Back to Journals » Infection and Drug Resistance » Volume 19
Clinical and Microbiological Characteristics and Antimicrobial Susceptibility Patterns of Multidrug-Resistant Myroides Spp. Infections in Intensive Care Units: A Retrospective Study
Authors Halipci Topsakal HN ![]() , Dundar B, Bozkurt F
, Dundar B, Bozkurt F
Received 29 January 2026
Accepted for publication 13 April 2026
Published 19 May 2026 Volume 2026:19 599727
DOI https://doi.org/10.2147/IDR.S599727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Hatice Nur Halipci Topsakal,1 Bagnu Dundar,2 Fatma Bozkurt3
1Department of Pharmaceutical Microbiology, Faculty of Pharmacy, Bezmialem Vakıf University, Istanbul, 34093, Turkiye; 2Department of Medical Biochemistry, Faculty of Medicine, Istanbul Atlas University, Istanbul, 34408 Turkiye; 3Department of Infectious Diseases and Clinical Microbiology, Faculty of Medicine, Istanbul Atlas University, Istanbul, 34408 Turkiye
Correspondence: Hatice Nur Halipci Topsakal, Department of Pharmaceutical Microbiology, Faculty of Pharmacy, Bezmialem Vakıf University, Topkapı mah, Adnan Menderes Blv., Fatih, İstanbul, 34093, Turkiye, Tel +90 (545) 578 24 79, Fax +90 (212) 489 08 00, Email [email protected]
Purpose: Patients in intensive care units are at risk of infections caused by multidrug-resistant (MDR) pathogens, including the opportunistic bacterium Myroides spp. This study aimed to describe the clinical and microbiological characteristics of MDR Myroides spp. infections and to report antimicrobial susceptibility patterns and treatment approaches used in clinical practice.
Methods: In this retrospective single-center study, 70 patients hospitalized in a tertiary care center in Türkiye between 2017 and 2023 who met criteria for true infection were included, although Myroides spp. was isolated from 509 clinical specimens. Demographic, clinical, and laboratory data were analyzed descriptively. Bacterial identification and antimicrobial susceptibility testing were performed using the VITEK® 2 GN system on specimens obtained from blood, urine, wound swabs, and invasive procedures.
Results: The isolates demonstrated high levels of resistance to most conventional antibiotics tested. Tigecycline showed the highest in vitro susceptibility rate, with 95.2% of isolates classified as susceptible. Tigecycline was also the most frequently used antimicrobial agent in clinical management, with a mean treatment duration of 10.3 days. The mean patient age was 72.7 years, and tigecycline treatment was administered to 88.5% of the patients. Most infections involved the urinary tract, while one patient developed invasive disease with concurrent bacteremia and pneumonia.
Conclusion: MDR Myroides spp. infections remain rare but clinically relevant in intensive care settings. The high in vitro susceptibility observed for tigecycline and its frequent use in treatment highlight its potential role in the management of these infections. However, further studies with comparative designs are needed to better define optimal therapeutic strategies. The infographic presents clinical and microbiological characteristics of multidrug-resistant Myroides spp. infections in ICU patients from 2017 to 2023 in Türkiye. The left section shows ICU patients with 509 Myroides spp. isolates and 70 true infections. The middle section describes multidrug-resistant Myroides spp. with high resistance to conventional antibiotics, majority urinary tract infections and invasive cases like bacteremia and pneumonia. The right section details treatment outcomes with tigecycline, showing 95.2 percent susceptibility, a mean treatment duration of 10.3 days and high microbial eradication. A note at the bottom emphasizes early identification and targeted tigecycline therapy improving outcomes in MDR Myroides spp. infections in ICU patients.ICU patients with resistant Myroides infections: outcomes and benefits of tigecycline therapy.
Keywords: Myroides spp, multidrug resistance, empirical treatment, opportunistic pathogen
Introduction
Myroides spp., previously classified as Flavobacterium odoratum, are aerobic, yellow-pigmented, non-fermentative, Gram-negative bacilli with a characteristic fruity odor.1 These organisms are primarily isolated from environmental sources such as water, soil, and sewage treatment facilities.2 Although human infections caused by Myroides spp. are considered rare, they can be life-threatening, particularly in vulnerable patient populations.3 Clinically, Myroides spp. are regarded as low-grade opportunistic pathogens and have been associated with a wide range of infections, with urinary tract infections being the most frequently reported, as well as endocarditis, ventriculitis, catheter-associated infections, and cutaneous infections, most commonly in severely immunocompromised individuals.4,5 Nevertheless, sporadic infections in immunocompetent hosts have also been documented, suggesting that host susceptibility alone may not fully explain disease development.
In recent years, Myroides spp. have increasingly been recognized as emerging nosocomial pathogens, particularly in intensive care unit (ICU) settings. Prolonged hospitalization, extensive use of invasive medical devices, broad-spectrum antibiotic exposure, and improved survival of critically ill patients have created conditions that facilitate infections caused by rare but intrinsically resistant microorganisms. Consequently, isolates once dismissed as environmental contaminants or colonizers are now being implicated in clinically significant infections with substantial morbidity.6,7
Despite their environmental ubiquity, Myroides infections remain uncommon. For example, a recent retrospective cohort study conducted at the Cleveland Clinic identified 52 Myroides-positive cultures between 2015 and 2023, of which only 21 represented clinically significant infections.8
The management of Myroides infections remains challenging due to pronounced intrinsic multidrug resistance, and clinical evidence for effective therapy is limited. While several antimicrobials show in vitro activity, caution is warranted when extrapolating these data to clinical efficacy. These bacteria are characteristically resistant to polymyxins and test positive for DNase and urease activity, and most clinical isolates exhibit high-level resistance to multiple antimicrobial classes, including penicillins, cephalosporins, aminoglycosides, monobactams, and carbapenems.8,9 For clarity, discussion of resistance mechanisms is focused on chromosomally encoded metallo-β-lactamases and other determinants consistently linked to multidrug resistance, avoiding speculation on less-established pathways. Identified risk factors for M. odoratimimus infections include diabetes mellitus and the presence of indwelling devices such as Foley catheters.9–11 Despite being traditionally linked to immunosuppression, the literature presents conflicting evidence regarding host susceptibility, with some studies reporting a strong association with immunocompromised patients, while others describe comparable infection rates among immunocompetent individuals.12,13
In ICU practice, antimicrobial therapy is frequently initiated empirically before definitive microbiological identification and susceptibility results are available.14 For rare but highly resistant pathogens such as Myroides spp., standard empirical regimens used for Gram-negative infections often fail to provide adequate coverage.15 Delayed administration of effective therapy may lead to persistent infection, prolonged hospitalization, and adverse clinical outcomes. Moreover, distinguishing true infection from colonization is particularly difficult in critically ill patients with indwelling medical devices, further complicating therapeutic decision-making.16
Tigecycline is a broad-spectrum glycylcycline antibiotic. It is effective against Gram-positive bacteria, Gram-negative bacteria and anaerobes, but generally has no activity against Pseudomonas or Proteus species. It is mainly used for complicated intra-abdominal infections, complicated skin and soft tissue infections, and certain systemic infections in ICU. Chemical structure of Tigecycline is given in Figure 1.
