Back to Journals » International Journal of Women's Health » Volume 18
Choriocarcinoma Histologically Mimicking Epithelioid Trophoblastic Tumor – A Diagnostic Pitfall in Gestational Trophoblastic Neoplasia
Authors Harsono AB, Nisa AS ![]() , Susilo AFP
, Susilo AFP ![]() , Kurniawan RA, Winarno GNA
, Kurniawan RA, Winarno GNA ![]()
Received 4 February 2026
Accepted for publication 1 May 2026
Published 16 May 2026 Volume 2026:18 601343
DOI https://doi.org/10.2147/IJWH.S601343
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Ali Budi Harsono, Aisyah Shofiatun Nisa, Artha Falentin Putri Susilo, Rommy Andika Kurniawan, Gatot Nyarumenteng Adhipurnawan Winarno
Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin General Hospital, Bandung, Indonesia
Correspondence: Ali Budi Harsono, Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran –Dr. Hasan Sadikin Hospital, Jl. Pasteur 38, Bandung, West Java, 40161, Indonesia, Email [email protected]
Background: Histopathological diagnosis can be challenging because epithelioid trophoblastic tumor (ETT) may closely mimic choriocarcinoma, particularly due to overlapping cytologic and architectural features of intermediate trophoblasts. Therefore, immunohistochemical studies are essential for accurate classification of GTN subtypes.
Case Illustration: A 27-year-old woman, para 4 abortion 1, with a history of two curettage procedures for partial hydatidiform mole, presented with persistent post-curettage vaginal bleeding for five months and was admitted to the emergency department with severe anemia. Serial β-hCG monitoring demonstrated a significant rise, raising suspicion for GTN. Ultrasonography revealed a vesicular pattern, while additional investigations showed no evidence of metastasis. Based on a FIGO score < 7, the patient was classified as low-risk GTN. The patient declined chemotherapy and opted for total hysterectomy with bilateral salpingectomy. Intraoperative gross examination revealed an irregular, friable, and necrotic uterine mass consistent with GTN. Initial histopathological evaluation suggested epithelioid trophoblastic tumor; however, further immunohistochemical analysis demonstrated negative p63 expression, high Ki-67 index, and positive β-hCG staining, findings more consistent with choriocarcinoma.
Discussion: This case highlights the importance of post-molar β-hCG surveillance as a cornerstone for early GTN diagnosis. The biological differences between ETT and choriocarcinoma have significant therapeutic implications, given the poorer chemotherapy response observed in ETT. Overlapping histopathological features emphasizes that diagnosis cannot rely solely on morphology but requires integration of clinical data, disease latency, β-hCG levels, and an appropriate immunohistochemical panel, particularly p63.
Conclusion: Delayed post-molar β-hCG monitoring may lead to GTN progression and increased morbidity. Immunohistochemical examination plays a crucial role in differentiating ETT from choriocarcinoma to ensure accurate diagnosis and appropriate management.
