Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Clinical and Pathological Analysis of 10 Cases of Eosinophilic Pustular Folliculitis
Authors Li Y ![]() , Chen G, Zhou X, Zheng X, Zhang M, Yao X, Lu J
, Chen G, Zhou X, Zheng X, Zhang M, Yao X, Lu J ![]() , Hu X
, Hu X
Received 26 June 2023
Accepted for publication 6 September 2023
Published 11 September 2023 Volume 2023:16 Pages 2467—2472
DOI https://doi.org/10.2147/CCID.S427718
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Yuan Li,1,2,* Gaihe Chen,3,* Xin Zhou,4,* Xiaole Zheng,1,* Ming Zhang,3 Xiaojuan Yao,1 Jiejie Lu,1 Xiaohuan Hu1
1Department of Cosmetic Dermatology, The Fifth People’s Hospital of Hainan Province, Haikou, Hainan, People’s Republic of China; 2Department of Dermatology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 3Department of Dermatology, The Fifth People’s Hospital of Hainan Province, Haikou, Hainan, People’s Republic of China; 4Medical Administration Department, The Fifth People’s Hospital of Hainan Province, Haikou, Hainan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaohuan Hu; Jiejie Lu, Department of Cosmetic Dermatology, The Fifth People’s Hospital of Hainan Province, No. 8 Longhua Road, Longhua District, Haikou, Hainan, 570100, People’s Republic of China, Email [email protected]; [email protected]
Abstract: We conducted a retrospective analysis of clinical and pathologic data from January 2020 to June 2023, focusing on 10 patients diagnosed with eosinophilic pustular folliculitis at our dermatology clinic. Four of the ten patients had the first rash on the face, five on the trunk, and one on the palms and feet, all of which were initially scattered papules that gradually increased and fused into erythematous plaques with a circular distribution. Seven had pustules with small surface desquamation, and three cases had micro swelling on the face. The rash involved only the face in 5 cases, the face and trunk in 5 cases, and the face, trunk, hands, and feet in 1 case. Seven of the ten patients were pruritic, and 3 had no obvious pruritus. The histopathological features were mild epidermal hyperplasia, lymphocytic and eosinophilic infiltration around the superficial middle dermal vessels and appendages, and eosinophilic and neutrophilic abscesses in the local hair follicles. Treatment with oral indomethacin, prednisone, and minocycline was effective.
Keywords: eosinophilic pustular folliculitis, eosinophils, indomethacin
Introduction
Eosinophilic pustular folliculitis (EPF), known as Ofuji’s disease (OD), was initially identified and documented by Japanese scholar Ofuji in 1970. This cutaneous follicular disease is of uncertain origin.1 EPF is a relatively uncommon dermatosis characterized by chronicity, pruritus, and septicity. Its aetiology remains unclear, currently categorized as a non-specific reaction. The condition is chronic, commonly affecting young adult males.2 It primarily manifests on seborrheic areas, notably the face, although the trunk and upper extremities can also be affected. The typical clinical presentation features erythematous-based, red follicular papules and pustules. These may appear clustered or circumscribed with distinct borders. The central area tends to self-heal, often leaving behind hyperpigmentation. Notably, intense itching accompanies the rash.3 In 1983, Katoh et al reported a pruritic skin condition diagnosed as eosinophilic folliculitis, highlighting its chronic nature.
Additionally, they presented the first case of EPF occurring on the scalp in a 9-year-old boy. Subsequently, Sb-eprono and Schinella reported three instances of HIV-associated EPF in 1986. In 2013, Japanese scholar Mayumi documented over 300 cases of Ofuji disease, with 113 cases reported in Japan since 1980.4 Between 2020 and 2023, our centre’s outpatient clinic diagnosed and treated ten cases of EPF. This report provides a detailed account of these cases.
