Back to Journals » ClinicoEconomics and Outcomes Research » Volume 16
Clinical and Economic Value of a Biosimilar Portfolio to Stakeholders: An Integrative Literature Review
Authors Fox GE ![]() , Bernauer M, Stephens JM
, Bernauer M, Stephens JM ![]() , Jackson B, Roth JA, Shelbaya A
, Jackson B, Roth JA, Shelbaya A
Received 20 October 2023
Accepted for publication 19 February 2024
Published 13 May 2024 Volume 2024:16 Pages 247—416
DOI https://doi.org/10.2147/CEOR.S445697
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Samer Hamidi
Grace E Fox,1 Mark Bernauer,1 Jennifer M Stephens,1 Bianca Jackson,1 Joshua A Roth,2 Ahmed Shelbaya2,3
1Strategic Market Access, OPEN Health, Bethesda, MD, USA; 2Global Access and Value, Pfizer Inc., New York, NY, USA; 3Department of Epidemiology, Mailman School of Public Health, Columbia University, New York, NY, USA
Correspondence: Mark Bernauer, Strategic Market Access, OPEN Health, Bethesda, MD, USA, Tel +1 240 821-1292, Email [email protected]
Purpose: While the value of individual biosimilars is evident, little is known about the value of a biosimilar portfolio beyond the cost savings between biosimilars and originators. Stakeholders may consider the value of a manufacturer’s biosimilar portfolio, especially when negotiating portfolio-based contracts or other rebate programs. However, little is known about what other types of value, in addition to financial benefits, decision-makers perceive regarding a manufacturer with a biosimilar portfolio compared to those without one. The objective of this integrative literature review was to describe a conceptual framework consisting of themes that may help define the value of a biosimilar portfolio.
Methods: An integrative literature review was conducted using Excerpta Medica Database (Embase) and Medical Literature Analysis and Retrieval System Online (MEDLINE). Grey literature searches of search engines, journals not indexed in Embase or MEDLINE, healthcare payers, health technology assessment bodies, value frameworks, and non-pharmaceutical industry analogs were also conducted. Eligible studies reported on the value of a biosimilar portfolio in decision-making by stakeholders. Apart from the literature, insights were gained from clinical experience and observation.
Results: No studies investigating biosimilar portfolio value were identified; however, several themes were identified that may help define the value of a biosimilar portfolio: Manufacturing; procurement, inventory, and storage; administration; education; and transaction costs. Several non-pharmaceutical industry analogs were identified: Product line length and single-supplier versus multiple-supplier procurement. Several themes were identified through other sources: Science credibility and research. Based on these themes, we developed a conceptual framework for biosimilar portfolio value.
Conclusion: To our knowledge, this is the first study to systematically assess and create a framework for biosimilar portfolio value. The conceptual framework described here could be tested to quantify the clinical and economic value associated with a biosimilar portfolio.
Plain Language Summary: Though the value of single biosimilars is evident, little is known about the value of a biosimilar portfolio beyond the cost savings incurred between biosimilars and originators.We identified seven themes that may help to define the value of a biosimilar portfolio: Manufacturing; procurement, inventory, and storage; administration; education; transaction costs; science credibility; and research.These themes may be integrated into a conceptual framework that may form a basis to help quantify the clinical and economic benefit of a biosimilar portfolio to stakeholders.
Keywords: biosimilar, portfolio, value, analog
Introduction
Generally defined as a collection of products or services a company offers, portfolios are used across industries to mitigate risk, improve cash flow, spur innovation, and increase brand awareness.1 For example, the Coca-Cola Company leverages its portfolio to develop exclusive distribution agreements.2 The use of portfolios has taken place more recently in the pharmaceutical industry, where manufacturers historically focused on one product or biological pathway.3 Work by Bleys et al suggests that the pharmaceutical industry first embraced the portfolio model in 2010.3 In a portfolio model, there is less investment risk versus a single product. Other advantages include a greater chance of financial incentives delivered across multiple assets. Potential disadvantages include scarce resources owing to diversification, impeded decision-clarity/lack of focus, and centralized functions that may cause prioritization and competition among assets.
