Back to Journals » Journal of Asthma and Allergy » Volume 18
Clinical, Biomarker, and Radiological Progression from Asthma to Systemic Eosinophilic Granulomatosis with Polyangiitis: A Retrospective Cohort Study
Authors Lu C, Ou C, Deng Y, Li N, Ma Y, Luo J, Zhou J, Chung KF, Deng Z, Zhang Q
Received 10 June 2025
Accepted for publication 22 October 2025
Published 11 November 2025 Volume 2025:18 Pages 1615—1626
DOI https://doi.org/10.2147/JAA.S542255
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Chenyang Lu,1,* Changxing Ou,1,* Yu Deng,2,* Na Li,3,* Yuwen Ma,1 JinXi Luo,1 Jiaxuan Zhou,2 Kian Fan Chung,4 Zhenan Deng,1 Qingling Zhang1,5
1State Key Laboratory of Respiratory Disease, National Clinical Research Center for Respiratory Disease, National Center for Respiratory Medicine, Department of Pulmonary and Critical Care Medicine, Guangzhou Institute of Respiratory Health, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Radiology, the First Affiliated Hospital of Guangzhou Medical University, Guangzhou, Guangdong, People’s Republic of China; 3Department of Pulmonary and Critical Care Medicine, Shenzhen Longgang Central Hospital, Shenzhen, Guangdong, People’s Republic of China; 4National Heart and Lung Institute, Imperial College London, London SW3, UK; Royal Brompton and Harefield Hospital, Guy’s and St Thomas’ NHS Foundation Trust, London SW3, UK; 5Guangzhou National Laboratory, Bioland, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qingling Zhang, Email [email protected] Zhenan Deng, Email [email protected]
Background: Eosinophilic granulomatosis with polyangiitis (EGPA) is a rare multi-organ autoimmune disease characterized by eosinophilic infiltration of peripheral blood and tissues, and necrotizing granulomatous inflammation of small and medium-sized blood vessels. In the prodromal stage of EGPA, patients may present with features of refractory asthma, with the involvement of other organs occurring later when the diagnosis of EGPA is made. The difficulty of early diagnosis makes treatment difficult.
Methods: We retrospectively describe patients (N=13) who attended the asthma clinic at the First Affiliated Hospital of Guangzhou Medical University between 2008 and 2024. The disease course was categorized into three stages: asthma, lung-limited or lung-dominant EGPA (L-EGPA), and systemic EGPA (S-EGPA). Patients with severe eosinophilic asthma served as controls. We evaluated baseline demographic, as well as organ involvement, complication, laboratory findings, lung function, high-resolution computed tomography (HRCT), and treatment across different disease stages. A case–crossover design and Bayesian conditional logistic regression were employed to evaluate the impact of medication use on disease progression.
Results: We identified a group of EGPA patients who exhibited consistent disease progression to transit from asthma to L-EGPA, and eventually to S-EGPA. These stages exhibit distinct clinical and imaging features, with significantly elevated eosinophilic inflammatory markers in induced sputum or blood being a hallmark of L-EGPA. This distinction may aid in differentiating refractory asthma from L-EGPA.
Conclusion: In conclusion, the L-EGPA phase may represent a distinct stage in EGPA development that is often challenging to distinguish from refractory asthma. Characterizing this phase and identifying specific biomarkers could facilitate earlier diagnosis and treatment, potentially improving patient outcomes—a hypothesis that warrants further validation.
Keywords: eosinophilic granulomatosis with polyangiitis, asthma, eosinophilia, rare pulmonary diseases
Introduction
Eosinophilic Granulomatosis with Polyangiitis (EGPA), formerly known as Churg-Strauss Syndrome, is a rare form of antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis that affects multiple organ systems, including the sinuses, lungs, heart, and kidneys. The global pooled estimate for the prevalence of EGPA was 15.27 (95% CI: 11.89–19.61) cases per million individuals.1 A recent study reported that EGPA prevalence in Japan increased from 4.2 per million in 2005 to 38.0 per million in 2017, while in Korea, it rose from 1.1 per million in 2007 to 11.2 per million in 2018.2,3
EGPA is characterised by asthma, eosinophilia, and granulomatous or vasculitic involvement of several organs.4 Diagnosing the disease presents a significant challenge due to its clinical heterogeneity and the absence of definitive biological markers. This is particularly acute in the early stages, where the clinical manifestations frequently overlap with those of refractory asthma, further complicating the diagnostic process.5 Asthma symptoms are observed in 90% to 100% of patients.6,7 The prevalence of EGPA is higher among asthmatics compared to the general population, and their immune manifestations exhibit similarities, suggesting a possible uninvestigated mechanistic link.8
Due to the rarity of EGPA, large cohort studies on its phenotypic presentation remain scarce. However, a number of case reports have documented the clinical course of affected patients. In some instances, individuals initially present to respiratory clinics with symptoms of an asthma exacerbation, with a definitive diagnosis of EGPA often being made only months or even years later, after the progression to multiorgan involvement. Notably, the lungs frequently emerge as the first major organ affected by vasculitis, with subsequent systemic manifestations reflecting the disease’s broader impact.9–13
EGPA that first involves the lungs is more difficult to identify accurately and in a timely manner than EGPA that first involves extrapulmonary organs, because its clinical manifestations closely resemble those of refractory asthma. In our retrospective analysis of EGPA patients attending an asthma clinic, we observed a period of vasculitis primarily confined to the lungs in some cases, preceding the onset of more prominent multiorgan involvement. The patient’s visits were classified into three distinct periods, based on the progression of their diagnosis: asthma (diagnosed according to asthma criteria, with no evidence of vasculitis), L-EGPA (lung-limited or lung-dominant eosinophilic or necrotizing vasculitis), and S-EGPA (clinical manifestations with multisystem involvement). Although we could not definitively establish whether patients with asthma or those in the early phase of L-EGPA exhibited vasculitic changes in other organs that were not clinically evident, identifying the characteristics of L-EGPA could significantly contribute to the timely diagnosis of EGPA.
