Back to Journals » Orthopedic Research and Reviews » Volume 17
Clinical and Radiological Outcomes of Single-Level Full Endoscopic Posterior Cervical Foraminotomy and Herniectomy: A 12 months Follow-up
Authors The Dinh H, Ngoc Dinh S, Hoang Nguyen L, Manh Do H, Van Nguyen T, Van Vu C
Received 19 July 2025
Accepted for publication 31 October 2025
Published 6 November 2025 Volume 2025:17 Pages 517—529
DOI https://doi.org/10.2147/ORR.S554908
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Clark Hung
Hung The Dinh,1,2,* Son Ngoc Dinh,1,2,* Long Hoang Nguyen,2 Hung Manh Do,2 Thach Van Nguyen,2 Cuong Van Vu2
1Faculty of Surgery, Ha Noi Medical University, Hanoi, Vietnam; 2Department of Spine Surgery, Viet Duc University Hospital, Hanoi, Vietnam
*These authors contributed equally to this work
Correspondence: Cuong Van Vu, Department of Spine Surgery, Viet Duc University Hospital, 40 Trang Thi Str, Hoan Kiem, Ha Noi, 100000, Vietnam, Email [email protected]
Background: To date, no comprehensive study has evaluated the outcomes of single-level full endoscopic posterior cervical foraminotomy and herniectomy in Vietnam.
Methods: This prospective, descriptive study was conducted before and after spinal disc herniation surgery at the Department of Spine Surgery, Viet Duc University Hospital, Hanoi, Vietnam, from March 2023 to December 2024. All patients follow-up during the 12 months with clinical, radiological and image outcomes.
Results: The study included 47 patients, with 23 males (48.9%) and 24 females (51.1%), with a mean age of 44.46 ± 8.47 years old. The location of the operated disc was predominantly at the C5-C6 level (61.7%) with 10.34 ± 0.7 incision length. The recovery outcomes revealed a strong trend toward excellent and good results, totalling 93.6% of the positive outcomes. A statistically significant reduction in all measured parameters over time (the Numerical Rating Scale (NRS) for pain and the Neck Disability Index (NDI) at multiple time points: pre-operation, post-operative day 1, and 1, 6, and 12 months post-operation) compared to pre-operative baseline values (p < 0.0001 for all comparisons). Radiological outcomes showed significantly improved cervical neural curvature from to C2-C7 at all the postoperative time points. Foraminal dimensions (height, diameter, and area) showed significant immediate postoperative increases. Disc height decreased significantly, while cervical range of motion showed variable changes. C2-C7 SVA and T1 slope remained stable, indicating no significant changes in the global alignment. Complications were generally low; two patients had intraoperative nerve root injury, and one patient had transient root palsy.
Conclusion: This study demonstrated that single-level full endoscopic posterior cervical foraminotomy and herniectomy are safe in the short-term with 12 months of follow-up and effective in the treatment of cervical disc herniation. Further study is needed with a larger sample size, with control group and long-term follow-up.
Keywords: clinical outcomes, radiological outcomes, single-level full endoscopic posterior cervical foraminotomy and discectomy, disc herniation
Background
Cervical disc herniation occurs when the disc tissue, including the nucleus pulposus or annulus fibrosus, displaces its physiological position within the intervertebral space. Depending on the location of the herniated mass and the structures it compresses, it may result in various clinical syndromes such as spinal cord compression or nerve root compression syndromes.1 In the United States, a 23-year study by Radhakrishnan K et al reported an incidence of cervical disc herniation of 107.3 per 100,000 in males and 63.5 per 100,000 in females, with the condition predominantly affecting individuals aged 30 to 60 years.2
There are two primary treatment approaches for cervical disc herniation: nonsurgical and surgical. Nonsurgical management includes pharmacotherapy, physical rehabilitation, and epidural nerve blocks. Surgical intervention is indicated when conservative treatment fails or when rapidly progressing neurological symptoms such as motor paralysis emerge. Anterior cervical discectomy and fusion (ACDF) is regarded as a cornerstone surgical procedure for treating cervical disc herniation, and its efficacy has been substantiated in numerous studies.3,4
However, long-term follow-up has revealed complications associated with the anterior approach, including injuries to the esophagus, trachea, and major blood vessels, as well as adjacent segment disease, which has been reported in 25% of patients within 10 years of surgery. Cervical disc arthroplasty was introduced to mitigate adjacent segment disease and to preserve cervical spinal mobility. Nevertheless, within one year of surgery, reports have indicated heterotopic ossification at the replacement disc site, limiting disc mobility in 27–67% of patients.5 For central-lateral or lateral cervical disc herniations, posterior decompression surgery has demonstrated nerve root decompression efficacy comparable to anterior approaches.6
However, traditional open posterior surgery has disadvantages, including paraspinal muscle fibrosis; postoperative instability; and disruption of the cervical musculature, facet joints, and articular surfaces due to extensive dissection.7 To address these limitations, posterior cervical endoscopic surgery has been adopted, offering advantages such as smaller incision, minimal soft tissue damage, reduced postoperative scarring, shorter recovery time, and earlier return to work. Consequently, this technique is a viable option that provides surgeons with a practical and tailored approach for patients.
The Viet Duc University Hospital pioneered the use of posterior endoscopic surgery for the treatment of cervical disc herniation in Vietnam. To date, no comprehensive study has evaluated the outcomes of this surgical approach. Therefore, we conducted this study to address this knowledge gap.
Materials and Methods
This prospective, descriptive study was conducted before and after spinal disc herniation surgery performed at the Department of Spine Surgery, Viet Duc University Hospital, Hanoi, Vietnam, from March 2023 to December 2024.
The inclusion criteria were patients diagnosed with cervical disc herniation who met the following criteria: clinical presentation of unilateral nerve root compression syndrome, magnetic resonance imaging showing evidence of a central-lateral or lateral disc herniation corresponding to the clinical symptoms, and a lack of symptom improvement after at least six weeks of conservative medical treatment. These patients underwent single-level posterior endoscopic discectomy for disc herniation removal, had complete medical records, and had regular follow-up. The exclusion criteria for the study encompassed the following: patients with concomitant spinal cord compression syndrome; cervical spine instability; multilevel disc herniation; calcified disc herniation; patients with severe systemic comorbidities such as severe liver failure, severe renal failure, coagulopathy, or active infection; Patients refused to participate in the study.
Procedure
Pre-Operative Preparation
The preoperative imaging, including radiography, computed tomography (CT), and magnetic resonance imaging (MRI) of the cervical spine. A standard preoperative laboratory workup, comprising basic surgical tests, abdominal ultrasound, chest radiography, and electrocardiography (was). The patients were evaluated by an anesthesiologist prior to surgery. Bowel preparation and fasting were performed before the procedure. Prophylactic antibiotics were administered preoperatively. The occipital region was shaved before the surgery.
