Back to Journals » Risk Management and Healthcare Policy » Volume 18
Cleaning, Disinfection, and Functional Tests for Bag Valve Masks in Hospitals Located in 117 Cities in China: A Cross-Sectional Study
Authors Qin N, Zhu J, Huang H, Chen H, Rao J, Zhou X
Received 24 March 2025
Accepted for publication 22 July 2025
Published 26 July 2025 Volume 2025:18 Pages 2479—2492
DOI https://doi.org/10.2147/RMHP.S530153
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Jongwha Chang
Nian Qin,1 Juan Zhu,2 Hao Huang,3 Hui Chen,1 Jingyu Rao,1 Xiaoli Zhou1
1Central Sterile Supply Department, West China Hospital, Sichuan University/West China School of Nursing, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 2Central Sterile Supply Department, Tongji Hospital, Tongji Medical College of Huazhong University of Science & Technology, Wuhan, Hubei, People’s Republic of China; 3Department of Nursing, West China Hospital, Sichuan University/West China School of Nursing, Sichuan University, Chengdu, Sichuan, People’s Republic of China
Correspondence: Juan Zhu, Email [email protected]
Background: This study aimed to investigate factors associated with cleaning failures and malfunctions of bag valve masks (BVMs).
Methods: Stratified sampling was used in this cross-sectional study. A questionnaire survey was conducted with central sterile supply department managerial personnel from 479 hospitals in China from December 2023 to July 2024. Data concerning BVM reprocessing, such as types of BVMs, methods of cleaning, disinfection and drying, functional tests, and storage conditions, were analyzed.
Results: The incidences of cleaning failures in BVMs under storage conditions partially meeting requirements, under storage conditions fully meeting requirements, and when storage conditions were not prioritized in practice were 30.50%, 16.22%, and 18.10%, respectively (χ2 = 11.358, P < 0.01). The incidences of malfunctions in BVMs which were not stored separately and which were in separate storage were 60% and 43.82%, respectively (χ2 = 4.726, P < 0.05). The incidences of malfunctions in infant BVMs and in non-infant BVMs were 48.77% and 35.09%, respectively (χ2 = 6.555, P < 0.05). The incidences of malfunctions in BVMs reprocessed using moist heat disinfection and using other disinfection methods were 37.89% and 49.37%, respectively (χ2 = 5.683, P < 0.05). The incidences of malfunctions in BVMs using high-temperature drying cabinets and using other drying methods were 50.55% and 38.73%, respectively (χ2 = 6.598, P < 0.05).
Conclusion: The types of BVMs and the methods of cleaning, disinfection, drying, and storage conditions could affect the cleaning quality or functional integrity. This highlights the urgent need for standardized national guidelines in China.
Keywords: central sterile supply department, bag valve mask, cleaning, disinfection, functional testing, cross-sectional study
Background
A bag valve mask (BVM), also known as a manual resuscitator or self-inflating bag, is a widely used device for first aid in clinical practice. It is often used for cardiopulmonary resuscitation.1,2 Ventilation with a BVM is also required before respiratory support in intensive care unit patients.3,4 BVMs can become contaminated by patient secretions. Failures in cleaning and disinfecting BVMs can expose patients to potential biological infection risks, resulting in adverse prognosis, such as respiratory tract and lung infections.
Recent studies on BVMs conducted in China and abroad have primarily focused on their clinical applications,5–9 with few studies addressing the reprocessing of BVMs. After reviewing a large number of literature references, it was found that only a few studies discuss BVM reprocessing. For example, the results of Zhu et al10 have shown that contamination of BVMs are closely associated with ventilator-associated pneumonia. The incidence rate of ventilator-associated pneumonia in patients using BVMs disinfected once every 3 days is significantly lower than that in patients using BVMs disinfected once every 7 days (28.33% versus 48.33%).11 The prevention of ventilator-associated pneumonia focuses more on the disinfection of respirator tubing, whereas insufficient attention is paid to cleaning and disinfection of BVMs.12 When BVMs are not disassembled into their smallest components for cleaning, as required by the Centers for Disease Control and Prevention in their “Guidelines for Disinfection and Sterilization in Healthcare Facilities”,13 the failure rate can reach as high as 31.7%.14
BVMs are classified into two categories: disposable and reusable. Reusable BVMs need to be cleaned and disinfected after use. Some primary healthcare institutions in China adopt manual cleaning and immersion disinfection with chemical disinfectants for BVMs. This can involve more human factors and pose a risk of failures in cleaning and disinfection. In some tertiary hospitals in China, reusable BVMs are routinely reprocessed by central sterile supply departments (CSSDs) before clinical redeployment,12 but the reprocessing of BVMs receives insufficient attention and lacks relevant guidelines. In some low- and middle-income countries, disposable BVMs are retained after use for reuse,15 posing challenges for their cleaning and disinfection.
