")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 14
Clinical and Laboratory Characteristics of Elderly Patients with Pruritus
Authors Aboeldahab Snr S, Khalil Jnr F, Ezz Eldawla R
Received 5 June 2021
Accepted for publication 22 July 2021
Published 10 August 2021 Volume 2021:14 Pages 1009—1015
DOI https://doi.org/10.2147/CCID.S322527
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Soha Aboeldahab Snr,1 Fatma Khalil Jnr,2 Reham Ezz Eldawla1
1Dermatology and Venerology, Faculty of Medicine, Sohag University, Sohag, Egypt; 2Dermatology Department, Sohag General Hospital, Sohag, Egypt
Correspondence: Reham Ezz Eldawla
Dermatology and Venereology, Faculty of Medicine, Sohag University, Sohag, 82524, Egypt
Tel +201006809003
Email [email protected]
Introduction: For elderly, pruritus is considered the most common complaint in outpatient clinic. Pruritus occurs in association with primary skin disorders and can also be caused by many diseases and drugs. The aim of the work was to study clinical and laboratory characteristics of elderly patients with pruritus in Sohag, Egypt.
Patients and Methods: A cross-sectional study was conducted on 225 patients aged ≥ 60 years of both sexes complaining of pruritus and 160 age- and sex-matched patient group complaining of non-pruritic dermatological diseases. CBC, ESR, renal function tests, serology for HBV and HCV and blood glucose levels were done routinely in all patients (both groups). Skin biopsy was done in some selected cases.
Results: The mean duration of pruritus was 4.23 ± 4.9 months and was generalized in 73.8% of cases with moderate severity in 35.1% with winter exacerbation in 20%. Dermatological causes of pruritus were detected in 54.2%, followed by systemic causes in 29.8%. Eczema was the most common skin cause of senile itching in 33.7%, while renal diseases were the most common systemic cause in 46.2%.
Conclusion: Senile pruritus is a common problem in elderly. Early and proper management is mandatory to improve their quality of life.
Keywords: pruritus, elderly, depression, anxiety
Introduction
Aging is a progressive degenerative process that leads to a decrement in the function and the reserve capacity of the whole-body systems, including the skin system. It also represents the gradual change in various physiological, biological, physical and social functions in human beings. It is usually accepted to be multi-factorial process.1
With aging, elderly people become more liable to many dermatological conditions due to degenerative and metabolic changes happening throughout the skin layers.2 These changes can be divided into two categories: intrinsic aging or natural aging process of the skin and extrinsic aging, which is metabolic reaction to environmental assaults from solar radiation and other factors.3
One of the main features of the Egyptian population over the last few decades is the gradual increase in the number of older people. This is expected to continue in the next decades. The percentage of older people was 6.27% in 2006, rising to 6.9% in 2015 and about 9.2% in 2021. By 2050, it is expected to be 20.8% so the number of old people is expected to be 23.7 million.4
It is believed that the incidence of pruritus increases with age so it is more common in elderly than adults.5 Found that the prevalence of itching increases to be from 12.3% in adult people to 20.3% in elderly through a working population survey in Germany.
Pruritus in elderly has many causes, it can occur in association with primary skin disorders, eg (xerosis, atopic dermatitis, scabies) but also can be caused by systemic diseases such as cancer, chronic renal failure, cholestasis, hyperthyroidism, diabetes mellitus, iron deficiency anemia, some drugs intake like NSAIDs, when no abnormality can be found, it is considered as a normal consequence of skin aging process.6
Pruritus in elderly can be very distressing and socially disabling, resulting in serious impairment of elderly quality of life. They struggle to sleep at night. Identifying underlying cause of the itch is important, whenever possible.7
This study is designed to examine clinical and laboratory characteristics of elderly patients with pruritus in Sohag, Egypt.