Patient Positioning and Anesthesia
The patient was placed in a prone position on a radiolucent operating table, with padding applied to pressure points, including both shoulders, both anterior superior iliac spines, both knees, and the dorsum of both feet. The shoulders were gently retracted and fixed with wide adhesive tape to facilitate intraoperative localization verification using the C-arm system. The patients underwent general anesthesia without the use of muscle relaxants.
Technique
A specialized endoscopic surgical instrument set from JoinMax (Germany) was used. The General Electric Health Care C-arm system was employed during the surgery to ensure precise localization throughout the procedure. The surgical technique for Spinal surgery was performed as follows: identification of the skin entry point and needle insertion), dilation of the access pathway, widening of the interlaminar foramen, removal of the ligamentum flavum, identification of anatomical structures within the interlaminar foramen region, localization and removal of the herniated disc, reassessment of the nerve root, hemostasis, and wound closure.
In this study, posterior cervical endoscopic surgery was performed to selectively remove the herniated disc fragment responsible for neural compression, without undertaking a complete discectomy. The procedure was conducted under endoscopic visualization, targeting only the compressive lesion and avoiding deep intervention within the disc space, thereby preserving spinal alignment and reducing the risk of postoperative cervical kyphosis. Herniations were classified according to the FFS system, with Zone A lesions typically associated with myelopathy, Zone B lesions presenting with either myelopathic or radicular symptoms, and Zone C lesions predominantly causing radiculopathy. The degree of neural compression was graded as follows: Grade 1 (small size) with minimal symptoms except in foraminal type 1C; Grade 2 (medium size) with significant compression leading to radiculopathy or moderate myelopathy; and Grade 3 (large size) with severe compression resulting in pronounced neurological deficits, particularly myelopathy with motor or bladder dysfunction. Surgical intervention was indicated for herniations classified as 1C, 2B, 3B, 2A, 3A, 2AB, or 3AB that were refractory to conservative management or associated with progressive neurological impairment. This technique enabled targeted decompression while maintaining disc integrity and spinal stability.
The Foramen Facet Spinal (FFS) classification offers distinct benefits in the assessment of intervertebral disc herniation.8 By enabling precise identification of both the anatomical site of the herniation and the degree of nerve root compression, it permits a thorough characterization of the condition. It also provides a reliable framework for interpreting postoperative magnetic resonance imaging, allowing clinicians to determine whether disc removal has been complete or partial. Notably, the system’s high Kendall’s W coefficient (0.888) reflects excellent agreement between different observers, underscoring its reproducibility. Its straightforward application in daily practice, coupled with its capacity to anticipate the extent of decompression required during surgery, reinforces its utility. Taken together, these attributes position the FFS classification as a robust, objective, and clinically valuable tool for both diagnosis and surgical planning in cases of spinal disc herniation.
Parameter Measurements
We evaluated the clinical characteristics of radiculopathy syndrome, including radicular pain, sensory disturbances, motor impairments, reflex abnormalities corresponding to the distribution of the affected nerve root, and muscle atrophy in patients with prolonged nerve root compression. Clinical assessment scales: Visual Analog Scale (VAS) and Neck Disability Index (NDI). Diagnostic Imaging: Conventional X-ray (XR), Figure 1; Dynamic XR Imaging; Computed Tomography (CT), Figure 2; Magnetic Resonance Imaging (MRI), Figure 3. The intraoperative variables, variables within the first 24 h post-surgery, variables during hospitalization, and postoperative variables at 1 month, 6 months, and 1 year post-surgery also recorded based on clinical and paraclinical parameters.
 |
Figure 1 A radiograph with pre- and post-operative measurements. (A) Pre-operative measurements. (B) Post-operative measurements. |
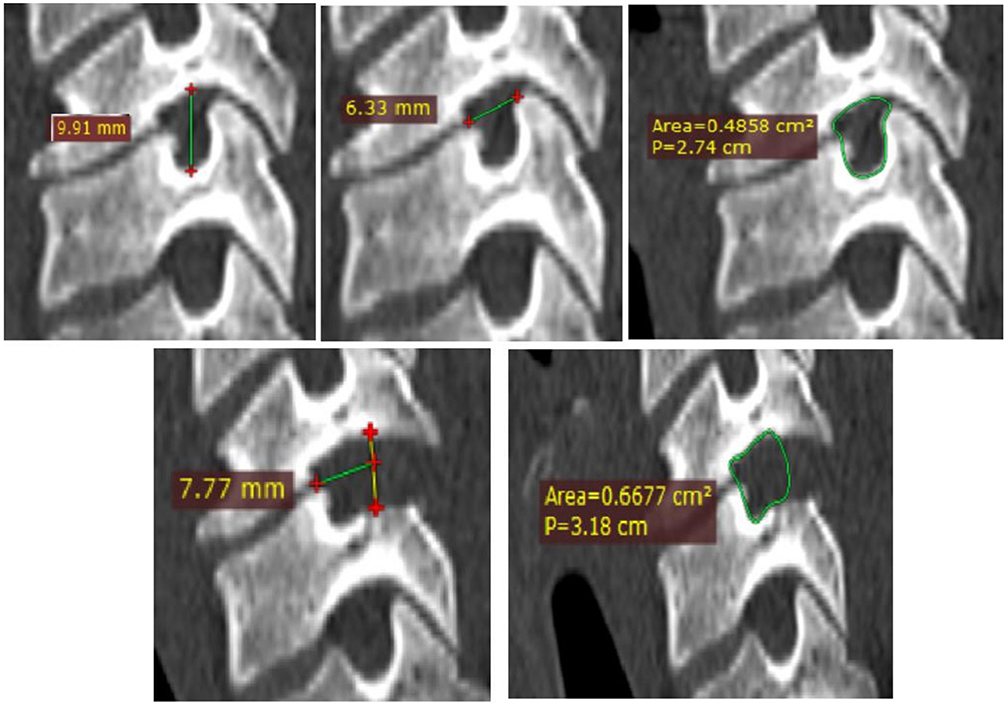 |
Figure 2 Computed Tomography (CT). |
 |
Figure 3 Magnetic Resonance Imaging (MRI). Red arrow: Herniated disc compressing the nerve root. White arrow: Site of the herniated disc after surgical removal. |
In our study, we used the Odom scale to assess postoperative outcomes. This scale categorizes results into four levels: Excellent, Good, Fair, and Poor. An “Excellent” outcome indicates that all preoperative symptoms were completely relieved. A “Good” outcome means the patient showed a clear improvement in symptoms, although some residual complaints remained. A “Fair” outcome reflects some improvement, but the overall result is largely unsatisfactory. A “Poor” outcome signifies that the patient’s condition either did not improve or worsened. The Odom scale is user-friendly and quick to apply in clinical settings, making it a valuable tool for surgeons to provide a concise overall evaluation of surgical success. Additionally, this scale has been utilized in studies such as Alomar et al (2022), reinforcing its relevance in medical research.9
Statistical Analysis
Data were entered and managed using the Epidata software. Statistical processing and analysis were performed using SPSS version 20.0. Descriptive statistics included mean, median, and standard deviation for quantitative variables and frequency and percentage for qualitative variables. Inferential statistics employed parametric and nonparametric tests (eg, T-Test, Mann–Whitney test) to identify differences between groups for quantitative data, whereas the chi-square test was used for qualitative data. Statistical significance was set at P < 0.05.