Pharmacoeconomic evaluation of pharmaceutical products is multifaceted but generally has only considered cost (eg, cost per quality-adjusted life-years [QALY] outside of the United States).4 There are other sources of value that are currently not considered in these assessments. Beyond cost, other elements may be helpful in evaluating value that may need to be considered in decision-making for pharmaceutical products, such as reduction in uncertainty, fear of contagion, and the value of hope.4
The European Medicines Agency (EMA) approved the first biosimilar Omnitrope® (somatropin) in 2006, while the Food and Drug Administration (FDA) approved the first United States (US) biosimilar Zarxio® (filgrastim-sndz) in 2015.5 Biosimilar approvals have steadily increased since then, with 80 authorized biosimilars in the European Union (EU) and 45 approved biosimilars in the US as of January 2024.6,7 In 2020, only 13% of biosimilars were being developed by six large pharmaceutical companies; thus, the majority of development was undertaken by smaller companies.8
Evidence suggests that stakeholders frequently use studies related to clinical efficacy and safety as well as pharmacoeconomic evidence in decision-making.9,10 Additionally, stakeholders may consider the value of a manufacturer’s biosimilar portfolio in a particular therapeutic area in decision-making, especially when negotiating portfolio-based contracts or other rebate programs. However, little is known about what other types of hidden value, in addition to financial benefits, decision-makers perceive regarding a pharmaceutical company with a biosimilar portfolio compared to those without a biosimilar portfolio. Large pharmaceutical companies often believe their size and breadth of products offer an advantage relative to smaller companies.
While the inherent value of single biosimilars is clear, little is known about the relative value of having a biosimilar portfolio beyond the cost savings incurred between biosimilars and originators. Furthermore, no studies have described a method to assess the value of a biosimilar portfolio beyond cost. For the purpose of this integrative literature review, a biosimilar portfolio is defined by the authors as a collection of ≥3 biosimilars produced by a single pharmaceutical company. The objective of this integrative literature review is to describe a conceptual framework consisting of themes that may help define the value of a biosimilar portfolio.
