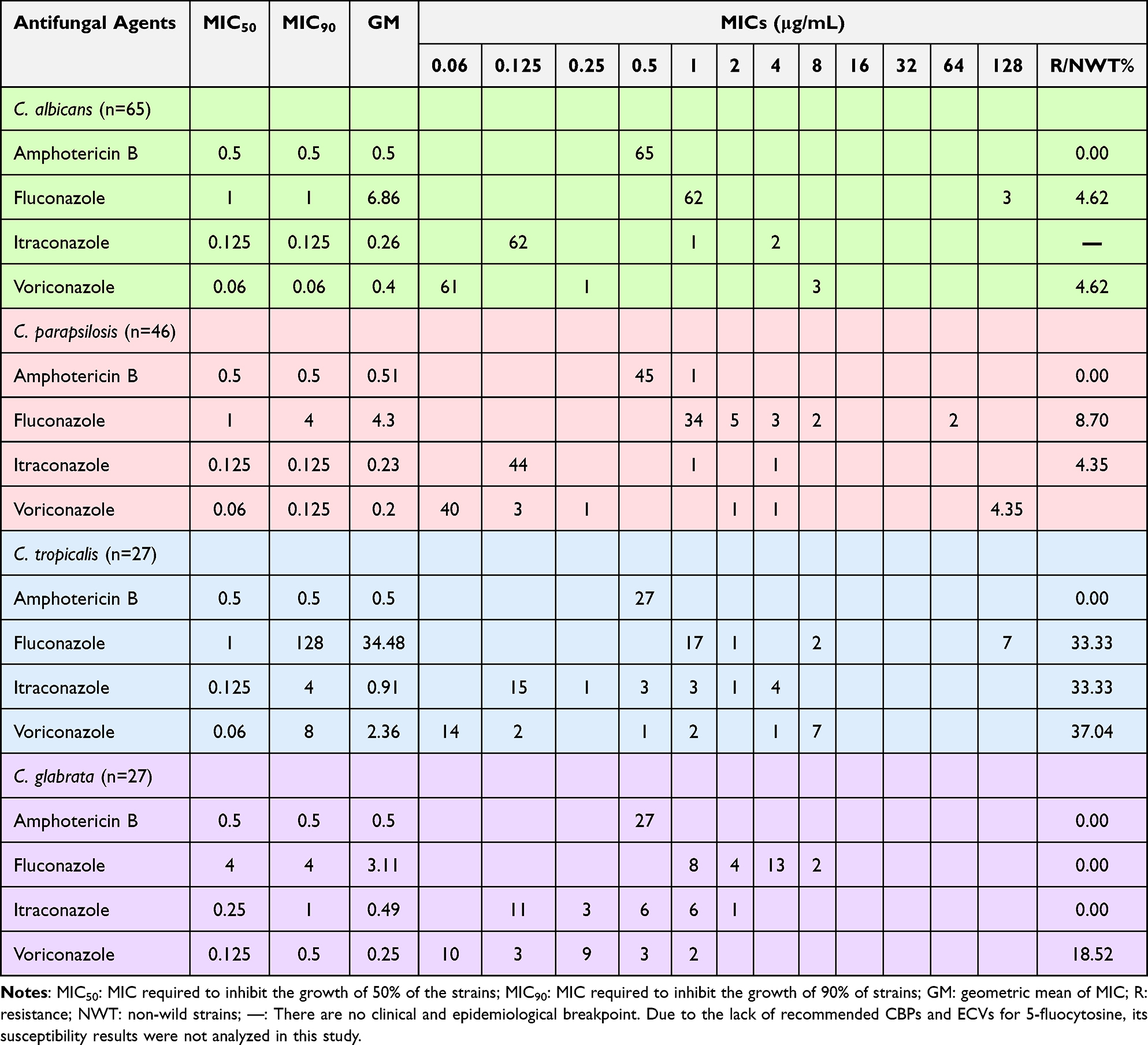 |
Table 1 In vitro Antifungal Susceptibility Testing Results of Four Prevalent Candida Species Isolated from Bloodstream Samples [N] |
Clinical Characteristics of Candidemia Patients
The cohort comprised 169 patients (111 males, 65.68%; 58 females, 34.32%) with a mean age of 65.13 ± 20.35 years. Most patients had invasive devices: indwelling urinary catheters (124/169, 73.37%), catheter insertion (111/169, 65.68%), and mechanical ventilation (135/169, 79.88%). Based on 28-day mortality following initial blood culture positivity, patients were stratified into survival (n=81) and non-survival (n=88) groups, yielding a 28-day mortality rate of 52.07% (88/169).
