Back to Journals » Clinical Ophthalmology » Volume 19
Clinical and Patient-Reported Outcomes After Mix-and-Match Implantation of a Trifocal and Non-Diffractive Extended Depth of Focus IOL
Received 8 April 2025
Accepted for publication 28 July 2025
Published 9 August 2025 Volume 2025:19 Pages 2625—2635
DOI https://doi.org/10.2147/OPTH.S533091
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Irene S Zhou,1 Dagny C Zhu2
1School of Medicine, Rutgers New Jersey Medical School, Newark, NJ, USA; 2NVISION Eye Centers, Rowland Heights, CA, USA
Correspondence: Irene S Zhou, School of Medicine, Rutgers New Jersey Medical School, Newark, NJ, 07103, USA, Tel +1 626-833-0435, Email [email protected]
Purpose: To evaluate cataract surgery outcomes following mix-and-match implantation of a trifocal and extended-depth-of-focus (EDOF) intraocular lens (IOL).
Setting: Single center, private practice.
Design: Single arm, non-interventional, ambispective study.
Methods: Patients who underwent femtosecond-laser assisted cataract surgery with mix-and-match implantation of the Clareon PanOptix trifocal IOL in the non-dominant eye and Clareon Vivity EDOF IOL in the dominant eye from September 2022 to November 2023 were reviewed. Only healthy eyes with postoperative absolute spherical equivalent (SE) ≤ 0.50 diopters (D) and cylinder ≤ 0.75 D were included. At 3 months postoperatively, binocular corrected and uncorrected visual acuity at distance (CDVA and UDVA), intermediate (DCIVA and UIVA), and near (DCNVA and UNVA) along with patient-reported outcomes (QUVID and IOLSAT questionnaires) were assessed.
Results: 100 eyes of 50 patients were included. Postoperatively, the mean binocular CDVA and UDVA was − 0.08 ± 0.05 logMAR and − 0.06 ± 0.05 logMAR, respectively. Overall, 100%, 98%, and 90% of patients achieved binocular UDVA, UIVA, and UNVA of 20/25 or better, respectively. Eighty-four percent of patients reported complete spectacle independence. Few patients were “bothered very much” by haloes, glare, or starbursts (0– 4%). No patients reported dissatisfaction with their vision. Overall, 94% and 92% of patients would elect the same IOLs and recommend the same procedure to friends and family, respectively.
Conclusion: Mix-and-match implantation of the Clareon PanOptix and Vivity IOLs yields good patient satisfaction potentially by combining the advantages of each lens resulting in a high degree of satisfaction and low rates of visual disturbances.
Keywords: EDOF IOL, mix-and-match, trifocal IOL
Introduction
Cataracts are the leading cause of treatable blindness worldwide.1 Several intraocular lens (IOL) technologies exist, each with advantages and disadvantages. Monofocal IOLs utilize a single focal point primarily for distance vision, but spectacles are often required for near and intermediate vision.2 In contrast, multifocal IOLs provide a greater range of vision, but may result in decreased contrast or nighttime dysphotopsias.3,4
The Clareon PanOptix (Alcon, Fort Worth, TX) is a non-apodized, diffractive, trifocal IOL made of a new hydrophobic acrylic material incorporating hydroxyethyl methacrylate (HEMA), which reduces IOL glistenings and enhances optical clarity.5–7 With three focal points at distance, intermediate (+2.17D, 60 cm), and near (+3.25D, 40 cm), the PanOptix provides full-range vision.6,7 It utilizes a quadrifocal design to ensure a comfortable working distance of 60 cm for intermediate tasks (eg, computer work) and redistributes the light energy at 120 cm to distance. Bilateral PanOptix implantation delivers high spectacle independence and patient satisfaction, though slight tradeoffs in contrast sensitivity and dysphotopsias persist.7–9
In contrast, non-diffractive, extended depth of focus (EDOF) IOLs reduce dysphotopsias and deliver a more natural extended focal range compared to monofocal IOLs, but provide less reading power than trifocals.8,10 The Clareon Vivity (Alcon, Fort Worth, TX) is an EDOF IOL that uses a wavefront-shaping technology to stretch and shift the wavefront, enhancing visual range without splitting light.11 The extended range is achieved by two surface elements over the central 2.2 mm optic: a slightly elevated (~1 µm) plateau that stretches the wavefront by delaying paraxial light rays as they pass through the IOL medium and a small curvature change that shifts the wavefront anterior to the retina to use all available light. These mechanisms enable the lens to provide excellent distance and intermediate vision (66 cm) while enabling functional near vision.11–13 Though its spectacle independence rate is lower than that of a trifocal, bilateral Vivity implantation offers a functional range of vision with fewer nighttime visual disturbances compared to multifocal and diffractive EDOF IOLs.13–16
Recently, more surgeons are leveraging binocular summation to give patients the widest range of vision with the least degree of visual disturbances by implanting a full-range multifocal IOL in the non-dominant eye and an EDOF IOL in the dominant eye.17,18 Only one study has evaluated this approach with the AcrySof PanOptix and Vivity IOLs in a limited fashion.19 This is the first comprehensive study assessing visual outcomes and patient satisfaction following mix-and-match implantation of the Clareon PanOptix and Clareon Vivity IOLs for cataract surgery.
Methods
This was a single-armed, non-interventional, ambispective case series performed at a single-surgeon, private practice. All charts of patients who underwent routine, uncomplicated femtosecond laser-assisted cataract surgery with mix-and-match implantation of the Clareon PanOptix trifocal IOL in the non-dominant eye and the Clareon Vivity EDOF IOL in the dominant eye between September 27, 2022 and November 21, 2023 were reviewed. In order to better assess IOL performance, only healthy eyes with postoperative absolute spherical equivalent (SE) ≤ ± 0.50 diopters (D) and cylinder ≤ 0.75 D were included for study evaluation at 3 months to eliminate refractive outliers that could otherwise affect outcomes such as spectacle independence, nighttime visual disturbances, and satisfaction. Patients with a history of keratorefractive surgery and/or underlying corneal, retinal, or optic nerve pathologies were excluded. The study adhered to the principles of the Declaration of Helsinki and was approved by the ethics committee of the Salus Institutional Board (IRB #23038). Prior to any study-specific testing, all patients provided written informed consent.