Keywords: gestational trophoblastic neoplasia, epithelioid trophoblastic tumor, choriocarcinoma, partial hydatidiform mole, β-hCG, immunohistochemistry
Introduction
Gestational trophoblastic neoplasia (GTN) comprises a group of malignant disorders arising from abnormal proliferation of trophoblastic tissue following pregnancy, including invasive mole, choriocarcinoma, placental site trophoblastic tumor (PSTT), and epithelioid trophoblastic tumor (ETT).1 Approximately 50% of GTN cases develop after molar pregnancy, while the remaining cases occur following miscarriage, ectopic pregnancy, or term delivery. Hydatidiform mole, particularly complete mole, remains the most common antecedent pregnancy associated with GTN development.1,2
In Southeast Asia and Japan, approximately 9.2 per 40,000 pregnant women and 3.3 per 40 patients with hydatidiform mole are at risk of developing choriocarcinoma. The incidence of GTN following complete mole is reported to be 15–20%, whereas after partial mole it is considerably lower, ranging from 1–5%.1 The high incidence of GTN remains a significant challenge, as delayed diagnosis and management are associated with increased maternal morbidity and mortality.3,4
Epithelioid trophoblastic tumor (ETT) is the rarest subtype within the spectrum of GTN, accounting for only approximately 1–2% of all cases.5 ETT may arise following various types of pregnancy, including term delivery, abortion, ectopic pregnancy, or hydatidiform mole.5 The biological and clinicopathological characteristics of ETT differ substantially from those of choriocarcinoma. Histopathologically, ETT has a distinct cellular origin, making accurate diagnosis highly dependent on tissue evaluation and immunohistochemical staining.6 Histopathological diagnosis can be challenging because ETT may closely mimic choriocarcinoma, particularly due to overlapping cytologic and architectural features of intermediate trophoblasts.6 Therefore, immunohistochemical studies are essential for accurate classification of GTN subtypes.7 This case report highlights delayed GTN diagnosis contributing to significant morbidity due to massive bleeding, as well as the pathological presentation of choriocarcinoma mimicking epithelioid trophoblastic tumor following partial hydatidiform mole.
Case Illustration
A 27-year-old woman, para 4 abortion 1 (four living children; youngest aged 3 years), presented to the emergency department with a chief complaint of generalized weakness for three days prior to admission, accompanied by nausea and vomiting more than five times daily. She reported vaginal bleeding for ten days before admission, which had worsened over the last two days, soaking 4–5 sanitary pads per day and associated with blood clots, without passage of grape-like vesicular tissue. Additional symptoms included palpitations, heat intolerance, decreased appetite, and an unintentional weight loss of approximately 1 kg over the preceding two months. She denied abdominal pain, neck swelling, hemoptysis, severe headache, visual disturbances, or other symptoms suggestive of distant metastasis. There was no history of chronic illness or familial malignancy.
The patient had previously undergone two dilation and curettage procedures for hydatidiform mole, performed on June 12, 2025, and September 15, 2025, at another institution. Histopathological examination of the first curettage specimen revealed partial hydatidiform mole. Between the first and second procedures, the patient reported abstaining from sexual intercourse due to persistent vaginal bleeding. A second curettage was subsequently performed for suspected residual molar tissue, with histopathology again demonstrating residual partial hydatidiform mole. After the second procedure, the patient experienced cessation of bleeding for approximately one month, followed by recurrent vaginal bleeding, prompting referral for further evaluation. The patient was referred to our tertiary center. Serial quantitative β-hCG monitoring demonstrated a rising trend, raising suspicion for progression to gestational trophoblastic neoplasia (GTN) before she came to emergency department.
On physical examination, the patient was conscious but showed signs of hypoperfusion. Initial blood pressure was 96/72 mmHg, improving to 108/61 mmHg after administration of 500 mL crystalloid fluid. Heart rate decreased from 128 to 110 beats per minute. Respiratory rate was 20 breaths per minute, body temperature 36.7°C, and oxygen saturation 98% on room air. Clinical findings were consistent with grade I hypovolemic shock, including pale conjunctivae, prolonged capillary refill time (>2 seconds), decreased skin turgor, and cold extremities.
Gynecological examination revealed a flat abdomen with an enlarged uterus consistent with a 10–12-week gestation size. No adnexal masses were palpated, and no active bleeding was observed on speculum examination. Transvaginal ultrasonography demonstrated an anteflexed uterus with a vesicular pattern, normal adnexa, and no free fluid in the pelvis (Figure 1).
