Back to Journals » International Journal of Women's Health » Volume 17
Clinical Application of Noninvasive Prenatal Testing in Singleton Pregnancy with and without in vitro Fertilization: A 6-year Observational Study at a Single Tertiary Center
Authors Zhang Q ![]() , Guo Y, Liang B
, Guo Y, Liang B ![]() , Chen M
, Chen M ![]() , Wu X
, Wu X ![]() , Lin N, Huang H
, Lin N, Huang H ![]() , Xu L
, Xu L ![]()
Received 18 June 2025
Accepted for publication 7 September 2025
Published 17 September 2025 Volume 2025:17 Pages 3067—3076
DOI https://doi.org/10.2147/IJWH.S547427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Qian Zhang,* Yuhong Guo,* Bin Liang, Meihuan Chen, Xiaoqing Wu, Na Lin, Hailong Huang, Liangpu Xu
Department of Medical Genetic Diagnosis and Therapy Center, Fujian Key Laboratory for Prenatal Diagnosis and Birth Defect, Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, 350001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liangpu Xu, Medical Genetic Diagnosis and Therapy Center, Fujian Key Laboratory for Prenatal Diagnosis and Birth Defect, Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, No. 18 Daoshan Road, Gulou District, Fuzhou, Fujian, 350001, People’s Republic of China, Email [email protected]
Background: Studies on the use of noninvasive prenatal testing (NIPT) in pregnancies conceived by in vitro fertilization (IVF) remain inadequate. This study aimed to evaluate the performance of NIPT in singleton pregnancies conceived by IVF and to compare it with that in naturally conceived (NC) pregnancies.
Methods: A retrospective analysis was performed on 86397 pregnancies (IVF=3723, NC=82674). The performance of NIPT was assessed by calculating the sensitivity, specificity, and positive predictive value (PPV).
Results: The failure rate in the IVF group was significantly higher than that in the NC group (0.16% vs 0.04%, p < 0.05). Among the 3717 cases successfully tested in the IVF group, the sensitivities of trisomy (T) 21 and sex chromosome aneuploidy (SCA) were both 100%, with specificities of 99.92% and 99.76%, respectively. The PPVs of T21 and SCA were both 50%. Of the 82630 cases successfully tested in the NC group, all corresponding sensitivities and specificities were greater than 98%. The PPVs of T21, T18, T13, SCA and rare autosomal aneuploidies were 70.86%, 41.67%, 20.51%, 39.90%, and 7.65%, respectively. Furthermore, although the median fetal fractions (FFs) in the IVF group were significantly lower than that in the NC group (11.23% vs 12.05%, p < 0.001), the kinetics of FFs during gestation demonstrated a very similar trend between these two groups.
Conclusion: Our findings suggest that NIPT is a valid technique for detecting fetal chromosomal aneuploidies in IVF singleton pregnancies.
Keywords: NIPT, IVF, natural conception, performance, kinetics of fetal fractions
Introduction
In vitro fertilization (IVF) is increasingly utilized worldwide for individuals who are unable to conceive naturally.1 As the population of people seeking IVF consists mainly of women with advanced maternal age, prenatal screening is essential to identify high-risk pregnancies.
Traditional prenatal testing includes noninvasive screening such as maternal serum screening (MSS) and invasive prenatal diagnostic (IPD) procedures. However, the MSS markers were significantly altered in pregnancies who conceived via IVF, with an increase in total human chorionic gonadotropin and a decrease in pregnancy-associated plasma protein A, leading to a higher false positive rate (FPR) in IVF compared to natural conception.2,3 The IPD procedures are more accurate than noninvasive screening, but the risk of procedure-related miscarriage discourages IVF pregnancies from opting for this method.4 For these reasons, efforts continue to develop noninvasive methods for prenatal testing.
The advent of noninvasive prenatal testing (NIPT) by detecting cell-free DNA (cfDNA) in maternal circulation has provided new insights for prenatal testing of IVF pregnancies. In 1997, Lo et al first reported the presence of cell-free fetal DNA in the plasma of pregnant women.5 Since 2011, NIPT has become an important part of prenatal screening in clinical practice.
Numerous studies have shown that NIPT is an effective screening method for fetal trisomies (T) 21, 18, and 13, with a higher sensitivity (91–99.7%) and a lower FPR (0.04–0.08%) than other currently available screening methods.6–8 However, considering the complexity of IVF pregnancies, such as, decreased fetal fractions (FFs),9 multiple pregnancies,10 and a higher prevalence of vanishing twins,11 the National Health and Family Planning Commission of the People’s Republic of China classified the IVF population as a group with cautious use of NIPT in 2016.12 In recent years, there have been only a limited number of studies showing the feasibility of NIPT in IVF pregnancies.13,14 This study aimed to assess the performance of NIPT in singleton IVF pregnancies and to compare it with that of naturally conceived (NC) pregnancies. The changing patterns of FFs during gestation will also be investigated.
