Back to Journals » Clinical Interventions in Aging » Volume 18
Clinical and Therapeutic Considerations for Older Adults with Head and Neck Cancer
Authors Dickstein DR ![]() , Powers AE, Vujovic D, Roof S, Bakst RL
, Powers AE, Vujovic D, Roof S, Bakst RL
Received 29 August 2022
Accepted for publication 4 March 2023
Published 17 March 2023 Volume 2023:18 Pages 409—422
DOI https://doi.org/10.2147/CIA.S366155
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Daniel R Dickstein,1,* Ann E Powers,2,* Dragan Vujovic,1 Scott Roof,2 Richard L Bakst1
1Department of Radiation Oncology, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 2Department of Otolaryngology, Icahn School of Medicine at Mount Sinai, New York, NY, USA
*These authors contributed equally to this work
Correspondence: Richard L Bakst, Icahn School of Medicine at Mount Sinai, 1184 5th Avenue 1st Fl, Box 1236, New York, NY, 10029, USA, Tel/Fax +1 212 241 3545, Email [email protected]
Abstract: Approximately 30% of patients with head and neck squamous cell carcinoma (HNSCC) are at least 70 years of age, and this percentage is expected to increase as the population increases and lives longer. Elderly patients are underrepresented in head and neck oncology clinical trials, and there is minimal evidence on the management of HNSCC for this population. Subsequently, despite their best intentions, physicians may unknowingly recommend an ill-suited course of therapy, which may result in suboptimal oncological or functional outcomes or adverse events. Surgical approaches have the potential to carry a higher risk of morbidity and mortality in older adults, especially in patients with multiple comorbidities. Definitive radiation therapy treatment in patients with HNSCC frequently involves 7 weeks of daily radiation, sometimes with concurrent chemotherapy, and this demanding treatment can be difficult for older adult patients, which may lead to treatment interruptions, potential removal of concurrent systemic therapy, compromised outcomes, and diminished quality of life. There are clinical trials currently underway investigating altered fractionation regimens and novel, less toxic systemic treatments in this population. This review provides an overview of how best to approach an older adult with HNSCC, from initial work-up to treatment selection.
Keywords: elderly, older adult, geriatric, head and neck squamous cell carcinoma, oropharynx, hypofractionation
Introduction
The global cancer burden is projected to increase in the elderly population, given increasing life expectancy and continued population growth. The head and neck squamous cell carcinoma (HNSCC) patient population is expected to mirror this global trend. HNSCC is the sixth most common malignancy worldwide, with approximately 30% of all patients diagnosed with HNSCC over the age of 70 years old.1–3 Between 2012 and 2016, the highest incidence of oral cavity and pharyngeal cancers was among those aged at least 70 years.4 Moreover, one of the most rapidly increasing populations with HNSCC is the human papillomavirus (HPV)-mediated HNSCC patient population, and while it is thought that this disease primarily affects a younger patient population, with initial diagnosis in the fifth or sixth decade of life, there are increasing numbers of elderly patients impacted by HPV-mediated HNSCC.5–8 Thus, a significant portion of the HNSCC population falls into the category of older adults or elderly people (age >70 years).
The elderly HNSCC population has grown significantly, but this demographic still represents <5% of enrolled participants in HNSCC clinical trials, as demonstrated in the MARCH-NC and MACH-NC meta-analyses.9–11 As such, the data extrapolated from HNSCC clinical trials, which inform clinical practice guidelines, may lack validity in older adults.
Concerns such as treatment-related toxicity may be more relevant for the elderly versus the broader patient population, given elderly people’s higher risk of this complication and their potential prioritization of quality of life over quantity of life.12 A multimodal approach to treating HNSCC is typical, often combining surgery, radiation therapy (RT), and systemic therapy with chemotherapy (and, in some circumstances, immunotherapy). Over the past several decades, there have been significant improvements in oncological outcomes, as well as the toxicity profile, with the aforementioned treatments. However, treatment-related side effects may diminish quality of life, with the most common implications affecting speech, swallowing, mastication, salivation, pain, and taste.
Side effects from HNSCC treatment are concerning for the elderly population, who are more likely to have other medical comorbidities. In addition, age-related physiological changes, including sarcopenia, decreased pulmonary function, cognitive changes, and reduced immune function, place elderly patients at risk for delayed recovery and adverse events. Acute and subacute side effects of HNSCC treatment include dermatitis, dysphagia, dysgeusia, mucositis, chronic pain, and xerostomia. Malnutrition and subsequent weight loss may result from side effects in the upper aerodigestive tract. In turn, this may lead to treatment interruptions and may require the use of a gastrostomy tube (G-tube) for short-term and potentially long-term nutritional sustenance. Cavities, trismus, osteoradionecrosis, and fibrosis are among the chronic side effects of RT or chemoradiotherapy (CRT).13,14 Despite the propensity of this patient population to develop treatment-related toxicity and morbidity, sufficient evidence-based guidelines for how to best treat older adults with HNSCC are not readily available.
There are numerous considerations that must be taken into account when determining an HNSCC treatment plan for an individual patient, including tumor-related factors such as subsite, stage, and histopathological features, and patient-related factors such as age, baseline functional status, and comorbidities. While some studies have demonstrated poorer tolerability of treatments such as chemotherapy in patients over the age of 70, it is unclear whether age is a confounder or a true independent risk factor. When determining a treatment plan for an older adult with HNSCC, it is important to recognize that older individuals represent a heterogeneous cohort and chronological age alone is often a poor surrogate for treatment-related outcomes. Patient age and functional status may have an impact on treatment planning; however, there is a gap in how to define standard therapy for the elderly demographic, given a lack of established guidelines for elderly HNSCC patient treatment.15 When making treatment recommendations, factors such as medical comorbidities, and functional and performance status must be taken into account.16–18
Treatment paradigms in HNSCC typically involve a surgical-based approach with adjuvant radiation or chemoradiation as necessary, or a non-surgical-based approach with radiation or chemoradiation. Surgery risks increase morbidity and mortality in elderly patients with significant comorbidities, which may yield an assessment of poor surgical candidacy. In addition, the ability to recover from surgery or the acute functional deficit caused by surgery may leave these patients with poorer outcomes. Non-surgical therapy typically involves definitive CRT over 7 weeks, which can be especially cumbersome on an older adult’s time, resources, and body, and result in treatment interruptions and worse outcomes.19 The elderly population has a higher risk of treatment interruptions, which are particularly concerning in patients with HNSCC, given that treatment interruptions have been associated with worse overall survival,19 but, interestingly, not with disease-specific outcomes.20–24 Thus, the etiology and impact of treatment interruptions in the elderly population is multifactorial and may serve as a substitute for other specific issues that contribute directly to poor outcomes.22,24–27
In order to optimize outcomes for this unique, albeit heterogeneous, population, comprehensive geriatric assessments (CGAs) are increasingly being used to assist with clinical decision making in elderly patients in most fields of medicine. However, there is still no formal recommendation for inclusion of these assessments in treating elderly HNSCC patients to help guide treatment. In addition, providers must acknowledge potential barriers to care by adequately assessing socioeconomic and psychosocial status, especially given the high rates of financial toxicity associated with HNSCC treatment for patients in the USA. Here, we review the clinical and therapeutic considerations for HNSCC treatment in elderly patients, highlighting key aspects of the work-up (geriatric assessments, medical comorbidities, barriers to care, polypharmacy, etc) and treatment.
