Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 18
Clinical and Microbiological Changes Following Multi-Strain Probiotic Mouthrinse Use in Dental Students with Halitosis: A Prospective Single-Arm Study
Authors Ahmed KM ![]()
Received 15 March 2026
Accepted for publication 19 May 2026
Published 26 May 2026 Volume 2026:18 609391
DOI https://doi.org/10.2147/CCIDE.S609391
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Christopher E. Okunseri
Khadija Muhamed Ahmed
Department of Oral Diagnosis (Oral Medicine), College of Dentistry, University of Sulaimani, Sulaymaniyah, Kurdistan Region, Iraq
Correspondence: Khadija Muhamed Ahmed, Email [email protected]
Background: Halitosis is a common oral health condition that negatively affects social interactions, psychological well-being, and professional confidence, particularly among dental students. Conventional antimicrobial mouthwashes, although effective, are associated with adverse effects and disruption of the oral microbiota. Probiotics have emerged as a promising alternative for modulating microbial communities and enhancing oral ecological balance. Quantitative real-time polymerase chain reaction (qPCR) enables detailed assessment of microbiological changes associated with halitosis.
Aim: To assess the clinical and microbiological changes associated with a multi-strain probiotic mouthrinse containing Lactobacillus reuteri and Lactobacillus paracasei in dental students with halitosis using qPCR.
Materials and Methods: This prospective single-arm study included dental students with clinically confirmed halitosis (organoleptic test [OLT] score ≥ 2). Participants used the probiotic mouthrinse three to four times daily for 14 days. Clinical parameters, including OLT, tongue-coating area (Ta), tongue-coating thickness (Tt), and total tongue-coating score (TCS), were assessed at baseline, day 7, and day 14. Stimulated whole saliva samples were collected at each time point and analyzed using qPCR to assess relative changes in Streptococcus mutans, Lactobacillus salivarius, and Porphyromonas gingivalis.
Results: Thirty-four participants completed the study. Significant reductions were observed in OLT, Ta, Tt, and TCS over the 14-day period (p < 0.001). qPCR analysis demonstrated reduced abundance of S. mutans and L. salivarius, with a modest decrease in P. gingivalis. Improvements in OLT were significantly associated with changes in bacterial profiles, particularly S. mutans and P. gingivalis (p < 0.001). A strong positive correlation was consistently observed between TCS and OLT at all time points (p < 0.001).
Conclusion: Within the limitations of this study, the probiotic mouthrinse was associated with improvements in clinical indicators of halitosis and favorable shifts in selected oral microbiota. These findings support further investigation through well-designed randomized controlled trials. An infographic on a 14-day probiotic mouthrinse study for halitosis outcomes in dental students.An infographic outlines a study on dental students with halitosis confirmed by organoleptic testing (OLT). The intervention involved using a multi-strain probiotic mouthrinse containing Lactobacillus reuteri and Lactobacillus paracasei, applied 3-4 times daily for 14 days. Outcomes assessed included clinical and microbiological changes. Clinical outcomes showed improvements in organoleptic and tongue coating scores. Microbiological outcomes, measured by qPCR, indicated changes in Ct values and a decrease in the relative abundance of specific bacteria, including Porphyromonas gingivalis, Streptococcus mutans and Lactobacillus salivarius. The study concluded that 14 days of using the probiotic mouthrinse led to significant clinical and microbiological changes in the oral microbiota.
Keywords: halitosis, lactobacillus paracasei, lactobacillus reuteri, organoleptic test, probiotic mouthrinse, qPCR, tongue coating
Introduction
Halitosis, or oral malodor, is a clinical condition characterized by offensive odors originating from the oral cavity and is the third most common reason for seeking dental consultations.1,2 Its etiology is multifactorial, with the primary cause being associated with microbial metabolic activity in the oral cavity. Approximately 90% of cases are derived from intraoral sources, which involve the production of volatile sulfur compounds (VSCs) such as hydrogen sulfide, methyl mercaptan, and dimethyl sulfide.3
In young adults, including dental students, halitosis exerts an influence that extends beyond physiological discomfort as an offensive odor to impose a significant psychosocial burden.4 It is associated with reduced social engagement, diminished self-esteem, embarrassment, and social isolation, adversely affecting quality of life.5 The presence of bad odors poses a significant challenge for dental students as they train to become oral healthcare providers. Persistent oral malodor in this demographic group can create a notable disconnect between their professional knowledge and personal experiences, resulting in impaired interpersonal interactions, diminished self-esteem, social anxiety, and possibly undermined self-confidence during engagement with patients or peers, all of which can adversely affect their clinical training and professional identity.5,6
Although the prevalence of self-perceived oral malodor differs by region, studies have consistently reported elevated rates among dental students. For example, a notable rate of 75.1% was documented in Lahore, Pakistan, underscoring the necessity for targeted and effective therapeutic strategies.7 Local studies indicate a significant prevalence, affecting approximately 40% of dental students.8 Despite widespread toothbrushing, the use of adjuncts such as dental floss and tongue cleaners remains inconsistent.9
Conventional halitosis management typically employs antimicrobial agents such as chlorhexidine to decrease bacterial load and mitigate symptoms.10,11 Long-term use of these products is linked to adverse effects such as tooth staining and dysgeusia, as they no selectively eliminate both pathogenic and beneficial bacteria, thereby disrupting the overall oral microbiome.12 These clinical findings highlight the need for safer and more innovative therapeutic strategies to treat this disease. Probiotics have emerged as promising alternatives for effective halitosis management and the promotion of a balanced oral microbiome.13
Probiotics are live microorganisms that provide health benefits to a host when administered in sufficient quantities. Their potential application in oral health management has been increasingly investigated. Their approach to managing halitosis involves interrupting biochemical pathways that contribute to VSC production.14,15 Recent systematic reviews have suggested that probiotic-based interventions may contribute to reductions in oral malodor and volatile sulfur compound levels, although variability in probiotic strains, intervention duration, and outcome measures remains considerable.16 Specific strains, such as Lactobacillus reuteri and Lactobacillus paracasei, operate through various mechanisms, including competitive inhibition of ecological niches and synthesis of antimicrobial compounds such as reuterin, which specifically targets and inhibits VSC-producing pathogens.17,18 It was hypothesized that short-term use of the multi-strain probiotic mouthrinse would be associated with reductions in clinical halitosis indicators and targeted bacterial species.17
The formulation of these probiotics into a mouthwash introduces a novel delivery method that extends their residence time in the oral cavity and improves direct interaction with pathogenic biofilms. This approach may provide a more targeted and safer alternative to systemic methods.19 Nonetheless, the gr0owing market for oral care probiotics includes products with unverified claims and include species and strains without established efficacy. This variability, coupled with a decentralized regulatory framework that shifts the burden of proof to manufacturers, creates confusion and mistrust among both consumers and clinicians.20 Consequently, a thorough evidence-based assessment of specific probiotic strains is essential.
Although the psychosocial effects of halitosis are well documented and probiotic therapies show promise, integrated studies combining clinical outcomes with molecular validation remain scarce. In particular, relatively few studies have evaluated a commercially available multi-strain probiotic mouthrinse in dental students using combined clinical halitosis assessment and targeted qPCR-based microbiological outcomes.
The present study therefore aimed to explore both the clinical and microbiological changes associated with probiotic mouthrinse use in halitosis management. The selected qPCR panel included Porphyromonas gingivalis, Streptococcus mutans, and Lactobacillus salivarius, based on their reported roles in oral microbial ecology and potential associations with oral malodor.Porphyromonas gingivalis is a well-recognized anaerobic pathogen with proteolytic activity that contributes to the production of volatile sulfur compounds (VSCs), which are directly associated with oral malodor.3,14 While Streptococcus mutans is primarily linked to dental caries, its involvement in biofilm formation and microbial interactions may contribute to oral dysbiosis and indirectly influence malodor development.13,21 Lactobacillus salivarius, although regarded as a beneficial commensal species, has also been identified as an indicator of oral microbial equilibrium, with variations in its abundance may reflect competitive interactions within the oral microbiome.14,22 Importantly, L. salivarius was evaluated in the present study as a resident oral commensal species rather than as a surrogate marker for the administered probiotic strains (Lactobacillus reuteri and Lactobacillus paracasei). Consequently, evaluating these bacterial species may yield insights into microbial alterations linked to probiotic mouthrinse application in halitosis treatment.
The primary objective of this study was to evaluate the clinical efficacy of probiotic mouthwashes containing Lactobacillus reuteri and Lactobacillus paracasei in alleviating the clinical symptoms of halitosis, including organoleptic, tongue coating, and microbial load assessments. To achieve this, dental students with halitosis, as verified by organoleptic assessment, were involved. The secondary objective was to investigate changes in selected oral bacterial species using targeted quantitative real-time polymerase chain reaction (qPCR). Although qPCR provides sensitive and specific quantification of predefined bacterial targets, it does not provide comprehensive profiling of overall microbial diversity.This prospective experimental study was designed as a preliminary investigation to provide substantial, clinically relevant data on oral microbiology, thereby providing preliminary clinically relevant data to inform future controlled trials.