Materials and Methods
Subjects
The study recruited 86397 women with singleton pregnancies who underwent NIPT in Fujian Provincial Maternity and Children’s Hospital (Fuzhou, China) from September 2018 to December 2024. The pregnancies were divided into two groups according to the mode of conception, including 3723 cases in the IVF group and 82674 cases in the NC group (Figure 1).
 |
Figure 1 Flow chat of the study. Abbreviations: NIPT, noninvasive prenatal testing; IVF, in vitro fertilization; NC, naturally conceived; IPD, invasive prenatal diagnosis; TOP, termination of pregnancy; T, trisomy; SCA, sex chromosome aneuploidy; RAAs, rare autosomal aneuploidies; TP, true positive; FP, false positive. |
Noninvasive Prenatal Testing
For each patient undergoing NIPT, 10 mL of peripheral venous blood was collected in an EDTA anticoagulant tube and separated through a double centrifugation procedure within 96 h, and those with problems of inadequate blood volume, hemolysis, incorrect tube labeling and delays in arrival to the laboratory were excluded. The cfDNA was extracted via a DNA extraction and purification kit (Berry Genomics Corporation, China), and the concentration was measured via a Qubit 2.0 fluorimeter (Thermo Fisher Scientific, Waltham, MA, USA). Follow-up DNA library preparation, purification, sequencing, and data analysis were performed with the Bambni™ assay (Berry Genomics Corporation). NextSeq CN500 sequencing platform (Berry Genomics Corporation) was used for massive parallel sequencing (MPS). The Z scores were calculated for the targeted chromosomes, as previously described (cut-off: | Z | = 3).15
Chromosome Karyotype Analysis
The process of karyotyping analysis, including cell culture and G-banded karyotyping, performed according to standard procedures. Karyotypes were described at a resolution of 320–500 bands level and was analyzed according to the international system for human cytogenetic nomenclature 2020 (ISCN 2020).
Chromosomal Microarray Analysis (CMA) and Data Interpretation
The genomic DNA (gDNA) of the fetus was extracted from amniotic fluid or umbilical cord blood by using a QIAGEN kit according to the manufacturer’s instructions. Next, the gDNA was digested, ligated, amplified, purified, fragmented, labeled, hybridized, stained, and scanned according to the standard operating procedure of the Affymetrix CytoScan 750 K array (Affymetrix Inc., Santa Clara, CA, USA). This array includes approximately 200000 probes for single nucleotide polymorphisms and 550000 probes for copy number variations (CNVs) distributed across the entire human genome. Chromosome Analysis Suite V3.2 software was used for data analysis. The human genome version GRCh37 (hg19) was used for annotation. CNVs larger than 400 kb and a loss of heterozygosity ≥ 10 Mb were considered. All detected CNVs were compared with public databases as follows: Database of Genomic Variants (DGV), Database of Chromosome Imbalance and Phenotype in Humans Using Ensemble Resources (DECIPHER), International Standards for Cytogenomic Arrays Consortium, and Online Mendelian Inheritance in Man (OMIM).
Statistical Analysis
The collected data were analyzed using SPSS v20.0 (SPSS Inc., Chicago, IL, USA) and the drawings were performed using Origin 2024 (Origin Lab Corporation, USA). The distribution of continuous variables was examined by histograms. Student’s t test was used for parametric continuous data and Mann-Whitney U-test for the non-parametric continuous data. Pearson’s chi-squared test, continuity correction, or Fisher’s exact test were used for categorical variables as appropriate. Normally distributed data are shown as means ± standard deviation (SD) or median ± interquartile range (IQR), and categorical data are presented as percentages. The 95% confidence intervals (CIs) were calculated using VassarStats (http://vassarstats.net/). Statistical significance was defined as p < 0.05.
Results
Study Population
A total of 86397 women with singleton pregnancies were enrolled and underwent NIPT, including 3723 pregnancies in the IVF group and 82674 in the NC group (Table 1). Compared to the NC group, the maternal age in the IVF group was significantly higher (p < 0.001), and the gestational age was significantly lower (p < 0.001). The indications for sampling between these two groups varied considerably (p < 0.001), and every indication except missing shows a significant difference (p < 0.05). Voluntary screening was the most common indications for testing in both groups and were higher for IVF pregnancies than for spontaneous pregnancies (42.06% vs 32.17%, p < 0.05). Advanced maternal age and high/moderate risk of MSS were the second common indications for sampling in the IVF group and the NC group, respectively (41.74% and 29.12%, respectively).