 |
Figure 1 Chemical structure of tigecycline. |
Current evidence guiding the treatment of Myroides spp. infections remains limited. The existing literature largely consists of isolated case reports and small case series, precluding the development of standardized treatment recommendations.17 Although several reports have suggested tigecycline as a potentially effective agent, the available data are fragmented, and systematic evaluations in larger patient cohorts are scarce, emphasizing that clinical effectiveness should be interpreted cautiously.
Data on the epidemiology, antimicrobial resistance patterns, and treatment outcomes of Myroides spp. infections in Türkiye are particularly limited. Regional surveillance data are essential, as resistance profiles and clinical responses may vary according to local antimicrobial usage practices and healthcare settings. Addressing this specific clinical gap, our study provides descriptive data linking microbiological susceptibility with clinical outcomes in ICU patients.
In this context, the present study aims to characterize the antimicrobial resistance profile of Myroides spp. and to evaluate clinical outcomes associated with empirical treatment strategies, with particular emphasis on presenting evidence-based guidance for initial therapy while awaiting culture confirmation, rather than asserting definitive treatment efficacy. We retrospectively analyzed patients with Myroides-positive cultures obtained in a tertiary care hospital over a six-year period, including only those who fulfilled the Centers for Disease Control and Prevention (CDC) criteria for true infection to minimize diagnostic ambiguity. We hypothesized that tigecycline-based therapy may provide required clinical outcomes and represent an effective treatment option for multidrug-resistant (MDR) Myroides spp. infections. By correlating microbiological findings with clinical outcomes, this study seeks to inform rational empirical therapy decisions for patients with suspected Myroides infections.
Material and Methods
Biological Materials and Statistical Analysis
A total of 70 Myroides spp. isolates were obtained from adult patients admitted to the combined medical-surgical intensive care unit (ICU) of a tertiary care hospital with 100 beds. This is a retrospective, single-center observational cohort study. These isolates were selected for inclusion based on retrospective evaluation of microbiological and clinical records. Although Myroides spp. was detected in 509 clinical specimens during the study period, only 70 isolates from the first isolate per patient that met Centers for Disease Control and Prevention/National Healthcare Safety Network CDC/NHSN criteria for true infection were included in the final analysis.
True infections were defined according to the Centers for Disease Control and Prevention (CDC) / National Healthcare Safety Network (NHSN) criteria, which included compatible clinical findings such as fever, leukocytosis, and site-specific symptoms together with microbiological evidence. Immunosuppression was defined as the use of systemic corticosteroids equivalent to ≥20 mg/day of prednisolone for at least 3–4 weeks or the presence of other clinically documented immunosuppressive conditions. Data were extracted retrospectively from electronic medical records and ICU patient files by the study investigators. Cases with incomplete data were excluded from variable-specific analyses. Recurrent infections and subsequent isolates from the same patient were also excluded.
Infection was defined in accordance with the Centers for Disease Control and Prevention/National Healthcare Safety Network (CDC/NHSN) surveillance definitions for healthcare-associated infections. A case was classified as true infection when clinical signs (eg, fever, leukocytosis), laboratory markers (eg, elevated C-reactive protein or procalcitonin), and microbiological findings consistent with infection (eg, pyuria in urinary tract isolates) were concurrently present. Isolates not meeting these criteria were considered colonizers and excluded.
The study was approved by the Ethics Committee of Istanbul Atlas University (Decision Number: E-22686390-050.99-26196). Written informed consent was obtained from all patients included in the study.
During the initial ICU admission, blood, urine, wound swabs, and specimens obtained through invasive procedures were collected from all patients presenting with suspected infections and submitted for routine bacterial culture. Among the 70 patients included in the study, invasive infection was confirmed in only one case, in which Myroides spp. was simultaneously isolated from urine, blood, and deep tracheal aspirate specimens. This patient was diagnosed with concurrent urinary tract infection and lower respiratory tract infection (pneumonia), consistent with an invasive clinical presentation. In all remaining cases, Myroides spp. isolates were obtained exclusively from urine specimens and were classified as causative agents of urinary tract infections based on clinical and laboratory criteria.
Data collected for each patient included demographic characteristics, comorbidities, invasive interventions, surgical history, immunosuppressive status, antimicrobial treatment details, and clinical outcomes.18 Information was obtained from the hospital’s electronic medical record system, ICU admission files, and data provided by the infection control committee.
Comorbidities were categorized based on the presence of central nervous system disorders, cardiovascular diseases, respiratory conditions, endocrine or metabolic disorders (eg, diabetes mellitus), peripheral vascular disease, and urinary tract pathology.
Invasive procedures assessed included central venous catheterization, nasogastric tube placement, endotracheal intubation, tracheostomy, and percutaneous endoscopic gastrostomy (PEG). Surgical interventions were classified by system, including respiratory, urogenital, ophthalmologic, orthopedic, neurologic, cardiovascular, and gastrointestinal surgeries.
The presence of malignancy, history of systemic corticosteroid use, and immunosuppressive therapy, defined as exposure to chemotherapy or radiotherapy, were also recorded. Patients were classified as immunosuppressed if they were receiving systemic corticosteroid therapy at a dose equivalent to <20 mg of prednisolone daily or on alternate days for a duration of 3–4 weeks, either short- or long-term.