Materials and Methods
Study Design and Setting
This prospective experimental study with repeated assessments at baseline, day 7, and day 14 aimed to evaluate the clinical and microbiological effectiveness of a probiotic mouth rinse in treating halitosis among dental students. The 14-day intervention period was selected to evaluate early short-term microbial and clinical responses to probiotic administration. This research was conducted at the College of Dentistry, University of Sulaimani (Kurdistan Region, Iraq) between July 2025 and December 2025. Ethical approval was obtained from the Ethics Committee of the College of Dentistry, University of Sulaimani (Approval No. 204/23; November 2, 2023). All participants were informed about the study aims and procedures and provided written consent prior to enrolment. This study was prospectively registered in the ISRCTN registry (ISRCTN10448956).
Sample size estimation the current study design was conducted using G*Power 3.1. With parameters set at α = 0.05, statistical power = 0.80, and a medium effect size (Cohen’s d = 0.5), the required sample size calculated was 30 participants. Our study enrolled 34 participants, thereby exceeding this threshold. Following study completion, a substantially larger post-hoc effect size was observed for OLT reduction (d ≈ 2.7), which should be interpreted cautiously given the exploratory nature and limited sample size of the study.
Furthermore, the achieved statistical power was greater than 0.99, confirming that the study was adequately powered to detect clinically meaningful differences.
Participants
Participants were recruited using a convenience sampling approach from eligible dental students attending the Oral Diagnosis Department, University of Sulaimani. Eligible students were instructed to use a commercially available probiotic mouthrinse (Riven Probiotic Mouthwash, USA, CGMP-certified facility) containing Lactobacillus reuteri and Lactobacillus paracasei strains three to four times daily, according to the manufacturer’s instructions, to enhance probiotic exposure and oral colonization throughout the study period. This frequency was selected to optimize probiotic activity and colonization within the oral cavity, rather than to replicate conventional antiseptic mouthwash regimens. Furthermore, participants were instructed to use approximately 10–15 mL of the mouthrinse per application, rinse for approximately 30–60 seconds, and avoid eating or drinking for at least 30 minutes afterward.
Inclusion Criteria
The participants were required to be dental students of either sex who voluntarily agreed to participate after receiving a full explanation of the study. Only students with clinically confirmed halitosis, defined as an organoleptic test (OLT) score of ≥2, were included. None of the participants used systemic antibiotics or antibacterial mouth rinses during the month preceding the study period. Furthermore, participants with dental caries were not excluded, as caries-associated microbial activity may contribute to oral malodor and reflects the clinical reality of the study population.
Exclusion Criteria
Students were excluded if they declined to participate or had systemic conditions known to cause halitosis, including endocrine, gastrointestinal, or respiratory disorders. The exclusion was primarily based on detailed medical history and clinical examination, and no advanced systemic diagnostic investigations were performed.
Additional exclusion criteria included the use of systemic or topical antibacterial therapy within the past month, current or previous smoking, alcohol consumption, or professional dental treatment, specifically for halitosis, during the study period. Students who discontinued product use were excluded to ensure the reliability of the outcome measures.
Forty dental students fulfilled the criteria and underwent clinical evaluation.
Sample Collection
Stimulated whole saliva samples were collected from each participant on three occasions: baseline (Day 1), Day 7, and Day 14. Stimulated whole saliva collection was selected to standardize sample volume and facilitate reproducible molecular analysis across all sampling intervals.Samples were collected between 9:00 a.m. and 11:00 a.m. to minimize diurnal variation. The participants were instructed to refrain from eating or drinking for at least two hours before sampling. All the participants were asked to chew a piece of sugar-free gum to stimulate salivation. No professional prophylaxis or toothbrushing instructions were provided before or during the experimental period, and adherence to this protocol was confirmed on Days 1, 7, and 14. This approach was intended to preserve the participants’ habitual oral hygiene practices and minimize artificial behavioral modification during the observational intervention period.
During sampling, the participants were seated comfortably and asked to expectorate 5–10 mL of saliva in a sterile disposable plastic container using the spitting method. Samples were temporarily stored in a cooling box and subsequently transferred to a refrigerator before being frozen at −80 °C until analysis.
Extra- and Intraoral Examination and Halitosis Scoring
All clinical examinations were performed by an investigator, using an artificial light source and disposable diagnostic instruments (mouth mirrors and probes). The oral mucosa was inspected for lesions, swelling, or ulceration at eight intraoral sites: the buccal and labial mucosa, gingiva, palate, floor of the mouth, tongue, retromolar region, and lips.
Oral health status was documented based on the number of teeth present, carious lesions, restorations, DMFT index, and simplified oral hygiene index (OHI-S). Because the age range of the student population was not optimal for reliable periodontal assessment, the periodontal parameters [like Plaque Index (PLI), Probing Depth (PD), Bleeding Index (BI) and Bleeding on Probing (BOP %)] were not recorded.
Halitosis was assessed in the morning (9:00–11:00 a.m.) under standardized conditions. For 24 h before evaluation, participants were instructed to avoid odorous foods such as garlic, onions, leeks, and alcoholic beverages. They also refrained from eating, drinking, or tooth-brushing for two hours before testing.
Organoleptic assessment was performed according to established clinical methods widely used in halitosis evaluation.21,23 Simply the assessment was performed on a scale of 0–5. Participants closed their mouths for one minute and then exhaled slowly toward the examiner at a 10-cm distance. The scores were assigned as follows:
- no odor;
- barely noticeable;
- slight but clearly noticeable;
- moderate;
- strong and offensive; and 5, extreme foul.
A reduction in OLT score was considered indicative of a positive response to treatment.
The tongue coating was evaluated by assessing both the area (Ta) and thickness (Tt) of the coating. Ta was scored from 0–3 (0 = none; 1 = <1/3 of dorsum; 2 = <2/3; 3 = >2/3). The Tt was scored from 0 to 2 (0 = no coating, 1 = thin coating with visible papillae, and 2 = thick coating with obscured papillae). The tongue coating score (TCS) was calculated by multiplying Ta with Tt, following a previously described method.24 Additional details of the study methodology are shown in Figure 1.
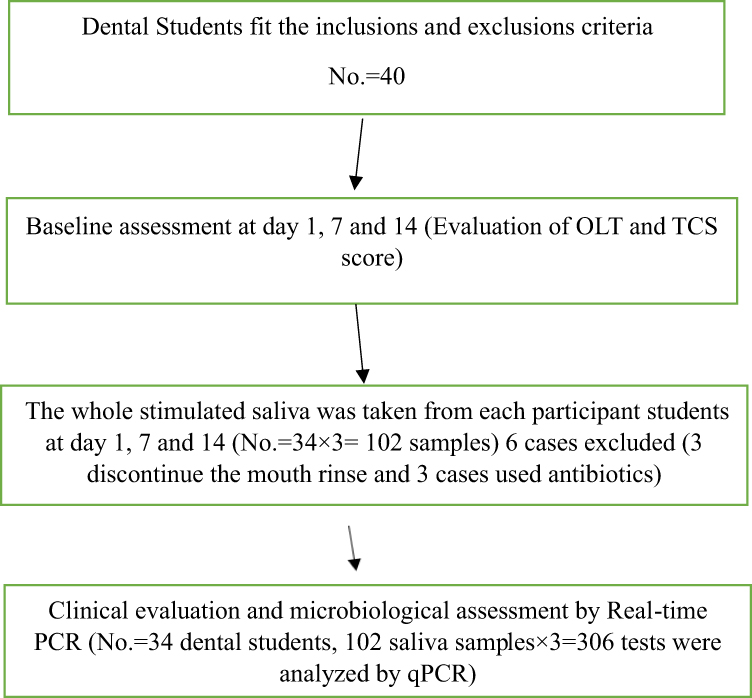 |
Figure 1 Schematic explanation of the study. Abbreviations: OLT, Organoleptic; TCS, Tongue coating score; PCR, Polymerase chain reaction. |
Microbiological Analysis
Genomic DNA Isolation
Bacterial genomic DNA was isolated from saliva samples using the AddBio® Blood and Tissue Genomic DNA Extraction Kit (AddBio Inc., South Korea), with minor modifications to optimize the protocol for liquid specimens. The procedure proceeds as followes: An initial volume of 1 mL of each mouthwash specimen was transferred to a 1.5-mL microcentrifuge tube and subjected to centrifugation at 10,000 × g for 10 min to concentrate the bacterial biomass. The resulting pellet was resuspended in 200 µL of lysis buffer and 20 µL of proteinase K, followed by incubation at 56 °C for 20 min to ensure efficient cellular lysis.
Subsequently, 200 µL of binding buffer and 200 µL of molecular-grade absolute ethanol (Merck, USA) were added sequentially. The mixture was then transferred to a silica-based spin column and centrifuged at 12,000 × g for 1 min. The column was washed consecutively with 500 µL of Wash Buffer 1 and 500 µL of Wash Buffer 2, with centrifugation at 12,000 × g after each step. A final dry spin was performed to remove any residual ethanol. For elution, 50–100 µL of pre-warmed nuclease-free water was applied to the column, incubated for 2 min, and collected by centrifugation at 6,000 × g. The concentration and purity of the extracted DNA were assessed using an Eppendorf BioPhotometer (Eppendorf AG, Hamburg, Germany). All samples were stored at −20 °C pending further analysis.