General Information
The general data of the ten patients with EPF are shown in Table 1, including five males and five females, with a male-to-female ratio of 1:1, aged 22 to 45 years, with a disease duration of 15 days to 10 years. All ten patients were residents of the province, with no similar patients in their family members. At the time of presentation to our centre, most patients (73.9%) had symptoms lasting less than six months. There were 9 cases with onset in winter and spring and 1 with onset in summer.
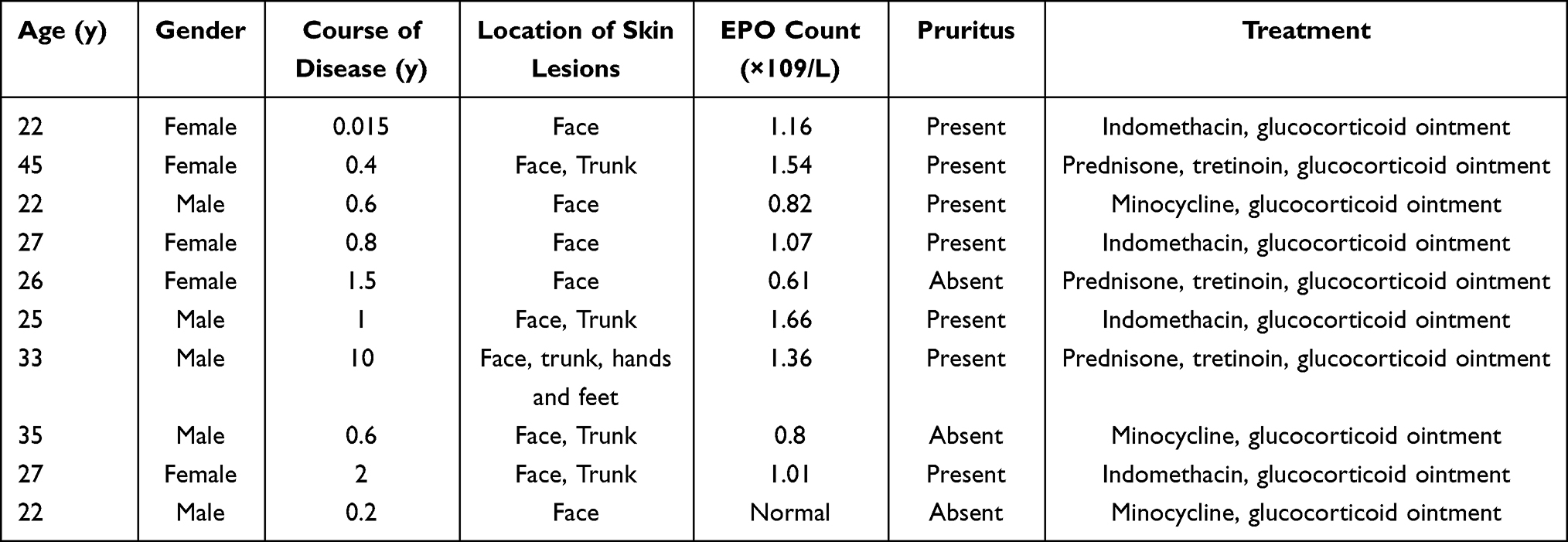 |
Table 1 Clinical Data and Treatment of EPF Patients |
Methods
We performed a retrospective analysis of case data from January 2020 to June 2023, as reported by our pathology department. This analysis focused on skin histopathology biopsies that confirmed the diagnosis of eosinophilic pustular folliculitis.
Clinical Data
The rash appeared first on the face in 4 of the ten patients, on the trunk in 5 cases, and on the palms and feet in 1 case, all of which were initially scattered papules that gradually increased and fused into erythematous plaques with circular distribution. The rash involved only the face in 5 cases, the face and trunk in 5 cases, and the face, trunk, hands, and feet in 1 case. Seven of the ten patients felt pruritus, and three had no obvious pruritus.