The demographic characteristics, clinical and laboratory findings, and treatment protocols of patients aged ≥18 years who were admitted to the combined ICU of Istanbul Atlas University Medical Hospital between January 2017 and May 2023 were reviewed. Patients were excluded if their culture results were interpreted as colonization in the absence of pyuria, or if the samples were polymicrobial.
Microbiological culture is routinely performed in our ICU when clinically indicated. Specimens from various sites are obtained as part of standard diagnostic workup. Only the first isolate per patient was included for analysis; repeat cultures were recorded but not counted as separate cases unless meeting criteria for recurrent infection, which were excluded.
Additionally, the time to post-treatment control culture collection was recorded for each patient. The interval from the initiation of therapy to Myroides spp. culture negativity was also documented, along with the total duration of antimicrobial treatment.
Bacterial Isolates and Antimicrobial Susceptibility Tests
Myroides spp. isolates were identified from clinical specimens using the automated identification system VITEK® 2 GN (BioMérieux, Marcy l’Étoile, France). Antimicrobial susceptibility testing (AST) was performed using VITEK® 2 GN AST-N cards, which determine minimum inhibitory concentrations (MICs) and resistance phenotypes. VITEK® 2 is a validated system for the reliable identification of Myroides species and assessment of their antimicrobial resistance profiles.19
MIC values were interpreted according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) clinical breakpoints.
Statistical Analysis
All statistical analyses were run using SPSS (Statistical Package for Social Sciences) Version 26.0 (IBM Corp., Armonk, NY, USA). All data are represented as mean ± standard deviation (SD). Descriptive statistics were applied. Categorical data were expressed as percentages, and numerical data as mean, standard deviation, and min-max values.
Results and Discussions
Data on the clinical characteristics, antimicrobial resistance patterns, and treatment outcomes of Myroides spp. infections in critically ill adult patients remain limited, particularly in the context of empirical management in intensive care units. In this study, we analyzed a large series of Myroides spp. isolates obtained over a six-year period, distinguishing true infection from colonization and focusing on patients with clinically significant infections. By integrating demographic features, comorbid conditions, invasive procedures, antimicrobial susceptibility profiles, and treatment responses, our findings provide real-world evidence on the clinical behavior of Myroides spp. and the effectiveness of targeted antimicrobial therapy in an ICU setting.
Isolation and Classification of Myroides spp. in ICU Patients
Between January 2017 and May 2023, a total of 509 clinical specimens yielding Myroides spp. were recovered from patients admitted to the intensive care unit. Based on predefined clinical and laboratory criteria, were classified as causative agents of infection and included in the analysis, while the remaining isolates were interpreted as colonization and excluded (Table 1).
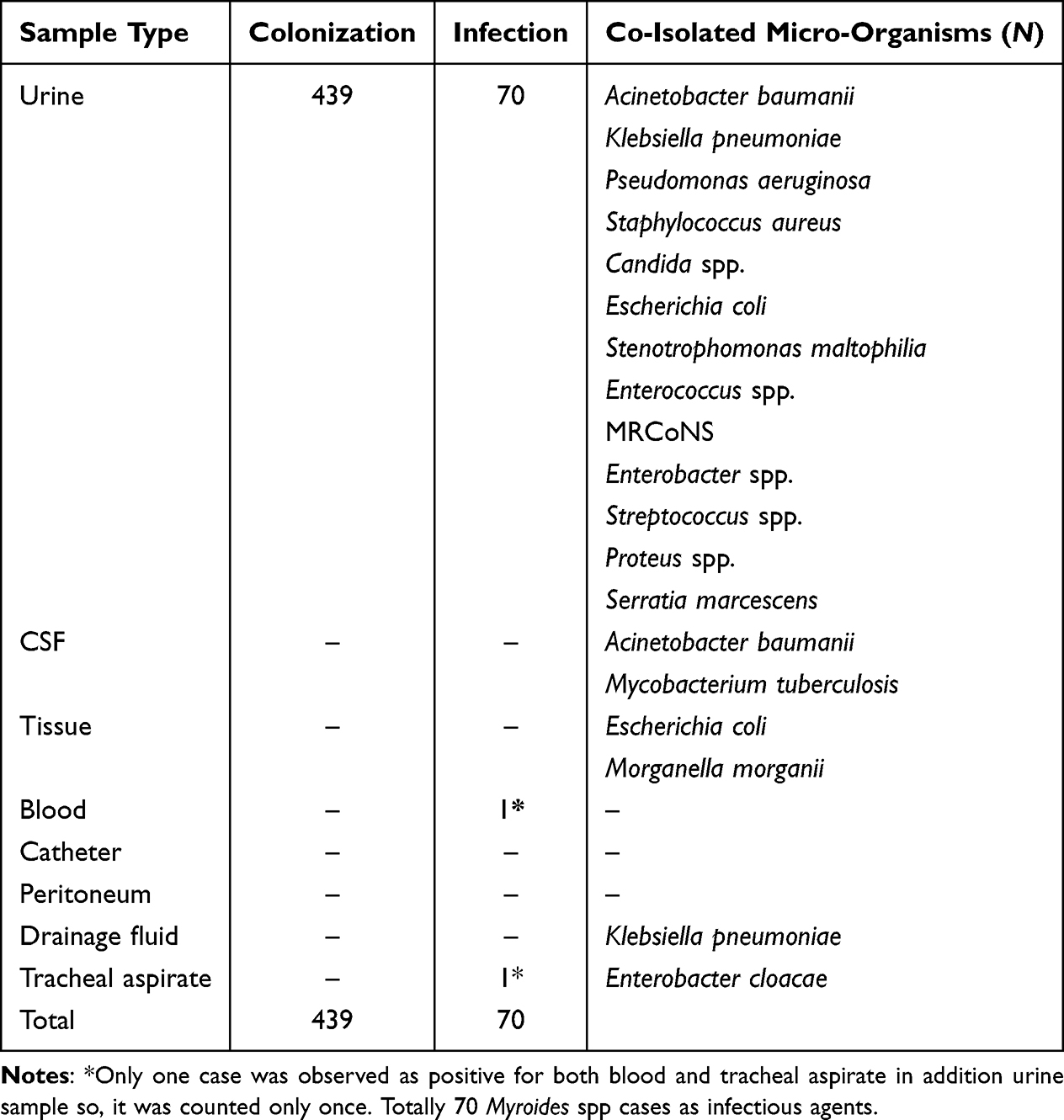 |
Table 1 Distribution of Myroides spp. Isolated in Culture by Sample Type, Colonization/Infection Status and Co-Isolated Microorganisms |
This distinction is particularly important in ICU settings, where Myroides spp. may frequently be isolated as colonizers, especially from urinary catheter–associated specimens, potentially leading to inappropriate antimicrobial treatment if microbiological findings are not carefully correlated with clinical evidence.
