Back to Journals » International Journal of Women's Health » Volume 17
Clinical and Management Challenges of Gestational Trophoblastic Neoplasia Involving the Cervix: A Case Report
Authors Homenta C, Harsono AB, Mawardinata P ![]() , Kharisma Sinaga FI
, Kharisma Sinaga FI ![]() , Andrianto Susilo S
, Andrianto Susilo S ![]() , Dwi Putra MG
, Dwi Putra MG ![]()
Received 15 May 2025
Accepted for publication 2 November 2025
Published 7 November 2025 Volume 2025:17 Pages 4281—4289
DOI https://doi.org/10.2147/IJWH.S540566
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Christian Homenta,1 Ali Budi Harsono,1 Phindo Mawardinata,1 Ferry Iskandar Kharisma Sinaga,1 Sulaeman Andrianto Susilo,1 Muhammad Gilang Dwi Putra2
1Department of Obstetrics and Gynecology, Faculty of Medicine, Padjadjaran University, Dr. Hasan Sadikin General Hospital, Bandung, Indonesia; 2Clinical Research Unit, Department of Child Health, Faculty of Medicine, Padjadjaran University, Dr. Hasan Sadikin General Hospital, Bandung, Indonesia
Correspondence: Christian Homenta, Department of Obstetrics and Gynecology, Faculty of Medicine, Padjadjaran University, Dr. Hasan Sadikin General Hospital, Bandung, Indonesia, Email [email protected]
Abstract: Gestational Trophoblastic Neoplasia (GTN) involving the cervix is an uncommon and potentially life-threatening condition that poses significant diagnostic and therapeutic challenges. Early recognition and risk-adapted management are essential to achieve optimal outcomes. We report a 36-year-old woman with a prior history of molar pregnancy who presented with abnormal vaginal bleeding and systemic symptoms suggestive of malignancy. Laboratory evaluation revealed markedly elevated serum β-hCG levels, and imaging demonstrated a hypervascular cervical mass. The diagnosis of GTN involving the cervix was established based on clinical, radiologic, and biochemical findings. The patient was managed with EMA-CO chemotherapy (etoposide, methotrexate, actinomycin D, cyclophosphamide, and vincristine) as per high-risk GTN protocol. She tolerated the regimen well with only mild adverse effects. Serial β-hCG monitoring demonstrated a consistent decline, and complete remission was achieved after 10 cycles of EMA-CO followed by 2 consolidation cycles. Follow-up imaging confirmed the absence of residual or recurrent disease. This case underscores the effectiveness of EMA-CO chemotherapy in achieving complete remission in high-risk GTN involving the cervix. It highlights the importance of early diagnosis, multidisciplinary coordination, and rigorous post-molar surveillance in improving outcomes for patients with this rare presentation.
Keywords: gestational trophoblastic neoplasia, cervical GTN, EMA-CO chemotherapy, β-hCG, post-molar surveillance, high-risk GTN
Introduction
Gestational Trophoblastic Disease (GTD) represents a spectrum of disorders characterized by abnormal trophoblastic proliferation, ranging from benign forms such as hydatidiform mole to malignant variants known as Gestational Trophoblastic Neoplasia (GTN). A hydatidiform mole results from abnormal fertilization and may be complete (absence of fetal tissue) or partial (presence of abnormal fetal development). GTN encompasses invasive mole, choriocarcinoma, epithelioid trophoblastic tumor, and placental site trophoblastic tumor, all of which possess malignant potential and the ability to metastasize to distant organs. Early diagnosis and appropriate treatment are crucial in preventing disease progression and reducing morbidity.1
GTN involving the cervix, possibly representing a choriocarcinomatous component, is an uncommon and highly aggressive manifestation of the disease. It is characterized by rapid trophoblastic proliferation, marked vascular invasion, and extensive hemorrhage and necrosis.2 This condition most commonly follows a molar pregnancy but can also develop after term gestation, abortion, or ectopic pregnancy, necessitating vigilance after all pregnancy outcomes.3 Cervical involvement in GTN is extremely rare and may present with life-threatening vaginal bleeding. Although its aggressive nature allows for early hematogenous spread to organs such as the lungs, liver, and brain, advances in chemotherapeutic regimens have markedly improved survival outcomes.4,5
In Indonesia, the availability of standard multi-agent chemotherapy, such as the EMA-CO regimen, remains variable. Tertiary hospitals in metropolitan centers like Jakarta, Surabaya, and Yogyakarta have greater access to these regimens compared with rural healthcare facilities. Hence, prompt referral to centers experienced in GTN management is essential to ensure optimal outcomes.5,6
Management of GTN is guided by the International Federation of Gynecology and Obstetrics (FIGO) staging system and the modified World Health Organization (WHO) prognostic scoring system, which facilitate accurate risk stratification.6 These systems differentiate low-risk and high-risk GTN, directing appropriate therapy, single-agent chemotherapy for low-risk cases and multi-agent regimens for high-risk disease.
