Back to Journals » Journal of Pain Research » Volume 14
Clinical Application of Laser Speckle Flowgraphy to Assess Changes in Blood Flow to the Foot After a Lumbar Sympathetic Ganglion Block: A Case Report
Authors Kanao-Kanda M, Kanda H ![]() , Iida T, Kikuchi S
, Iida T, Kikuchi S ![]() , Azuma N
, Azuma N
Received 5 February 2021
Accepted for publication 19 May 2021
Published 26 May 2021 Volume 2021:14 Pages 1451—1456
DOI https://doi.org/10.2147/JPR.S305543
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Erika Petersen
Megumi Kanao-Kanda,1 Hirotsugu Kanda,1 Takafumi Iida,1 Shinsuke Kikuchi,2 Nobuyoshi Azuma2
1Department of Anesthesiology and Critical Care Medicine, Asahikawa Medical University, Asahikawa, Hokkaido, 078-8510, Japan; 2Department of Vascular Surgery, Asahikawa Medical University, Asahikawa, Hokkaido, 078-8510, Japan
Correspondence: Hirotsugu Kanda
Department of Anesthesiology and Critical Care Medicine, Asahikawa Medical University, Midorigaoka-higashi 2-1-1-1, Asahikawa, Hokkaido, 078-8510, Japan
Tel +81-166-68-2583
Fax +81-166-68-2589
Email [email protected]
Background: The lumbar sympathetic ganglion block (LSGB) has been used as a diagnostic and therapeutic procedure for treating pain conditions such as neuropathic and ischemia-related pain, affecting the lower extremities. In general, an increase in skin temperature is useful in confirming the effectiveness of the sympathetic nerve block in clinical settings. However, the assessment of skin temperature in patients with peripheral arterial disease (PAD) occasionally provides false negatives.
Case Presentation: A novel technology, laser speckle flowgraphy (LSFG) enables noninvasive quantitative and qualitative blood flow assessments. LSFG is a novel neuro-monitor for quantitative blood flow detection in the optic nerve head during cardiac surgery. Herein, we report on measuring foot blood flow using LSFG before and after LSGB in a PAD patient. This research aimed to determine whether LSFG could detect any improvement in the dynamics of foot blood flow after an LSGB in a situation where changes in skin temperature alone could not determine the procedure’s outcome.
Conclusion: LSFG can be used to assess blood flow changes in a foot with PAD, following a LSGB.
Keywords: laser speckle flowgraphy, lumbar sympathetic ganglion block, peripheral vascular disease
Introduction
The lumbar sympathetic ganglion block (LSGB) has been used as a diagnostic and therapeutic procedure for treating pain conditions such as neuropathic and ischemia-related pain, affecting the lower extremities. These types of pain are thought to be associated with the components of the sympathetic nervous system. In general, an increase in skin temperature is useful in confirming the effectiveness of the sympathetic nerve block in clinical settings.1 However, the assessment of skin temperature in patients with peripheral arterial disease (PAD) occasionally provides false negatives. The lack of temperature change in the lower extremities of these patients makes it difficult to confirm the effectiveness of the sympathetic block.
A novel technology, laser speckle flowgraphy (LSFG) enables noninvasive quantitative and qualitative blood flow assessments. LSFG is a novel neuro-monitor for the quantitative detection of blood flow in the optic nerve head during cardiac surgery.2–4 Recently, Kikuchi et al showed the utilization of LSFG in evaluating lower extremity blood flow during pre-and post-surgical revascularization in PAD patients.5
Herein, we report measuring foot blood flow using LSFG before and after LSGB in a PAD patient. This research aimed to determine whether LSFG could detect any improvement in the dynamics of foot blood flow after an LSGB in a situation where the outcome of the changes in skin temperature alone could not determine the procedure outcome.
Materials and Methods
Clinical Case Timeline
An 83-year-old woman was admitted to our hospital to evaluate pain in the dorsum of the left foot. Examination revealed that her left superficial femoral artery had narrowed, causing ischemic pain. She was diagnosed with PAD. Percutaneous transluminal angioplasty failed to alleviate the pain in her left foot.