The high proportion of isolates interpreted as colonization in the present study is consistent with previous reports indicating that Myroides spp. are often recovered from urinary samples without clear clinical significance. Several authors have emphasized the importance of applying strict clinical and laboratory criteria to distinguish true infection from colonization, particularly in catheterized ICU patients, in order to avoid unnecessary antimicrobial exposure.20,21
According to the table, polymicrobial infections (co-isolation with other microorganisms) were observed predominantly in urine samples. Among the urine samples, 439 isolates were evaluated as colonization and 70 as infection. In these samples, several microorganisms were co-isolated with Myroides spp., including Acinetobacter baumannii, Klebsiella pneumoniae, Pseudomonas aeruginosa, Staphylococcus aureus, Candida spp., Escherichia coli, Stenotrophomonas maltophilia, Enterococcus spp., MRCoNS, Enterobacter spp., Streptococcus spp., Proteus spp., and Serratia marcescens.
In addition, one infection was detected in blood cultures and one in tracheal aspirate samples, where polymicrobial associations were also observed. No significant infection numbers were reported in other sample types such as CSF, catheter, or peritoneal fluid. Overall, these findings indicate that Myroides spp. isolates are most frequently associated with polymicrobial infections in urine samples and may coexist with various opportunistic pathogens.
Clinical Presentation and Infection Localization
Invasive infection was identified in only one case (1.4%), in which Myroides spp. were concurrently isolated from urine and deep tracheal aspirate specimens during the same infectious episode. All remaining 69 infection episodes (98.6%) were exclusively associated with urine samples and were classified as urinary tract infections.
This distribution suggests that, in the ICU setting, Myroides spp. infections predominantly manifest as localized urinary tract infections rather than invasive disease. The predominance of urinary tract involvement is consistent with the high frequency of urinary catheterization observed in this cohort and underscores the importance of differentiating true infection from colonization when interpreting urinary isolates. Despite the extensive multidrug-resistant profile of the organism, the rare occurrence of invasive infection is presented descriptively; no generalized statements about low virulence are made.
Demographic Characteristics of the Study Population
A total of 70 infection episodes meeting the inclusion criteria were analyzed. The mean age of the affected population was 72.7 ± 17.6 years, with a median age of 79 years (range: 18–97), reflecting a predominantly elderly ICU population. Male patients accounted for 54.3% (n = 38), while 45.7% (n = 32) were female (Table 2).
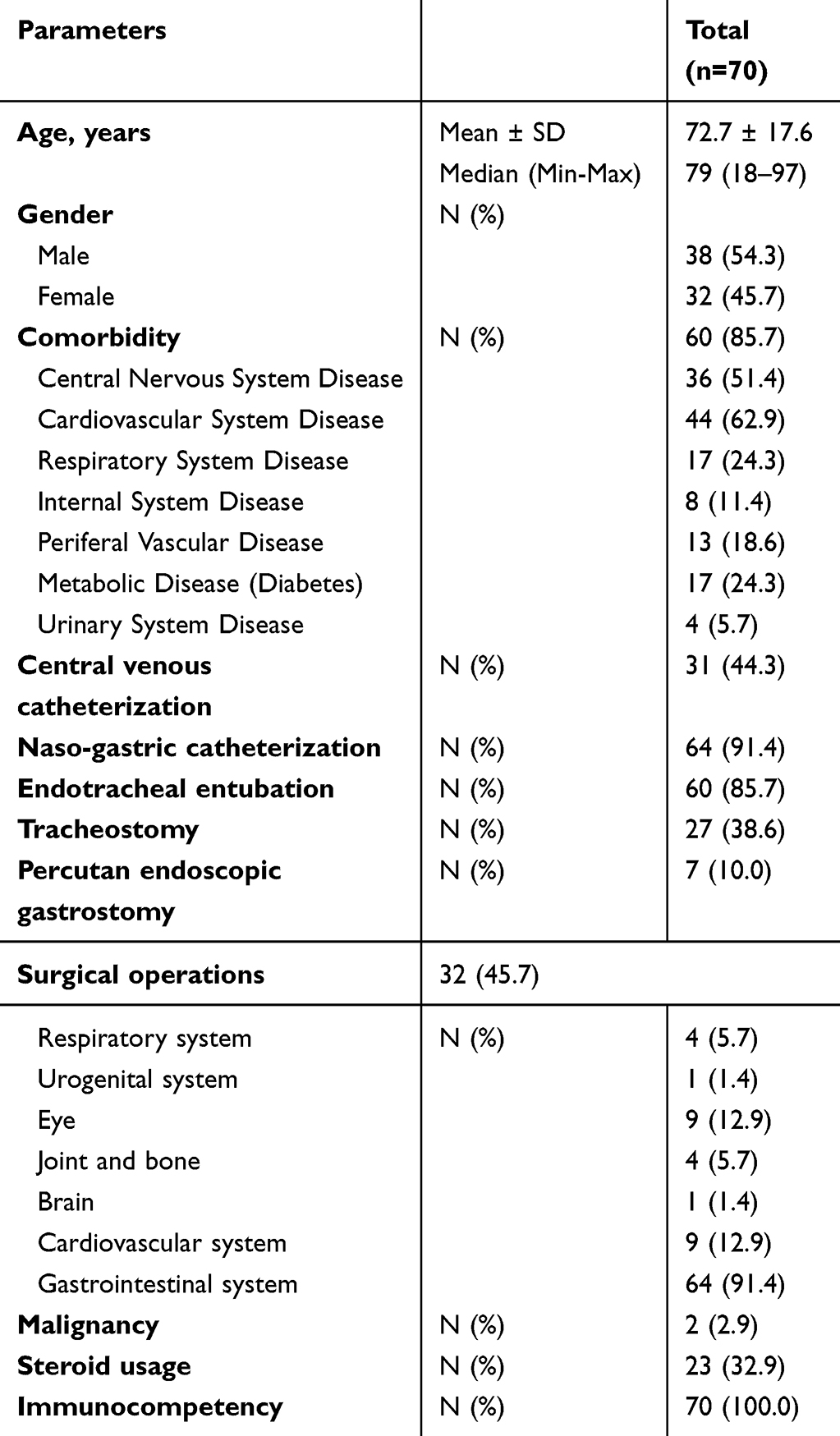 |
Table 2 Demographic and Clinical Settings of the Patients |
Notably, all patients were immunocompetent at the time of infection. However, the majority (85.7%, n = 60) had at least one underlying comorbid condition, most commonly cardiovascular and central nervous system disorders. Advanced age and comorbidities are described as potential contributing factors without implying causality.