Materials and Methods
An integrative literature review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.11 The literature search was conducted in Excerpta Medica Database (Embase) and Medical Literature Analysis and Retrieval System Online (MEDLINE) via the ProQuest platform in May 2022. Subject headings and free-text terms for portfolio and value were combined with those for study design and publication type (Table 1). The search was limited to 2010 to May 2022, as work by Bleys et al suggests that the portfolio model was implemented by the biotech industry in 2010.3 Grey literature searches of search engines, journals not indexed in Embase or MEDLINE, healthcare payers, health technology assessment (HTA) bodies, value frameworks, and non-pharmaceutical industry analogs (eg, beverage brand portfolios, product line length, and supplier procurement) were conducted using search strings, such as “Portfolio” and “Biosimilar portfolio”.
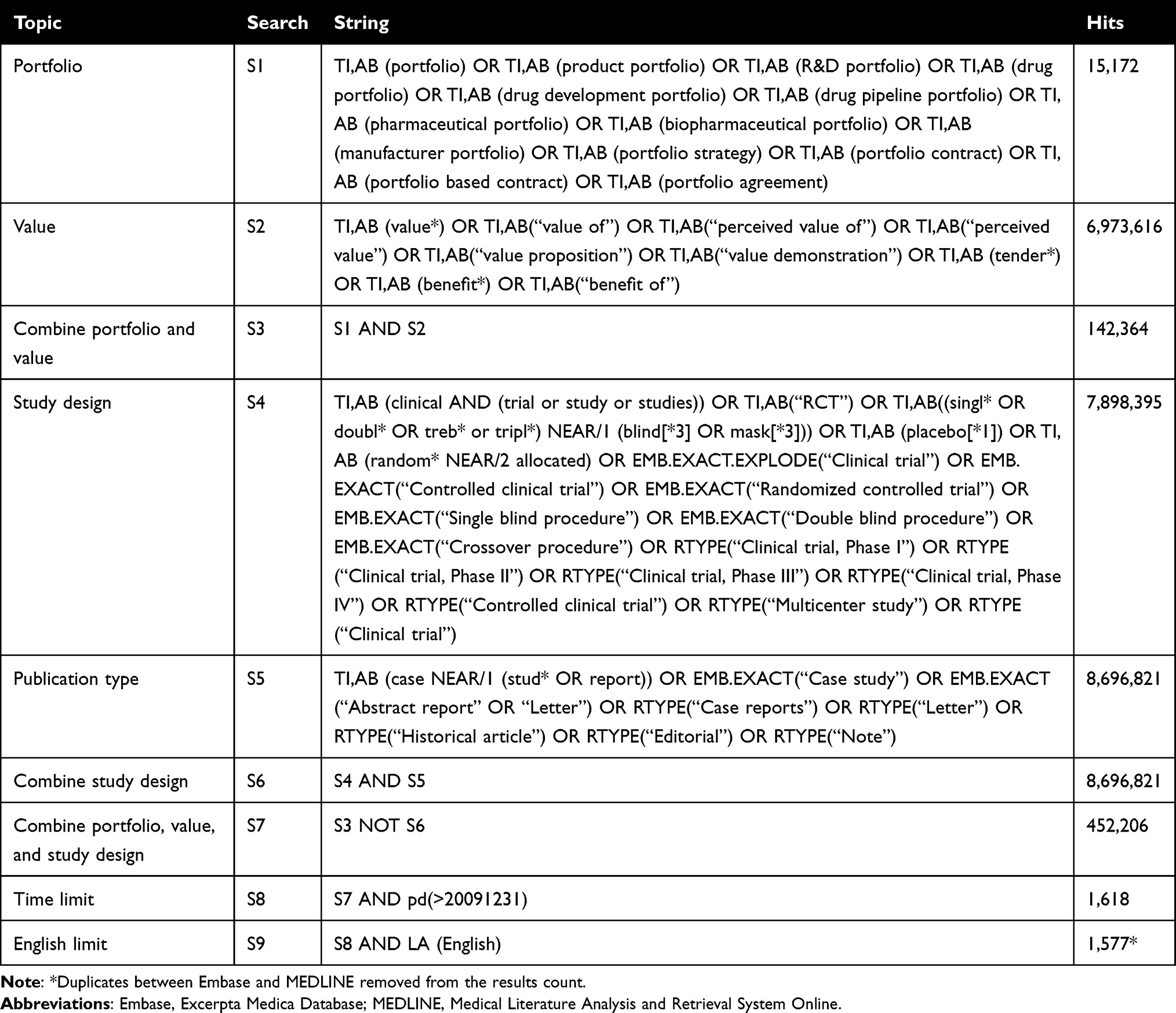 |
Table 1 Embase/MEDLINE Search Strategy |
Pre-specified eligibility criteria regarding study population, intervention, comparator, outcome, and study design (PICOS) are outlined in Table 2. The PICOS was designed to capture studies reporting on the value of a biosimilar portfolio to key stakeholders, including patients, clinicians, pharmacy staff, nursing staff, and the institution/finance staff. The outcome of interest was the value of a biosimilar portfolio, as defined by the studies. Study designs of interest were observational studies, systematic literature reviews, non-systematic or narrative reviews. Relevant studies were limited to those published after 2009 in English.
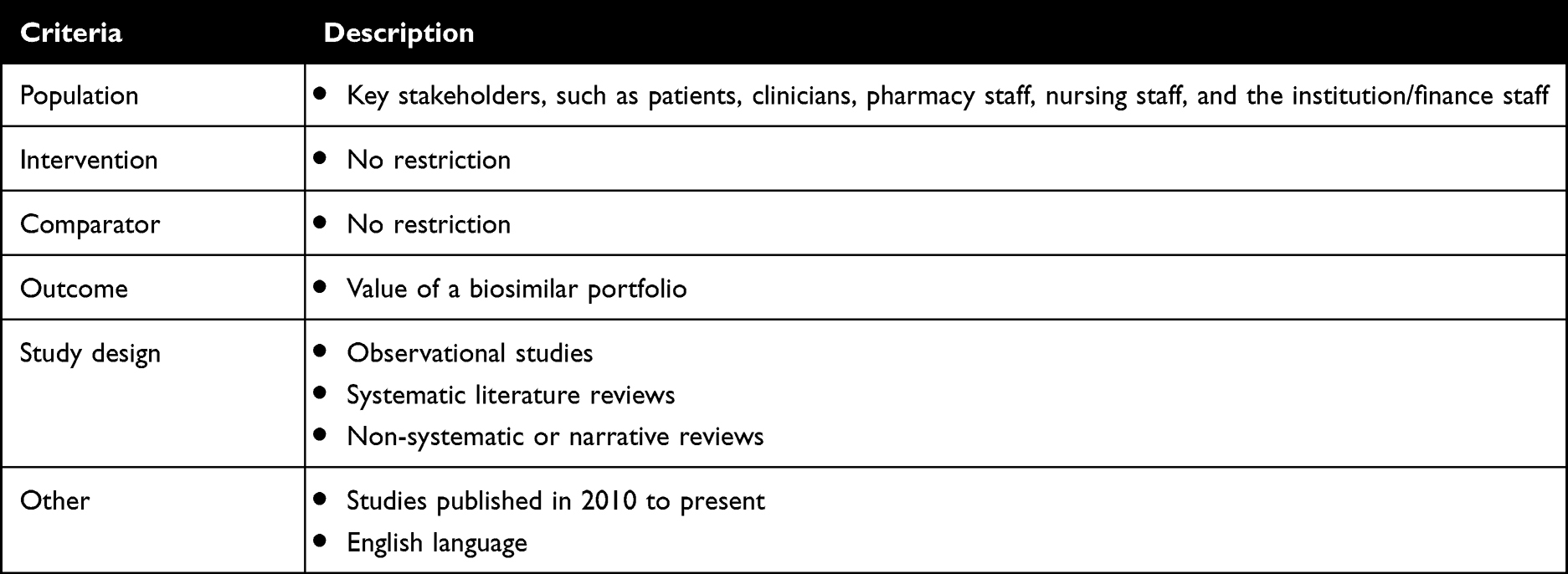 |
Table 2 Eligibility Criteria |
One reviewer screened titles/abstracts for potentially eligible studies. Full-text publications corresponding to the included studies were then retrieved and screened by one reviewer. Themes related to the use and value of a biosimilar portfolio in decision-making by stakeholders were extracted by a single reviewer. No formal quality assessment was undertaken.