Ethics
This study was approved by the Ethics Committee of Hanoi Medical University (No. 812/GCN-HĐĐĐNCYSH-ĐHYHN, dated March 3, 2023) and adhered to the principles of the Declaration of Helsinki. Written informed consent was obtained from all the patients. Patients underwent history taking and clinical symptom evaluation, with corresponding diagnostic imaging, followed by approval from a departmental consultation board. Surgery was performed according to a standardized protocol. Patients voluntarily agreed to participate in the study after receiving thorough counselling and reviewing the consent form, which detailed the study’s significance, objectives, procedures, participants’ rights and obligations, right to withdraw from the study, and assurances of personal confidentiality throughout the research process and its outcomes. All information in the medical records was strictly confidential and used solely for research purposes.
Results
This study included 47 patients; their demographic and clinical characteristics are shown in Table 1. The cohort was characterized by a balanced sex ratio with 23 males (48.9%) and 24 females (51.1%), with a mean age of 44.46 ± 8.47 years old. Clinically, spontaneous onset (97.9%), neck pain (85.1%), radicular pain (100%), and sensory disturbances (74.5%) dominated the presentation, while motor deficits (12.8%) were less frequent. No sphincter dysfunction was observed.
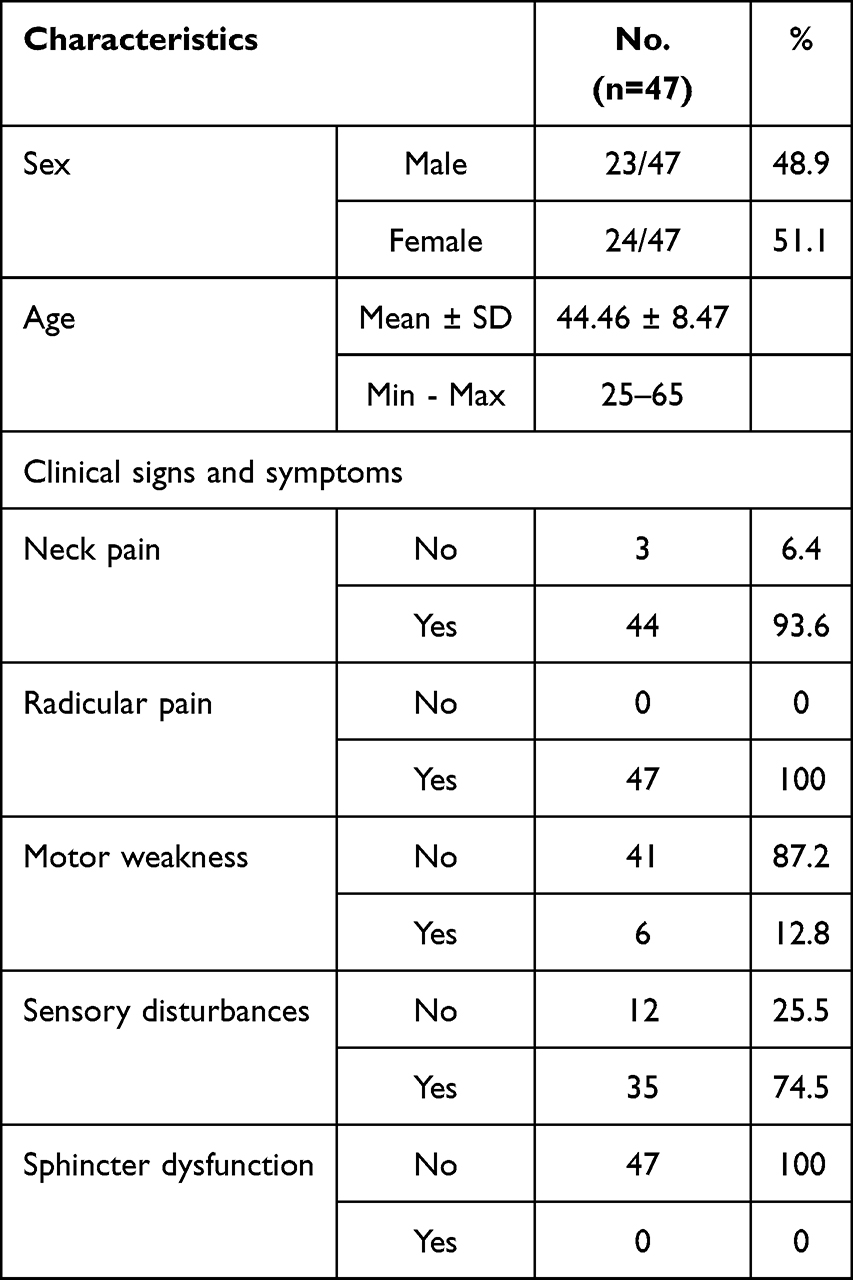 |
Table 1 Demographics of Patients |
The surgical characteristics of the 47 patients who underwent intervention are shown in Table 2. The operated disc was predominantly at the C5-C6 level, accounting for 29 patients (61.7%), followed by C6-7 in 15 patients (31.9%) and C4-C5 in 3 patients (6.4%). The study was characterized by a slight right-sided predominance (55.3%) with 10.34 ± 0.7 incision length. The duration of treatment, interpreted as the time from surgery to a defined endpoint (eg, discharge or follow-up), had a mean of 2.07 ± 1.02 days, with a range of 1 to 5days.