Comorbidities and Underlying Clinical Conditions
The most frequently observed comorbidities among infection episodes included cardiovascular diseases (62.9%, n = 44) and central nervous system disorders (51.4%, n = 36), reflecting the advanced age and critical illness profile of the ICU population. Respiratory system diseases (24.3%, n = 17), diabetes mellitus (24.3%, n = 17), and peripheral vascular disease (18.6%, n = 13) were also commonly documented, while urinary system disorders were less frequent (5.7%, n = 4).
Malignancy was identified in only two cases (2.9%), and corticosteroid use was documented in 32.9% (n = 23) of the cohort. The high burden of comorbidities is presented descriptively as a possible factor for susceptibility to Myroides spp. infection, avoiding causal statements.
Surgical History and Clinical Interventions
Surgical interventions were documented in 45.7% (n = 32) of the study population. When evaluated across the entire cohort, the most frequently involved surgical site was the gastrointestinal system (91.4%, n = 64), followed by ophthalmologic (12.9%, n = 9) and cardiovascular procedures (12.9%, n = 9). Surgical interventions involving the joints and bones (5.7%, n = 4), respiratory system (5.7%, n = 4), brain (1.4%, n = 1), and urogenital system (1.4%, n = 1) were less common (Table 2).
Invasive device utilization was highly prevalent. Urinary catheterization was present in all cases (100%, n = 70), followed by nasogastric tube placement (91.4%, n = 64), endotracheal intubation (85.7%, n = 60), central venous catheterization (44.3%, n = 31), tracheostomy (38.6%, n = 27), and percutaneous endoscopic gastrostomy (10.0%, n = 7). This extensive use of invasive devices reflects the severity of illness in the ICU population and represents a potential facilitating factor for Myroides spp. colonization and infection.
Antimicrobial Resistance Profile and Treatment Outcomes
All Myroides spp. isolates included in the analysis were classified as multidrug-resistant (MDR), exhibiting high resistance rates to nearly all routinely used antimicrobial classes. Resistance was particularly pronounced against penicillins (95.3%), third- and fourth-generation cephalosporins (96.5% and 89.2%, respectively), fluoroquinolones (98.4%), aminoglycosides (96.9%), monobactams (100%), and carbapenems (96.8%) (Table 3). This extensive resistance profile highlights the limited role of conventional empirical regimens for the treatment of Myroides spp. infections in ICU settings.
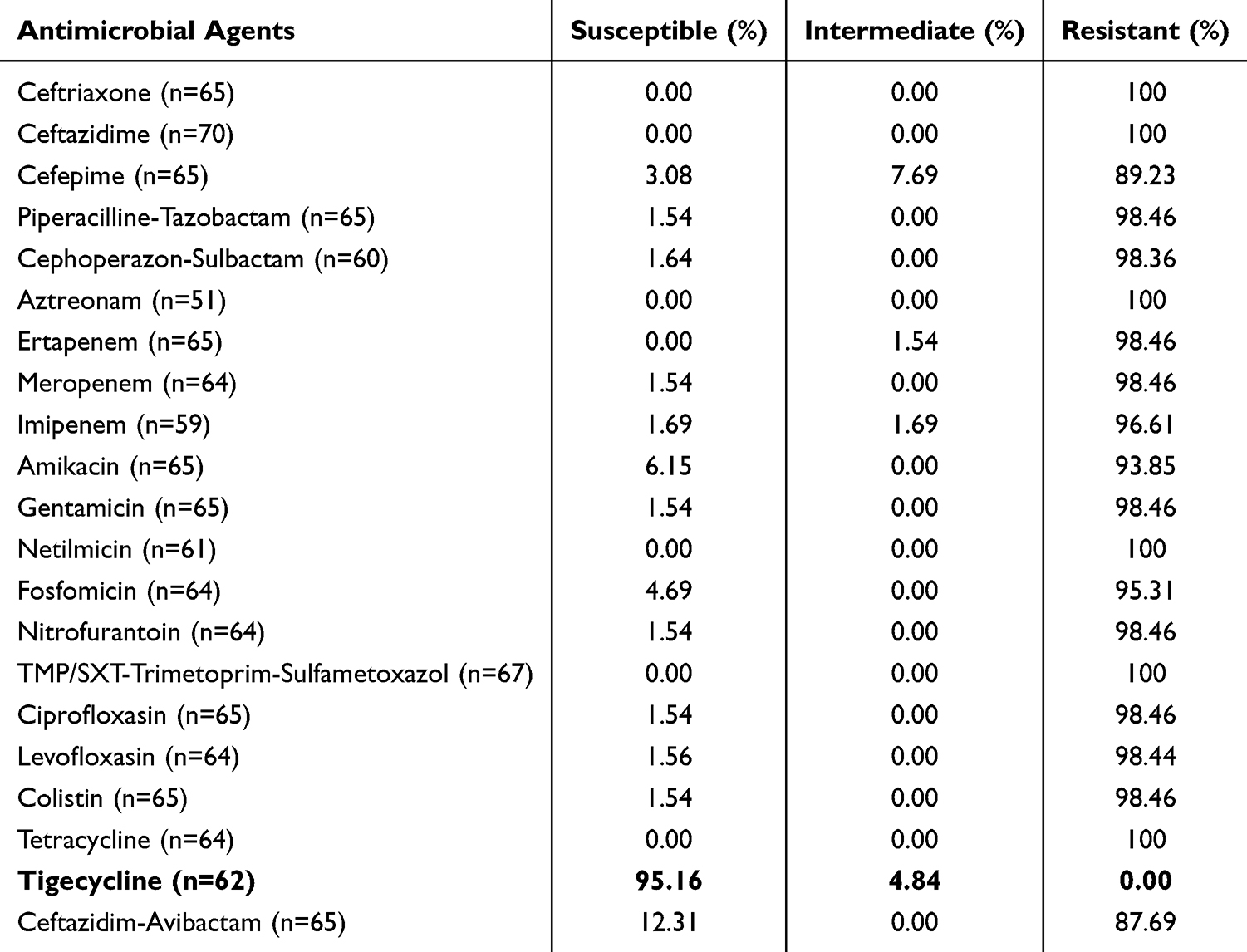 |
Table 3 Antimicrobial Susceptibility Test Results of Myroides Spp |
Among the tested agents, tigecycline demonstrated the highest in vitro activity, with 95.1% of isolates classified as susceptible. Tigecycline showed high in vitro activity and clinical use, but no claims of therapeutic superiority beyond descriptive observations are made. The mean duration of tigecycline therapy was 10.3 ± 6.05 days, reflecting its use as a short- to mid-term definitive treatment rather than prolonged suppressive therapy. Treatment outcomes are reported descriptively; claims of superiority of tigecycline over other agents are avoided.