Univariate analysis showed that age, coronary heart disease, respiratory disease, bacterial bloodstream infections (BSIs), septic shock, APACHE II score, catheter insertion, mechanical ventilation, glucocorticoid use, antifungal treatment within 48 h, and duration of antifungal therapy (≥ 14 days) were factors associated with 28-day outcome in patients with candidemia (P < 0.05) (Table 2).
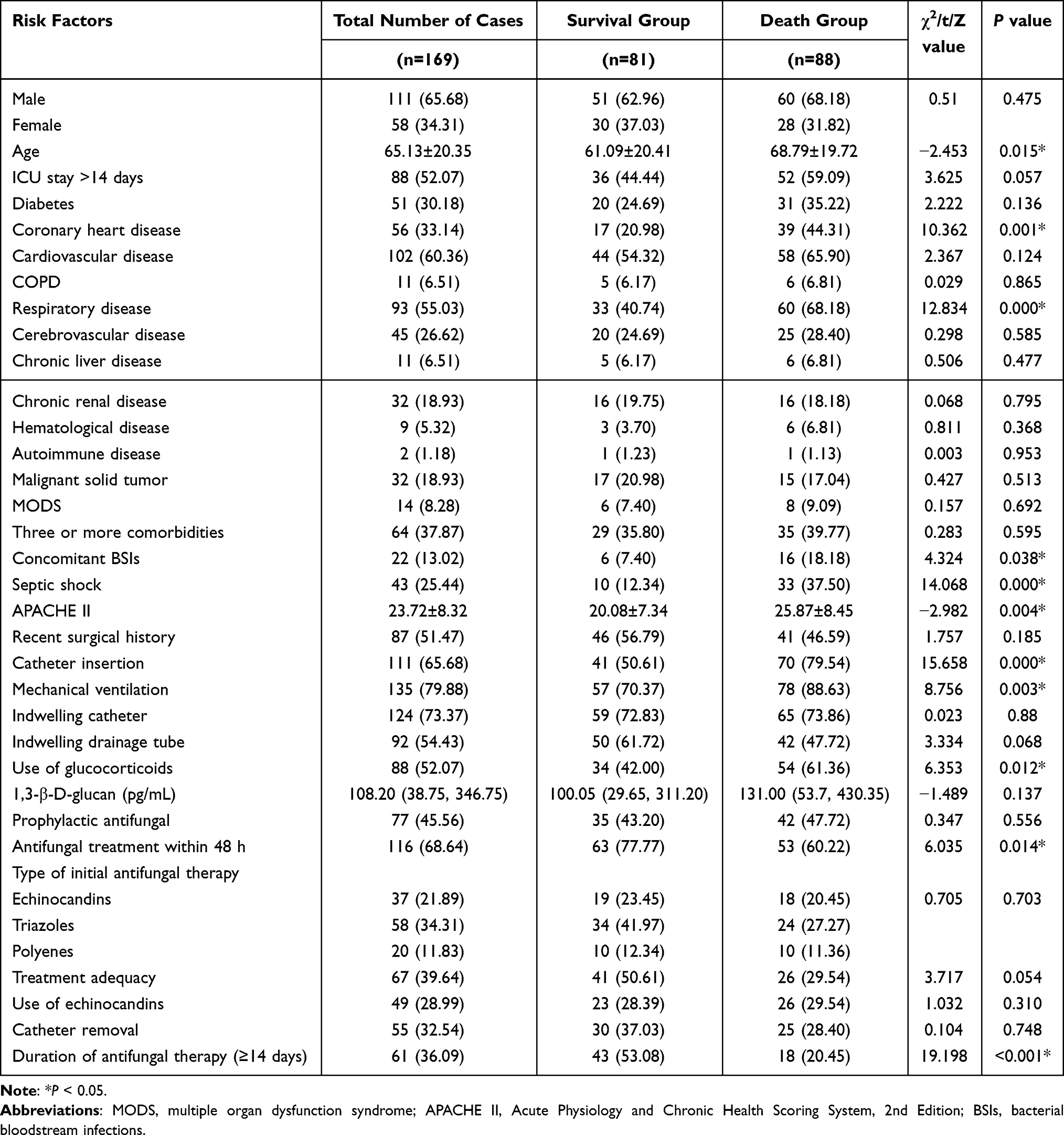 |
Table 2 Univariate Analysis of Prognostic Factors for Candidemia [n(%)] |
Multivariable Logistic Regression Analysis of 28-Day Mortality
Multivariate logistic regression analysis indicated that the duration of antifungal therapy (≥ 14 days) was a statistically significant independent risk factor for the outcome (OR = 6.875; 95% CI: 2.194–21.549; P = 0.001). In contrast, APACHE II score, presence of coronary heart disease, catheter insertion, and glucocorticoid, age, underlying respiratory disease, BSIs, and initiation of antifungal therapy within 48 hours showed no statistically significant association with the study outcome (all P > 0.05) (Table 3).
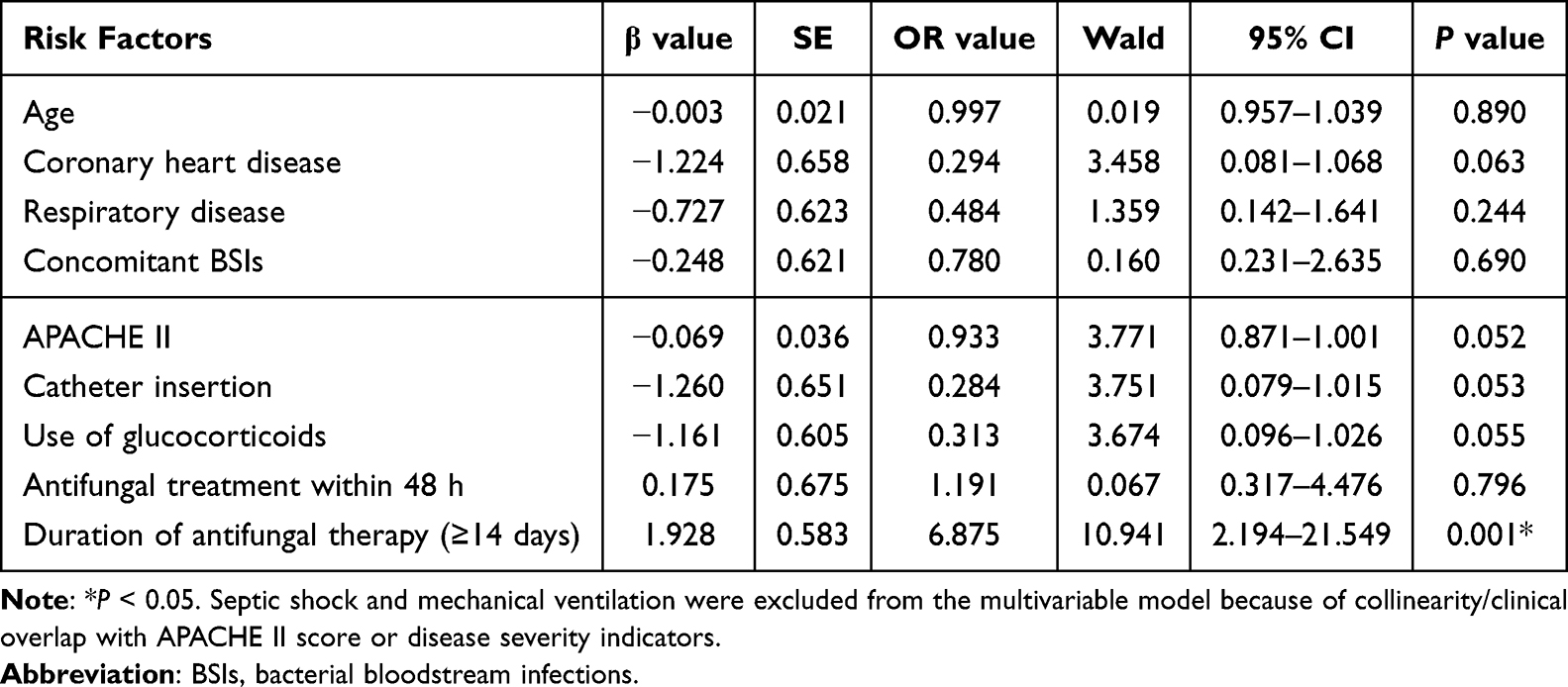 |
Table 3 Multivariate Logistic Regression Model Analysis of Prognostic Risk Factors in Patients with Candidemia |
Discussion