Work-Up
Psychosocial and Socioeconomic Status
Psychosocial factors play an important role in head and neck cancer outcomes, and this is no exception for the elderly population. Specifically, socioeconomic status, insurance status, and race have been demonstrated to impact both treatments received and outcomes. A SEER-Medicare database study, published in 2021, found that socioeconomic status is a key prognosticator in older adults, and that Black, non-Hispanic older adults have worse HNSCC prognosis compared to older adults of other races and ethnicities.28 The authors postulate that this may be secondary to a lack of access and barriers to healthcare and prevention measures (eg smoking cessation resources). Another SEER-Medicaid study, assessing outcomes based on insurance status, found that uninsured patients and Medicaid patients are more likely to present with metastatic disease (adjusted odds ratio 1.60; p<0.001) and to have higher rates of head and neck cancer-related mortality, and are less likely to receive definitive therapy.29 HNSCC treatment is also associated with high rates of financial toxicity for patients residing in the USA,30 which can have significant implications, especially for elderly patients, who are more likely to be retired and without wages. A cross-sectional study of 104 HNSCC survivors found that up to 40% of patients experienced high financial toxicity and up to 60% of patients ultimately had to use savings and/or take out loans in order to help finance treatment. Patients at highest risk for financial toxicity were patients who were not married, had lower levels of education, and had primary tumors of the larynx/hypopharynx.31 While little is published on financial toxicity specifically in the elderly HNSCC population, it is an important to identify at risk patients and discuss potential financial toxicity concerns with patients and their caregivers.30
Medical Comorbidities
Medical comorbidities tend to be more common among elderly HNSCC patients, and some of these comorbidities may interfere with treatment tolerability and recovery. Assessments such as the Charlson Comorbidity Index (CCI), Adult Comorbidity Evaluation-27 (ACE-27), and Kaplan–Feinstein Comorbidity Index (KFI) are helpful in quantifying the implications of comorbid conditions on outcomes.32–34 While these tools were not specifically developed for cancer patients or the elderly population, they can be very informative and can be used to quantify the burden of comorbid conditions more accurately. The CCI is a predictor of 10-year survival and incorporates comorbidities such as neurological, cardiac, pulmonary, and gastrointestinal conditions into its scoring system. Reid et al demonstrated that overall comorbidity, quantified by the CCI, is an independent predictor of survival in elderly patients with HNSCC.35 Similarly, Datema et al showed that comorbidity is an independent prognostic factor and impacts both the short-term mortality of HNSCC patients and overall survival.36 It is worth noting that there are three neurological components/comorbidities included in the CCI: cerebrovascular accident (CVA), transient ischemic attack (TIA), and dementia. All three of these factors have the potential to lead to cognitive decline, but research is lacking into the potential effect on outcomes of cognitive impairment in older adult HNSCC populations. That considered, van Deudekom et al demonstrated that cognitive impairment in older HNSCC patients correlates with postoperative delirium in patients undergoing surgery.37 Still, the impact of cognitive delirium on non-surgical HNSCC therapy has been poorly studied to date.
In addition, sarcopenia, age-related involuntary loss of skeletal muscle mass and strength, has been shown to be an independent prognostic factor for elderly HNSCC patients and a predictor of chemotherapy dose-limiting toxicity.38–43 Depending on a patient’s comorbidities, patients may tolerate treatments differently. Thus, a patient’s comorbidities should be carefully evaluated before making treatment decisions to understand the risks and the patient’s ability to undergo treatment.
Medication Management
Polypharmacy, the simultaneous use of multiple medications, is common in the elderly population and may be another contributor to worse outcomes in this population. Polypharmacy is common in the USA and is an indirect measure of the medical comorbidity burden. Approximately 90% of elderly adults (age >65 years) take at least one prescription medication in a typical month, 66% take at least three medications, and 42% take at least five medications.44 A systematic review analyzing elderly cancer patients showed an association between polypharmacy and chemotherapy-induced toxicities in addition to postoperative complications.45 In addition, there are medications that may not be appropriate for elderly adults: the American Geriatrics Society (AGS) maintains the Beers Criteria medication list, which is a list of potentially inappropriate or harmful medications for older adults that should be avoided in the elderly population.46 Another systematic review and meta-analysis showed that potentially inappropriate medication use is associated with worse mortality in elderly patients.47 A retrospective study of elderly patients, defined as age greater than 70 years, with oropharyngeal squamous cell carcinoma (OPSCC) evaluated the effects of polypharmacy, potentially inappropriate medication use, and comorbidities, and found that a comorbidity–polypharmacy score, and not the comorbidity score alone, was associated with worse overall survival.48 These studies illustrate that is essential to consider potential medication interactions and minimizing polypharmacy when appropriate in elderly patients with HNSCC and to educate patients and/or caregivers accordingly.
Geriatric Assessments
It is essential to consider an older adult patient’s functional status and social support network during the initial work-up. Patient age, medical comorbidities, and functional status may affect treatment planning, as well as the patient’s priorities and goals of care. Several methods have emerged to systematically assess frailty and functional status to identify which patients are at increased risk for adverse outcomes, including the CGA and Geriatric 8 (G8).49–53 The CGA is a very thorough assessment developed by the International Society of Geriatric Oncology (SIOG), and can be impractical to complete in the clinical setting, potentially limiting its use.54 Since publication of the CGA, subsequent abbreviated versions of this survey, such as the G8 questionnaire, have been efficacious in predicting the survival of elderly cancer patients.49,55 The G8 panel incorporates eight items, comprising food intake, weight loss, mobility, neurological and psychological problems, body mass index (BMI), polypharmacy, self-reported health status, and age. The G8 is accurate in risk stratifying overall survival and quality-adjusted survival for elderly patients with HNSCC, and can accurately identify vulnerable patients who may have lengthened postoperative courses and prematurely terminated radiotherapy courses.56,57 In addition to geriatric assessments, there are predictive algorithms that can be incorporated to estimate treatment risks or identify patients at risk for treatment-related adverse effects. For example, the Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) is a scoring system that identifies patients at risk for chemotherapy-related side effects.58 Risk assessments, such as CRASH and other geriatric assessments, should be incorporated to help guide HNSCC management in this special population. A more aggressive, standard therapy may be selected for a fit older adult and a less aggressive treatment may be more appropriate for a more frail older adult. A prospective trial evaluating the use of geriatric assessment for HNSCC, utilizing the G8 screening tool and CGA to guide treatment planning, found that after the use of a geriatric assessment, the proposed therapy changed from what the physician was originally going to recommend in 12% of patients. The researchers also found that specific supportive needs, including nutritional, psychological, and chronic medication support, were altered after the use of the geriatric assessment. This study placed patients with locally advanced HNSCC into one of three categories: fit, vulnerable, and frail, as defined by the assessments.59 Despite emerging evidence regarding the utility of the CGA, assessments currently do not seem to be routinely incorporated in routine practice. In a survey study published in 2020, only 10% of the HNSCC radiation oncologists in Italy stated that they performed a CGA in older adult patients.60
In addition to geriatric assessments, there are several predictive models to calculate probabilities of cancer-related events. The Generalized Competing Event (GCE) model is a way of risk-stratifying patients by weighing the relative hazard of cancer- and non-cancer-related events.61–66 The GCE is also known as the omega (ω) score, and is a ratio that was developed for all cancer patients. The ratio is a proportion of the risk of cancer recurrence to non-cancer mortality, such that the closer the ratio is to 1, the higher the risk of cancer progression relative to mortality from other causes, while a value closer to 0 designates a higher likelihood of mortality from other causes. Variables incorporated in the GCE model include age, Eastern Cooperative Oncology Group (ECOG) status, BMI, primary tumor site, N stage, and p16 status. This model has been validated in patients with locally advanced HNSCC in the Meta-Analysis of Radiotherapy in HNSCC (MARCH)11,67 and Meta-Analysis of Chemotherapy in HNSCC (MACH-NC) studies.9,11 Furthermore, the GCE has been validated in a SEER database cohort study especially for elderly patients with HNSCC, which showed that this model is a more reliable way to risk stratify elderly patients and risk of HNSCC-related mortality than other existing models.62 Table 1 and an online, open-access nomogram tool68 outline the numerous predictive tools available, including GCE, G8, CCI, Cancer and Aging Research Group (CARG), ACE-27, and the Cumulative Illness Rating Scale – Geriatric (CIRS-G). These resources are referenced and utilized in an ongoing clinical trial (NCT: 03258554: Radiation Therapy With Durvalumab or Cetuximab in Treating Patients with Stage III–IVB Head and Neck Cancer Who Cannot Take Cisplatin), which investigates the efficacy of durvalumab or cetuximab in patients with HNSCC unable to tolerate cisplatin, which includes many elderly patients.65
 |
Table 1 Validated Assessments and Nomograms That Are Available to Guide Treatment Planning and Predict Treatment-Related Toxicity and Help Guide Clinicians in Informing Patients on Their Specific Expected Disease Course and Treatment Course |
Developing a standard comprehensive assessment tool for HNSCC patients would be beneficial to personalize care for this population. Predictive nomograms specific to elderly patients with HNSCC are continuing to be developed and refined. One example is a predictive nomogram specific to elderly patients with HNSCC that was developed using data from 284 patients at least 65 years of age, which incorporated Karnofsky Performance Status (KPS), CCI, and baseline serum CRP, published in 2021. Long-term data are needed, but this predictive nomogram has the potential to help guide treatment decisions for the elderly population in the future.69 In 2022, Zhou et al published a predictive nomogram utilizing different clinical variables, including BMI, nodal status, hemoglobin level, and neutrophil–lymphocyte ratio (NLR), to prognosticate elderly patients with oral cavity squamous cell carcinoma (OCSCC), with the intention of specifically guiding treatment for elderly patients.70 A similar model developed by another group, using retrospective data from 583 patients and including variables such as EBV viral load, tumor and nodal stage, and albumin level, was created to characterize elderly patients with nasopharyngeal SCC.71 The aforementioned predictive models are limited given that they have yet to be validated in the prospective setting; however, these predictive nomograms offer useful information and can serve as a guide for clinical discussions with elderly patients. An assessment of frailty in tandem with relevant biomarkers, not just chronological age, should be conducted for elderly patients with HNSCC in the future. Table 1 lists the most commonly referenced assessment nomograms currently in use.