Patients and Methods
Patients
This was a single-center retrospective study. The patients enrolled in this study attended the asthma clinic at the First Affiliated Hospital of Guangzhou Medical University between 2008 and 2024. Based on the Global Initiative for Asthma (GINA) Guidelines and the American College of Rheumatology (ACR) 1990 Criteria for the Classification of Eosinophilic Granulomatosis with Polyangiitis, they were initially diagnosed with asthma and, months or years later, were subsequently diagnosed with systemic EGPA (S-EGPA, clinical manifestations with multi-system involvement).14,15 In the progression from asthma diagnosis to the eventual diagnosis of S-EGPA, patients undergo a similar intermediate phase characterized by eosinophilic and necrotizing vasculitis of the lungs, corresponding to lung-limited or lung-dominant EGPA (L-EGPA). We included 27 patients meeting the GINA criteria for severe eosinophilic asthma as a control group.
The diagnostic time point for L-EGPA was clearly established for 11 patients based on the 1990 ACR criteria, supported by definitive respiratory histopathology. For the remaining two patients without contemporaneous biopsy, it was determined retrospectively as the first documentation of meeting ACR criteria alongside specific pulmonary manifestations—migratory infiltrates, elevated sputum eosinophils, and lung function decline—after excluding infections, allergic disorders (eg, allergic bronchopulmonary aspergillosis), and drug reactions. None of the 13 patients had extra-pulmonary organ involvement at the time of L-EGPA diagnosis. Progression to S-EGPA was defined as the first occurrence of extra-pulmonary involvement, including abnormalities on echocardiography or cardiac MRI, skin purpura, gastrointestinal biopsy demonstrating vasculitis, or electrophysiological abnormalities. Newly observed systemic manifestations were attributed to EGPA when their temporal sequence and the absence of alternative explanations supported such a relationship.
We evaluated their baseline demographic, as well as organ involvement, complication, laboratory findings, lung function, high-resolution computed tomography (HRCT), and treatment across different disease stages. The study received approval from the Ethics Committee of the First Affiliated Hospital of Guangzhou Medical University (EGPA cohort and severe eosinophilic asthma cohort No.: ES-2024-196-02) and was registered with the Chinese Clinical Trial Registry (Registration No.: ChiCTR-IIC-15007622). All patients have signed informed consent and all identifiers within the article are anonymized.
Methods
The clinical histories of 13 EGPA patients with a similar disease course were retrospectively reviewed through outpatient and inpatient records from the Department of Respiratory and Critical Care Medicine. To minimise lead-time bias, the control group consisted of twenty-seven patients with severe eosinophilic asthma whose disease duration exceeded six years, aligning with the mean interval for progression to L-EGPA. Respiratory physicians and rheumatologists jointly conducted diagnosis and evaluation, while radiologists provided expert HRCT scoring. The pulmonary HRCT inflammation scoring criteria was based on previously published literature.16 The imaging evaluation of sinus inflammation was conducted using the Lund-Mackay Scoring System (LMS).17 Where appropriate, data are presented as median (range), n (%), or median (interquartile range [IQR]). To assess long-term trends in medication exposure prior to EGPA diagnosis, categorical data were analyzed using Fisher’s exact tests due to the small sample size (N ≤ 13). In the case-crossover analysis, the 2-month and 3-month periods preceding EGPA diagnosis were used as separate index periods. The corresponding 2–4 months and 3–6 months prior to diagnosis served as control periods to assess the robustness of the findings.18–20 Odds ratios (ORs) were calculated using a Bayesian conditional logistic regression model in this study due to the small sample size.21
Statistical analyses used non-parametric methods (Friedman test with post-hoc Holm-Bonferroni adjusted Wilcoxon tests) due to the small sample size (N=13), which limits the power of normality assessment (performed via Shapiro–Wilk test and Q-Q plots).22 A two-sided P-value of less than 0.05 was considered statistically significant. All analyses were conducted using R (version 4.4.0) and RStudio (version 19.1.3). The R packages rstatix, tidyverse, brms, and rstan were used for data analysis, while ggplot2, ggpubr, fmsb, ggprism, and scales were employed for data visualization.
Results
Patient Demographics and Clinical Characteristics
13 patients were included in this study. They were initially diagnosed with asthma, subsequently developed EGPA with predominant pulmonary involvement, and ultimately progressed to systemic EGPA with multisystem involvement. (Supplementary Tables 1 and 2) The median time from asthma diagnosis to the diagnosis of L-EGPA was 6.0 (0.6, 19.0) years, while the interval from L-EGPA to the diagnosis of S-EGPA was 1.8 (0.2, 9.0) years. All 13 patients had a history of atopy. Among the respiratory symptoms, wheezing, chest tightness, and dyspnea were present in all patients. Additionally, 92.31% of patients exhibited asthma with elevated eosinophil counts. Eosinophilic gastroenteritis is the most common manifestation of extrapulmonary organ involvement. Only one patient tested positive for ANCA in his blood (Table 1).
 |
Table 1 Characteristics of Patients |
Comparison of Biological Parameters and Lung Function at Different Stages
Indicators of lung inflammation, such as the peak and means percentage of eosinophils in induced sputum, as well as levels of fractional exhaled nitric oxide (FeNO), were observed to be elevated in the L-EGPA phase compared to the other two phases (p.adj ranging from <0.05 to <0.001). Compared with the S-EGPA phase, the L-EGPA phase showed lower peak peripheral blood eosinophil percentage and IgE concentrations (p.adj ranging from <0.01 to <0.001); analysis of mean values showed a significant difference only for eosinophil percentage (p.adj < 0.01). Serum complement C3 concentrations were lower in the EGPA phase than in the asthma phase. Pulmonary function tests suggested a progressive decline in carbon monoxide diffusing capacity (DLCO) from asthma to L-EGPA (p.adj < 0.01), with minimal difference between the L-EGPA and S-EGPA phases. Concurrently, there was a gradual and modest upward trend in forced expiratory volume in 1 second to forced vital capacity ratio (FEV1/FVC), and forced expiratory volume in 1 second as a percentage of predicted value (FEV1%pred). Serum IgG4 concentrations were examined in six patients at all three periods, and progression from L-EGPA to S-EGPA was accompanied by elevated serum IgG4 concentrations in five of them. (Figure 1 and Supplementary Figure 1) To characterise the differences between L-EGPA and asthma, and given that the average time from asthma onset to L-EGPA progression was 6 years in our cohort, we selected a control group of 27 patients with severe eosinophilic asthma of more than 6 years’ duration to match this interval. Compared with this control group, patients with L-EGPA exhibited elevated indicators of systemic and local eosinophilic inflammation, including peripheral blood and sputum eosinophil percentages, and FeNO levels (p ranging from <0.05 to <0.01) (Supplementary Figure 2).