One month later, an LSGB was scheduled in an attempt to reduce this pain. Just before the LSGB, skin temperature measurements were taken and LSFG was performed. The patient was placed in a right lateral position on the operating table Under fluoroscopic guidance, 22G needles were directed to the anterior disc surface of L2, L3 and L4, respectively, using a loss of resistance technique to guide the needles. After each needle was placed correctly, 2 mL of a one-to-one mixture of 1% lidocaine and radiographic dye was injected. After 20 minutes of the lidocaine infusion, the patient underwent a sensory test by cold ice touch and pinprick to confirm the absence of neurological abnormality in the lower extremity. To note, the patient’s pain in the dorsum of the left foot disappeared following lidocaine injection. Although pain relief was observed twenty minutes after LSGB, the skin temperature of the left foot remained unchanged, resulting in uncertainty about LSGB success.
The LSFG was performed immediately thereafter to assess the circulation dynamics of the left foot. An increase in blood flow was confirmed. Written, informed consent to publish this case report was obtained from the patient. Institutional approval was not required to publish the case details
Technical Details Related to Use of the LSFG Equipment
Kikuchi et al have previously described the LSFG device.5 As shown in Figure 1A, foot hemodynamics were determined by using the LSFG- PFI (Cat.No.P001-0JP, Softcare Co., Ltd., Fukuoka, Japan) to visualize the distribution of blood flow in a 20×15 cm target skin area on foot from a 25 cm working distance, and to generate a map with a resolution of 710 (width) × 480 (height) pixels. A near-real-time measurement was possible to complete the standard measurement and data analysis was 4 s and 10 s, respectively. An 830-nm diode laser beam, emitted from the camera unit, was applied to the surface of the entire foot, where it penetrated the dermis to a depth of 1 mm and was then scattered by flowing red blood cells. The imaging sensor in the camera unit captured the returning scattered light, and the resulting interference produced a moving laser speckle field. The moving speed of speckles detected at each pixel point in the image field was proportional to the average flow speed of the red blood cells passing each corresponding objective point. Blood cells moving faster than other cells created blurrier speckle patterns. The software from the device calculated an estimated mean blur rate (MBR), which indicated the blood flow, from the moving speckle image and created 2-D color-coded maps (Figure 1B). The MBR value represents signal strength related to heartbeats, a quantitative index of the relative blood flow velocity. MBR is a parameter widely used to observe retinal blood flow by ophthalmologists.6,7 