For high-risk GTN, defined as FIGO stage I–III with a WHO score ≥7 or stage IV, the standard of care is multi-agent chemotherapy due to the disease’s aggressive course and high metastatic potential.7 Among available regimens, EMA-CO, comprising etoposide, methotrexate, actinomycin D, cyclophosphamide, and vincristine, has become the globally accepted first-line treatment, offering excellent remission rates with manageable toxicity.5 The introduction of this regimen has markedly improved survival, transforming high-risk GTN into a highly curable malignancy.
Patients with low-risk GTN (FIGO stage I–III, WHO score <7) typically achieve complete remission with single-agent chemotherapy. In contrast, those with high-risk disease have a 70–80% remission rate following initial therapy, and an additional 10–15% can be successfully treated with further chemotherapy or surgical intervention.1 Despite favorable outcomes, challenges remain in optimizing treatment duration, managing drug resistance, and addressing long-term consequences such as fertility preservation and chemotherapy-induced toxicity.8,9
This case report presents a 36-year-old woman diagnosed with FIGO stage II and a high WHO prognostic score, representing high-risk GTN involving the cervix. The report describes her clinical course, diagnostic evaluation, and successful management using the EMA-CO regimen. It also highlights the challenges of treating GTN in resource-limited settings, emphasizing the importance of multidisciplinary coordination, early diagnosis, and adherence to follow-up to ensure favorable outcomes.
Case Presentation
A 36-year-old woman, G4P2A2, presented to the emergency department with vaginal bleeding and lower abdominal pain that had persisted for four hours. The bleeding was bright red, soaking through two sanitary pads, without clots, and accompanied by cramping pain. She denied nausea, vomiting, or changes in bowel or bladder habits. The patient reported an 8-kg weight loss over the past year, accompanied by decreased appetite.
Her obstetric history revealed a molar pregnancy in December 2022, treated with uterine curettage at another hospital. She did not undergo routine serum β-hCG monitoring or follow-up visits afterward. Despite this, she reported regular menstrual cycles until June 2023. From July to October 2023, she experienced intermittent brown spotting between cycles, which progressed to more frequent reddish spotting by November 2023, prompting medical evaluation. Given her history of molar pregnancy and systemic symptoms, recurrence of Gestational Trophoblastic Disease (GTD) or development of Gestational Trophoblastic Neoplasia (GTN) was suspected.
In December 2023, a second curettage was performed due to persistent bleeding, with histopathology revealing chronic non-specific endometritis. In January 2024, she re-presented to the emergency department with worsening vaginal bleeding, and a friable cervical mass was identified on examination. Her obstetric history included two term vaginal deliveries, one spontaneous abortion managed by curettage in June 2021, and one molar pregnancy in December 2022.