Patients and Methods
A cross-sectional study was conducted on 225 patients aged ≥60 years of both sexes complaining of pruritus (group A) and 160 age- and sex-matched patients complaining of nonpruritic dermatological diseases (group B) who attended the Dermatology Outpatient Clinics at Sohag University Hospital in the period from October 2018 to September 2019. The authors assert that all procedures contributing to this work comply with the ethical standards of relevant national and institutional guidelines on human experimentation (Ethics of Research Committee, Sohag Faculty of Medicine, approval number was 12/2018), and with Helsinki declaration of 1975 as revised in 2008.
Written informed consent was obtained from all the participants in the study after explaining its steps.
All cases in this study were subjected to Medical history with emphasis on Medical history of pruritus: Onset, course, duration, site, diurnal, seasonal variation, and exacerbating and relieving factors, therapeutic historyː previous and recent history of drug intake for any systemic or any dermatological disease and history of chronic medical disease:
Any history suggestive of systemic disease such as (liver disease, renal disease, thyroid disease, DM).
Examination included: Full clinical examination: Complete general examination was done to exclude any systemic causes of pruritus. Dermatological examination: It was done to detect the exact site of pruritus, presence or absence of skin rash and character of specific skin lesions of certain dermatological diseases if present.
Assessment of Pruritus Intensity
It was done by using the verbal rating scale (VRS), which is a four-point scale and consists of a list of adjectives describing various levels of symptom intensity.8
- = no itch.
- = mild itch.
- = moderate itch.
- = severe itch.
Laboratory Investigations
The following investigations were done routinely in all patients (cases and controls):
- Complete blood count (Iron deficiency anemia was considered if hemoglobin level <12 g/dl).
- Erythrocytic sedimentation rate (ESR).
- Renal function test.
- Serology for hepatitis B and C.
- Fasting and post-prandial glucose level.
Other investigations were done according to primary patient evaluation such as:
- Serum ferritin level. - Liver function tests.
- Thyroid function test.
- Skin biopsy: 4mm punch skin biopsy was done in 18 patients with pruritus and 23 patients of non-pruritic group. According to the results of skin biopsy, mycosis fungoides was detected in (6 cases), dermatitis herpetiformis (5 cases), disseminated contact dermatitis (2 cases), psoriasis (2 cases), porokeratosis (1 case), chromoblastomycosis (1 case) and bullous pemphigoid (1 case).
Statistical Analysis
Statistical analysis was carried out using SPSS statistics software version 23. Qualitative variables were presented as frequencies and percentages and compared by using chi-square test. Quantitative variables were presented as means ± standard deviation (SD) and were compared by independent student t- test. The test was considered significant when P value <0.05.
Results
The mean (± SD) of age in group (A) was 65.1 ± 5.7 years while in group (B) was 65.37 ± 5.9 years. Males constituted 77.3% and 73.1% of both groups, respectively. Regarding the residence of patients, most of the cases were residents in rural areas (55.1% of group (A) and 61.3% of group (B)), as shown in Table 1, there was a statistically significant relation between residence and both groups (P value = 0.01). There was no statistically significant difference between both groups regarding smoking and its severity.