The mean length of hospitalization prior to the diagnosis of Myroides spp. infection was 43.91 ± 31.7 days (Table 4), indicating that infections predominantly developed after prolonged ICU stays. This finding suggests that Myroides spp. infections are closely associated with long-term hospitalization, extensive antimicrobial exposure, and the presence of invasive devices, rather than representing early-onset ICU-acquired infections. Detailed treatment durations and microbiological eradication outcomes are summarized in Table 4.
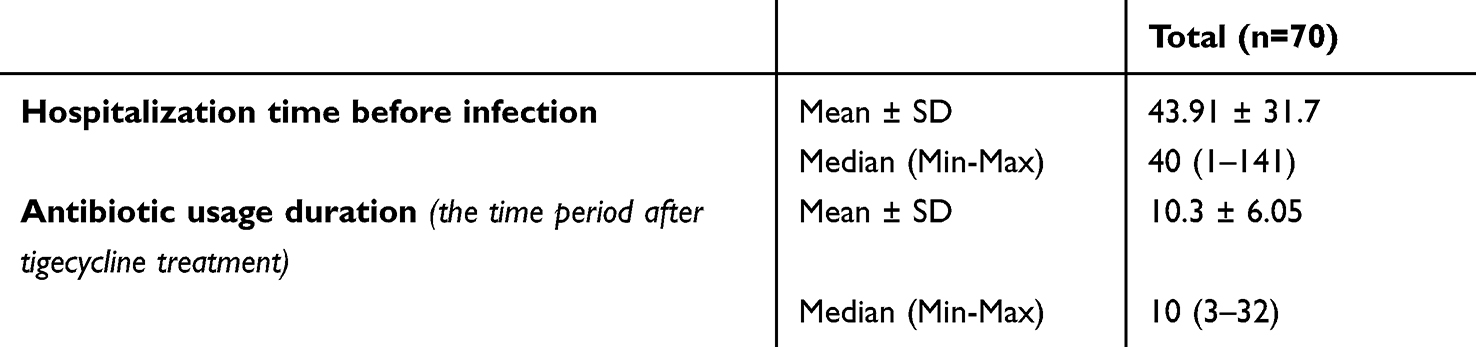 |
Table 4 Microbial Eradication of Myroides Spp. After Antimicrobial Therapy |
These findings suggest that while Myroides spp. can exhibit multidrug resistance, its clinical behavior is typically non-aggressive and localized, particularly in immunocompetent individuals. Notably, empirical therapies that did not include tigecycline were largely ineffective. The high susceptibility of the isolates to tigecycline, both in vitro and in clinical application, highlights the importance of early adjustment of therapy based on culture and susceptibility results. Our findings support the use of tigecycline as an effective treatment option for MDR Myroides spp. infections, particularly in settings where species-level identification and broader susceptibility testing are limited.
Ktari et al21 reported that all Myroides spp. isolates in their study were resistant to the panel of antibiotics tested. While three patients were successfully treated with a combination of ciprofloxacin and rifampicin, most of the isolates exhibited resistance to both agents. Additionally, their study highlighted the pathogenic potential of M. odoratus, which was implicated in cases of cellulitis in immunocompromised patients and urinary tract infections, particularly in those with urinary stones or neoplasms. The authors emphasized the species’ broad antimicrobial resistance and its role in prolonged nosocomial outbreaks, underscoring the need to consider M. odoratimimus as a significant hospital-acquired pathogen.
In contrast to these findings, Myroides spp. isolates in our cohort, although multidrug-resistant, were not associated with widespread or invasive infections. Most cases involved localized urinary tract infections, and no outbreaks were observed during the study period. Furthermore, while Bektas et al20 reported clinical success in 5 out of 7 patients treated with ciprofloxacin and rifampicin, our isolates showed minimal susceptibility to ciprofloxacin. Tigecycline was the only antimicrobial agent with consistently high efficacy, with a susceptibility rate of 95.16%. Notably, Bektas et al also identified poorly controlled diabetes as a potential risk factor for Myroides-related outbreaks, a factor that was present in a subset of patients in our study.