On physical examination, the patient was hemodynamically stable, with a blood pressure of 102/68 mmHg, a pulse rate of 109 beats/min, a respiratory rate of 20 breaths/min, and a temperature of 36.5°C. She was pale, with a hemoglobin level of 6.6 g/dL, consistent with severe anemia. Abdominal examination was unremarkable. On speculum examination, an exophytic mass protruding from the external cervical os was observed, suggestive of cervical infiltration, confirmed by bimanual palpation (Figure 1). The uterus was normal in size and consistency, and no adnexal masses were palpable.
 |
Figure 1 Speculum examination revealed an exophytic mass protruding from the external cervical os with apparent cervical infiltration. |
Laboratory tests showed leukocytosis (19,650/μL) and thrombocytosis (492,000/μL). The quantitative β-hCG level was markedly elevated at 181,735.9 mIU/mL (January 30, 2024). Chest X-ray showed no evidence of pulmonary metastasis.
Transvaginal ultrasonography (February 5, 2024) revealed an anteverted uterus with inhomogeneous echotexture (10.36 × 5.01×4.19 cm) and marked vascularity on color Doppler (grade 4), without intrauterine gestational sac. MRI (Figure 2) demonstrated a well-defined, irregular mass measuring 4.27×3.15 × 2.78 cm, extending from the corpus to the cervix and originating from the posterior junctional zone. The lesion showed inhomogeneous isointense signal on T1WI, hypointense signal on T2WI, restricted diffusion on DWI, and heterogeneous enhancement post-contrast. Both adnexa were normal, with no pelvic free fluid or distant metastases. Additionally, the liver and kidneys were unremarkable on imaging, with no signs of metastasis or organ involvement.
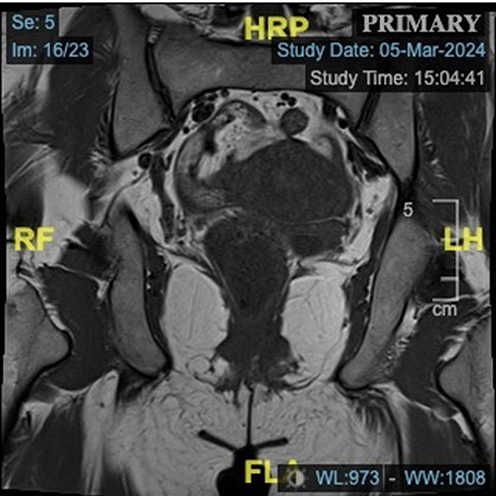 |
Figure 2 MRI examination revealed well-defined mass with irregular borders, approximately measuring 4.27×3.15 x 2.78 cm, located in the region extending from the corpus to the cervix uteri and appearing to originate from the posterior junctional zone. |
Histopathological examination of the cervical tissue demonstrated extensive necrosis and hemorrhage with sheets of large pleomorphic trophoblastic cells exhibiting hyperchromatic, bizarre nuclei and moderate cytoplasm, consistent with choriocarcinoma (Figure 3). However, in view of the pathologist’s recommendation for clinicopathologic correlation, the final diagnosis was determined as high-risk Gestational Trophoblastic Neoplasia (GTN) involving the cervix, supported by markedly elevated β-hCG levels and characteristic MRI findings.
 |
Figure 3 Histopathological picture of cervical biopsy consistent with choriocarcinoma of the cervix uteri. |
Based on the FIGO 2021 classification, the patient was diagnosed with Stage II Gestational Trophoblastic Neoplasia involving the cervix. Her WHO prognostic score was 10, indicating high-risk GTN, derived from an antecedent pregnancy interval >12 months (4 points), pretreatment β-hCG >100,000 mIU/mL (4 points), and largest tumor size ≥4 cm (2 points).
Initial management focused on stabilizing the patient with blood transfusions to correct anemia and intravenous tranexamic acid (500 mg three times daily) to control bleeding. The patient subsequently received multi-agent chemotherapy with the EMA-CO regimen, consisting of:
- Day 1: Etoposide 100 mg/m2 IV, Methotrexate 100 mg/m2 IV bolus followed by 200 mg/m2 infusion over 12 hours, and Actinomycin D 0.5 mg IV.
- Day 2: Etoposide 100 mg/m2 IV, Actinomycin D 0.5 mg IV, and Folinic acid 15 mg PO/IM every 12 hours for 4 doses starting 24 hours after Methotrexate.