At the routine preoperative visit, a slit lamp and dilated fundus exam were performed. Snellen monocular uncorrected distance visual acuity (UDVA), monocular corrected distance visual acuity (CDVA), binocular Jaeger uncorrected near visual acuity (UNVA), and binocular distance-corrected near visual acuity (DCNVA) were assessed. Eye dominance was assessed by asking the patient to create a triangular opening with both hands and then centering the opening on a distant object with both eyes open. The patient was then asked to close each eye and assess which opened eye allowed the object to stay centered (ie the dominant eye). In equivocal cases, a loose trial lens (+2.00 D) was held in front of each eye (over their refractive correction) to determine which eye the patient preferred the add in (ie the non-dominant eye). Manifest refraction, brightness acuity testing (BAT), optical biometry (Carl Zeiss IOL Master 500, Germany; Alcon Argos, Fort Worth, TX), corneal tomography (Oculus Pentacam, Wetzlar, Germany), specular microscope (Konan SP-9000, Hyogo, Japan), and optical coherence tomography of the optic nerve head and macula (Optovue iVue, Fremont, CA) were obtained. IOL calculations were done using the Barrett II Universal (https://calc.apacrs.org/barrett_universal2105/) and the Barrett toric calculator (www.ascrs.org/tools/barrett-toric-calculator). The A-constants 119.1 and 119.2 were used for the Clareon PanOptix and Vivity IOLs, respectively. Emmetropia was targeted for both eyes.
One experienced surgeon completed all cataract surgeries using a femtosecond laser (LensAR Inc, Winter Park, FL, USA) to perform a 5.0 mm capsulotomy, lens fragmentation, arcuate incisions for mild corneal astigmatism correction (toric IOL used for ≥ 0.75 D against-the-rule and ≥ 1.25 D with-the-rule astigmatism), and a 2.4 mm clear corneal incision. Each patient underwent immediate sequential bilateral cataract surgery (ISBCS) with separate and thorough sterilization of all supplies and instruments between eyes according to the ISBCS Principles of Excellence. A Clareon PanOptix IOL was implanted in the non-dominant eye, and Clareon Vivity IOL in the dominant eye. All cases were performed under topical anesthesia combined with one MKO Melt tab (midazolam, ketamine, ondansetron; Melt Pharmaceuticals, Inc. Brentwood, TN), oral midazolam, or without oral sedation. Phacoemulsification was completed with the Centurion (Alcon, Fort Worth, TX), and dilute 0.16% moxifloxacin (ImprimisRx, Carlsbad, CA) was injected intracamerally at the end of each case. A postoperative compounded drop (prednisolone acetate 1%, moxifloxacin 0.5%, and bromfenac 0.075%; ImprimisRx, Carlsbad, CA) was used four times daily on a tapering schedule for 4 weeks.
At 3 months, study assessments were performed, including binocular CDVA, monocular UDVA and CDVA, binocular uncorrected intermediate visual acuity (UIVA) and distance-corrected intermediate visual acuity (DCIVA) at 66 cm, binocular UNVA and DCNVA at 40 cm, and manifest refraction spherical equivalent (MRSE). Manifest refraction was completed in a standard 6 m optical lane, and all ETDRS distance visual acuity measurements were obtained in a 4 m lane with an infinity adjustment using a +0.25 D lens. Distance visual acuity was collected using an ETDRS chart (luminance 85 cd/m2), and intermediate and near visual acuities were measured with ETDRS cards designed to be used at 66 cm and 40 cm, respectively. Patients also completed two validated questionnaires. The QUVID (Copyright 2017, Alcon Research, LLC – All rights reserved) assesses visual disturbances using illustrative examples of different dysphotopsia types.20 The IOLSAT (Copyright 2017, Alcon Research, LLC – All rights reserved) assesses spectacle independence and overall patient satisfaction.
Statistical analyses were done using MATLAB (Natick, Massachusetts: The MathWorks Inc). Mean and standard deviation were calculated for continuous variables (eg, logarithm of the minimum angle of resolution (logMAR) visual acuity); percentage and number of eyes were reported for categorial variables (eg, Snellen visual acuity). Continuous variables were compared using a two-tailed Student’s t test and categorical values with a Chi-Square test. A p value <0.05 was considered significant.
Results
A total of 185 consecutive cataract patient charts that had undergone routine femtosecond laser-assisted cataract surgery with mix-and-match implantation of the Vivity and PanOptix IOLs were reviewed. Of these, 135 did not meet inclusion/exclusion criteria, with the majority of patients falling outside the 3-month study window or having had a history of refractive surgery or underlying amblyopia. Overall refractive accuracy was high with over 90% of eyes reviewed achieving ≤ ± 0.50 D SE, but only eyes that met the refractive inclusion criteria were included. In total, one hundred eyes of 50 patients (56% female) were enrolled and analyzed at 3 months (mean 99.4 ± 13.7 days) with a mean age of 57 ± 6 years. The mean preoperative SE was +1.57 ± 1.42 diopters (D). Patient demographics preoperative data are demonstrated in Table 1.
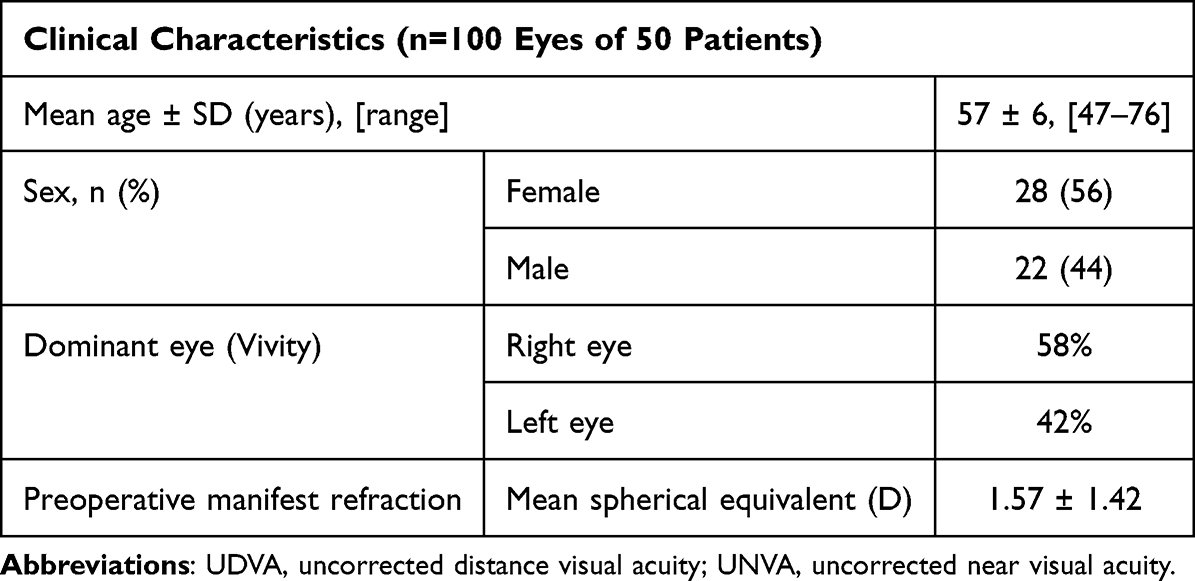 |
Table 1 Preoperative and Demographic Data |
Best-Corrected Visual Acuity
The 3-month monocular CDVA and binocular CDVA, DCIVA, and DCNVA are summarized in Figure 1 and Table 2. Binocularly, the mean CDVA was −0.08 ± 0.05 logMAR (Snellen 20/17), with 100% (50) of patients achieving 20/20 or better (Figure 1A). Monocularly, the mean CDVA was −0.03 ± 0.05 logMAR (approximately 20/19) (Figure 1B). Ninety-nine percent (99) and 100% (100) of eyes achieved of 20/20 and 20/25 or better, respectively.