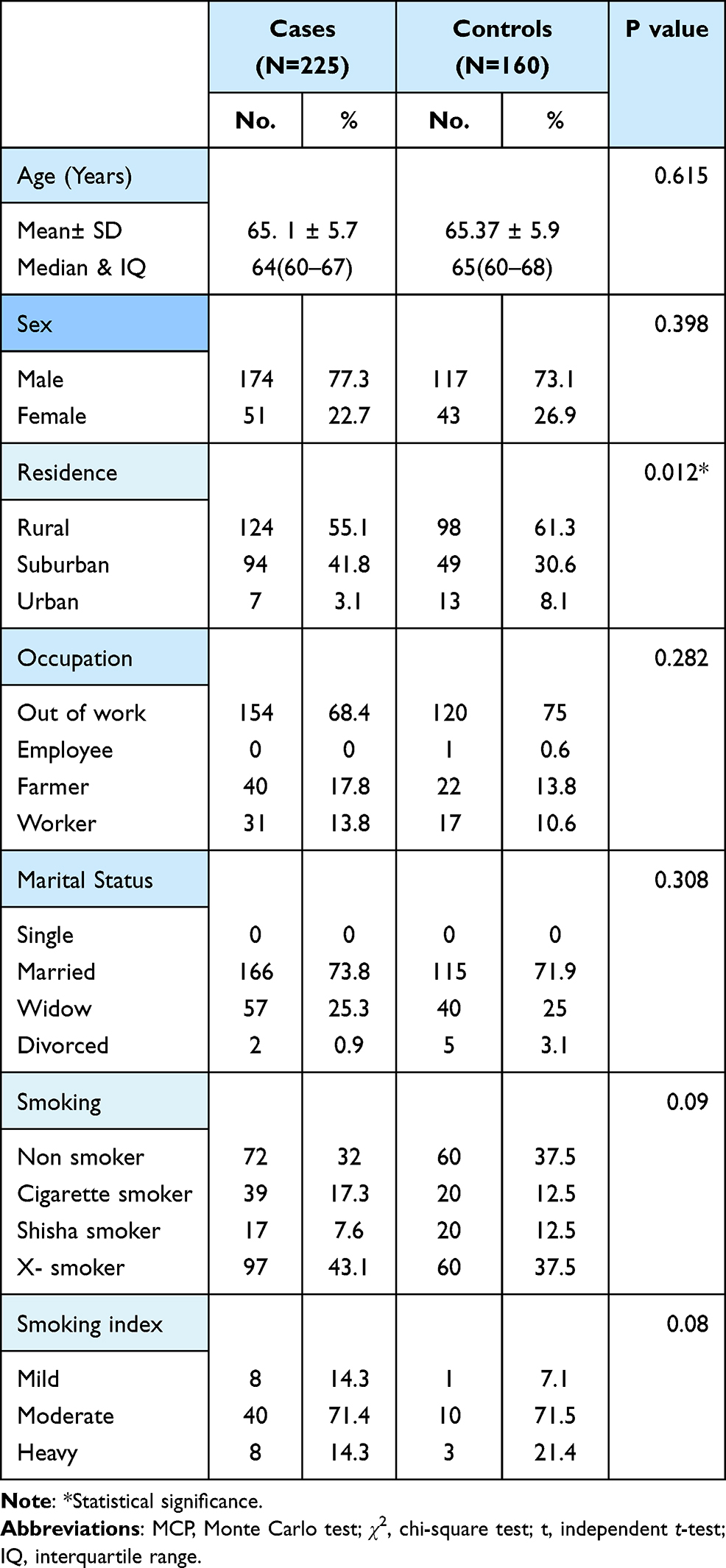 |
Table 1 Comparison Between Cases and Controls Regarding Sociodemographic Characteristics |
The current study showed that pruritus was of gradual onset in 93.3% of the patients and progressive course in 44.8%. The mean duration of pruritus was 4.23 ±4.9 months.
Pruritus was generalized in 73.8% of cases, the most common affected sites were upper, lower extremities and back, while anus and genitalia were the least reported sites by patients.
There was night exacerbation of itching in 20%; however, 55.2% of the cases did not report any diurnal variation. Regarding seasonal variation, winter exacerbation of itching was detected in 20% of the cases, followed by summer in 5.8%. Systemic antihistaminic drugs were an effective way to relieve itching in 22.2% of cases, while topical soothing creams were used in 8.9% of the cases.
There was a statistically significant difference between both groups as regard ESR as the mean (± SD) among cases was 31.6 ±20.52, while in controls was 14.6±6.6 (p-value = 0.0001). Also, there was a statistically significant difference between both groups as regard (creatinine and postprandial sugar level) as (p-value = 0.01 and 0.003, respectively). There was no statistically significant difference between both groups regarding (RBCs, Hb, WBCs, PLTs and FBS).
