Back to Journals » Cancer Management and Research » Volume 18

Clinical and Histopathological Prognostic Factors for Disease-Free Survival in Early-Stage Acral and Non-Acral Cutaneous Melanoma: A Retrospective Asian Cohort Analysis
Authors Chiu YJ ![]() , Cheng CY, Chen KC, Li CY
, Cheng CY, Chen KC, Li CY ![]() , Wang TH, Tsai CH
, Wang TH, Tsai CH
Received 16 November 2025
Accepted for publication 24 February 2026
Published 24 March 2026 Volume 2026:18 577632
DOI https://doi.org/10.2147/CMAR.S577632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Javier-David Benitez-Fuentes
Yu-Jen Chiu,1,2 Chiao-Yun Cheng,1 Kuan-Cheng Chen,1 Cheng-Yuan Li,3,4 Tien-Hsiang Wang,1,2 Chi-Han Tsai1
1Division of Plastic and Reconstructive Surgery, Department of Surgery, Taipei Veterans General Hospital, Taipei, 11217, Taiwan; 2Department of Surgery, School of Medicine, National Yang Ming Chiao Tung University, Taipei, 112304, Taiwan; 3Department of Dermatology, Taipei Veterans General Hospital, Taipei, 11217, Taiwan; 4Faculty of Medicine, School of Medicine, National Yang Ming Chiao Tung University, Taipei, 112304, Taiwan
Correspondence: Yu-Jen Chiu, Division of Plastic and Reconstructive Surgery, Department of Surgery, Taipei Veterans General Hospital, 19/F, No. 201, Sec. 2, Shipai Road, Beitou, Taipei, 11217, Taiwan, Email [email protected]
Background: Melanoma in Asian populations exhibits distinct clinicopathological features compared to Western populations. While acral melanoma (AM) is the predominant subtype among Asians, recent studies have demonstrated unique genomic profiles across melanoma subtypes within this population, suggesting underlying biological differences. Despite these observations, prognostic factors affecting disease-free survival (DFS) in early-stage melanoma remain insufficiently characterized among Asian patients. Improved DFS-based risk stratification may inform risk-adapted surveillance strategies in clinical practice. This study investigates clinicopathological factors associated with DFS in early-stage melanoma among Taiwanese patients.
Methods: A retrospective analysis was performed on 186 Asian patients with early-stage melanoma. Key factors, including age, gender, tumor location, histological subtype, Breslow thickness, mitotic rate, Lymphovascular Invasion (LVI), lactate dehydrogenase (LDH) levels, and ulceration, were analyzed. Cox proportional hazards models assessed the influence of these factors on DFS.
Results: Advanced age (≥ 65) was associated with poorer DFS (HR 1.87, 95% CI 1.23– 2.83, p = 0.003). Female sex was associated with a lower risk of disease recurrence compared with male sex (HR 0.657, 95% CI 0.436– 0.989, p = 0.044). Ulceration (HR 2.09, 95% CI 1.42– 3.09, p = 0.0002), Breslow thickness, and mitotic rate (HR 2.09, 95% CI 1.13– 3.86, p = 0.0183) were associated with an increased risk of disease recurrence. In the multivariate analysis, LVI (HR 8.69, 95% CI 1.73– 43.73, p = 0.009) and ulceration (HR 2.01, 95% CI 1.05– 3.85, p = 0.035) were identified as independent risk factors for worse DFS; notably, the markedly elevated hazard ratio observed for LVI should be interpreted with caution given its relatively low prevalence in the cohort.
Conclusion: Clinicopathological factors, including age, gender, Breslow thickness, mitotic rate, ulceration, and LVI were associated with disease-free survival in univariate analyses. Importantly, LVI and ulceration emerged as independent prognostic factors in multivariate analysis in early-stage melanoma among Asian patients. These findings emphasize the need for tailored follow-up and management strategies to improve outcomes.
Keywords: acral melanoma, disease-free survival, prognostic factors, Breslow thickness, lymphovascular invasion, Asian population
Introduction
Melanoma is an aggressive form of skin cancer originating from melanocytes in the epidermis.1 Characterized by a high propensity for metastasis and poor prognosis, melanoma represents a significant clinical challenge globally.2–4 While the majority of research and clinical guidelines have focused on cutaneous melanoma in Caucasian populations, where ultraviolet (UV) radiation is a major etiologic factor, the epidemiological and pathological features of melanoma differ substantially in non-Caucasian populations, particularly in Asians.1,5–7
In Asian countries such as Taiwan, where over 70% of melanomas are acral in origin, acral melanoma (AM) represents the predominant subtype,5,8–11 unlike in Western populations, where it accounts for only 1% to 7%.12–14 AM which arises in sun-protected areas like the palms, soles, and nail beds, often occurs in less visible anatomical locations, leading to delayed diagnosis and resulting in deeper tumor invasion and worse clinical outcomes.5,15 Recent genomic studies have highlighted significant genetic differences between melanomas in Asian and Caucasian populations. In Caucasian cohorts, melanoma pathogenesis is strongly associated with UV radiation exposure, leading to a high frequency of characteristic UV-induced mutations such as BRAF and NRAS.1,16 Conversely, melanomas occurring in Asian populations, particularly AM, exhibit distinct genetic profiles marked by fewer UV-related mutations and a higher prevalence of unique structural variations and copy number alterations, including mutations or amplifications in genes such as KIT, CCND1, CDK4, and TERT.2,17 These ethnicity-specific genomic alterations suggest alternative oncogenic mechanisms in Asian melanoma, independent of UV exposure.