The rash mainly appeared as a follicular papule with a diameter of about 1–2 mm on top of the erythema. It expanded eccentrically in a circular or protruding pattern (Figure 1A–I), among which abscesses were seen in 7 patients (Figure 2A and B). All ten patients with EPF had similar histopathological changes in the lesions: intraepithelial spongiform oedema with eosinophil migration in the hair follicles, eosinophilic microabscesses around the sebaceous glands, sweat glands, perivascular and collagen fibres (Figure 2C and D). No fungal hyphae or spores were seen on PAS staining, and all antacid staining was negative. Systemic examinations were standard in all patients except for one with downregulated complement C4 and positive rheumatoid factor.
 |
Figure 1 Clinical pictures: (A–I) Follicular papules with a diameter of about 1–2 mm are seen based on erythema on the face and trunk and expand eccentrically to the periphery in a circular or creeping pattern, and pustules are seen in some patients. |
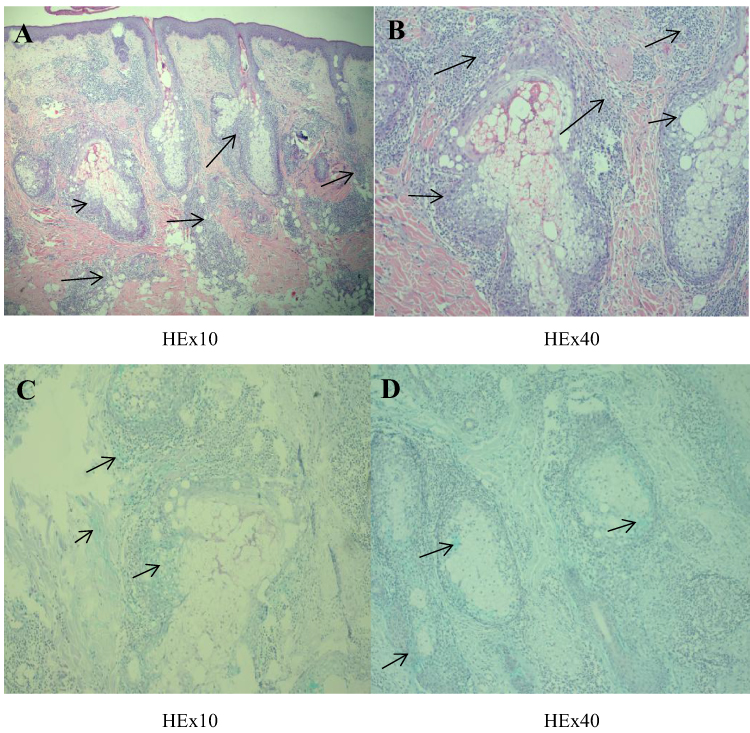 |
Figure 2 Histopathology: (A) Mild epidermal hyperplasia, lymphocytic and eosinophilic infiltration around the superficial middle dermal vessels and appendages (black arrow), (B) eosinophilic and neutrophilic abscesses seen in local hair follicles (black arrow). (C and D) Acidic mucin deposits around the hair follicle and the hair follicle’s sebaceous glands (black arrow). |
Misdiagnosis
Seven of the ten patients had been misdiagnosed, with the most common initial diagnoses suspected to be acne vulgaris (8/10), eczema (7/10), allergic dermatitis (2/10), and lupus erythematosus (1/10). Other secondary differential diagnoses included skin infections, folliculitis, seborrheic dermatitis, and cutaneous lymphocytic infiltration.
Histopathology and Related Examinations
All ten patients were diagnosed by histopathology, with lesions taken from obvious pustules or papules and fused erythema. Histopathology of the skin showed mild hyperplasia of the epidermis and infiltration of lymphocytes and eosinophils around the superficial middle dermal vessels and appendages. Eosinophilic and neutrophilic abscesses in local hair follicles were seen in 7 cases with follicular destruction. The blood count was elevated in 2 patients, and the blood eosinophil count and its ratio were elevated in 9 patients. 1 patient had a positive fungal test in the facial erythema, and ten patients were negative for HIV.
