Back to Journals » Risk Management and Healthcare Policy » Volume 19
Climate Extremes and Healthcare Access: Assessing the Impact of Severe Weather Events on Emergency Motorcycle Ambulance Availability
Authors Apiratwarakul K ![]() , Cheung LW, Pearkao C
, Cheung LW, Pearkao C ![]() , Gaysonsiri D
, Gaysonsiri D ![]() , Ienghong K
, Ienghong K ![]()
Received 7 October 2025
Accepted for publication 26 February 2026
Published 4 March 2026 Volume 2026:19 572604
DOI https://doi.org/10.2147/RMHP.S572604
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Keon-Hyung Lee
Korakot Apiratwarakul,1 Lap Woon Cheung,2,3 Chatkhane Pearkao,4 Dhanu Gaysonsiri,5 Kamonwon Ienghong1
1Department of Emergency Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 2Accident & Emergency Department, Princess Margaret Hospital, Kowloon, Hong Kong, People’s Republic of China; 3Department of Emergency Medicine, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Pokfulam, Hong Kong, People’s Republic of China; 4Department of Adult Nursing, Faculty of Nursing, Khon Kaen University, Khon Kaen, Thailand; 5Department of Pharmacology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
Correspondence: Kamonwon Ienghong, Department of Emergency Medicine, Faculty of Medicine, Khon Kaen University, 123 Mittraphap Road, Mueang Khon Kaen District, Khon Kaen, 40002, Thailand, Tel +66 43 366 869, Fax +66 43 366 870, Email [email protected]
Purpose: Climate extremes are a catastrophic manifestation of climate change. Motorcycle ambulances are an emerging sort of vehicle that is intended to offer quick access in large cities. This study evaluated the effect of extreme weather events on the accessibility of emergency motorcycle ambulance services.
Patients and Methods: We conducted a retrospective analysis of motorcycle ambulance operation data from January 2020 to December 2024. Data on motorcycle ambulance operating times, rainfall levels in the operational area, and ground temperatures at the Emergency medical services (EMS) unit were collected. Continuous data were presented as means and standard deviations (SD), while categorical data were reported as frequencies and percentages. Associations between categorical variables were evaluated using the chi-square test. A two-tailed p-value of less than 0.05 was considered statistically significant.
Results: With a total of 569 operations documented over the five years, services were postponed during rainy weather and when ground temperatures exceeded 40°C. The availability of operational motorcycle ambulances declined from 81.28% to 34.03%. Increased rainfall (hours lost increased from 1065.1 to 2711.7; p< 0.001) and rising temperatures exceeding 40°C (hours lost increased from 574.9 to 3067.3; p< 0.001) were the main causes of service interruptions. This occurred despite increased utilization of motorcycle ambulances for emergency responses (65 to 165 operations annually; p=0.022) and a growing use of AED-equipped units for cardiac emergencies (4.6% to 23.6% of operations; p=0.014).
Conclusion: This quantitative evidence of the impact of climate extremes on emergency healthcare access due to reduced motorcycle ambulance availability. The gradual reduction in operational hours was caused by rising rainfall and elevated temperatures.
Keywords: climate change, emergency medical services, global warming, health policy, motorlance
Introduction
Today, the term “global warming” is commonly used to describe the increase in the Earth’s average surface temperature. Previous studies have shown that most of the problems stem from human activities that emit gases degrading the atmosphere and increasing the amount of sunlight that reaches the Earth’s surface.1–3 As a result, surface temperatures rise.
Global warming significantly impacts climate change, particularly through variations in temperature, rainfall, and sea levels.4–7 These changes have led to increased occurrences of mudslides, floods, and emerging infectious diseases. In relation to the four fundamentals of human existence: food, clothing, shelter, and health. The climate change has caused a decline in agricultural and livestock production,8,9 and clothing and textile manufacturing has fallen short of expectations. Residential areas have been impacted by particular natural disasters,10 and the utilization of pharmaceuticals for illness treatment is growing.
Climate change has resulted in significant deviations from typical weather patterns, which are a devastating consequence of climate extremes. Changes like these impact the welfare of humans, plants, and wildlife.11,12 Heatwaves in certain areas lead to a significant increase in temperatures beyond seasonal regulations, resulting in heat-related injuries and fatalities over sustained durations. During such events, most countries in the Northern Hemisphere typically experience elevated temperatures compared to their Southern counterparts. These transformations significantly impact livelihoods, modifying economies, public health, and societies as a whole. In equatorial regions characterized by tropical climates, heatwaves may seriously disrupt outdoor activities and elevate the risk of life-threatening conditions. Moreover, climatic extremes have caused heightened precipitation, leading to catastrophic floods and mudslides that profoundly disrupt individuals’ livelihoods.