Consequently, prognostic models and therapeutic strategies developed from Western datasets might inadequately represent the risk and biological behavior of melanoma among Asian patients. Understanding these distinctive genetic backgrounds provides a critical rationale for investigating tailored prognostic indicators and improving individualized clinical management within Asian populations.
Multiple studies have identified age, Breslow thickness, ulceration, and lymphovascular invasion (LVI) as significant prognostic factors in melanoma.8,12,18–20 Whether these same variables carry equivalent prognostic weight in Asian cohorts, particularly those dominated by acral melanoma, remains uncertain. Furthermore, there is inconsistent evidence regarding the prognostic significance of other histopathological markers such as mitotic rate and ulceration across different ethnic groups.5,15,19,21,22
Given that most prognostic models are based on Western data, they may not adequately reflect the risk profiles of Asian populations, particularly in AM-dominant regions like Taiwan, thereby limiting the development of tailored clinical strategies that can guide clinical decision-making. In early-stage melanoma, accurate identification of prognostic factors is critical for determining follow-up protocols and treatment intensity.22,23 Without reliable prognostic markers reflective of local patient characteristics, clinicians may under- or over-treat individuals, leading to either unnecessary interventions or missed opportunities for early recurrence detection. For instance, while Taiwan’s national melanoma guideline currently stratifies follow-up intensity primarily based on clinical stage,24 it remains unclear whether additional high-risk features such as older age, greater tumor thickness, or lymphovascular invasion, should prompt more personalized surveillance.
To address these knowledge gaps, we conducted a retrospective analysis of early-stage melanoma patients treated at Taipei Veterans General Hospital between 2000 and 2023. Using Kaplan–Meier survival analysis and Cox proportional hazards modeling, we aimed to identify independent prognostic factors that influence disease free survival (DFS) in an Asian cohort. Rather than relying solely on traditional staging criteria, we sought to uncover which clinicopathological features within early-stage disease may help stratify patients by risk and guide surveillance intensity. This personalized approach to risk assessment may better capture the heterogeneity of melanoma presentation in Asian patients and improve long-term outcomes through earlier intervention and tailored follow-up care.
Methods
This is a retrospective analysis of patients with melanoma. The medical record of patients with early-stage melanoma between 2000 and 2023 at Taipei Veteran Hospital, a tertiary medical center in Taiwan were retrieved. The Strengthening the Reporting of Observational Studies in Epidemiology guidelines were followed in this study. This retrospective cohort study was approved by the Institutional Review Board of Taipei Veterans General Hospital (approval numbers: 2025-04-014AC). The requirement for informed consent was waived by the ethics committee because of the retrospective study design. Clinicopathological staging was determined according to the American Joint Committee on Cancer staging criteria. The patients’ demographics and tumor characteristics, including age, sex, location, Breslow thickness (tumor depth classified as T1 [≤1.0 mm], T2 [1.1–2.0 mm], T3 [2.1–4.0 mm], or T4 [>4.0 mm]), primary tumor site, lymphovascular invasion and ulceration were collected and analyzed. Finally, only cases with adequate histopathological data were included. Of the 375 eligible patients, totaling 186 patients had TNM clinical stage 0, I or II.
All analyses were performed using R version 4.2.0 (R Core Team, Vienna, Austria). Fisher’s exact test or the Chi-Square test were used to compare between categorical variables as appropriate. The Kaplan–Meier method was used to estimate 5-year cumulative DFS and Log rank test determined it’s significancy between different groups. Cox proportional regression was used to analyze independent risk factors affecting 5-year DFS in a univariant and multivariant model. Variables included in the multivariate Cox model were selected based on a priori clinical relevance and statistical significance in univariate analysis. Analysis were conducted using a complete-case approach; cases with missing values for covariates (including mitotic rate and serum lactate dehydrogenase [LDH]) were excluded from the corresponding models. The proportional hazards assumption was assessed using Schoenfeld residuals, and no significant violation was detected. Statistical significance was set at p < 0.05.
This study was approved by the Institutional Review Board of Taipei Veterans General Hospital. The requirement for informed consent was waived because of the retrospective nature of the study and the use of de-identified patient data, which posed minimal risk to the participants. All patient data were handled in strict accordance with institutional guidelines to ensure confidentiality and privacy. The study was conducted in compliance with the principles of the Declaration of Helsinki.
Results
We retrospectively analyzed data from patients diagnosed with melanoma at Taipei Veterans General Hospital between 2000 and 2023. After excluding 189 patients with stage III and IV disease, 186 patients with early-stage melanoma (stage 0–II) were included in the final analysis. This study population provides a valuable opportunity to explore prognostic indicators in a predominantly acral melanoma cohort and contribute region-specific insights to the global melanoma literature.
The overall characteristics of the cohort are presented in Table 1. Most patients were aged ≥65 years (59.1%) and were male (56.5%). Tumor locations were predominantly on the extremities (77.4%), consistent with the common anatomical distribution of AM in Asian populations. Histopathologically, 70.4% of tumors were acral melanomas, while the remaining 29.6% were non-acral. Regarding serum lactate dehydrogenase (LDH) levels, 51.1% of patients had LDH <225 U/L, and 17.2% had levels ≥225 U/L. In terms of tumor depth, 28.0% of tumors had a Breslow thickness of <1 mm, while 23.1% were >4 mm, indicating a broad distribution of tumor invasiveness. Ulceration was observed in 40.9% of cases, and LVI was present in a small but clinically important subset (2.7%). Mitosis rates varied, with only 16.7% of patients demonstrating a high mitotic index (>3 mitoses/mm2), although over half of the cases (52.2%) had unknown mitotic data, limiting this variable’s interpretability.