Apart from the literature, clinical experience and observation were used to identify additional themes.
Results
Integrative Literature Review
No specific studies investigating biosimilar portfolio value were identified in the peer-reviewed or grey literature (Figure 1). Since no studies were identified, we conducted a targeted literature review of the peer-reviewed and grey literature to find articles that discussed biosimilar process or cost. We searched for themes or economic factors in these articles that could form a basis for assessing biosimilar portfolio value.
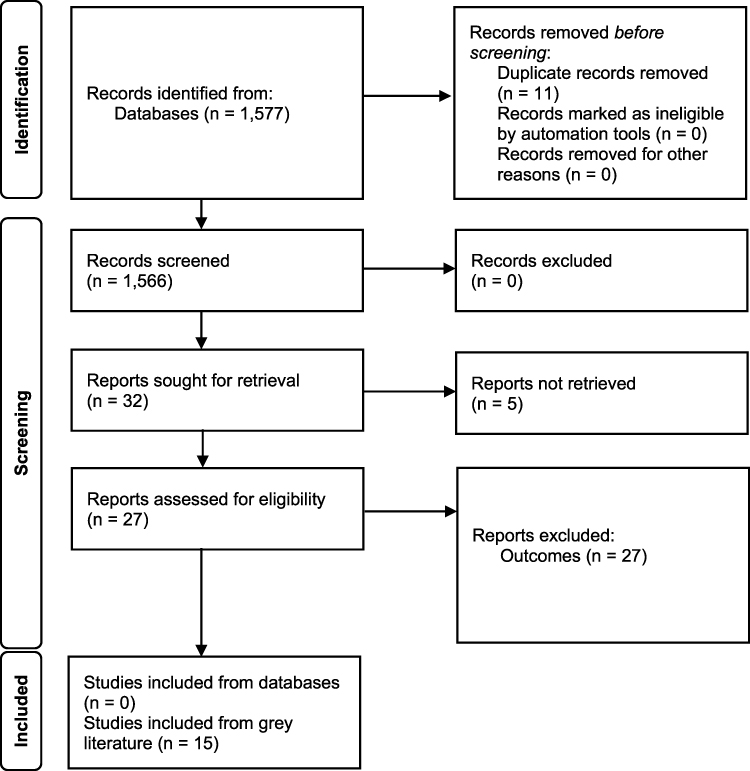 |
Figure 1 PRISMA flow diagram for study selection. |
This targeted literature review resulted in the identification of 15 studies from which several themes emerged. The following themes may help to define the clinical and economic value of a biosimilar portfolio:
- Manufacturing.
- Procurement, inventory, and storage.
- Administration.
- Education.
- Transaction costs.
Additionally, several non-pharmaceutical industry analogs were identified; namely, product line length and single-supplier versus multiple-supplier procurement. Several potential topics based on clinical experience and observation were also identified: Science credibility and research.
Some of the identified themes may also be differentiators in biosimilar portfolio value and are described below.
Manufacturing
Processing and packing biosimilars presents a challenge for manufacturers. Biosimilars are produced in cell lines with multiple purification and production stages.12 Given this innate complexity, modest changes in the manufacturing process can disrupt the final structure and function of biosimilars and ultimately impact interchangeability with the reference product.12
Further, drug shortages are not uncommon.13 Clinicians and pharmacy staff may develop a preference for biosimilars from reliable manufacturers owing to the low likelihood of supply disruptions, positive history regarding recalls, safe handling practices, supply chain security, and counterfeit protection.14–17 For these reasons, there may be clinical value that is realized by clinicians and clinical and economic value that is realized by pharmacy staff.