Treatment
Four of the ten patients received oral indomethacin 25 mg three times a day and topical glucocorticoid ointment; three patients received oral prednisone 30 mg once a day, along with oral Rehmannia polysaccharide 20 mg three times a day and topical glucocorticoid ointment; three patients received oral minocycline 100 mg once a day and topical glucocorticoid; all patients had relief of symptoms after two weeks of treatment, follicular After two weeks of treatment, all patients had relief of symptoms and reduction of follicular papules, 3 cases of pustules subsided and no new rash. In three patients treated with prednisone, the drug was reduced by 5 mg every two weeks and discontinued after four months. In four cases, indomethacin was discontinued after three months of maintenance treatment. Six were followed up for 3 months without recurrence, two were lost, and two patients still had recurrent episodes, controlled with minocycline 0.1g, taken orally once a day, and still under treatment.
Discussion
EPF is mainly seen in Japan and China, but cases have also been reported in Europe and North America. EPF is generally classified into three types: classic EPF (C-EPF), immunosuppression-associated EPF (IS-EPF), and infantile EPF (I-EPF), of which C-EPF is the most common type.5 EPF is the most common clinical type. The pathogenesis is unknown, but it may be a non-specific response to various antigenic stimuli that impair the immune system.1,6 The ten patients reported in this paper were all from Hainan Province, with a mean age of 31 years and a male-to-female incidence ratio of 1:1, which is different from the incidence ratios in Japan (5:1) and Singapore (1:1.6), probably due to geographical differences.7 The classic EPF lesions appear as follicular papular pustules on an erythematous base, 1 to 2 mm in diameter, and extend eccentrically around in a circular or creeping pattern for 7 to 10 days, alternating between self-remission and exacerbation, and recurring once every 3 to 4 weeks.8 A few patients may present early with symmetrical butterfly-shaped erythema of the face without papules or pustules, which is difficult to distinguish from lupus erythematosus, and three of our ten patients presented with this manifestation (Figure 1A, D and G). EPF lesions tend to occur on the face, trunk, and upper extremities, with rashes also appearing on the scalp and lower extremities, occasionally involving the lip mucosa, and 20% of rashes have been reported to involve the palmoplantar region.9 This form was present in only one of our patients. Seven of the ten patients in our collection presented with persistent facial erythema annulare with pustules, three patients presented with facial erythema with micro swelling due to atypical lesions treated outside the hospital before coming to us, five patients had lesions involving the trunk, and one patient had simultaneous involvement of the face, trunk, and hands and feet, all without systemic symptoms. 90% (9/10) of the patients had elevated absolute peripheral blood eosinophils. Upon examination of facial erythema, a single patient exhibited positive results for fungal spores, with no observed presence of mycelium. Ten patients were negative for HIV. All could be classified as classic EPF.Typical histology of EPF: In the early stages of pustule formation, sponge formation due to fragmentation and degeneration of epithelial cells or small blister formation in the outer hair root sheath with eosinophilic leukocytes and some mononuclear cell infiltration. In the progressive stage, longitudinal blisters appear in the outer hair root sheaths with many eosinophilic leukocytes mixed with mononuclear cells, polymorphonuclear leukocytes, and epithelial cells. Lymphocytes and histiocytes with eosinophilic leukocytes also infiltrate around the vessels and hair follicles.10 In terms of pathogenesis, the activity of the sebaceous glands had been suspected as a cause of eosinophilic leukocyte accumulation in the hair follicles because the preference is limited to the sebaceous area, and many cases have a history of common acne.11 It has been found that 40% of patients with EPF have mucin deposits around the hair follicles and sebaceous glands. The cause of mucin production is not yet clear. Still, it has been suggested that follicular damage may be due to an increase in eosinophilic leukocytes in the blood, which is nonspecifically recruited into the sebaceous follicles by chemotactic substances and mixed with neutrophils, which in turn cause fragmentation of the follicular epithelium and the formation of These cells, cause fragmentation of the follicular epithelium, resulting in small abscesses and mucinosis-like changes.12,13 One patient in this group had follicular mucin deposits, and the clinical and laboratory tests ruled out connective tissue disease.