- Day 8: Cyclophosphamide 600 mg/m2 IV and Vincristine 1 mg/m2 IV (maximum 2 mg).
The patient tolerated chemotherapy well, with only mild nausea and fatigue. Vaginal bleeding gradually subsided and ceased entirely after the first cycle. Serial β-hCG levels demonstrated a progressive decline: February 27, 2024: 11,911.2 mIU/mL → March 13, 2024: 557.7 → March 27, 2024: 103.1 → April 30, 2024: 16.1 → May 29, 2024: 9.0 → June 26, 2024: 5.8 → July 29, 2024: 4.1 mIU/mL.
The patient completed 10 cycles of EMA-CO followed by two consolidation cycles. Throughout treatment, she underwent regular β-hCG monitoring, clinical evaluations, and imaging studies to ensure sustained remission and detect recurrence (Figure 4). At the time of reporting, she remains in complete remission with stable β-hCG levels and no clinical or radiological evidence of disease.
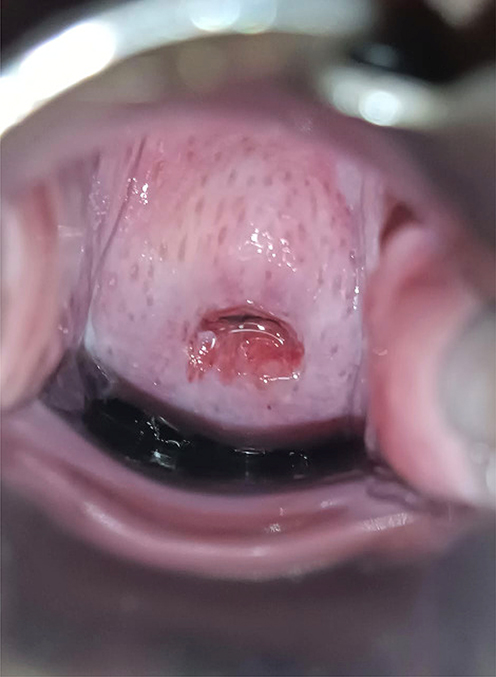 |
Figure 4 Speculum examination of post-EMA-CO therapy. |
Discussion
This case report illustrates the successful management of high-risk Gestational Trophoblastic Neoplasia (GTN) involving the cervix using the EMA-CO chemotherapy regimen, emphasizing its effectiveness in achieving complete remission. The patient was diagnosed with FIGO stage II GTN and classified as high-risk based on a WHO prognostic score of 10, necessitating aggressive multi-agent chemotherapy. Her initial presentation with vaginal bleeding and a history of molar pregnancy reflects a common pattern in GTN, highlighting the critical importance of vigilant post-molar follow-up. The absence of regular β-hCG monitoring after her molar pregnancy contributed to delayed diagnosis and disease progression, underscoring the need for structured surveillance programs and patient education. According to current guidelines, patients should undergo weekly β-hCG monitoring until three consecutive normal values are achieved, followed by monthly monitoring for 6–12 months to detect early signs of GTN.10
Failure to adhere to post-molar surveillance significantly increases the risk of delayed GTN detection. This case reinforces the importance of educating patients about the necessity of follow-up after molar evacuation and the implications of noncompliance on prognosis.
Markedly elevated β-hCG levels supported the diagnosis of GTN in this patient, imaging findings consistent with uterine and cervical involvement, and the absence of chorionic villi on histopathology. Transvaginal ultrasonography and pelvic MRI played pivotal roles in evaluating tumor location, vascularity, and treatment response.11,12 The absence of pulmonary metastasis on chest X-ray was a favorable prognostic factor, as lung involvement is commonly associated with worse outcomes.
Although histopathology demonstrated features consistent with choriocarcinoma of the cervix, the final diagnosis was established through multidisciplinary correlation, integrating β-hCG levels, imaging findings, and clinical presentation, in line with current GTN diagnostic guidelines. This integrative approach was essential in confirming the diagnosis and guiding appropriate risk-adapted management.