There are no unified guidelines for the whole chain management of BVM cleaning and disinfection in China, and the supervision in China remains unclear. Greater attention should be paid to BVM reprocessing, its compliance with clinical requirements, and its potential negative impact on clinical use. This study aimed to investigate factors associated with cleaning failures and malfunctions of BVMs, providing a foundation for developing a standard operating procedure for BVM reprocessing and improving related guidelines. This study may serve as a reference for the disinfection and management of reusable medical devices. It may also draw increased attention from CSSDs on BVM reprocessing, promoting more scientific and standardized procedures and enhancing patient safety.
Methods
Ethical Approval
Ethical approval of this study was obtained from the Biomedical Ethics Committee of West China Hospital, Sichuan University [2024 Nian Shen (2578)]. Waiver of informed consent was approved by the Biomedical Ethics Committee of West China Hospital, Sichuan University.
Study Design
A questionnaire survey was conducted with CSSD managerial personnel from 479 hospitals in 117 cities across 20 provinces in China from December 2023 to July 2024 to investigate the hospitals’ attention levels in BVM reprocessing, collection, the procedures of cleaning and disinfection, and functional testing and to understand the hospitals’ demands for technical guidelines for BVM reprocessing (Supplementary file 1).
Through a survey on BVM reprocessing and feedback from clinical users about adverse events caused by BVMs, issues in BVM reprocessing by CSSDs could be identified, and key factors associated with these adverse events could be examined. This can improve BVM reprocessing by the CSSDs, thereby enhancing the quality of clinical BVM use and ensuring patient safety.
The collected data were summarized by reviewing relevant literature and integrating it with the guidelines (WS310-2016) for CSSDs in the People’s Republic of China,16–18 the guidelines (WS/T 367-2012) for regulation of disinfection technique in healthcare settings,19 the Guidelines (YY 0600.4-2013/ISO 10651-4:2002) for health and pharmaceutical sector of the People’s Republic of China - Lung ventilators for medical use - Particular requirements for basic safety and essential performance - Part 4: operator-powered resuscitators,20 China’s BVM cleaning procedures (Figure 1) and management principles, and hospital requirements for controlling nosocomial infections. Subsequently, a questionnaire titled “Investigation on BVM Cleaning, Disinfection, and Functional Testing” was developed following discussions with 5 sterile supply experts from the Nursing Equipment and Materials Branch of the China Association of Medical Equipment. Six other experts then scored the relevance of questionnaire items. The item-level content validity index ranged from 0.833 to 1.000, and the scale-level content validity index/average was 0.974, indicating good content validity. After the pre-survey with 13 questionnaires, the wording of some questions was revised, and the final questionnaire was formulated.