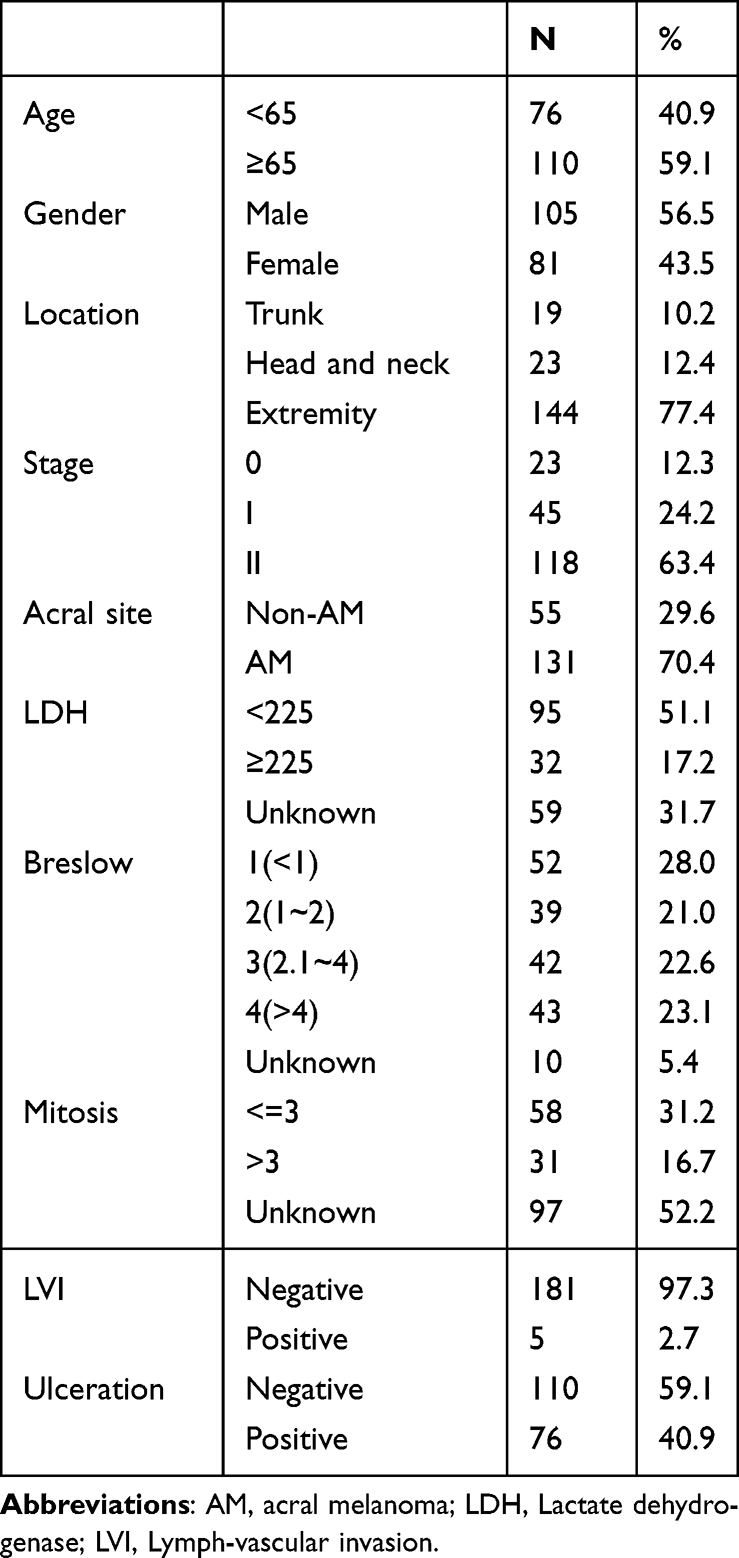 |
Table 1 Clinicopathological Characteristics |
Overall, our findings reveal that the presence of ulceration and LVI were significantly associated with shorter DFS in both univariate and multivariate analysis. Older age, male and mitosis rate also showed trends toward poorer prognosis but with less consistent statistical significance. These results are largely in agreement with Western studies but extend their relevance to an Asian cohort dominated by AM cases. Notably, the high percentage of AM cases in our population (70.4%) reinforces the distinct epidemiology of melanoma in Taiwan and underscores the need for subtype-specific prognostic tools, as shown in Table 2.