Quantitative Real-Time PCR (qPCR)
Quantitative real-time PCR (qPCR) was employed to quantify the abundance of selected bacterial species within the saliva samples. The bacterial load of Streptococcus mutans, Lactobacillus salivarius, and Porphyromonas gingivalis was determined through qPCR by analysis of cycle threshold (Ct) values, utilizing species-specific primers (detailed in Table 1).
 |
Table 1 Sequences of the Primers Used in This Study |
Each qPCR assay was conducted in a 20 µL reaction mixture. This mixture comprised 10 µL of 2× SYBR Green Master Mix, 0.3 µM of each forward and reverse primer, 2 µL of DNA template (standardized to a concentration of 100 ng per reaction), and nuclease-free water to reach the final volume. The amplification protocol consisted of an initial denaturation step at 95 °C for 3 min, followed by 40 cycles of denaturation at 95 °C for 10s and a combined annealing/extension step at 60 °C for 30s.
Amplification specificity was verified by performing a melt-curve analysis over a temperature gradient of 65–95 °C, which confirmed the presence of a single, distinct melting peak for each target amplicon. To ensure quantitative accuracy, amplification efficiency was evaluated using serial dilutions of template DNA; only assays demonstrating efficiencies between 90% and 110% and correlation coefficients (R2) of 0.98 or higher were considered acceptable for further analysis.
To monitor for potential contamination, both no-template controls and extraction-blank controls were included in each qPCR run. Finally, to evaluate shifting in the microbial profile over time, the Ct values for the targeted bacteria were analyzed comparatively across the three sampling time points for the participant students, thereby allowing for the assessment of relative changes in bacterial abundance.
Training and Calibration
To minimize examiner-related variability, all evaluations were performed by a single calibrated investigator. Calibration was obtained through duplicate assessment of 10 volunteers, giving intra-examiner reliability scores of κ = 0.82 for OLT and κ = 0.79 for TCS. Additionally, because all evaluations were conducted by a single examiner, inter-examiner agreement assessment was not applicable.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics (version 26.0; IBM Corp., Armonk, NY, USA). Continuous variables are summarized as mean ± standard deviation (SD), while categorical variables are presented as frequencies and percentages. The normality of data distribution was assessed using both the Shapiro–Wilk test and the Kolmogorov–Smirnov test, selected based on sample size and variable characteristics.
For ordinal clinical parameters, including tongue area (Ta), tongue thickness (Tt), tongue coating score (TCS), and organoleptic test score (OLT), changes across the three time points were first assessed using the Friedman test. Where significant overall differences were detected, post-hoc pairwise comparisons were subsequently performed using the Wilcoxon signed-rank test.
For microbiological quantification of bacterial species (Streptococcus mutans, Lactobacillus salivarius, and Porphyromonas gingivalis), Ct values obtained from real-time PCR were analyzed using repeated-measures analysis of variance (ANOVA) only after confirming acceptable parametric assumptions. Normality was assessed using the Shapiro–Wilk test, and sphericity was evaluated using Mauchly’s test, with Greenhouse–Geisser correction applied where appropriate. This approach allowed for the assessment of temporal changes in bacterial load across the three time points (sphericity was assessed using Mauchly’s test, and the Greenhouse–Geisser correction was applied where appropriate).
Additionally, Spearman’s rank correlation coefficient was employed to assess the associations between clinical parameters (TCS and OLT) and bacterial counts, as well as inter-bacterial relationships. This non-parametric test was selected because of the ordinal nature of the clinical scales and the non-linear distribution of the microbiological data.
Results
A total of 34 dental students, representing a young adult cohort aged 19–25 years, were enrolled in this study. The mean age was 22.18 ± 1.73 years (95% CI: 21.57–22.78).
The sex distribution revealed a modest female predominance, with female participants accounting for 55.88% (n = 19) and males comprising 44.12% (n = 15), with a female-to-male ratio of approximately 1.2:1.
The mean Decayed, Missing, and Filled Teeth (DMFT) index was 9.93 ± 2.89 (95% CI: 8.52–10.54), reflecting a substantially elevated burden of dental caries among the study population. According to the World Health Organization (WHO) caries experience classification, the majority of participants (88.24%, n = 30) were categorized as having very high caries experience, while 5.88% (n = 2) demonstrated moderate, 2.94% (n = 1) high, and 2.94% (n = 1) low caries experience.
The Simplified Oral Hygiene Index (OHI-S) recorded a mean score of 1.53 ± 0.66 (95% CI: 1.30–1.67), 55.88% (n = 19) of participants exhibited good oral hygiene, whereas 44.12% (n = 15) presented with fair hygiene levels as clearly elaborated in Table 2.
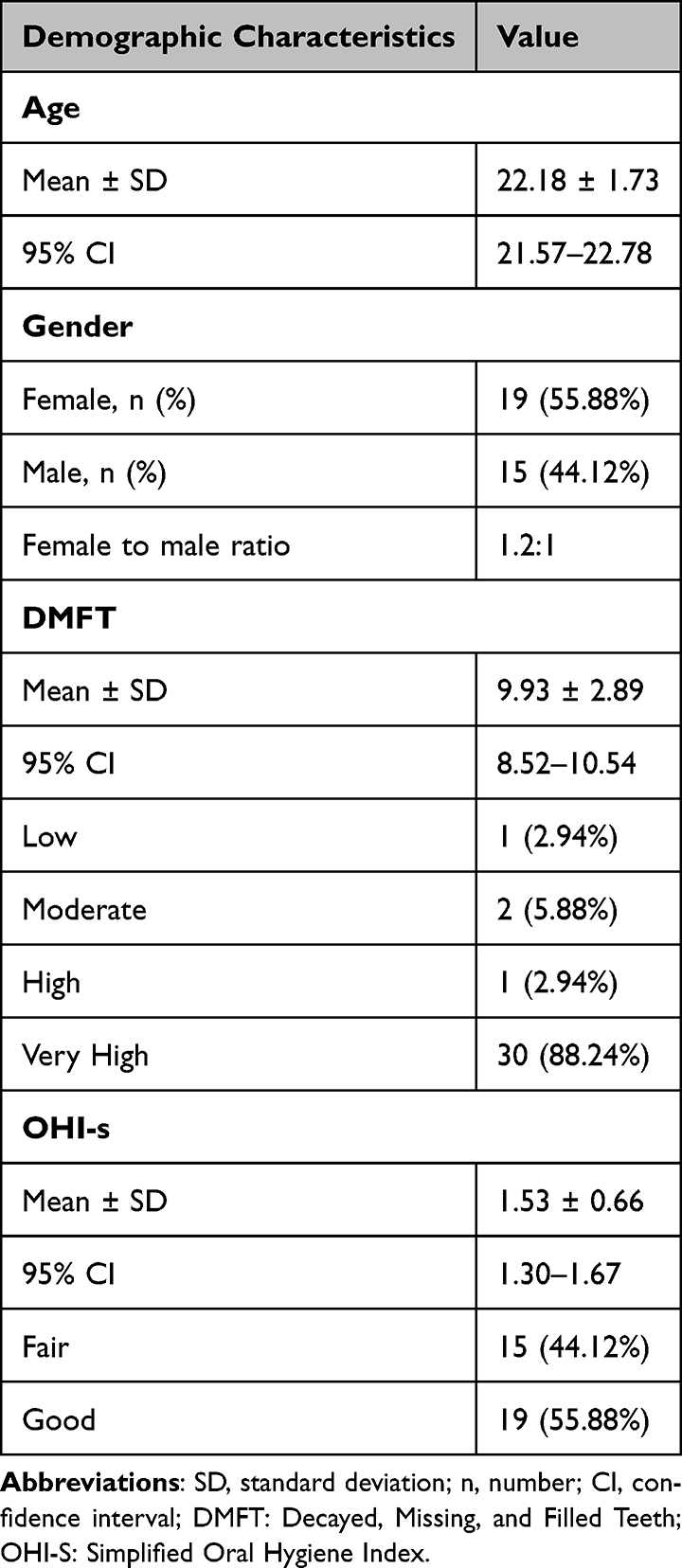 |
Table 2 Demographic and Oral Health Characteristics of Dental Students (n = 34) |
As shown in Table 3 and Figure 2, significant improvements were observed in the clinical and organoleptic parameters following probiotic mouth rinse over 14 days. The tongue area score (Ta) showed a progressive reduction from baseline (1.74 ± 0.67) to day 7 (1.58 ± 0.61) and day 14 (1.38 ± 0.62), with statistically significant differences across all time points (Pa = 0.034, Pb = 0.002, Pc = 0.014). Similarly, tongue thickness (Tt) decreased markedly from baseline (1.53 ± 0.71) to day 7 (1.06 ± 0.50) and remained stable at day 14 (1.03 ± 0.50), with highly significant reductions between baseline and both follow-up points (Pa < 0.001, Pb = 0.001), although the change between day 7 and day 14 was not significant (Pc = 0.655). The composite tongue coating score (TCS), derived by multiplying Ta and Tt, declined substantially from 2.65 ± 1.74 at baseline to 1.72 ± 0.96 on day 7 and 1.42 ± 1.02 on day 14, with all comparisons reaching statistical significance (Pa and Pb < 0.001; Pc = 0.033). Most notably, the organoleptic test (OLT) score, a direct measure of oral malodor, demonstrated a pronounced reduction from 3.97 ± 0.87 at baseline to 2.06 ± 0.67 on day 7 and 1.62 ± 0.68 on day 14. These changes were highly significant across all intervals (Pa and Pb < 0.001; Pc = 0.001), indicating a robust and sustained improvement in the severity of halitosis following probiotic intervention.