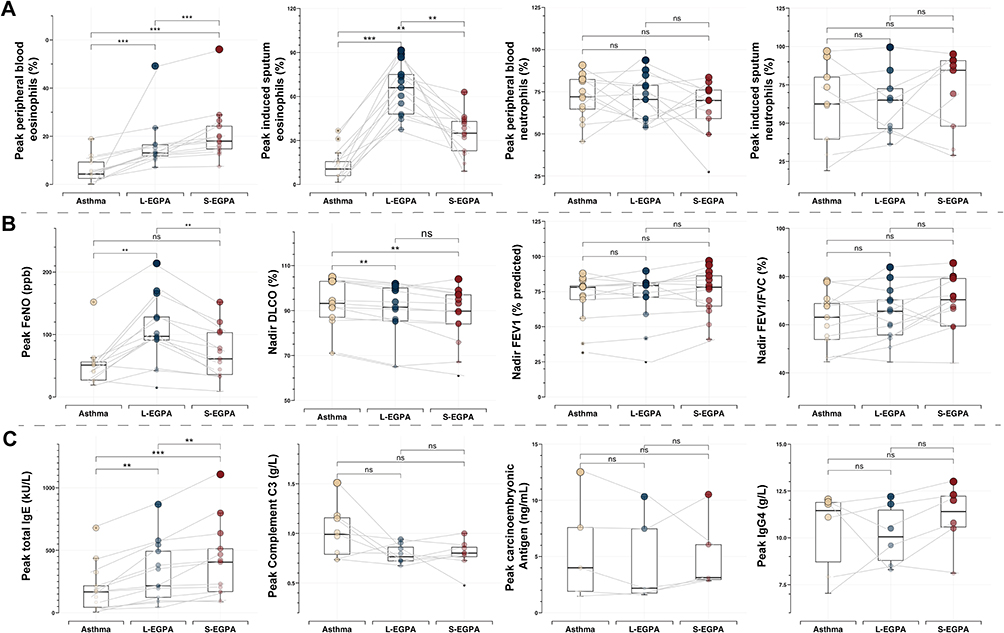 |
Figure 1 Biological Parameters and lung function. At each disease stage, peak values from multiple assessments were recorded for inflammatory cell proportions, FeNO, and inflammatory biomarkers, whereas the lowest pulmonary function values were used. (A) Inflammatory cell profiles (blood and induced sputum); (B) Airway inflammation (FeNO) and pulmonary function; (C) Serum Biomarkers. ns (not significant); **p.adj < 0.01, ***p.adj < 0.001. |
Comparison of Imaging Features at Different Stages
Of the 13 patients, 11 underwent complete, full-course imaging. These data were analyzed by specialized radiologists for sinus inflammatory conditions and the nine classic imaging manifestations of chronic lung inflammation. Inflammation of the sinuses and paranasal sinuses progresses through three stages, with pulmonary imaging showing distinct features at each stage. (Figure 2A) Thickening of the bronchial wall was a common feature across all three periods. Ground-glass opacities were observed to be more prevalent during the asthma period, while consolidation showed an increase during the L-EGPA period, while both imaging manifestations decreased during the S-EGPA period. (Figure 2B) Although overall sinusitis LMS scores did not differ significantly across the three stages, further analysis suggested distinct patterns. With the exception of the ostiomeatal complex, other sinus structures appeared to exhibit milder inflammation during the L-EGPA stage, whereas more pronounced inflammatory changes tended to be observed in the asthma and S-EGPA stages. This pattern may, at least in part, be attributable to the effects of local anti-inflammatory therapy rather than to intrinsic differences in disease activity (Figure 2C).
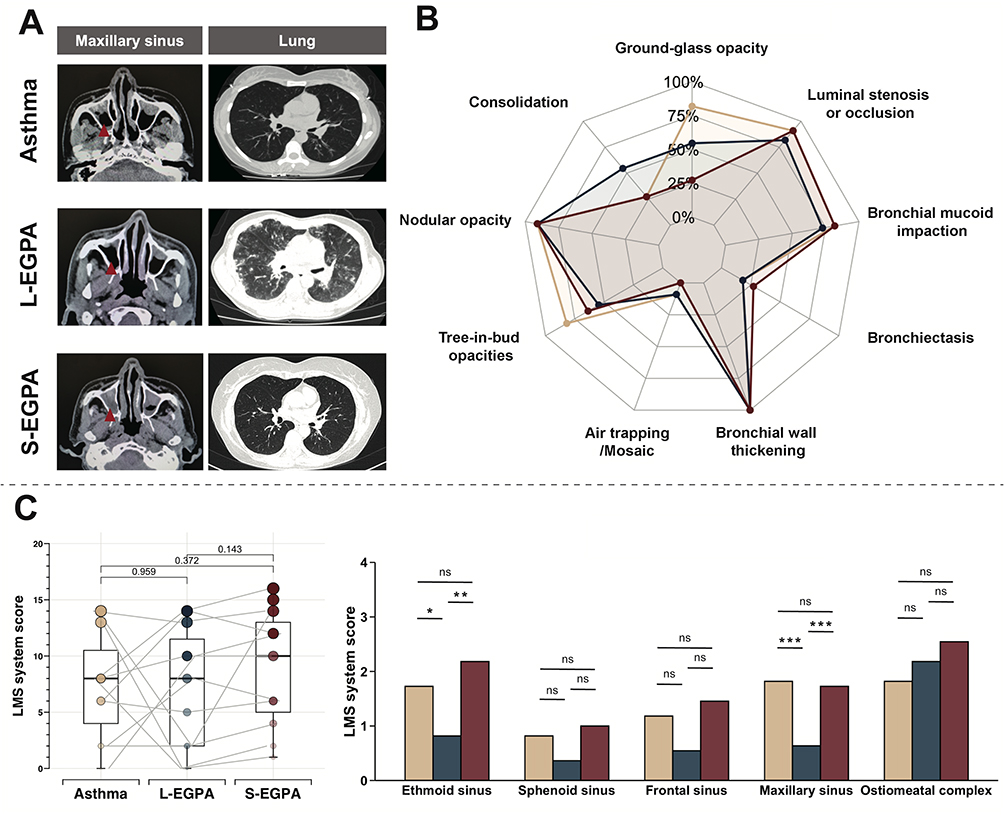 |
Figure 2 Imaging features at different stages. (A) Temporal Imaging Changes in the Maxillary Sinus and Lungs. The red arrows indicate sinus inflammation. (B) Temporal Characterization of HRCT Findings in the Lungs. Proportions reflect the percentage of patients presenting with each imaging feature relative to the total study population. (C) Sinus LMS Imaging Scores across Three Disease Stages. Box plots illustrate the total sinus LMS scores across the three stages, while bar graphs compare LMS scores for different sinuses at each stage. Data are shown for patients with asthma (beige), L-EGPA (dark blue), and S-EGPA (dark red). ns: not significant; *p.adj < 0.05, **p.adj < 0.01, ***p.adj < 0.001. |