Procurement, Inventory, and Storage
There are challenges for end users (eg, institutions and clinical staff) associated with managing multiple brands, and mistakes can be costly.18 Across biosimilars, there could be differences in packaging, shelf life, etc. between a biosimilar and its reference product. In the US, many health plans may differ on the preferred biosimilar brand. Administration of the wrong brand of biosimilar may result in non-payment from the health plan. Thus, the institution/finance staff would absorb the cost of the biosimilar.
Administration
Patients, pharmacy staff, and nursing staff may develop preferences for differentiated forms of delivery (eg, intravenous versus subcutaneous).19–21 Further, the timing of administration or patient experience may impact the preferences of these stakeholders.
Oncology biosimilars are considered “look alike, sound alike” medications; thus, minimizing medication errors is essential.22 Thus, patients, pharmacy staff, and nursing staff may realize clinical and economic value associated with a biosimilar portfolio, as it may reduce resources associated with administration. Economic value may also be realized by the institution/finance staff.
Education
Educating patients, clinicians, pharmacy staff, and nursing staff on biosimilars is resource-intensive.23 Through the use of a biosimilar portfolio, educational materials from the manufacturer may be shared across stakeholders, reducing resource use associated with internally collating and managing this knowledge. This may manifest as clinical value to patients, clinicians, pharmacy staff, and nursing staff while providing economic value to pharmacy staff, nursing staff, and the institution/finance staff.
Transaction Costs
Both patients and the institution/finance staff incur costs associated with switching from a reference product to a biosimilar or from one biosimilar to another.24 The economic value of a biosimilar portfolio may be realized when patients can switch products without changing manufacturers. This may be related to resources saved associated with the billing, coding, and reimbursement process.
A biosimilar portfolio may also provide value related to reimbursement support and other programs, such as product replacement, co-pay assistance, and insurance denial support. The manufacturer of the biosimilar portfolio may serve as a single, reliable source for patients and the institution/finance; thus, removing the need for resources associated with contacting multiple manufacturers.
Potential Topics Based on Observation but Lacking Literature Support
Science Credibility
Science credibility may be assigned to manufacturers based on innovation or first-to-launch therapies.25 Manufacturers have a 6% market share advantage when introducing a novel product/treatment compared to companies that launch afterwards, thus there seems to be a reward for innovation.25 Moreover, companies with previous experience in a therapeutic area receive nearly twice the first-to-launch advantage relative to companies with no experience.25 Perceived science credibility may also be related to company size. For example, Pfizer’s COVID-19 vaccine was used more widely than Moderna’s COVID-19 vaccine, partially owing to greater commercial and manufacturing capabilities with Pfizer.26
It is possible that more science credibility may be assigned to companies with a biosimilar portfolio versus small companies with a single biosimilar, though no evidence has been published on this attribute. Manufacturers with a large portfolio in a therapeutic area may have greater credibility with stakeholders (eg, patients, clinicians, institutions) due to their volume of research in a therapeutic area compared to a small company with a single drug. This could manifest in stakeholder value based on reliability for support and breadth of therapeutic knowledge when contacting the manufacturer with a biosimilar portfolio.
Research
Manufacturers with biosimilar portfolios may have larger and sustained funding for research in a therapeutic area for clinical and investigator-initiated trials. For institutions or organization that drive revenue through clinical research, a manufacturer with a biosimilar portfolio may provide more confidence financially in sustaining their research business and simplify procedures in contracting for the research business.
Non-Pharmaceutical Industry Analogs
Product Line Length
Work by Berger et al suggests that product line length can positively affect brand choice by influencing perceived brand quality.27 The authors argued that companies with a wider variety of compatible products are generally perceived as having greater category experience, thereby increasing perceived quality and purchase likelihood. Thus, biosimilar portfolios may provide value relative to single biosimilar agents through greater brand quality associated with product line length.
Single-Supplier versus Multiple-Supplier Procurement
Work by Costantino et al outlined differences between single-supplier and multi-supplier procurement.28 Advantages of single-supplier procurement included collaboration, shared benefits, and long-term relationships. In the context of a biosimilar portfolio, this may manifest as high levels of trust between the manufacturer and stakeholders.
The authors also noted that multiple-supplier procurement is associated with greater costs related to the management of more than one supplier and loss of scale economies. Thus, biosimilar portfolios may provide economic value owing to reduced supply management costs, as described above in the Manufacturing theme.