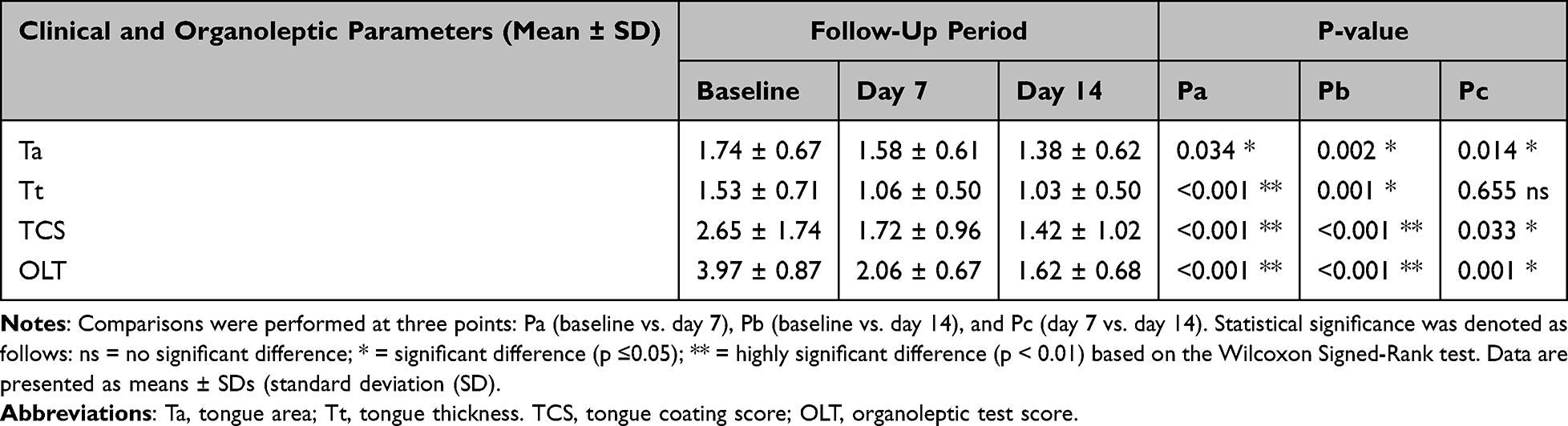 |
Table 3 Changes in the Clinical and Oral Malodor Parameters Between days 1, 7, and 14 |
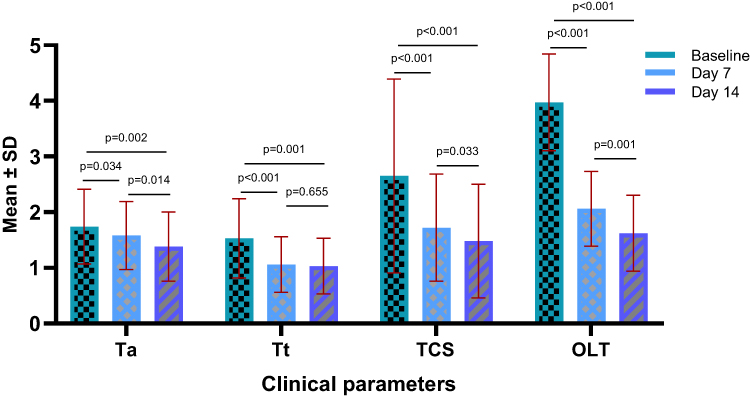 |
Figure 2 Longitudinal changes in tongue coating and oral malodor parameters following probiotic mouth rinse intervention. Abbreviations: OLT, organoleptic test; TCS, tongue coating score; Ta, tongue-coating area; Tt, tongue-coating thickness; Ct, cycle threshold. |
Threehundres six samples were quantified from 102 saliva samples. Quantitative PCR revealed dynamic shifts in the oral microbiota following probiotic mouth rinse administration, as reflected by changes in cycle threshold (Ct) values. [Lower Ct values indicate higher bacterial DNA abundance, whereas higher Ct values reflect a reduced bacterial load]. Notably, Streptococcus mutans exhibited an increase in Ct values from 25.03 ± 1.86 at baseline to 27.02 ± 1.28 on day 7 and 26.66 ± 1.97 on day 14, indicating a progressive reduction in its DNA abundance over time. The differences between the baseline and days 7 and 14 were highly significant (Pa and Pb < 0.001), whereas the change between days 7 and 14 was not significant (Pc = 0.317). Similarly, Lactobacillus salivarius showed a marked rise in Ct values from 29.34 ± 2.31 at baseline to 31.70 ± 2.20 on day 7 and 31.40 ± 1.99 on day 14, indicating reduced relative DNA abundance of the targeted Lactobacillus salivarius species. Because L. salivarius was not one of the administered probiotic strains in this study, this finding should be interpreted cautiously and may reflect species-specific ecological modulation or competitive microbial interactions rather than a generalized reduction in beneficial lactobacillia. Significant increase in Ct values was observed, indicating reduced bacterial DNA levels (which likely reflects competitive niche displacement rather than suppression of beneficial microbiom, as Lactobacillus salivarius was not the administered probiotic strain in this study). These differences were highly significant between baseline and both follow-up points (Pa and Pb < 0.001), with no significant difference between days 7 and 14 (Pc = 0.210). In contrast, Porphyromonas gingivalis demonstrated a modest increase in Ct values from 24.52 ± 2.47 at baseline to 25.62 ± 2.89 on day 7 and 25.77 ± 3.16 on day 14, also reflecting a reduction in bacterial DNA levels. The changes between baseline and both follow-up points were statistically significant (Pa = 0.007, Pb = 0.001), whereas the difference between days 7 and 14 was not significant (Pc = 0.857) (Table 4 and Figure 3).
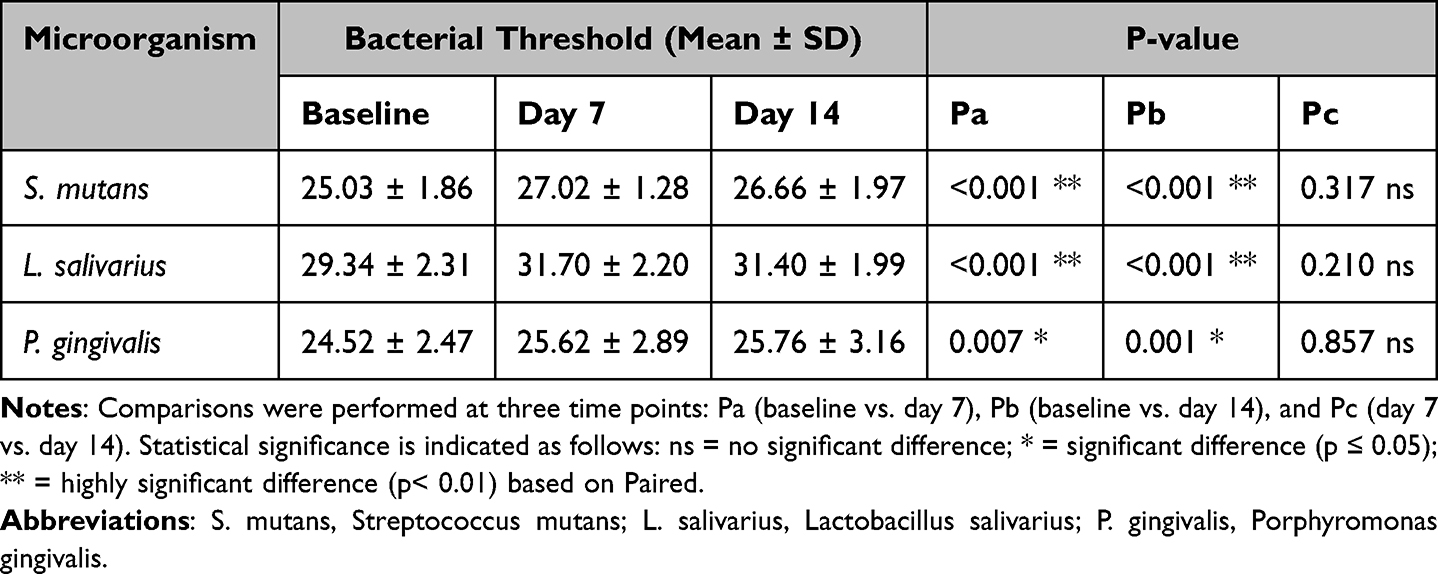 |
Table 4 Cycle Threshold (Ct) Values of Oral Bacterial Species at Three Time Points Using 100 ng DNA per qPCR Reaction |
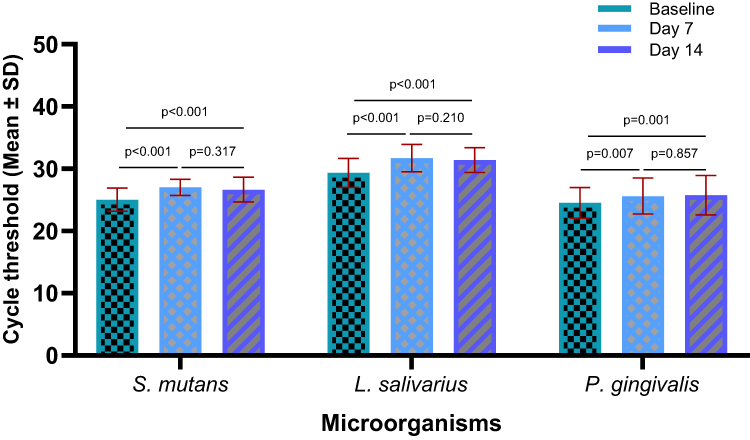 |
Figure 3 Cycle threshold-based quantification of oral bacterial species over time following probiotic mouth rinse intervention. |
Correlation analysis was conducted to investigate the relationships among clinical parameters, including tongue coating score (TCS), organoleptic test (OLT), and bacterial species (Streptococcus mutans, Lactobacillus salivarius, and Porphyromonas gingivalis) in dental students following probiotic mouth rinse use. A strong and consistent positive correlation was observed between TCS and OLT throughout the study period, confirming that greater tongue coating is closely associated with higher oral malodor severity. Specifically, TCS and OLT were significantly correlated at baseline (rho = 0.551, p = 0.001), day 7 (rho = 0.532, p = 0.002), and day 14 (rho = 0.443, p = 0.016).