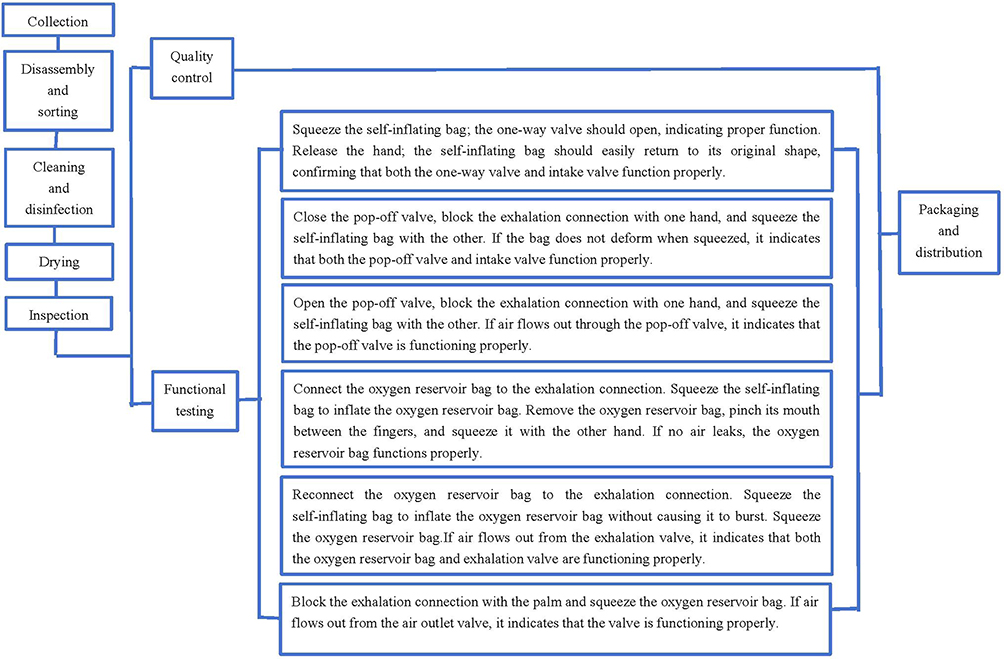 |
Figure 1 Reprocessing procedures for bag valve masks. |
This study focused on the key steps and process management of BVM reprocessing. After the cleaning, disinfection, and sterilization of the BVMs, feedback on the occurrence of cleaning failures and malfunction cases was collected from the CSSDs and clinical department staff. The following information and variables were collected for this study:
- Basic information about the CSSDs which reprocessed the BVMs. Basic information of the CSSDs and hospitals; CSSD management mode (centralized management or decentralized management); department responsible for BVM reprocessing (directly reprocessed by their respective hospital or outsourced to the third-party healthcare institutions); job titles of BVM reprocessing personnel (nurses, technical workers, or other).
- Types of BVMs. For adult, child, and infant.
- Methods of BVM reprocessing. Methods of collection, disassembly, cleaning, disinfection and drying, functional testing, and storage conditions.
- Management of BVM reprocessing. Knowledge sources, CSSD work rules, and standard operating procedures.
Data Collection
Stratified sampling was used in this cross-sectional study. Questionnaires were randomly distributed online to CSSD staff from hospitals of different levels across different regions. Survey was conducted with some CSSD staff by telephone interview. A total of 709 responses were returned. The collected responses were preliminarily processed in order to ensure the quality of the data. Because this survey aimed to investigate the factors associated with failures in BVM cleaning and malfunctions, incomplete responses were excluded. Whether answers were provided to all items regarding the occurrence of failures in BVM cleaning and malfunctions served as the criteria for determining a valid response. In addition, the outliers of numerical variables were detected using the 3σ-rule. Finally, 230 invalid responses and those with outliers were removed, leaving a total of 479 valid responses.
Statistical Analysis
SPSS 25 was used for data analysis. Categorical variables were described by frequency (percentage), and numerical variables were described as means ± standard deviation. Chi-square tests or Fisher’s exact tests were performed with radio and enumeration data to compare groups. Logistic regression analysis was conducted on factors associated with categorical data. The significance level was set at 0.05.
Results
Demographic Information of Respondents
The demographic information of the respondents from the 479 valid responses is presented in Table 1. For the classification of hospitals, 290 (60.55%) worked in tertiary hospitals. For the nature of hospitals, 455 (94.99%) were from public hospitals. For types of hospitals, 405 (84.55%) were from general hospitals. For the number of hospital beds, 179 (37.37%) were from hospitals with 501–1000 beds, and 167 (34.86%) were from hospitals with fewer than 500 beds. The reusable BVMs were reprocessed by the CSSDs of the hospitals where the respondents worked and not outsourced to any third-party healthcare institutions.