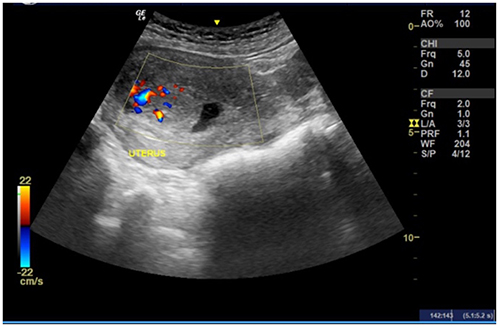 |
Figure 1 Ultrasonographic appearance showing a vesicular pattern. |
Laboratory investigations revealed severe anemia with a hemoglobin level of 5.5 g/dL, mild leukocytosis (12,180/µL), and a normal platelet count (362,000/µL). Serial β-hCG measurements showed a marked increase from 142,740 mIU/mL on November 7, 2025, to >225,000 mIU/mL on November 21, 2025, occurring at 8 and 10 weeks following the second curettage, respectively. On December 1, 2025, the β-hCG level was 162,751 mIU/mL. These markedly elevated and rising β-hCG levels were clinically more suggestive of particularly choriocarcinoma or invasive mole, rather than ETT.
Based on clinical findings, ultrasonographic features, and β-hCG trends, the patient was diagnosed with post-molar gestational trophoblastic neoplasia complicated by severe anemia and grade I hypovolemic shock due to vaginal bleeding. Initial management included hemodynamic stabilization with intravenous fluids, planned packed red cell transfusion targeting a hemoglobin level >10 g/dL, and adjunctive therapy with tranexamic acid, omeprazole, and ondansetron.
As part of further evaluation prior to definitive therapy, chest radiography and non-contrast cranial computed tomography were performed to assess for pulmonary or central nervous system involvement. Both imaging studies showed no evidence of metastasis. Following comprehensive evaluation, the patient was classified as having low-risk GTN (FIGO low-risk category) with a prognostic score ≤6. In accordance with FIGO guidelines, first-line therapy with single-agent chemotherapy (methotrexate or actinomycin-D) was recommended. The treatment plan, including potential side effects, high response rate (>98%), and the importance of strict β-hCG monitoring, was explained to the patient.
However, after thorough discussion with the medical team and family, the patient declined chemotherapy and opted for definitive surgical management, citing completion of childbearing, concerns regarding chemotherapy-related adverse effects, and the need for prolonged treatment. Despite her young age, the patient chose to undergo total hysterectomy with bilateral salpingectomy after receiving detailed counseling regarding permanent loss of fertility. The hysterectomy was performed due to recurrent vaginal bleeding and based on informed consent after explanation of risks, benefits, success rates, and alternative management options.
The patient underwent total hysterectomy with bilateral salpingectomy on December 25, 2025 (Figure 2A). Gross examination of the bisected uterus revealed a friable, irregular mass with hemorrhage and necrosis filling the uterine cavity and infiltrating the myometrium, consistent with malignant features (Figure 2B).
 |
Figure 2 (A) Uterus during surgery. (B) Bisected uterus showing an irregular hemorrhagic mass. |
Histopathological examination initially demonstrated epithelioid trophoblastic tumor (ETT) infiltrating up to one-half of the myometrial thickness, with evidence of lymphovascular invasion. Both fallopian tubes were free of tumor involvement. Postoperative β-hCG level measured on December 26, 2025, was 90,532 mIU/mL. Serial postoperative β-hCG monitoring was subsequently planned.
Microscopic examination revealed nests of intermediate trophoblastic cells with round morphology, hyperplasia, and compact clustering. The tumor cells exhibited pleomorphic, hyperchromatic nuclei (Figure 3). The clinical course of the disease is summarized in Figure 4. Because the histopathological impression was discordant with the aggressive clinical presentation and markedly elevated β-hCG levels, additional immunohistochemical studies were performed. Further immunohistochemical analysis demonstrated negative p63 staining, positive β-hCG, Ki-67 labeling index >80% of tumor cells, and positive cytokeratin expression, which, in combination with morphology and clinical findings, supported a diagnosis of choriocarcinoma rather than ETT (Figure 5).