Regarding microbial associations, OLT was significantly negatively correlated with S. mutans at baseline (rho = –0.406, p = 0.017), day 7 (rho = –0.364, p = 0.040), and day 14 (rho = –0.378, p = 0.043). This inverse numerical relationship indicated that higher OLT scores (reflecting worse malodor or higher CTS) were accompanied by increased S. mutans counts, suggesting a positive biological association between bacterial load and oral malodor severity. In contrast, no significant correlations were observed between OLT and L. salivarius throughout the study, whereas a significant negative association was found between OLT and P. gingivalis on day 14 (rho = –0.600, p = 0.001), suggesting that elevated P. gingivalis levels are linked to greater malodor intensity at this stage.
Correlations between the TCS and individual bacterial species remained weak and non-significant, indicating that the tongue coating index alone may not directly mirror bacterial abundance. Interbacterial analyses revealed significant and biologically relevant interactions on day 14, including a positive correlation between S. mutans and P. gingivalis (rho = 0.397, p = 0.033) and a moderate correlation between L. salivarius and P. gingivalis (rho = 0.492, p = 0.007). These findings suggest a possible synergistic coexistence among specific taxa during the later stages of probiotic intervention. As shown in Table 5.
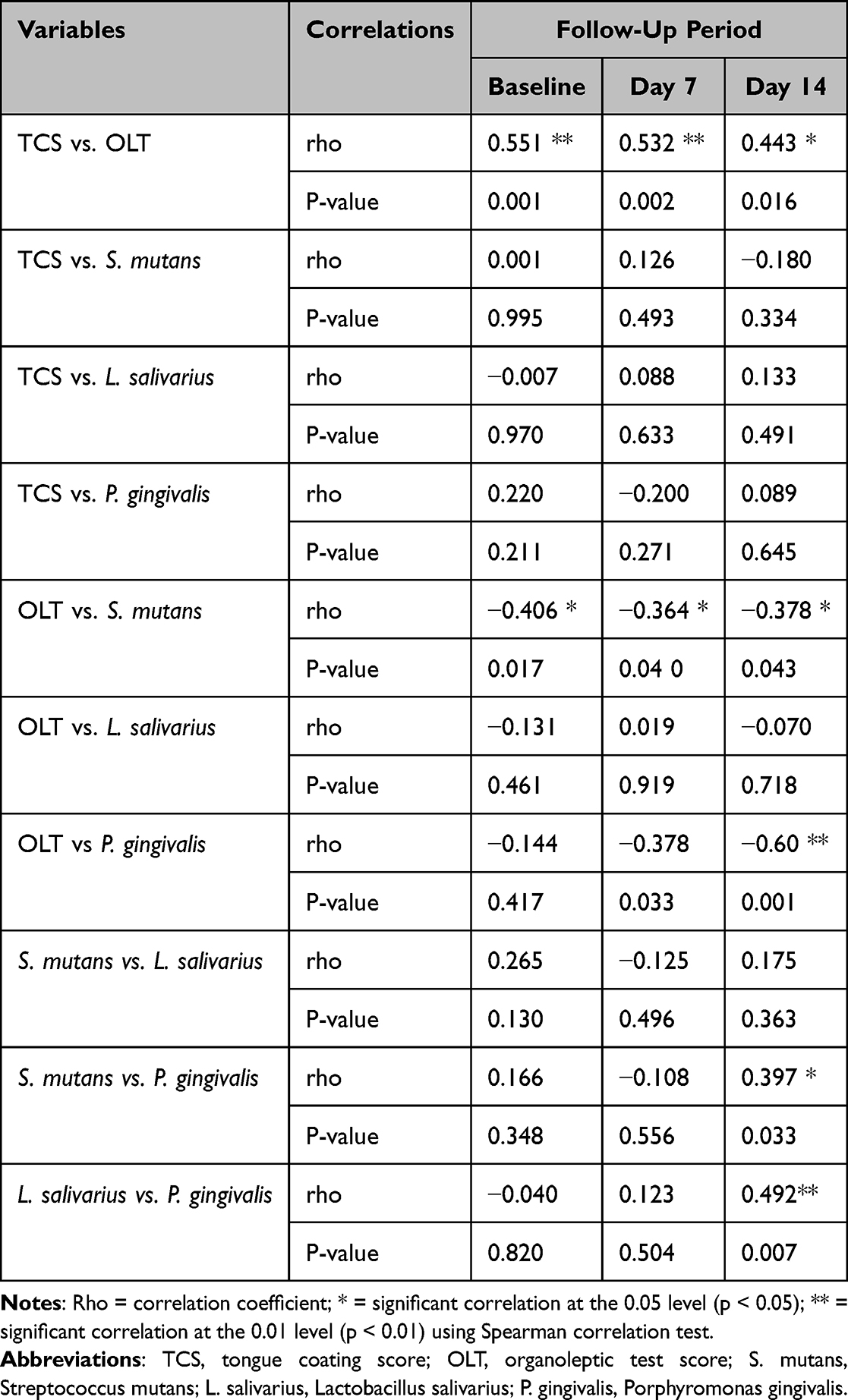 |
Table 5 Spearman’s Rho Correlations Between Clinical Parameters (TCS and OLT) and the Composite Bacterial CTS Index (Inverse of Bacterial Load) in Dental Students Following Probiotic Mouth Rinse |
The results of this study were further analyzed by linear regression analysis. The between tongue coating score (TCS) and organoleptic test (OLT) at different time points illustrated in Figure 4. At baseline, a positive correlation was observed (R2 = 0.264), indicating a modest but meaningful linear relationship between TCS and OLT. On day 7, the association remained positive (R2 = 0.231), showing that higher TCS values were related to higher OLT scores. By day 14, the correlation persisted but was weaker (R2 = 0.142), suggesting a gradual attenuation of the relationship over time.
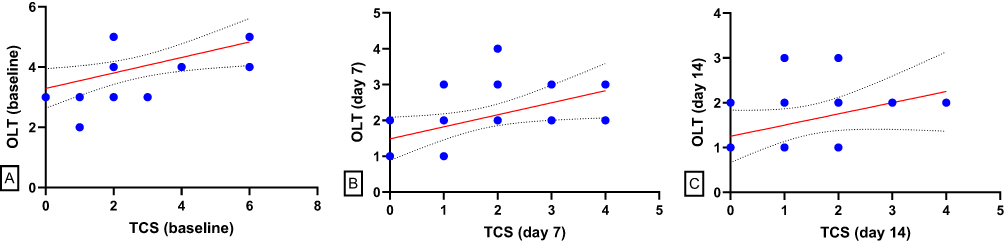 |
Figure 4 Linear regression analysis between tongue coating score (TCS) and organoleptic test (OLT) at different time points. (A–C) illustrate the linear regression relationships between tongue coating scores (TCS) and organoleptic test (OLT) values at baseline, day 7, and day 14, respectively. At baseline, a positive correlation was observed (R2 = 0.264), indicating a modest but meaningful linear relationship between TCS and OLT. On day 7, the association remained positive (R2 = 0.231), showing that higher TCS values were related to higher OLT scores. By day 14, the correlation persisted but was weaker (R2 = 0.142), suggesting a gradual attenuation of the relationship over time. Dotted lines represent the 95% confidence intervals of the regression line. |
The linear regression analysis between Streptococcus mutans cycle threshold (Ct) values and organoleptic test (OLT) scores at different time intervals are shown in Figure 5. At baseline (A), a modest negative correlation was observed (R2 = 0.115), which became stronger on day 7 (B; R2 = 0.238) and remained evident on day 14 (C; R2 = 0.172). The negative slopes indicate that higher Ct values—reflecting lower bacterial load—were associated with reduced organoleptic scores.