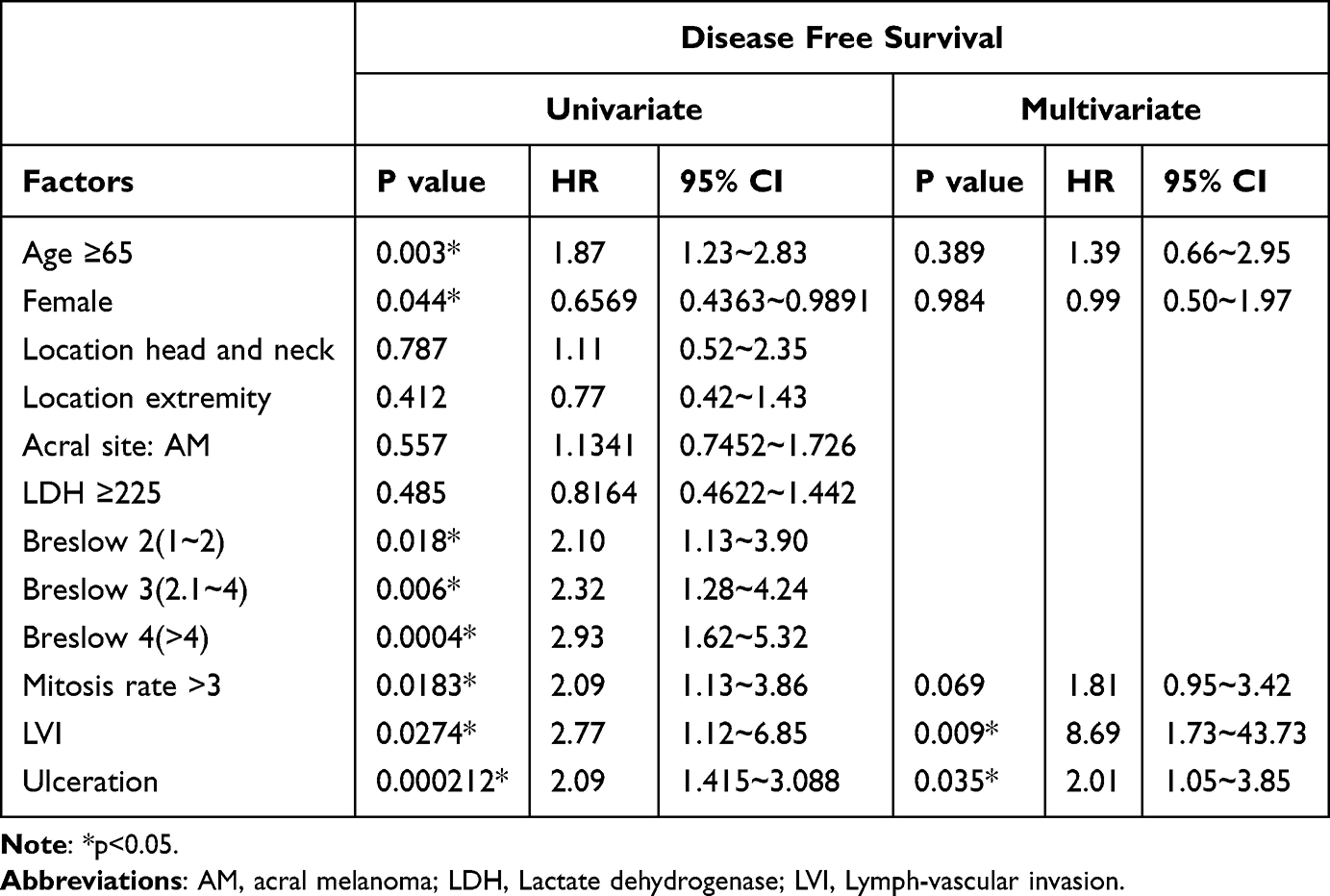 |
Table 2 Disease Free Survival |
To facilitate a deeper understanding of these associations, we now present a series of Kaplan–Meier survival curves illustrating the impact of key clinicopathological variables on disease-free survival. These include age, gender, location, histology, Breslow thickness, mitotic rate, ulceration, LDH and LVI. Each graph is accompanied by a narrative interpretation that highlights the clinical implications and statistical significance of the observed survival trends.
The Kaplan-Meier survival curve indicates that age is significantly associated with disease-free survival in early-stage melanoma patients. Patients aged ≥65 years exhibited a notably poorer DFS compared to those under 65. The separation between the survival curves is clear and persistent throughout the follow-up period, suggesting that older age is an independent risk factor for earlier recurrence. This finding underscores the importance of age as a prognostic marker and highlights the need for closer surveillance in elderly patients, even in early-stage disease, as shown in Figure 1.
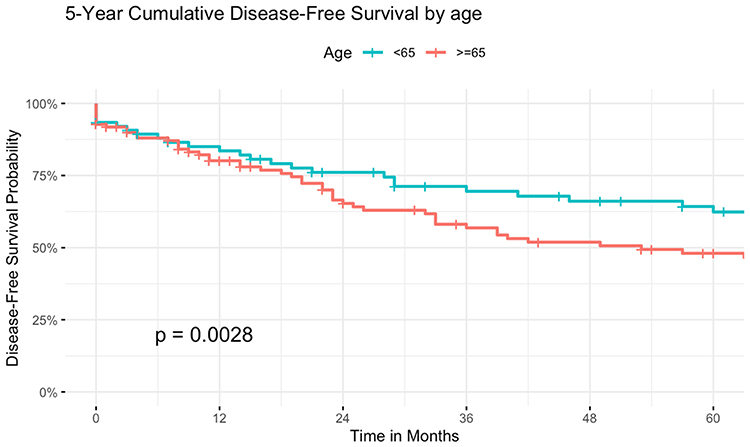 |
Figure 1 Kaplan–Meier curves of 5 year disease-free survival in patients with early-stage melanoma stratified by Age. |
The Kaplan–Meier survival curve of 5-year disease-free survival stratified by gender demonstrates a distinct separation, with female patients showing superior outcomes compared to male patients, as shown in Figure 2. The divergence becomes more apparent after the first year and persists throughout the follow-up period. The Log rank test confirmed that this difference was statistically significant (P = 0.043). These results indicate that male gender is associated with poorer DFS, supporting its potential role as an adverse prognostic factor in this cohort.