Disease Progression and Therapeutic Strategies
The time from diagnosis of L-EGPA to S-EGPA was observed to be shorter than that from diagnosis of asthma to L-EGPA. During both the asthma and L-EGPA phases, some patients exhibited poor control of their asthma symptoms. In the three months preceding the diagnosis of L-EGPA, eight patients received oral glucocorticoids at a dose of ≥10 mg/day, which is considered a relatively medium-high dose in the treatment of eosinophilic asthma.23,24 In the S-EGPA phase, larger doses of oral corticosteroids (OCS) were required for symptom control, and more patients receive non-OCS immunosuppressive therapy as well as biologic therapy. (Table 2) Only one patient required more than two biologically targeted therapies during disease progression. In the S-EGPA phase, the patient initially received two injections of omalizumab as routine treatment, but due to issues with efficacy and tolerability, treatment was switched to dupilumab for one year. Mepolizumab was then added for symptomatic relief but was later discontinued. The patient was subsequently maintained on dupilumab alone.
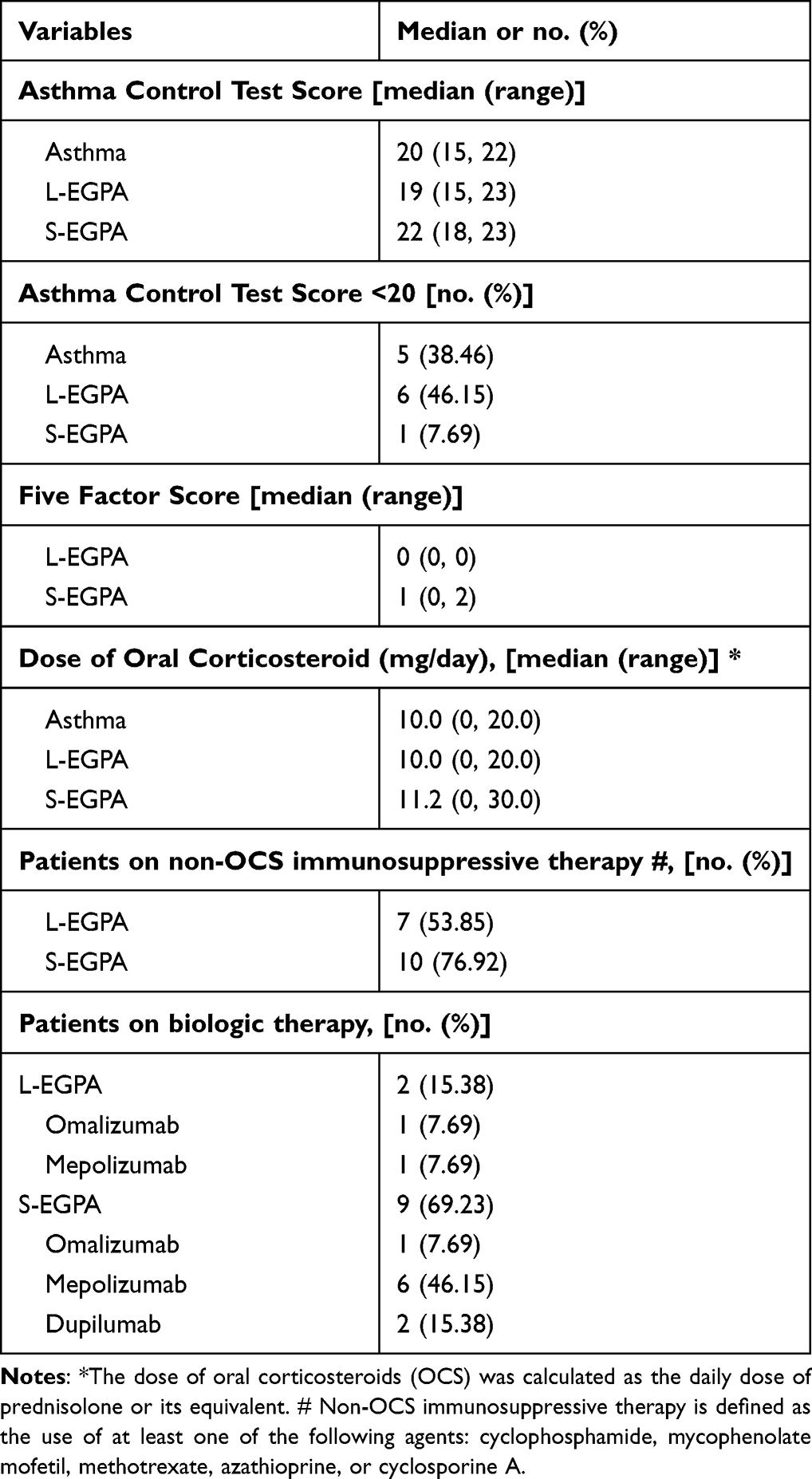 |
Table 2 Disease Progression and Therapeutic Strategies |
This study conducted both a short-term exposure risk analysis and a long-term trend analysis of medication use in patients prior to EGPA diagnosis. In the 12 months preceding EGPA diagnosis, exposure to montelukast, inhaled corticosteroids (ICS), OCS, and long-acting β2-agonists (LABAs) increased over time, with a significant upward trend observed for OCS. (Table 3) In the short-term exposure analysis, OCS suggested an inverse relationship with a reduced risk of L-EGPA onset across both index periods, with ORs of 0.39 (95% CI 0.00, 2.14) and 0.25 (0.03, 1.59), respectively. Montelukast, LABAs and ICS also suggested inverse associations with disease onset. (Supplementary Figure 3) A key limitation in interpreting these associations is the potential for reverse causality. These medications might have been initiated in response to early, pre-diagnostic symptoms of EGPA. Moreover, the progressive reduction in sample size across the control periods (from N = 11 to N = 6) markedly limits the statistical power of this analysis. As such, these findings should be interpreted with caution and considered exploratory and hypothesis-generating rather than definitive.