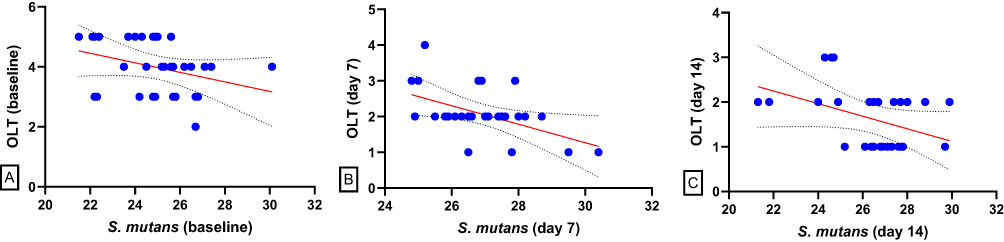 |
Figure 5 Linear regression analysis between Streptococcus mutans cycle threshold (Ct) values and organoleptic test (OLT) scores at baseline, day 7, and day 14. Scatter plots with fitted regression lines (A–C) illustrate the inverse associations between S. mutans Ct values and OLT scores across the study period. At baseline (A) a modest negative correlation was observed (R2 = 0.115), which became stronger on day 7 (B; R2 = 0.238) and remained evident on day 14 (C; R2 = 0.172). The negative slopes indicate that higher Ct values—reflecting lower bacterial load—were associated with reduced organoleptic scores. Dotted lines represent the 95% confidence intervals for the regression fits. |
Linear regression analysis between Porphyromonas gingivalis cycle threshold (Ct) values and organoleptic test (OLT) scores across different time intervals are demonstrated in Figure 6. Analyses demonstrated weak negative correlations (A: R2 = 0.085; B: R2 = 0.071), indicating that higher Ct values—reflecting lower bacterial abundance—were associated with slightly reduced OLT scores. However, the relationships were not statistically significant, suggesting that the reduction in P. gingivalis load contributed only marginally to changes in oral malodor.
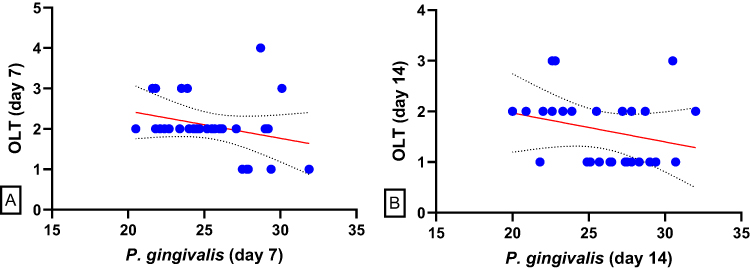 |
Figure 6 Linear regression analysis between Porphyromonas gingivalis cycle threshold (Ct) values and organoleptic test (OLT) scores at day 7 and day 14. (A and B) depict the relationship between P. gingivalis Ct values and OLT scores at day 7 and day 14, respectively. Both analyses demonstrated weak negative correlations (A) R2 = 0.085; (B) R2 = 0.071), indicating that higher Ct values—reflecting lower bacterial abundance—were associated with slightly reduced OLT scores. However, the relationships were not statistically significant, suggesting that the reduction in P. gingivalis load contributed only marginally to changes in oral malodor. Dotted lines represent the 95% confidence intervals of the regression lines. |
Further analysis by Linear regression was performed between Porphyromonas gingivalis cycle threshold (Ct) values and the othertwo oral bacterial species at day 14 (Figure 7). The data revealed positive correlations (A: R2 = 0.137; B: R2 = 0.205), suggesting that reductions or increases in P. gingivalis abundance were accompanied by similar trends in the other bacterial species. Although the associations were modest, these findings indicate potential interspecies interactions within the oral microbiota following probiotic mouth-rinse administration. More details are shown in Figures 4–7.
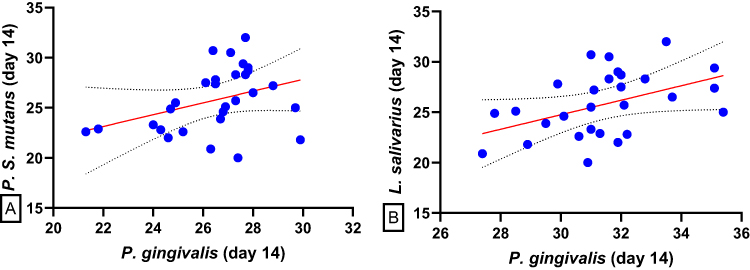 |
Figure 7 Linear regression analysis between Porphyromonas gingivalis cycle threshold (Ct) values and those of other oral bacterial species at day 14. (A and B) depict the relationships between P. gingivalis Ct values and those of Streptococcus mutans and Lactobacillus salivarius, respectively, at day 14. Both models revealed positive correlations (A) R2 = 0.137; (B) R2 = 0.205), suggesting that reductions or increases in P. gingivalis abundance were accompanied by similar trends in the other bacterial species. Although the associations were modest, these findings indicate potential interspecies interactions within the oral microbiota following probiotic mouth-rinse administration. Dotted lines represent the 95% confidence intervals of the regression lines. |
Discussions
Oral malodor or halitosis— is often exacerbated by poor oral hygiene and a high prevalence of caries. The observed improvements in tongue coating and organoleptic scores following probiotic mouth rinse use are associated with prior evidence supporting the role of probiotics in oral malodor management.
The sustained reduction in organoleptic scores observed in this study is consistent with multiple probiotic interventions targeting halitosis. For instance, Lactobacillus paracasei ET-22 was shown to significantly improve breath odor and modulate oral microbiome dysbiosis in a randomized trial involving 60 participants (Wuri et al, 2023).28 Similarly, Lactobacillus reuteri demonstrates antimicrobial activity against volatile sulfur compound (VSC)-producing bacteria such as Porphyromonas gingivalis and Fusobacterium nucleatum, as highlighted in a comprehensive review by Liu et al (2024).18 In contrast, Streptococcus salivarius K12 exerts its effects through bacteriocin production and colonization of the tongue dorsum, as evidenced by He et al (2020), who reported in a rigorously designed double-blind, placebo-controlled trial, significant reductions in VSC levels and improved organoleptic scores in a double-blind, placebo-controlled trial.24 These strain-specific mechanisms, ranging from competitive exclusion and immune modulation to direct antimicrobial action, collectively reinforce the therapeutic potential of probiotics in the management of halitosis and support the clinical outcomes observed in the present study.
Most notably, the organoleptic test (OLT) score—a direct clinical measure of halitosis severity by a clinician’s nose—suggested a robust and sustained reduction from baseline to day 14 (p < 0.001). This outcome reinforces the hypothesis that probiotic strains suppress malodor-producing bacteria and reduce VSC levels. A systematic review by Huang et al (2022) concluded that probiotic interventions significantly improved OLT scores and reduced halitosis in both short- and long-term trials. The rapid improvement observed by day 7 in the current study suggests early colonization and activity of the administered strains, which may be attributed to their oral cavity adaptability and antimicrobial properties.17 In addition, this rapid and sustained improvement mirrors the findings from a 2023 clinical trial by Samiraninezhad et al, where an L. reuteri-derived probiotic formulation significantly improved oral mucosal health and reduced inflammation in patients with recurrent aphthous stomatitis, indirectly supporting its role in microbial modulation and odor control.29
In the current study, quantitative PCR analysis revealed dynamic shifts in the oral microbiota following probiotic mouth rinse administration, with statistically significant increases in Ct values for Streptococcus mutans, Lactobacillus salivarius, and Porphyromonas gingivalis, indicating reduced bacterial DNA abundance. These findings might reflect the antimicrobial and ecological modulation capabilities of Lactobacillus reuteri and Lactobacillus paracasei, which are consistent with previous research.However, because these mechanisms were not directly investigated in the present study, the findings should be interpreted cautiously. Importantly, the observed reduction in L. salivarius should not be interpreted as a generalized suppression of beneficial oral microbiota, as the administered probiotic strains were Lactobacillus reuteri and Lactobacillus paracasei, rather than L. salivarius.
Although clinically meaningful reductions in OLT and tongue coating scores were observed, the magnitude of microbiological Ct shifts was comparatively modest. Therefore, the observed clinical improvements may partially reflect additional non-microbiological influences, including placebo responses, examiner expectancy, behavioral modification, Hawthorne effects, or regression to the mean within the context of a single-arm exploratory design.
Iwamoto et al (2010) conducted an open-label pilot trial to evaluate Lactobacillus salivarius WB21 in individuals with halitosis. The study reported significant improvements in breath odor and reductions in tongue coating, alongside enhanced salivary flow and oral hygiene indices. Although L. salivarius showed a decline in abundance in this study, this may reflect strain-specific dynamics or competitive interactions between L. reuteri and L. paracasei. Nonetheless, the clinical improvements observed in both studies underscore the broad potential of Lactobacillus strains in managing halitosis through microbiota modulation and biofilm disruption.22
The reduction in S. mutans is particularly noteworthy given its role in dental caries and biofilm formation, especially in young individuals, such as dental students. The greater reduction observed in S. mutans compared with P. gingivalis may suggest that the intervention exerted broader ecological modulation effects beyond exclusively halitosis-associated anaerobic pathways. A crossover randomized trial by Gedam and Katre (2022) suggested that probiotic mouth rinses significantly reduced S. mutans counts in children aged 8–12 years with an efficacy comparable to that of chlorhexidine and sodium fluoride.30 Similarly, Park et al (2025) confirmed the antibacterial activity of probiotic strains against S. mutans, Aggregatibacter actinomycetemcomitans, and P. gingivalis, supporting the broad-spectrum potential of probiotics in oral pathogen suppression.31
Although the current study did not focus on Candida albicans, the randomized trial by Mishra et al (2023) provided valuable insights into the antimicrobial efficacy of probiotic oral rinses in pediatric populations. This study demonstrated that probiotic formulations significantly reduced the fungal load and improved oral hygiene markers. These findings support the broader antimicrobial potential of probiotic rinses and reinforce the outcomes of the present study regarding bacterial suppression and clinical improvement. Moreover, the pediatric context aligns with our young adult cohort, suggesting an age-related responsiveness to probiotic interventions.