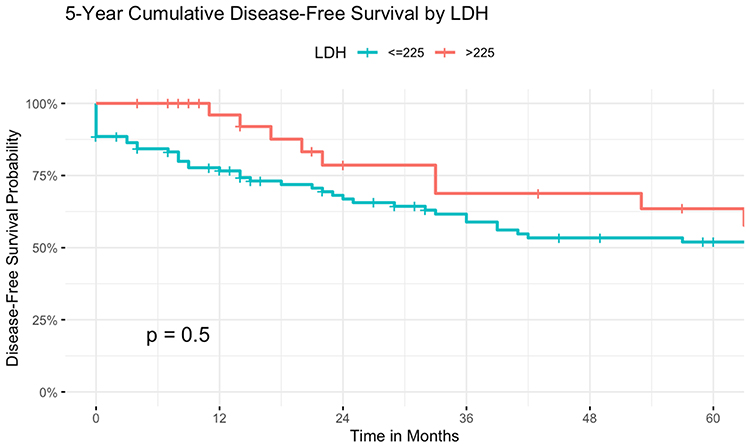 |
Figure 2 Kaplan–Meier curves of 5 year disease-free survival in patients with early-stage melanoma stratified by Gender. |
This survival analysis demonstrates a significant inverse relationship between Breslow thickness and DFS. Patients with thicker melanomas (higher Breslow depth) had substantially poorer DFS compared to those with thinner lesions. The survival curves diverge early and remain separated over time, indicating that Breslow thickness is a critical predictor of recurrence risk. This result aligns with previous studies and reinforces the role of tumor depth as a core component of melanoma staging and prognosis, as shown in Figure 3.
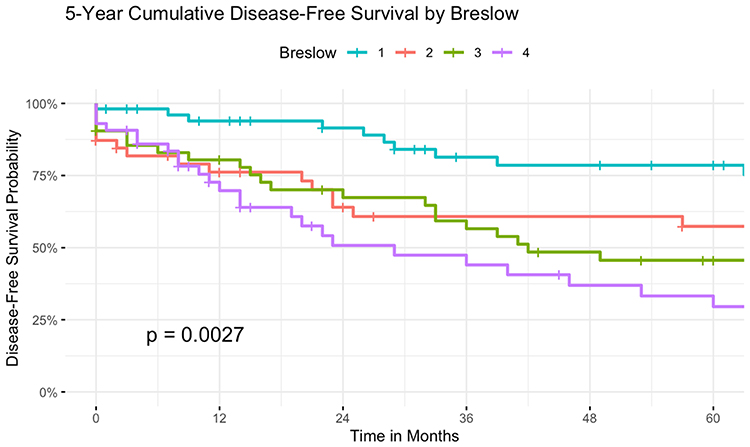 |
Figure 3 Kaplan–Meier curves of 5 year disease-free survival in patients with early-stage melanoma stratified by Breslow. |
The DFS curve based on mitotic rate shows that patients with higher mitotic activity tend to have worse outcomes, although the degree of separation is less pronounced than in other variables like Breslow or age. The trend suggests a possible association between rapid tumor cell proliferation and increased recurrence risk. Although mitotic rate is not consistently included in all staging systems, its role as a secondary prognostic factor should not be overlooked, as shown in Figure 4.
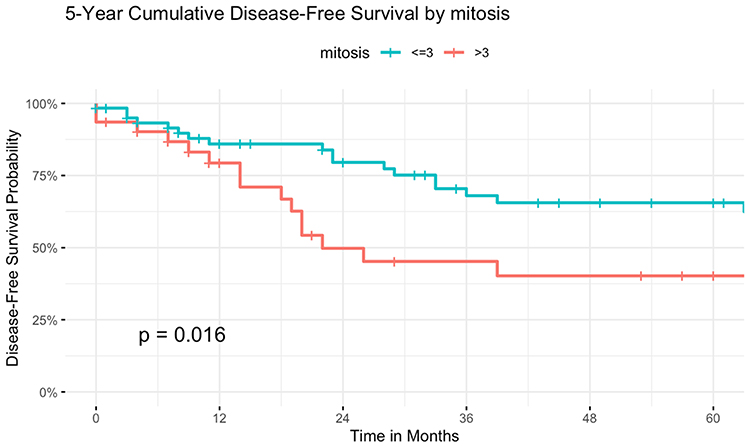 |
Figure 4 Kaplan–Meier curves of 5 year disease-free survival in patients with early-stage melanoma stratified by Mitosis. |
Patients whose tumors exhibited ulceration demonstrated significantly shorter DFS compared to those without ulceration, as shown in Figure 5. The survival curves diverge notably early in the follow-up period and continue to separate over time. This result confirms ulceration as a negative prognostic indicator, consistent with global melanoma literature.
 |
Figure 5 Kaplan–Meier curves of 5 year disease-free survival in patients with early-stage melanoma stratified by Ulceration. |
LVI showed a strong and statistically significant correlation with poor DFS, as shown in Figure 6. Patients with LVI-positive tumors had the lowest survival probabilities among all subgroups analyzed. The survival curve drops sharply compared to the LVI-negative group, underscoring the aggressive nature of tumors with vascular or lymphatic spread. In multivariate analysis, LVI was associated with a markedly increased hazard ratio, despite its relatively low prevalence in the cohort. This supports the inclusion of LVI in multivariate prognostic models and suggests its potential utility in identifying high-risk patients requiring intensified follow-up.
 |
Figure 6 Kaplan–Meier curves of 5 year disease-free survival in patients with early-stage melanoma stratified by LVI. |
In univariate Cox proportional hazards analysis, neither tumor location nor histologic subtype was significantly associated with disease-free survival. Compared to tumors on the trunk (reference), head and neck lesions had a hazard ratio of 1.11 (95% CI: 0.52–2.35, p = 0.787), and extremity tumors had an HR of 0.77 (95% CI: 0.42–1.43, p = 0.412). For histology, acral melanoma (AM) showed an HR of 1.13 (95% CI: 0.75–1.73, p = 0.557) compared to non-AM, indicating no significant prognostic impact on DFS. These results align with the Kaplan–Meier curves, which suggested potential trends but did not reach statistical significance.