Treatment
Surgical Management
Surgical outcomes of HNSCC have significantly improved, especially with regard to the functional morbidity associated with the surgery for HNSCC patients. This has been enhanced by a critical appraisal and review of surgeons’ functional outcomes, as well as the use of more advanced surgical techniques, such as the use of free flap reconstruction and minimally invasive techniques such as transoral robotic surgery (TORS) and transoral laser microsurgery (TLM). Surgery can still carry significant risks, despite the substantial advances in surgical techniques, improvements in perioperative care, and anesthesia.72 Data on postoperative complications in elderly patients with HNSCC are heterogeneous and contradictory, with some studies reporting increased risks associated with surgery for HNSCC in the elderly population based on age alone,73,74 and others demonstrating that frailty, higher rate of pre-existing comorbidities, advanced tumor stage, surgery time, poor G8 score, and smoking are correlated with perioperative complications independent of age.75–82 Free flap reconstructive surgery has become the standard of care for larger ablative defects to restore form and function. Despite being associated with longer operative times, studies have demonstrated that elderly patients (even in patients ≥90 years of age) who undergo free flap reconstruction experience similar outcomes to their younger counterparts; however, elderly patients are more likely to have longer hospital stays and longer length of intensive care unit stays when treated at lower volume head and neck cancer centers.83–86 Similarly to free flap reconstruction, TORS is generally well tolerated in the elderly population, with the exception of elderly patients with severe comorbidity, as demonstrated in a multi-institutional retrospective review of patients greater than 70 years of age with HPV-positive OPSCC.87 Similarly to TORS, TLM for early-stage laryngeal surgery has been shown to be safe and effective in patients with laryngeal cancer, regardless of age.88,89 Surgical options for early-stage laryngeal cancer include TLM and partial laryngectomy; however, despite similar overall survival rates between the two surgical options, TLM is favored given the improved functional outcomes.90–92 Minimally invasive and major head and neck surgeries have been shown to be generally well tolerated in the elderly population.
Radiation Therapy
A main trend in HNSCC RT is de-escalation therapy, which involves minimizing any of the following variables: radiation target volumes, fractions, and/or dosage, in order to minimize treatment toxicity. De-escalation trials have not been thoroughly studied in the HNSCC elderly population. Hypofractionation is a salient component of de-escalation therapy, and involves reducing total dosage by reducing the number of fractions. Hypofractionation is critical to study given that standard regimens of RT for HNSCC can cause significant toxicity. Active areas of HNSCC de-escalation research involve investigating radiation dose reduction in HNSCC to better delineate the balance between treatment efficacy and minimizing toxicity. Alternative fractionation regimens and hypofractionation are based on foundational research by Withers et al, which determined that there is a relationship between radiation treatment time and total dose needed for adequate tumor control in patients with HNSCC. This sentinel study demonstrated that a greater dose of radiation is needed to achieve the same tumor control after 4 weeks of radiation given because of tumor repopulation. This study provided proof of concept for alternative fractionation regimens for HNSCC treatment.93 Radiobiological modeling has demonstrated that 3 Gy per fraction or accelerated hyperfractionation (1.8 Gy given twice daily) is effective in achieving tumor control for HNSCC patients and was determined to reduce late effects compared to the standard 2 Gy per fraction standard of care regimen.94 Hypofractionation with curative intent in patients with HNSCC is a new and emerging area of research, and the elderly population is an ideal cohort set to benefit from this area of research.
Hypofractionation, shortening total treatment time, and decreasing total dose have been shown to decrease malignancy-associated burden in the palliative care setting; however, the primary objectives of several studies involved assessing for improvement in symptoms rather than local disease control.95–101 During the COVID-19 pandemic, the American Society of Radiation Oncology and European Society of Radiation Oncology released a statement promoting a hypofractionated treatment regimen for appropriate patients with HNSCC.102
There are a small series of published studies assessing the efficacy of hypofractionation specifically in the older adult HNSCC population. One such example is a study conducted by Ortholan et al investigating a split-course, hypofractionated plan in elderly and vulnerable populations with HNSCC (the ELAN study), which is one of the first prospective trials designed specifically for elderly patients. In this study, patients are stratified into one of three arms based on fitness, using different geriatric assessments, and disease stage: unfit non-metastatic, fit metastatic, and unfit metastatic disease. Unfit patients with non-metastatic HNSCC receive a hypofractionated split course of 30 Gy in 10 fractions over the course of 2 weeks followed by a 2-week break, subsequently followed by 25 Gy in 10 fractions for a total of 6 weeks. This study aims to show that split-course therapy may achieve good local control tumor response rates at 6 months for those patients who are unfit to tolerate continuous therapy, and may be better tolerated, with decreased side effects.103 Appropriate patient selection is critical, given that split-course therapy carries the potential risk of rapid repopulation typical for head and neck cancers after 4 weeks of treatment initiation.104 It is worth noting that a split course in combination with hypofractionation may cause more long-term side effects, and further studies are needed to determine the long-term effects of hypofractionation regimens in the elderly population.105
Our institution treats a high volume of HNSCC patients, and our experience with unfit, frail, elderly patients is consistent with the published literature in terms of challenges in receiving treatment.105–107 For elderly patients with HNSCC who cannot or do not want to receive standard RT, a new hypofractionation regimen is being investigated, with shortening of adjuvant and definitive standard treatment regimens. The study aims to evaluate the efficacy of hypofractionated RT without chemotherapy with curative intent in elderly patients with HNSCC. Inclusion criteria for the definitive arm include patients unfit for standard of care, and the adjuvant arm includes patients with adverse features on pathology following definitive resection. Patients with HNSCC at least 70 years old and at least ECOG grade 1 can be enrolled to receive definitive RT (45 Gy in 15 fractions over 3 weeks) or adjuvant RT (40.5 Gy in 15 fractions over 3 weeks). Similarly to Ortholan et al, the primary endpoint of our study is locoregional control at 6 months (NCT04284540: Hypofractionated Radiotherapy in Elderly Patients With Head and Neck Squamous Cell Carcinoma). Our investigators hypothesize that this hypofractionated regimen will significantly improve treatment tolerance, with no change in disease control efficacy at 6 months.108,109
There are conflicting data regarding RT-related toxicity in the elderly population, with studies reporting either increased or similar RT-induced toxicity in elderly patients compared to a younger cohort;10,19,110–112 however, the association between increased RT toxicity and the addition of chemotherapy in the elderly population is well established.10,110 A review of Radiation Therapy Oncology Group (RTOG) CRT trials for HNSCC demonstrated significantly higher rates of severe late toxicity (defined as chronic grade 3+ pharyngeal/laryngeal toxicity and/or requirement for a feeding tube ≥2 years after registration and/or potential treatment-related death within 3 years) in the elderly cohort.111 A retrospective study of HNSCC patients compared elderly patients, 70 years of age or older, with a younger cohort who underwent surgery followed by adjuvant CRT, and determined that chronic nephrotoxicity was the only toxicity that was significantly increased in the elderly cohort.112 A retrospective study assessing patients greater than or equal to 70 years of age with HNSCC treated with curative intent demonstrated that comorbidity (measured with the CCI) did not predict treatment toxicity; however, there was a higher G-tube placement than expected (24% prophylactic and 18% reactive), which is consistent with other studies suggesting that G-tubes are more frequently placed in older adult patients with HNSCC.19,113 Treatment-related toxicity can be a barrier for novel hypofractionation regimens. De Felice et al published a trial investigating a hypofractionated RT course treating with 60 Gy over 4 weeks (3 Gy/fraction) with concurrent cetuximab (400 mg/m2 given a week before radiation followed by 250 mg/m2 during treatment), with a primary endpoint of partial or complete objective response at 3 months. The median age was 77.5 years and the trial included only six patients in total owing to premature closure from treatment-related toxicity. These toxicities included grade 3+ oral mucositis, acneiform eruption, dermatitis, and nausea.114 All patients completed the radiation schedule; however, only two of the patients successfully completed the concurrent cetuximab course. A partial response was observed in three patients, the remaining three patients had progressive disease, and none of the patients had a complete response. Providers should be cautious when considering hypofractionation regimens in combination with radiosensitizing chemotherapy.