There was a statistically significant difference between both groups with regard to infection by HBV and HCV (P-value = 0.004). HCV infection was detected in 20.9% in group A and 9.4% in group B.
In the current study, the most common causes of pruritus were dermatological causes in
54.2%, followed by systemic causes in 29.8%, and lastly combined causes in 15.6%, Figure 1.
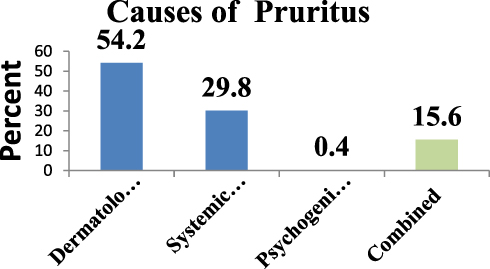 |
Figure 1 Causes of pruritus among cases. |
Regarding dermatological causes, eczema was the most common dermatological cause of senile pruritus in 33.7%, followed by xerosis 12.7%, then fungal infections and immunobullous diseases 11.4% for each.
Regarding systemic causes of senile pruritus, renal diseases were the most common in 46.2% of cases, 83% of these renal patients were previously known to have renal disease but 17% of the patients were firstly diagnosed at the time of examination. Hepatic cause of senile itching was detected in 34.3%, 62.8% of these hepatic patients were previously known to have liver disorders but 37.2% of these patients were firstly diagnosed at time of presentation. Diabetes mellitus was detected in 9% and 79.6% of these patients were previously known to be diabetic.
Pattern of dermatological disease among group (B) vitiligo was the most common skin disease among them in 17.5% of the patients followed by bacterial skin infections in 14.3%, as revealed in Table 2.
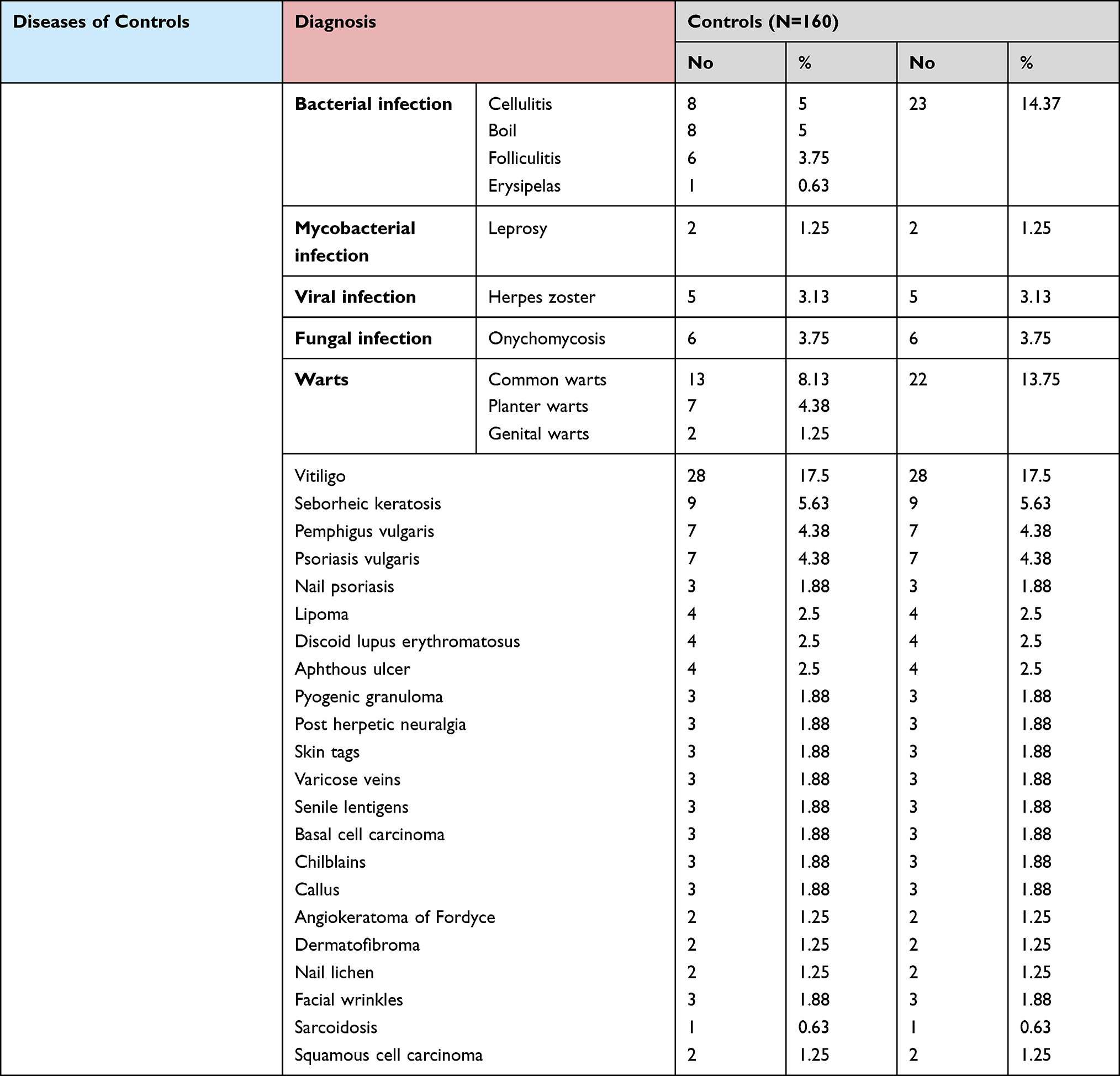 |
Table 2 Dermatological Diseases Among Control Group |
As regards VRS of itching, 133 out of 225 examined patients (59.1%) had moderate itching, 79 (35.1%), as shown in Figure 2.
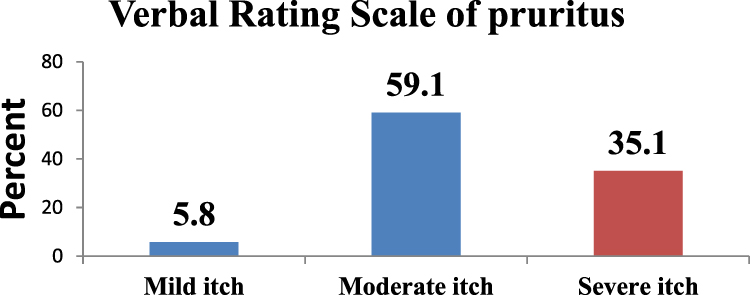 |
Figure 2 Verbal rating scale among cases. |
Discussion
Pruritus is the most common skin disorder in the geriatric population. In a Thai-study in elderly patients, pruritic diseases were the most common one (41%).9 Chronic pruritus refers to itching that has been present for six weeks or more, it is a very common and debilitating problem in geriatric population.10
According to a Turkish study, senile pruritus was reported in 11.5%, whereas the highest prevalence was in patients older than 85 years.11
In current study, the sex difference between two groups was statistically insignificant. Male constituted 77.3% of cases, which was not in agreement with Thaipisuttikul (1998) who found that itchy skin diseases in elderly were more common in females 58.4% than males.9
As regards residence in the present study, rural areas constituted 55.1% of cases and 61.3% of controls (MCP=0.012), our finding might be attributed to poor hygiene and lower health care, but El-Hamd et al found that 74.7% of the patients were residents in urban and suburban areas. Regarding occupation, 68.4% of cases and 75% of controls were out of work.12