Candidemia is a bloodstream infection caused by Candida spp. In recent years, the incidence and mortality of candidemia have been increasing year by year, and it has become a serious public health problem worldwide.5,16 At the same time, the composition of candidemia species is also changing. C. albicans remains the leading species, whereas NCAC species are increasing.17 In this study, it was found that the causative agent of candidemia in our hospital was still represented by C. albicans (38.46%), C. parapsilosis (27.22%), C. glabrata (15.98%), and C. tropicalis (15.98%). This distribution is generally consistent with recent Chinese multicenter surveillance data, in which C. albicans remains the most common species (approximately 33.8%–46.0%), while C. parapsilosis (15.6%-22.0%), C. tropicalis (17.6%-21.5%), and C. glabrata (11.2%-14.8%) are the predominant NCAC species.18 We found that C. parapsilosis rose from 18.18% to 28.26% to 36.84% over the same period. The rising incidence of C. parapsilosis infections warrants focused clinical and microbiological attention, given its growing epidemiological prominence and documented association with the emergence and dissemination of azole-resistant isolates. In recent years, C. parapsilosis has emerged as a leading cause of candidemia in multiple geographic regions, with several outbreaks linked to clonal expansion of fluconazole-resistant strains.2,13
Blood culture is still the gold standard for the diagnosis of candidemia, but it has been reported that blood culture has low sensitivity, a long TTP, with a reported median of 48 h, and species differences.19 This study found that C. tropicalis had the shortest median TTP (18.73 h), followed by C. albicans (28.70 h), while C. parapsilosis (38.34 h) and C. glabrata (37.15 h) showed the longest TTP, which is consistent with relevant reports.20 In their report, TTPs of C. tropicalis and C. glabrata were 21.26 ± 3.20 h and 66.84 ± 30.87 h, respectively. A Korean single-center study also observed that C. tropicalis isolates were associated with shorter TTPs compared with other common Candida species.11 Current studies have clarified that TTPs variation is predominantly determined by the intrinsic growth rate of different Candida species, rather than the initial fungal load in peripheral blood.11 This characteristic endows TTPs with important practical value in clinical practice. Before formal species identification results are available, clinicians may preliminarily infer the probable pathogen based on TTPs: a TTP shorter than 24 hours may suggest C. tropicalis. Therefore, TTPs may aid in the initial clinical characterization of fungal isolates prior to definitive species identification. In addition, mortality varied markedly by Candida species: C. glabrata and C. tropicalis had the highest mortality at 66.67%, followed by C. albicans (52.31%), and C. parapsilosis had the lowest rate at 36.96%. Clinicians should prioritize intensive monitoring for patients suspected of being infected with these two high-risk strains according to TTPs.