Despite its probiotic classification, the observed decline in L. salivarius may reflect competitive niche displacement or strain-specific interactions. Importantly, the reduction observed in L. salivarius should not be interpreted as evidence of generalized suppression of beneficial lactobacilli, as L. salivarius was evaluated as a resident oral commensal species rather than as one of the administered probiotic strains. Arnal et al (2021) reported that oral galenic formulations of L. salivarius can modulate the microbiota composition depending on the delivery form and strain survival, emphasizing the complexity of probiotic-host interactions.32
The modest yet significant reduction in P. gingivalis DNA abundance aligns with the findings of Kamianowski et al (2025), who conducted a systematic review of the inhibitory effects of Lactobacillus strains against P. gingivalis, a key pathogen in periodontal disease. Their review highlighted mechanisms such as bacteriocin production and immune modulation.33 Additionally, Bakri et al (2025) demonstrated that Lactobacillus helveticus exerted strong antibacterial effects against P. gingivalis in vitro, reinforcing the therapeutic potential of probiotics in periodontal health.34
The lack of significant changes between days 7 and 14 across all three species suggests that microbial suppression may plateau after initial colonization and competitive exclusion. The relative plateau observed between Day 7 and Day 14 may indicate stabilization of the initial response rather than progressive cumulative improvement. Although the absence of a control group prevents definitive interpretation of the underlying mechanism however, this stabilization phase is consistent with the colonization dynamics described by Lundtorp-Olsen et al (2024), who reviewed the temporal effects of probiotic supplements on oral microbiota and emphasized the importance of sustained dosing for long-term modulation.35
The consistent and statistically significant positive correlation between the tongue coating score (TCS) and organoleptic test (OLT) across all time points reinforced the established relationship between tongue biofilm accumulation and halitosis severity. This association has been well-documented in the literature. For instance, Popa et al (2025) conducted a cross-sectional study suggesting that an increased tongue coating burden is directly associated with elevated morning breath odor, particularly in individuals with reduced salivary flow.36 Similarly, Seerangaiyan et al (2018) emphasized that the tongue coating serves as a primary reservoir for anaerobic bacteria responsible for volatile sulfur compound (VSC) production, thereby exacerbating intraoral halitosis.37
The inverse correlation between OLT and Streptococcus mutans observed in this study is intriguing. Although S. mutans is traditionally associated with cariogenicity rather than malodor, emerging evidence suggests that its metabolic byproducts may contribute to oral dysbiosis. Kannan et al (2025) reviewed the systemic and oral implications of S. mutans, noting its role in biofilm maturation and acidogenic shifts, which may indirectly influence malodor.38 However, Ghapanchi et al (2015) found no direct association between S. mutans presence and halitosis, highlighting the complexity of microbial contributions to oral odor.39
In contrast, the significant negative correlation between OLT and Porphyromonas gingivalis on day 14 aligns with its well-established role in periodontal diseases and halitosis. Lee and Hong (2023) reviewed the dual contribution of P. gingivalis to periodontitis and oral malodor, emphasizing its proteolytic activity and VSC generation as key pathogenic mechanisms.3 Moreover, Yasukawa et al (2010) demonstrated that P. gingivalis colonization of subgingival and tongue plaques was significantly associated with halitosis severity in periodontally healthy adults.40
The absence of significant correlations between TCS and individual bacterial species suggests that tongue coating, although clinically relevant, may not directly reflect microbial abundance. This observation is associated with the findings of Lundtorp-Olsen et al (2024), who noted that probiotic interventions can alter the microbial composition without visibly affecting biofilm thickness.35
Finally, the inter-bacterial correlations observed on day 14, particularly between S. mutans and P. gingivalis and L. salivarius and P. gingivalis, suggest potential microbial synergy or co-aggregation during probiotic colonization. Gönczi et al (2021) explored such interactions and revealed that probiotic strains can influence pathogenic bacterial behavior through quorum sensing and competitive inhibition.41
Overall, the findings of this exploratory study are interesting, suggesting that that a multi-strain probiotic mouthrinse may be associated with short-term improvements in clinical indicators of halitosis. However, because the study lacked a control group and did not include randomization, blinding, volatile sulfur compound measurement, or broad microbiome profiling, these findings should be interpreted cautiously.
To the best of current knowledge, relatively few studies have evaluated a commercially available multi-strain probiotic mouthrinse in dental students using combined clinical halitosis assessment and targeted qPCR-based microbiological outcomes. By integrating the organoleptic scores, tongue-coating scores, and qPCR-based quantification of S. mutans, P. gingivalis, and L. salivarius, this study addresses a notable gap in the literature on halitosis. Although previous studies have primarily focused on clinical improvements, few have examined parallel microbial changes. The combined reduction in clinical symptoms and modulation of key oral bacteria observed here provide a valuable translational link between probiotic use and microbiological shifts in vivo. These findings support the feasibility of targeted probiotic mouth rinses as microbiome-compatible alternatives to conventional antiseptic agents and offer preliminary estimates to guide the design of future large-scale randomized controlled trials.
The current study has some limitations, as the design of the study employed a single-arm before–after design without a placebo or parallel control group therefore, causal relationships between the probiotic intervention and the observed outcomes cannot be definitively established. Second, although standardized conditions were applied, organoleptic assessment remains inherently subjective despite substantial intra-examiner reliability. The absence of objective volatile VSC measurements, limited direct biochemical assessment of oral malodor and may reduce comparability with future VSC-centered studies and meta-analyses.Third, the intervention period was limited to 14 days, and the long-term effects on oral microbiota stability and halitosis recurrence could not be assessed. Fourth, qPCR targeted selected bacterial species and did not include full microbial profiling; thus, broader community shifts may not have been observed. Fifth, the relatively small sample size (n = 34) limits the statistical generalizability of the findings Finally, the cohort consisted of dental students, which may not interpret to a wider population. Therefore, the findings should be interpreted as preliminary study, needing further investigations.
Conclusion
Short term use the probiotic mouth rinse containing Lactobacillus reuteri and Lactobacillus paracasei was associated with measurable clinical improvements in halitosis-related clinical indicators, including reductions in organoleptic scores and tongue coating levels. The qPCR findings further indicated that these clinical benefits were accompanied by shifts in the oral microbiota, including a progressive decline in Streptococcus mutans and Lactobacillus salivarius abundance and modest suppression of Porphyromonas gingivalis. The strong positive correlation between the tongue coating score and organoleptic test severity throughout the follow-up period reinforces the central role of tongue biofilms in halitosis. These preliminary findings support further investigation through well-designed randomized, placebo-controlled studies with longer follow-up periods and objective volatile sulfur compound measurements to better clarify the clinical role of probiotic-based mouthrinse in halitosis management.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the College of Dentistry, University of Sulaimani (Approval No. 204/23; November 2, 2023). The study was registered with the ISRCTN UK registry under the reference number ISRCTN10448956.
Data Sharing Statement
The data presented in this study are available upon reasonable request from the corresponding author. The data is not publicly available because of restrictions, such as information that could compromise the privacy of the research participants.
Informed Consent Statement
Informed consent was obtained from all participants involved in this study, and written informed consent was obtained from all participants(s) to publish this paper.
Acknowledgment
The author would like to thank all the participants who were helpful in collecting saliva samples.
Author Contributions
The author made a significant contribution to the work reported, including the conception, study design, execution, data acquisition, analysis and interpretation; took part in drafting, revising and critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors furthermore, the probiotic mouthrinse used in this study was independently purchased by the investigator. No financial support, product donation, or manufacturer involvement was received.
Disclosure
The author declares no conflicts of interest in this work.
References
1. Min K, Glowacki AJ, Bosma ML, et al. Quantitative analysis of the effects of essential oil mouthrinses on clinical plaque microbiome: a parallel-group, randomized trial. BMC Oral Health. 2024;24(1):578. doi:10.1186/s12903-024-04365-9
2. Li F, Wang C, Xu J, et al. Evaluation of the antibacterial activity of elsholtzia ciliate essential oil against halitosis-related fusobacterium nucleatum and porphyromonas gingivalis. Front Microbiol. 2023;14:1219004. doi:10.3389/fmicb.2023.1219004
3. Lee YH, Hong JY. Oral microbiome as a co-mediator of halitosis and periodontitis: a narrative review. Front Oral Health. 2023;4:1229145. doi:10.3389/froh.2023.1229145
4. Alazmi S. Prevalence and psychosocial impact of halitosis: a cross-sectional study. Int J Dent Sci Res. 2021;9(1):11–18. doi:10.12691/ijdsr-9-1-3
5. Heboyan A, Avetisyan A, Vardanyan A. Halitosis as an issue of social and psychological significance. J Res Med Dent Sci. 2019;7(4):33–40.