Systemic Therapy
Numerous studies have raised concerns about the use of chemotherapeutics in elderly patients with HNSCC, as chemotherapy can incur severe toxicities that outweigh its benefits in tumor control. Special considerations need to be made when treating the elderly population, as several physiological differences differentiate them from the younger adult population, which has the potential to alter the response to systemic chemotherapeutics. For example, older patients often have reduced glomerular filtration rate (GFR) and hepatic metabolism, which can affect the distribution of chemotherapeutics.115 In addition, polypharmacy and potentially inappropriate medications are an ongoing area of concern in the elderly population and could potentially interfere with systemic therapy.116
The benefit of chemotherapy in the treatment of HNSCC has been well established, with the most benefit seen with concomitant chemotherapy as opposed to induction, adjuvant, or neoadjuvant chemotherapy.9,117,118 It is worth noting that the efficacy of chemotherapy appears to decline with increasing age.119 The 2009 MACH-NC patient-based meta-analysis of 16,485 patients found that patients older than 70 years of age received no significant survival benefit in 5 years with the addition of chemotherapy; this was in stark contrast to the younger cohort, which experienced a 4.5% 5-year survival benefit.9 The updated 2021 MACH-NC large study with 18,951 patients reinforced this notion of decreasing efficacy of concomitant chemotherapy with increasing age and cautioned providers to carefully consider the use of systemic therapy in the elderly HNSCC population.120 Other studies have similarly reported on the toxicity and drawbacks of chemotherapeutics in the elderly HNSCC population. A subset analysis of three RTOG trials with 230 patients reported a significant correlation of older age with severe late toxicity from CRT.111 A retrospective study of 4042 patients aged 71 years or older from the National Cancer Data Base (NCDB) directly disputed the claims from the 2009 MACH-NC study; specifically, they found a 5-year survival difference of 8% with CRT from propensity score matching for older adults with HNSCC. While not all cohorts in their study experienced a longer median overall survival, they found that patients aged greater than 70 years with a low Charlson–Deyo comorbidity score and T1–2/N2–3 or T3–4/N0–3 disease had a significantly longer median overall survival with CRT compared to RT alone. The authors speculated that the MACH-NC study did not find a longer median overall survival with CRT compared to RT alone since only 4% of their population were in the over-70 age category, which limited the statistical power.121 These results were supported by another review of patients from the NCDB, which found increased systemic chemotherapy use in elderly patients from 2004 to 2012 and noted that it was significantly associated with improved overall survival in a multivariate model.122 Furthering this controversy, there is no consensus regarding the optimal systemic treatment regimen for older adults with HNSCC. Cisplatin is the standard cytotoxic agent that has been used for decades to treat a wide spectrum of malignancies, including HNSCC, and has been shown to be effective for older adults if they are able to tolerate it.123–125 The regimen of cisplatin and 5-fluorouracil has been widely used as therapy in older adults with HNSCC; however, owing to the toxicity of cisplatin and the advent of more targeted biologics, such as the epidermal growth factor receptor (EGFR) inhibitor cetuximab, there is ongoing debate on the optimal systemic therapy in this patient population.
Even though the immune system wanes with increasing age, immunotherapy appears to be efficacious in the older adult population; however, it is worth noting that the elderly population has been excluded from many immunotherapy trials.126–131 Currently, there are conflicting data in the literature regarding immunotherapy toxicity in the elderly population – some studies report similar rates of toxicities between older and younger patients and others report higher rates of toxicity in the older adult cohort.132,133 A trial published in 2021, assessing single-modality immunotherapy and immunotherapy combination therapy in the HNSCC population (average age of 60 years), demonstrated immunotherapy to be well tolerated, with approximately 15% of patients experiencing serious treatment-related adverse events.134 To date, no specific study has been conducted assessing immunotherapy toxicity rates specifically in the elderly HNSCC population.
Both RT and chemotherapy, notably cisplatin, can cause permanent sensorineural hearing loss (SNHL), principally by causing degeneration of outer hair cells in the organ of Corti.135–137 This has major implications for older adults, who are more likely to have presbycusis at baseline, and can negatively affect quality of life. RT-induced ototoxicity is directly proportional to the radiation dose (typically >45 cGy) and type of radiation, while cisplatin-induced ototoxicity is related to both dose and schedule.138–140 It is worth noting that the ototoxic radiation dose in patients undergoing concomitant chemotherapy with cisplatin is lowered.141 There is a validated predictive nomogram for assessing who is at highest risk for developing HNSCC treatment-related SNHL, with high sensitivity and specificity, 80% and 75%, respectively,142,143 and at-risk patients should be counseled accordingly.
Conclusion
How to best treat HNSCC in the older adult population varies depending on several factors, including subsite, comorbidities, performance status, frailty, and social support. There is no established standard of care specifically for older adults with HNSCC. Figure 1 demonstrates a proposed work flow for the therapeutic considerations for elderly patients with HNSCC. To determine the best treatment approach for older adult patients with HNSCC, it is strongly recommended to administer a geriatric assessment (paying special attention to medical comorbidities, socioeconomic status, psychosocial status, and polypharmacy) in combination with a predictive treatment nomogram to help predict treatment toxicity. Geriatric assessments and the involvement of a geriatrician in multidisciplinary care will afford the patient more accurate information and enable them to make the most informed decision regarding their treatment plan. Treatment modalities for HNSCC may involve monotherapy or multimodal therapy, and include surgery, RT, chemotherapy, and, in some instances, immunotherapy. Surgical considerations for older adults center around anesthetic risk. Elderly patients tend to tolerate major HNSCC reconstructive surgery generally well; however, they may have longer hospital stays compared to younger patients. RT and chemotherapy are often used in combination and can lead to treatment-related toxicity. Hypofractionated trials and de-escalation therapy, especially for HPV-positive OPSCC, are currently being investigated to minimize treatment-related toxicity and increase quality of life while maximizing treatment efficacy. As new studies are being developed, the elderly HNSCC population is the ideal group to benefit from these initiatives.
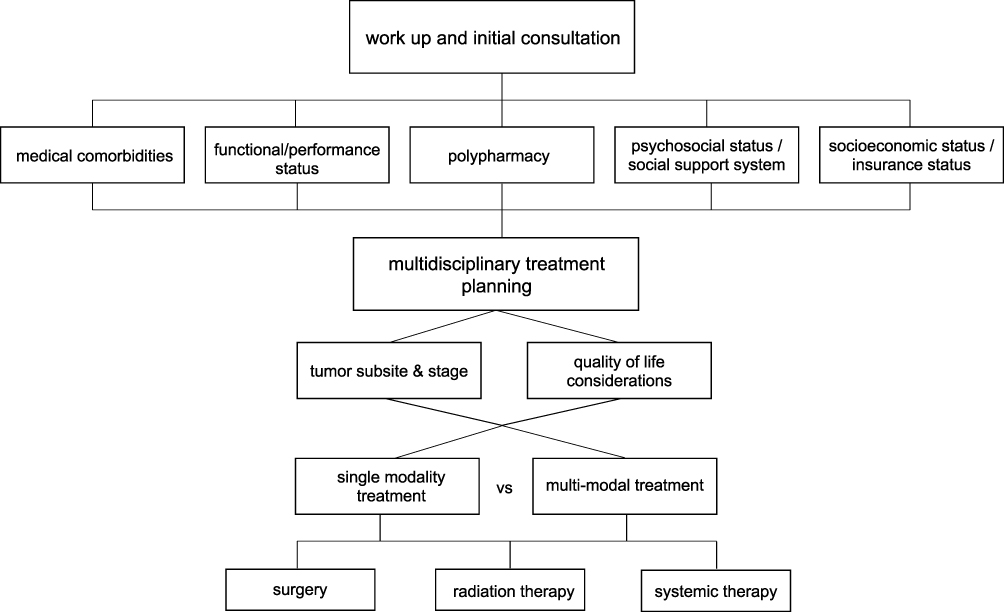 |
Figure 1 Proposed work flow for therapeutic considerations for elderly patients with HNSCC. |
It is essential to optimize treatment for the elderly population, which is particularly vulnerable to treatment-related toxicity. This review should serve to guide clinical decision making for elderly patients with HNSCC. In addition, this review emphasizes that clinical considerations and treatment decisions for older adults with HNSCC should be approached holistically and go beyond chronological age alone.
Abbreviations
HNSCC, head and neck squamous cell carcinoma, RT, radiation therapy, CRT, chemoradiotherapy, CGA, comprehensive geriatric assessment, G8, geriatric 8, SIOG, society of geriatric oncology, CRASH, chemotherapy risk assessment scale for high age patients, GCE, generalized competing event, MARCH, meta-analysis of radiotherapy in HNSCC, CCI, Charleston comorbidity index, KFI, Kaplan Feinstein comorbidity index, ACE-27, adult comorbidity evaluation-27, AGS, American geriatrics society, TORS, transoral robotic surgery, TLM, transoral laser microsurgery, ECOG performance status, Eastern Cooperative Oncology Group performance status, CD, Charlson-deyo index, 5FU, 5-fluorouracil, SNHL, sensorineural hearing loss, OCSS, oral cavity squamous cell carcinoma.