Discussion
Hypothetical Value of Biosimilar Portfolio
Based on the themes that emerged from the methods used in this integrative literature review, we hypothesize that many stakeholders may realize clinical and/or economic value associated with a biosimilar portfolio according to their role (Figure 2). Specifically, the value of a biosimilar portfolio to patients and clinicians/healthcare personnel may be related to favorable administration through enhanced devices, patient education supporting shared decision-making on treatment of the patient’s disease, transaction costs as biosimilars generate lower overall cost of therapy. Companies with biosimilar portfolios may be nationally recognized by the patients and healthcare staff which may enhance their perception of rigorous clinical research behind the biosimilar development and the science credibility of the manufacturer.
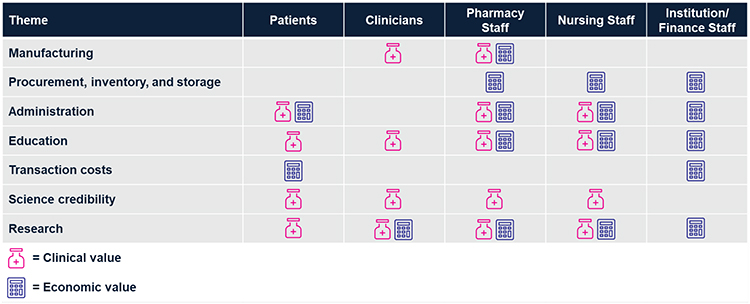 |
Figure 2 Hypothetical biosimilar portfolio value to specific stakeholders. |
Apart from the value described above, additional value of a biosimilar portfolio to pharmacists and institution/finance staff might be realized in less time involved in the procurement, inventory management, and storage with biosimilars with better stability. In addition, companies with a portfolio likely will have larger budgets to support clinical research for clinical sites involved in clinical research, providing more security and value in sustaining this revenue stream for the institution and staff.
Potential Drawbacks of Biosimilar Portfolio
While the themes from the literature and other sources suggest value associated with a biosimilar portfolio, there are potentially some negative aspects. In a targeted literature review and survey on US outcomes-based risk-sharing agreements (OBRSA), Goodman et al suggest that portfolios may enable unfavorable drug selection.29 This may occur when a drug offered in an OBRSA outperforms another in the same indication. With a biosimilar portfolio, it is less likely that an OBRSA is needed for originators since biosimilars have equivalent efficacy; thus, they will take the vast majority of the market share saving institutions a substantial amount.
However, new products launched in the same therapeutic area of the biosimilar portfolio may be more likely to be required to have an OBRSA. New products generally have substantially higher prices, which makes it difficult to show incremental cost-effectiveness benefit when compared to a biosimilar due to the lower cost of biosimilars. Thus, payers will likely require an OBRSA for new competitive products.
While single-supplier procurement can be advantageous, there are inherent risks involved with this practice related to greater dependency on the supplier and increased vulnerability to supply chain disruption.28 These risks may be mitigated by sourcing from dependable manufacturers with a history of minimal supply disruptions.
Policy/Managerial Implications
As previously stated, this framework was developed to assess biosimilar portfolio beyond cost savings between originator and biosimilar. Policies that shift utilization of biosimilars first in the treatment of an illness may be affected if not considering the elements in the value framework. For example, there may be inherent risk in policies that list one preferred biosimilar brand from a company that does not have a portfolio due to increase supply interruptions. In this situation, a second biosimilar may need to be added as a preferred option which may negatively impact the negotiated price leading to extra staff time in managing supply shortages, procurement time in negotiations, and potential increase for errors.
In institutions that generated part of their revenue and profit from clinical research may find adverse effects if they only drive selection of preferred biosimilars based on cost savings. Presumably, companies without a biosimilar portfolio may have less to no funding committed for research for innovative therapies. Selecting companies without a biosimilar portfolio may have adverse effects on the clinical research revenue generated.
Strengths and Limitations
This integrative literature review employed sensitive searches of peer-reviewed literature as well as extensive searches of grey literature. However, similar to all literature reviews, there is a risk that relevant studies published before 2010 and after May 2022 may not have been captured.
A defining weakness of this integrative literature review is the paucity of studies reporting on the value of a biosimilar portfolio. However, themes from the literature emerged that were formed into a conceptual framework.