 |
Figure 3 Microscopic histopathological features. |
 |
Figure 4 Timeline of the patient’s disease course. |
 |
Figure 5 Immunohistochemical staining results: (A) p63 negative; (B) Ki-67 showing strong nuclear positivity; (C) Cytokeratin positive on cell membranes; (D) β-hCG positive in the cytoplasm. |
Discussion
Gestational trophoblastic disease (GTD) is a spectrum of disorders that includes both premalignant and malignant forms.8 Molar pregnancies account for 80% of GTD cases and consist of complete and partial hydatidiform moles.8 Management of hydatidiform mole is generally performed through evacuation of the mass with dilation and curettage (D&C).9 Following evacuation, patients undergo serial β-hCG monitoring to detect early development of post-molar gestational trophoblastic neoplasia (GTN).9 The role of a second curettage in hydatidiform mole remains controversial.3 Some countries, such as Japan, Vietnam, and Hong Kong, routinely perform a second curettage approximately seven days after the first evacuation, whereas in other countries, it is performed selectively if residual molar tissue is suspected on ultrasonography.3
In a retrospective cohort study involving 173 patients treated between 2002 and 2019, the incidence of GTN was reported to be 15.2% in patients who underwent routine second curettage, compared to 20.6% in those who underwent elective curettage (p > 0.05).3 These results indicate that routine second curettage does not significantly reduce the incidence of post-molar GTN, and the clinical benefit of this procedure requires further evaluation.3 In this case, the patient underwent a second curettage approximately 12 weeks after the first without β-hCG monitoring, preventing calculation of the FIGO/WHO score and optimal risk classification. Lack of β-hCG monitoring can delay GTN diagnosis and the initiation of appropriate management, despite post-molar pregnancies having the highest incidence of GTN.
After the second curettage, the patient continued to experience persistent vaginal bleeding and was subsequently referred to a tertiary referral center, Dr. Hasan Sadikin General Hospital. During the subsequent evaluation, β-hCG measurement was performed as part of diagnostic assessment and determination of further management strategy. Serial β-hCG monitoring is recognized as the standard examination for diagnosing post-molar GTN, as this hormone directly reflects the proliferative activity of trophoblastic cells.1 According to the National Comprehensive Cancer Network (NCCN) and FIGO Gynecologic Oncology Committee, the diagnosis of post-molar GTN is based on serial β-hCG changes or histopathological findings of choriocarcinoma. The FIGO criteria, first established in 2000 and updated in 2021, state that post-molar GTN can be diagnosed if there is a plateau in β-hCG levels over four measurements spanning three or more weeks (days 1, 7, 14, 21), an increase of >10% in three consecutive weekly measurements over at least two weeks (days 1, 7, 14), persistence of β-hCG for more than six months after mole evacuation, histologic diagnosis of choriocarcinoma, or evidence of metastasis.1,2 Therefore, GTN can generally be diagnosed biochemically via β-hCG surveillance, even before clinical symptoms or metastases appear.
Management strategy for GTN is determined using a risk scoring system based on FIGO, which includes age, type of prior pregnancy, pregnancy interval, initial β-hCG level, largest tumor size, number and location of metastases, and history of chemotherapy failure. Patients with a score ≤6 are classified as low risk and generally respond very well to single-agent chemotherapy, such as methotrexate or actinomycin-D. In contrast, patients with a score ≥7 are considered high-risk and require multi-agent combination chemotherapy from the outset. In this patient, the FIGO score was 5, corresponding to low-risk GTN, which generally has a good prognosis with high cure rates using single-agent chemotherapy.
Serial β-hCG monitoring in this patient showed a pattern that objectively met the FIGO and NCCN criteria for GTN diagnosis. β-hCG levels increased significantly from 142,740 mIU/mL (07/11/2025) to >225,000 mIU/mL (21/11/2025), indicating a repeated rise inconsistent with the physiological post-evacuation decline, thus meeting the defined criteria for β-hCG increase according to both guidelines. These markedly elevated and rising β-hCG levels were also clinically more suggestive of choriocarcinoma or invasive mole than of ETT.