In relation to marital status, 73.6% of cases and 75% of controls were married. There was no statistically significant difference regarding marital status as (MCP =0.308), which was in agreement with Thaipisuttikul (1998) who found that 58.4% of elderly patients with pruritus were married.9 But7 found that social relationships (with marital status as a proxy measure) may be protective of morbidity by aiding in economic well-being, healthier lifestyles, lower stress, and social support.7
In the current study, 71.4% of cases of group A and 70% of group B were moderate smokers. There was a statistically insignificant difference between both groups regarding smoking and smoking index. Eltony and Ali found that smoking provokes aging changes of the skin. Tobacco smoke causes oxidative stress so that insufficient oxygen is supplied to the skin resulting in tissue ischemia and blood vessel occlusion.13 Our work showed that pruritus was of gradual onset in 93.3% and progressive course in 44.8% of cases, the mean duration of pruritus was 4.23± 4.9 months. Pruritus was generalized in 73.8% and localized in 26.2%. This was not in agreement with14 those who reported localized itch in 84.6% of elderly patients Regarding affected sites by itching, the upper and lower limbs, and back were the most often affected sites.14 Anus and genitalia were the least reported by patients, this is in agreement with14,15 those who reported that upper extremities in (63.6%) were the most affected sites by itch, and anogenital and genital areas were the least affected.14
Nocturnal pruritus was reported in 20%, and no diurnal variation in 55.2% of cases. Also,16 found that nocturnal pruritus has been proposed to be a result of pathophysiologic alterations of key functions of the skin during sleep such as thermoregulation, maintenance of fluid balance and barrier function. Additionally, they reported that daily activities can play a role; hence, the absence of other stimuli during the night increases the perception of itch.16
In this work, no seasonal variation of itching was reported in 55.6% of cases, winter was the most common season associated with itching (20%), which was similar to17 who found that chronic pruritus in elderly was the most intense during winter due to changes in air humidity, which may affect the skin barrier and was related to the aggravation of xerosis.17
We found that systemic antihistaminic drugs were effective in relieving itching in 22.2% of cases and emollients in 8%.14 Kopyciok reported that cream, cold compress and/or a cold shower were stated by 92.3% as a relieving factor of itch.15