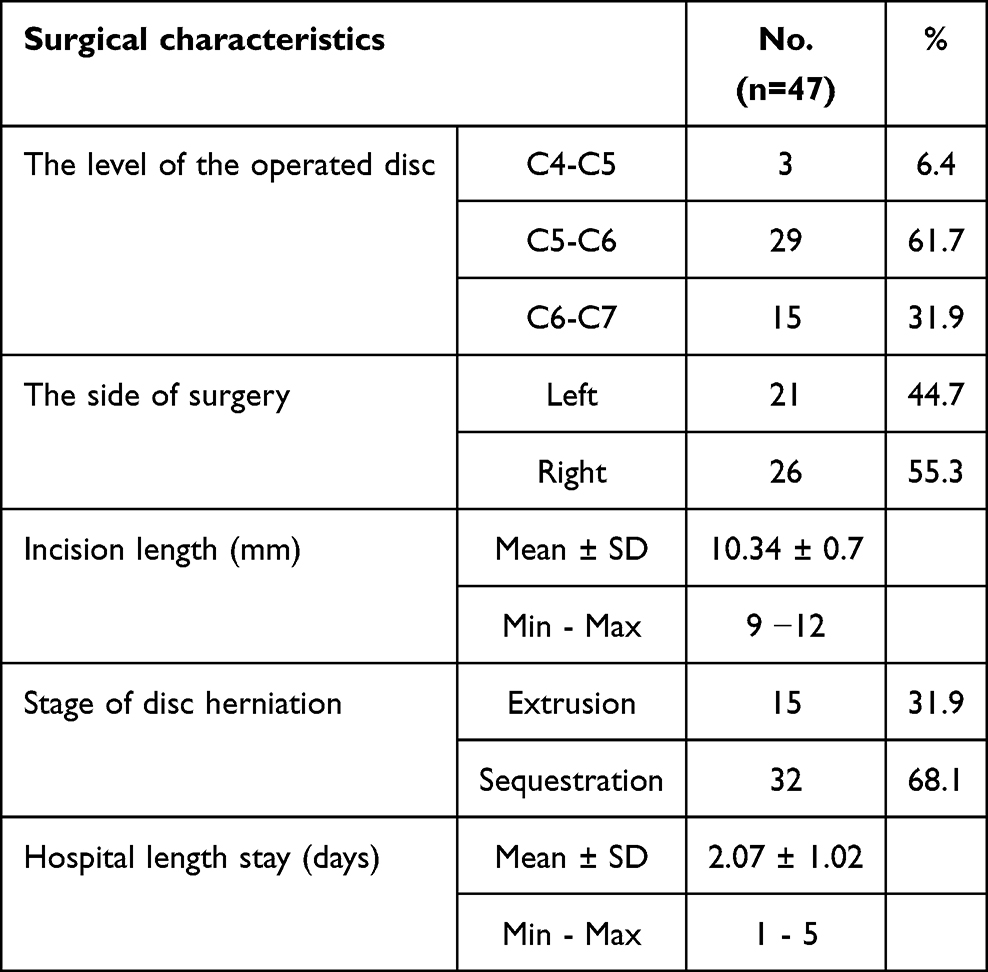 |
Table 2 Surgical Characteristics |
Complications were generally low (Table 3), with most occurring at a frequency of 4.3% intraoperative nerve root injury (one patient with incomplete nerve root injury recovery within one months and one patient with complete nerve root injury sustained the injury after one years). Transient root palsy was observed in 2.1% of the patients (one patient fully recovered before discharge).
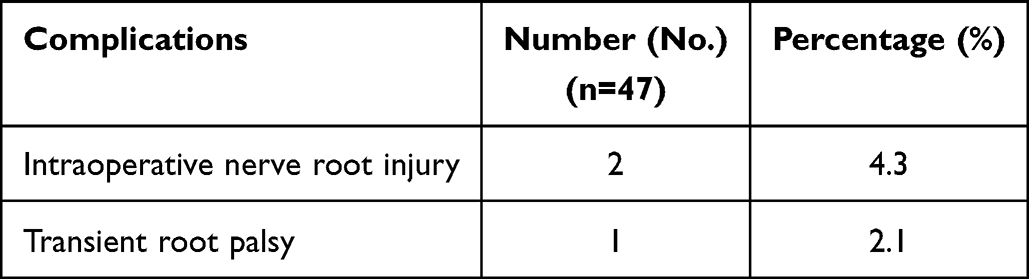 |
Table 3 Peri-Operative and Post-Operative Complications |
Clinical Outcomes
The recovery outcomes of the 47 patients were assessed post-intervention using Odom’s criteria, a standardized measure of clinical recovery. According to Odom’s criteria, the distribution of recovery outcomes revealed a strong trend toward excellent and good results, with 74.5% and 19.1% of patients in these categories, respectively, totaling 93.6% with positive outcomes. Fair and poor recoveries were notably less common, occurring in 4.3% and 2.1% of cases, respectively, highlighting the intervention’s high efficacy across the cohort.
Table 4 shows the evaluation of the efficacy of the intervention on neck pain, arm pain, and neck disability. For neck pain (Neck-NRS), the pre-operative mean score was 5.06 ± 2.52 This decreased markedly to 1.64 ± 1.48 by post-operative day 1. Further improvements were observed at 1 month (0.81 ± 1.08), 6 months (0.74 ± 1.13), and 12 months (0.60 ± 0.99) post-operation. Arm pain (Arm-NRS) showed a significant decline from the pre-operative mean of 7.32 ± 2.11 to 1.02 ± 1.15 on post-operative day 1. This reduction continued at 1 month (0.45 ± 0.95), 6 months (0.36 ± 0.87), and 12 months (0.28 ± 0.77) post-operation. The Neck Disability Index (NDI) also showed significant and sustained improvement. Pre-operatively, The mean NDI score was 52.81 ± 17.68. This decreased to 14.68 ± 7.04 by post-operative day 1, at 1 month (10.51 ± 7.23), 6 months (10.04 ± 8.83).
