Back to Journals » Infection and Drug Resistance » Volume 19
Clinical and Microbiological Characteristics Associated with Treatment Outcomes Among Rifampicin-Resistant Tuberculosis Patients in Limpopo Province
Authors Rukasha I, Rakgate KA, Kaapu KG
Received 1 April 2026
Accepted for publication 15 May 2026
Published 14 July 2026 Volume 2026:19 613052
DOI https://doi.org/10.2147/IDR.S613052
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Ivy Rukasha,1,2 Kgothatso Ashley Rakgate,1 Kabelo Gabriel Kaapu1
1Division of Medical Microbiology, Department of Pathology, School of Medicine, University of Limpopo, Polokwane, South Africa; 2Department of Microbiology, Polokwane Laboratory, National Health Laboratory Service, Polokwane, South Africa
Correspondence: Ivy Rukasha, Email [email protected]
Background: Drug-resistant tuberculosis (DR-TB) remains a major public health concern in South Africa, particularly in rural provinces such as Limpopo, where access to specialized care is limited. High HIV prevalence, population mobility, and constrained diagnostic capacity further complicate disease control. Province-specific data are essential to guide targeted interventions; however, factors associated with treatment outcomes in rural settings remain poorly characterized.
Methods: A retrospective cohort study was conducted using routinely collected laboratory and programmatic data. All laboratory-confirmed DR-TB cases recorded in Limpopo Province between 2023 and 2025 were included. Microbiological data were obtained from the National Health Laboratory Service, while demographic, clinical, and treatment outcome data were extracted from the Electronic Drug-Resistant Tuberculosis Register. Descriptive statistics summarized patient characteristics. Associations with treatment outcomes were assessed using chi-square tests and multivariable logistic regression. Kaplan–Meier analysis compared survival by HIV status.
Results: A total of 86 RR-TB patients were included. Most were aged 25– 44 years (65.1%), with males comprising 70.9%, and 55.8% were HIV co-infected. Favourable treatment outcomes were observed in 62 (71.4%) patients, while 12 (14.3%) experienced unfavourable outcomes and 12 (14.3%) remained on treatment. In multivariable analysis, younger age (15– 24 years) (AOR = 9.97, 95% CI: 1.48– 67.33) and smear-negative status (AOR = 39.62, 95% CI: 3.33– 471.83) were independently associated with unfavourable outcomes, whereas HIV status was not significant after adjustment. Kaplan–Meier analysis showed poorer survival among HIV-positive patients (log-rank p = 0.002), although this was not retained in the adjusted model.
Conclusion: DR-TB in Limpopo is characterized by a high burden of TB–HIV co-infection and rifampicin resistance. Clinical factors, rather than resistance patterns, were key determinants of unfavourable outcomes. Strengthening integrated TB–HIV services, improving early diagnosis, and expanding drug susceptibility testing are critical to improving outcomes.
Keywords: drug-resistant tuberculosis, rifampicin-resistant tuberculosis, tuberculosis–hiv co-infection, antimicrobial resistance, treatment outcomes, survival analysis, public health surveillance, South Africa
Introduction
Tuberculosis (TB) remains a major global public health challenge and the leading cause of death from a single infectious agent worldwide. Sub-Saharan Africa carries a disproportionate burden of disease, with South Africa ranking among the 30 high TB burden countries globally. In 2023, South Africa reported approximately 270,000 TB cases, including nearly 13,000 cases of rifampicin-resistant or multidrug-resistant tuberculosis (RR/MDR-TB). Despite advances in diagnostics and treatment, outcomes for DR-TB remain suboptimal because of delayed diagnosis, prolonged treatment regimens, drug toxicity, inconsistent adherence, and health system constraints.1–3
Limpopo Province presents distinct epidemiological dynamics that justify focused investigation. The province is predominantly rural, with limited access to specialised diagnostic services and DR-TB treatment centres. It shares international borders with Botswana, Zimbabwe, and Mozambique, functioning as a major transit corridor for regional migration. Literature has shown that high population mobility contributes to delayed diagnosis, treatment interruption, and amplification of resistant strains. These structural and cross-border dynamics create a complex transmission environment that may differ substantially from national averages.4,5
Sociodemographic and clinical factors, including age, sex, occupation, and HIV status, significantly shape TB risk, disease progression, and treatment outcomes. Literature has consistently demonstrated that TB disproportionately affects individuals within the economically active age group (15–44 years), with men more frequently affected than women. HIV co-infection remains a major driver of both incident TB and reactivation of latent infection, particularly in high-burden settings.6 In provinces such as Limpopo, where HIV prevalence and population mobility intersect, these factors may further influence DR-TB patterns and clinical outcomes.
Despite ongoing national surveillance efforts, province-specific data describing demographic, clinical, and microbiological factors associated with treatment outcomes among RR-TB patients remain limited in rural South African settings. Understanding local determinants of RR-TB treatment outcomes is essential for strengthening decentralized TB control strategies and optimizing integrated TB–HIV care in high-burden communities.4,6 This study aimed to describe the demographic, clinical, and microbiological characteristics of rifampicin-resistant tuberculosis patients and evaluate factors associated with treatment outcomes in Limpopo Province, South Africa.