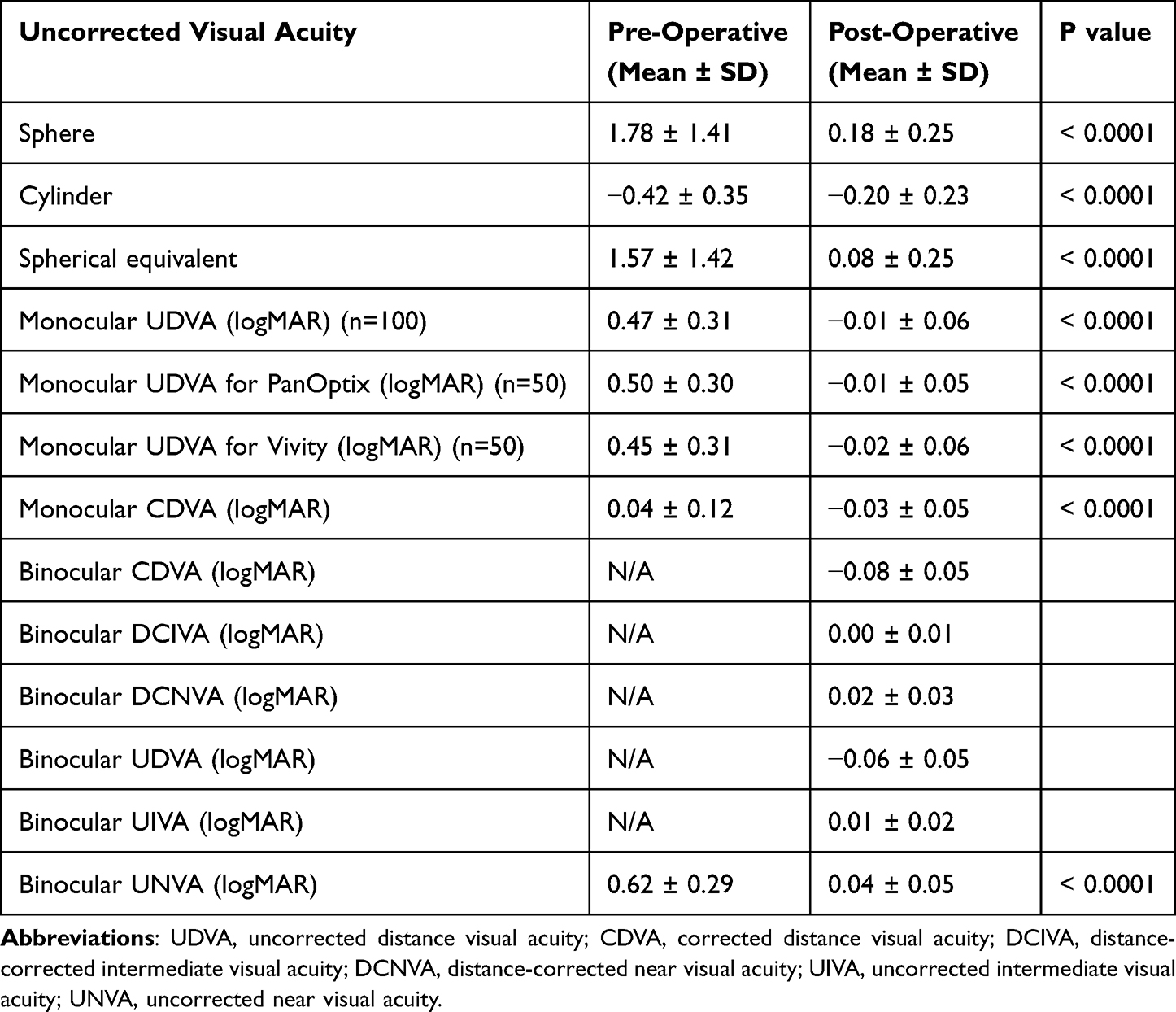 |
Table 2 Pre- and Post-Operative Visual Acuity and Refractive Outcomes |
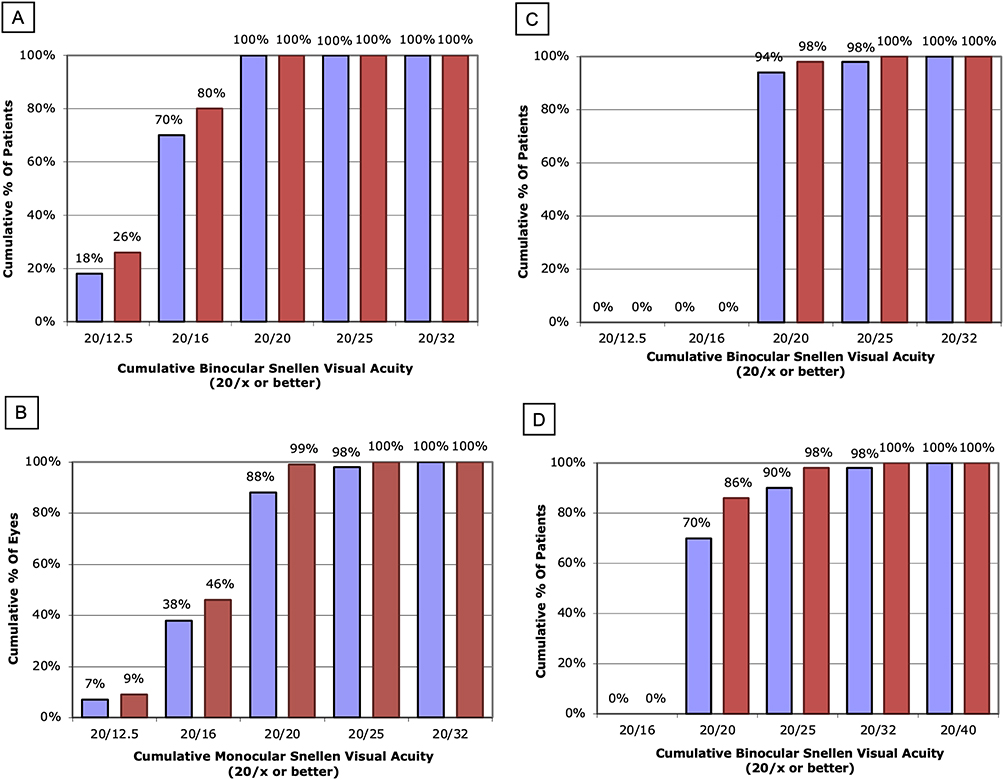 |
Figure 1 Cumulative uncorrected and best-corrected visual acuity at 3 months postoperatively. (A) Cumulative binocular uncorrected and best-corrected distance visual acuity at 3 months postoperatively. 50 patients (plano target) at 3 months postop. The purple bar represents postop UDVA. The red bar represents postop CDVA. (B) Cumulative monocular uncorrected and best-corrected distance visual acuity at 3 months postoperatively. 100 eyes (plano target) at 3 months postop. The purple bar represents postop UDVA. The red bar represents postop CDVA. (C) Cumulative binocular uncorrected and best-corrected intermediate visual acuity at 3 months postoperatively. 50 patients (plano target) at 3 months postop. The purple bar represents postop UIVA. The red bar represents postop DCIVA. (D) Cumulative binocular uncorrected and best-corrected near visual acuity at 3 months postoperatively. 50 patients (plano target) at 3 months postop. The purple bar represents postop UNVA. The red bar represents postop DCNVA. Abbreviations: UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity: UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity: UIVA, uncorrected intermediate visual acuity; DCIVA, distance-corrected intermediate visual acuity: UNVA, uncorrected near visual acuity; DCNVA, distance-corrected near visual acuity. |
At intermediate, the mean binocular DCIVA was 0.00 ± 0.01 logMAR (Snellen 20/20), with 98% (49) and 100% (50) of patients achieving 20/20 and 20/25 or better, respectively (Figure 1C).