The MBR maps were sequentially shown with 120 flame-shaped flows for 4 s on display. This enabled rapid detection of any change in blood flow. The software displayed a Heartbeat Map that included multiple blood flow maps, searched for heartbeats over 120 frames, and calculated an average pattern for a single heartbeat (Figure 1C). The blood flow in up to six regions of interest (ROIs) was investigated, and the results are shown in Figure 2B. The pulse waveforms in each area corresponded to distinct heartbeats and were compared by using LSFG, which then converted the signals to blood flow. No specific training was required to use this device.
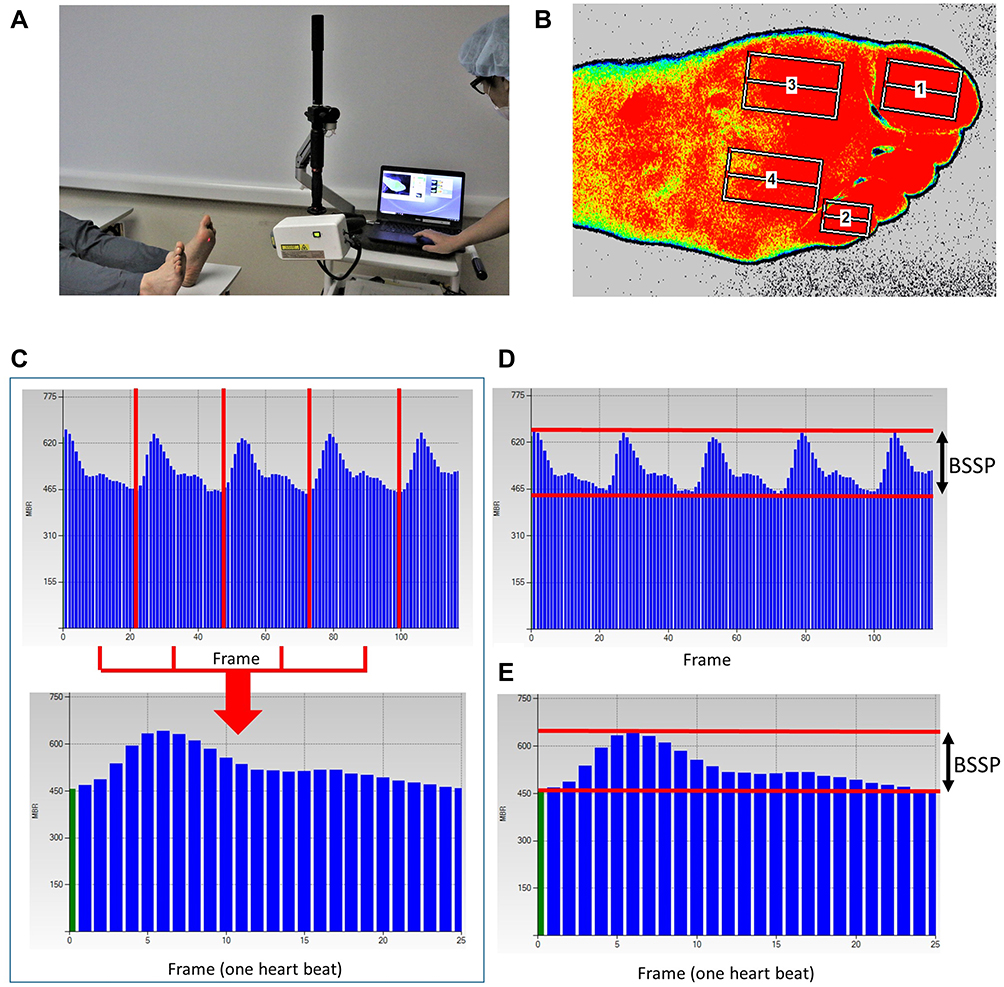 |
Figure 1 Method of laser speckle flowgraphy (LSFG) measurement. A photograph acquired by LSFG (A) and a 2-D color-coded map with the four regions of interest (B) showing the blood flow measurement in the feet of a healthy volunteer (without peripheral arterial disease). The pulse wave velocity (mean blur rate [MBR] on the y-axis) is shown before (top) and after (bottom) synchronization with 4.5 heartbeats in 4 s. The subject’s heart rate was 68 beats per minute. The four red lines separate the heartbeats, with each heartbeat represented by approximately 27 frames on the x-axis (C). The amplitude of the pulse wave is expressed as the beat strength of skin perfusion (BSSP) (D). A pulse wave for one heartbeat was synthesized and the mean BSSP was calculated (E). |
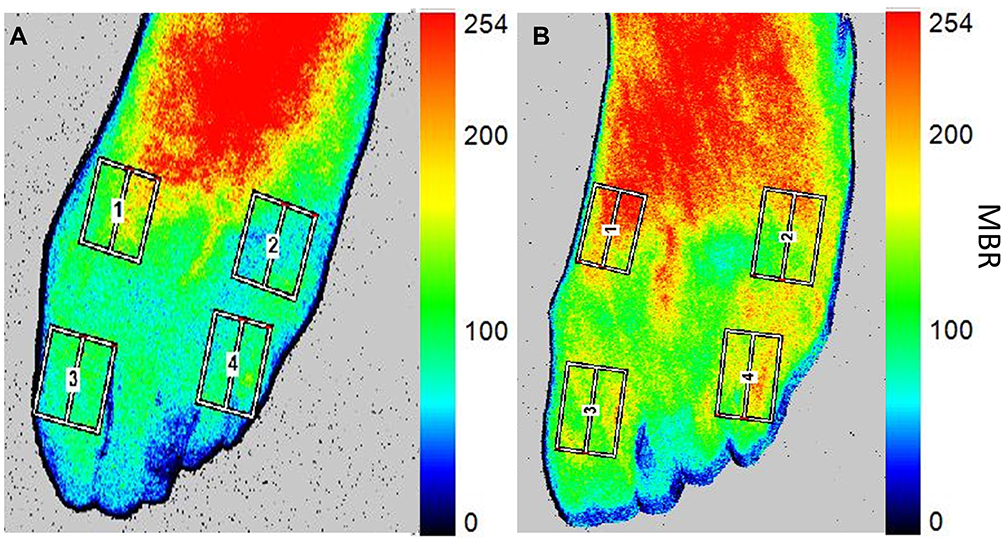 |
Figure 2 A 2-D colored mean blur rate (MBR) map for the four regions of interest examined in this case before (A) and after (B) lumbar sympathetic ganglion block (LSGB). The MBR map, which enabled qualitative analysis, shows increased blood flow after LSGB compared to baseline measurements. After the measurement, MBR was automatically calculated and shown in near-real-time on the y-axis in color, with high and low MBR levels indicated by red and blue, respectively. The numbers 1, 2, 3, and 4 indicate medial, lateral, first toe, and fifth toe areas on the dorsum, respectively. |
Beat strength of skin perfusion (BSSP) is a new parameter of blood flow, especially blood flow in the lower extremities that can be determined by LSFG. BSSP, according to the device manufacturer, shows the average amplitude of dynamic cutaneous blood flow change, synchronized to the heartbeat rhythm obtained from an ROI (Figure 1D). Since blood flow waves vary between cardiac cycles, the BSSP value is calculated from the mean amplitude of the blood flow (Figure 1E). The BSSP value is an indicator of signal strength that takes into account heartbeat signals conveyed to the cutaneous tissue of the foot. The BSSP value is a sensitive and reliable measure of the signal strength of heartbeats conveyed to the cutaneous tissue of the foot.