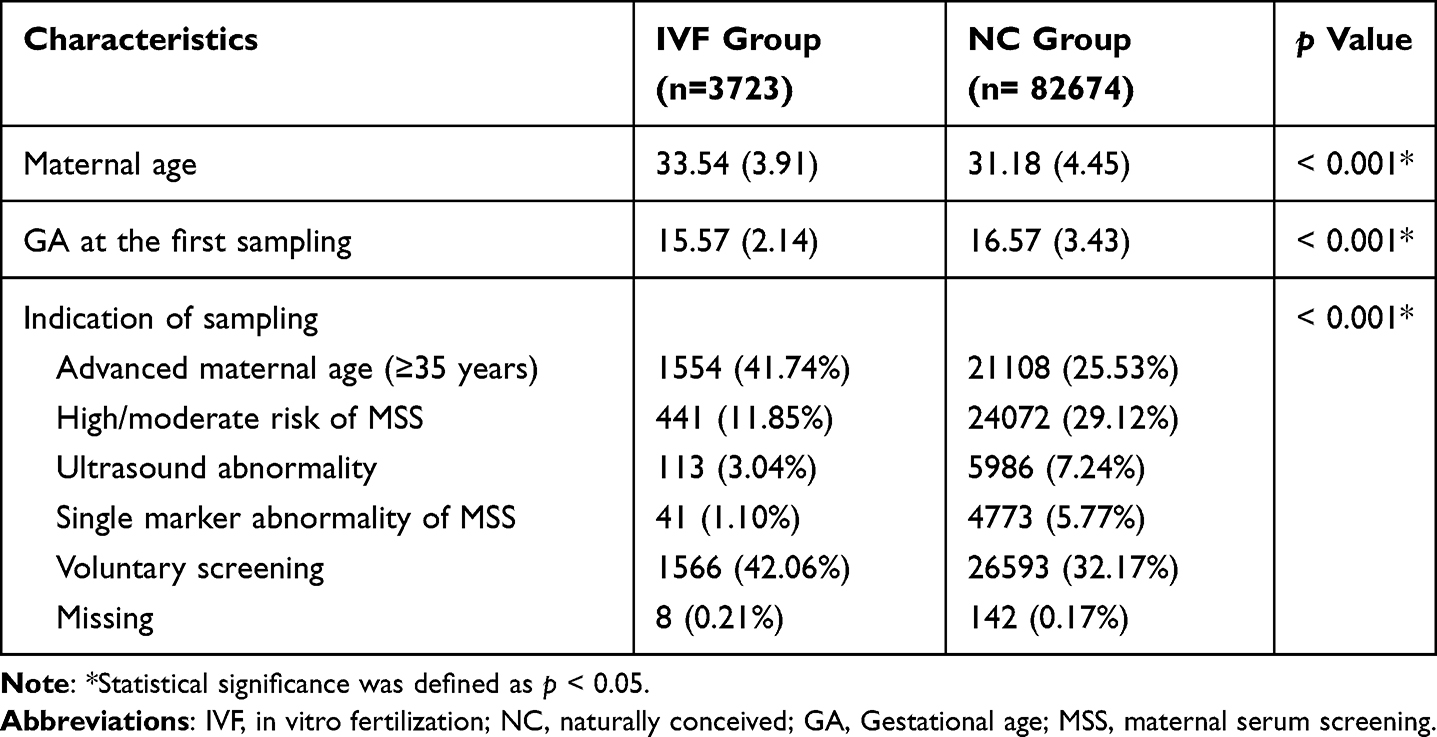 |
Table 1 Maternal Characteristics of Study Population |
The Rate of NIPT Test Failure
Overall, after first sequencing, 86 (2.31%, 86/3723) cases in the IVF group did not yield results, and 1403 (1.70%, 1403/82674) cases in the NC group also failed to obtain results. Of the 1403 cases that failed in the NC group, 9 declined retesting, including 1 who experienced a spontaneous miscarriage. After retesting, 80 and 1359 cases were detected in these two groups, with success rates of 93.02% (80/86) and 97.49% (1359/1394), respectively. The final failure rates in the IVF group and NC group were 0.16% (6/3723) and 0.04% (35/82665), respectively. Both the failure rate after the first sequencing (2.31% vs 1.70%, p < 0.05) and the final failure rate (0.16% vs 0.04%, p < 0.05) in the IVF group were significantly higher than those in the NC group.
Performance of NIPT for Detecting Fetal Chromosomal Aneuploidies
In the IVF group, 3717 cases were successfully tested. Among these, 45 were NIPT-positive, which included trisomy (T) 21 in 6 cases, T18 in 2 cases, T13 in 3 cases, sex chromosome aneuploidy (SCA) in 21 cases and rare autosomal aneuploidies (RAAs) in 13 cases. In the NC group, 82630 cases were successfully tested, with 1003 yielding positive NIPT results. This included T21 in 177 cases, T18 in 56 cases, T13 in 46 cases, SCA in 497 cases and RAAs in 227 cases (Figure 1).
Among the 1048 NIPT-positive cases, 853 cases underwent IPD (IVF=36; NC=817), with the total IPD rate of 81.39% (853/1048). The remaining 195 (IVF=9; NC=186) cases did not receive IPD (Figure 1 and Table 2), including 69 (IVF=5; NC=64) cases with live birth, 32 (IVF=1; NC=31) cases with termination of pregnancy (TOP), and 94 (IVF=3; NC=91) cases lost to follow-up, representing a follow-up rate of 91.03% (954/1048).