The decision to initiate the EMA-CO regimen was guided by the patient’s high-risk status according to the WHO prognostic score. EMA-CO, comprising etoposide, methotrexate, actinomycin D, cyclophosphamide, and vincristine, remains the gold standard for high-risk GTN due to its excellent remission rates and tolerable toxicity profile.6 Lydol et al (2022) reported complete remission rates of 80–90% even in patients with metastatic disease.13 In this case, the patient tolerated the regimen well, experienced minimal adverse effects, and demonstrated a steady decline in β-hCG levels until normalization, confirming treatment efficacy.
Cervical involvement in GTN is rare and poses diagnostic and therapeutic challenges due to the risk of severe hemorrhage and the difficulty of local control. The literature supports multi-agent chemotherapy as first-line therapy in such presentations, with surgery reserved for chemoresistant disease or uncontrollable bleeding.9,12,14,15 Table 1 summarizes key studies that have informed diagnostic and management strategies for high-risk GTN with cervical involvement.
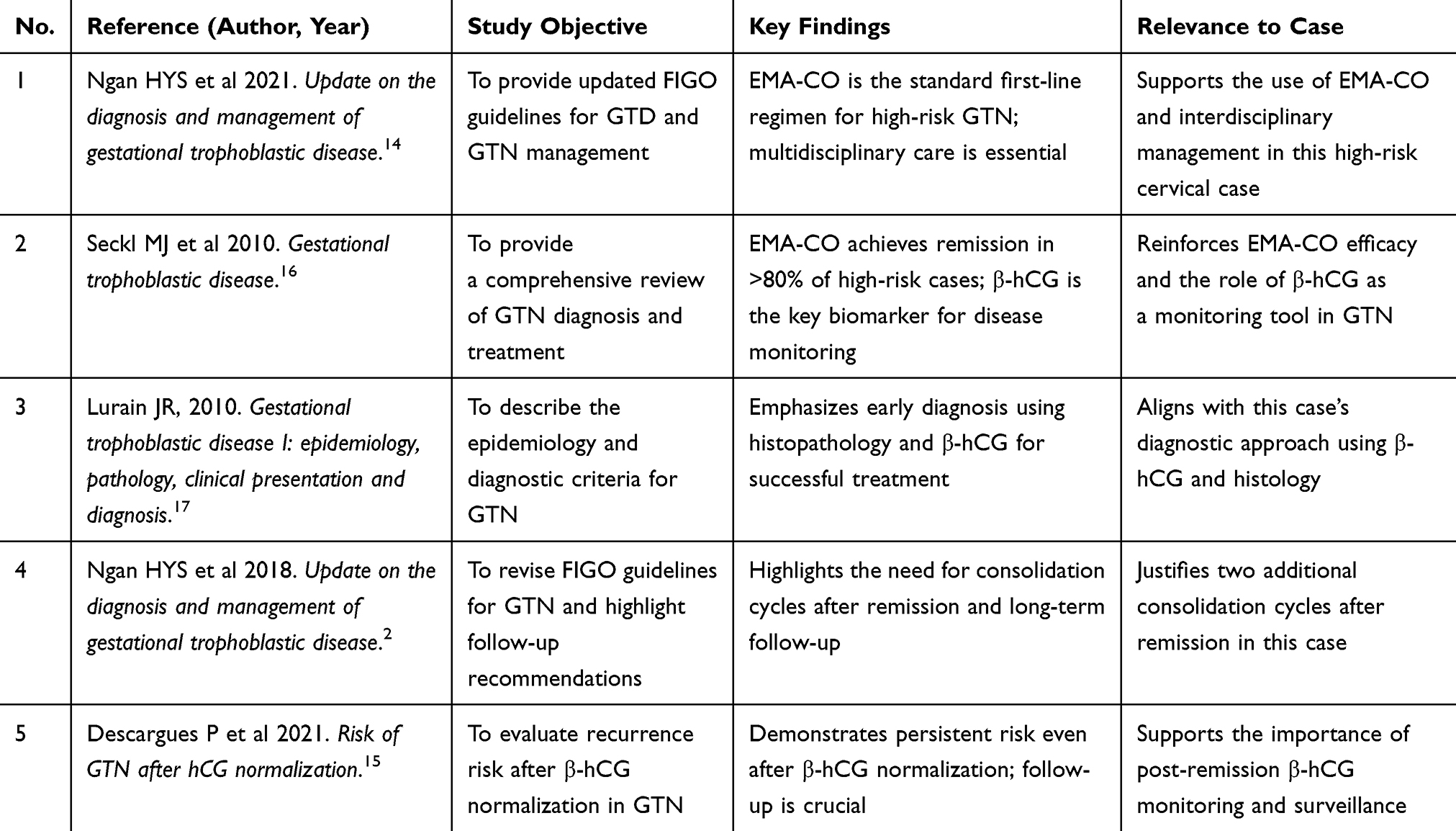 |
Table 1 Summary of Key Literature Supporting the Diagnosis and Management of High-Risk Cervical Gestational Choriocarcinoma |
The patient achieved β-hCG normalization (<5 mIU/mL) after five months of therapy. The decision to complete ten cycles of EMA-CO, followed by two consolidation cycles, aligns with current recommendations for high-risk GTN management. Consolidation therapy is crucial to reduce relapse risk, although the optimal number of cycles remains debated, with most experts recommending two to three cycles after β-hCG normalization.14,18 Most common adverse effects of EMA-CO include neutropenia, mucositis, alopecia, and peripheral neuropathy,19 but in this case, side effects were mild, likely due to close monitoring and appropriate supportive care.
Pelvic MRI was instrumental in monitoring treatment response, providing superior anatomical detail compared to ultrasound.20 Complete remission was achieved without surgical intervention, reflecting the efficacy of chemotherapy alone in suitable cases. However, hysterectomy remains an option in chemoresistant or recurrent disease, particularly in patients with no future fertility desire.21,22 In this case, conservative management preserved the patient’s fertility potential.
Long-term prognosis after remission from high-risk GTN treated with EMA-CO is excellent, with reported survival rates exceeding 85–94%.23 Nevertheless, relapse most often occurs within the first year, necessitating strict follow-up with serial β-hCG monitoring and periodic imaging.24