Our findings confirm the multidrug-resistant (MDR) nature of Myroides spp., with resistance rates exceeding 95% for commonly used antibiotics, including penicillins, cephalosporins, aminoglycosides, monobactams, and carbapenems. Tigecycline stood out as the only agent with consistent efficacy, demonstrating a susceptibility rate of 95.16%, in alignment with previous studies.20,22,23 Meyer et al reported that all Myroides spp isolates in their series exhibited resistance to nearly all tested antimicrobials.23 While two patients responded favorably to tigecycline therapy, one was concurrently receiving treatment for an unrelated infection. Interestingly, although some isolates in their study were reportedly resistant to tigecycline in vitro, the clinical response was comparable to our findings. One notable difference, however, was the predominance of immunosuppressed patients in their cohort, whereas the majority of our patients were immunocompetent. Taskin Kafa and Hasbek24 explored the in vitro efficacy of cefotaxime, meropenem, and ciprofloxacin, individually and in combination, against both planktonic and biofilm forms of M. odoratimimus. Their results supported the use of cefotaxime/meropenem and ciprofloxacin-based combinations, particularly in ICU patients with immunosuppression. In contrast, the isolates in our study were resistant to these antibiotics, and our clinical management relied on tigecycline monotherapy.25 Agrawal et al described 16 cases of Myroides infections among catheterized ICU patients, with 69% having diabetes mellitus.26 Despite the overall high resistance, all isolates were susceptible to minocycline. While we did not utilize minocycline, our findings are consistent with the efficacy of tetracycline-class antibiotics; tigecycline, a newer-generation agent from this class, achieved successful treatment outcomes in our cohort.27–30 Our study further strengthens these findings by providing data from a larger patient population. Oyardi et al12 reported that Myroides spp. infections predominantly occurred in immunosuppressed individuals. In contrast, most of our cases were observed in immunocompetent patients, and corticosteroid use was relatively uncommon in our cohort.
Limitations
The study has some limitations. The inability to perform species-level identification (ie, M. odoratus vs M. odoratimimus) due to reliance on VITEK 2 remains a key limitation. Future studies should incorporate molecular typing techniques to elucidate species-specific resistance patterns. Authors recognize that the study does not explore novel resistance mechanisms, comparative treatment effectiveness, predictive modeling, or inferential risk factor analysis. In summary, while the study findings are not transformative, it provides meaningful descriptive epidemiological insights, particularly regarding infection localization, colonization prevalence, and regional resistance patterns, which are valuable for clinicians managing ICU patients with Myroides spp infections.
While tigecycline demonstrated high in vitro susceptibility and favorable clinical outcomes in our cohort, the underlying mechanisms of multidrug resistance, including potential metallo-β-lactamase activity, were not explored in detail. Finally, as multivariate analyses were not conducted, associations between patient characteristics, comorbidities, and outcomes should be interpreted with caution. Despite these limitations, our findings provide valuable real-world evidence supporting the use of tigecycline in empirical therapy for MDR Myroides infections in ICU settings, particularly in regions where case reports currently dominate the literature.
Conclusion
In this study, Myroides spp. is confirmed as a rare but clinically significant opportunistic pathogen in hospital settings, particularly among critically ill adult patients. The isolates exhibited extensive multidrug resistance, with resistance rates exceeding 95% for most commonly used antibiotics, including penicillins, cephalosporins, aminoglycosides, monobactams, and carbapenems. Among the 70 cases analyzed, only one patient developed an invasive infection, whereas the majority were localized urinary tract infections, demonstrating that Myroides spp. infections are generally non-aggressive and localized, even in the presence of multidrug resistance. Notably, the affected patients were largely immunocompetent, yet many had underlying comorbidities such as cardiovascular and central nervous system disorders, suggesting that advanced age and comorbidity, rather than immunosuppression, play a key role in susceptibility to clinically significant infections.
Tigecycline emerged as the most effective therapeutic option, achieving rapid microbiological eradication and proving superior to other empirical therapies that were largely ineffective. This underscores the critical importance of early, culture-guided, and species-specific antimicrobial therapy in managing MDR Myroides infections. Despite the overall non-invasive nature of most cases, the potential for severe outcomes, including bacteremia and pneumonia, highlights the necessity for timely diagnosis, vigilant clinical monitoring, and evidence-based antimicrobial management. These findings challenge the conventional view that Myroides primarily affects immunosuppressed individuals and support tigecycline as a first-line treatment for multidrug-resistant isolates, while also emphasizing the need for future research on resistance mechanisms and alternative therapeutic strategies to optimize patient outcomes.
In conclusion, the isolates demonstrated near-universal resistance to commonly used antimicrobial agents, while tigecycline exhibited high in vitro susceptibility and favorable clinical outcomes, supporting its potential role as an empirical treatment option for MDR Myroides spp infections. These findings also challenge the traditional association of Myroides spp infections exclusively with immunosuppressed hosts. Future studies should further investigate resistance mechanisms and monitor the potential emergence of tigecycline resistance with increasing clinical use.
Ethics
The study was approved by the Ethics Committee of Istanbul Atlas University (Decision Number: E-22686390-050.99-26196). Written informed consent was obtained from all patients included in the study.
Acknowledgments
We would like to thank Istanbul Atlas University Medicine Hospital Medical Laboratory workers and Infection Diseases Committee staff.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study has no received financial support.
Disclosure
The authors have no conflict of interest to declare.