At near, the mean binocular DCNVA was 0.02 ± 0.03 logMAR (Snellen 20/20), with 86% (43), 98% (49), and 100% (50) of patients achieving 20/20, 20/25, and 20/32 or better, respectively (Figure 1D).
Uncorrected Visual Acuity
The 3-month monocular UDVA and binocular UDVA, UIVA, and UNVA are summarized in Figure 1 and Table 2. Binocularly, the mean UDVA was −0.06 ± 0.05 logMAR (Snellen 20/17), with 100% (50) of patients achieving 20/20 or better (Figure 1A). The mean postoperative monocular UDVA was −0.01 ± 0.06 logMAR (Snellen 20/19). Eighty-eight percent (88), 98% (98), and 100% (100) of eyes achieved 20/20, 20/25, and 20/32 or better, respectively (Figure 1B).
At intermediate, the mean binocular UIVA was 0.01 ± 0.02 logMAR (Snellen 20/20), with 94% (47), 98% (49), and 100% (50) of patients achieving 20/20, 20/25, and 20/32 or better, respectively (Figure 1C).
At near, the mean binocular UNVA was 0.04 ± 0.05 logMAR (Snellen 20/22), with 70% (35), 90% (45), and 98% (49) of patients achieving 20/20, 20/25, and 20/32 or better, respectively (Figure 1D).
Refractive Outcomes
Table 2 shows a statistically significant reduction of sphere, cylinder, and SE at 3 months. Seventy-four percent (74) and 94% (94) of eyes achieved UDVA same or better than CDVA and UDVA within 1 Snellen line of CDVA, respectively (Figure 2A). The mean postoperative SE was 0.08 ± 0.25 D, which was close to the intended plano target for both eyes. All eyes fell within ± 0.50 D of emmetropia per inclusion criteria (Figure 2B). Refractive cylinder was ≤ 0.50 D in 95% (95) of eyes (Figure 2C).
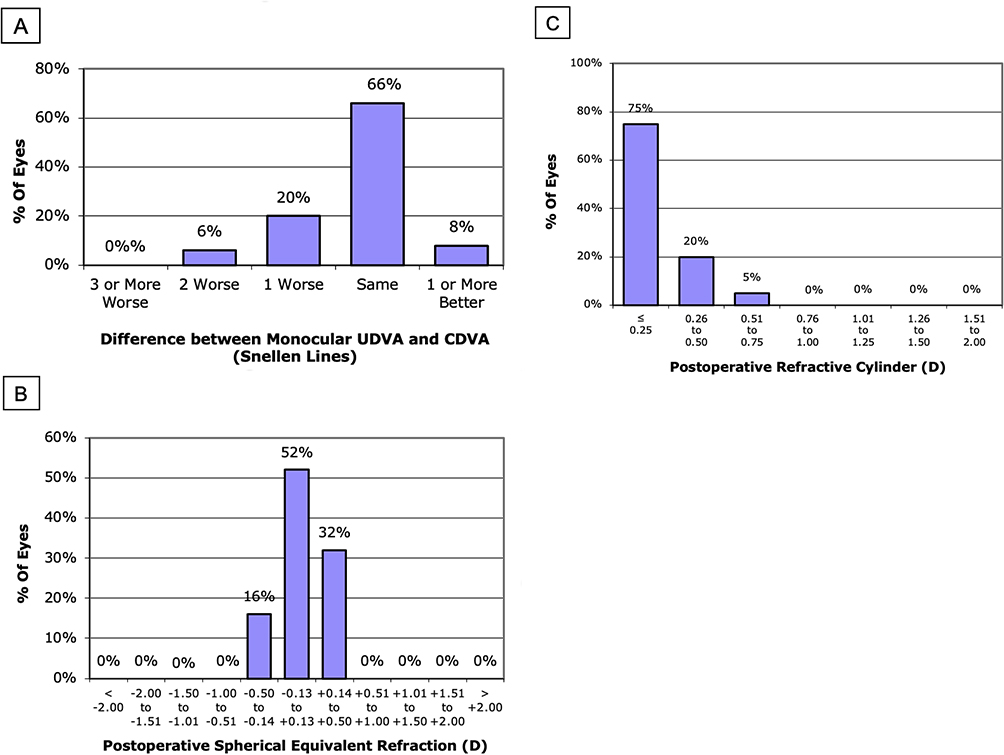 |
Figure 2 Spherical equivalent refraction at 3 months postoperatively. (A) Difference in Snellen lines between postoperative UDVA and CDVA. 100 eyes (plano target) at 3 months postop. UDVA same or better than CDVA: 74%. UDVA within 1 line of CDVA: 94%. (B) Spherical equivalent refraction accuracy. 100 eyes at 3 months postop. ± 0.50 (D) 100%. ± 1.00 (D) 100%. (C) Postoperative refractive cylinder distribution. 100 eyes at 3 months postop. ≤ 0.50 (D) 95%. ≤ 1.00 (D) 100%. Abbreviations: UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity. |
Patient-Reported Outcomes
Visual Disturbances (QUVID Questionnaire)
The patient-reported frequency of visual disturbances at 3 months is summarized in Table 3. Most patients reported “never” experiencing starbursts, haloes, or glare (58%, N=29, 62%, N=31, and 64%, N=32, respectively). The most commonly reported visual disturbances overall were starbursts (42%, N=21), haloes (38%, N=19), and glare (36%, N=18) followed by hazy vision (24%, N=12), blurred vision (20%, N=10), “dark area” (ie, negative dysphotopsia; 18%, N=9), and double vision (6%, N=3).