In the area of public health systems, emergency medical services (EMS) are a critical frontline component of healthcare delivery and disaster response, yet they are particularly vulnerable to weather extremes. Changes in climatic conditions can both increase emergency caseloads and impede EMS mobility and availability, undermining timely access to life‑saving care. In Thailand, emergency patients can access EMS by calling 1669, a toll-free number available 24 hours a day and covering all areas of the country.13–15 Various modes of transportation are used, including air, land, and sea vehicles. Emergency motorcycle ambulances are one of the key vehicles used to reach patients quickly, allowing for initial assessment and treatment.16,17 Since these motorcycles are outfitted with automated external defibrillators (AEDs), resuscitation efforts can start as soon as they arrive in situations like out-of-hospital cardiac arrest. Modern emergency vehicles are especially beneficial in regions with significant traffic congestion, where patient access is frequently hindered. While motorcycle ambulances improve access under normal conditions, their small size and exposure to the elements make them susceptible to weather‑related operational constraints. During heavy rain or flooding, emergency motorcycles cannot be deployed. Likewise, extremely high temperatures that make outdoor driving unsafe can restrict operating hours.
Although motorcycle ambulances are increasingly utilized in low- and middle-income countries, there is insufficient scientific proof quantifying the impact of extreme weather, particularly heavy rainfall and extreme heat—on their operational availability and, consequently, access to emergency care.16–18 Understanding the climatological factors influencing EMS unavailability is crucial for risk management, resource allocation, and formulating adaptive policies that ensure the continuity of emergency care regardless of increasingly inconsistent weather conditions. Assessing service disruptions linked to particular weather thresholds may inform institutional protocols, workforce protections, vehicle design modifications, and contingency planning for alternative dispatch strategies during anticipated extreme heat or rainfall events. The primary objective of this study was to measure the effect of extreme climate events on the accessibility of emergency motorcycle ambulance services, potentially offering insights to inform EMS risk-management strategies and policy interventions to ensure emergency access amid increasing climate risks.
Materials and Methods
This retrospective observational study analyzed EMS operational and meteorological data from the EMS unit of Srinagarind Hospital in Thailand. The hospital, affiliated with a university and performing over 2200 EMS operations annually, serves as the primary training center for emergency physicians and EMS personnel in the region. The EMS division, managed by a dispatch center, oversees six van ambulances, two motorcycle ambulances, and a telemedicine service that provides 24-hour online medical directions. Each motorcycle ambulance is staffed by a two-person crew, consisting of an emergency physician and an emergency medical technician.
All motorcycle ambulance operations conducted by the EMS unit from January 2020 to December 2024 were included in this evaluation. To ensure consistency in annual comparisons, each year was standardized to 365 days. As a result, February 29, 2020, and February 29, 2024, were excluded from the study period.
Data Collection
The motorcycle ambulance (Figure 1) was a modified Honda New Forza 300 model (Honda Motor Company, Ltd.; Tokyo, Japan). The vehicle measures 75.30 centimeters in width, 216.60 centimeters in length, 118.90 centimeters in height, with a seat height of 71.60 centimeters and a ground clearance of 13.90 centimeters. It has a net weight of 192 kilograms. Three equipment boxes were mounted, behind the passenger seat, on the left and right sides of the vehicle, and at the rear. The AED device was securely stored in a side-mounted box for easy access. Additional features included emergency sirens, radio communication, and reflective stickers to enhance safety during operation.
 |
Figure 1 Motorcycle ambulance. |
Data on motorcycle ambulance operating times including activation time (minute), response time (minute), operation shifts (morning, afternoon, and night shifts) were collected using EMS record form. The total number of hours of rainfall in the operational area and the hours during which ground temperatures exceeded 40 degrees Celsius at the EMS unit were recorded. Three emergency physicians, each with over five years of EMS experience, monitored and analyzed EMS intervals for motorcycle ambulances recorded in the hospital’s EMS database. Rainy weather conditions were documented using closed-circuit television (CCTV) located in the motorcycle ambulance parking area, along with data from the Thai Meteorological Department (Khon Kaen, Thailand).
The operational protocol for motorcycle ambulance deployment enforced a zero-tolerance policy regarding precipitation throughout the study period. Service suspension was automatically initiated upon confirmation of any active rainfall within the operational area, as validated by either CCTV footage or meteorological reports. Consequently, precipitation was examined categorically (Presence/Absence), excluding significant stratification by rainfall intensity.
Ground temperature was measured at the front of the emergency department using a Wet Bulb Globe Temperature (WBGT) device, which has a measurement range of 10–50°C, a resolution of 0.1°C, and an accuracy of ±2°C. Currently, there is no legislation in Thailand governing outdoor work standards for EMS personnel, including temperature thresholds or duration.