An important consideration in women of reproductive age is the potential impact of chemotherapy on fertility. Multi-agent regimens such as EMA-CO may cause transient amenorrhea or earlier menopause onset but rarely result in permanent ovarian failure.25 Most post-treatment pregnancies result in favorable outcomes, although patients remain at a slightly higher risk of recurrent molar pregnancy and adverse obstetric outcomes. This underscores the importance of preconception counseling and careful monitoring during subsequent pregnancies.
Finally, this case underscores the indispensable role of multidisciplinary collaboration among gynecologic oncologists, medical oncologists, radiologists, and pathologists. Coordinated care ensures accurate diagnosis, tailored treatment, and vigilant follow-up, ultimately optimizing patient outcomes. Such team-based management is particularly essential in high-risk GTN, where early intervention and individualized therapy significantly influence prognosis. Institutional Review Board approval was approved by Institutional Review Board of Hasan Sadikin Hospital, Bandung, Indonesia to publish the case details.
Conclusion
This case highlights the successful management of high-risk Gestational Trophoblastic Neoplasia (GTN) involving the cervix, achieving complete remission and normalization of β-hCG levels through EMA-CO multi-agent chemotherapy. The case underscores the effectiveness of prompt, risk-adapted chemotherapy and the essential role of post-molar surveillance in facilitating early detection and intervention, thereby preventing disease progression. The delay in initial diagnosis emphasizes the importance of consistent follow-up and awareness among clinicians. A comprehensive diagnostic approach integrating β-hCG measurement, imaging, and clinical assessment was crucial for accurate staging and treatment planning. Furthermore, this case illustrates the potential for fertility preservation through chemotherapy alone, avoiding the need for hysterectomy in responsive patients. Continuous β-hCG monitoring and imaging-guided decisions ensured early relapse detection and effective disease control. Multidisciplinary collaboration among gynecologic oncologists, medical oncologists, radiologists, and pathologists was pivotal in optimizing patient outcomes. While this case demonstrated a favorable prognosis, future research should focus on refining risk stratification, exploring targeted therapies, and reducing chemotherapy-related toxicities to further improve the management of high-risk GTN.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Institutional approval was granted by the Institutional Review Board of Hasan Sadikin Hospital, Bandung, Indonesia. Institutional approval was also required and obtained for the publication of the case details.