However, there was a delay in diagnosing GTN because serial β-hCG monitoring was not performed optimally following the first curettage. According to post-evacuation standards, routine β-hCG surveillance is intended to detect early failure of regression or recurrence of elevated levels, signaling transformation into GTN. Had monitoring been conducted rigorously from the beginning, the diagnosis could have been established earlier, allowing timely treatment. The delay resulted in GTN diagnosis approximately six months after the first curettage, at which point the disease had progressed, causing massive vaginal bleeding and severe anemia. This highlights a major clinical complication of untreated GTN and emphasizes the importance of adherence to serial β-hCG monitoring in preventing severe morbidity post-mole.
An alternative treatment for low-risk GTN is hysterectomy with salpingectomy, which may be considered in patients who no longer desire fertility or in cases of uncontrolled uterine bleeding, as in this case. This procedure can reduce intrauterine tumor burden and lower the risk of acute hemorrhage. Nevertheless, hysterectomy does not eliminate the possibility of residual disease or metastasis, so serial β-hCG monitoring remains mandatory post-procedure. If β-hCG does not normalize or rises again, systemic chemotherapy is still required to achieve biochemical remission and prevent disease progression. In this patient, both ovaries were preserved.
Therapeutic response in GTN is generally excellent, as trophoblastic cells are highly sensitive to cytotoxic chemotherapy, both in non-metastatic and metastatic disease.1 Cure rates for GTN with pulmonary metastases exceed 90% when treatment is administered according to FIGO risk stratification.10 Prognosis is significantly worse with brain or liver metastases, which are associated with higher mortality.11
Thus, serial β-hCG monitoring is an essential component in GTN management to ensure complete remission and detect recurrence early.1 International guidelines recommend weekly β-hCG measurement until normalization, followed by monthly monitoring for at least 12 months post-remission.12 Hormonal contraception is advised during this period, as new pregnancies may increase β-hCG levels, complicate interpretation of remission status, and potentially delay detection of GTN recurrence.
This case underscores the importance of structured and continuous post-mole monitoring. Limited patient education and failure to conduct serial β-hCG assessments contributed to delayed diagnosis, allowing disease progression with clinical complications and necessitating more aggressive therapy. Therefore, β-hCG interpretation should consider serial patterns and clinical correlation, including awareness of possible assay artifacts such as hook effect or phantom hCG. Risk stratification using the FIGO score is critical for determining appropriate management and preventing avoidable morbidity and mortality in GTN patients.
Histopathological examination of the uterus revealed epithelioid trophoblastic tumor (ETT). First identified in 1998 and recognized by the World Health Organization in 2003 as a distinct form of GTN, ETT, along with placental site trophoblastic tumor (PSTT), represents the rarest types of GTN.13 Both originate from intermediate trophoblasts, showing biological, clinical, and morphological differences compared to choriocarcinoma.13 Histologically, PSTT generally shows extensive myometrial infiltration with relatively low pleomorphism, whereas ETT has a more epithelioid appearance and may mimic squamous carcinoma.13 These differences directly impact diagnostic approach and management. Clinical manifestations of PSTT and ETT are often non-specific, leading to delayed diagnosis, and may appear months to years after a prior pregnancy.13 Diagnosis requires a combination of clinical, radiological, and histopathological assessments.13
Characteristic biology of ETT shows a slow latent disease course, ranging from approximately 1 to 40 years.5 ETT typically demonstrates relatively low β-hCG compared to other GTN. In a systematic review, 50 of 147 patients had β-hCG <100 mIU/mL, while only 36 had levels >1000 mIU/mL.5 In this case, the patient had a history of hydatidiform mole followed by development of an initial pathological impression of ETT within six months. This unusually short interval is inconsistent with typical ETT biology, which usually shows a slow latent period. Moreover, the markedly elevated β-hCG level and hemorrhagic presentation were atypical for pure ETT. Immunohistochemical staining suggested choriocarcinoma.