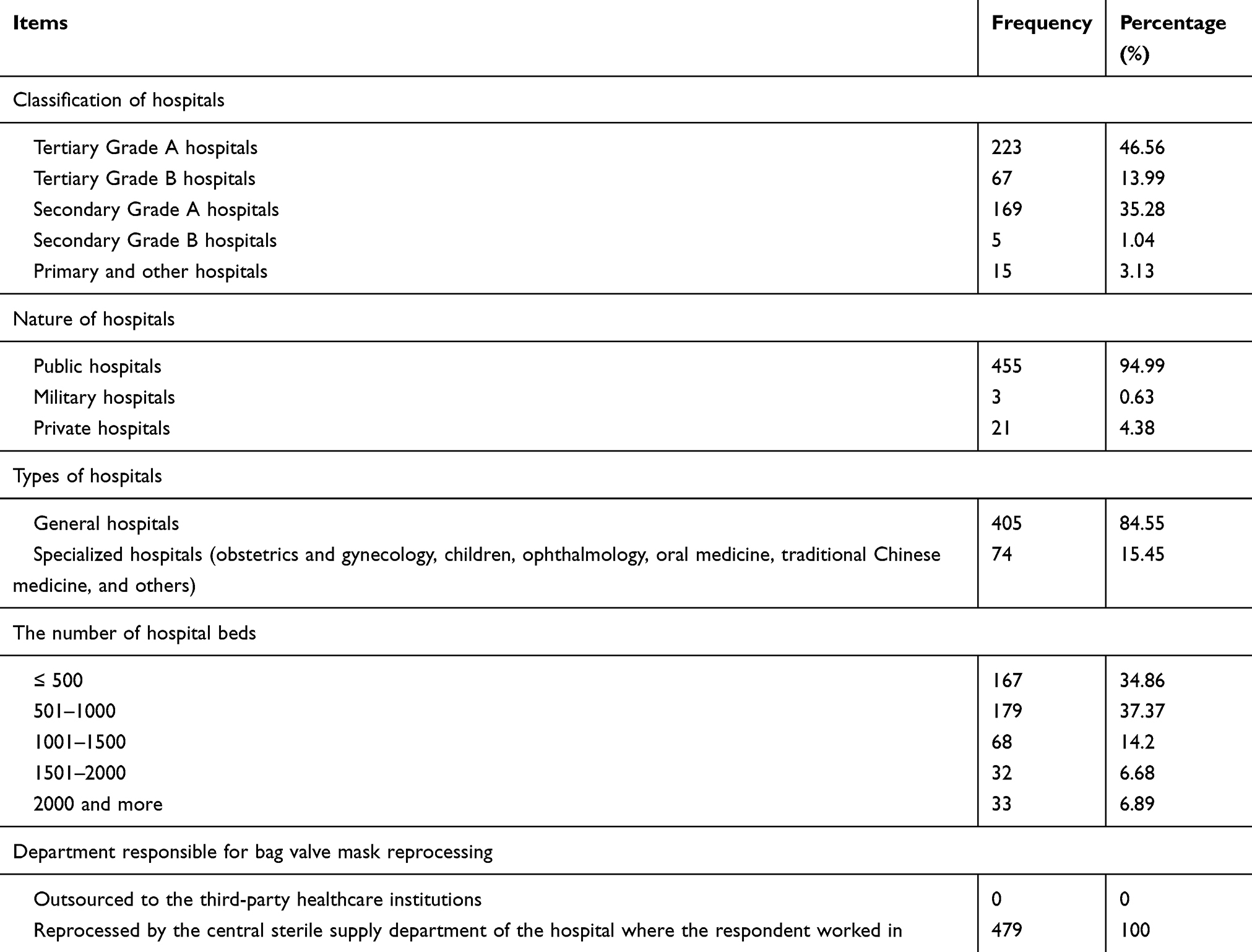 |
Table 1 Demographic Information of Respondents |
Status Quo of BVM Reprocessing
Based on the 479 valid responses, it was found that, for manual cleaning, 84 (17.54%) respondents answered that BVM cavity was not cleaned. For functional testing methods for BVM components, 231 (48.23%) respondents were somewhat familiar with the methods, and 6 (1.25%) respondents were not at all familiar with the methods. For the implementation of functional tests, 353 (73.69%) respondents answered that the tests were not performed or were performed on some components of BVMs. 164 (34.24%) respondents reported that functional tests were implemented on reusable oxygen tubing, and 190 (39.67%) reported that functional tests were implemented on reusable oxygen reservoir bags. 135 (28.18%) reported that the hospitals had no relevant standard operating procedures or quality criteria for BVM reprocessing. 449 (93.74%) wanted to be provided with relevant technical guidelines by the hospitals (Tables 2 and 3).