Data Sharing Statement
The data supporting the reported results are not publicly available due to privacy and ethical restrictions. However, they can be provided by the corresponding author upon reasonable request.
Informed Consent Statements
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper based on Declaration of Helsinki. Written informed consent was obtained from the patient for publication of the case details and accompanying images.
Acknowledgments
The authors would like to thank the medical and administrative staff of Hasan Sadikin Hospital for their support during the study. We also appreciate the technical assistance provided by the team and the valuable input from colleagues who contributed to the discussion and refinement of this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. duPont NC, Enserro D, Brady MF, et al. Prognostic significance of ethnicity and age in advanced stage epithelial ovarian cancer: an NRG oncology/gynecologic oncology group study. Gynecol Oncol. 2022;164(2):398–405. doi:10.1016/j.ygyno.2021.11.013
2. Ngan HYS, Seckl MJ, Berkowitz RS, et al. Update on the diagnosis and management of gestational trophoblastic disease. Int J Gynecol Obstet. 2018:143. doi:10.1002/ijgo.12615
3. Braga A, Burlá M, Freitas F, et al. Centralized coordination of decentralized assistance for patients with gestational trophoblastic disease in Brazil: a viable strategy for developing countries. J Reprod Med. 2016;61(3).
4. Eysbouts YK, Bulten J, Ottevanger PB, et al. Trends in incidence for gestational trophoblastic disease over the last 20 years in a population-based study. Gynecol Oncol. 2016;140(1). doi:10.1016/j.ygyno.2015.11.014
5. Brown J, Naumann RW, Seckl MJ, Schink J. 15 years of progress in gestational trophoblastic disease: scoring, standardization, and salvage. Gynecol Oncol. 2017;144(1):1–9. doi:10.1016/j.ygyno.2016.08.330
6. Agarwal R, Alifrangis C, Everard J, et al. Management and survival of patients with FIGO high-risk gestational trophoblastic neoplasia: the U.K. experience, 1995-2010. J Reprod Med. 2014;59(1–2).
7. Lawrie TA, Alazzam M, Tidy J, Hancock BW, Osborne R. First-line chemotherapy in low-risk gestational trophoblastic neoplasia. Cochrane Database Syst Rev. 2016;2016(6):1–9. doi:10.1002/14651858.CD007102.pub4
8. Mangili G, Lorusso D, Brown J, et al. Trophoblastic disease review for diagnosis and management a joint report from the international society for the study of trophoblastic disease, european organisation for the treatment of trophoblastic disease, and the gynecologic cancer intergroup. Int J Gynecol Cancer. 2014;24(9):1–10. doi:10.1097/IGC.0000000000000294
9. Seckl MJ, Sebire NJ, Fisher RA, Golfier F, Massuger L, Sessa C. Gestational trophoblastic disease: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(SUPPL.6). doi:10.1093/annonc/mdt345
10. Bolze PA, Attia J, Massardier J, et al. Formalised consensus of the European organisation for treatment of trophoblastic diseases on management of gestational trophoblastic diseases. Eur J Cancer. 2015;51(13). doi:10.1016/j.ejca.2015.05.026
11. Dhanda S, Ramani S, Thakur M. Gestational trophoblastic disease: a multimodality imaging approach with impact on diagnosis and management. Radiol Res Pract. 2014;2014. doi:10.1155/2014/842751