The critical threshold for high-temperature suspension was established at ground temperatures above 40°C. This threshold was not determined by general climatological metrics but was directly derived from institutional safety regulations. This temperature denotes the maximum threshold advised for maintaining the long-term operational integrity of the portable Automated External Defibrillator (AED) units on motorcycles, consistent with safety protocols regarding occupational heat stress for physically active individuals in full protective gear within high-humidity tropical settings.
Sample Size
While previous studies18,19 utilized similar sample sizes, we used an analysis of two samples with repeated measures20 with confirmed adequacy through a power analysis. Based on an estimated medium effect size (Cohen’s d = 0.5), an alpha of 0.05, and a power of 0.80, the minimum required sample was 340. Our final sample of 569 exceeds this threshold, ensuring sufficient statistical power.
Statistical Analysis
Statistical analysis was performed using IBM SPSS for Windows, version 27.0, licensed by Khon Kaen University (Khon Kaen, Thailand) (IBM Corp., Armonk, New York, USA). Continuous data were presented as means and standard deviations (SD), while categorical data were reported as frequencies and percentages. Associations between categorical variables were evaluated using the chi-square test. A two-tailed p-value of less than 0.05 was considered statistically significant.
Results
With a total of 569 operations documented over the five years, Table 1 summarizes the features of motorcycle ambulance operations. The number of operations increased significantly from 65 cases (11.4%) in 2020 to 165 cases (29.0%) in 2024 (p=0.022). The mean age of patients ranged from 30.8 to 36.2 years across the study period. Trauma cases represented the majority of operations throughout the five years, accounting for 50.7% to 61.5% of cases. Activation time and response time remained consistent over the study period. Use of AEDs showed a significant increase, rising from 4.6% of operations in 2020 to 23.6% in 2024 (p=0.014).