Hypothetical Conceptual Framework
To our knowledge, this is the first study to systematically assess and create a framework for biosimilar portfolio value from the perspective of the pharmaceutical industry. While the integrative literature review identified no studies assessing the value of a biosimilar portfolio to stakeholders, seven themes emerged that might inform the value of a biosimilar portfolio. As shown in Figure 3, these themes have been integrated into an overarching framework that could be used to empirically test the clinical and economic value of a biosimilar portfolio.
 |
Figure 3 Hypothetical conceptual framework for composition of biosimilar portfolio value. |
Validation and Future Research
The conceptual framework described here creates a basis for validating the elements through future research efforts. For example, a stakeholder survey could help to quantify the clinical and economic benefit of a biosimilar portfolio by key stakeholders in institutions (patients, clinicians, pharmacy staff, nursing staff, and the institution/finance staff). It may be possible that new themes may emerge with a stakeholder survey and that some of the hypothetical themes may be deemed non-essential in describing biosimilar portfolio value. Additionally, it would be of interest to complete the survey across countries and regions given intrinsic differences in healthcare systems.
Conclusion
This is the first study to assess and create a framework for biosimilar portfolio value from the perspective of the pharmaceutical industry and affected stakeholders. Our findings suggest that the concept of biosimilar portfolio value is multi-faceted and literature on this topic to date has been limited to singular elements of value and not comprehensive value.
Potential themes have emerged in the literature to describe the value of a biosimilar portfolio. The conceptual framework described here may form a basis to help quantify the clinical and economic benefit of a biosimilar portfolio through further research.
Acknowledgments
This manuscript has been partially presented at ISPOR 2024 during May 5-8, 2024.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Concept and design: Fox, Bernauer, Stephens, Roth, Shelbaya.
Acquisition of data: Fox, Bernauer, Stephens, Jackson.
Analysis and interpretation of data: Fox, Bernauer, Stephens, Jackson, Roth.
Drafting of the manuscript: Fox, Stephens, Roth.
Critical revision of the paper for important intellectual content: Fox, Bernauer, Stephens, Jackson, Roth, Shelbaya.
Statistical analysis: None.
Provision of study materials or patients: None.
Obtaining funding: Fox, Bernauer, Stephens.
Administrative, technical, or logistic support: Fox, Bernauer, Stephens, Roth, Shelbaya
Supervision: Fox, Bernauer, Stephens, Roth, Shelbaya.
Funding
This study was funded by Pfizer Inc. The publication of study results was not contingent on the sponsor’s approval or censorship of the manuscript.
Disclosure
Grace E. Fox, Mark Bernauer, Jennifer Stephens, and Bianca Jackson are consultants for Pfizer Inc. and work for OPEN Health. Josh Roth and Ahmed Shelbaya are employees of and hold stock/stock options in Pfizer Inc. The authors report no other conflicts of interest in this work.
References
1. Wind J, Mahajan V. Designing product and business portfolio. Harvard Bus Rev. 1981;59:155–165.
2. Lafontaine F, Slade M. Franchising and exclusive distribution. In: The Oxford Handbook of International Antitrust Economics. Vol. 2. Oxford; 2014:387.
3. Bleys J, Coravos J, Fleming E, Quigley D. A new portfolio model for biotech. Available from: https://www.mckinsey.com/industries/life-sciences/our-insights/a-new-portfolio-model-for-biotech.
4. Sun L, Li S, Peng X. Should additional value elements be included in cost-effectiveness analysis in pharmacoeconomic evaluation: a novel commentary. Cost Eff Resour Alloc. 2023;21(1):79. doi:10.1186/s12962-023-00490-4
5. Daller J. Biosimilars: a consideration of the regulations in the United States and European Union. Regul Toxicol Pharmacol. 2016;76:199–208. doi:10.1016/j.yrtph.2015.12.013
6. U.S. Food & Drug Administration. Biosimilar product information. Available from: https://www.fda.gov/drugs/biosimilars/biosimilar-product-information.
7. European Medicines Agency. Search results. European Medicines Agency. Available from: https://www.ema.europa.eu/en/search?f%5B0%5D=ema_med_status%3A100108&f%5B1%5D=ema_medicine_bundle%3Aema_medicine&f%5B2%5D=ema_search_categories%3A83&f%5B3%5D=ema_search_topics%3A45&landing_from=73303.
8. IQVIA. Biosimilars in the United States 2020–2024. IQVIA; 2020. Available from: https://www.iqvia.com/insights/the-iqvia-institute/reports-and-publications/reports/biosimilars-in-the-united-states-2020-2024#:~:text=1%20Currently%2C%2013%25%20of%20biosimilar%20products%20in%20development,developed%20and%20launched%20by%20seven%20large%20pharma%20companies.