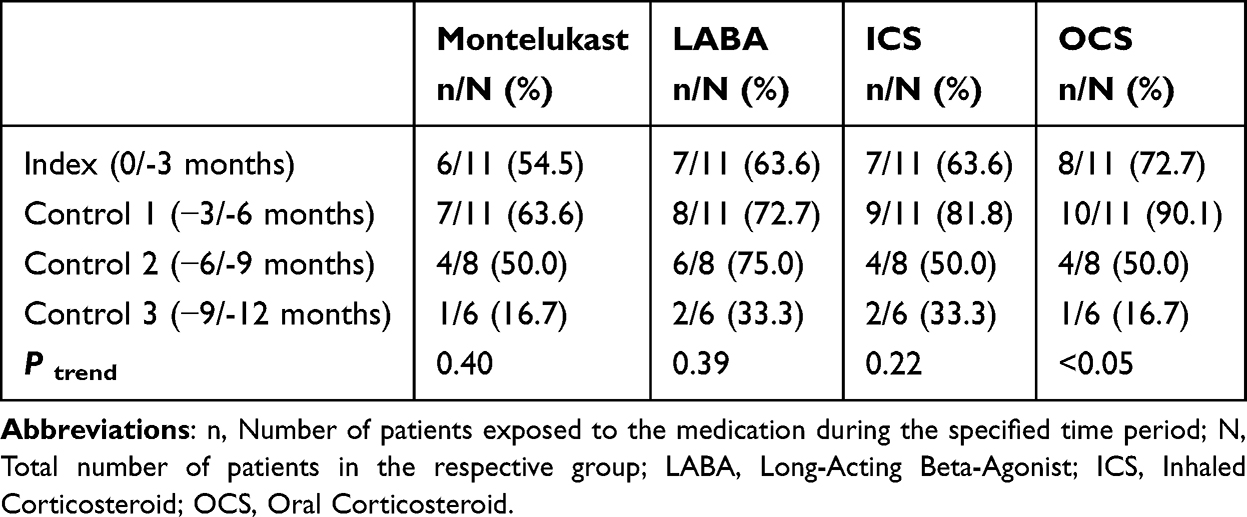 |
Table 3 Proportion of Patients Exposed to Asthma Medications in the 12 months Preceding L-EGPA Onset |
Discussion
We retrospectively analyzed 13 patients with a progression from asthma to L-EGPA and subsequently to S-EGPA. Early recognition and diagnosis of EGPA in these patients is particularly challenging, as vasculitic manifestations affecting organs beyond the respiratory system are often absent in the early stages. Additionally, the respiratory vasculitis symptoms frequently overlap with those of refractory asthma and may be obscured by the therapeutic effects of asthma medications, further complicating timely diagnosis.25 The median time from asthma diagnosis to the onset of L-EGPA was 6.00 (0.60, 19.00) years, whereas the progression from L-EGPA to S-EGPA occurred in a shorter span of 1.75 (0.25, 9.00) years. Given that EGPA with multi-organ involvement is associated with a poorer prognosis, our findings suggest that identifying clinical markers that distinguish L-EGPA from asthma, improving clinicians’ awareness to recognize L-EGPA, and initiating early interventions may help slow disease progression.
Currently, there are no established diagnostic criteria for EGPA, only classification criteria. The most widely recognized include the EGPA classification criteria developed by the American College of Rheumatology (ACR) in 1990,15 the French Orphan Lung Disease Study Group and the European Respiratory Society (GERMOP/ERS) in 2017,26 the MIRRA study in 2017,27 and the updated EGPA classification criteria by the ACR/European League Against Rheumatism (EULAR) in 2022.28 In this retrospective study, which included patient data from 2008 to 2024, we uniformly applied the 1990 ACR classification criteria for disease categorization. Additionally, according to the updated criteria, all 13 patients with L-EGPA stage met the diagnosis of EGPA. Pathological evidence is crucial in the diagnostic process. Notably, the increasing significance of ANCA in EGPA diagnosis was highlighted in the MIRRA 2017 criteria and the GERMOP/ERS 2017.26,27
ANCA, primarily produced by B lymphocytes,29 plays a crucial role in the clinical and pathological landscape of EGPA. EGPA is classified into ANCA-positive and ANCA-negative subtypes, which may differ in clinical presentation, pathology, and immune mechanisms.4 Among our 13 patients, only one tested positive for blood ANCA, a rate lower than the reported 40% ANCA positivity in EGPA.30 This may be due to the fact that all patients were recruited from the respiratory department, as studies have shown that lung involvement is more common in ANCA− than in ANCA+ patients.4 Notably, sputum and blood ANCA levels in EGPA patients with lung involvement do not always correlate, with sputum ANCA more closely reflecting eosinophilic inflammation in the lungs.31 This suggests that localized ANCA may emerge earlier than circulating ANCA in the disease course of EGPA with lung involvement, potentially explaining the low blood ANCA positivity in our cohort.