Discussion
Melanoma is a heterogeneous disease comprising biologically and prognostically distinct clinicopathological subtypes.22 Most prognostic models, particularly those emphasizing age, Breslow thickness, and ulceration, are derived primarily from studies in Western populations,18 which often underrepresent the AM subtype prevalent in Asian cohorts. Given the high incidence of AM in Taiwan,24,25 our study aimed to identify prognostic factors specific to early-stage melanoma (stage 0–II) using a large, long-term dataset from a single tertiary medical center. In our cohort, age, gender, Breslow thickness, mitosis, LVI and ulceration emerged as independent prognostic indicators for DFS. These findings are largely consistent with those from European and American studies,12,13 where tumor thickness and ulceration have been widely validated as strong predictors of recurrence. While our results align with existing literature, they also offer novel insights that reflect the distinct clinicopathological characteristics of Taiwanese patients.
Age, as a traditional prognostic factor, however only showed poor DFS in Kaplan–Meier analysis. The poorer prognosis observed in older patients may be attributed to factors such as delayed diagnosis, reduced attention to skin changes, lower awareness of early melanoma signs, the presence of seborrheic keratoses that may mask malignancy or anatomical tumor locations that are less visible and biologically more aggressive tumor features such as increased thickness, ulceration, and higher mitotic activity.15,25,26
Breslow thickness has been a cornerstone of prognostic indicator across diverse populations and melanoma subtypes. In our study, increased thickness was strongly associated with poorer DFS. This is biologically plausible, as thicker tumors frequently exhibit BRAF-driven MAPK pathway activation and matrix metalloproteinase overexpression, which promote tumor cell proliferation and invasion.1 These mechanisms support the observed correlation between tumor depth and aggressive clinical behavior.
LVI defined as the presence of melanoma cells within lymphatic or blood vessels and is thought to facilitate metastatic spread to regional lymph nodes and distant sites.27 Although not currently included in AJCC staging systems, LVI has been associated with other poor prognostic features such as increased Breslow thickness, ulceration, mitotic rate, and sentinel lymph node positivity.27,28 Our findings support its prognostic relevance, with LVI significantly associated with reduced DFS.
Ulceration retained prognostic significance in acral melanoma, consistent with Western studies where it is a well-established predictor of recurrence and survival.19,22 This indicates that ulceration represents a universal marker of tumor aggressiveness across melanoma subtypes. Given the disproportionately high prevalence of AM in Asian populations, the clinical impact of ulceration may be even more pronounced.5,29 These findings support its inclusion in current staging systems while underscoring the need for further studies in Asian cohorts.
Although high mitotic rate, age and gender did not reach statistical significance in our multivariate Cox regression analysis, both factors demonstrated trends toward poorer DFS in Kaplan-Meier analysis and are widely recognized as important prognostic indicators in previous studies.4,5,19,21,30 The lack of statistical significance in our model may be partly explained by the relatively small number of patients exhibiting these features and the presence of missing data, which could have limited the power of the analysis.
These findings have important clinical implications, suggesting that even within early-stage melanoma, risk stratification based on patient and tumor features is feasible and necessary. This challenges current uniform follow-up protocols that rely solely on tumor staging and supports the development of more individualized surveillance schedules—particularly for elderly patients or those with deeper tumors or LVI-positive pathology.
These findings also have direct implications for post-treatment surveillance strategies. Current NCCN guidelines generally recommend symptom-driven imaging and do not support routine imaging for asymptomatic patients with early-stage melanoma.24 In contrast, local practice in Taiwan adopts a more proactive, stage-adapted follow-up approach, including baseline imaging and more frequent surveillance in selected patients, reflecting population-specific disease characteristics and healthcare system considerations.24 In light of our findings, patients with adverse prognostic features (eg, lymphovascular invasion and ulceration) may warrant closer surveillance in the early post-treatment period, when the risk of recurrence is generally considered higher in clinical practice, followed by regular long-term follow-up thereafter. Such risk-adapted follow-up strategies may help bridge the gap between uniform stage-based protocols and individualized surveillance tailored to high-risk subgroups within early-stage melanoma, particularly in AM-dominant populations such as those in Taiwan, while patients at lower risk may be appropriately managed with standard surveillance.
Our study further emphasizes the need for ethnic and regional specificity in melanoma prognostication, especially in AM-dominant populations like Taiwan. When comparing our findings with existing literature from both Western and Asian cohorts, we observed a mix of concordant and distinct prognostic patterns. Similar to prior studies from the United States and Europe, as well as several East Asian cohorts, our univariate analysis confirmed age, gender, Breslow thickness, mitotic rate, LVI, and ulceration as significant predictors of DFS. However, in multivariate analysis, only LVI and ulceration retained independent prognostic significance, highlighting their potential underappreciated value in early-stage melanoma risk stratification, especially within AM-dominant populations. Western-derived prognostic models may not fully capture the risk dynamics in Asian populations, especially in Taiwan. Our study contributes to a growing body of evidence advocating for the adaptation of clinical guidelines to reflect local disease characteristics and serves as a foundation for prospective validation in multicenter Asian cohorts.
Future research should aim to include larger, more diverse Asian populations and multi-institutional datasets to validate and strengthen the generalizability of our findings. While key oncogenic drivers such as BRAF, NRAS, NF1, and KIT mutations are well-documented in cutaneous melanoma, substantial genomic differences have been observed between cutaneous and acral melanoma. Specifically, acral melanoma is characterized by a lower burden of point mutations but a higher frequency of large-scale chromosomal aberrations, reflecting distinct tumor biology.1,31 Despite these differences, most molecular studies to date have focused predominantly on populations with cutaneous melanoma, leaving acral melanoma underrepresented in genomic and biomarker research. Given the high prevalence of AM in Asian populations, especially in Taiwan, there is a critical need for further research specifically targeting AM-dominant cohorts. Integrating molecular markers, such as immune-related biomarkers, gene expression signatures, and metabolic indicators, with established clinicopathological features (eg, Breslow thickness, ulceration, LVI) may facilitate the development of more precise and personalized prognostic models tailored to the biological characteristics of AM-dominant population.