Addressing this evidence gap is critical for informing province-specific TB control strategies and strengthening implementation of South Africa’s National TB Recovery Plan. Generating locally relevant data on demographic distribution, clinical characteristics, and microbiological resistance patterns is essential for guiding targeted interventions and enhancing surveillance within a high-burden, resource-limited setting. Despite national surveillance, limited data exist on factors associated with treatment outcomes among DR-TB patients in rural South African settings. Understanding these determinants is critical for risk stratification and targeted interventions. Therefore, this study aimed to describe the demographic, clinical, and microbiological characteristics of rifampicin-resistant tuberculosis patients and evaluate factors associated with treatment outcomes in Limpopo Province, South Africa.
Methodology
Study Area
Limpopo Province, located in northern South Africa, is the country’s fifth most populous province, accounting for approximately 10% of the national population of over 60 million people.7 Predominantly rural, the province faces persistent disparities in access to specialized diagnostic services and DR-TB treatment centres, which may influence case detection and clinical outcomes.8 Recent analyses highlight that DR-TB continues to threaten TB control efforts in resource-limited provinces such as Limpopo, where weak laboratory infrastructure and limited genomic surveillance capacity hinder timely detection of resistance patterns.4,6 In addition, high levels of cross-border migration with Botswana, Zimbabwe, and Mozambique contribute to population mobility and treatment interruption, further amplifying resistant strains.4
Ethical Approval
Ethical approval for this study was obtained from the Turfloop Research Ethics Committee (TREC) of the University of Limpopo (Reference: TREC/108/2024: PG), the National Health Laboratory Service (NHLS) (Reference: PR2456259), and the Limpopo Department of Health (Reference: LP_2025-03-011). Permission to access routine programmatic data was granted by the relevant provincial health authorities.
The requirement for informed consent was waived by all approving bodies, as the study utilized routinely collected laboratory and Department of Health data with no direct patient interaction. All data were fully anonymized prior to analysis to ensure confidentiality and privacy. The study was conducted in accordance with the principles of the Declaration of Helsinki, the South African National Health Act (No. 61 of 2003), and national Good Clinical Practice guidelines.
Study Site and Population
This study was conducted in Limpopo Province, South Africa, and included rifampicin-resistant tuberculosis (RR-TB) patients diagnosed between January 2023 and July 2025. Study samples were collected at National Health Laboratory Service (NHLS) Polokwane Microbiology laboratory.
Study Design
A retrospective cohort study was conducted to assess demographic, clinical, and microbiological characteristics associated with treatment outcomes among RR-TB patients in Limpopo Province, South Africa.
Data Collection
Data were compiled from complementary laboratory and routine programmatic sources. Microbiological data were obtained from the NHLS, while demographic, clinical, treatment, and treatment outcome data were sourced from Department of Health routine programmatic records. The variables collected included patient age, sex, HIV status, type of tuberculosis, drug resistance profile, treatment history, treatment regimen, and final treatment outcome. Treatment outcomes were defined according to national tuberculosis programme guidelines and categorized as cure, treatment completion, death, treatment failure, or loss to follow-up.
Inclusion and Exclusion Criteria
Eligible participants included all patients diagnosed with laboratory-confirmed DR-TB, between 1 January 2023 and 31 July 2025 in Limpopo Province. Cases were included if microbiological confirmation was available from NHLS Polokwane microbiology laboratory and corresponding demographic, clinical, treatment, and outcome data were available from Department of Health routine programmatic records. Patients with incomplete or missing key variables required for analysis (eg., demographic, clinical, microbiological, or treatment outcome data) or with unspecified TB classification were excluded.
Definitions
Treatment outcomes were classified according to national DR-TB treatment outcome definitions. Favourable outcomes included treatment completed, while unfavourable outcomes included death and loss to follow-up. Patients who were still on treatment at the time of data extraction were retained for descriptive analyses but excluded from regression analyses assessing predictors of treatment outcomes. Rifampicin-resistant tuberculosis was defined as tuberculosis caused by Mycobacterium tuberculosis resistant to rifampicin, with or without resistance to additional anti-tuberculosis drugs.
Data Analysis
Data were cleaned and coded using Microsoft Excel and subsequently exported to IBM SPSS Statistics version 30.0 for statistical analysis.
Descriptive statistics were used to summarize demographic and clinical characteristics. Categorical variables were expressed as frequencies and percentages. Associations between categorical variables were assessed using the chi-square test; where the assumption of expected cell counts ≥5 was violated, Fisher’s exact test was applied. A p-value <0.05 was considered statistically significant, and effect sizes (Cramer’s V) were reported to quantify the strength of associations.