Consistent with this, in our study, markers of respiratory inflammation in the L-EGPA stage, including the percentage of eosinophils in induced sputum, as well as FeNO, were the highest among the three stages, indicating more severe local inflammation at this stage. Sinus inflammation was reduced during the L-EGPA stage, which may reflect the effects of sinusitis-related treatments initiated during the asthma stage. Sinusitis, mainly affecting the ethmoid and maxillary sinuses — tended to worsened again in the S-EGPA stage, aligning with previous reports.32 At this stage, FeNO levels fell, likely reflecting reduced inflammation in the lower airways. The assessment of nasal nitric oxide (nNO) may help further distinguish sinus inflammation from lower airway involvement.33
In contrast, although blood eosinophil levels were elevated, they remained lower than those observed at the S-EGPA stage. Although a recent study reported that some patients with EGPA did not exhibit a higher percentage of induced sputum eosinophils compared to those with asthma, it is important to note that a subset of patients in that study was classified within a specific asthma subgroup due to the absence of lung pathological evidence.34 It is plausible that this group represented cases with localized eosinophilic inflammation, possibly corresponding to the L-EGPA stage in our study. These findings suggest that focusing on local markers like ANCA and eosinophil counts in induced sputum or bronchoalveolar lavage fluid (BALF) may help identify EGPA in patients with asthma, sinus abnormalities, and blood eosinophils >10%, but without systemic vasculitis. Non-invasive markers provide valuable diagnostic information; however, lung biopsy can offer additional confirmation in selected cases of L-EGPA. Histopathology may reveal early vasculitic changes. Due to its invasive nature, biopsy is typically reserved for cases where non-invasive assessments are inconclusive or differentiation from other eosinophilic lung diseases is needed.12,35 Although IgG4 levels have been linked to EGPA development in asthmatic patients, we did not observe a significant difference in IgG4 levels between the asthma and EGPA stages in our cohort.36,37
To investigate the impact of medication on the progression to EGPA in patients with asthma, we conducted a retrospective analysis of patients’ medication history. Previous studies have suggested that the use of leukotriene receptor antagonists, switching between multiple biologically-targeted agents, and use of oral glucocorticoids may be associated with the development of EGPA.18,38,39 We examined the association between asthma medications and EGPA onset. OCS use increased appeared to increase during the 12 months before diagnosis. In case-crossover analyses, montelukast, LABAs, ICS, and OCS were observed to be associated with a lower risk. The inverse association with OCS was most pronounced but likely reflects reverse causality, as rising use suggests initiation in response to early, pre-diagnostic symptoms. There are notable discrepancies between our findings and those of previous studies. These differences may be explained, in part, by variations in the distribution of EGPA subtypes (ANCA-positive: 7.7% in our cohort vs 40.5% in earlier study).18 Moreover, our analysis specifically focused on the diagnostic window of L-EGPA, whereas prior investigations largely examined cases with systemic, multi-organ involvement.18 Additionally, although both studies employed a case-crossover design, our study had a smaller sample size, leading to differences in statistical methods.21 Furthermore, it remains unclear whether asthma medications contribute to the development of EGPA or simply serve as markers of asthma exacerbation.40 Suboptimal inhaler technique or adherence may have contributed to a relatively greater reliance on OCS. During the Index and Control 1 periods, the slightly higher OCS use compared with ICS or LABA was mainly driven by a single patient. In Control 2, two patients received LABA without concomitant ICS, likely reflecting real-world variability in treatment adherence or patients’ personal choice to minimize corticosteroid exposure. Confounding by indication arising from treatments or interventions based on a patient’s condition should be mitigated through more comprehensive statistical approaches.41 These observations should be regarded as hypothesis-generating and interpreted with caution given the exploratory nature of our analysis.
We identified a distinct group of EGPA patients who exhibited a consistent disease progression: transitioning from asthma to lung-limited or lung-dominant EGPA, and eventually to EGPA with systemic multi-organ involvement. A retrospective analysis of this subgroup allowed us to explore the disease characteristics and biological markers associated with the progression from asthma to lung-limited or lung-dominant EGPA could facilitate early diagnosis and treatment, potentially slowing the systemic progression of EGPA.
Conclusion
This retrospective study of 13 patients with eosinophilic granulomatosis with polyangiitis (EGPA) suggests a stepwise progression from asthma to lung-limited or lung-dominant EGPA, and potentially to systemic disease.
Timely identification of patients with early EGPA among those presenting primarily with asthma may facilitate earlier intervention, inform treatment decisions, and potentially improve long-term outcomes. In this cohort, elevations in FeNO and sputum eosinophil proportions indicate that the L-EGPA stage is associated with increased pulmonary eosinophilic inflammation. Integrating these pulmonary inflammatory changes with other clinical and imaging characteristics could represent a useful strategy for enhancing the early detection of EGPA, although further studies with larger samples are needed to confirm these observations.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article and/or its supplementary materials. Any other information related to this study is available from the corresponding author, Qingling Zhang, upon reasonable request.
Ethical
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The study was registered with the Chinese Clinical Trial Registry (Registration No.: ChiCTR-IIC-15007622). The manuscript has been approved by the First Affiliated Hospital of Guangzhou Medical University and can be published (EGPA cohort and Severe eosinophilic asthma cohort No.: ES-2024-196-02).
Informed Consent
Written informed consent was obtained from all participants for both participation in the study and for the publication of the findings.