Acknowledgments
The authors would like to express deep gratitude to Lynda Rath for her enthusiastic assistance in clinical research and data management related to older adults at our institution. Daniel R Dickstein and Ann E Powers are co-first authors for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ferlay J, Colombet M, Soerjomataram I, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2019;144(8):1941–1953. doi:10.1002/ijc.31937
2. Sikora AG, Toniolo P, DeLacure MD. The changing demographics of head and neck squamous cell carcinoma in the United States. Laryngoscope. 2004;114(11):1915–1923. doi:10.1097/01.mlg.0000147920.66486.bc
3. Hankey BF, Ries LA, Edwards BK. Surveillence, Epidemiology, and End Results Program. N.C. Institute; 2017.
4. Howlader N. SEER Cancer Statistics Review, 1975–2016. Bethesda, MD: National Cancer Institute; 2019.
5. Gillison ML, Broutian T, Pickard RKL, et al. Prevalence of oral HPV infection in the United States, 2009–2010. JAMA. 2012;307(7):693–703. doi:10.1001/jama.2012.101
6. Zumsteg ZS, Cook-Wiens G, Yoshida E, et al. Incidence of oropharyngeal cancer among elderly patients in the United States. JAMA Oncol. 2016;2(12):1617–1623. doi:10.1001/jamaoncol.2016.1804
7. Windon MJ, D’Souza G, Rettig EM, et al. Increasing prevalence of human papillomavirus-positive oropharyngeal cancers among older adults. Cancer. 2018;124(14):2993–2999. doi:10.1002/cncr.31385
8. Rettig EM, Fakhry C, Khararjian A, et al. Age profile of patients with oropharyngeal squamous cell carcinoma. JAMA Otolaryngol Head Neck Surg. 2018;144(6):538–539. doi:10.1001/jamaoto.2018.0310
9. Pignon JP, Maître AL, Maillard E, et al. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): an update on 93 randomised trials and 17,346 patients. Radiother Oncol. 2009;92(1):4–14. doi:10.1016/j.radonc.2009.04.014
10. VanderWalde NA, Fleming M, Weiss J, et al. Treatment of older patients with head and neck cancer: a review. Oncologist. 2013;18(5):568–578. doi:10.1634/theoncologist.2012-0427
11. Lacas B, Bourhis J, Overgaard J, et al. Role of radiotherapy fractionation in head and neck cancers (MARCH): an updated meta-analysis. Lancet Oncol. 2017;18(9):1221–1237. doi:10.1016/S1470-2045(17)30458-8
12. Windon MJ, D’Souza G, Faraji F, et al. Priorities, concerns, and regret among patients with head and neck cancer. Cancer. 2019;125(8):1281–1289. doi:10.1002/cncr.31920
13. Haehl E, Rühle A, David H, et al. Radiotherapy for geriatric head-and-neck cancer patients: what is the value of standard treatment in the elderly? Radiat Oncol. 2020;15(1):31. doi:10.1186/s13014-020-1481-z
14. Tobias JS, Monson K, Gupta N, et al. Chemoradiotherapy for locally advanced head and neck cancer: 10-year follow-up of the UK Head and Neck (UKHAN1) trial. Lancet Oncol. 2010;11(1):66–74. doi:10.1016/S1470-2045(09)70306-7
15. Szturz P, Vermorken JB. Treatment of elderly patients with squamous cell carcinoma of the head and neck. Front Oncol. 2016;6:199. doi:10.3389/fonc.2016.00199
16. Coca‐Pelaz A, Halmos GB, Strojan P, et al. The role of age in treatment-related adverse events in patients with head and neck cancer: a systematic review. Head Neck. 2019;41(7):2410–2429. doi:10.1002/hed.25696
17. Rim CH, Yoon WS, Lee JA, et al. Factors predicting intolerance to definitive conventional radiotherapy in geriatric patients. Strahlenther Onkol. 2018;194(10):894–903. doi:10.1007/s00066-018-1318-y
18. Mady LJ, Baddour K, Hodges JC, et al. The impact of frailty on mortality in non-surgical head and neck cancer treatment: shifting the clinical paradigm. Oral Oncol. 2022;126:105766. doi:10.1016/j.oraloncology.2022.105766
19. Dickstein DR, Egerman M, Monrose E, et al. Treatment tolerability and outcomes in elderly patients with head and neck cancer. Head Neck. 2021;43(3):858–873. doi:10.1002/hed.26548
20. Bese NS, Hendry J, Jeremic B. Effects of prolongation of overall treatment time due to unplanned interruptions during radiotherapy of different tumor sites and practical methods for compensation. Int J Radiat Oncol Biol Phys. 2007;68(3):654–661. doi:10.1016/j.ijrobp.2007.03.010
21. Patel UA, Thakkar KH, Holloway N. Patient compliance to radiation for advanced head and neck cancer at a tertiary care county hospital. Laryngoscope. 2008;118(3):428–432. doi:10.1097/MLG.0b013e31815ae3d2
22. Thomas K, Martin T, Gao A, et al. Interruptions of head and neck radiotherapy across insured and indigent patient populations. J Oncol Pract. 2017;13(4):e319–e328. doi:10.1200/JOP.2016.017863
23. Lazarev S, Gupta V, Ghiassi-Nejad Z, et al. Premature discontinuation of curative radiation therapy: insights from head and neck irradiation. Adv Radiat Oncol. 2018;3(1):62–69. doi:10.1016/j.adro.2017.10.006
24. Ohri N, Rapkin BD, Guha C, et al. Radiation therapy noncompliance and clinical outcomes in an urban academic cancer center. Int J Radiat Oncol Biol Phys. 2016;95(2):563–570. doi:10.1016/j.ijrobp.2016.01.043
25. Salloum RG, Smith TJ, Jensen GA, et al. Factors associated with adherence to chemotherapy guidelines in patients with non-small cell lung cancer. Lung Cancer. 2012;75(2):255–260. doi:10.1016/j.lungcan.2011.07.005
26. Kroenke CH, Kubzansky LD, Schernhammer ES, et al. Social networks, social support, and survival after breast cancer diagnosis. J Clin Oncol. 2006;24(7):1105–1111. doi:10.1200/JCO.2005.04.2846
27. DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. 2000;160(14):2101–2107. doi:10.1001/archinte.160.14.2101
28. McDermott JD, Eguchi M, Morgan R, et al. Elderly black non-Hispanic patients with head and neck squamous cell cancer have the worst survival outcomes. J Natl Compr Canc Netw. 2020;19(1):57–67. doi:10.6004/jnccn.2020.7607
29. Inverso G, Mahal BA, Aizer AA, et al. Health insurance affects head and neck cancer treatment patterns and outcomes. J Oral Maxillofac Surg. 2016;74(6):1241–1247. doi:10.1016/j.joms.2015.12.023
30. Goyal N, Day A, Epstein J, et al. Head and neck cancer survivorship consensus statement from the American Head and Neck Society. Laryngoscope Investig Otolaryngol. 2022;7(1):70–92. doi:10.1002/lio2.702
31. Mady LJ, Lyu L, Owoc MS, et al. Understanding financial toxicity in head and neck cancer survivors. Oral Oncol. 2019;95:187–193. doi:10.1016/j.oraloncology.2019.06.023
32. Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
33. Piccirillo JF, Sasaki CT, Wells CK, et al. New clinical severity staging system for cancer of the larynx. Five-year survival rates. Ann Otol Rhinol Laryngol. 1994;103(2):83–92. doi:10.1177/000348949410300201
34. Kaplan MH, Feinstein AR. The importance of classifying initial co-morbidity in evaluating the outcome of diabetes mellitus. J Chronic Dis. 1974;27(7–8):387–404. doi:10.1016/0021-9681(74)90017-4
35. Reid BC, Alberg AJ, Klassen AC, et al. Comorbidity and survival of elderly head and neck carcinoma patients. Cancer. 2001;92(8):2109–2116. doi:10.1002/1097-0142(20011015)92:8<2109::AID-CNCR1552>3.0.CO;2-M
36. Datema FR, Ferrier MB, van der Schroeff MP, et al. Impact of comorbidity on short-term mortality and overall survival of head and neck cancer patients. Head Neck. 2010;32(6):728–736. doi:10.1002/hed.21245
37. van Deudekom FJ, Schimberg AS, Kallenberg MH, et al. Functional and cognitive impairment, social environment, frailty and adverse health outcomes in older patients with head and neck cancer, a systematic review. Oral Oncol. 2017;64:27–36. doi:10.1016/j.oraloncology.2016.11.013
38. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on sarcopenia in older people. Age Ageing. 2010;39(4):412–423. doi:10.1093/ageing/afq034
39. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy169
40. Chargi N, Bril SI, Emmelot-Vonk MH, et al. Sarcopenia is a prognostic factor for overall survival in elderly patients with head-and-neck cancer. Eur Arch Otorhinolaryngol. 2019;276(5):1475–1486. doi:10.1007/s00405-019-05361-4
41. Wendrich AW, Swartz JE, Bril SI, et al. Low skeletal muscle mass is a predictive factor for chemotherapy dose-limiting toxicity in patients with locally advanced head and neck cancer. Oral Oncol. 2017;71:26–33. doi:10.1016/j.oraloncology.2017.05.012
42. Bril SI, Al‐Mamgani A, Chargi N, et al. The association of pretreatment low skeletal muscle mass with chemotherapy dose-limiting toxicity in patients with head and neck cancer undergoing primary chemoradiotherapy with high-dose cisplatin. Head Neck. 2022;44(1):189–200. doi:10.1002/hed.26919
43. Haehl E, Alvino L, Rühle A, et al. Sarcopenia as a prognostic marker in elderly head and neck squamous cell carcinoma patients undergoing (chemo-)radiation. Cancers. 2022;14(22):5536. doi:10.3390/cancers14225536