Kaplan–Meier survival analysis was used to estimate time to death among DR-TB patients. Time-to-event was calculated as days from treatment initiation to death, with treatment completion, cure, or ongoing treatment treated as censoring events. Survival curves were compared using the Log rank test and stratified by HIV status. Kaplan–Meier survival analysis was performed as an exploratory descriptive approach to visualize differences in survival by HIV status.
To identify factors independently associated with unfavourable treatment outcomes, multivariable logistic regression analysis was performed. Patients who were still on treatment at the time of analysis were excluded from the regression model. Crude and adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were reported. The adjusted model included key covariates such as age group, sex, HIV status, and smear status. Variables included in the adjusted model were selected based on clinical relevance and univariate associations. Complete-case analysis was performed for regression modeling, and no imputation procedures were undertaken because of the retrospective nature of the dataset and limited sample size. All analyses were two-tailed, and statistical significance was set at p <0.05. Reporting was conducted in accordance with the STROBE guidelines.
Results
Characteristics of DR-TB Patients
Among the 86 patients included in the study, most were aged 25–44 years (65.1%), and males accounted for 70.9% of cases (Table 1). Cases were distributed across all five districts of Limpopo Province, with the highest proportions observed in Capricorn (29.1%) and Mopani (26.7%). HIV co-infection was present in 55.8% of patients. All isolates were confirmed as Mycobacterium tuberculosis, with culture positivity observed in 98.8% of cases. Smear microscopy demonstrated varying bacillary loads, with 2+ smear positivity being the most common (48.8%). Drug susceptibility testing identified resistance to multiple first- and second-line anti-tuberculosis drugs, including isoniazid (46.5%), fluoroquinolones (19.8%), ethionamide (8.1%), amikacin (1.2%), bedaquiline (16.3%), and linezolid (1.2%).
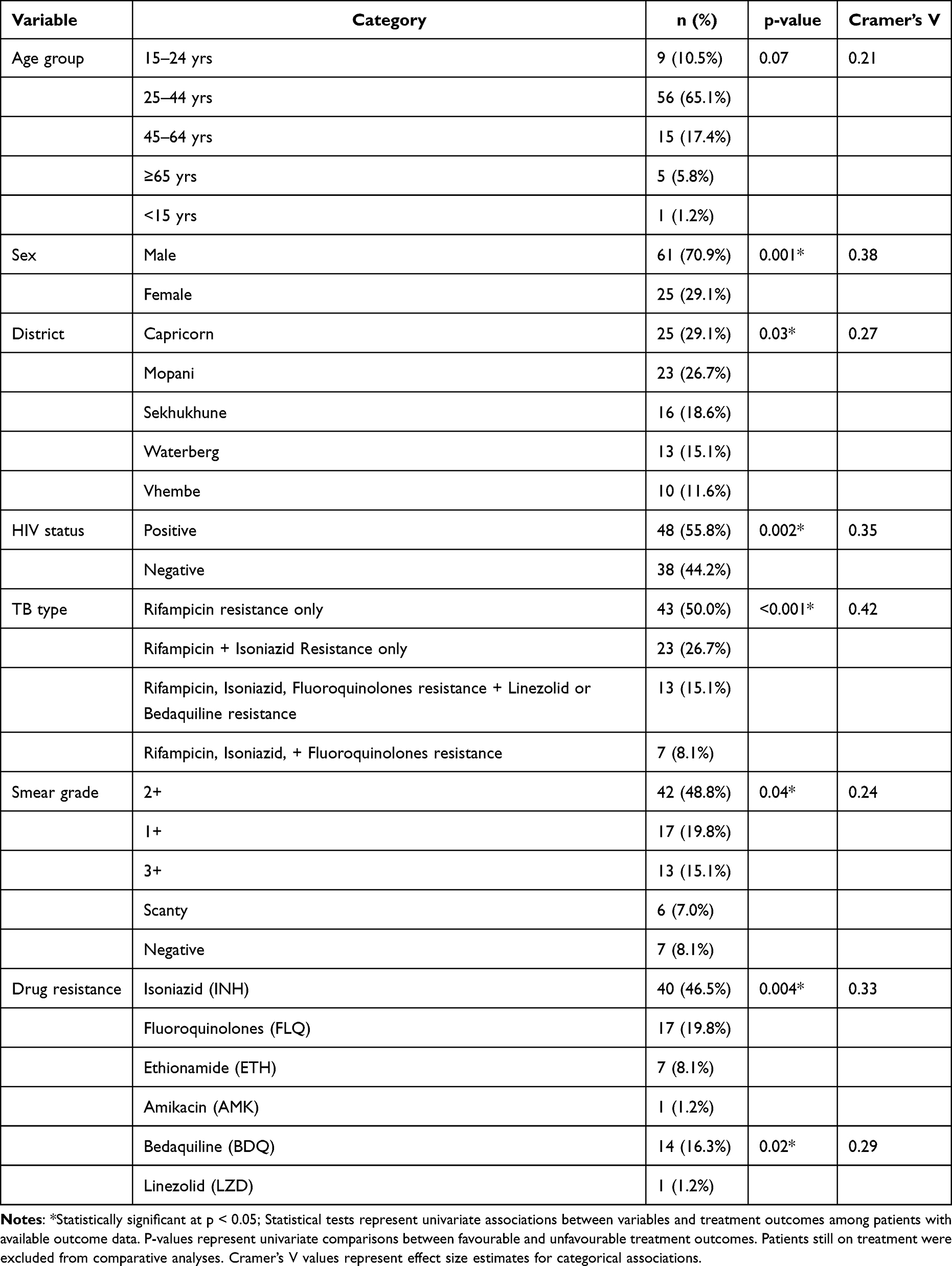 |
Table 1 Demographic, Clinical, and Microbiological Characteristics of DR-TB Patients in Limpopo (2023–2025) |
Treatment Outcomes of DR-TB Patients
Among the 86 RR-TB patients with available treatment outcome data, favourable outcomes (treatment completion) were observed in 62 (71.4%) patients. Unfavourable outcomes (death or loss to follow-up) occurred in 12 (14.3%) patients, while 12 (14.3%) patients were still on treatment at the time of analysis and were treated as censored observations.