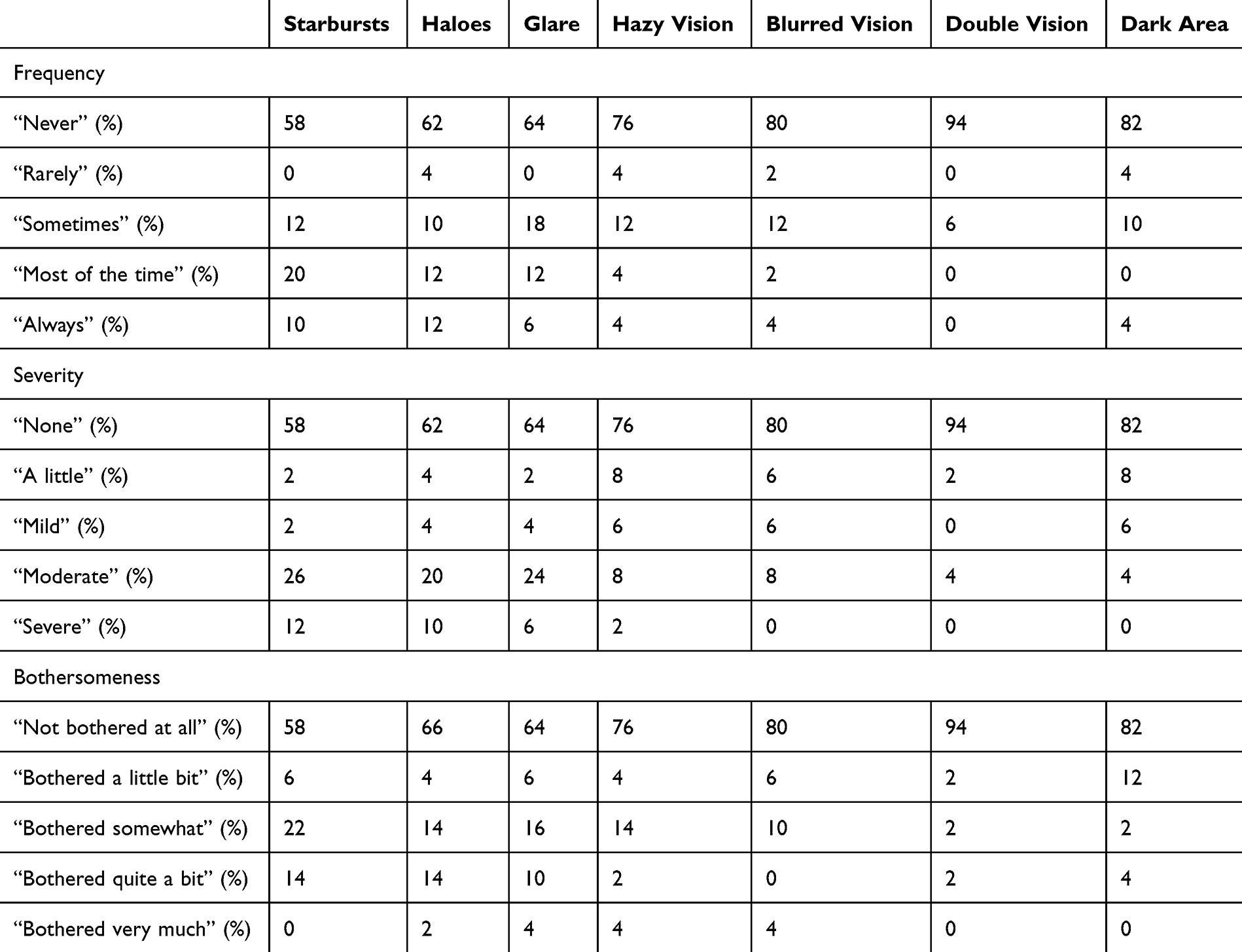 |
Table 3 Patient-Reported Frequency, Severity, and Bothersomeness of Visual Disturbances at 3 Months Postoperatively (n=50) |
The patient-reported severity and bothersomeness of visual disturbances at 3 months is summarized in Table 3. The majority rated their positive dysphotopsias as “none” to “mild” or “not bothered at all”. Starbursts, haloes, and glare were rated as “severe” by 12% (6), 10% (5), and 6% (3) of patients, respectively (p = 0.20) (Table 3). Only 0% (0), 2% (1), and 4% (2) of patients reported being “bothered very much” by starbursts, haloes, and glare, respectively (p = 0.39) (Table 3).
Spectacle Independence (IOLSAT Questionnaire)
At 3-months, most patients (84%, N=42) reported “never” needing glasses for any distance in the last 7 days (Supplemental Table 1A). For patients that needed glasses, only 4% (2), 8% (4), and 4% (2) of patients reported needing glasses “most of the time”, “sometimes”, or “rarely”, respectively (Supplemental Table 1A). Overall, 98% (49), 94% (47), and 86% (43) of patients reported never needing glasses to see far away, at arm’s length, or up close, respectively (Supplemental Table 1A). The majority of patients reported “good” or “very good” vision without glasses at all distances under bright (Supplemental Table 1B) and dim lighting (Supplemental Table 1C).
Patient Satisfaction (IOLSAT Questionnaire)
Overall, 90% (45) of patients reported being “satisfied” or “very satisfied” with their vision. Ten percent (5) of patients were “neither satisfied nor dissatisfied”. No patients were “dissatisfied” or “very dissatisfied”. When asked if they would choose the same lens again, 94% (47) of patients responded “yes” and 92% (46) would recommend the same surgery to others. Negative feedback was attributed to dry eye symptoms, light sensitivity, floaters, and inadequate reading vision.
Adverse Events
No perioperative complications were seen. No eye lost more than one line of CDVA compared to pre-op (p < 0.001). No IOL exchanges or enhancements were required.