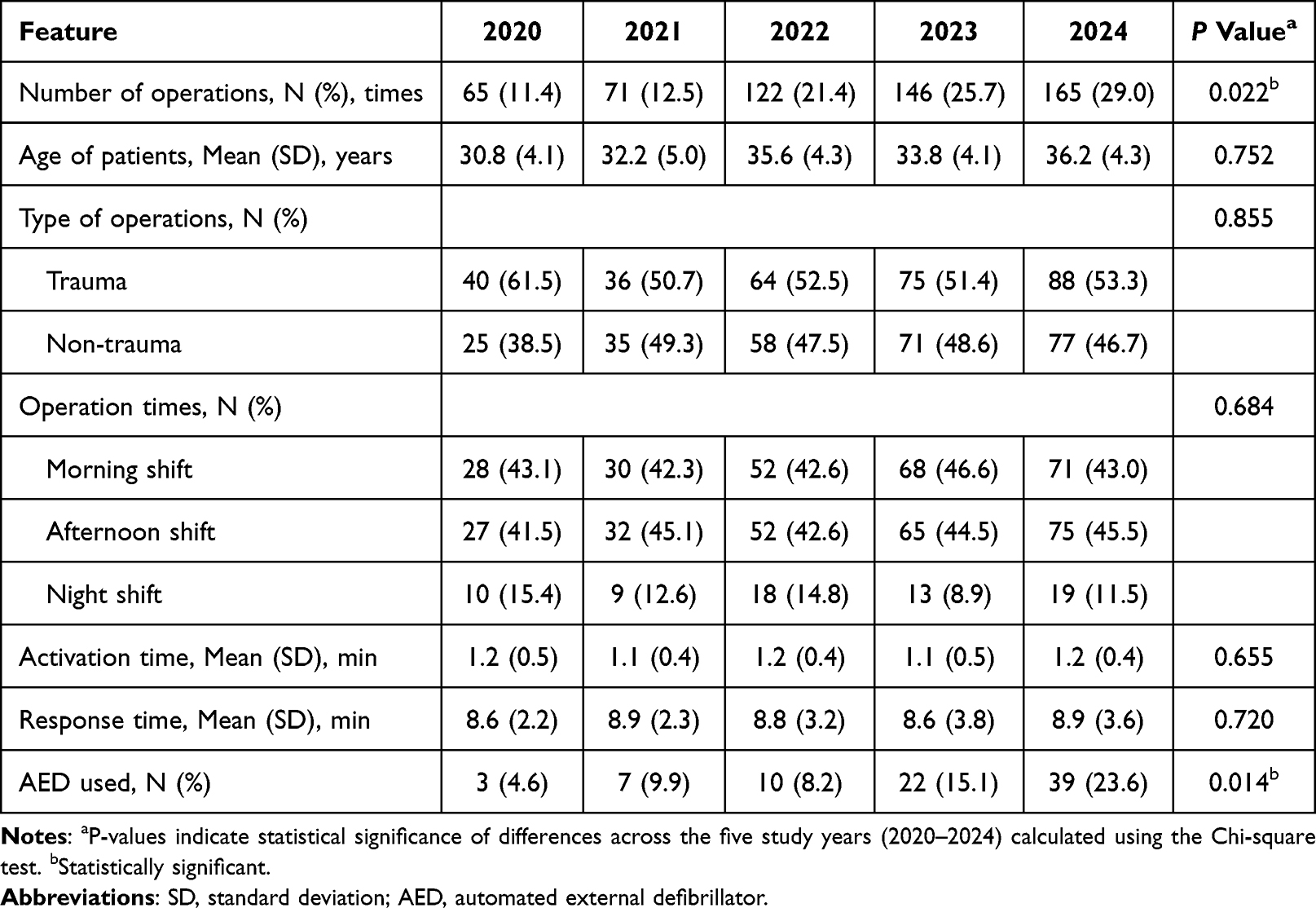 |
Table 1 Characteristics of Motorcycle Ambulance Operation (N=569) |
During the five-year period, motorcycle ambulance operational availability decreased to 47.25% (Table 2), with the biggest decline of 28.89% occurring between the years 2022 and 2023. The two primary factors contributing to the increasing unavailability were rainy weather, resulting in a rise in lost operating hours from 1065.1 hours in 2020 to 2711.7 hours in 2024 (p<0.001), and high temperatures, with hours lost due to heat increasing from 574.9 hours in 2020 to 3067.3 hours in 2024 (p<0.001).
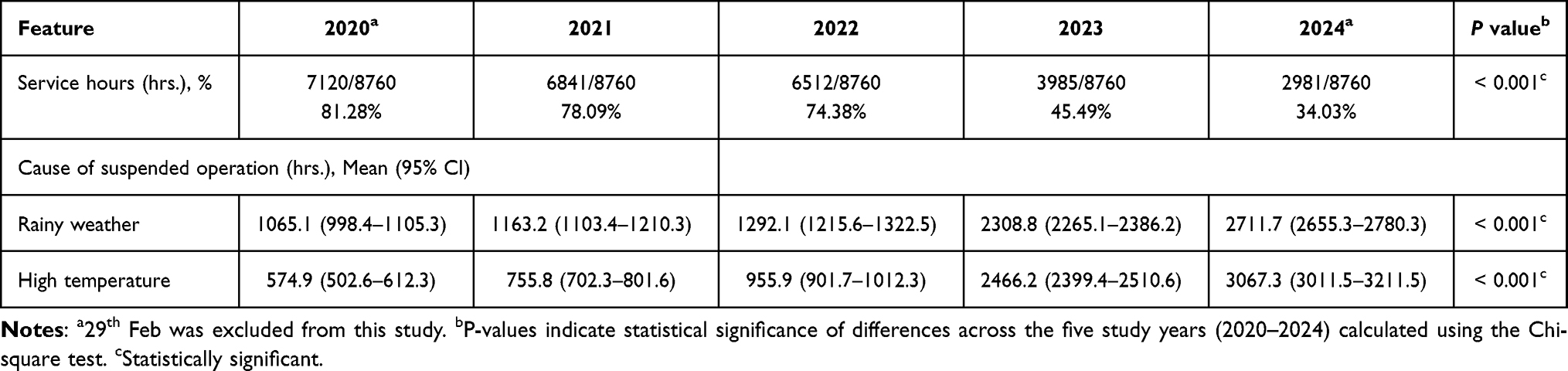 |
Table 2 Motorcycle Ambulances Operations |
Figure 2 represents the monthly rainfall hours over the five-year period from 2020 to 2024. According to the data, there has been a steady increase in rainfall hours starting in January, reaching a peak in August, and then progressively decreasing through December. In August of 2024, the highest peak was notable, with more than 400 hours of rainfall. Subsequent years, including 2022 and 2023, demonstrated a comparable seasonal pattern but displayed less pronounced peaks relative to 2024.
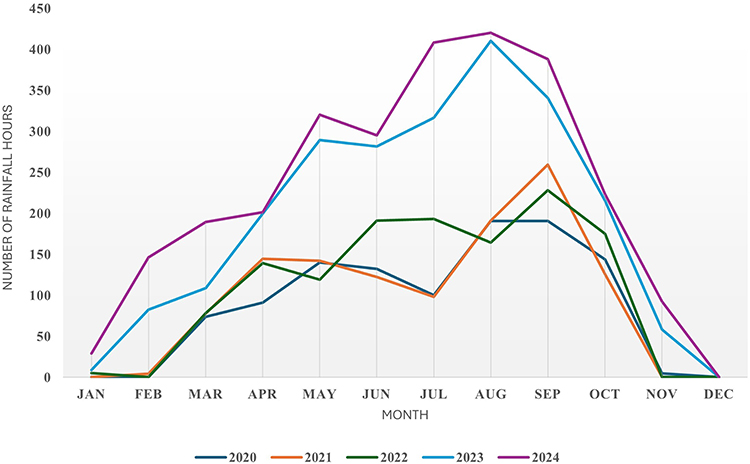 |
Figure 2 Number of hours of rainfall per month over a 5-year period (hrs.). |
Figure 3 illustrates the hours during which temperatures exceeded 40°C across different months from 2020 to 2024. March through July, which is when the summer season in this area occurs, experienced the highest hours of high temperatures. With the highest recorded in April 2024, at around 1700 hours, the data show an increasing trend in high-temperature hours over time. No hours with temperatures higher than 40°C were observed between September and December.