Factors Associated with Treatment Outcomes
Demographic and Clinical Factors
In univariate analysis (Table 1), HIV co-infection was significantly associated with treatment outcomes (χ2 = 9.7, p = 0.002), with a higher proportion of unfavourable outcomes observed among HIV-positive patients. Smear grade was also associated with treatment outcomes (χ2 = 5.4, p = 0.04). Age group and sex were not significantly associated with treatment outcomes in univariate analysis. Effect size estimates based on Cramer’s V indicated predominantly small-to-moderate associations between categorical variables and treatment outcomes However, in multivariable logistic regression analysis (Table 2), only age 15–24 years (AOR = 9.97, 95% CI: 1.48–67.33, p = 0.018) and smear-negative status (AOR = 39.62, 95% CI: 3.33–471.83, p = 0.004) remained independently associated with unfavourable outcomes. HIV status and sex were not significantly associated after adjustment.
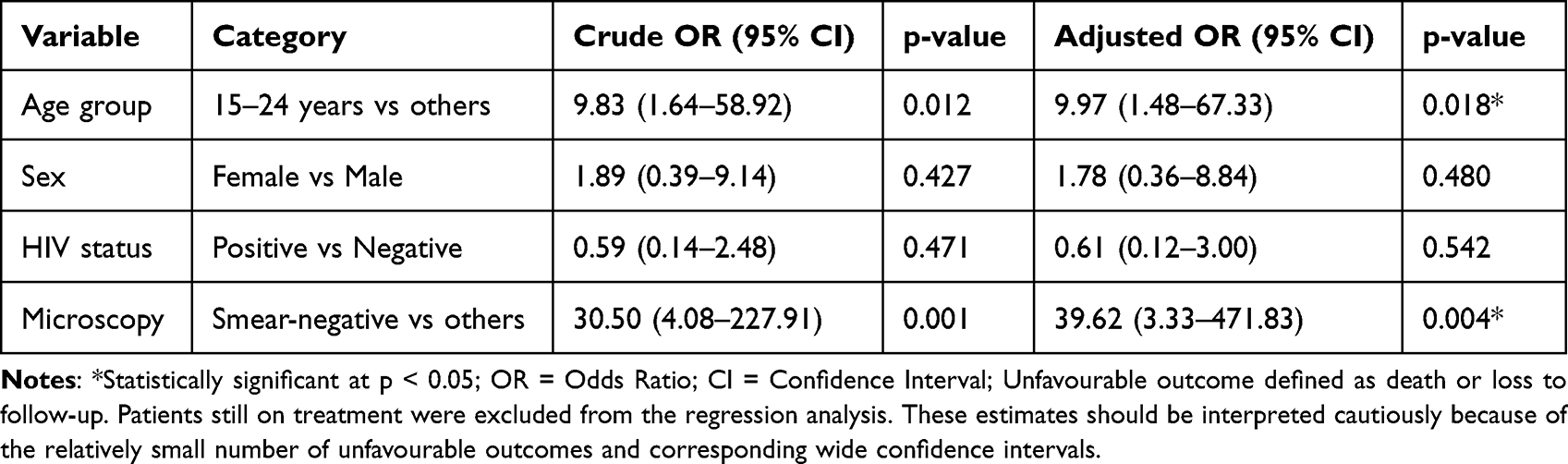 |
Table 2 Logistic Regression Analysis of Factors Associated with Unfavourable Treatment Outcomes Among DR-TB Patients |
Microbiological and Resistance Factors
Among the included patients, MDR-TB, pre-XDR-TB, and XDR-TB phenotypes were identified based on additional resistance patterns. (Table 1). In univariate analysis, resistance profile was not significantly associated with treatment outcomes.
Isoniazid resistance was observed in 46.5% of isolates, while fluoroquinolone resistance was present in 19.8%. Resistance to bedaquiline was identified in 16.3% of cases. No statistically significant associations were observed between individual drug resistance patterns and treatment outcomes in univariate analysis.