9. Wang A, Halbert RJ, Baerwaldt T, Nordyke RJ. US payer perspectives on evidence for formulary decision making. J Oncol Pract. 2012;8(3 Suppl):22s–7s. doi:10.1200/jop.2011.000526
10. Sendyona S, Odeyemi I, Maman K. Perceptions and factors affecting pharmaceutical market access: results from a literature review and survey of stakeholders in different settings. J Mark Access Health Policy. 2016;4. doi:10.3402/jmahp.v4.31660
11. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi:10.1136/bmj.b2535
12. Ramanan S, Grampp G. Drift, evolution, and divergence in biologics and biosimilars manufacturing. BioDrugs. 2014;28(4):363–372. doi:10.1007/s40259-014-0088-z
13. Shukar S, Zahoor F, Hayat K, et al. Drug shortage: causes, impact, and mitigation strategies. Front Pharmacol. 2021;12:693426. doi:10.3389/fphar.2021.693426
14. Blackstone EA, Joseph PF. The economics of biosimilars. Am Health Drug Benefits. 2013;6(8):469–478.
15. Griffith N, McBride A, Stevenson JG, Green L. Formulary selection criteria for biosimilars: considerations for US health-system pharmacists. Hosp Pharm. 2014;49(9):813–825. doi:10.1310/hpj4909-813
16. Jacoby R, Smith E, Wilkins D, Divya I, Peltre S. Winning with biosimilars Opportunities in global markets Available from: https://www2.deloitte.com/content/dam/Deloitte/us/Documents/life-sciences-health-care/us-lshc-biosimilars-whitepaper.pdf.
17. Pfizer. Biosimilar implementation: potential best practices and other considerations Available from: https://www.pfizerbiosimilars.com/images/sites/default/files/Downloadables/PP-BIO-USA-0624%20Leave-Behind_DIGITAL.pdf.
18. Pacific Business Group on Health. Biosimilar uptake: the physician perspective. Available from: https://www.pbgh.org/wp-content/uploads/2021/01/Biosimilars-from-the-physician-perspective-FINAL.pdf.
19. U.S. Pharmacist. Biosimilar IV and SC trastuzumab in clinical practice; 2022. Available from: https://www.uspharmacist.com/article/biosimilar-iv-and-sc-trastuzumab-in-clinical-practice.
20. Waller CF, Möbius J, Fuentes-Alburo A. Intravenous and subcutaneous formulations of trastuzumab, and trastuzumab biosimilars: implications for clinical practice. Br J Cancer. 2021;124(8):1346–1352. doi:10.1038/s41416-020-01255-z
21. Whitemore M. Future biosimilars: pros and cons. Available from: https://www.hemophiliafed.org/future-bisomilars-pros-and-cons/.
22. Garg M, Chatterjee A, Chambers CR. Education strategy for the implementation of oncology biosimilars essential for operational and patient safety in Alberta, Canada. J Oncol Pharm Pract. 2021;27(5):1189–1194. doi:10.1177/10781552211007535
23. Oskouei ST, Kusmierczyk AR. Biosimilar uptake: the importance of healthcare provider education. Pharmaceut Med. 2021;35(4):215–224. doi:10.1007/s40290-021-00396-7
24. Allocati E, Godman B, Gobbi M, Garattini S, Banzi R. Switching among biosimilars: a review of clinical evidence. Front Pharmacol. 2022;13:917814. doi:10.3389/fphar.2022.917814
25. Cha M, Yu F. Pharma’s first-to-market advantage. McKinsey and Company. Available from: https://www.mckinsey.com/industries/life-sciences/our-insights/pharmas-first-to-market-advantage.
26. Hopkins JS, Uribe A. Pfizer-BioNTech Covid-19 vaccine is world’s preferred shot. The Wall Street Journal. Available from: https://www.wsj.com/articles/pfizer-biontech-covid-19-vaccine-is-worlds-preferred-shot-11633950181.
27. Berger J, Draganska M, Simonson I. The influence of product variety on brand perception and choice. Marketing Sci. 2007;26(4):460–472. doi:10.1287/mksc.1060.0253
28. Costantino N, Pellegrino R. Choosing between single and multiple sourcing based on supplier default risk: a real options approach. J Purchasing Supply Manage. 2010;16(1):27–40. doi:10.1016/j.pursup.2009.08.001
29. Goodman C, Villarivera C, Gregor K, van Bavel J. Regulatory, policy, and operational considerations for outcomes-based risk-sharing agreements in the U.S. market: opportunities for reform. J Manag Care Spec Pharm. 2019;25(11):1174–1181. doi:10.18553/jmcp.2019.19167
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.