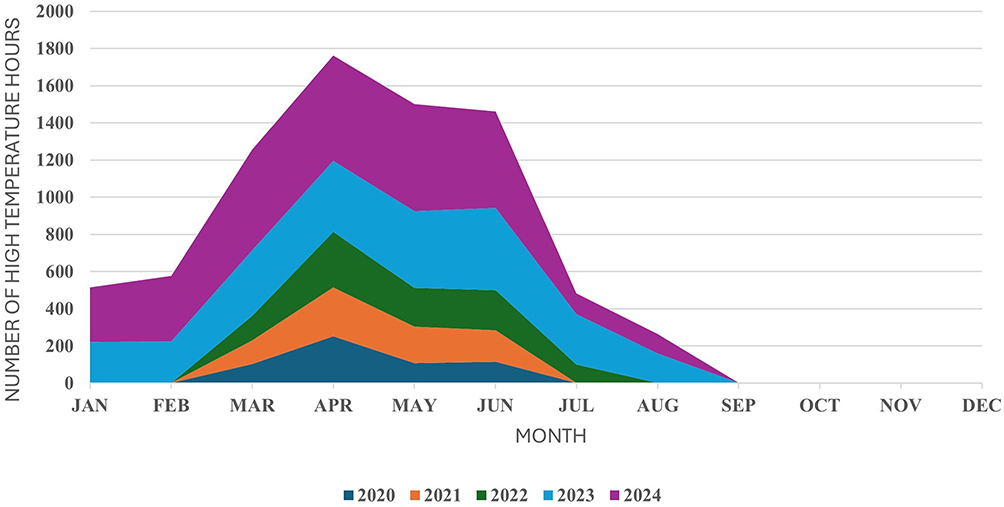 |
Figure 3 Number of hours of high temperature (> 40°C) over a 5-year period (hrs.). |
Discussion
This study provides compelling evidence of the significant impact climate extremes have on emergency healthcare access, particularly through the availability of motorcycle ambulance services. Over the five-year period examined (2020–2024), a notable decline in the operational availability of motorcycle ambulances was observed, dropping from 81.28% in 2020 to just 34.03% in 2024, a 47.25% reduction in service availability.
The study clearly demonstrates that two climate-related factors are primarily responsible for this concerning trend, increased rainfall and rising temperatures.18,19,21–23 Hours lost due to rainy weather rose significantly from 1065.1 hours in 2020 to 2711.7 hours in 2024, while hours lost due to high temperatures (>40°C) increased more than fivefold, from 574.9 hours in 2020 to 3067.3 hours in 2024.
The seasonal patterns observed in our data are consistent with climate change projections for tropical regions.24–26 Rainfall intensity increased during the monsoon season, peaking in August, with 2024 showing an unprecedented more than 400 hours of rainfall in that month alone. Similarly, high-temperature hours followed an upward trend from March to July, with April 2024 recording approximately 1700 hours above 40°C, exceeding the threshold at which motorcycle ambulance operations must be suspended for safety reasons and prevent heat-related illness.27–31 The gradual decrease in operational hours presents a substantial risk to emergency healthcare accessibility,32,33 particularly in regions where motorcycle ambulances function as essential first responders.
The consequences for the provision of emergency medical care are significant. Climate-imposed restrictions pose a threat to the growing use of motorcycle ambulances for emergency response, which increased from 65 operations in 2020 to 165 in 2024. The increasing utilization of motorcycle ambulances equipped with AEDs for cardiac emergencies is particularly alarming, rising from 4.6% of operations in 2020 to 23.6% in 2024. As climate extremes further limit service availability, the timely delivery of life-saving interventions for cardiac arrest patients may be jeopardized.34,35
The findings suggest that the current motorcycle ambulance model is becoming increasingly unsustainable under conditions of extreme weather. In the absence of adaptation, we anticipate that operational availability may decline to below 30% by 2025, resulting in significant deficiencies in emergency response capabilities, particularly during the peak heat months (March to July) and the monsoon season (July to October).