In the multivariable logistic regression model (Table 2), microbiological resistance variables were not independently associated with unfavourable treatment outcomes.
Smear microscopy grading showed that 2+ smear positivity was the most frequent (48.8%), followed by 1+ (19.8%) and 3+ (15.1%). In univariate analysis, smear grade was significantly associated with treatment outcomes; however, in the multivariable model, smear-negative status (compared with other smear grades) remained independently associated with unfavourable outcomes.
Multivariable Analysis of Predictors of Unfavourable Outcomes
Multivariable logistic regression was performed to identify factors independently associated with unfavourable treatment outcomes among DR-TB patients, excluding those still on treatment at the time of analysis. In the adjusted model, patients aged 15–24 years had significantly higher odds of experiencing an unfavourable outcome compared with older age groups (AOR = 9.97, 95% CI: 1.48–67.33, p = 0.018). Similarly, smear-negative patients had markedly increased odds of unfavourable outcomes compared with non-smear-negative patients (AOR = 39.62, 95% CI: 3.33–471.83, p = 0.004). This should be interpreted more cautiously because estimates are imprecise. Female sex (AOR = 1.78, 95% CI: 0.36–8.84, p = 0.480) and HIV-positive status (AOR = 0.61, 95% CI: 0.12–3.00, p = 0.542) were not significantly associated with unfavourable outcomes after adjustment. The wide confidence intervals observed for some predictors indicate limited precision of the estimates, likely reflecting the relatively small number of unfavourable outcomes. These estimates should be interpreted cautiously because of the relatively small number of unfavourable outcomes and corresponding wide confidence intervals.
Survival Analysis by HIV Status
Kaplan–Meier survival analysis demonstrated differences in survival between HIV-positive and HIV-negative DR-TB patients (Figure 1), with HIV-positive patients exhibiting a lower probability of survival over time compared with HIV-negative patients.
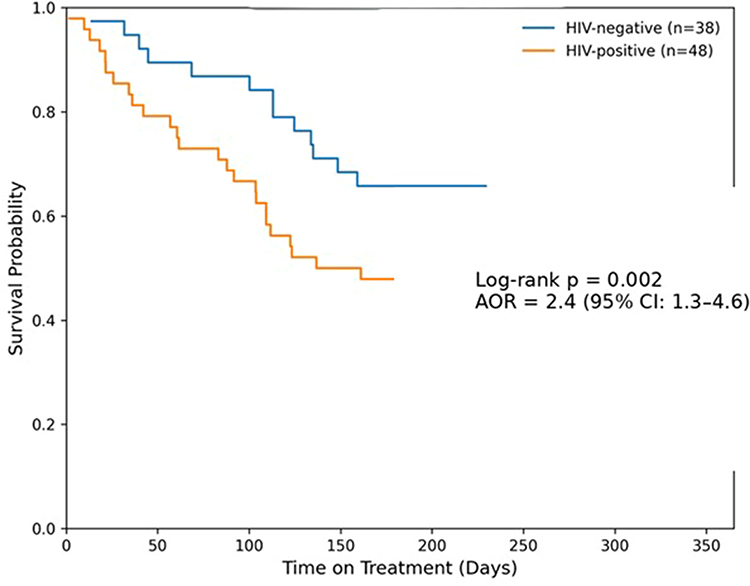 |
Figure 1 Kaplan–Meier survival curves comparing HIV-positive and HIV-negative drug-resistant TB patients in Limpopo Province (2023–2025). |
The difference in survival distributions between the two groups was statistically significant (Log rank test, p = 0.002). However, this association was not retained in the multivariable logistic regression model (Table 2). However, HIV status was not significantly associated with unfavourable outcomes in the adjusted logistic regression model.
Discussion
This province-wide analysis from Limpopo Province provides a comprehensive assessment of the demographic, clinical, and microbiological characteristics of drug-resistant tuberculosis (DR-TB). The study identified a predominance of RR-TB, a concentration of cases among working-age males, and a high prevalence of TB–HIV co-infection. These findings are consistent with national trends in South Africa and global estimates reported by the World Health Organization (WHO), while also reflecting context-specific transmission dynamics that warrant targeted public health interventions.4,8,9 The predominance of male patients is consistent with previous studies reporting delayed healthcare-seeking behaviour, occupational mobility, treatment interruption and loss to follow-up among men; however, the present study was not sufficiently powered to robustly assess outcome-specific differences such as mortality versus loss to follow-up.