Discussion
Patients have increasingly higher expectations following cataract surgery. Diffractive multifocal IOLs offer full-range vision, but postoperative visual disturbances may lead to dissatisfaction. Non-diffractive EDOF IOLs minimize these dysphotopsias but increase reliance on spectacles for up-close work. Combining IOLs as a surgical approach could potentially balance these benefits and drawbacks.
Gunenc and Celik hypothesized that contralateral implantation of different multifocal IOLs (eg, diffractive and refractive) could enhance vision and satisfaction.17,18,21 Earlier mix-and-match studies evaluated a low-add power bifocal IOL in the dominant eye and a high-add power bifocal IOL in the non-dominant eye to fill in gaps for a better range of vision.22,23 Since the advent of newer EDOF IOLs along with trifocal and continuous-range multifocal IOLs, several studies have assessed visual outcomes with various EDOF, diffractive, and refractive IOL combinations.19,24–27 These include combinations such as Symfony with Synergy, FineVision Triumf with FineVision HP, and AT LARA with AT LISA.
To our knowledge, this is the first study evaluating mix-and-match outcomes of Clareon PanOptix and Vivity EDOF IOLs in cataract patients. A previous study assessed a mix-and-match approach using the older AcrySof PanOptix and Vivity IOL models (n=30 patients) but did not specifically evaluate dysphotopsias, spectacle independence, or patient satisfaction.19 However, it found that the mix-and-match approach yielded the best defocus curve, visual range, and visual function scores (NEI-VFQ 25) compared to bilateral PanOptix and bilateral Vivity.19 This supports the positive findings highlighted in our study. It is also worth noting that the Clareon model may offer better visual quality outcomes than the previous AcrySof model, as it is made from a hydrophobic acrylic material with HEMA that reduces IOL glistenings and improves optical clarity, all of which can affect optical performance over time. While this improvement is promising, further research is needed to confirm its long-term impact on patient satisfaction and visual outcomes.
Photic phenomena impact postoperative visual quality and satisfaction. In our study, implanting a non-diffractive EDOF IOL in the dominant eye may have resulted in significantly fewer visual disturbances compared to bilateral trifocal IOLs. Unlike some bilateral PanOptix studies where the majority of patients have experienced haloes, starbursts, and/or glare, most patients (58–64%) in our study reported “none” at 3 months.28,29 Furthermore, a lower percentage of our mix-and-match patients (0%) were “bothered very much” by starbursts compared to bilateral PanOptix patients (4.8%), with starbursts being the most bothersome dysphotopsia in several diffractive IOL studies. This reduced incidence of bothersome dysphotopsias is a key benefit of the mix-and-match approach.
A recent meta-analysis found very low rates of “severe” and “very bothersome” dysphotopsias (5% and 3%, respectively) for bilateral PanOptix, similar to our mix-and-match outcomes.29 This may reflect our relatively younger demographic with milder cataracts and better baseline vision (with a lower tolerance for visual disturbances). However, only 3 of the 11 studies utilized the same QUVID questionnaire, potentially affecting data interpretation. Studies evaluating direct head-to-head of mix-and-match versus bilateral implantation trials with Vivity and PanOptix IOLs are limited. Further research is needed to validate the reduced incidence of dysphotopsias observed with the mix-and-match approach through a prospective head-to-head study.
Our previous study on bilateral PanOptix in refractive lens exchange (RLE) patients also reported higher rates of positive dysphotopsias, with 36% and 26% of patients reporting “severe” and “most bothersome” starbursts at 6 months, respectively.4 Direct comparisons are challenging due to differing dissatisfaction thresholds between RLE and cataract patients. Nonetheless, the mix-and-match Vivity/PanOptix approach appears to provide a low rate of bothersome dysphotopsias and may be a better option for patients who drive frequently at night.
Conversely, bilateral Vivity studies have reported lower rates of dyshotopsias compared to our mix-and-match study. McCabe et al found that most Vivity patients were not bothered at all by positive dysphotopsias (74–83%), similar to the monofocal IOL cohort in the AcrySof Vivity FDA trial.30 Scheepers et al reported that only 11.8% experienced starbursts, haloes, and glare utilizing the same QUVID questionnaires as McCabe et al and our study.16 Zero percent, 0%, and 2.9% of their patients reported being “bothered quite a bit” or “bothered very much” by starbursts, haloes, and glare, respectively, compared to approximately 15% of our patients. This is to be expected given that a diffractive trifocal IOL was implanted in the contralateral eye in our study.
Interestingly, our Vivity and PanOptix mix-and-match approach demonstrated fewer visual disturbances compared to other combinations, including those with a diffractive EDOF IOL in the dominant eye and a diffractive mixed EDOF/multifocal IOL in the non-dominant eye. Soscia et al found that over 70% of mix-and-match TECNIS Symfony EDOF (Johnson & Johnson Vision) and TECNIS Synergy IOL (Johnson & Johnson Vision) patients experienced haloes.31 Similarly, Acar and Tabakci reported that 60% of mix-and-match Zeiss AT LISA trifocal and AT LARA EDOF IOL patients experienced haloes.22 Still, they noted better nighttime driving satisfaction and contrast sensitivity with the mix-and-match versus bilateral trifocal approach.22 Our study’s lower dysphotopsia rates likely stem from Vivity’s non-diffractive nature and the PanOptix IOL’s optical design that utilizes 88% of total light.16 Thus, combining Vivity and PanOptix does appear to decrease visual disturbances compared to other mix-and-match IOL approaches.
While bilateral Vivity results in fewer dysphotopsias, we achieved a much higher rate of complete spectacle independence (84%) with mix-and-match than what has been reported for bilateral Vivity, reflecting the main advantage of implanting a trifocal IOL in the non-dominant eye. McCabe et al reported only 21.6% complete spectacle independence with bilateral Vivity implantation (plano aim) in the AcrySof Vivity trial.30 With a mini-monovision approach, Van Amelsfort et al reported 38% spectacle independence at near, compared to 86% in our study.32 Our complete spectacle independence rate also surpassed the 70% reported by Soscia et al for mix-and-match Synergy and Symfony patients, likely due to variations in optical designs.31
Compared to bilateral PanOptix, our complete spectacle independence of 84% was lower than the 91.6% reported in a recent meta-analysis analyzing spectacle independence for bilateral PanOptix.33 However, individual bilateral PanOptix studies have reported rates of 80–85% similar to ours.34,35 Notably, 90% of our mix-and-match patients reported never or rarely needing glasses to see at near, approaching the pooled spectacle independence rate of bilateral PanOptix. Variability in reported spectacle independence may arise from differences in questionnaires and spectacle requirements related to occupations and hobbies. Our practice’s patient demographic includes many skilled laborers (eg, jewelers, electricians, etc.) who regularly perform visually-demanding tasks at near. Even so, our patients demonstrated excellent binocular UNVA with 90% achieving 20/25 or better.