12. Wang W, Kong Y, Li Y, et al. Pulmonary resection of residual lesions of pulmonary metastasis from gestational trophoblastic neoplasia. Int J Gynecol Cancer. 2023;33(9). doi:10.1136/ijgc-2023-004375
13. Lybol C, Thomas CMG, Blanken EA, et al. Comparing cisplatin-based combination chemotherapy with EMA/CO chemotherapy for the treatment of high risk gestational trophoblastic neoplasia. Eur J Cancer. 2013;49(4). doi:10.1016/j.ejca.2012.09.015
14. Ngan HYS, Seckl MJ, Berkowitz RS, et al. Diagnosis and management of gestational trophoblastic disease: 2021 update. Int J Gynecol Obstet. 2021;155(S1). doi:10.1002/ijgo.13877
15. Descargues P, Hajri T, Massardier J, et al. Gestational trophoblastic neoplasia after human chorionic gonadotropin normalization in a retrospective cohort of 7761 patients in France. Am J Obstet Gynecol. 2021;225(4). doi:10.1016/j.ajog.2021.05.006
16. Seckl MJ, Sebire NJ, Berkowitz RS. Gestational trophoblastic disease. Lancet. 2010;376(9742):717–729. doi:10.1016/S0140-6736(10)60280-2
17. Lurain JR. Gestational trophoblastic disease I: epidemiology, pathology, clinical presentation and diagnosis of gestational trophoblastic disease, and management of hydatidiform mole. Am J Obstet Gynecol. 2010;203(6):1–10. doi:10.1016/j.ajog.2010.06.073
18. Deleuze A, Hajri T, Bolze PA, De La Motte Rouge T. 797P Impact of consolidation cycles in predicting recurrence in patients treated with EMA-CO for high-risk gestational trophoblastic neoplasia. Ann Oncol. 2023;34. doi:10.1016/j.annonc.2023.09.1975
19. Mangili G, Sabetta G, Cioffi R, et al. Current evidence on immunotherapy for gestational trophoblastic neoplasia (GTN). Cancers. 2022;14(11). doi:10.3390/cancers14112782
20. Lima LD, Parente RCM, Maestá I, et al. Clinical and radiological correlations in patients with gestational trophoblastic disease. Radiol Bras. 2016;49(4):1–10. doi:10.1590/0100-3984.2015.0073
21. Dhand S, Thakur M, Kerkar R, Jagmohan P. Diffusion-weighted imaging of gynecologic tumors: diagnostic pearls and potential pitfalls. Radiographics. 2014;34(5). doi:10.1148/rg.345130131
22. Eoh KJ, Chung YS, Yim GW, et al. Role of surgical therapy in the management of gestational trophoblastic neoplasia. Obstet Gynecol Sci. 2015;58(4). doi:10.5468/ogs.2015.58.4.277
23. Xie Y, Kong W, Zhao X, Zhang H, Luo D, Chen S. Immune checkpoint inhibitors in cervical cancer: current status and research progress. Front Oncol. 2022;12(1):1–12. doi:10.3389/fonc.2022.984896
24. Braga A, Maestá I, Short D, Savage P, Harvey R, Seckl MJ. Hormonal contraceptive use before hCG remission does not increase the risk of gestational trophoblastic neoplasia following complete hydatidiform mole: a historical database review. BJOG an Int J Obstet Gynaecol. 2016;123(8). doi:10.1111/1471-0528.13617
25. Joneborg U, Coopmans L, Van Trommel N, Seckl M, Lok CAR. Fertility and pregnancy outcome in gestational trophoblastic disease. Int J Gynecol Cancer. 2021;31(3):399–411. doi:10.1136/ijgc-2020-001784
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Choriocarcinoma Histologically Mimicking Epithelioid Trophoblastic Tumor – A Diagnostic Pitfall in Gestational Trophoblastic Neoplasia
Harsono AB, Nisa AS, Susilo AFP, Kurniawan RA, Winarno GNA
International Journal of Women's Health 2026, 18:601343
Published Date: 16 May 2026