Rifampicin resistance remains a major programmatic concern because of its association with multidrug-resistant tuberculosis and its central role in frontline molecular diagnostics. The identification of additional MDR-TB, pre-XDR-TB, and XDR-TB phenotypes within this cohort highlights the ongoing evolution of resistance patterns in Limpopo Province and reinforces the importance of sustained resistance surveillance.10,11 Rifampicin’s central role in first-line therapy generates sustained selective pressure, particularly in contexts of incomplete adherence, drug stock-outs, or delayed resistance detection.9 In addition, frontline molecular diagnostics such as Xpert MTB/RIF prioritize rifampicin resistance detection and operationally classify RR-TB as a proxy for MDR-TB, increasing its reported frequency.12 Provincial genomic analyses similarly emphasize rifampicin resistance as the dominant phenotype in Limpopo, supporting the interpretation that primary transmission of RR strains substantially contributes to the local DR-TB burden.8
Demographically, DR-TB disproportionately affected males (70.9%) and individuals aged 25–44 years (65.1%), consistent with WHO global epidemiology indicating peak TB incidence among working-age adults.9 Male predominance has been associated with occupational exposure, labour migration, smoking, alcohol use, and delayed healthcare-seeking behaviour.4,13 A similar male-skewed distribution of DR-TB has been reported in regional surveillance data, reinforcing the influence of gendered social determinants. The underrepresentation of children and older adults likely reflects diagnostic challenges in paediatric TB and healthcare access barriers among elderly populations.14
The resistance profile raises important programmatic considerations. High isoniazid resistance (46.5%) reflects global trends of increasing INH mono-resistance and its contribution to MDR evolution.9,15 Fluoroquinolone resistance (19.8%) is concerning given the central role of this class in MDR-TB regimens. Encouragingly, most isolates remained susceptible to bedaquiline and linezolid, which are classified as Group A drugs in the current WHO DR-TB treatment guidelines.9 Low resistance to these agents supports the continued effectiveness of all-oral regimens in this setting. Nonetheless, emerging reports of bedaquiline resistance from South Africa and other high-burden countries highlight the need for continuous drug resistance surveillance to preserve the effectiveness of these critical agents.8,16 The observed prevalence of bedaquiline resistance is clinically concerning given the central role of bedaquiline in contemporary DR-TB treatment regimens. However, the study design could not distinguish between primary transmission of resistant strains and acquired resistance resulting from prior drug exposure, treatment interruption, or regimen-related factors. These findings nevertheless underscore the importance of ongoing resistance surveillance and expanded access to drug susceptibility testing for newer anti-tuberculosis agents. Although resistance to amikacin and linezolid remained low, vigilance remains essential as expanded use of newer agents may increase selective pressure over time. Limited pretomanid susceptibility data reflect laboratory capacity constraints rather than confirmed susceptibility patterns. The high culture positivity rate (98.8%) strengthens confidence in bacteriological confirmation and laboratory performance within the province.
Smear microscopy grading showed a predominance of 2+ smear positivity, indicating moderate to high bacillary loads among patients at diagnosis. Smear grade is widely used as a proxy indicator of bacterial burden and potential infectiousness.17,18 The predominance of 2+ smear grades is consistent with reports from other high-burden TB settings and suggests that many patients present with substantial bacillary loads at the time of diagnosis. The relatively lower frequency of smear-negative or scanty results may reflect the limited sensitivity of smear microscopy in detecting paucibacillary disease, particularly among HIV-positive individuals.19 The association was observed as imprecise estimates that may reflect delayed diagnosis, atypical disease presentation, or paucibacillary disease rather than a direct biological relationship.
The survival analysis highlighted differences in outcomes by HIV status, with Kaplan–Meier curves demonstrating significantly poorer survival among HIV-positive patients compared with HIV-negative individuals. However, this association was not retained in the multivariable logistic regression model, suggesting that the observed differences in survival may be influenced by confounding factors rather than HIV status alone. In contrast, younger age (15–24 years) and smear-negative status were independently associated with unfavourable treatment outcomes and should be interpreted more cautiously because estimates are imprecise. The increased risk observed among younger patients may reflect challenges related to treatment adherence, health-seeking behaviour, or delayed engagement with care. Similarly, smear-negative disease may be indicative of atypical or advanced disease presentation, particularly in immunocompromised individuals, which may contribute to delayed diagnosis and poorer clinical outcomes.20–22 Although HIV-positive patients demonstrated poorer survival in the Kaplan–Meier analysis, HIV status was not independently associated with unfavourable outcomes in the adjusted logistic regression model. These approaches address related but distinct analytical questions and may therefore yield different findings. The relatively small number of unfavourable outcomes may also have limited the precision of adjusted estimates. These findings highlight the importance of considering multiple interacting determinants when evaluating treatment outcomes in drug-resistant tuberculosis.6,23–25
Overall, this study provides important insights into the epidemiology and resistance patterns of DR-TB in Limpopo Province. The findings highlight the continued predominance of RR-TB, the high burden of TB–HIV co-infection, and the presence of resistance to both first-line and second-line anti-tuberculosis drugs. While microbiological resistance patterns were not independently associated with treatment outcomes, clinical factors such as younger age and smear-negative disease were associated with unfavourable outcomes. This association may reflect delayed diagnosis, atypical disease presentation, or paucibacillary disease rather than a direct biological relationship. Interpretation of some associations should be undertaken cautiously because the relatively small number of unfavourable outcomes contributed to wide confidence intervals and limited precision of certain regression estimates.