44. National Health. National Center for Health Statistics. United States: In Health; 2019.
45. Mohamed MR, Ramsdale E, Loh KP, et al. Associations of polypharmacy and inappropriate medications with adverse outcomes in older adults with cancer: a systematic review and meta-analysis. Oncologist. 2020;25(1):e94–e108. doi:10.1634/theoncologist.2019-0406
46. By the American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2019 updated AGS Beers Criteria(R) for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67(4):674–694. doi:10.1111/jgs.15767
47. Chen LJ, Trares K, Laetsch DC, et al. Systematic review and meta-analysis on the associations of polypharmacy and potentially inappropriate medication with adverse outcomes in older cancer patients. J Gerontol a Biol Sci Med Sci. 2021;76(6):1044–1052. doi:10.1093/gerona/glaa128
48. Caparrotti F, O’Sullivan B, Bratman SV, et al. Exploring the impact of human papillomavirus status, comorbidity, polypharmacy, and treatment intensity on outcome of elderly oropharyngeal cancer patients treated with radiation therapy with or without chemotherapy. Int J Radiat Oncol Biol Phys. 2017;98(4):858–867. doi:10.1016/j.ijrobp.2016.11.044
49. Bellera CA, Rainfray M, Mathoulin-Pélissier S, et al. Screening older cancer patients: first evaluation of the G-8 geriatric screening tool. Ann Oncol. 2012;23(8):2166–2172. doi:10.1093/annonc/mdr587
50. Overcash J, Ford N, Kress E, et al. Comprehensive geriatric assessment as a versatile tool to enhance the care of the older person diagnosed with cancer. Geriatrics. 2019;4(2):39. doi:10.3390/geriatrics4020039
51. Overcash JA, Beckstead J, Extermann M, et al. The abbreviated comprehensive geriatric assessment (aCGA): a retrospective analysis. Crit Rev Oncol Hematol. 2005;54(2):129–136. doi:10.1016/j.critrevonc.2004.12.002
52. Saliba D, Elliott M, Rubenstein LZ, et al. The Vulnerable Elders Survey: a tool for identifying vulnerable older people in the community. J Am Geriatr Soc. 2001;49(12):1691–1699. doi:10.1046/j.1532-5415.2001.49281.x
53. Drubbel I, Bleijenberg N, Kranenburg G, et al. Identifying frailty: do the Frailty Index and Groningen Frailty Indicator cover different clinical perspectives? A cross-sectional study. BMC Fam Pract. 2013;14(1):64. doi:10.1186/1471-2296-14-64
54. Almodovar T, Teixeira E, Barroso A, et al. Elderly patients with advanced NSCLC: the value of geriatric evaluation and the feasibility of CGA alternatives in predicting chemotherapy toxicity. Pulmonology. 2019;25(1):40–50. doi:10.1016/j.pulmoe.2018.07.004
55. Pottel L, Lycke M, Boterberg T, et al. Serial comprehensive geriatric assessment in elderly head and neck cancer patients undergoing curative radiotherapy identifies evolution of multidimensional health problems and is indicative of quality of life. Eur J Cancer Care. 2014;23(3):401–412. doi:10.1111/ecc.12179
56. Pottel L, Lycke M, Boterberg T, et al. G-8 indicates overall and quality-adjusted survival in older head and neck cancer patients treated with curative radiochemotherapy. BMC Cancer. 2015;15(1):875. doi:10.1186/s12885-015-1800-1
57. Neve M, Jameson MB, Govender S, et al. Impact of geriatric assessment on the management of older adults with head and neck cancer: a pilot study. J Geriatr Oncol. 2016;7(6):457–462. doi:10.1016/j.jgo.2016.05.006
58. Extermann M, Boler I, Reich RR, et al. Predicting the risk of chemotherapy toxicity in older patients: the Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) score. Cancer. 2012;118(13):3377–3386. doi:10.1002/cncr.26646
59. Bossi P, Vecchio AE, Gurizzan C, et al. Role of geriatric assessment in tailoring treatment of locally advanced head and neck cancer: the ELDERLY study. Annals Oncol. 2021;32:S789. doi:10.1016/j.annonc.2021.08.1274
60. Belgioia L, De Felice F, Bacigalupo A, et al. Results of a survey on elderly head and neck cancer patients on behalf of the Italian Association of Radiotherapy and Clinical Oncology (AIRO). Acta Otorhinolaryngol Ital. 2020;40(6):405–409. doi:10.14639/0392-100X-N0618
61. Mell LK, Dignam JJ, Salama JK, et al. Predictors of competing mortality in advanced head and neck cancer. J Clin Oncol. 2010;28(1):15–20. doi:10.1200/JCO.2008.20.9288
62. Carmona R, Zakeri K, Green G, et al. Improved method to stratify elderly patients with cancer at risk for competing events. J Clin Oncol. 2016;34(11):1270–1277. doi:10.1200/JCO.2015.65.0739
63. Mell LK, Shen H, Nguyen-Tân PF, et al. Nomogram to predict the benefit of intensive treatment for locoregionally advanced head and neck cancer. Clin Cancer Res. 2019;25(23):7078–7088. doi:10.1158/1078-0432.CCR-19-1832
64. Nelson TJ, Thompson CA, Zou J, et al. Validation of NRG Oncology’s prognostic nomograms for oropharyngeal cancer in the Veterans Affairs database. Cancer. 2022;128(10):1948–1957. doi:10.1002/cncr.34141
65. Vitzthum LK, Feng CH, Noticewala S, et al. Comparison of comorbidity and frailty indices in patients with head and neck cancer using an online tool. JCO Clin Cancer Inform. 2018;2(2):1–9. doi:10.1200/CCI.18.00082
66. Zakeri K, Rotolo F, Lacas B, et al. Predictive classifier for intensive treatment of head and neck cancer. Cancer. 2020;126(24):5263–5273. doi:10.1002/cncr.33212
67. Bourhis J, Overgaard J, Audry H, et al. Hyperfractionated or accelerated radiotherapy in head and neck cancer: a meta-analysis. Lancet. 2006;368(9538):843–854. doi:10.1016/S0140-6736(06)69121-6
68. Mell L, Vitzthum L, Wong H, et al. Comogram: an online tool to inform clinical decision making for cancer patients based on their competing risks. 2019; Available from: www.comogram.org.