Our findings highlight the urgent need for climate-adaptive strategies in emergency medical services. Several approaches warrant consideration including (1) Regarding operational and dispatch policy, in order to minimize this risk, EMS systems should transition from basic binary suspension rules to complex, risk-based operational protocols linked to objective meteorological and road condition metrics (such as rainfall intensity, waterlogging) and anticipated duration. This approach facilitates partial deployment with adjusted mission profiles under moderate risk—shorter durations, closer coverage, and restricted mission types, while ensuring safety. Dynamic dispatch that integrates real-time weather data and road conditions can optimize motorcycle ambulances for the most time-sensitive and advantageous missions when feasible and automatically transition to alternative transport methods when necessary. Implementation of complementary emergency response vehicles that can operate effectively during extreme weather conditions, such as Tuk Tuks (three-wheeled vehicles). (2) Automobile design and equipment modifications, enhancing the safe operating parameters of motorcycle ambulances will likely necessitate both incremental modifications and more significant design alterations. Development of motorcycle ambulances equipped with enhanced cooling systems for operators and weather-protective enclosures that maintain maneuverability while providing protection from rainfall. Operator protection measures—ventilated helmets, cooling vests, shade canopies, are equally crucial, as is maintaining the functionality of medical equipment in adverse conditions. Every adaptation must undergo evaluation for safety, response time considerations, and maintenance needs prior to scaling up. (3) Workforce protection and training, safeguarding EMS personnel is an ethical obligation and a practical requirement for service continuity. Emergency Medical Services organizations should implement evidence-based occupational standards for extreme heat and precipitation, defining work/rest cycles, hydration protocols, mandatory breaks, and exposure limits. Specialized training needs to prepare crews for secure operation in wet or inundated environments, identification and management of heat-related illnesses, and adjusted patient-handling protocols when complete transport is impractical. Organizational support, encompassing mental health resources and explicit policies for shift modifications during extended weather disruptions, will alleviate operational stress and burnout among frontline personnel.
A critical consideration when interpreting the trends observed across the 2020–2024 study period is the unprecedented disruption caused by the global COVID-19 pandemic. As our data collection substantially overlaps with peak pandemic mobilization and subsequent recovery phases, the influence of public health mandates and behavioral shifts on operational metrics must be explicitly acknowledged. In the early stages of the pandemic (2020–2021), we noted considerable divergences from the typical inter-annual trends, especially concerning total call volume and service delivery latency. This is likely due to consecutive nationwide movement restrictions, which directly restricted public mobility and, as a result, decreased accident and emergency rates necessitating ambulance deployment. Moreover, changes in public health priorities and the reallocation of resources within the broader EMS framework may have temporarily affected the prioritization or deployment schedules of our motorcycle ambulance units, regardless of environmental factors such as extreme heat or heavy rainfall.
Various limitations require being recognized. This was a single-center study, potentially constraining the generalizability of our findings. The possible impact of neighboring weather patterns constitutes an additional geographical factor that may be examined in multi-center studies. The main constraint of this study is the dependence on precipitation data obtained from designated, stationary sites (the hospital grounds and the Thai Meteorological Department station in Khon Kaen). Precipitation displays considerable spatial variability; thus, the documented total rainfall hours may not accurately represent the actual weather conditions throughout the entire operational area served by the motorcycle ambulances. Although we employed data sources near the main response hub, it is conceivable that regions at the periphery of our service radius encountered varying precipitation intensities or timings, possibly resulting in an inaccurate assessment of the overall impact on service accessibility throughout the entire geographical area. Furthermore, our definition of operational unavailability was predicated on institutional protocols, specifically halting of services during rainfall or when temperatures over 40°C, rather than on real-world information from actual service attempts. Finally, the study did not assess the direct clinical consequences of the unavailability of motorcycle ambulances on patient outcomes, an issue that necessitates additional investigation. Future research should utilize mixed-method approaches, integrating quantitative data with qualitative interviews of EMS operators, to comprehensively define the decision-making processes during marginal weather conditions. Furthermore, comparative analyses with alternative tropical EMS systems are necessary to ascertain whether the thresholds established above (suspension at >40°C or any precipitation) are universally applicable or necessitate context-specific modifications.
Conclusion
Our study offers statistical evidence of the significant influence that climate extremes have on emergency medical access due to the unavailability of motorcycle ambulances. The delivery of emergency medical services is seriously and increasingly threatened by the gradual reduction in operating hours over the course of the five-year study period, which is being caused by rising temperatures and rainfall. As climate change increases, it is crucial for emergency healthcare systems to embrace adaptive strategies for guaranteeing service continuity during extreme weather events. A combination of short‑term operational changes (tiered dispatch, forecast‑driven pre‑positioning, and alternative asset deployment), medium‑term investments in vehicle and equipment adaptations, and long‑term policy actions (occupational standards, dedicated financing, and cross‑sector planning) will be required to sustain equitable emergency access as climate extremes intensify.