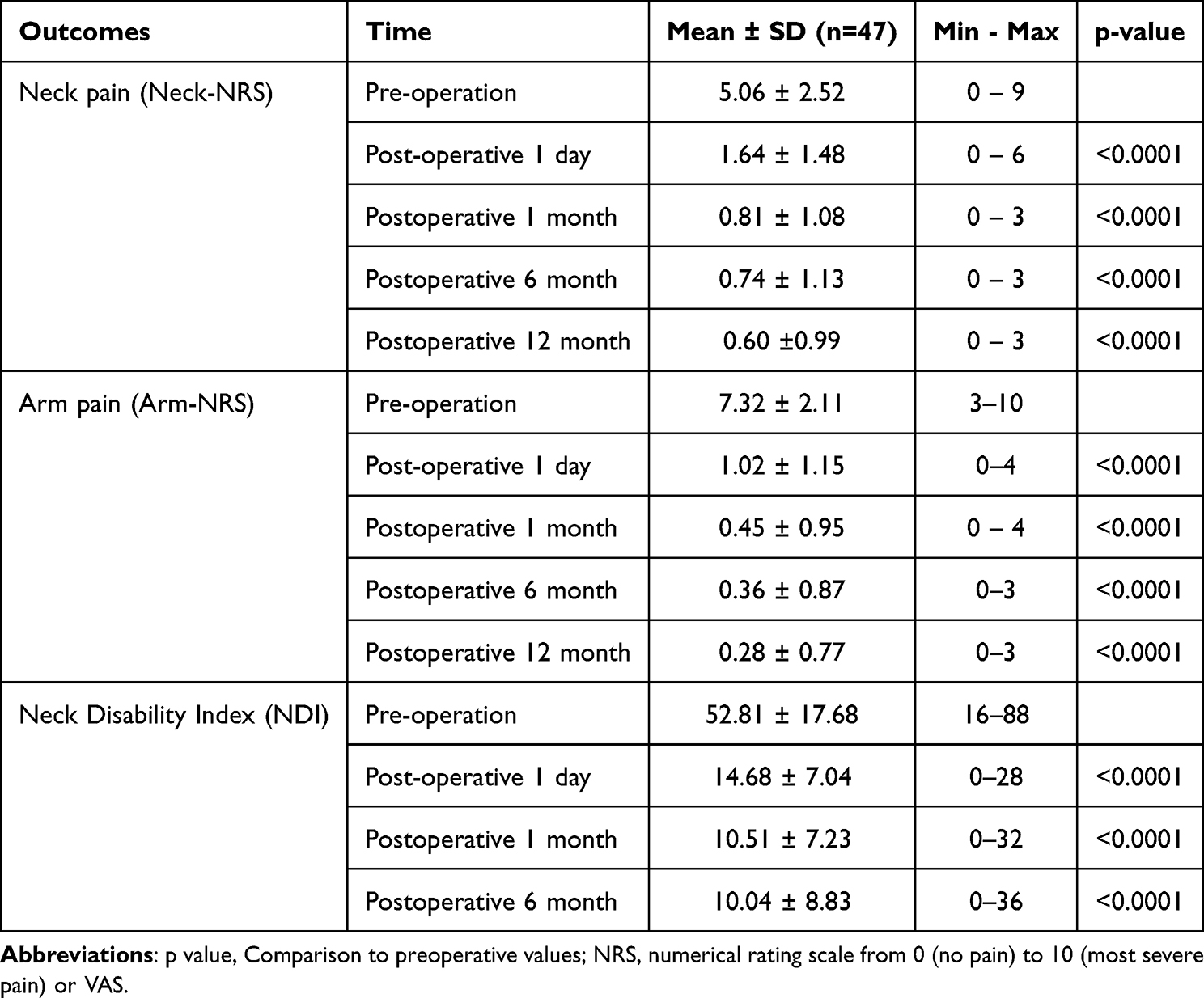 |
Table 4 The Efficacy of the Intervention on Neck Pain, Arm Pain, and Neck Disability |
Radiological outcomes were assessed in 47 patients who underwent spinal surgery, with measurements taken preoperatively and at 1, 6, and 12 months postoperatively, unless otherwise specified (Table 5). Surgical intervention significantly improved the cervical neural curvature from C2-C7 at all postoperative time points. The foraminal dimensions (diameter and area) showed significant immediate postoperative increase. Disc height decreased significantly, while cervical range of motion showed variable changes. C2-C7 SVA and T1 slope remained stable, indicating no significant changes in the global alignment. These improvements suggest successful decompression and expansion of the neural foramen after the surgery.
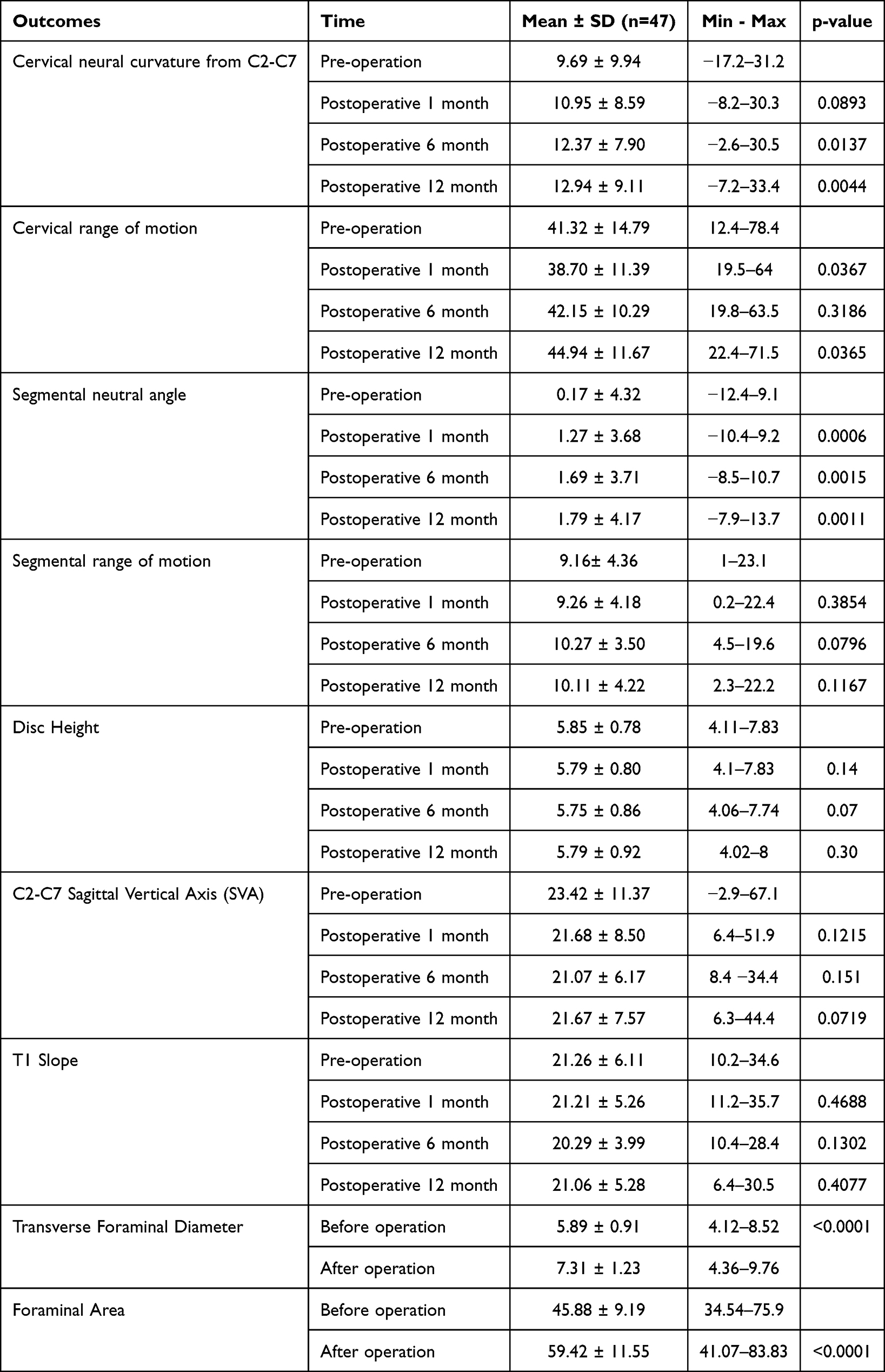 |
Table 5 Radiological Outcomes |
The cervical neural curvature from to C2-C7 was 9.69° ± 9.94°. Postoperatively, it increased to 10.95° ± 8.59° at 1 month (p = 0.0893), 12.37° ± 7.90° at 6 months (p = 0.0137), and 12.94° ± 9.11° at 12 months (p = 0.0044), indicating statistically significant improvement at 6 and 12 months. The Preoperative segmental neutral angle was 0.17° ± 4.32 Â °. It increased significantly to 1.27° ± 3.68° at one month (p = 0.0006), 1.69° ± 3.71° at six months (p = 0.0015), and 1.79° ± 4.17° at 12 months (p = 0.0011), demonstrating sustained improvement.