References
1. Beharrysingh R. Myroides bacteremia: a case report and concise review. IDCases. 2017;8:34–12. doi:10.1016/j.idcr.2017.02.012
2. O’Neal M, Labay CE, Harris JE, et al. Extensively drug-resistant Myroides odoratus in critically ill patients: a case series and literature review. Case Rep Infect Dis. 2022;2022(1):6422861. doi:10.1155/2022/6422861
3. Ram H, Kumar A, Thomas L, Dastager SG, Mawlankar R, Singh VP. Myroides indicus sp. nov. isolated from garden soil. Int J Syst Evolut Microbiol. 2015;65(Pt_11):4008–4012. doi:10.1099/ijsem.0.000530
4. Lorenzin G, Piccinelli G, Carlassara L, et al. Myroides odoratimimus urinary tract infection in an immunocompromised patient: an emerging multidrug-resistant micro-organism. Antimicrob Resist Infect Control. 2018;7(1):96. doi:10.1186/s13756-018-0391-4
5. Pérez-Lazo G, Morales-Moreno A, Soto-Febres F, et al. First report of Myroides phaeus bacteraemia identified by Polymerase chain reaction and genetic sequencing. IDCases. 2020;19:e00695. doi:10.1016/j.idcr.2020.e00695
6. Sahu C, Chaudhary R, Bhartiya C, Patel SS, Bhatnagar N. A retrospective study on UTI by Myroides species: an emerging drug resistant nosocomial pathogen. Indian J Crit Care Med. 2024;28(4):399–403. doi:10.5005/jp-journals-10071-24683
7. Savci U, Eser B, Sungur M, et al. A new emerging threat in critical care: Myroides odoratimimus outbreak in a tertiary hospital. Indian J Crit Care Med. 2025;29(10):829–838. doi:10.5005/jp-journals-10071-25071
8. Alabdely MH, Englund K, Shrestha NK. Clinical features and outcomes of Myroides species infections. Open Forum Infect Dis. 2025;12(2):ofaf049. doi:10.1093/ofid/ofaf049
9. Benedetti P, Rassu M, Pavan G, Sefton A, Pellizzer G. Septic shock, pneumonia, and soft tissue infection due to Myroides odoratimimus: report of a case and review of Myroides infections. Infection. 2011;39(2):161–165. doi:10.1007/s15010-010-0077-1
10. Hu S-H, Yuan S-X, Qu H, et al. Antibiotic resistance mechanisms of Myroides sp. J Zhejiang Univ Sci B. 2016;17(3):188–199. doi:10.1631/jzus.B1500068
11. Choudhury B, Durairaj E, Khyriem A, Rajbongshi J, Lyngdoh V. Septicaemia caused by Myroides spp. - A case report. JMM Case Rep. 2015;2. doi:10.1099/jmmcr.0.000097
12. Oyardi O, Eltimur T, Demir ES, et al. Antibacterial and antibiofilm activities of ceragenins alone and in combination with levofloxacin against multidrug resistant Myroides spp. clinical isolates from patients with urinary tract infections. Curr Microbiol. 2023;80(6):210. doi:10.1007/s00284-023-03321-0
13. Gülmez A, Ceylan AN, Özalp O. An increasing threat in intensive care units: evaluation of multi-drug-resistant Myroides spp. infections and risk factors. J Hosp Infect. 2023;137:8–16. doi:10.1016/j.jhin.2023.04.010
14. Al-Dorzi HM, Asiri AM, Shimemri A, et al. Impact of empirical antimicrobial therapy on the outcome of critically ill patients with Acinetobacter bacteremia. Ann Thorac Med. 2015;10(4):256–262. doi:10.4103/1817-1737.164302
15. Riccobene T, Ye G, Lock J, et al. Outcomes of inadequate empiric therapy and timing of newer antibacterial therapy in hospitalized adults with culture-positive Enterobacterales and Pseudomonas aeruginosa: a multicenter analysis. BMC Infect Dis. 2024;24(1):810. doi:10.1186/s12879-024-09700-7
16. Ippolito M, Cortegiani A. Empirical decision-making for antimicrobial therapy in critically ill patients. BJA Educ. 2023;23(12):480–487. doi:10.1016/j.bjae.2023.09.001
17. Khan U, Pandey E, Gandham N, et al. A case series and literature review of infections due to Myroides spp.: identification of contributing factors and emerging antibiotic susceptibility trends. Access Microbiol. 2023;5(5). doi:10.1099/acmi.0.000549.v2
18. Licker M, Sorescu T, Rus M, et al. Extensively drug-resistant Myroides odoratimimus - a case series of urinary tract infections in immunocompromised patients. Infect Drug Resist. 2018;11:743–749. doi:10.2147/idr.S161069
19. Schröttner P, Rudolph WW, Eing BR, Bertram S, Gunzer F. Comparison of VITEK2, MALDI-TOF MS, and 16S rDNA sequencing for identification of Myroides odoratus and Myroides odoratimimus. Diagn Microbiol Infect Dis. 2014;79(2):155–159. doi:10.1016/j.diagmicrobio.2014.02.002
20. Bektas S, Tümtürk A, Akdağ A, Izdes S. An outbreak of urinary tract infections due to Myroides spp in adult intensive care unit: risk factors and control procedures. J Cardio-Vascular-Thor Anaesth Intens Care Soc. 2021. doi:10.5222/GKDAD.2021.46704
21. Ktari S, Mnif B, Koubaa M, et al. Nosocomial outbreak of Myroides odoratimimus urinary tract infection in a Tunisian hospital. J Hosp Infect. 2012;80(1):77–81. doi:10.1016/j.jhin.2011.09.010
22. Kurt AF, Mete B, Houssein FM, et al. A pan-resistant Myroides odoratimimus catheter-related bacteremia in a COVID-19 patient and review of the literature. Acta Microbiol Immunol Hung. 2022;69(2):164–170. doi:10.1556/030.2022.01702
23. Meyer A, Dang H, Roland W. Myroides spp. cellulitis and bacteremia: a case report. IDCases. 2019;18:e00638. doi:10.1016/j.idcr.2019.e00638
24. Taşkın Kafa AH, Hasbek M. Synergistic efficacy of meropenem, ciprofloxacin and colistin antibiotics against planktonic and biofilm forms of Myroides odoratimimus bacterial isolates. Indian J Med Microbiol. 2022;40(3):399–403. doi:10.1016/j.ijmmb.2022.04.004
25. LaVergne S, Gaufin T, Richman D. Myroides injenensis Bacteremia and Severe Cellulitis. Open Forum Infect Dis. 2019;6(7):ofz282. doi:10.1093/ofid/ofz282
26. Agarwal M, Mamoria V, Mittal S, Sharma A. Myroides: an emerging pathogen causing urinary tract infections in hospitalized patients. Int J Contem Med Res. 2019;6. doi:10.21276/ijcmr.2019.6.11.28
27. Jiang LZ, Shen Y, Liang F, Ye XM, Chen J, Yu YM. Intracranial Myroides odoratimimus infection after EVD successfully treated with intravenous plus intraventricular tigecycline: a case report. Infect Drug Resist. 2023;16:1955–1963. doi:10.2147/idr.S403088
28. Ezer B, Arslan GK, Doğan M, Özdemir M. Antibiogram susceptibility of the Myroides species isolated from clinical specimens. Mev Med Sci. 2021;1(3):75–78.
29. Duman Y, Çelik D, Parmaksız EN, Ersoy Y, Özer AB. Are Myroides spp. isolated from urinary catheter cultures of patients in intensive care units an infection or colonization? Analysis of 36 cases. Turk J Intens Care. 2024;22(3):207–211. doi:10.4274/tybd.galenos.2023.64497
30. Kara I, Kalem F, Unaldi O, Arslan U. Myroides sp, a rare opportunistic infective agent, at a hospital in Turkey. Southeast Asian J Trop Med Public Health. 2019;50(2):248–257.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.