Dermatitis was the most common dermatological cause of itching in 33.7% of our cases, this is in agreement with9 those who reported that dermatitis was a cause of pruritus in 22.8% of elderly.9 Also,12 found in an Egyptian study in elderly, eczema was present in 20% of study population. Xerosis was reported in 12.7% of the cases and represented the second cause of pruritus in this work. Also, they observed that xerosis in 9.7% of study population,12 however,9 found that xerosis was the most common cause of itching in elderly (38.9%), the difference may be related to that our study was conducted in early winter with a mean temperature was of 27.2°C and humidity of 70%9
Xerosis, or dry skin, is one of the most common causes of pruritus in the elderly. The prevalence of xerosis in patients with chronic itch was found to be as high as 69%.18
Pruritus with systemic causes constituted 29.8% of our patients.19 Reported that 14–50% of pruritic adult and elderly patients without a clear dermatologic cause have an underlying internal cause for their symptom.19 Renal diseases were the most common systemic cause of pruritus in elderly in the present study affecting 46.2% of the cases, as there was statistically significant difference between both groups regarding creatinine level (p value =0.012), which was not in agreement with9 who found that kidney diseases represent only 9.7% of systemic causes of pruritus in elderly, but in line with our study20 reported that renal pruritus was the most common systemic cause of pruritus and it affects 50–90% of patients undergoing peritoneal dialysis or hemodialysis.20
Hepatic diseases were detected in 34.3% of the cases and represented the second systemic cause of pruritus in elderly. The prevalence of HCV infection increases with age.21,22 Alhmada reported that itching affected 15% of positive C patients.22 It was also23 found that pruritus occurs in approximately 20–25% of jaundiced patients.23 Throughout our study, diabetes was found to be a cause of itching in 9% of the patients, there was statistically significant difference between two groups as regards post-prandial sugar as (P value = 0.003). Post-prandial sugar was higher among group A than group B patients and HbA1c was higher than normal in group A. This was not similar to Thaipisuttikul (1998) who reported the diabetes as the most common systemic cause of pruritus in elderly in 80.9%,9,24 showed that pruritus was the second most common cutaneous manifestation in diabetes, 49% of diabetic patients had pruritus.24
One of the causes of pruritus in DM is severe skin xerosis, as xerosis cutis occur in one of four diabetic patients as reported by Ikarashi, 2021.25 However, pruritus in our diabetic patients was not associated with xerosis.