The segmental neutral angle and T1 slope did not change significantly after surgery. The preoperative C2-C7 SVA was 23.42 mm ± 11.37 mm. Postoperatively, it decreased to 21.68 mm ± 8.50 mm at 1 month (p = 0.1215), 21.07 mm ± 6.17 mm at 6 months (p = 0.151), and 21.67 mm ± 7.57 mm at 12 months (p = 0.0719). No significant changes were observed across time points. The preoperative T1 slope was 21.26° ± 6.11°. Postoperatively, it was 21.21° ± 5.26° at 1 month (p = 0.4688), 20.29° ± 3.99° at 6 months (p = 0.1302), and 21.06° ± 5.28° at 12 months (p = 0.4077), with no significant changes.
The Preoperative disc height was 5.85 ± 0.78 mm. It decreased slightly to 5.79 ± 0.80 mm at 1 month (p = 0.14), 5.75 ± 0.86 mm at 6 months (p = 0.07), and 5.79 ± 0.92 mm at 12 months (p = 0.30). Preoperative foraminal dimensions increasing significantly after surgery such as foraminal height (8.45 mm ± 1.04 mm to 9.10 mm ± 1.02 mm); transverse foraminal diameter (5.89 mm ± 0.91 mm to 7.31 mm ± 1.23 mm); foraminal area (45.88 mm2 ± 9.19 mm2 to 59.42 mm2 ± 11.55 mm2).
A total of 47 patients undergoing spinal surgery were evaluated using magnetic resonance imaging (MRI) to assess intervertebral disc degeneration and herniation characteristics before surgery, immediately after surgery, and 12 months post-surgery (Table 6). These findings highlight the effectiveness of surgical intervention in reducing the prevalence and severity of disc herniation, with stable disc degeneration grades over the 12-month follow-up period.
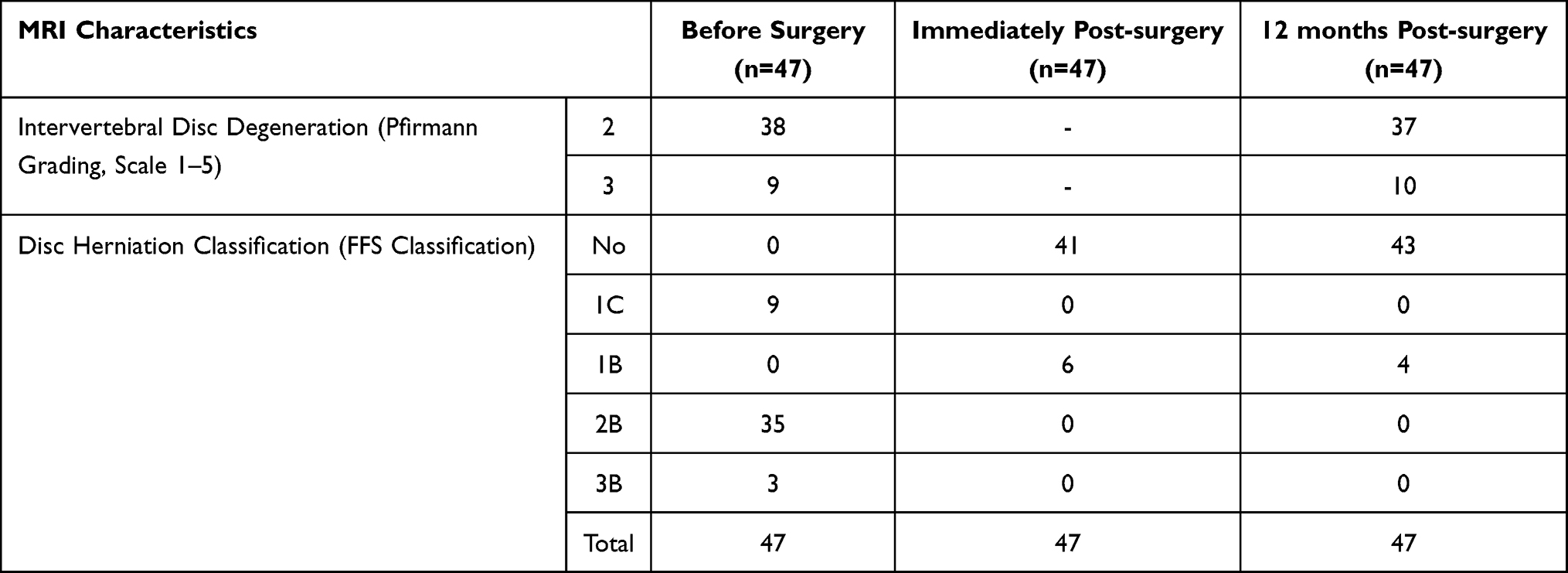 |
Table 6 Magnetic Resonance Imaging (MRI) to Assess Intervertebral Disc Degeneration and Herniation Characteristics Before Surgery |
Discussion
This study aimed to evaluate the efficacy and safety of single-level posterior endoscopic surgery (PES) for cervical disc herniation (CDH) in a Vietnamese cohort to address the gap in local data on minimally invasive spinal techniques. Cervical disc herniation (CDH) is a prevalent condition characterized by the protrusion or extrusion of intervertebral disc material into the spinal canal or neural foramen, often resulting in nerve root compression, radiculopathy, or myelopathy. Patients typically present with symptoms such as neck pain, arm pain, numbness, and in severe cases, motor weakness or coordination deficits. Traditional treatment approaches for CDH range from conservative management, such as physical therapy, medications, and epidural steroid injections, to surgical intervention when nonoperative measures fail to alleviate symptoms or when neurological deficits progress. Surgical intervention is often required if conservative measures fail.1 Traditional anterior cervical discectomy and fusion (ACDF) has been widely used, but its associated complications, such as dysphagia and adjacent segment disease, have prompted exploration of posterior endoscopic approaches.10 The intervention led to immediate and sustained reductions in neck pain, arm pain, and neck disability, with statistically significant improvements observed at all post-operative assessments compared with the pre-operative levels.11 In our study, the most pronounced changes occurred within the first postoperative day, followed by progressive stabilization at minimal pain and disability levels by 12 months, indicating both short-term efficacy and long-term benefits. The outcomes of this study align closely with recent global research on posterior endoscopic cervical discectomy (PECD); however, subtle differences highlight the influence of the technique, patient demographics, and study design. Dinh et al (2022), also at Viet Duc University Hospital, reported full-endoscopic posterior cervical foraminotomy and discectomy (PCFD) with a 95% symptom resolution rate and minimal complications in a cohort of 42 patients.12 A systematic review by Zhang et al (2022) analyzed studies on PECD and reported that the VAS scores one week after PECD for cervical disc herniation were significantly lower than those pre-operatively.13 This is in line with an another study showing that the 1-week postoperative and last follow-up arm and neck VAS scores were significantly reduced compared with the pre-operation scores.14 In a study on the changes after posterior full-endoscopic cervical foraminotomy, the pain-free survival rate was 91% for disc herniation and 83% for foraminal stenosis, with no significant difference between the groups.15 For the long-term outcome, mean VAS scores significantly improved at 1 month postoperatively compared to preoperative values, and these improvements were maintained at 2 years after surgery.16
The surgical outcomes in our study demonstrated a clinical success rate of 93.6%. Comparatively, a 2024 study by Tusheng Li et al reported an 88.10% success rate for ACDF (anterior cervical discectomy and fusion) procedures. Both surgical techniques for treating cervical disc herniation achieved favorable clinical results, significantly reducing patient pain and improving neurological function postoperatively. However, when comparing incision length and hospitalization duration, our endoscopic surgery demonstrated a significantly shorter incision length at 10.34 ± 0.7 mm and mean hospital stay of 2.07 ± 1.02 days, compared to ACDF with an incision length of 3.68 ± 0.29 cm and hospitalization of 8.07 ± 0.84 days. Regarding radiological outcomes, postoperative disc height increased and was well maintained in the ACDF group, as reported by Junyou Zhang et al in 2023. In contrast, our endoscopic group exhibited a gradual decrease in disc height over time, although this difference was not statistically significant. This reduction is likely attributed to the natural degeneration of disc tissues and more severe degeneration caused by surgical disruption of normal disc structure. Additionally, the C2-C7 lordotic angle and cervical spine range of motion (ROM) at C2-C7 significantly improved at 12 months postoperatively in our study, consistent with findings from ACDF studies such as Zhang’s 2023 investigation. Endoscopic surgery thus preserves neck mobility and biomechanical function without the use of internal fixation devices, avoiding complications related to implants and heterotopic ossification. ACDF remains a well-established gold standard, endoscopic cervical discectomy offers comparable clinical effectiveness with advantages of minimally invasive surgery, including shorter incisions, reduced hospital stay, preserved spinal motion, and fewer implant-related complications.