Measurement in Practice
In this case report, the LSFG assessment and skin temperature assessment on the left and right foot dorsum were performed before and after the LSGB (the lidocaine injection). LSFG was used to measure the pre-and-post-LSGB blood flow on the dorsal surface of the feet and at the first and fifth toes. The color-coded MBR map is shown in Figure 2.
Statistics
The mean BSSP was calculated from four areas of the foot: the first and fifth toes, and the medial and lateral points on the dorsal surface. BSSP values are reported as mean ± standard deviation. The difference in the mean BSSP between pre-and post-LSGB was evaluated using a paired t-test with the significance level set at p < 0.05.
Results
BSSP, a measure derived from MBR to assess blood flow at each point, was increased after the LSGB (Table 1). The skin temperature of both feet, however, was unchanged following the LSGB (Table 1).
 |
Table 1 Changes in BSSP for Each Area of the Foot and Changes in Foot Skin Temperature Before and After the LSGB |
Discussion
Several reports have shown the usefulness of LSGB in lower limb pain resulting from ischemia.8–10 LSGB has a direct vasodilating effect on blood vessels. In addition, LSGB blocks the sympathetic nerves that control the lower limbs, indirectly improves the circulation of the lower extremities, and relieves pain associated with sympathetic afferents. For these mechanisms, measuring changes in blood flow following LSGB is considered an effective method to determine the success of the block.
Conventional methods of assessing skin blood flow include determination of the ankle brachial index (ABI), skin perfusion pressure (SPP), and transcutaneous oximetry (TcPO2).4 However, patients who have foot pain are sometimes difficult to evaluate using these measurement methods. ABI and SPP cause pain in patients because they rely on devices that touch the skin directly. In addition, SSP requires 5 minutes per measurement. TcPO2, although non-invasive, has the disadvantage of long measurement times and variable results.
LSFG, on the other hand, is an excellent measurement tool that overcomes the disadvantages of conventional methods. LSFG is characterized by being contact-free, simple to use, requires extremely short measurement time (only 4 seconds), and has high reliability level. In this case report, the measurement of blood flow by SPP was not feasible due to the high degree of body movement by the patient caused by pain. The measurement using LSFG was fast and simple. Park et al reported that successful LSGB was considered to have occurred when changes in the ipsilateral temperature between pre-block and post-block time points were ≥ 2 °C.1 However, in this case report, LSFG immediately showed an improvement in blood flow after the LSGB, while there was no marked increase in the foot temperature.
In PAD patients with severe lower extremity pain, the sympathetic nervous system plays a dominant role, causing patients to experience excessive stress. As mentioned previously, LSGB improves blood flow by blocking the sympathetic nervous system and relieving pain. In this case report, the magnitude of skin temperature change was negligible compared to the degree of blood flow improvement. We speculate that the skin temperature of PAD patients, who already experience a decreased blood flow to the lower extremities due to the severe peripheral arterial stenosis, does not increase, even with an increase in blood flow due to the sympathetic nervous system blockade.