 |
Table 2 Performance of NIPT for Detecting Fetal Chromosomal Aneuploidies |
In the IVF group, a total of 36 NIPT-positive cases underwent IPD, resulting in an IPD rate of 80% (36/45). Among these cases, there were 12 true positives, including 3 cases of T21 and 9 cases of SCA, with an overall detection rate of 0.32% (12/3717, 95% CIs: 0.18–0.58%). The sensitivities of T21 and SCA were both 100%, with specificities of 99.92% and 99.76%, respectively. The positive predictive values (PPVs) of T21 and SCA were both 50%. In the NC group, 817 were verified through IPD, resulting in an IPD rate of 81.46% (817/1003). Among these cases, 307 were identified as true positives, including 107 cases of T21, 20 cases of T18, 8 cases of T13, 158 cases of SCA and 14 cases of RAAs, with an overall detection rate of 0.37% (307/82630, 95% CIs: 0.33–0.42%). There was no significant difference in overall detection rate between the two groups (0.32% vs 0.37%, p > 0.05). Besides, 2 cases were identified with false negative for T21. All corresponding sensitivities and specificities were greater than 98%. The corresponding PPVs were 70.86%, 41.67%, 20.51%, 39.90%, and 7.65%. The overall FPR was 0.65% (24/3696, 95% CIs: 0.44–0.97%) in the IVF group and 0.62% (510/82135, 95% CIs: 0.57–0.68%) in the NC group, with no significant difference between the two groups (p > 0.05). Details of NIPT for detecting SCA and RAAS in two groups were shown in Supplementary Tables S1 and S2.
Comparison of the Kinetics of FFs at Different Gestational Ages in the Two Groups
Even though the median FFs in the IVF group were significantly lower than that in the NC group (11.23% vs 12.05%, p < 0.001), the kinetics demonstrated a very similar trend between these two groups (Figure 2). There was a slight increase of median FFs from the 12th to the 20th week in both two group (IVF: 10.21% to 12.94%, NC: 12.25% to 12.26%, respectively). The median FFs rose from 12.94% to 21.8% from the 21th to the 27th week in IVF pregnancies, and rose from 12.46% to 19.85% from the 21th to the 31th week in the NC group. The box-plot graph exhibited that FFs increased rapidly after 21th week than before in both two groups.
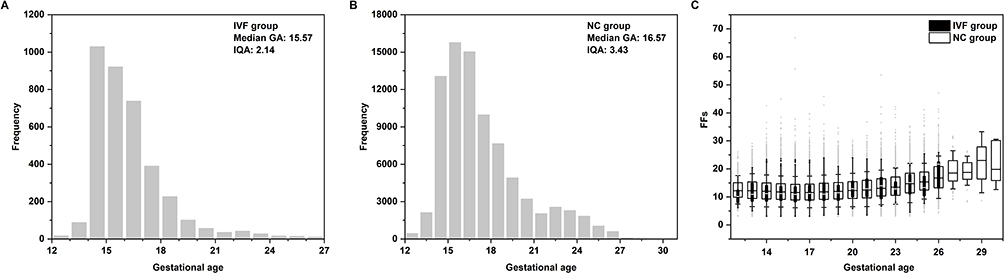 |
Figure 2 Frequency distribution and kinetics of FFs during gestational age. (A and B) Frequency distribution of the gestational age of pregnant women in two groups; (C) The box-plot graph of FFs at different gestational age in two groups. |
Discussion
In recent years, NIPT has emerged as an effective tool for screening fetal chromosomal aneuploidies, particularly in NC pregnancies.6,16 Several studies had demonstrated that NIPT is also effective in twin pregnancies.1,17 However, researches on the use of NIPT in IVF pregnancies is limited.13,18 Most of these studies did not provide detailed comparisons between IVF and NC populations, and large-scale studies remain scarce.
This study retrospectively compares IVF-conceived singleton pregnancies that underwent NIPT with NC counterparts. Women undergoing IVF treatment often face challenges in conceiving naturally and tend to be older at the time of conception.19 In this study, the mean maternal age was higher in the IVF group than in the NC group (33.54 vs 31.18, p < 0.001), consistent with a previous report.20 Although the proportion of pregnancies with advanced maternal age was significantly higher in the IVF pregnancies than in the NC group, the overall detection rates of chromosomal abnormalities with NIPT showed no significant difference between the two groups (0.32% vs 0.37%, p > 0.05). A cross-sectional analysis demonstrated that there was no significant difference in diagnosis of genetic conditions between infants conceived with assisted reproductive technology or unassisted (10.1% vs 13.2%), which was confirmed in our results.21 The gestational age at the first sampling in the IVF group was slightly earlier than that in the NC group (15.57 vs 16.57, p < 0.001), consistent with previous study.22 This difference can be attributed to the physical and mental stress experienced by the IVF population, which drives them to seek results as quickly as possible.