The majority of operated discs were at the C5-6 level (61.7%), followed by C6-7 (31.9%) and C4-5 (6.4%). A slight right-sided predominance was observed (55.3%) and most incisions were 10 mm (59.6%). Nearly all cases involved a ruptured herniation (97.9%) in the axillary position (93.6%). The mean treatment duration was 2.07 ± 1.02 months, ranging from 1 to 5 months. These findings highlight the uniformity of the pathological profile and technical consistency of the procedure in this cohort. The high prevalence of C5-6 herniations can be attributed to biomechanical stress at this level, where the cervical spine transitions from the relatively fixed upper segments to the more mobile lower segments. The axillary position of most herniations (93.6%) likely reflects the anatomical tendency of the disc material to migrate laterally toward the nerve root, causing radiculopathy, which is the primary indication for surgery. The posterior endoscopic approach allows direct access to the herniated disc fragment, minimizing disruption to posterior stabilizing structures such as the facet joints and ligaments. This approach likely contributes to the short treatment duration observed, as it reduces postoperative inflammation and accelerates recovery compared to open techniques.
The low overall complication rate (2.1% for most complications) supports the safety of posterior endoscopic surgery for cervical disc herniation, making it a viable alternative to the traditional open surgery. However, the relatively high rate of postoperative sensory disturbances (10.6%) suggests the need for refined surgical techniques such as improved visualization tools or intraoperative neuromonitoring to reduce nerve root irritation. The complications observed in this study can be linked to anatomical and technical challenges associated with posterior endoscopic cervical surgery. The complication rates observed in this study were consistent with those reported in literature on posterior endoscopic cervical surgery. A previous study has reported no nerve root injury, cerebrospinal fluid leakage, wound infection, or other complications.14 Another study showed one patient had transient motor palsy due to root retraction.16 This shows that this technique is safe and has the advantage of being minimally invasive.17
The incidence of neurological complications in our study was 6.4%, including two patients (4.3%) with intraoperative nerve root injury and one patient (2.1%) with transient neurological deficit. In a 2025 review by Vit Kotheeranurak et al, the most common postoperative complication was transient nerve root palsy, with an incidence of 1.15–4.5%, followed by intraoperative nerve injury at 0.88–1.5%.18 Thus, the complication rates observed in our study are higher than those reported by Kotheeranurak et al. This discrepancy may be attributed to the steep learning curve associated with posterior endoscopic cervical discectomy (PECD), which, despite being a minimally invasive technique, requires significant technical expertise. Additionally, the relatively small sample size and limited follow-up duration in our study may have contributed to the observed differences.
The significant improvement in cervical neural curvature likely results from decompression of neural structures and restoration of lordotic alignment through endoscopic removal of herniated disc material. This decompression reduces pressure on the spinal cord and nerve roots, as evidenced by the increased foraminal dimensions, which facilitate nerve root mobility and reduce radicular symptoms. The reduction in disc height may be attributed to the partial removal of disc material during surgery, which, while effective for decompression, compromises the disc integrity. The stability of the C2-C7 SVA and T1 slope suggests that single-level endoscopic surgery minimally affects global cervical alignment and preserves overall spinal balance. Variable changes in range of motion (ROM) reflect the balance between restored mobility from decompression and potential stiffness from surgical trauma or scar tissue formation. The observed improvements in cervical neural curvature align with findings from Chen et al, who reported that the difference was statistically significant when compared to preoperative (14.23±3.06°) to 1-week postoperative cervical curvature was (14.65 °±2.89)°, but there was no significant difference at 12 months (14.64±2.68°).14
A significant reduction in disc herniation prevalence was observed from 100% before surgery to 46.8% immediately after surgery and 25.5% at 12 months after surgery. Intervertebral disc degeneration, assessed using the Pfirrmann grading scale, remained relatively stable, with minor shifts from grade 2 to grade 3 in some patients over the 12-month period. These findings suggest that posterior endoscopic surgery effectively alleviates disc herniation, while maintaining disc integrity over time. The reduction in disc herniation observed in this study aligns with the findings from previous research on posterior endoscopic surgery. For instance, Ruetten et al (2008) reported a significant decrease in herniation prevalence postoperatively, with 87% of patients showing no residual herniation on MRI at 12 months.17 The observed reduction in disc herniation is likely due to the precise removal of herniated disc material via posterior endoscopic surgery, which minimizes disruption of the surrounding tissues. The endoscopic approach allows targeted decompression of neural structures and reduces the pressure on the spinal cord and nerve roots. The stability in Pfirrmann grades suggests that the procedure does not significantly accelerate disc degeneration, possibly because it preserves the annulus fibrosus and avoids excessive resection of disc tissue. This mechanism is supported by biomechanical studies indicating that endoscopic techniques maintain spinal stability better than open surgeries.19 The shift in herniation classification (eg, from Wang 2b to Wang 1b) reflects the resolution of extruded disc fragments, further alleviating neurological symptoms.