There are some limitations in this present case. The first is a change in blood flow possibility in the deep tissue of this patient. We believe that there is a link between skin blood flow and patient pain because LSFG detected an increase in skin blood flow after LSGB treatment and the pain disappeared. LSGB treatment may have caused an increase in skin blood flow on the lower extremities’ surface while altering deep blood flow. In this case, we did not evaluate whether deep blood flow increased, decreased, or remained unchanged. The second limitation is the patient’s skin temperature measurement timing. In this case, we only measured the patient’s skin temperature while in the operating room. The patient left the operating room within 1 hour after the LSGB was performed. In other words, the patient’s skin temperature may have risen one hour or more after the LSGB was performed. Therefore, although blood flow measurement using LSFG is superior to skin temperature measurement to grasp LSGB effect on lower extremity pain more quickly, it cannot be said that there is no increase in skin temperature. Further studies are required to discover the relationship between blood flow to the lower extremities and skin temperature in PAD patients.
Conclusions
Our case report demonstrates a novel clinical application of LSFG technology in its application of the technology to assess the blood flow changes in the foot following an LSGB. The increases in the mean BSSP assessed by LSFG are indicative of improved circulation in the feet. It could be used to determine the success of the LSGB procedure, even without an apparent change in foot temperature after LSGB. Because a lack of temperature change in the lower extremities is common in PAD patients following LSGB, this technology and its rapid results may indicate treatment success in this patient group. Therefore, LSFG may be a promising clinical tool to assess blood flow in patients with peripheral arterial disease. In addition, LSFG may be faster than changes in skin temperature to confirm LSGB success in these patients.
Acknowledgments
We want to thank Editage (www.editage.com) for English language editing services.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Park SY, Nahm FS, Kim YC, Lee SC, Sim SE, Lee SJ. The cut-off rate of skin temperature change to confirm successful lumbar sympathetic block. J Int Med Res. 2010;38(1):266–275. doi:10.1177/147323001003800131
2. Kanda H, Kunisawa T, Iida T, et al. Cerebral circulation during retrograde cerebral perfusion: evaluation using laser speckle flowgraphy. Ann Thorac Surg. 2019;107(6):1747–1752. doi:10.1016/j.athoracsur.2018.11.067
3. Kanda H, Kimura F, Iida T, et al. Combined use of intra-aortic balloon pump and venoarterial extracorporeal membrane oxygenation support with femoral arterial cannulation impairs cerebral microcirculation: evaluation with laser speckle flowgraphy. J Cardiothorac Vasc Anesth. 2017;31(3):1021–1024. doi:10.1053/j.jvca.2016.09.012
4. Kanda H, Kitahara H, Toyama Y, Kanao-Kanda M, Kunisawa T, Kamiya H. Intra-aortic balloon pump does not impede cerebral microcirculation during central extracorporeal membrane oxygenation support: evaluation with laser speckle flowgraphy. J Cardiothorac Vasc Anesth. 2017;31(4):e67–e68. doi:10.1053/j.jvca.2017.04.030
5. Kikuchi S, Miyake K, Tada Y, et al. Laser speckle flowgraphy can also be used to show dynamic changes in the blood flow of the skin of the foot after surgical revascularization. Vascular. 2019;27(3):242–251. doi:10.1177/1708538118810664
6. Sugiyama T. Basic technology and clinical applications of the updated model of laser speckle flowgraphy to ocular diseases. Photonics. 2014;1(3):220–234. doi:10.3390/photonics1030220
7. Shiba T, Takahashi M, Hori Y, Maeno T, Shirai K. Optic nerve head circulation determined by pulse wave analysis is significantly correlated with cardio ankle vascular index, left ventricular diastolic function, and age. J Atheroscler Thromb. 2012;19(11):999–1005. doi:10.5551/jat.13631
8. Cross FW, Cotton LT. Chemical lumbar sympathectomy for ischemic rest pain. A randomized, prospective controlled clinical trial. Am J Surg. 1985;150(3):341–345. doi:10.1016/0002-9610(85)90075-3
9. Tomlinson L. Case study to illustrate a multidisciplinary approach to a case of critical limb ischaemia and the role of chemical lumbar sympathectomy. J Tissue Viability. 2000;10(4):140–143. doi:10.1016/S0965-206X(00)80003-0
10. Alexander JP. Chemical lumbar sympathectomy in patients with severe lower limb ischaemia. Ulster Med J. 1994;63(2):137–143.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.