Another advantage of the mix-and-match approach is its compatibility with ISBCS. By allowing patients to use both eyes from the first day after surgery, ISBCS promotes faster neuroadaptation, optimizes binocular summation, and reduces the tendency to compare visual outcomes between eyes—a challenge often encountered with delayed sequential surgery. This is particularly beneficial for mix-and-match patients, as it allows the complementary strengths of each IOL to function together immediately, potentially enhancing the patient satisfaction and visual outcomes achieved in our study.
Limitations of this study include the relatively small sample size, lack of a control arm, ambispective nature, and short follow-up time. While refractive stability is typically achieved by 3 months, patient perceptions may change over longer periods of time. Visual disturbances, however, typically improve with time due to neuroadaptation. Furthermore, we cannot directly compare our Clareon outcomes to studies using older AcrySof IOL models as the newer Clareon material possesses improved optical clarity with reduced glistenings that may enhance optical and visual performance. Formal contrast sensitivity testing was also not conducted. Another limitation is the fact that our inclusion criteria limited analysis to eyes with a postoperative spherical equivalent (SE) within ±0.50 D and cylinder ≤0.75 D. This was intended to evaluate IOL performance in eyes that achieved the target refraction, minimizing the confounding effects of residual refractive error on visual quality and dysphotopsia outcomes. Of course, this approach may introduce selection bias and limits the generalizability of our findings to real-world populations. It is important to note, however, that the overall refractive accuracy was high amongst the cases reviewed with over 90% of eyes achieving ± 0.50 D SE. Finally, direct comparisons between our mix-and-match outcomes cannot be made with bilateral same-IOL approaches. Future studies should compare mix-and-match versus bilateral implantation outcomes in a head-to-head study with defocus curves, larger sample sizes, and longer follow-up duration in order to better elucidate the advantages of a mix-and-match approach.
In conclusion, mix-and-match implantation of the Clareon PanOptix trifocal and Vivity EDOF IOLs is a safe and effective approach that may leverage the advantages of each IOL to produce high patient satisfaction with good spectacle independence and minimal visual disturbances.
Value Statement
What Was Known
- Bilateral implantation of the Clareon PanOptix trifocal and Clareon Vivity EDOF IOLs provide good refractive and visual outcomes resulting in high patient satisfaction following cataract surgery.
- Limitations of the PanOptix IOL and Vivity IOL include presence of photic phenomena and reliance on spectacles for near-work, respectively.
- Studies evaluating a mix-and-match approach for Clareon PanOptix trifocal and Clareon Vivity EDOF IOLs implantation are limited.
What This Paper Adds
- To the authors’ knowledge, this is the first study evaluating visual outcomes and patient satisfaction following mix-and-match implantation of the Clareon PanOptix and Vivity IOLs for cataract surgery.
- Mix-and-match implantation of the Clareon PanOptix and Vivity IOLs yields excellent patient satisfaction by combining the advantages of each lens, resulting in a high degree of spectacle independence and low rate of visual disturbances.
Acknowledgments
Previous presentation: American Society of Cataract and Refractive Surgery Annual Meeting, Boston, MA, USA, 2024.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Supported by an investigator-initiated trial grant from Alcon, Forth Worth, Texas. Alcon has had no role in the study design, data collection, analysis, interpretation, decision for submission, or writing of the report.
Disclosure
One author (DZ) is a consultant and grant recipient for Alcon. The other author (IZ) has no financial or proprietary interest in any material or method mentioned.
References
1. Brian G, Taylor H. Cataract blindness: challenges for the 21st century. Bull World Health Organ. 2001;79:249–256.
2. Leyland M, Zinicola E. Multifocal versus monofocal intraocular lenses in cataract surgery: a systematic review. Ophthalmology. 2003;110(9):1789–1798. doi:10.1016/S0161-6420(03)00722-X
3. Salerno LC, Tiveron MC Jr, Alió JL. Multifocal intraocular lenses: types, outcomes, complications and how to solve them. Taiwan J Ophthalmol. 2017;7(4):179–184. doi:10.4103/tjo.tjo_19_17
4. Yim CK, Dave A, Strawn A, Chan J, Zhou I, Zhu DC. Visual outcomes and patient satisfaction after bilateral refractive lens exchange with a trifocal intraocular lens in patients with presbyopia. Ophthalmol Ther. 2023;12(3):1757–1773. doi:10.1007/s40123-023-00708-x
5. Werner L, Thatthamla I, Ong M, et al. Evaluation of clarity characteristics in a new hydrophobic acrylic IOL in comparison to commercially available IOLs. J Cataract Refract Surg. 2019;45(10):1490–1497. doi:10.1016/j.jcrs.2019.05.017
6. Lee YW, Choi CY, Moon K, et al. Clinical outcomes of new multifocal intraocular lenses with hydroxyethyl methacrylate and comparative results of contrast sensitivity, objective scatter, and subjective photic phenomena. BMC Ophthalmol. 2022;22(1):379. doi:10.1186/s12886-022-02600-x
7. Sudhir RR, Dey A, Bhattacharrya S, Bahulayan A. AcrySof IQ PanOptix intraocular lens versus extended depth of focus intraocular lens and trifocal intraocular lens: a clinical overview. Asia-Pac J Ophthalmol. 2019;8(4):335–349. doi:10.1097/APO.0000000000000253
8. Pieh S, Weghaupt H, Skorpik C. Contrast sensitivity and glare disability with diffractive and refractive multifocal intraocular lenses. J Cataract Refract Surg. 1998;24(5):659–662. doi:10.1016/S0886-3350(98)80261-7
9. Jo E, Kim B, Kim MK, Choi CY, Choi CY. Clinical outcomes of a new hydrophobic trifocal intraocular lens with hydroxyethyl methacrylate in cataract surgery: a prospective multicenter study. Korean J Ophthalmol. 2024;38(3):212. doi:10.3341/kjo.2023.0140
10. Kohnen T, Suryakumar R. Extended depth-of-focus technology in intraocular lenses. J Cataract Refract Surg. 2020;46(2):298–304. doi:10.1097/j.jcrs.0000000000000109
11. Kohnen T. Nondiffractive wavefront-shaping extended range-of-vision intraocular lens. J Cataract Refract Surg. 2020;46(9):1312–1313. doi:10.1097/j.jcrs.0000000000000247
12. Bala C, Poyales F, Guarro M, et al. Multicountry clinical outcomes of a new nondiffractive presbyopia-correcting IOL. J Cataract Refract Surg. 2022;48(2):136–143. doi:10.1097/j.jcrs.0000000000000712
13. US FDA. Clareon aspheric hydrophobic Intraocular Lens (IOL): summary of safety and effectiveness data. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf19/P190018B.pdf. Accessed June 7, 2024.