The need for such research is particularly pressing in developing countries, where access to advanced surgical technologies and specialized healthcare infrastructure is often limited. In countries such as Vietnam, for instance, the burden of spinal disorders is increasing due to aging populations, occupational hazards, and increasing road traffic injuries; however, the healthcare system faces challenges such as insufficient funding, shortage of trained neurosurgeons, and reliance.
Limitation
However, limitations include the relatively small sample size (n=47), which may limit generalizability, and the lack of a control group undergoing alternative treatments such as anterior cervical discectomy. Additionally, the 12-month follow-up period may not capture long-term outcomes such as potential disc degeneration beyond one year. Further studies with larger cohorts and longer follow-up periods are needed to address these gaps. Despite limitations such as a small sample size and short follow-up period, the results contribute to the growing evidence base for endoscopic spine surgery, with implications for improved patient outcomes and healthcare delivery in Vietnam.
Conclusion
This study demonstrated that single-level full endoscopic posterior cervical foraminotomy and herniectomy are safe in the short-term with 12 months of follow-up and effective in the treatment of cervical disc herniation. Further study is needed with a larger sample size, with control group and long-term follow-up.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The research was conducted following the guidelines and approval of the Ethics Committee of Hanoi Medical University (No. 812/GCN-HĐĐĐNCYSH-ĐHYHN, dated March 3, 2023). All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and the Helsinki Declaration of 1975, revised in 2013. Written informed consent was obtained from all the participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Hung The Dinh and Son Ngoc Dinh are co-first authors for this study. The authors declare that they have no conflicts of interest regarding the content of this article.
References
1. Sharrak S, Al Khalili Y. Cervical disc herniation. In: StatPearls. StatPearls Publishing; 2019.
2. Radhakrishnan K, Litchy WJ, O’fallon WM, Kurland LT. Epidemiology of cervical radiculopathy: a population-based study from Rochester, Minnesota, 1976 through 1990. Brain. 1994;117(2):325–335. doi:10.1093/brain/117.2.325
3. Bertalanffy H, Eggert H-R. Clinical long-term results of anterior discectomy without fusion for treatment of cervical radiculopathy and myelopathy: a follow-up of 164 cases. Acta neurochirurgica. 1988;90:127–135. doi:10.1007/BF01560567
4. Donaldson JW, Nelson PB. Anterior cervical discectomy without interbody fusion. Surg Neurol. 2002;57(4):219–224. doi:10.1016/S0090-3019(02)00638-9
5. Mehren C, Suchomel P, Grochulla F, et al. Heterotopic ossification in total cervical artificial disc replacement. Spine. 2006;31(24):2802–2806. doi:10.1097/01.brs.0000245852.70594.d5
6. Wirth FP, Dowd GC, Sanders HF, Wirth C. Cervical discectomy: a prospective analysis of three operative techniques. Surg Neurol. 2000;53(4):340–348. doi:10.1016/S0090-3019(00)00201-9
7. Witzmann A, Hejazi N, Krasznai L. Posterior cervical foraminotomy. A follow-up study of 67 surgically treated patients with compressive radiculopathy. Neurosurg Rev. 2000;23:213–217. doi:10.1007/PL00011957
8. Wang S, Zhao T, Han D, et al. Classification of cervical disc herniation myelopathy or radiculopathy: a magnetic resonance imaging-based analysis. Quant Imaging Med Surg. 2023;13(8):4984–4994. doi:10.21037/qims-22-1387
9. Alomar SA, Maghrabi Y, Baeesa SS, L. Alves Ó. Outcome of anterior and posterior endoscopic procedures for cervical radiculopathy due to degenerative disk disease: a systematic review and meta-analysis. Global Spine J. 2022;12(7):1546–1560. doi:10.1177/21925682211037270
10. Carrier CS, Bono CM, Lebl DR. Evidence-based analysis of adjacent segment degeneration and disease after ACDF: a systematic review. Spine J. 2013;13(10):1370–1378. doi:10.1016/j.spinee.2013.05.050
11. Bhatia S, Brooks NP. Posterior endoscopic cervical foraminotomy. Neurosurg Clin N Am. 2020;31(1):9–16. doi:10.1016/j.nec.2019.08.001
12. Dinh SN, Dinh HT. The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital. Sci Rep. 2022;12(1):8314. doi:10.1038/s41598-022-12493-x
13. Zhang J, Zhou Q, Yan Y, et al. Efficacy and safety of percutaneous endoscopic cervical discectomy for cervical disc herniation: a systematic review and meta-analysis. J Orthopaedic Surg Res. 2022;17(1):519. doi:10.1186/s13018-022-03365-1
14. Chen BL, Li YJ, Lin YP, et al. [Clinical outcomes of cervical disc herniation treated by posterior percutaneous endoscopic cervical discectomy]. Zhonghua Wai Ke Za Zhi. 2017;55(12):923–927. doi:10.3760/cma.j.issn.0529-5815.2017.12.009
15. Paik S, Choi Y, Chung CK, et al. Cervical kinematic change after posterior full-endoscopic cervical foraminotomy for disc herniation or foraminal stenosis. PLoS One. 2023;18(2):e0281926. doi:10.1371/journal.pone.0281926
16. Youn MS, Shon MH, Seong YJ, et al. Clinical and radiological outcomes of two-level endoscopic posterior cervical foraminotomy. Eur Spine J. 2017;26:2450–2458. doi:10.1007/s00586-017-5017-7
17. Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic cervical posterior foraminotomy for the operation of lateral disc herniations using 5.9-mm endoscopes: a prospective, randomized, controlled study. Spine. 2008;33(9):940–948. doi:10.1097/BRS.0b013e31816c8b67
18. Kotheeranurak V, Lokhande PV, Tangdamrongtham T, et al. Complications in full-endoscopic posterior cervical surgery: a review of the literature and preventive strategies. Global Spine J. 2025;21925682251328615.
19. Panjabi MM. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis. Clin Spine Surg. 1992;5(4):390–397.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.