Hyperthyroidism was found to be a systemic cause of pruritus in 6%, as we found that T3 and T4 level were higher than normal. In line with our results,26 we found that hyperthyroidism was proved to be associated with cutaneous manifestation as itching.26 We found that iron deficiency anemia affected 4.5% of elderly patient, which was in agreement with Thaipisuttikul (1998) who reported that iron deficiency anaemia is a cause of pruritus in elderly in 3.3% of patients.9
Among group B patients in the present study, vitiligo was the most common non-pruritic skin disease in 17.5%, followed by bacterial infections 14.37%, then warts in 13.75%, which was not in agreement with12 who found that 6.4% of the studied population had bacterial skin infections, 3% vitiligo, and 2% common warts.12 In the current study, verbal rating score (VRS) of itching revealed that 133/225 (59.1%) of cases had moderate itching, 79 (35.1%) severe itching and 13 (5.8%) mild itching, which was similar to27 those who reported that moderate to severe pruritus is known to affect 60% of the elderly individuals.27
Conclusion
Senile pruritus in elderly is relatively not well examined in our society. There is a need for awareness and identification of cases to put preventive strategies as it affects the quality of life of these patients. Every patient with pruritus should undergo careful history, full general and dermatologic examination. Further diagnostic tests, including skin biopsy, might be helpful in the diagnosis of unclear dermatological cases. Physical and mental deprivation may complicate proper assessment of pruritus severity. The cognitive and emotional component must be evaluated as depression and anxiety can aggravate senile pruritus Future studies are recommended to be on larger sample size of elderly patients with pruritus.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rose M, Flatt T, Graves J
2. Dillin A, Gottschling DE, Nyström T. The good and the bad of being connected: the integrons of aging. Curr Opin Cell Biol. 2014;26:107–112. doi:10.1016/j.ceb.2013.12.003
3. Zhang S, Duan E. Fighting against skin aging: the way from bench to bedside. Cell Transplant. 2018;27(5):729–738.
4. Sweed H. Population ageing- Egypt report. Middle East J Age Ageing. 2016;13:10–17. doi:10.5742/MEJAA.2016.92881
5. Ständer S, Schäfer I, Phan NQ, et al. Prevalence of chronic pruritus in Germany: results of a cross-sectional study in a sample working population of 11,730. Dermatology. 2010;221(3):229–235. doi:10.1159/000319862
6. Ständer S, Weisshaar E, Mettang T, et al. Clinical classification of itch: a position paper of the International Forum for the Study of itch. Acta Derm Venereol. 2007;87(4):291–294. doi:10.2340/00015555-0305
7. Kini SP, DeLong LK, Veledar E, McKenzie-Brown AM, Schaufele M, Chen SC. The impact of pruritus on quality of life: the skin equivalent of pain. Arch Dermatol. 2011;147(10):1153–1156. doi:10.1001/archdermatol.2011.178
8. Phan NQ, Blome C, Fritz F, et al. Assessment of pruritus intensity: prospective study on validity and reliability of the visual analogue scale, numerical rating scale and verbal rating scale in 471 patients with chronic pruritus. Acta Derm Venereol. 2012;92(5):502–507. doi:10.2340/00015555-1246
9. Thaipisuttikul Y. Pruritic skin diseases in the elderly. J Dermatol. 1998;25(3):153–157. doi:10.1111/j.1346-8138.1998.tb02371.x