Following the acquisition of identification and AFST results, therapeutic regimens should be adjusted based on susceptibility profiles and resistance patterns. This study found no NWT isolates of amphotericin B were detected. However, C. albicans, C. tropicalis, and C. parapsilosis exhibited varying degrees of resistance to fluconazole and voriconazole. Notably, C. tropicalis demonstrated resistance rates of 33.33% to fluconazole and 37.04% to voriconazole, consistent with relevant reports.4 Globally, C. tropicalis has exhibited prominent azole resistance, with its fluconazole resistance rate reported at 30%–35% and voriconazole resistance rate at 35%-40%.5,6 This trend is particularly concerning: azoles remain the cornerstone of first-line antifungal therapy, and increasing azole resistance in Candida spp. not only undermines the efficacy of empirical treatment but is also independently associated with higher rates of treatment failure and adverse clinical outcomes. Therefore, it is necessary to actively send blood cultures for clinical testing, and laboratories should carry out in vitro antifungal susceptibility tests to grasp the changes in drug susceptibility of Candida. Clinically, for patients with extremely short TTPs suggestive of C. tropicalis, echinocandins are recommended as initial antifungal therapy in settings with prevalent azole resistance to mitigate the risk of treatment failure.
The overall 28-day mortality rate of 52.07% in our cohort falls within the global mortality range of 35%-70% for candidemia.5 We found that age, coronary heart disease, respiratory disease, bacterial bloodstream infections, septic shock, APACHE II score, catheter insertion, mechanical ventilation, glucocorticoid use, antifungal treatment within 48 h, and duration of antifungal therapy (≥ 14 days) were the variables associated with non-survival in univariate analysis at 28 days, which were slightly different from those reported in related studies, mainly in the association of age and chronic cardiopulmonary diseases with mortality.1,7,21 These discrepancies may be related to the differences in medical environment and level in different regions.
At present, it is believed that the main causes of candidemia are low immunity and damaged mucosal barrier, and most of the patients (70.41%) are distributed in ICU, and such patients have a long hospital stay, often with urinary catheters (73.37%), central venous catheters (65.68%), mechanical ventilation (79.88%), and glucocorticoids (52%), etc., which make it difficult for the patients’ digestive tract to be used normally, and the physiological barrier is destroyed. Candida and bacteria colonizing the body surface and environment are prone to invasion of the bloodstream, often complicated by respiratory diseases and septic shock, resulting in a high mortality rate (52.07%), which is similar to that reported in the literature.19 The APACHE II scoring system is widely used in the ICU, and its score is proportional to the patient’s prognosis. In this study, we found that the APACHE II score in the dead group was higher than that in the survival group (25.87 ± 7.57 vs 20.08 ± 7.18), indicating that the patients in the death group were more severely ill and had a worse prognosis. As documented in the relevant report, the APACHE II score strongly predicts ICU mortality, with higher scores in deceased than in surviving patients.1,2 Additionally, univariate analysis identified antifungal treatment within 48 hours as a notable prognostic factor: patients who received timely antifungal intervention within 48 hours after the first positive blood culture achieved a higher survival rate. This finding is consistent with multiple previous studies, which also confirmed that early antifungal intervention within 48 hours was significantly associated with improved survival outcomes in patients with Candida bloodstream infections.1,9,18 Delayed initiation of antifungal therapy may exacerbate fungal dissemination, amplify systemic inflammatory responses, and further deteriorate organ function, ultimately increasing the risk of death.2,11
Nonetheless, our study confirmed that survivors were more likely than non-survivors to receive antifungal therapy for ≥14 days (53.08% vs. 20.45%), largely because patients who died early were unable to complete a full treatment course. Accordingly, long-course antifungal therapy was identified as an independent risk factor for 28-day mortality in the regression model, rather than a protective factor. In the multivariable model, duration of antifungal therapy ≥14 days was independently associated with higher 28-day mortality. This finding is largely explained by the fact that patients who died early could not complete a full course of antifungal treatment. Clinicians should determine treatment duration dynamically according to disease severity, microbiological clearance, source control, and clinical response. Recent research also indicates that the standard 14-day regimen is primarily indicated for complicated candidemia, while shortened treatment courses may be applicable to patients with uncomplicated cases.21,22 A 16-year retrospective study conducted in Argentina further verified that severe illness and complicated clinical conditions are strongly linked to unfavorable prognosis in candidemia patients.19 Thus, clinicians should assess severity and response dynamically and tailor therapy to avoid unnecessary prolongation.