These findings underscore the need to strengthen integrated TB-HIV services, enhance early diagnosis, particularly in atypical presentations and expand access to comprehensive drug susceptibility testing. Sustained surveillance for emerging resistance, alongside targeted interventions for high-risk patient groups, will be critical for improving DR-TB control in this high-burden setting.
Strengths
This study has several strengths. It provides province-wide, laboratory-confirmed data, offering comprehensive regional coverage rather than isolated district-level analyses. The high culture confirmation rate enhances the reliability of microbiological findings. The inclusion of both first- and second-line drug susceptibility testing enables detailed characterization of resistance patterns. Integration of demographic and clinical variables allows for contextual epidemiological interpretation of DR-TB within the province. Furthermore, the consistency of these findings with prior provincial genomic studies8 supports the internal validity of the observed resistance patterns.
Limitations
This study has several limitations. The relatively small sample size reflects the number of DR-TB patients registered in the provincial programme during the study period and may limit the statistical power to detect smaller associations. As a retrospective, laboratory-based study, detailed clinical variables—including prior treatment history, adherence patterns, and socioeconomic status—were not available. Incomplete second-line drug susceptibility data, particularly for pretomanid, limit the comprehensive interpretation of emerging resistance patterns. The absence of routine whole-genome sequencing restricts the ability to differentiate between primary transmission and acquired resistance. Referral bias may have led to an overrepresentation of bacteriologically confirmed or more severe cases, while underestimating paucibacillary disease. Smear microscopy is subject to inter-observer variability, and the cross-sectional nature of the data limits causal inference regarding transmission dynamics and treatment outcomes. Additionally, the wide confidence intervals observed in the multivariable analysis indicate limited precision of some estimates, likely due to the relatively small sample size and low number of unfavourable outcomes.
Conclusion
The demographic and clinical profile of RR-TB patients in this study highlights a concentration of disease among economically active men, suggesting possible ongoing transmission within the community, although transmission dynamics could not be directly assessed. Strengthening decentralized molecular diagnostics, expanding genomic surveillance, and integrating TB–HIV services remain essential for improving early detection and treatment outcomes. Importantly, clinical factors particularly younger age and smear-negative disease - were associated with unfavourable outcomes, underscoring the need for risk-stratified patient management and improved recognition of atypical disease presentations. These findings provide actionable, context-specific evidence to support the strengthening of DR-TB diagnostics, surveillance systems, and integrated TB–HIV care in rural, high-burden settings in sub-Saharan Africa.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no specific funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zumla A, Sahu S, Yeboah-Manu D, et al. Breaking dependency: strengthening the global tuberculosis response in the face of USAID cuts. The Lancet. 2025;405(10483):958–10. doi:10.1016/S0140-6736(25)00335-6
2. Estaji F, Kamali A, Keikha M. Strengthening the global Response to Tuberculosis: insights from the 2024 WHO global TB report. J Clin Tuberc Other Mycobact Dis. 2025;39:100522. doi:10.1016/j.jctube.2025.100522
3. World Health Organization. Global Tuberculosis Report 2025. WHO international. 2024. Available from: https://www.who.int/teams/global-programme-on-tuberculosis-and-lung-health/tb-reports/global-tuberculosis-report-2025.
4. Makondo VT, Kaapu KG, Wells F, et al. Empowering tuberculosis genomic surveillance in Limpopo, South Africa through capacity building. Front Public Health. 2025;13:1567382. doi:10.3389/fpubh.2025.1567382
5. Seloma NM, Makgatho ME, Maimela E. Evaluation of drug-resistant tuberculosis treatment outcome in Limpopo province, South Africa. Afr J Prim Health Care Fam Med. 2023;15(1). doi:10.4102/PHCFM.V15I1.3764
6. Kaapu KG, Rukasha I. Trends and treatment outcomes of drug resistant tuberculosis in Limpopo Province, South Africa (2011–2019): a Retrospective Study. PLoS One. 2025;20(11):e0335600. doi:10.1371/journal.pone.0335600
7. Statistics South Africa | improving Lives Through Data Ecosystems. Available from: https://www.statssa.gov.za/.
8. Rukasha I, Kaapu KG, Fortune SM, Lekalakala-Mokaba MR. Treatment Outcomes for Drug-Resistant Tuberculosis Patients on Bedaquiline-Based Regimens in a Mostly Rural South Africa. Infect Drug Resist. 2025;18:1819–1829. doi:10.2147/IDR.S502302
9. Global Tuberculosis Report 2023. Available from: https://www.who.int/teams/global-programme-on-tuberculosis-and-lung-health/tb-reports/global-tuberculosis-report-2023.