Pruritus was a common symptom reported by patients, and eosinophilia was increased in varying degrees, but not in all patients, probably related to the onset and time of consultation, indicating that eosinophilia is not a constant feature,14 and one study noted that eosinophilia was found in 25–86% of this group of patients. In one of the patients, no eosinophilia was seen in the routine blood, and the patient had been treated with methylprednisolone injection in an outside hospital for this disease, which may explain the lack of eosinophilia in his routine blood.
Many therapeutic agents have been used for EPF, including topical and oral corticosteroids, antibiotics such as minocycline, isotretinoin, ultraviolet (UV)B phototherapy, and interferon therapy, but no specific treatment is available. Notably, many of our patients have been treated with a variety of therapeutic agents before being diagnosed with EPF, including topical, oral, and IV corticosteroids, topical and systemic antifungals, glucocorticoid creams, systemic antibiotics such as erythromycin and tetracycline, and isotretinoin.15,16 However, there are no specific drugs for the treatment of this disease. Ellis et al considered topical glucocorticoids and oral indomethacin the first-line treatment for EPF, and about 75% of patients showed significant improvement in symptoms.17 Nervi et al reported that drug allergy to minocycline was associated with the onset of EPF. However, minocycline can still be used to treat EPF, so a detailed history should be taken when treating with minocycline.3 Four of the ten patients we report were treated with oral indomethacin, and 3 (90%) responded well to treatment with a mean starting indomethacin dose of 75 mg/day. Most (90%) of cases responded within 2–4 weeks, and most patients had lesion clearance with residual pigmentation but no scar formation. One patient (10%) was orally switched to minocycline at 100 mg/day for symptomatic relief after intolerance of gastrointestinal reactions to indomethacin.
Similar to previous reports,18 our study confirmed that EPF has a chronic relapsing course and that some patients require maintenance medication to control the disease. The disease is mainly limited to skin involvement without systemic manifestations such as fever, weight loss, or arthralgia.19 After successful treatment, most lesions heal with post-inflammatory hyperpigmentation but no scarring.
Conclusion
In summary, EPF is an uncommon disease characterized by unclear pathogenesis, varied clinical presentations, and diverse subtypes. Accurate diagnosis demands a comprehensive approach, incorporating medical history, laboratory tests, and histopathology to prevent misdiagnosis. Indomethacin commonly serves as the preferred therapeutic agent for this condition.
Ethics Statement
The publications of images were included in the patient’s consent for publication of the case. The Hospital Ethics Committees of the Fifth People’s Hospital of Hainan Province approved to publish the case details.
Consent Statement
Informed consent was provided by the patient for publication of the case.
Funding
This project is supported by Hainan Province Clinical Medical Center.
Disclosure
Yuan Li, Gaihe Chen and Xin Zhou are the co-first authors of this study. Xiaohuan Hu, Xiaole Zheng and Jiejie Lu are Co-corresponding authors for this study. The authors have no conflicts of interest to declare for this work.