14. Arrigo A, Gambaro G, Fasce F, Aragona E, Figini I, Bandello F. Extended depth-of-focus (EDOF) AcrySof® IQ Vivity® intraocular lens implant: a real-life experience. Graefes Arch Clin Exp Ophthalmol. 2021;259(9):2717–2722. doi:10.1007/s00417-021-05245-6
15. Hovanesian JA, Jones M, Allen Q. The vivity extended range of vision IOL vs the PanOptix trifocal, ReStor 2.5 active focus and ReStor 3.0 multifocal lenses: a comparison of patient satisfaction, visual disturbances, and spectacle Independence. Clin Ophthalmol. 2022;18:145–152. doi:10.2147/OPTH.S347382
16. Scheepers MA, Hall B. Randomized and double-blind comparison of clinical visual outcomes of 2 EDOF intraocular lenses. J Cataract Refract Surg. 2023;49(4):354–359. doi:10.1097/j.jcrs.0000000000001113
17. Yoon SY, Song IS, Kim JY, Kim MJ, Tchah H. Bilateral mix-and-match versus unilateral multifocal intraocular lens implantation: long-term comparison. J Cataract Refract Surg. 2013;39(11):1682–1690. doi:10.1016/j.jcrs.2013.04.043
18. Lubiński W, Podborączyńska-Jodko K, Gronkowska-Serafin J, Karczewicz D. Visual outcomes three and six months after implantation of diffractive and refractive multifocal IOL combinations. Klinika Oczna/Acta Ophthalmologica Polonica. 2011;113(3):209–215.
19. Labiris G, Panagis C, Ntonti P, Konstantinidis A, Bakirtzis M. Mix-and-match vs bilateral trifocal and bilateral EDOF intraocular lens implantation: the spline curve battle. J Cataract Refract Surg. 2024;50(2):167–173. doi:10.1097/j.jcrs.0000000000001336
20. Lasch K, Marcus JC, Seo C, et al. Development and validation of a visual symptom–specific patient-reported outcomes instrument for adults with cataract intraocular lens implants. Am J Ophthalmol. 2022;237:91–103. doi:10.1016/j.ajo.2021.10.023
21. Gunenc U, Celik L. Long-term experience with mixing and matching refractive array and diffractive CeeOn multifocal intraocular lenses. J Refract Surg. 2008;24(3):233–242. doi:10.3928/1081597X-20080301-04
22. Yesilirmak N, Akova YA, Donmez O. Comparison of mix-and-match implanted bifocal IOLs and bilateral implanted trifocal IOLs after femtosecond laser–assisted cataract surgery. J Refract Surg. 2019;35(9):559–564. doi:10.3928/1081597X-20190806-01
23. Acar B, Nurozler Tabakci B. Clinical outcome comparison: bilateral trifocal vs. mix–match extended depth of focus and trifocal intraocular lenses. Intl Ophthalmol. 2021;41:3675–3686. doi:10.1007/s10792-021-01925-8
24. Lee JH, Chung HS, Moon SY, et al. Clinical outcomes after mix‐and‐match implantation of extended depth of focus and diffractive multifocal intraocular lenses. J Ophthalmol. 2021;2021(1):8881794. doi:10.1155/2021/8881794
25. Ke S, Wan W, Li C. Comparisons of visual outcomes between bilateral implantation and mix-and-match implantation of three types intraocular lenses. Int Ophthalmol. 2023;43(4):1143–1152. doi:10.1007/s10792-022-02513-0.
26. Kim S, Yi R, Chung SH. Comparative analysis of the clinical outcomes of mix-and-match implantation of an extended depth-of-focus and a diffractive bifocal intraocular lens. Eye & Contact Lens. 2022;48(6):261–266. doi:10.1097/ICL.0000000000000887
27. Xiong T, Chen H, Fan W. Comparison of bilateral implantation of an extended depth of focus lenses and a blend approach of extended depth of focus lenses and bifocal lenses in cataract patients. BMC Ophthalmol. 2023;23(1):476. doi:10.1186/s12886-023-03228-1
28. FDA. Summary of safety and effectiveness data (PMA P040020/S087). Food and Drug Administration, USA. 2019. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf4/P040020S087B.pdf.
29. Zhu D, Zhang J. Patient-reported outcomes of visual disturbances with a trifocal intraocular lens: a meta-analysis.
30. McCabe C, Berdahl J, Reiser H, et al. Clinical outcomes in a US registration study of a new EDOF intraocular lens with a nondiffractive design. J Cataract Refract Surg. 2022;48(11):1297–1304. doi:10.1097/j.jcrs.0000000000000978
31. Soscia WL, DeRojas JO, Mathews PM, et al. Clinical performance after implantation of an EDOF intraocular lens in the dominant eye and a presbyopia-correcting intraocular lens in the nondominant eye. J Cataract Refract Surg. 2024;50(6):578–584. doi:10.1097/j.jcrs.0000000000001412
32. van Amelsfort T, Webers VS, Bauer NJ, Clement LH, van den Biggelaar FJ, Nuijts RM. Visual outcomes of a new nondiffractive extended depth-of-focus intraocular lens targeted for minimonovision: 3-month results of a prospective cohort study. J Cataract Refract Surg. 2022;48(2):151–156. doi:10.1097/j.jcrs.0000000000000825
33. Zhu D, Ren S, Mills K, Hull J, Dhariwal M. Rate of complete spectacle Independence with a trifocal intraocular lens: a systematic literature review and meta-analysis. Ophthalmol Ther. 2023;12(2):1157–1171. doi:10.1007/s40123-023-00657-5
34. Modi S, Lehmann R, Maxwell A, et al. Visual and patient-reported outcomes of a diffractive trifocal intraocular lens compared with those of a monofocal intraocular lens. Ophthalmology. 2021;128(2):197–207. doi:10.1016/j.ophtha.2020.07.015
35. Hovanesian JA, Jones M, Allen Q. The PanOptix trifocal IOL vs the ReSTOR 2.5 active focus and ReSTOR 3.0-add multifocal lenses: a study of patient satisfaction, visual disturbances, and uncorrected visual performance. Clin Ophthalmol. 2021;4:983–990. doi:10.2147/OPTH.S285628
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Satisfaction and Visual and Refractive Outcomes Combining an Enhanced Monofocal and a Trifocal Intraocular Lens in Patients with Specific Visual Demands
Mayordomo-Cerdá F, Ortega-Usobiaga J, Bilbao-Calabuig R, Llovet-Osuna F, Albelda-Vallés JC, Beltrán-Sanz J, Baviera-Sabater J
Clinical Ophthalmology 2025, 19:3515-3526
Published Date: 22 September 2025