Limitations
This study has several limitations that warrant consideration. First, the number of patients with certain adverse features such as LVI, ulceration, and high mitotic rate were limited, which may reduce the statistical power to detect significance in some subgroup analyses and raises concerns about model overfitting, particularly for rare variables like LVI (2.7% incidence). Second, a proportion of pathological variables had missing data, which may have biased multivariate model selection or attenuated the apparent impact of some prognostic factors. Third, although the cohort reflects real-world clinical practice in Taiwan, it was drawn from a single tertiary medical center, and thus generalizability to the broader Taiwanese or pan-Asian melanoma population may be limited. Finally, molecular or genetic markers such as BRAF, NRAS, or KIT mutations were not available in this dataset, limiting our ability to integrate clinicopathologic and genomic risk stratification.
Conclusion
Our study highlights the strong prognostic factors of age, gender, Breslow, mitosis, ulceration and LVI for early-stage melanoma in an Asian cohort predominantly composed of AM cases. These findings support the feasibility and necessity of risk stratification beyond standard staging. With patients harboring adverse pathological features—particularly LVI and ulceration—representing a higher-risk subgroup that may benefit from closer, individualized surveillance, whereas patients without these features may be appropriately managed with standard follow-up. Given the distinct epidemiological profile of melanoma in Taiwan, our results emphasize the need for population-specific prognostic models. By addressing a long-standing research gap, this study contributes to more accurate risk assessment, provides a rationale for risk-adapted follow-up strategies within existing guideline frameworks, and lays the groundwork for future multicenter validation in Asian population with melanoma.
AI-Assistance Statement
This manuscript was edited for English grammar and clarity using ChatGPT (GPT-5, OpenAI, 2025). The tool was used solely to improve language fluency and readability of the text under the supervision of the authors. No content generation, data analysis, or interpretation of scientific results was performed by the AI tool. The authors reviewed and approved all final text to ensure accuracy and integrity.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to express their sincere gratitude to Taipei Veteran General Hospital for their invaluable assistance throughout the course of this research.
Funding
This study was supported by a grant (No. V115C-013) from Taipei Veterans General Hospital, Taiwan, Taiwan (NSTC 114-2314-B-075-049) from the National Science and Technology Council, Taiwan; Medical scholarship foundation in memory of professor Albert Ly-Young Shen, Taiwan.; Melissa Lee Cancer Foundation, Taiwan (MLCF_V115_B11512).
Disclosure
The authors declare no competing interests in this work.
References
1. Davey MG, Miller N, McInerney NM. A review of epidemiology and cancer biology of malignant melanoma. Cureus. 2021;13(5):e15087. doi:10.7759/cureus.15087
2. Csányi I, Houshmand N, Szűcs M, et al. Acral lentiginous melanoma: a single-centre retrospective review of four decades in East-Central Europe. J Eur Acad Dermatol Venereol. 2020;34(9):2004–11. doi:10.1111/jdv.16227
3. Kolla AM, Vitiello GA, Friedman EB, et al. Acral lentiginous melanoma: a united states multi-center substage survival analysis. Cancer Control. 2021;28:10732748211053567. doi:10.1177/10732748211053567
4. Chen KC, Wang TH, Li CY, Chiu YJ. The diameter of cutaneous melanoma serves as a prognostic indicator for survival among acral‐melanoma predominant East Asian patients. World J Surg. 2024;48(7):1692–1699. doi:10.1002/wjs.12192
5. Lv J, Dai B, Kong Y, Shen X, Kong J. Acral melanoma in Chinese: a clinicopathological and prognostic study of 142 cases. Sci Rep. 2016;6(1):31432. doi:10.1038/srep31432
6. Chiu YJ, Li CY, Wang TH, Ma H, Chou TY. Comparative transcriptomic analysis reveals differences in gene expression and regulatory pathways between nonacral and acral melanoma in Asian individuals. J Dermatol. 2024;51(5):659–670. doi:10.1111/1346-8138.17187
7. Chiu YJ, Weng HY, Lin YY, et al. Genomic profiling with whole‐exome sequencing revealed distinct mutations and novel pathways in Asian melanoma. J Dermatol. 2022;49(12):1299–1309. doi:10.1111/1346-8138.16579
8. Oh Y, Choi S, Cho MY, et al. Male sex and Breslow thickness are important risk factors for recurrence of localized melanoma in Korean populations. J Am Acad Dermatol. 2020;83(4):1071–1079. doi:10.1016/j.jaad.2019.09.029
9. Lee TL, Lin MH, Liao YH, Liau JY, Sheen YS. Clinicopathological characteristics and prognosis in significantly thick acral lentiginous melanoma in Taiwan. J Formos Med Assoc. 2022;121(11):2338–2344. doi:10.1016/j.jfma.2021.12.001