According to our findings, NIPT showed high sensitivity and specificity for both T21 and SCA in the IVF group (both greater than 99%), whereas the corresponding PPVs were both moderate (both 50%). In the NC group, NIPT was comparably sensitive and specific for all trisomies (all greater than 98%), whereas overall PPV was only 37.58% (95% CIs: 34.26–41.01%). The PPVs for T21, T18, T13, SCA, RAAs were 70.86%, 41.67%, 20.51%, 39.90%, and 7.65%, respectively. There was no significant difference in the PPVs for T21 and SCA between the two groups (50% vs 70.86%, p > 0.05, 50% vs 39.9%, p > 0.05, respectively). However, the PPV for T21 was higher in the NC group than in the IVF group, possibly due to the limited number of true positive cases in the IVF group. When sensitivity and specificity remain constant, the PPV increases with disease prevalence in the population. The incidence of T21 is approximately 0.15% in China.23 According to our results, the detection rate of T21 was 0.08% (3/3717) in the IVF group and 0.13% (107/82630) in the NC group, both slightly below reported values. This discrepancy is probably due to the exclusion of high-risk pregnancies that bypassed NIPT, including cases involving advanced maternal age or early ultrasound abnormalities, where direct IPD was performed instead. Consequently, the observed NIPT detection rates were substantially lower than those previously documented. The overall incidence of SCA is approximately 0.23%, exceeding the prevalence of common T21 based on prior research.24,25 In the IVF group, the SCA detection rate was 0.24% (9/3717), consistent with prior findings. The NC group showed a lower rate of 0.19% (158/82630), which falls below previously reported values. This discrepancy can also due to not all pregnant women undergo NIPT. The incidence of SCA in the IVF group was slightly higher than in the NC group (0.24% vs 0.19%), aligning with prior findings.14 However, a retrospective Korean study found no correlation between conception method and the incidence of fetal SCA.25 Given the limited sample size and true positive cases in this and prior IVF studies, broader validation is still necessary. Theoretically, since the incidence of SCA marginally exceeds that of T21, the PPV for SCA should surpass that of T21. Nevertheless, the PPV of SCA in the NC group was lower than that of T21 in this study, which may be due to the fact that SCA includes various subtypes. Previous studies have shown that NIPT is more effective at detecting sex chromosome trisomies than monosomy,25,26 which is consistent with our findings (Supplementary Table S1). Our data confirm that both groups exhibit this characteristic. Furthermore, our results suggest that lower FFs may contribute to a higher rate of test failure in the IVF group, but their impact on the accuracy of successful tests may be limited. The results demonstrate that NIPT is an effective screening method in both IVF and NC pregnancies, consistent with prior findings.12,14,25,27,28 These results have significant implications for post-test counseling in both NC and IVF pregnancies. For example, a positive NIPT result for T21 suggests a minimum 50% probability of confirmed fetal aneuploidy.
However, it is too early to assess the performance of NIPT for SCA, as these syndromes are not easily identified clinically in the early stages, and long-term follow-up is necessary. A comparative analysis of the performance on T18, T13, and RAAs was not conducted due to insufficient data in the IVF group. In the NC group, the sensitivity, specificity, and PPV of T18 (100%, 99.97% and 41.67%, respectively) and T13 (100%, 99.96% and 20.51%, respectively) were in line with previous study.16 It’s worth noting that in pregnancies with high-risk of RAAs, the most common results were T7 (Supplementary Table S2), which is consistent with previous reports.29,30 Fourteen cases of true positives were CNVs rather than aneuploidy abnormalities. The PPV of the RAAs was 7.65% in the NC group, which is lower than that of T21. It has been reported that the PPV for rare autosomal trisomies (RATs) is low or cannot be calculated due to limited sample sizes, and the majority of RATs are mosaic trisomies, primarily confined to the placenta.31–33 In clinical practice, when receiving positive results of RAAs, appropriate genetic counseling should be provided. Although the PPV remains low, IPD or serial ultrasound monitoring of fetal growth should still be recommended.
Of the false positive cases in the NC group, 8 cases of pregnant women had peripheral blood chromosomes abnormalities (7 for sex chromosomes, 1 for chromosome), and the fetal karyotype and CMA of these cases were normal. Since approximately 80–90% of the free DNA detected by NIPT originates from maternal sources,34 NIPT was not applicable for pregnancies with peripheral blood chromosome abnormalities, these 8 cases were unknown of their karyotypes before undergoing NIPT. The necessity of conducting karyotype testing prior to NIPT from an economic perspective requires further discussion. Additionally, 2 cases of false negative T21 were identified in the NC group. One of false negative case (Z score: −0.85) identified by ultrasound signs and a subsequent amniocentesis with complete fetal T21. After the TOP procedure, cytogenetic analysis of the placenta revealed the presence of mosaicism. The second case (Z score: 1.81) was an obese pregnant woman, with body mass index 37.28. Obesity can lead to a dilution of the placental fraction of cfDNA in maternal blood.35 The FFs was 5.54% in this case, which is much lower than the median FFs. Furthermore, obesity can reduce the accuracy of ultrasound results, and no abnormal findings were identified in this case. The symptoms and signs were suspected to be T21 after birth, and a peripheral blood karyotype analysis was subsequently performed, confirming a complete T21. These cases highlight the importance of thorough and accurate pre-test counseling for the risks and limitations of NIPT.