Abbreviations
ED, emergency department; EMS, emergency medical services; AEDs, automated external defibrillators; CCTV, closed-circuit television; WBGT, Wet Bulb Globe Temperature; SD, standard deviations.
Data Sharing Statement
As the data include information that could compromise patient anonymity, the datasets analyzed in this study are not publicly available. However, they may be obtained from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The Khon Kaen University Ethics Committee for Human Research approved the study, which was conducted in accordance with the Declaration of Helsinki and the ICH Good Clinical Practice Guidelines (HE681041). Informed consent was not required. All identifying information was removed from the collected data to ensure confidentiality.
Acknowledgments
The authors would like to express their sincere gratitude to Josh Macknick for serving as an English consultant.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Fundamental Fund of Khon Kaen University, which received funding support from the National Science, Research, and Innovation Fund (NSRF).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Varela R, de Castro M, Dias JM, Gómez‑Gesteira M. Coastal warming under climate change: global, faster and heterogeneous. Sci Total Environ. 2023;886:164029. doi:10.1016/j.scitotenv.2023.164029
2. Slingo JM, Slingo ME. The science of climate change and the effect of anaesthetic gas emissions. Anaesthesia. 2024;79:252–9. doi:10.1111/anae.16189
3. Ren C, Zhang X, Reis S, et al. Climate change unequally affects nitrogen use and losses in global croplands. Nat Food. 2023;4:294–304. doi:10.1038/s43016-023-00730-z
4. Rijal M, Luo P, Mishra BK, Zhou M, Wang X. Global systematical and comprehensive overview of mountainous flood risk under climate change and human activities. Sci Total Environ. 2024;941:173672. doi:10.1016/j.scitotenv.2024.173672
5. Munz L, Mosimann M, Kauzlaric M, Martius O, Zischg AP. Storylines of extreme precipitation events and flood impacts in alpine and pre-alpine environments under various global warming levels. Sci Total Environ. 2024;957:177791. doi:10.1016/j.scitotenv.2024.177791
6. Romanello M, Walawender M, Hsu SC, et al. The 2024 report of the Lancet Countdown on health and climate change: facing record-breaking threats from delayed action. Lancet. 2024;404:1847–1896. doi:10.1016/S0140-6736(24)01822-1
7. Churchill LR, Henderson GE, King NMP. Why climate literacy is health literacy. AMA J Ethics. 2024;26:E147–E152. doi:10.1001/amajethics.2024.147
8. Godde CM, Mason-D’Croz D, Mayberry DE, Thornton PK, Herrero M. Impacts of climate change on the livestock food supply chain; a review of the evidence. Glob Food Sec. 2021;28:100488. doi:10.1016/j.gfs.2020.100488
9. Ray DK, West PC, Clark M, Gerber JS, Prishchepov AV, Chatterjee S. Climate change has likely already affected global food production. PLoS One. 2019;14(5):e0217148. doi:10.1371/journal.pone.0217148
10. Hochrainer-Stigler S, Laurien F, Velev S, Keating A, Mechler R. Standardized disaster and climate resilience grading: a global scale empirical analysis of community flood resilience. J Environ Manage. 2020;276:111332. doi:10.1016/j.jenvman.2020.111332
11. Ahmad QU, Moors E, Masih I, Shaheen N, Biemans H, Adnan M. The coincidence of climate extremes with sensitive crop growth phases: projected impact on sustainable crop water use and crop yield in the IGB river basins. Sci Total Environ. 2024;916:169680. doi:10.1016/j.scitotenv.2023.169680
12. Stamper AR, Mahmud AS, Nuzzo JR, Baker RE. Modeling the impact of climate extremes on seasonal influenza outbreaks across tropical and temperate locations. Geohealth. 2025;9:e2024GH001138. doi:10.1029/2024GH001138
13. Phungoen P, Cheung LW, Ienghong K, Apiratwarakul K. Characteristics and outcomes of patient transport to the hospital by Emergency Medical Services (EMS); a cross-sectional study. Arch Acad Emerg Med. 2023;11:e69. doi:10.22037/aaem.v11i1.2112
14. Apiratwarakul K, Cheung LW, Prasitphuriprecha M, Ienghong K. Transition of EMS workflow from radio to bell signals to shorten activation time in multiple casualty incident. Sci Rep. 2025;15:6889. doi:10.1038/s41598-025-91790-7