References
1. Nomura T, Katoh M, Yamamoto Y, Kabashima K, Miyachi Y. Eosinophilic pustular folliculitis: the transition in sex differences and interracial characteristics between 1965 and 2013. J Dermatol. 2015;42(4):343–352. doi:10.1111/1346-8138.12783
2. Camacho-Martinez F. Eosinophilic pustular folliculitis. J Am Acad Dermatol. 1987;17(4):686–688. doi:10.1016/S0190-9622(87)80457-7
3. Nervi SJ, Schwartz RA, Dmochowski M. Eosinophilic pustular folliculitis: a 40 year retrospect. J Am Acad Dermatol. 2006;55(2):285–289. doi:10.1016/j.jaad.2006.02.034
4. Katoh M, Nomura T, Miyachi Y, Kabashima K. Eosinophilic pustular folliculitis: a review of the Japanese published works. J Dermatol. 2013;40(1):15–20. doi:10.1111/1346-8138.12008
5. Sato S, Chiba T, Nakahara T, Furue M. Upregulation of IL-36 cytokines in folliculitis and eosinophilic pustular folliculitis. Australas J Dermatol. 2020;61(1):e39–e45. doi:10.1111/ajd.13143
6. Marzano AV, Genovese G. Eosinophilic dermatoses: recognition and management. Am J Clin Dermatol. 2020;21(4):525–539. doi:10.1007/s40257-020-00520-4
7. Tang MB, Tan E, Chua SH. Eosinophilic pustular folliculitis (Ofuji’s disease) in Singapore: a review of 23 adult cases. Australas J Dermatol. 2003;44(1):44–47. doi:10.1046/j.1440-0960.2003.00636.x
8. Ichimura R, Kamiya K, Komine M, et al. Possible interaction between eosinophils and other immune cells in the pathomechanism of eosinophilic pustular folliculitis. Int J Dermatol. 2022;61(12):e499–e501. doi:10.1111/ijd.16203
9. Ohata C, Nii S, Furumura M, Nakama T. Vesicles and pustules on the fingers as an initial manifestation of eosinophilic pustular folliculitis. J Dermatol. 2015;42(9):914–915. doi:10.1111/1346-8138.12946
10. Fujiyama T, Tokura Y. Clinical and histopathological differential diagnosis of eosinophilic pustular folliculitis. J Dermatol. 2013;40(6):419–423. doi:10.1111/1346-8138.12125
11. Chen J, Beatty CJ, Falcone LM, English JC, Kazlouskaya V. Eosinophilic pustular folliculitis in the setting of solid organ transplant immunosuppression. Dermatol Pract Concept. 2023;13(2):e2023078. doi:10.5826/dpc.1302a78
12. Grant GJ, Sahni DR, Florell AJ, et al. An atypical case of eosinophilic pustular folliculitis with associated secondary follicular mucinosis treated with indomethacin. JAAD Case Rep. 2023;34:86–89. doi:10.1016/j.jdcr.2022.12.022
13. Lee MW, Lee DP, Choi JH, Moon KC, Koh JK. Failure to detect clonality in eosinophilic pustular folliculitis with follicular mucinosis. Acta Derm Venereol. 2004;84(4):305–307. doi:10.1080/00015550410026966
14. Long H, Zhang G, Wang L, Lu Q. Eosinophilic skin diseases: a comprehensive review. Clin Rev Allergy Immunol. 2016;50(2):189–213. doi:10.1007/s12016-015-8485-8
15. Gallo G, Conti L, Quaglino P, Ribero S. Treatment of eosinophilic pustular folliculitis with low-dose isotretinoin. Int J Dermatol. 2022;61(7):e262–e264. doi:10.1111/ijd.15929
16. Nomura T, Katoh M, Yamamoto Y, Miyachi Y, Kabashima K. Eosinophilic pustular folliculitis: trends in therapeutic options. J Dermatol. 2016;43(7):847–849. doi:10.1111/1346-8138.13296
17. Ellis E, Scheinfeld N. Eosinophilic pustular folliculitis: a comprehensive review of treatment options. Am J Clin Dermatol. 2004;5(3):189–197. doi:10.2165/00128071-200405030-00007
18. Kanaki T, Hadaschik E, Esser S, Sammet S. Eosinophilic pustular folliculitis (EPF) in a patient with HIV infection. Infection. 2021;49(4):799–801. doi:10.1007/s15010-020-01543-z
19. Lankerani L, Thompson R. Eosinophilic pustular folliculitis: case report and review of the literature. Cutis. 2010;86(4):190–194.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Successful Treatment of Eosinophilic Pustular Folliculitis with Secondary Follicular Mucin Deposition Using Indomethacin: An Atypical Case and Literature Review
Li W, Hu X, Li Y, Chen G
Clinical, Cosmetic and Investigational Dermatology 2025, 18:1063-1070
Published Date: 1 May 2025