6. Briceag R, Caraiane A, Raftu G, et al. Emotional and social impact of halitosis on adolescents and young adults: a systematic review. Medicina. 2023;59(3):564. doi:10.3390/medicina59030564
7. Nazir MA, Almas K, Majeed MI. The prevalence of halitosis (oral malodor) and associated factors among dental students and interns, lahore, Pakistan. Eur J Dent. 2017;11(04):480–485.
8. Zardawi FM, Khursheed DA, Zorab SS. Self-perceived oral malodorous among sulaimani dental students. Biomed Pharmacol J. 2018;11(3):1675–1680. doi:10.13005/bpj/1536
9. Noori A. Oral health behaviours, knowledge and attitudes among dental college students in sulaimani city, Iraq. Sulaimani Dent J. 2021;8(1):8–16. doi:10.17656/sdj.10125
10. Santos V, Maquera-Huacho PM, Imbriani MJM, Minhaco V, Spolidorio DMP. Effects of bluem(r) against streptococcus mutans biofilm and its virulence gene expression. Braz Dent J. 2023;34(1):19–28. doi:10.1590/0103-6440202305133
11. Mishra V, Shettar L, Bajaj M, Math AS. Comparison of a commercially available herbal and 0.2% chlorhexidine mouthrinse for prevention of oral malodor: a clinical trial. J Int Soc Prev Community Dent. 2016;6(1):S6–S11. doi:10.4103/2231-0762.181160
12. Takenaka S, Sotozono M, Ohkura N, Noiri Y. Evidence on the use of mouthwash for the control of supragingival biofilm and its potential adverse effects. Antibiotics. 2022;11(6):727. doi:10.3390/antibiotics11060727
13. Li Z, Li J, Fu R, Liu J, Wen X, Zhang L. Halitosis: etiology, prevention, and the role of microbiota. Clin Oral Investig. 2023;27(11):6383–6393. doi:10.1007/s00784-023-05292-9
14. Hampelska K, Jaworska MM, Babalska ZL, Karpinski TM. The role of oral microbiota in intra-oral halitosis. J Clin Med. 2020;9(8):2484. doi:10.3390/jcm9082484
15. Foo LH, Balan P, Pang LM, Laine ML, Seneviratne CJ. Role of the oral microbiome, metabolic pathways, and novel diagnostic tools in intra-oral halitosis: a comprehensive update. Crit Rev Microbiol. 2021;47(3):359–375. doi:10.1080/1040841X.2021.1888867
16. Passadakis G, Neophytou C, Davidopoulou S, Papadimitriou K. Effectiveness of probiotics in managing oral halitosis: a systematic review of randomized controlled trials. J Int Soc Prev Community Dent. 2025;15(4):301–312. doi:10.4103/jispcd.jispcd_19_25
17. Huang N, Li J, Qiao X, et al. Efficacy of probiotics in the management of halitosis: a systematic review and meta-analysis. BMJ Open. 2022;12(12):e060753. doi:10.1136/bmjopen-2022-060753
18. Liu Z, Cao Q, Wang W, et al. The impact of lactobacillus reuteri on oral and systemic health: a comprehensive review of recent research. Microorganisms. 2024;13(1):45. doi:10.3390/microorganisms13010045
19. Wang ZD, Zhang W, Liang TX. Advancements in oral delivery systems for probiotics based on polysaccharides. Polymers. 2025;17(2):144. doi:10.3390/polym17020144
20. Beattie RE. Probiotics for oral health: a critical evaluation of bacterial strains. Front Microbiol. 2024;15:1430810. doi:10.3389/fmicb.2024.1430810
21. Murata T, Yamaga T, Iida T, Miyazaki H, Yaegaki K. Classification and examination of halitosis. Int Dent J. 2002;52(S5P1):181–186. doi:10.1002/j.1875-595X.2002.tb00921.x
22. Iwamoto T, Suzuki N, Tanabe K, Takeshita T, Hirofuji T. Effects of probiotic lactobacillus salivarius wb21 on halitosis and oral health: an open-label pilot trial. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110(2):201–208. doi:10.1016/j.tripleo.2010.03.032
23. Rosenberg M, Mcculloch CA. Measurement of oral malodor: current methods and future prospects. J Periodontol. 1992;63(9):776–782. doi:10.1902/jop.1992.63.9.776
24. He L, Yang H, Chen zouyang X. The effect of streptococcus salivarius k12 on halitosis: a double-blind, randomized, placebo-controlled trial. Probiotics Antimicrob Proteins. 2020;12(4):1321–1329. doi:10.1007/s12602-020-09646-7
25. Byun R, Nadkarni MA, Chhour KL, Martin FE, Jacques NA, Hunter N. Quantitative analysis of diverse lactobacillus species present in advanced dental caries. J Clin Microbiol. 2004;42(7):3128–3136. doi:10.1128/JCM.42.7.3128-3136.2004
26. Yoshida Y, Suzuki N, Nakano Y, Shibuya K, Ogawa Y, Koga T. Distribution of actinobacillus actinomycetemcomitans serotypes and porphyromonas gingivalis in japanese adults. Oral Microbiol Immunol. 2003;18(3):135–139. doi:10.1034/j.1399-302x.2003.00034.x
27. Oho T, Yamashita Y, Shimazaki Y, Kushiyama M, Koga T. Simple and rapid detection of streptococcus mutans and streptococcus sobrinus in human saliva by polymerase chain reaction. Oral Microbiol Immunol. 2000;15(4):258–262. doi:10.1034/j.1399-302x.2000.150408.x
28. Wuri G, Liu F, Sun Z, et al. Lactobacillus paracasei et-22 and derived postbiotics reduce halitosis and modulate oral microbiome dysregulation - a randomized, double-blind placebo-controlled clinical trial. Food Funct. 2023;14(16):7335–7346. doi:10.1039/d3fo02271d
29. Samiraninezhad N, Kazemi H, Rezaee M, Gholami A. Effect of lactobacillus reuteri-derived probiotic nano-formulation on recurrent aphthous stomatitis: a double-blinded randomized clinical trial. BMC Oral Health. 2023;23(1):1019. doi:10.1186/s12903-023-03756-8
30. Gedam KY, Katre AN. Efficacy of probiotic, chlorhexidine, and sodium fluoride mouthrinses on mutans streptococci in 8- to 12-year-old children: a crossover randomized trial. Lifestyle Genom. 2022;15(1):35–44. doi:10.1159/000519916
31. Park J-Y, Lee JY, Kim Y, Kim B-K, Kim BK, Choi S-I. Biosafety characteristics and antibacterial activity of probiotic strains against streptococcus mutans, aggregatibacter actinomycetemcomitans, and porphyromonas gingivalis. Ann Microbiol. 2025;75(1):2. doi:10.1186/s13213-024-01790-7
32. Arnal ME, Denis S, Uriot O, et al. Impact of oral galenic formulations of lactobacillus salivarius on probiotic survival and interactions with microbiota in human in vitro gut models. Benef Microbes. 2021;12(4):75–90. doi:10.3920/BM2020.0187
33. Kamianowski C, Kamianowski A, Nikitiuk J, et al. The effect of probiotic lactobacillus strains on porphyromonas gingivalis, the etiological factor of periodontal diseases-a systematic review. Probiotics Antimicrob Proteins. 2025:1–39. doi:10.1007/s12602-025-10607-1
34. Bakri HH, Syed Abdul Rahman SN, Abd Halim AA, et al. In vitro study of probiotic lactobacillus helveticus: antibacterial effects on porphyromonas gingivalis. PLoS One. 2025;20(8):e0329497. doi:10.1371/journal.pone.0329497
35. Lundtorp-Olsen C, Markvart M, Twetman S, Belstrom D. Effect of probiotic supplements on the oral microbiota-a narrative review. Pathogens. 2024;13(5):419. doi:10.3390/pathogens13050419
36. Popa M, Dinu S, Luca MM, Bumbu BA, Talpos S. Salivary flow, tongue-coating burden, and morning breath odor: a cross-sectional study. J Clin Med. 2025;14(17):6072. doi:10.3390/jcm14176072
37. Seerangaiyan K, Juch F, Winkel EG. Tongue coating: its characteristics and role in intra-oral halitosis and general health-a review. J Breath Res. 2018;12(3):034001. doi:10.1088/1752-7163/aaa3a1
38. Kannan S, Balakrishnan J, Ramachandran N, Nair V, Vijayakumar K. Streptococcus mutans - the life on human teeth –an extensive review on molecular mechanisms and consequences for systemic health. Microbes Infect Dis. 2024. doi:10.21608/mid.2024.266348.1781
39. Ghapanchi J, Kamali F, Jalaly Z, et al. Lack of association between halitosis and the presence of streptococcus mutans in saliva. Br J Med Med Res. 2015;10(3):1–7. doi:10.9734/bjmmr/2015/19571
40. Yasukawa T, Ohmori M, Sato S. The relationship between physiologic halitosis and periodontopathic bacteria of the tongue and gingival sulcus. Odontology. 2010;98(1):44–51. doi:10.1007/s10266-009-0110-7
41. Gönczi NN, Strang O, Bagi Z, Rákhely GKovács KL. Interactions between probiotic and oral pathogenic strains. Biologia Futura. 2021;72(4):461–471. doi:10.1007/s42977-021-00088-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.