10. Chu P-Y, Chen Y-F, Li C-Y, Wang T-H, Chiu Y-J, Ma H. Influencing factors associated with lymph node status in patients with cutaneous melanoma: an Asian population study. J Chin Med Assoc. 2023;86(1):72–79. doi:10.1097/JCMA.0000000000000809
11. Chen K-C, Chu P-Y, Li C-Y, Wang T-H, Chiu YJ. Diagnostic value of 18F-fluoro-2-deoxyglucose positron emission tomography/computed tomography imaging in acral melanoma–predominant Asian patients. J Chin Med Assoc. 2023;86(11):975–980. doi:10.1097/JCMA.0000000000001002
12. Huang K, Fan J, Misra S. Acral Lentiginous melanoma: incidence and survival in the United States, 2006–2015, an analysis of the SEER Registry. J Surg Res. 2020;251:329–339. doi:10.1016/j.jss.2020.02.010
13. Helkkula T, Christensen G, Mikiver R, Ingvar Å, Isaksson K, Nielsen K. Acral Melanoma incidence and survival trends in 1990–2020: a nationwide, population-based study. Acta Derm Venereol. 2024;104:adv40242. doi:10.2340/actadv.v104.40242
14. Chu P-Y, Lien K-P, Chen K-C, et al. Unraveling the obesity paradox: exploring the impact of body weight on cutaneous melanoma prognosis in Asian Population. Diabetes Metab Syndr Obes. 2024;17:3863–3873. doi:10.2147/DMSO.S477649
15. Yeo PM, Lim ZV, Tan WDV, et al. Melanoma in Singapore: a 20-year review of disease and treatment outcomes. Ann Acad Med Singap. 2021;50(6):456–466. doi:10.47102/annals-acadmedsg.2020535
16. Chiu YJ, Yang JS, Tsai FJ, et al. Curcumin suppresses cell proliferation and triggers apoptosis in vemurafenib‐resistant melanoma cells by downregulating the EGFR signaling pathway. Environ Toxicol. 2022;37(4):868–879. doi:10.1002/tox.23450
17. Fortuna A, Amaral T. Multidisciplinary approach and treatment of acral and mucosal melanoma. Front Oncol. 2024;14:1340408. doi:10.3389/fonc.2024.1340408
18. Balch CM, Gershenwald JE, Soong SJ, et al. Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol. 2009;27(36):6199–6206. doi:10.1200/JCO.2009.23.4799
19. Lino-Silva LS, Domínguez-Rodríguez JA, Aguilar-Romero JM, et al. Melanoma in Mexico: clinicopathologic features in a population with predominance of acral lentiginous subtype. Ann Surg Oncol. 2016;23(13):4189–4194. doi:10.1245/s10434-016-5394-x
20. Chu PY, Chen YF, Li CY, et al. Factors influencing locoregional recurrence and distant metastasis in Asian patients with cutaneous melanoma after surgery: a retrospective analysis in a tertiary hospital in Taiwan. J Chin Med Assoc. 2021;84(9):870–876. doi:10.1097/jcma.0000000000000586
21. Kim JE, Chung BY, Sim CY, et al. Clinicopathologic features and prognostic factors of primary cutaneous melanoma: a multicenter study in Korea. J Korean Med Sci. 2019;34(16):e126. doi:10.3346/jkms.2019.34.e126
22. Mandalà M, Rutkowski P, Galli F, et al. Acral lentiginous melanoma histotype predicts outcome in clinical stage I-II melanoma patients: an International multicenter study. ESMO Open. 2022;7(3):100469. doi:10.1016/j.esmoop.2022.100469
23. Serrano AVO, Contreras F, Triana I, et al. Clinical outcomes and prognostic factors of patients with early malignant melanoma in one Latin American Country: results of the epidemiological registry of malignant melanoma in colombia study. JCO Global Oncol. 2023;9:e2200377. doi:10.1200/go.22.00377
24. Wu CE, Liao YH, Wu CL, et al. Clinical practice consensus for the diagnosis and management of melanoma in Taiwan. J Formos Med Assoc. 2024;123(1):7–15. doi:10.1016/j.jfma.2023.07.016
25. Tsai K-C, Hung S-J, Wang J-H, et al. Cutaneous malignant melanoma in Eastern Taiwan: clinicopathologic analysis of 56 cases. Dermatologica Sinica. 2019;37(4):187–193. doi:10.4103/ds.ds_13_19
26. Wu PC, Chen YC, Chen HM, Chen LW. Prognostic factors and population-based analysis of melanoma with sentinel lymph node biopsy. Sci Rep. 2021;11(1):20524. doi:10.1038/s41598-021-99950-1
27. Namikawa K, Aung PP, Gershenwald JE, Milton DR, Prieto VG. Clinical impact of ulceration width, lymphovascular invasion, microscopic satellitosis, perineural invasion, and mitotic rate in patients undergoing sentinel lymph node biopsy for cutaneous melanoma: a retrospective observational study at a comprehensive cancer center. Cancer Med. 2018;7(3):583–593. doi:10.1002/cam4.1320
28. Namubiru P, Dalleywater W, Lashin S, Elsheikh S. Can angiotropism and lymphovascular invasion refine the current cutaneous melanoma staging system? J Cutan Pathol. 2024;51(4):288–298. doi:10.1111/cup.14561
29. Park SM, Jeong HY, Kim H-S, Kwak M-J, Yi CC, Bae YC. Epidemiology and prognostic factors of malignant melanoma among 200 Asian patients from a Single Medical Center. Indian J Surg. 2024;86(2):310–317. doi:10.1007/s12262-023-03857-2
30. Mejbel HA, Torres-Cabala CA, Milton DR, et al. Prognostic significance of acral lentiginous histologic type in T1 melanoma. Mod Pathol. 2021;34(3):572–583. doi:10.1038/s41379-020-0641-x
31. Basurto-Lozada P, Molina-Aguilar C, Castaneda-Garcia C, et al. Acral lentiginous melanoma: basic facts, biological characteristics and research perspectives of an understudied disease. Pigm Cell Melanoma Res. 2021;34(1):59–71. doi:10.1111/pcmr.12885
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.