In pathological examination, neoplastic cells may resemble other tumor types, especially when the cells are poorly differentiated or show non-specific growth patterns.6 ETT can histologically resemble choriocarcinoma because both originate from the trophoblastic lineage; intermediate trophoblast components in ETT can mimic trophoblast cells in choriocarcinoma morphometrically and architecturally.14 This may complicate histopathological classification, particularly if evaluation relies solely on morphology. Accurate differentiation is clinically important because intermediate trophoblastic tumors respond poorly to chemotherapy compared to choriocarcinoma. Therefore, NCCN recommends immunohistochemistry to distinguish between GTN types.12 The comparison of IHC findings in PSTT, ETT, and choriocarcinoma was summarized in Table 1.12 The key learning point in this case was the discordance between routine histology suggesting ETT and the clinical presentation strongly favoring choriocarcinoma, prompting further ancillary testing.
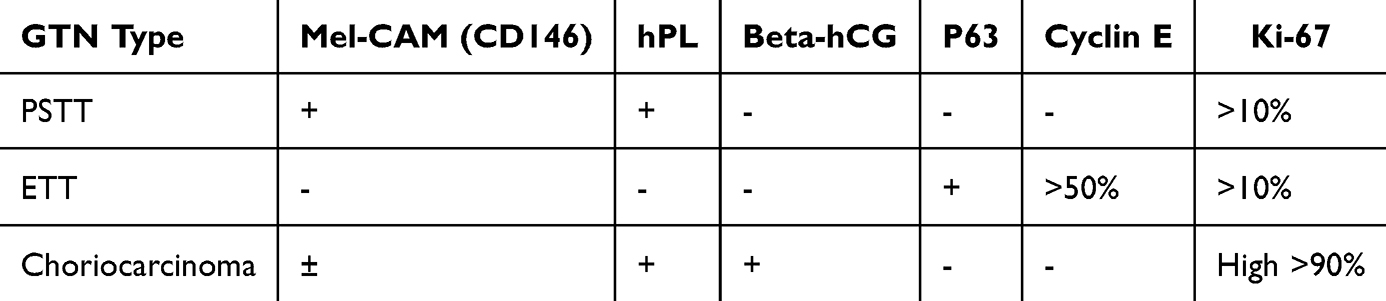 |
Table 1 Comparison of IHC Findings in PSTT, ETT, and Choriocarcinoma |
In this patient, immunohistochemistry showed negative p63, which significantly opposes an ETT diagnosis. Biologically, ETT originates from chorionic-type intermediate trophoblast, which consistently expresses p63 as a marker of epithelioid differentiation and chorionic trophoblastic proliferation. p63 is positive in most ETT cases and is a key marker to differentiate ETT from PSTT or choriocarcinoma. However, p63 should be interpreted as part of a broader immunohistochemical panel together with β-hCG, Ki-67, morphology, and clinical context. Lack of p63 expression in this case indicates that tumor proliferation did not reflect the chorionic intermediate trophoblast phenotype, making ETT an unlikely diagnosis.14,15 Thus, integrating clinical history, disease latency, β-hCG levels, histopathology, and immunohistochemical profile is crucial for accurate diagnosis of trophoblastic neoplasia, as misclassification affects not only pathological interpretation but also therapy strategy and patient prognosis.
Conclusion
This case illustrates the complexity of diagnosing GTN, particularly when post-molar β-hCG surveillance is not performed adequately, leading to delayed diagnosis and preventable complications. The unique aspect of this case was the discordance between the aggressive clinical presentation, strongly suggestive of choriocarcinoma, and the initial histopathological impression of ETT. ETT differs from choriocarcinoma in biological behavior and treatment response. Histopathological overlap may occur, making immunohistochemical analysis essential for accurate diagnosis. Misclassification may lead to inappropriate management and delayed therapy. This case highlights the importance of integrating clinical findings, β-hCG trends, morphology, and immunohistochemistry when pathology is inconsistent with the clinical patient.
Institutional Approval
Institutional approval was not required for the publication of this single-patient case report, in accordance with institutional policies and the ethical standards of the Declaration of Helsinki.
Informed Consent Patient Statement
The authors confirm that written informed consent was obtained from the patient. The patient was informed about the details of the case and provided approval for the publication of the case report, including any accompanying images. All identifying information has been appropriately anonymized to ensure patient confidentiality.