Acknowledgments
We thank the patients and families involved in this study. We are grateful to Lu Peng, Yongkang Liao, Junjie Wen, Mingkai Huang, and Bocai Zhang (First Affiliated Hospital of Guangzhou Medical University) for technical assistance. We also appreciate Dandan Chen (Shenzhen People’s Hospital), Enli Zhang (Xingyi People’s Hospital), Xiaohui Wang (Guangzhou Women and Children’s Medical Center), and Jie Yan (Guangzhou Medical University) for their advisory input.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Guangzhou Municipal Science and Technology Bureau Basic Research Program (2025A03J4397), National Natural Science Foundation of China (82570040, 82400031), National Science and Technology Major Project (2024ZD0529803), Major clinical research project of the Guangzhou Medical University Research Ability Enhancement Program (GMUCR2024-01010), ZHONGNANSHAN MEDICAL FOUDATION OF GUANGDONG PROVINCE (ZNSA-2020013, ZNSXS-20220083, ZNSXS-20240005), Guangzhou Science and Technology Plan Project and ZHONGNANSHAN MEDICAL FOUDATION OF GUANGDONG PROVINCE (202102010355, ZNSA-2020003), Science and Technology Innovation Project of Guangzhou Medical University (2022A015), Undergraduate Innovation Ability Improvement Program of Guangzhou Medical University (02-408-2304-01023XM), Foundation of Featured Clinical Technique of Guangzhou (2019TS24), Clinical and Epidemiological Research Project of State Key Laboratory of Respiratory Disease (SKLRD-L-202404), Construction Project of Guangzhou Demonstration Unit for Collaborative Treatment of Critical and Difficult Diseases with Traditional Chinese and Western Medicine.
Disclosure
Kian Chung reports grants from Medical Research Council, personal fees from GSK, personal fees from Novartis, personal fees from Merck, personal fees from Reckitt-Beckinson, personal fees from Trevi, personal fees from Nocion, personal fees from Haleon, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Jakes RW, Kwon N, Nordstrom B, et al. Burden of illness associated with eosinophilic granulomatosis with polyangiitis: a systematic literature review and meta-analysis. Clin Rheumatol. 2021;40(12):4829–4836. doi:10.1007/s10067-021-05783-8
2. Sada KE, Suzuki T, Joksaite S, et al. Trends in prevalence, treatment use, and disease burden in patients with eosinophilic granulomatosis with polyangiitis in Japan: real-world database analysis. Mod Rheumatol. 2024;34(5):988–998. doi:10.1093/mr/road104
3. Lee JH, Hong SH, Yu I, et al. Incidence, prevalence, and mortality of eosinophilic granulomatosis with polyangiitis in Korea: a nationwide population-based study. Allergy Asthma Immunol Res. 2024;16(2):168–178. doi:10.4168/aair.2024.16.2.168
4. Emmi G, Bettiol A, Gelain E, et al. Evidence-based guideline for the diagnosis and management of eosinophilic granulomatosis with polyangiitis. Nat Rev Rheumatol. 2023;19(6):378–393. doi:10.1038/s41584-023-00958-w
5. Sacoto G, Boukhlal S, Specks U, Flores-Suárez LF, Cornec D. Lung involvement in ANCA-associated vasculitis. Presse Med. 2020;49(3):104039. doi:10.1016/j.lpm.2020.104039
6. Comarmond C, Pagnoux C, Khellaf M, et al. Eosinophilic granulomatosis with polyangiitis (Churg-Strauss): clinical characteristics and long-term followup of the 383 patients enrolled in the French vasculitis study group cohort. Arthritis Rheum. 2013;65(1):270–281. doi:10.1002/art.37721
7. Puan Y, Ong KY, Tiew PY, et al. Characteristics of severe asthma clinic patients with eosinophilic granulomatosis with polyangiitis. J Allergy Clin Immunol Pract. 2025;13(2):361–368.e2. doi:10.1016/j.jaip.2024.10.013
8. White J, Dubey S. Eosinophilic granulomatosis with polyangiitis: a review. Autoimmun Rev. 2023;22(1):103219. doi:10.1016/j.autrev.2022.103219
9. Ou C, Ma J, Lai N, et al. Severe asthma with viral infection can develop into eosinophilic granulomatosis with polyangiitis. Rheumatol Immunol Res. 2021;2(4):249–254. doi:10.2478/rir-2021-0034
10. Mahmood K, Butt NI, Ashfaq F, Aftab S. Eosinophilic Granulomatosis with Polyangiitis (EGPA): a case report with atypical presentation. Pak J Med Sci. 2023;39(1):307–309. doi:10.12669/pjms.39.1.6436
11. Lee W, Teo FS, Santosa A, Teng GG. Eosinophilic granulomatosis with polyangiitis preceding allergic bronchopulmonary aspergillosis. Eur Ann Allergy Clin Immunol. 2015;47(6):228–231.
12. Nasser M, Thivolet-Béjui F, Sève P, Cottin V. Lung-limited or lung-dominant variant of eosinophilic granulomatosis with polyangiitis. J Allergy Clin Immunol Pract. 2020;8(6):2092–2095. doi:10.1016/j.jaip.2020.01.058
13. Ou Y, Zhang L, Zhou L, Shen C, Ouyang R. Clinical characteristics of eosinophilic granulomatosis with polyangiitis involving the lung in 13 patients. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022;47(10):1355–1364. doi:10.11817/j.issn.1672-7347.2022.210579
14. Bateman ED, Hurd SS, Barnes PJ, et al. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J. 2008;31(1):143–178. doi:10.1183/09031936.00138707
15. Masi AT, Hunder GG, Lie JT, et al. The American college of rheumatology 1990 criteria for the classification of churg-strauss syndrome (allergic granulomatosis and angiitis). Arthritis Rheum. 1990;33(8):1094–1100. doi:10.1002/art.1780330806
16. Akira M, Inoue G, Yamamoto S, Sakatani M. Non-specific interstitial pneumonia: findings on sequential CT scans of nine patients. Thorax. 2000;55(10):854–859. doi:10.1136/thorax.55.10.854
17. Lund VJ, Mackay IS. Staging in rhinosinusitus. Rhinology. 1993;31(4):183–184.
18. Hauser T, Mahr A, Metzler C, et al. The leucotriene receptor antagonist montelukast and the risk of Churg-Strauss syndrome: a case-crossover study. Thorax. 2008;63(8):677–682. doi:10.1136/thx.2007.087825
19. Etminan M, Gill S, Fitzgerald M, Samii A. Challenges and opportunities for pharmacoepidemiology in drug-therapy decision making. J Clin Pharmacol. 2006;46(1):6–9. doi:10.1177/0091270005283285
20. Wang PS, Schneeweiss S, Glynn RJ, Mogun H, Avorn J. Use of the case-crossover design to study prolonged drug exposures and insidious outcomes. Ann Epidemiol. 2004;14(4):296–303. doi:10.1016/j.annepidem.2003.09.012
21. Greenland S, Schwartzbaum JA, Finkle WD. Problems due to small samples and sparse data in conditional logistic regression analysis. Am J Epidemiol. 2000;151(5):531–539. doi:10.1093/oxfordjournals.aje.a010240
22. Mohd Razali N, Yap B. Power comparisons of shapiro-wilk, kolmogorov-smirnov, lilliefors and anderson-darling tests. J Stat Model Analytics. 2011;2:21–33.