10. Campbell PJ, Morlock GP, Sikes RD, et al. Molecular detection of mutations associated with first- and second-line drug resistance compared with conventional drug susceptibility testing of Mycobacterium tuberculosis. Antimicrob Agents Chemother. 2011;55(5):2032–2041. doi:10.1128/AAC.01550-10
11. Miotto P, Tessema B, Tagliani E, et al. A standardised method for interpreting the association between mutations and phenotypic drug resistance in Mycobacterium tuberculosis. European Respiratory Journal. 2017;50(6):31. doi:10.1183/13993003.01354-2017
12. Lawn SD, Xpert® NMP. MTB/RIF assay: development, evaluation and implementation of a new rapid molecular diagnostic for tuberculosis and rifampicin resistance. Future Microbiol. 2011;6(9):1067–1082. doi:10.2217/fmb.11.84
13. Horton KC, MacPherson P, Houben RMGJ, White RG, Corbett EL. Sex differences in tuberculosis burden and notifications in low- and middle-income countries: a systematic review and meta-analysis. PLoS Med. 2016;13(9):e1002119. doi:10.1371/journal.pmed.1002119
14. Jenkins HE, Tolman AW, Yuen CM, et al. Incidence of multidrug-resistant tuberculosis disease in children: systematic review and global estimates. Lancet. 2014;383(9928):1572–1579. doi:10.1016/S0140-6736(14)60195-1
15. Gegia M, Winters N, Benedetti A, van Soolingen D, Menzies D. Treatment of isoniazid-resistant tuberculosis with first-line drugs: a systematic review and meta-analysis. Lancet Infect Dis. 2017;17(2):223–234. doi:10.1016/S1473-3099(16)30407-8
16. Marks GB, V NN, Nguyen PTB, et al. Community-wide Screening for Tuberculosis in a High-Prevalence Setting. New England Journal of Medicine. 2019;381(14):1347–1357. doi:10.1056/nejmoa1902129
17. WHO. Guidelines for laboratory and field-testing of long-lasting insecticidal nets WHO Library Cataloguing-in-Publication Data Guidelines for laboratory and field testing of long-lasting insecticidal nets. Available from: www.who.int.
18. Sutton BJ, Parsons AC, Palavecino EL. Filamentous bacteria masquerading as fungi: a diagnostic pitfall in direct smear interpretation with report of two cases. J Clin Pathol. 2011;64(10):927–929. doi:10.1136/jcp.2011.089284
19. Beynon F, Theron G, Respeito D, et al. Correlation of Xpert MTB/RIF with measures to assess Mycobacterium tuberculosis bacillary burden in high HIV burden areas of Southern Africa. Sci Rep. 2018;8(1). doi:10.1038/s41598-018-23066-2
20. Wondmeneh TG, Mekonnen AT. The incidence rate of tuberculosis and its associated factors among HIV-positive persons in Sub-Saharan Africa: a systematic review and meta-analysis. BMC Infect Dis. 2023;23(1). doi:10.1186/s12879-023-08533-0
21. Koenig R. Drug-resistant tuberculosis: in South Africa, XDR TB and HIV prove a deadly combination. Science (1979). 2008;319(5865):894–897. doi:10.1126/science.319.5865.894
22. Kubjane M, Osman M, Boulle A, Johnson LF. The impact of HIV and tuberculosis interventions on South African adult tuberculosis trends, 1990-2019: a mathematical modeling analysis. International Journal of Infectious Diseases. 2022;122:811–819. doi:10.1016/j.ijid.2022.07.047
23. Wu L, Cai X, Xu S, Lin X, Peng T, Jiang X. Trends in Drug Resistance and Epidemiological Patterns of Tuberculosis in Elderly Patients in Wenzhou, China (2014-2023). Infect Drug Resist. 2025;18:3459–3470. doi:10.2147/IDR.S530067
24. Alemu A, Bitew ZW, Worku T, Gamtesa DF, Alebel A. Predictors of mortality in patients with drug-resistant tuberculosis: a systematic review and meta-analysis. PLoS One. 2021;16(6):e0253848. doi:10.1371/journal.pone.0253848
25. Liu H, Zou L, Yu JJ, et al. Treatment outcomes and associated influencing factors among elderly patients with rifampicin-resistant tuberculosis: a multicenter, retrospective, cohort study in China. BMC Infectious Diseases. 2025;25(1):1086. doi:10.1186/s12879-025-11491-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Patient-Centered Care on Treatment Outcomes of Multidrug-Resistant/Rifampicin-Resistant Tuberculosis in Xi’an

Luo H, Ma J, He X, Ruan Y, Ren F, Dang L, Xu Y, Zhao A
Infection and Drug Resistance 2025, 18:1425-1437
Published Date: 13 March 2025
Treatment Outcomes for Drug-Resistant Tuberculosis Patients on Bedaquiline-Based Regimens in a Mostly Rural South Africa
Rukasha I, Kaapu KG, Fortune SM, Lekalakala-Mokaba MR
Infection and Drug Resistance 2025, 18:1819-1829
Published Date: 12 April 2025
Improving Tuberculosis Treatment Outcomes in Somalia: A Narrative Review of Strategies, Challenges, and Policy Recommendations
Mohamoud JH
Risk Management and Healthcare Policy 2026, 19:595510
Published Date: 17 April 2026