Acknowledgement
This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/ B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ngan HYS, Seckl MJ, Berkowitz RS, et al. Diagnosis and management of gestational trophoblastic disease: 2025 update. Int J Gynecol Obstet. 2025;171(S1):78–9. doi:10.1002/ijgo.70275
2. Lurain JR. Gestational trophoblastic disease I: epidemiology, pathology, clinical presentation and diagnosis of gestational trophoblastic disease, and management of hydatidiform mole. Am J Clin Exp Obstet Gynecol. 2010;203(6):531–539. doi:10.1016/j.ajog.2010.06.073
3. Yamamoto E, Nishino K, Niimi K, Ino K. Epidemiologic study on gestational trophoblastic diseases in Japan. J Gynecol Oncol. 2022;33(6):e72. doi:10.3802/jgo.2022.33.e72
4. Lok C, Frijstein M, van Trommel N. Clinical presentation and diagnosis of gestational trophoblastic disease. Best Pract Res Clin Obstet Gynaecol. 2021;74:42–52. doi:10.1016/j.bpobgyn.2020.12.001
5. Gorun F, Tomescu L, Motoc A, et al. Clinical features and management of trophoblastic epithelioid tumors: a systematic review. Medicine. 2022;101(30):e29934. doi:10.1097/MD.0000000000029934
6. Borch WR, Monaco SE. Current approach to undifferentiated neoplasms, with focus on new developments and novel immunohistochemical stains. Arch Pathol Lab Med. 2023;147(12):1364–1373. doi:10.5858/arpa.2022-0459-RA
7. Hacker NF. Hacker & Moore’s Essentials of Obstetrics and Gynecology: First South Asia Edition-E-Book. Elsevier Health Sciences; 2016.
8. Chawla T, Bouchard-Fortier G, Turashvili G, Osborne R, Hack K, Glanc P. Gestational trophoblastic disease: an update. Abdom Radiol. 2023;48(5):1793–1815. doi:10.1007/s00261-023-03820-5
9. Cue L, Farci F, Ghassemzadeh S, Kang M. Hydatidiform mole. In: StatPearls. StatPearls Publishing; 2024.
10. Seckl MJ, Sebire NJ, Berkowitz RS. Gestational trophoblastic disease. Lancet. 2010;376(9742):717–729. doi:10.1016/S0140-6736(10)60280-2
11. Lurain JR. Gestational trophoblastic disease II: classification and management of gestational trophoblastic neoplasia. Am J Clin Exp Obstet Gynecol. 2011;204(1):11–18. doi:10.1016/j.ajog.2010.06.072
12. National Comprehensive Cancer Network. NCCN guideline gestational trophoblastic neoplasia; 2025.
13. Hancock BW, Tidy J. Placental site trophoblastic tumour and epithelioid trophoblastic tumour. Best Pract Res Clin Obstet Gynaecol. 2021;74:131–148. doi:10.1016/j.bpobgyn.2020.10.004
14. Sung WJ, Shin HC, Kim MK, Kim MJ. Epithelioid trophoblastic tumor: clinicopathologic and immunohistochemical analysis of three cases. Korean J Pathol. 2013;47(1):67–73. doi:10.4132/KoreanJPathol.2013.47.1.67
15. McCarthy WA, Paquette C, Gundogan F, Lawrence WD. Comparison of p63 and p40 immunohistochemical stains to distinguish epithelioid trophoblastic tumor from other trophoblastic lesions. Int J Gynecol Pathol. 2018;37(4):401–404. doi:10.1097/PGP.0000000000000420
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical and Management Challenges of Gestational Trophoblastic Neoplasia Involving the Cervix: A Case Report
Homenta C, Harsono AB, Mawardinata P, Kharisma Sinaga FI, Andrianto Susilo S, Dwi Putra MG
International Journal of Women's Health 2025, 17:4281-4289
Published Date: 7 November 2025