23. Roberts E. Oral corticosteroids for patients with eosinophilic diseases: an expert panel view on use, overuse, and strategies to reduce use. Eur Med J. 2023;69–79. doi:10.33590/emj/10303904
24. Sood V, Rogers L, Khurana S. Managing corticosteroid-related comorbidities in severe asthma. Chest. 2021;160(5):1614–1623. doi:10.1016/j.chest.2021.05.021
25. Xie H, Zhang X, Zhang J, Liu M, Che X. The diagnosis of eosinophilic granulomatosis with polyangiitis has been ‘masked’ by asthma: a case report. AME Case Rep. 2025;9:31. doi:10.21037/acr-24-79
26. Cottin V, Bel E, Bottero P, et al. Revisiting the systemic vasculitis in eosinophilic granulomatosis with polyangiitis (Churg-Strauss): a study of 157 patients by the Groupe d’Etudes et de recherche sur les maladies orphelines pulmonaires and the European respiratory society taskforce on eosinophilic granulomatosis with polyangiitis (Churg-Strauss). Autoimmun Rev. 2017;16(1):1–9. doi:10.1016/j.autrev.2016.09.018
27. Wechsler ME, Akuthota P, Jayne D, et al. Mepolizumab or placebo for eosinophilic granulomatosis with polyangiitis. N Engl J Med. 2017;376(20):1921–1932. doi:10.1056/NEJMoa1702079
28. Robson JC, Grayson PC, Ponte C, et al. 2022 American college of rheumatology/European alliance of associations for rheumatology classification criteria for granulomatosis with polyangiitis. Arthritis Rheumatol. 2022;74(3):393–399. doi:10.1002/art.41986
29. Bashford-Rogers RJM, Bergamaschi L, McKinney EF, et al. Analysis of the B cell receptor repertoire in six immune-mediated diseases. Nature. 2019;574(7776):122–126. doi:10.1038/s41586-019-1595-3
30. McBrien C, Menzies-Gow A. Sputum antineutrophil cytoplasmic antibodies in eosinophilic granulomatosis with polyangiitis. time to start sampling the right compartment? Am J Respir Crit Care Med. 2019;199(2):131–133. doi:10.1164/rccm.201809-1640ED
31. Mukherjee M, Thomas SR, Radford K, et al. Sputum antineutrophil cytoplasmic antibodies in serum antineutrophil cytoplasmic antibody-negative eosinophilic granulomatosis with polyangiitis. Am J Respir Crit Care Med. 2019;199(2):158–170. doi:10.1164/rccm.201804-0809OC
32. Nakamaru Y, Takagi D, Suzuki M, et al. Otologic and rhinologic manifestations of eosinophilic granulomatosis with polyangiitis. Audiol Neurootol. 2016;21(1):45–53. doi:10.1159/000442040
33. Rimmer J, Hellings P, Lund VJ, et al. European position paper on diagnostic tools in rhinology. Rhinology. 2019;57(Suppl S28):1–41. doi:10.4193/Rhin19.410
34. Latorre M, Seccia V, Puxeddu I, et al. Severe eosinophilic asthma or eosinophilic granulomatosis with polyangiitis: potential biomarkers for novel diagnostic strategies. J Allergy Clin Immunol Pract. 2024;12(11):3057–3067. doi:10.1016/j.jaip.2024.08.011
35. Cottin V, Bel E, Bottero P, et al. Respiratory manifestations of eosinophilic granulomatosis with polyangiitis (Churg–Strauss). Eur Respir J. 2016;48(5):1429–1441. doi:10.1183/13993003.00097-2016
36. Dong ZM, Lin E, Wechsler ME, et al. Pulmonary eosinophilic granulomatosis with polyangiitis has IgG4 plasma cells and immunoregulatory features. Am J Pathol. 2020;190(7):1438–1448. doi:10.1016/j.ajpath.2020.03.005
37. Flament T, Marchand-Adam S, Gatault P, Dupin C, Diot P, Guilleminault L. What are the characteristics of asthma patients with elevated serum IgG4 levels? Respir Med. 2016;112:39–44. doi:10.1016/j.rmed.2016.01.014
38. Berti A, Cornec D, Casal Moura M, et al. Eosinophilic granulomatosis with polyangiitis: clinical predictors of long-term asthma severity. Chest. 2020;157(5):1086–1099. doi:10.1016/j.chest.2019.11.045
39. Eger K, Pet L, Weersink EJM, Bel EH. Complications of switching from anti-IL-5 or anti-IL-5R to dupilumab in corticosteroid-dependent severe asthma. J Allergy Clin Immunol Pract. 2021;9(7):2913–2915. doi:10.1016/j.jaip.2021.02.042
40. Park HJ, Jeon S, Lee HS, et al. A comparison of the effectiveness of asthma medications on asthma exacerbations in real world national cohort. J Asthma Allergy. 2022;15:1155–1165. doi:10.2147/JAA.S379394
41. Secrest MH, Platt RW, Dormuth CR, et al. Extreme restriction design as a method for reducing confounding by indication in pharmacoepidemiologic research. Pharmacoepidemiol Drug Saf. 2020;29 Suppl 1(S1):26–34. doi:10.1002/pds.4708
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.