69. Ruhle A, Stromberger C, Haehl E, et al. Development and validation of a novel prognostic score for elderly head-and-neck cancer patients undergoing radiotherapy or chemoradiation. Radiother Oncol. 2021;154:276–282. doi:10.1016/j.radonc.2020.11.023
70. Zhou W, Peng C, Liu Z, et al. A novel clinical signature predicts the survival of elderly patients with oral squamous cell carcinoma. Eur Arch Otorhinolaryngol. 2022;279(1):391–398. doi:10.1007/s00405-021-06786-6
71. Kou J, Zhang -L-L, Yang X-L, et al. Development of a nomogram model for treatment of elderly patients with locoregionally advanced nasopharyngeal carcinoma. J Pers Med. 2021;11(11):1065. doi:10.3390/jpm11111065
72. Turrentine FE, Wang H, Simpson VB, et al. Surgical risk factors, morbidity, and mortality in elderly patients. J Am Coll Surg. 2006;203(6):865–877. doi:10.1016/j.jamcollsurg.2006.08.026
73. Spyropoulou GA, Jeng S-F, Hsieh C-H, et al. Microsurgical reconstruction for head and neck cancer in elderly patients. J Reconstr Microsurg. 2014;30(2):91–96. doi:10.1055/s-0033-1357277
74. Bhama PK, Patel S, Khan U, et al. Head and neck free flap reconstruction in patients older than 80 years. J Reconstr Microsurg. 2014;30(8):523–530. doi:10.1055/s-0034-1384664
75. L’Esperance HE, Kallogjeri D, Yousaf S, et al. Prediction of mortality and morbidity in head and neck cancer patients 80 years of age and older undergoing surgery. Laryngoscope. 2018;128(4):871–877. doi:10.1002/lary.26858
76. Wu Y, Zhang B, Huang Z, et al. Study of surgical treatment for elderly patients with head and neck cancer. Int J Oral Maxillofac Surg. 2018;47(7):824–829. doi:10.1016/j.ijom.2018.01.018
77. Goh CS, Kok Y-O, Yong CP-C, et al. Outcome predictors in elderly head and neck free flap reconstruction: a retrospective study and systematic review of the current evidence. J Plast Reconstr Aesthet Surg. 2018;71(5):719–728. doi:10.1016/j.bjps.2017.12.011
78. Goldstein DP, Sklar MC, Almeida JR, et al. Frailty as a predictor of outcomes in patients undergoing head and neck cancer surgery. Laryngoscope. 2020;130(5):E340–E345. doi:10.1002/lary.28222
79. Peters TT, van Dijk BAC, Roodenburg JLN, et al. Relation between age, comorbidity, and complications in patients undergoing major surgery for head and neck cancer. Ann Surg Oncol. 2014;21(3):963–970. doi:10.1245/s10434-013-3375-x
80. Peters TTA, Post SF, van Dijk BAC, et al. Free flap reconstruction for head and neck cancer can be safely performed in both young and elderly patients after careful patient selection. Eur Arch Otorhinolaryngol. 2015;272(10):2999–3005. doi:10.1007/s00405-014-3268-z
81. Nakayama Y, Ohkoshi A, Ishii R, et al. The geriatric-8 screening tool for predicting complications in older adults after surgery for locally advanced head and neck cancer with free flap reconstruction. Eur Arch Otorhinolaryngol. 2022;279(5):2565–2571. doi:10.1007/s00405-021-07038-3
82. Grammatica A, Piazza C, Paderno A, et al. Free flaps in head and neck reconstruction after oncologic surgery: expected outcomes in the elderly. Otolaryngol Head Neck Surg. 2015;152(5):796–802. doi:10.1177/0194599815576905
83. Wester JL, Lindau RH, Wax MK. Efficacy of free flap reconstruction of the head and neck in patients 90 years and older. JAMA Otolaryngol Head Neck Surg. 2013;139(1):49–53. doi:10.1001/jamaoto.2013.1138
84. Beausang ES, Ang EE, Lipa JE, et al. Microvascular free tissue transfer in elderly patients: the Toronto experience. Head Neck. 2003;25(7):549–553. doi:10.1002/hed.10240
85. Jalisi S, Rubin SJ, Wu KY, et al. Outcomes of head and neck cancer surgery in the geriatric population based on case volume at academic centers. Laryngoscope. 2017;127(11):2539–2544. doi:10.1002/lary.26750
86. Rubin SJ, Wu KY, Kirke DN, et al. Head and neck cancer complications in the geriatric population based on hospital case volume. Ear Nose Throat J. 2021;100(2):NP62–NP68. doi:10.1177/0145561319856006
87. Jackson RS, Chen S, Last A, et al. Multi-institutional analysis of outcomes following transoral surgery for HPV-positive oropharyngeal squamous cell carcinoma in elderly patients. Head Neck. 2019;41(11):3933–3939. doi:10.1002/hed.25946
88. Rodrigo JP, García‐Velasco F, Ambrosch P, et al. Transoral laser microsurgery for glottic cancer in the elderly: efficacy and safety. Head Neck. 2019;41(6):1816–1823. doi:10.1002/hed.25616
89. Lee C, Forner D, Noel CW, et al. Functional and oncologic outcomes of octogenarians undergoing transoral laser microsurgery for laryngeal cancer. OTO Open. 2021;5(3):2473974X211046957. doi:10.1177/2473974X211046957
90. Hendriksma M, Heijnen BJ, Sjogren EV. Oncologic and functional outcomes of patients treated with transoral CO2 laser microsurgery or radiotherapy for T2 glottic carcinoma: a systematic review of the literature. Curr Opin Otolaryngol Head Neck Surg. 2018;26(2):84–93. doi:10.1097/MOO.0000000000000438
91. Spielmann PM, Majumdar S, Morton RP. Quality of life and functional outcomes in the management of early glottic carcinoma: a systematic review of studies comparing radiotherapy and transoral laser microsurgery. Clin Otolaryngol. 2010;35(5):373–382. doi:10.1111/j.1749-4486.2010.02191.x
92. Gokmen MF, Buyukatalay ZC, Beton S, et al. Functional and oncological outcomes of open partial laryngectomy vs. transoral laser surgery in supraglottic larynx cancer. Turk Arch Otorhinolaryngol. 2020;58(4):227–233. doi:10.5152/tao.2020.5573
93. Withers HR, Taylor JM, Maciejewski B. The hazard of accelerated tumor clonogen repopulation during radiotherapy. Acta Oncol. 1988;27(2):131–146. doi:10.3109/02841868809090333
94. Shuryak I, Hall EJ, Brenner DJ. Optimized hypofractionation can markedly improve tumor control and decrease late effects for head and neck cancer. Int J Radiat Oncol Biol Phys. 2019;104(2):272–278. doi:10.1016/j.ijrobp.2019.02.025
95. Toya R. Hypofractionated palliative volumetric modulated arc radiotherapy with the Radiation Oncology Study Group 8502 “QUAD shot” regimen for incurable head and neck cancer. Radiat Oncol. 2020;15(1):123. doi:10.1186/s13014-020-01548-w
96. Kancherla KN, Oksuz DC, Prestwich RJ, et al. The role of split-course hypofractionated palliative radiotherapy in head and neck cancer. Clin Oncol. 2011;23(2):141–148. doi:10.1016/j.clon.2010.09.006
97. Pearson RA, Bannister-Young RH, Ivison D, et al. Split-course hypofractionated palliative radiotherapy for patients with head and neck squamous cell carcinoma - a worthwhile treatment schedule in the UK? Clin Oncol. 2010;22(10):890–891. doi:10.1016/j.clon.2010.06.003
98. Al-mamgani A, Tans L, Van Rooij PHE, et al. Hypofractionated radiotherapy denoted as the “Christie scheme”: an effective means of palliating patients with head and neck cancers not suitable for curative treatment. Acta Oncol. 2009;48(4):562–570. doi:10.1080/02841860902740899
99. Corry J, Peters LJ, Costa ID, et al. The ‘QUAD SHOT’--a Phase II study of palliative radiotherapy for incurable head and neck cancer. Radiother Oncol. 2005;77(2):137–142. doi:10.1016/j.radonc.2005.10.008
100. Lok BH, Jiang G, Gutiontov S, et al. Palliative head and neck radiotherapy with the RTOG 8502 regimen for incurable primary or metastatic cancers. Oral Oncol. 2015;51(10):957–962. doi:10.1016/j.oraloncology.2015.07.011
101. Ferro M, Macchia G, Re A, et al. Advanced head and neck cancer in older adults: results of a short course accelerated radiotherapy trial. J Geriatr Oncol. 2021;12(3):441–445. doi:10.1016/j.jgo.2020.10.006
102. Thomson DJ, Palma D, Guckenberger M, et al. Practice recommendations for risk-adapted head and neck cancer radiotherapy during the COVID-19 pandemic: an ASTRO-ESTRO consensus statement. Radiother Oncol. 2020;151:314–321. doi:10.1016/j.radonc.2020.04.019
103. Bledsoe TJ, Noble AR, Reddy CA, et al. Split-Course Accelerated Hypofractionated Radiotherapy (SCAHRT): a safe and effective option for head and neck cancer in the elderly or infirm. Anticancer Res. 2016;36(3):933–939.
104. Hall EJ. Radiobiology for the Radiologist. Hagerstown, Md: Medical Dept., Harper & Row; 1973.
105. Ortholan C, Auperin A, Mertens C, et al. Radiothérapie hypofractionnée des cancers ORL chez le sujet âgé [Hypofractionad radiotherapy for elderly with head and neck cancer]. Cancer Radiother. 2018;22(6–7):640–643. French. doi:10.1016/j.canrad.2018.06.008
106. Dickstein DR, Egerman MA, Bui AH, et al. A new face of the HPV epidemic: oropharyngeal cancer in the elderly. Oral Oncol. 2020;109:104687. doi:10.1016/j.oraloncology.2020.104687
107. Dave E, Lehrer EJ, Hsieh K, et al. Human papilloma virus-positive oropharyngeal squamous cell carcinoma in the elderly. Anticancer Res. 2017;37(4):1847–1851.
108. Dickstein DR. Hypofractionated radiotherapy for elderly patients with head and neck squamous cell carcinoma - interim results from a propective phase II trial. in American Radium Society. Scottsdale, Arizona; 2022.