10. Valdes-Rodriguez R, Mollanazar NK, González-Muro J, et al. Itch prevalence and characteristics in a Hispanic geriatric population: a comprehensive study using a standardized itch questionnaire. Acta Derm Venereol. 2015;95(4):417–421. doi:10.2340/00015555-1968
11. Yalçın B, Tamer E, Toy GG, Öztaş P, Hayran M, Allı N. The prevalence of skin diseases in the elderly: analysis of 4099 geriatric patients. Int J Dermatol. 2006;45(6):672–676. doi:10.1111/j.1365-4632.2005.02607.x
12. El-Hamd MA, Abd-Elmaged WM, Mohammed NA. Skin disorders among elderly patients: clinicodemographic characteristics of 808 Egyptian patients. Egypt J Dermatol Venerol. 2020;40(1):38. doi:10.4103/ejdv.ejdv_22_19
13. Eltony SA, Ali SS. Histological study on the effect of nicotine on adult male guinea pig thin skin. Anat Cell Biol. 2017;50(3):187–199. doi:10.5115/acb.2017.50.3.187
14. Dyhre-Petersen N, Gazerani P. Presence and characteristics of senile pruritus among Danish elderly living in nursing homes. Future Sci OA. 2019;5(6):FSO399. doi:10.2144/fsoa-2019-0036
15. Kopyciok ME, Ständer HF, Osada N, Steinke S, Ständer S. Prevalence and characteristics of pruritus: a one-week cross-sectional study in a German dermatology practice. Acta Derm Venereol. 2016;96(1):50–55.
16. Lavery MJ, Stull C, Kinney MO, Yosipovitch G. Nocturnal pruritus: the battle for a peaceful night’s sleep. Int J Mol Sci. 2016;17(3):425. doi:10.3390/ijms17030425
17. Patel T, Ishiuji Y, Yosipovitch G. Nocturnal itch: why do we itch at night? Acta Derm Venereol. 2007;87(4):295–298. doi:10.2340/00015555-0280
18. Norman R. Xerosis and pruritus in the elderly, recognition and management. Dermatol Ther. 2003;16(3):254–259. doi:10.1046/j.1529-8019.2003.01635.x
19. Tammaro A, Chello C, Di Fraia M, et al. Iron-deficiency and pruritus: a possible explanation of their relationship. Int J Res Dermatol. 2018;4:605. doi:10.18203/issn.2455-4529.IntJResDermatol20184470
20. Narita I, Iguchi S, Omori K, Gejyo F. Uremic pruritus in chronic hemodialysis patients. J Nephrol. 2008;21(2):161–165.
21. Garibyan L, Chiou AS, Elmariah SB. Advanced aging skin and itch: addressing an unmet need. Dermatol Ther. 2013;26(2):92–103. doi:10.1111/dth.12029
22. Alhmada Y, Selimovic D, Murad F, et al. Hepatitis C virus associated pruritus: etiopathogenesis and therapeutic strategies. World J Gastroenterol. 2017;23(5):743–750. doi:10.3748/wjg.v23.i5.743
23. Bunchorntavakul C, Reddy KR. Pruritus in chronic cholestatic liver disease. Clin Liver Dis. 2012;16(2):331–346. doi:10.1016/j.cld.2012.03.010
24. Al-Mutairi N, Zaki A, Sharma AK, Al-Sheltawi M. Cutaneous manifestations of diabetes mellitus. Study from Farwaniya hospital, Kuwait. Med Princ Pract. 2006;15(6):427–430. doi:10.1159/000095488
25. Ikarashi N, Mizukami N, Chenchen P, et al. Role of cutaneous Aquaporins in the development of xeroderma in type 2 diabetes. Biomedicines. 2021;9(2):104. doi:10.3390/biomedicines9020104
26. Lause M, Kamboj A, Fernandez Faith E. Dermatologic manifestations of endocrine disorders. Transl Pediatr. 2017;6(4):300–312. doi:10.21037/tp.2017.09.08
27. Rajagopalan M, Saraswat A, Godse K, et al. Diagnosis and management of chronic pruritus: an expert consensus review. Indian J Dermatol. 2017;62(1):7–17. doi:10.4103/00195154.198036
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.