Although NIPT offers many advantages in the IVF and NC populations, test failures are inevitable Test failure is a concern highlighted by the American College of Medical Genetics and Genomics.36 Both the failure rate after the first sequencing (2.31% vs 1.70%, p < 0.05) and the final failure rate (0.16% vs 0.04%, p < 0.05) in the IVF group were significantly higher than those in the NC group, which in line with the previous reports.14,37 The lower FF leads to a higher failure rate, which might be the result of associated impaired placentation during IVF pregnancies.37 The retesting success rates in these two groups were 93.02% (80/86) and 97.49% (1359/1394), respectively. It indicated that the majority of pregnancies that failed after initial sequencing yielded successful outcomes upon retesting, which aligns with the findings of previous studies.38,39
The reported failure rates for NIPT tests vary by assay technology, with methods based on MPS ranging from 0.1% to 1.58%.7,38,40 In the current study, the overall final failure rate was 0.05% (41/86388), which was within the low range. This may be due to different laboratories using different FF cut-offs. Although most previous studies have established a cut-off of 4% in their routine NIPT procedures,38,41 we opted to use a cut-off of 3%. A higher cut-off correlates with a higher failure rate. Additionally, it is important to consider the varying definitions of test failure. Some studies categorize administrative issues, such as sample collection errors, mislabeling, and transport problems, as test failures. Taneja et al observed that out of a total of 1.6% of cancellations, only 0.1% were attributed to technical reasons, with the majority being due to administrative issues (ie, the testing process did not commence).40 Problems related to inadequate blood volume, hemolysis, and mislabeling were not addressed in this study, which contributed to a low failure rate. Our research only involved a comparison of failure rates in two groups, and we did not conduct an in-depth analysis of the underlying reasons for failure. This is one of the limitations of our research.
In this study, the median FFs in the IVF pregnancies was significantly lower than that in the NC group (11.23% vs 12.05%, p < 0.001), which is consistent with the findings of previous study.42 An increased maternal inflammatory response and epithelial damage resulting from assisted reproductive technology treatment have been proposed as alternative explanations for the decreased FFs observed in women undergoing IVF, while the underlying mechanisms have not been clarified.22 Zhou et al indicated that the change in FFs during gestation was a plateau stage from the 10th to 19th weeks, followed by a rapid growth stage from the 19th to 30th weeks,43 which is consistent with our findings. Furthermore, the kinetics exhibited a similar trend in both groups, which indicating that the method of conception has no impact on the kinetics of FFs. However, the FFs were absent after the 27th week of IVF pregnancies and further investigation is required. Besides, follow-up data for NIPT-negative cases in both IVF and NC pregnancies were insufficient. Insurance coverage will be initiated for confirmed false negative cases involving T21, T18, or T13, specifically excluding CNVs associated with these chromosomes. Another limitation was the lack of stratification by treatment type within the IVF group. The extremely small number of positive cases also precluded meaningful performance evaluation of NIPT for T18, T13, and RAAs in this cohort. However, our findings suggest that undergoing IVF does not affect the performance of NIPT. Compared to all currently published research, this study represents the largest sample size of singleton pregnancies within the IVF group to date in studies on the application of NIPT in IVF. Furthermore, a comparative analysis of the detailed detection results of SCA, RAAs and FF kinetics between the two groups has not been performed in any prior studies. This study further demonstrates the utility of NIPT in IVF populations and provides evidence to inform clinical genetic counseling decisions.
Conclusions
NIPT exhibits high sensitivity and specificity for detecting T21 and SCA in both IVF and NC pregnancies, and its PPV for these conditions remains moderate in both groups. Furthermore, although the FFs in IVF pregnancies was lower than those in the NC group and the failure rate was higher in the IVF group, the kinetics of FFs exhibited similar trends in the two groups. Consequently, NIPT can be used to screening for common chromosomal aneuploidies in IVF singleton pregnancy with voluntary and fully informed consent.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. All procedures were reviewed and approved by the local ethics committee of Fujian Maternity and Child Health Hospital, China (Approval No. 2023KY108). Informed consent was obtained from all individual participants included in the study.
Acknowledgments
We thank all the patients and research workers for their participation.
Funding
This work was supported by the Startup Fund for scientific research, Fujian Medical University (Grant number: 2021QH1180 and 2024QH1208).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Luo Y, Hu B, Long Y, et al. Clinical application of noninvasive prenatal testing in twin pregnancies: a single-center experience. Expert Rev Mol Diagn. 2023;23(4):335–340. doi:10.1080/14737159.2023.2193291