109. Dickstein DR, Lehrer EJ, Hsieh K, et al. Management of older adults with locally advanced head and neck cancer. Cancers. 2022;14(11):2809. doi:10.3390/cancers14112809
110. Michal SA, Adelstein DJ, Rybicki LA, et al. Multi-agent concurrent chemoradiotherapy for locally advanced head and neck squamous cell cancer in the elderly. Head Neck. 2012;34(8):1147–1152. doi:10.1002/hed.21891
111. Machtay M, Moughan J, Trotti A, et al. Factors associated with severe late toxicity after concurrent chemoradiation for locally advanced head and neck cancer: an RTOG analysis. J Clin Oncol. 2008;26(21):3582–3589. doi:10.1200/JCO.2007.14.8841
112. Mayer A, Wenzel W, Wollschläger D, et al. Adjuvant chemoradiotherapy in elderly patients with head and neck cancer: a monoinstitutional, two-to-one pair-matching analysis. Strahlenther Onkol. 2022;198(2):159–170. doi:10.1007/s00066-021-01890-2
113. Sachdev S, Refaat T, Bacchus ID, et al. Age most significant predictor of requiring enteral feeding in head-and-neck cancer patients. Radiat Oncol. 2015;10(1):93. doi:10.1186/s13014-015-0408-6
114. De Felice F, Vetrone L, Bulzonetti N, et al. Hypofractionated radiotherapy combined with cetuximab in vulnerable elderly patients with locally advanced head and neck squamous cell carcinoma. Med Oncol. 2019;36(8):68. doi:10.1007/s12032-019-1292-y
115. Sarris EG, Harrington KJ, Saif MW, et al. Multimodal treatment strategies for elderly patients with head and neck cancer. Cancer Treat Rev. 2014;40(3):465–475. doi:10.1016/j.ctrv.2013.10.007
116. Park JW, Roh J-L, Lee S-W, et al. Effect of polypharmacy and potentially inappropriate medications on treatment and posttreatment courses in elderly patients with head and neck cancer. J Cancer Res Clin Oncol. 2016;142(5):1031–1040. doi:10.1007/s00432-015-2108-x
117. Pignon JP, Bourhis J, Domenge C, et al. Chemotherapy added to locoregional treatment for head and neck squamous-cell carcinoma: three meta-analyses of updated individual data. MACH-NC Collaborative Group. Meta-Analysis of Chemotherapy on Head and Neck Cancer. Lancet. 2000;355(9208):949–955. doi:10.1016/S0140-6736(00)90011-4
118. Nehlsen AD, Lehrer EJ, Dickstein DR, et al. Functional larynx preservation in patients with locally advanced squamous cell carcinoma of the larynx and hypopharynx treated with induction chemotherapy vs. concurrent chemoradiation alone. Cureus. 2021;13(7):e16310. doi:10.7759/cureus.16310
119. Blanchard P, Baujat B, Holostenco V, et al. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): a comprehensive analysis by tumour site. Radiother Oncol. 2011;100(1):33–40. doi:10.1016/j.radonc.2011.05.036
120. Lacas B, Carmel A, Landais C, et al. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): an update on 107 randomized trials and 19,805 patients, on behalf of MACH-NC Group. Radiother Oncol. 2021;156:281–293. doi:10.1016/j.radonc.2021.01.013
121. Amini A, Jones BL, McDermott JD, et al. Survival outcomes with concurrent chemoradiation for elderly patients with locally advanced head and neck cancer according to the National Cancer Data Base. Cancer. 2016;122(10):1533–1543. doi:10.1002/cncr.29956
122. Ward MC, Reddy CA, Adelstein DJ, et al. Use of systemic therapy with definitive radiotherapy for elderly patients with head and neck cancer: a National Cancer Data Base analysis. Cancer. 2016;122(22):3472–3483. doi:10.1002/cncr.30214
123. Zandberg DP, Cullen K, Bentzen SM, et al. Definitive radiation with concurrent cetuximab vs. radiation with or without concurrent cytotoxic chemotherapy in older patients with squamous cell carcinoma of the head and neck: analysis of the SEER-medicare linked database. Oral Oncol. 2018;86:132–140. doi:10.1016/j.oraloncology.2018.09.023
124. VanderWalde NA, Meyer AM, Deal AM, et al. Effectiveness of chemoradiation for head and neck cancer in an older patient population. Int J Radiat Oncol Biol Phys. 2014;89(1):30–37. doi:10.1016/j.ijrobp.2014.01.053
125. McDermott JD, Amini A, Molina E, et al. Treatment outcomes and cost comparisons for older adults with T4 laryngeal squamous cell cancer. Head Neck. 2023;45(3):664–674. doi:10.1002/hed.27284
126. Hurria A, Levit LA, Dale W, et al. Improving the evidence base for treating older adults with cancer: American Society of clinical oncology statement. J Clin Oncol. 2015;33(32):3826–3833. doi:10.1200/JCO.2015.63.0319
127. Kanesvaran R, Cordoba R, Maggiore R. Immunotherapy in older adults with advanced cancers: implications for clinical decision-making and future research. Am Soc Clin Oncol Educ Book. 2018;38(38):400–414. doi:10.1200/EDBK_201435
128. Muller L, Di Benedetto S, Pawelec G. The immune system and its dysregulation with aging. Subcell Biochem. 2019;91:21–43.
129. Wagner A, Garner-Spitzer E, Jasinska J, et al. Age-related differences in humoral and cellular immune responses after primary immunisation: indications for stratified vaccination schedules. Sci Rep. 2018;8(1):9825. doi:10.1038/s41598-018-28111-8
130. Nishijima TF, Muss HB, Shachar SS, et al. Comparison of efficacy of immune checkpoint inhibitors (ICIs) between younger and older patients: a systematic review and meta-analysis. Cancer Treat Rev. 2016;45:30–37. doi:10.1016/j.ctrv.2016.02.006
131. Elias R, Giobbie-Hurder A, McCleary NJ, et al. Efficacy of PD-1 & PD-L1 inhibitors in older adults: a meta-analysis. J Immunother Cancer. 2018;6(1):26. doi:10.1186/s40425-018-0336-8
132. Ridolfi L, De Rosa F, Petracci E, et al. Anti-PD1 antibodies in patients aged >/= 75 years with metastatic melanoma: a retrospective multicentre study. J Geriatr Oncol. 2020;11(3):515–522. doi:10.1016/j.jgo.2019.12.012
133. Van holstein Y, Kapiteijn E, Bastiaannet E, et al. Efficacy and adverse events of immunotherapy with checkpoint inhibitors in older patients with cancer. Drugs Aging. 2019;36(10):927–938. doi:10.1007/s40266-019-00697-2
134. Sacco AG, Chen R, Worden FP, et al. Pembrolizumab plus cetuximab in patients with recurrent or metastatic head and neck squamous cell carcinoma: an open-label, multi-arm, non-randomised, multicentre, Phase 2 trial. Lancet Oncol. 2021;22(6):883–892. doi:10.1016/S1470-2045(21)00136-4
135. Moretti JA. Sensori-neural hearing loss following radiotherapy to the nasopharynx. Laryngoscope. 1976;86(4):598–602. doi:10.1288/00005537-197604000-00018
136. Brock P, Bellman S. Ototoxicity of cisplatinum. Br J Cancer. 1991;63(1):159–160. doi:10.1038/bjc.1991.35
137. Skinner R, Pearson A, Amineddine HA, et al. Ototoxicity of cisplatinum in children and adolescents. Br J Cancer. 1990;61(6):927–931. doi:10.1038/bjc.1990.208
138. Pan CC, Eisbruch A, Lee JS, et al. Prospective study of inner ear radiation dose and hearing loss in head-and-neck cancer patients. Int J Radiat Oncol Biol Phys. 2005;61(5):1393–1402. doi:10.1016/j.ijrobp.2004.08.019
139. Talarico L, Chen G, Pazdur R. Enrollment of elderly patients in clinical trials for cancer drug registration: a 7-year experience by the US Food and Drug Administration. J Clin Oncol. 2004;22(22):4626–4631. doi:10.1200/JCO.2004.02.175
140. Camet ML, Spence A, Hayashi SS, et al. Cisplatin ototoxicity: examination of the impact of dosing, infusion times, and schedules in pediatric cancer patients. Front Oncol. 2021;11:673080. doi:10.3389/fonc.2021.673080
141. Hitchcock YJ, Tward JD, Szabo A, et al. Relative contributions of radiation and cisplatin-based chemotherapy to sensorineural hearing loss in head-and-neck cancer patients. Int J Radiat Oncol Biol Phys. 2009;73(3):779–788. doi:10.1016/j.ijrobp.2008.05.040
142. Schuette A, Lander DP, Kallogjeri D, et al. Predicting hearing loss after radiotherapy and cisplatin chemotherapy in patients with head and neck cancer. JAMA Otolaryngol Head Neck Surg. 2020;146(2):106–112. doi:10.1001/jamaoto.2019.3550
143. Deutsch BC, Collopy C, Kallogjeri D, et al. Validation of hearing loss prediction tool for cisplatin chemotherapy and radiation in head and neck cancer treatment. JAMA Otolaryngol Head Neck Surg. 2021;147(2):182–189. doi:10.1001/jamaoto.2020.4620
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Treatment of Substance Misuse in Older Adults: Beyond Early Adulthood
Hu J, Kulkarni N, Maliha P, Grossberg G
Substance Abuse and Rehabilitation 2024, 15:87-98
Published Date: 12 July 2024