15. Riyapan S, Sanyanuban P, Chantanakomes J, et al. Enhancing survival outcomes in developing emergency medical service system: continuous quality improvement for out-of-hospital cardiac arrest. Resusc Plus. 2024;19:100683. doi:10.1016/j.resplu.2024.100683
16. Apiratwarakul K, Suzuki T, Celebi I, et al. “Motorcycle Ambulance” policy to promote health and sustainable development in large cities. Prehosp Disaster Med. 2022;37:78–83. doi:10.1017/S1049023X21001345
17. Yurt E, Gümüşsoy S. Exploring the experiences and challenges of motorcycle ambulance personnel in pre-hospital emergency healthcare services: a qualitative study. Work. 2025;80:691–700. doi:10.3233/WOR-240113
18. Xu M, Bravo de Guenni L, Córdova JR. Climate change impacts on rainfall intensity-duration-frequency curves in local scale catchments. Environ Monit Assess. 2024;196:372. doi:10.1007/s10661-024-12532-2
19. Adeyeri OE, Folorunsho AH, Adeliyi TE, et al. Climate change is intensifying rainfall erosivity and soil erosion in West Africa. Sci Total Environ. 2024;955:177174. doi:10.1016/j.scitotenv.2024.177174
20. Bacchetti P, Leung JM. Sample size calculations in clinical research. Anesthesiology. 2002;97:1028–1032. doi:10.1097/00000542-200210000-00050
21. Alam E, Hridoy AE, Tusher SMSH, Islam ARMT, Islam MK. Climate change in Bangladesh: temperature and rainfall climatology of Bangladesh for 1949–2013 and its implication on rice yield. PLoS One. 2023;18:e0292668. doi:10.1371/journal.pone.0292668
22. Lu K, Ban J, Wang Q, Li T. Protocol for estimating exposure to compound heat wave and ozone pollution under future climate change. STAR Protoc. 2023;4:102090. doi:10.1016/j.xpro.2023.102090
23. Gao M, Wang F, Ding Y, et al. Large-scale climate patterns offer preseasonal hints on the co-occurrence of heat wave and O3 pollution in China. Proc Natl Acad Sci U S A. 2023;120:e2218274120. doi:10.1073/pnas.2218274120
24. Hu J, He G, Meng R, et al. Temperature-related mortality in China from specific injury. Nat Commun. 2023;14:37. doi:10.1038/s41467-022-35462-4
25. Yuan L, Madaniyazi L, Vicedo‑Cabrera AM, et al. A nationwide comparative analysis of temperature-related mortality and morbidity in Japan. Environ Health Perspect. 2023;131:127008. doi:10.1289/EHP12854
26. Sharma A, Deng L, Wang YC. Estimation of effects of extreme temperature on the risk of hospitalisation in Taiwan. J Epidemiol Community Health. 2023;77:375–383. doi:10.1136/jech-2022-220142
27. Gardner J, Caley L, Poche M, Trammell S. Heat-related illness. Nursing. 2024;54:16–23. doi:10.1097/NSG.0000000000000029
28. Green S, Deering S, Ng D, Lee KS. Approach to heat-related illness. Can Fam Physician. 2024;70:546–550. doi:10.46747/cfp.7009546
29. Krishna S, Kim R, Pochtar E, Papaioannou H. Heat-related illness and sun safety strategies for pediatric populations. Curr Opin Pediatr. 2024;36:702–709. doi:10.1097/MOP.0000000000001382
30. Eifling KP, Gaudio FG, Dumke C, et al. Wilderness medical society clinical practice guidelines for the prevention and treatment of heat illness: 2024 update. Wilderness Environ Med. 2024;35:112S–127S. doi:10.1177/10806032241227924
31. Apiratwarakul K, Cheung LW, Pearkao C, Ienghong K. The impact of global warming on the rise in heat-related illnesses in emergency medical services. J Multidiscip Healthc. 2024;17:5211–5216. doi:10.2147/JMDH.S501721
32. Fentie EA, Asmamaw DB, Negash WD, et al. Spatial distribution and determinants of barriers of health care access among female youths in Ethiopia, a mixed effect and spatial analysis. Sci Rep. 2023;13:21517. doi:10.1038/s41598-023-48473-y
33. Beach B, Steel N, Steptoe A, Zaninotto P. Associations of cognitive impairment with self-isolation and access to health and care during the COVID-19 pandemic in England. Sci Rep. 2023;13:5026. doi:10.1038/s41598-023-31241-3
34. Simmons KM, McIsaac SM, Ohle R. Impact of community-based interventions on out-of-hospital cardiac arrest outcomes: a systematic review and meta-analysis. Sci Rep. 2023;13:10231. doi:10.1038/s41598-023-35735-y
35. Watanabe K, Mori K, Sato K, Abe T, Imaki S, Takeuchi I. Out-of-hospital cardiac arrest patients during the coronavirus disease 2019 pandemic. Sci Rep. 2023;13:23005. doi:10.1038/s41598-023-50150-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.