In summary, the patients with candidemia in our hospital are mainly intensive care patients, who are seriously ill and have a poor prognosis. C. albicans remains the predominant pathogen in candidemia, while C. parapsilosis isolation rates showed an increasing trend over the study period. Bloodstream infections caused by Candida species exhibit species-specific differences in TTPs, which may provide early supportive information while awaiting definitive identification. Moreover, a substantial proportion of these isolates demonstrate reduced susceptibility, or outright resistance, to fluconazole and voriconazole. Clinical monitoring and intervention should be focused on risk factors, and changes in drug resistance of Candida should be grasped in a timely manner to improve the prognosis of patients and reduce mortality.
This study has several limitations. First, its retrospective design at a single center limits generalizability. Second, incomplete records may introduce bias, and the modest sample size reduces statistical power. Third, AFST used the ATB Fungus 3 kit rather than the gold standard broth microdilution method, which may result in lower accuracy for certain fungi and azoles, with variable reproducibility across different species and drug combinations.
Conclusions
Our study highlights shifting Candida epidemiology dominated by NCAC species and rising azole resistance. Concomitant BSIs and glucocorticoid exposure were associated with outcome in univariate analysis, demanding intensified surveillance in critical care settings. TTP may provide valuable preliminary information for early species prediction while awaiting definitive identification, supporting antifungal stewardship in this higher-risk cohort. Clinicians should prioritize early detection of co-infections, judicious corticosteroid use, and tailored antifungal therapy guided by local resistance patterns to improve outcomes. Special attention should be paid to patients requiring prolonged antifungal treatment, as this factor was linked to poor 28-day outcomes.
Ethical Statement
This study received ethical approval from the Ethics Committee of Guangdong Provincial People’s Hospital (KY2025-106-01) and Suzhou Ninth People’s Hospital Affiliated to Soochow University (KYLW2025-025-01) in accordance with the Declaration of Helsinki. Due to the retrospective nature of this study, the requirement for written informed consent was waived by the ethics committees while maintaining strict confidentiality of patient data.
Acknowledgments
We extend our gratitude to all involved colleagues from the Clinical Microbiology Laboratory, Department of Laboratory Medicine, Guangdong Provincial People’s Hospital, for their support to this project.
Funding
The current study was funded by Research on a new technology for the combined detection of three small molecules of Suzhou Ninth People’s Hospital Affiliated to Soochow University (No. YK202534), the National Natural Science Foundation of China (82402505), and Research on the Direct Identification of Blood Culture Positive Samples from Patients with Bloodstream Infections and the Rapid Detection of Carbapenem Resistance (WWK202508).
Disclosure
The authors declare no conflict of interest in this work.