2. Lanes A, Huang T, Sprague AE, et al. Maternal serum screening markers and nuchal translucency measurements in in vitro fertilization pregnancies: a systematic review. Fertil Steril. 2016;106(6):1463–1469.e1462. doi:10.1016/j.fertnstert.2016.07.1120
3. Bellver J, Casanova C, Garrido N, et al. Additive effect of factors related to assisted conception on the reduction of maternal serum pregnancy-associated plasma protein A concentrations and the increased false-positive rates in first-trimester Down syndrome screening. Fertil Steril. 2013;100(5):1314–1320. doi:10.1016/j.fertnstert.2013.06.045
4. Gjerris AC, Loft A, Pinborg A, Christiansen M, Tabor A. Prenatal testing among women pregnant after assisted reproductive techniques in Denmark 1995–2000: a national cohort study. Hum Reprod. 2008;23(7):1545–1552. doi:10.1093/humrep/den103
5. Lo YM, Corbetta N, Chamberlain PF, et al. Presence of fetal DNA in maternal plasma and serum. Lancet. 1997;350(9076):485–487. doi:10.1016/S0140-6736(97)02174-0
6. Baranova EE, Sagaydak OV, Galaktionova AM, et al. Whole genome non-invasive prenatal testing in prenatal screening algorithm: clinical experience from 12,700 pregnancies. BMC Pregnancy Childbirth. 2022;22(1):633. doi:10.1186/s12884-022-04966-8
7. Gil MM, Accurti V, Santacruz B, Plana MN, Nicolaides KH. Analysis of cell-free DNA in maternal blood in screening for aneuploidies: updated meta-analysis. Ultrasound Obstet Gynecol. 2017;50(3):302–314. doi:10.1002/uog.17484
8. Zhang H, Gao Y, Jiang F, et al. Non-invasive prenatal testing for trisomies 21, 18 and 13: clinical experience from 146,958 pregnancies. Ultrasound Obstet Gynecol. 2015;45(5):530–538. doi:10.1002/uog.14792
9. Sarno L, Revello R, Hanson E, Akolekar R, Nicolaides KH. Prospective first-trimester screening for trisomies by cell-free DNA testing of maternal blood in twin pregnancy. Ultrasound Obstet Gynecol. 2016;47(6):705–711. doi:10.1002/uog.15913
10. Cha W, Yun I, Nam CM, Nam JY, Park EC. Evaluation of assisted reproductive technology health insurance coverage for multiple pregnancies and births in Korea. JAMA Network Open. 2023;6(6):e2316696. doi:10.1001/jamanetworkopen.2023.16696
11. Hartwig TS, Ambye L, Sorensen S, Jorgensen FS. Discordant non-invasive prenatal testing (NIPT) - a systematic review. Prenat Diagn. 2017;37(6):527–539. doi:10.1002/pd.5049
12. Xiang L, Zhu J, Deng K, et al. Non-invasive prenatal testing for the detection of trisomies 21, 18, and 13 in pregnant women with various clinical indications: a multicenter observational study of 1,854,148 women in China. Prenat Diagn. 2023;43(8):1036–1043. doi:10.1002/pd.6312
13. Jin X, Xu Y, Ying X, et al. Clinical application of noninvasive prenatal testing for pregnant women with assisted reproductive pregnancy. Int J Womens Health. 2021;13:1167–1174. doi:10.2147/ijwh.S337249
14. Wei R, Li J, Xia Y, et al. Application of non-invasive prenatal testing to 91,280 spontaneous pregnancies and 3477 pregnancies conceived by in vitro fertilization. Mol Cytogenet. 2023;16(1):25. doi:10.1186/s13039-023-00656-y
15. He S, Zhang Q, Chen M, et al. Analysis of retest reliability for pregnant women undergoing cfDNA testing with a no-call result. Mol Biol Rep. 2023;50(9):7649–7657. doi:10.1007/s11033-023-08591-2
16. Zhang Y, Xu H, Zhang W, Liu K. Non-invasive prenatal testing for the detection of trisomy 13, 18, and 21 and sex chromosome aneuploidies in 68,763 cases. Front Genet. 2022;13:864076. doi:10.3389/fgene.2022.864076
17. Fosler L, Winters P, Jones KW, et al. Aneuploidy screening by non-invasive prenatal testing in twin pregnancy. Ultrasound Obstet Gynecol. 2017;49(4):470–477. doi:10.1002/uog.15964
18. La-Verde M, De-Falco L, Torella A, et al. Performance of cell-free DNA sequencing-based non-invasive prenatal testing: experience on 36,456 singleton and multiple pregnancies. BMC Med Genomics. 2021;14(1):93. doi:10.1186/s12920-021-00941-y
19. Baranov AA, Namazova-Baranova LS, Belyaeva IA, Bombardirova EP, Smirnov IE. Medical and social problems of assisted reproductive technologies from the perspective of pediatrics. Vestn Ross Akad Med Nauk. 2015;70(3):307–314. doi:10.15690/vramn.v70i3.1326
20. Costa JM, Letourneau A, Favre R, et al. Cell-free fetal DNA versus maternal serum screening for trisomy 21 in pregnant women with and without assisted reproduction technology: a prospective interventional study. Genet Med. 2018;20(11):1346–1353. doi:10.1038/gim.2018.4
21. Huang Z, Xiao F, Xiao H, et al. Comparison of genetic profiles of neonates in intensive care units conceived with or without assisted reproductive technology. JAMA Network Open. 2023;6(4):e236537. doi:10.1001/jamanetworkopen.2023.6537
22. Balaguer N, Mateu-Brull E, Gómez-López M, Simón C, Milán M. Cell-free fetal DNA testing performance and fetal fraction estimation are not affected in ART-conceived pregnancies. Hum Reprod. 2022;37(12):2743–2756. doi:10.1093/humrep/deac217
23. Ministry of Health of the People’s Republic of China. National stocktaking report on birth defect prevention. Ministry of Health of the People’s Republic of China; 2012. Available from: https://www.gov.cn/gzdt/att/att/site1/20120912/1c6f6506c7f811bacf9301.pdf.