References
1. Chen X, Yang Y, Li Y, et al. Clinical characteristics and risk factors for death in patients with Candida bloodstream infection in Intensive Care Unit. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2021;46(7):719–11. doi:10.11817/j.issn.1672-7347.2021.201012
2. A CO, Sprute R, Bassetti M, et al. Global guideline for the diagnosis and management of candidiasis: an initiative of the ECMM in cooperation with ISHAM and ASM. Lancet Infect Dis. 2025;25(5):e280–e293. doi:10.1016/S1473-3099(24)00749-7
3. Wisplinghoff H, Bischoff T, M TS, et al. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis. 2004;39(3):309–317. doi:10.1086/421946
4. W DD. Global incidence and mortality of severe fungal disease - Author’s reply. Lancet Infect Dis. 2024;24(5):e269. doi:10.1016/S1473-3099(24)00103-8
5. Fan X, C DR, Zhang S, et al. Tandem gene duplications contributed to high-level azole resistance in a rapidly expanding Candida tropicalis population. Nat Commun. 2023;14(1):8369. doi:10.1038/s41467-023-43380-2
6. C FM, Alastruey-Izquierdo A, Berman J, et al. Tackling the emerging threat of antifungal resistance to human health. Nat Rev Microbiol. 2022;20(9):557–571. doi:10.1038/s41579-022-00720-1
7. Gong Y, Li C, Wang C, et al. Epidemiology and mortality-associated factors of invasive fungal disease in elderly patients: a 20-year retrospective study from Southern China. Infect Drug Resist. 2020;13:711–723. doi:10.2147/IDR.S242187
8. Lamoth F, R LS, L BE, et al. Changes in the epidemiological landscape of invasive candidiasis. J Antimicrob Chemother. 2018;73:i4–i13. doi:10.1093/jac/dkx444
9. L HD, Neofytos D, J AE, et al. Epidemiology and outcomes of candidemia in 2019 patients: data from the prospective antifungal therapy alliance registry. Clin Infect Dis. 2009;48(12):1695–1703. doi:10.1086/599039
10. Huygens S, Dunbar A, Buil JB, et al. Clinical Impact of polymerase chain reaction-based aspergillus and azole resistance detection in invasive aspergillosis: a prospective multicenter study. Clin Infect Dis. 2023;77(1):38–45. doi:10.1093/cid/ciad141
11. H KS, K YY, J KM, et al. Clinical impact of time to positivity for Candida species on mortality in patients with candidaemia. J Antimicrob Chemother. 2013;68(12):2890–2897. doi:10.1093/jac/dkt256
12. Kreitmann L, Helms J, Martin-Loeches I, et al. ICU-acquired infections in immunocompromised patients. Intensive Care Med. 2024;50(3):332–349. doi:10.1007/s00134-023-07295-2
13. Lass-Florl C, S KS, P GN, et al. Invasive candidiasis. Nat Rev Dis Primers. 2024;10(1):20. doi:10.1038/s41572-024-00503-3
14. Clinical and Laboratory Standards Institute.epidemiological cutoff values for antifungal susceptibility testing.
15. Clinical and Laboratory Standards Institute. Performance Standards for Antifungal Susceptibility Testing of Yeasts.
16. A PM, N JR, V DG, et al. International surveillance of blood stream infections due to Candida species in the European SENTRY Program: species distribution and antifungal susceptibility including the investigational triazole and echinocandin agents. SENTRY Participant Group (Europe). Diagn Microbiol Infect Dis. 1999;35(1):19–25. doi:10.1016/s0732-8893(99)00046-2
17. M RT, B AD, C WR, et al. Management of bacterial and fungal infections in the icu: diagnosis, treatment, and prevention recommendations. Infect Drug Resist. 2023;16:2709–2726. doi:10.2147/IDR.S390946
18. Xiao G, Liao W, Zhang Y, et al. Analysis of fungal bloodstream infection in intensive care units in the Meizhou region of China: species distribution and resistance and the risk factors for patient mortality. BMC Infect Dis. 2020;20(1):599. doi:10.1186/s12879-020-05291-1
19. N TI, C PN, Farias L, et al. Epidemiology, species, antifungal resistance and outcome of candidemia in a university hospital in Buenos Aires, Argentina for 16 years. Rev Chilena Infectol. 2017;34(5):431–440. doi:10.4067/S0716-10182017000500431
20. Vaquero-Herrero MP, Ragozzino S, Iriart X, et al. Candida bloodstream infection in patients with systemic autoimmune diseases. Med Mal Infect. 2020;50(4):372–376. doi:10.1016/j.medmal.2020.01.014
21. Wisplinghoff H, Ebbers J, Geurtz L, et al. Nosocomial bloodstream infections due to Candida spp. in the USA: species distribution, clinical features and antifungal susceptibilities. Int J Antimicrob Agents. 2014;43(1):78–81. doi:10.1016/j.ijantimicag.2013.09.005
22. Reinhold I, Picardi S, Liss B, et al. Towards shorter therapy for candidaemia: defining uncomplicated candidaemia in adults. Lancet Infect Dis. 2026;26(2):e112–e123. doi:10.1016/S1473-3099(25)00409-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.