24. Pieters JJPM, Kooper AJA, Van Kessel AG, Braat DDM, Smits APT. Incidental prenatal diagnosis of sex chromosome aneuploidies: health, behavior, and fertility. ISRN Obstet Gynecol. 2011;2011:1–10. doi:10.5402/2011/807106
25. Kim H, Park JE, Kang KM, et al. Clinical evaluation of noninvasive prenatal testing for sex chromosome aneuploidies in 9,176 Korean pregnant women: a single-center retrospective study. BMC Pregnancy Childbirth. 2024;24(1):93. doi:10.1186/s12884-024-06275-8
26. Luo X, Liu W, Hu L, et al. Prenatal diagnosis, pregnancy determination and follow up of sex chromosome aneuploidy screened by non-invasive prenatal testing from 122 453 unselected singleton pregnancies: a retrospective analysis of 7-year experience. Congenit Anom. 2024;64(3):99–106. doi:10.1111/cga.12558
27. Xu L, Huang H, Lin N, et al. Non-invasive cell-free fetal DNA testing for aneuploidy: multicenter study of 31 515 singleton pregnancies in southeastern China. Ultrasound Obstet Gynecol. 2020;55(2):242–247. doi:10.1002/uog.20416
28. Margiotti K, Cesta A, Dello Russo C, et al. Cell-free DNA screening for sex chromosomal aneuploidies in 9985 pregnancies: italian single experience. BMC Res Notes. 2020;13(1):167. doi:10.1186/s13104-020-05009-1
29. Chen Y, Wu X, Li H, Yin Y, Zhang Y. Evaluation of the prenatal diagnostic value of non-invasive prenatal testing for the detection of rare fetal autosomal trisomies: a single center study of 83,842 cases. Sci Rep. 2025;15(1):26254. doi:10.1038/s41598-025-09757-7
30. Dai P, Zhao G, Hu S, Liu N, Kong X. Prenatal diagnosis and pregnancy outcome of fetuses with rare autosomal trisomies indicated by non-invasive prenatal testing. Zhonghua Yi Xue Yi Chuan Xue Za Zhi. 2023;40(5):513–518. doi:10.3760/cma.j.cn511374-20211021-00838
31. Bedei I, Wolter A, Weber A, Signore F, Axt-Fliedner R. Chances and challenges of new genetic screening technologies (NIPT) in prenatal medicine from a clinical perspective: a narrative review. Genes. 2021;12(4):501. doi:10.3390/genes12040501
32. Zhang M, Tang J, Li J, et al. Value of noninvasive prenatal testing in the detection of rare fetal autosomal abnormalities. Eur J Obstet Gynecol Reprod Biol. 2023;284:5–11. doi:10.1016/j.ejogrb.2023.03.002
33. Harasim T, Neuhann T, Behnecke A, et al. Initial clinical experience with NIPT for rare autosomal aneuploidies and large copy number variations. J Clin Med. 2022;11(2):372. doi:10.3390/jcm11020372
34. Benn P, Cuckle H, Pergament E. Non‐invasive prenatal testing for aneuploidy: current status and future prospects. Ultrasound Obstet Gynecol. 2013;42(1):15–33. doi:10.1002/uog.12513
35. Prodan NC, Schmidt M, Hoopmann M, Abele H, Kagan KO. Obesity in prenatal medicine: a game changer? Arch Gynecol Obstet. 2023;309(3):961–974. doi:10.1007/s00404-023-07251-x
36. Gregg AR, Skotko BG, Benkendorf JL, et al. Noninvasive prenatal screening for fetal aneuploidy, 2016 update: a position statement of the American College of Medical Genetics and Genomics. Genet Med. 2016;18(10):1056–1065. doi:10.1038/gim.2016.97
37. Galeva S, Gil MM, Konstantinidou L, Akolekar R, Nicolaides KH. First-trimester screening for trisomies by cfDNA testing of maternal blood in singleton and twin pregnancies: factors affecting test failure. Ultrasound Obstet Gynecol. 2019;53(6):804–809. doi:10.1002/uog.20290
38. Zhang B, Zhou L, Feng C, Liu J, Yu B. More attention should be paid to pregnant women who fail non-invasive prenatal screening. Clin Biochem. 2021;96:33–37. doi:10.1016/j.clinbiochem.2021.07.004
39. Karlsson F, Ahola T, Dahlberg J, et al. Evaluation of repeat testing of a non-sequencing based NIPT test on a Finnish general-risk population. Acta Obstet Gynecol Scand. 2021;100(8):1497–1500. doi:10.1111/aogs.14125
40. Taneja PA, Snyder HL, De Feo E, et al. Noninvasive prenatal testing in the general obstetric population: clinical performance and counseling considerations in over 85 000 cases. Prenat Diagn. 2016;36(3):237–243. doi:10.1002/pd.4766
41. Chang J, Qi Q, Zhou X, et al. Factors associated with test failure in pregnant women undergoing cell-free DNA-based testing for fetal trisomy. J Med Screen. 2021;28(4):411–418. doi:10.1177/09691413211009940
42. Talbot AL, Ambye L, Hartwig TS, et al. Fetal fraction of cell-free DNA in pregnancies after fresh or frozen embryo transfer following assisted reproductive technologies. Hum Reprod. 2020;35(6):1267–1275. doi:10.1093/humrep/deaa110
43. Zhou Y, Wang Y, Addai FP, et al. Analysis of cell-free fetal DNA in 16,843 pregnant women from a single center in China using targeted sequencing approach. Placenta. 2022;122:18–22. doi:10.1016/j.placenta.2022.03.126
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.