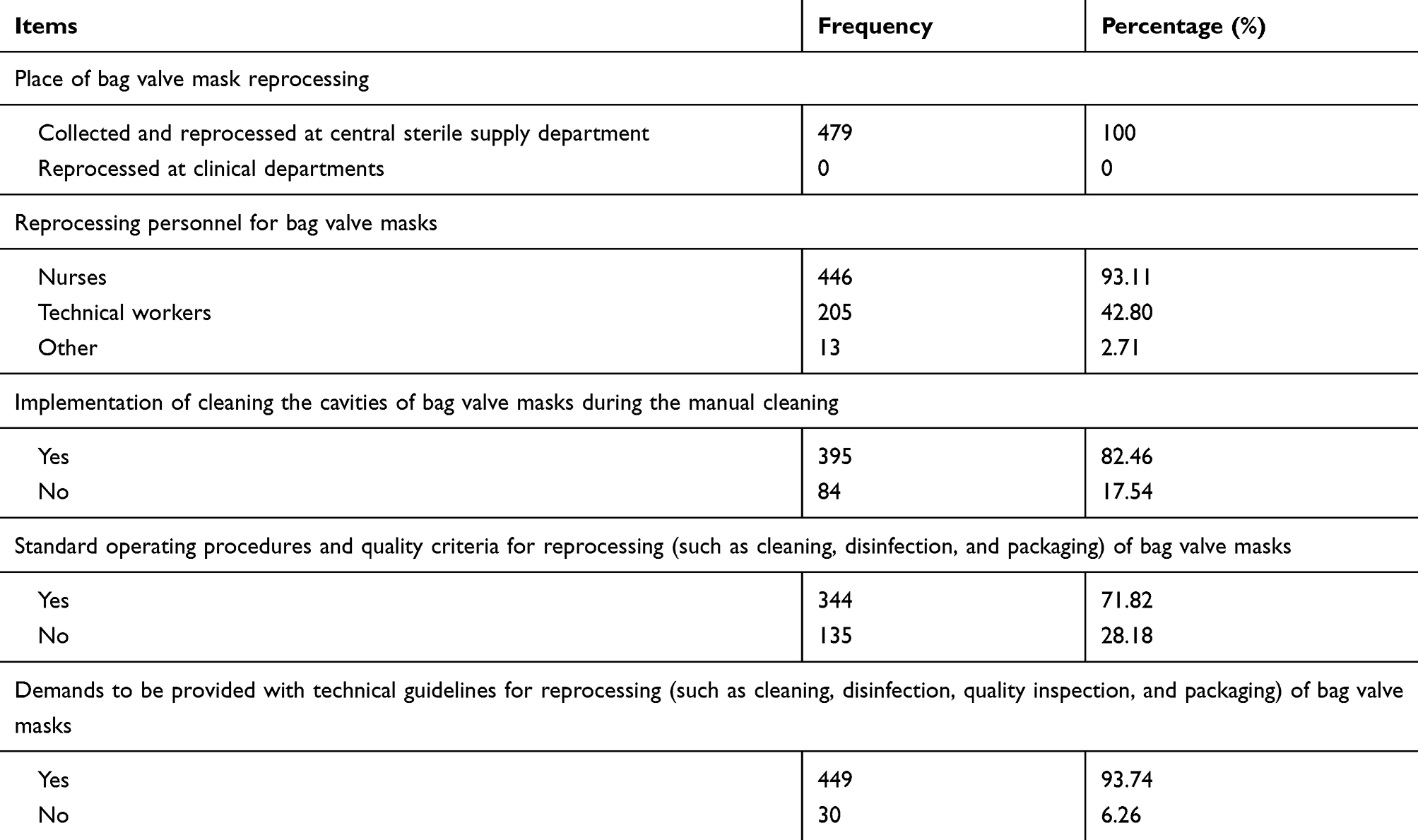 |
Table 2 Personnel and Standard Operating Procedures for Bag Valve Mask Reprocessing |
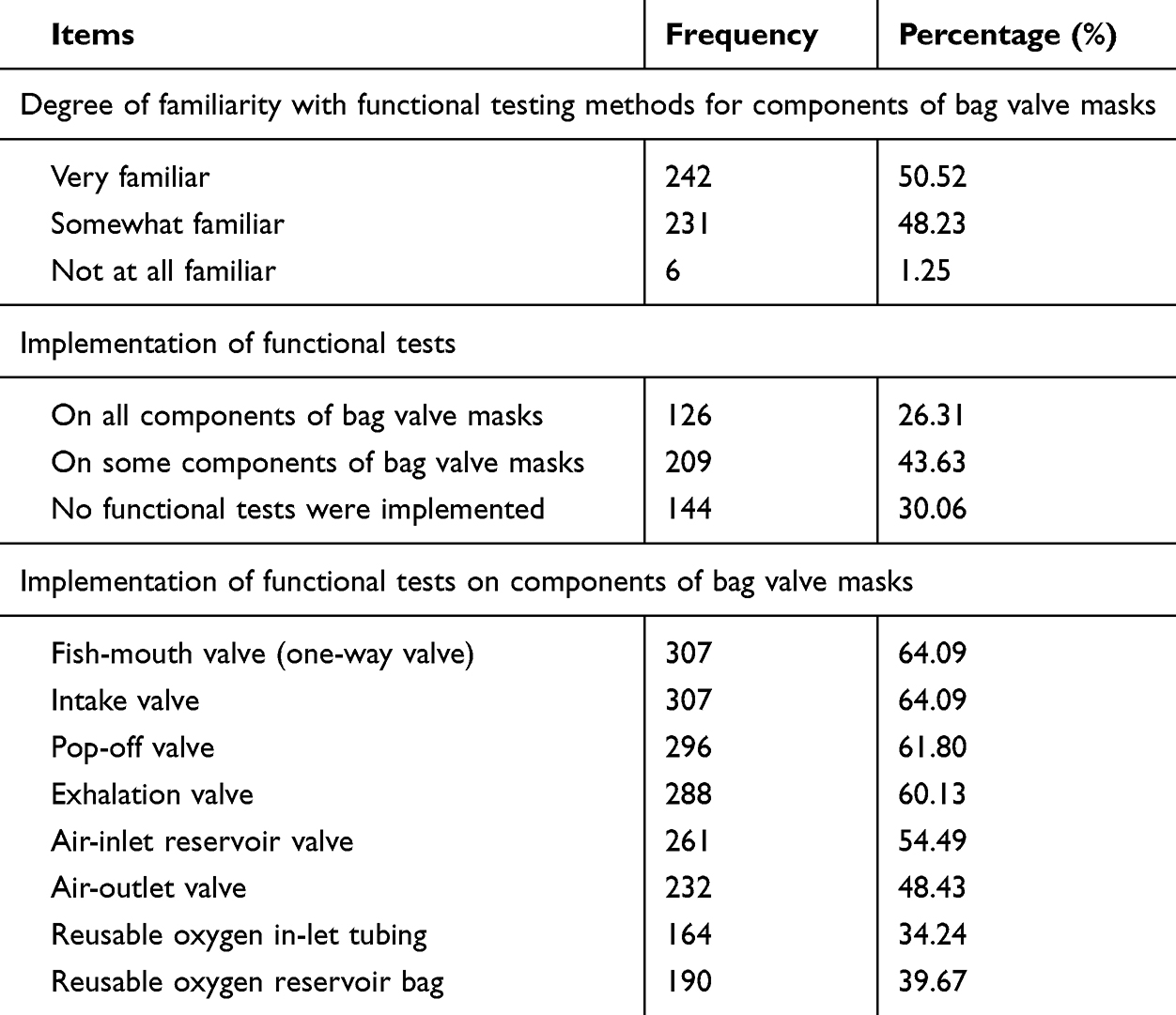 |
Table 3 Functional Testing Practices |
Differential Analysis of Incidences of Cleaning Failures and Malfunctions
The Chi-square tests were performed to investigate whether significant differences existed in the incidence of cleaning failures and malfunctions between different reprocessing conditions.
Differential Analysis of Incidences of Cleaning Failures
Table 4 shows that the incidence of cleaning failures under storage conditions that partially met requirements was 30.50%, significantly higher than that (16.22%) when BVMs were stored under conditions fully meeting requirements and that (18.10%) when storage conditions were not prioritized in practice (χ2 = 11.358, P < 0.01). The incidence of cleaning failures in infant BVMs was 23.01%, significantly higher than in non-infant BVMs (14.04%) (χ2 = 4.239, P < 0.05). The incidence of cleaning failures occurred in child BVMs was 23.72%, significantly higher than in non-child BVMs (8.05%) (χ2=10.595, P < 0.01).
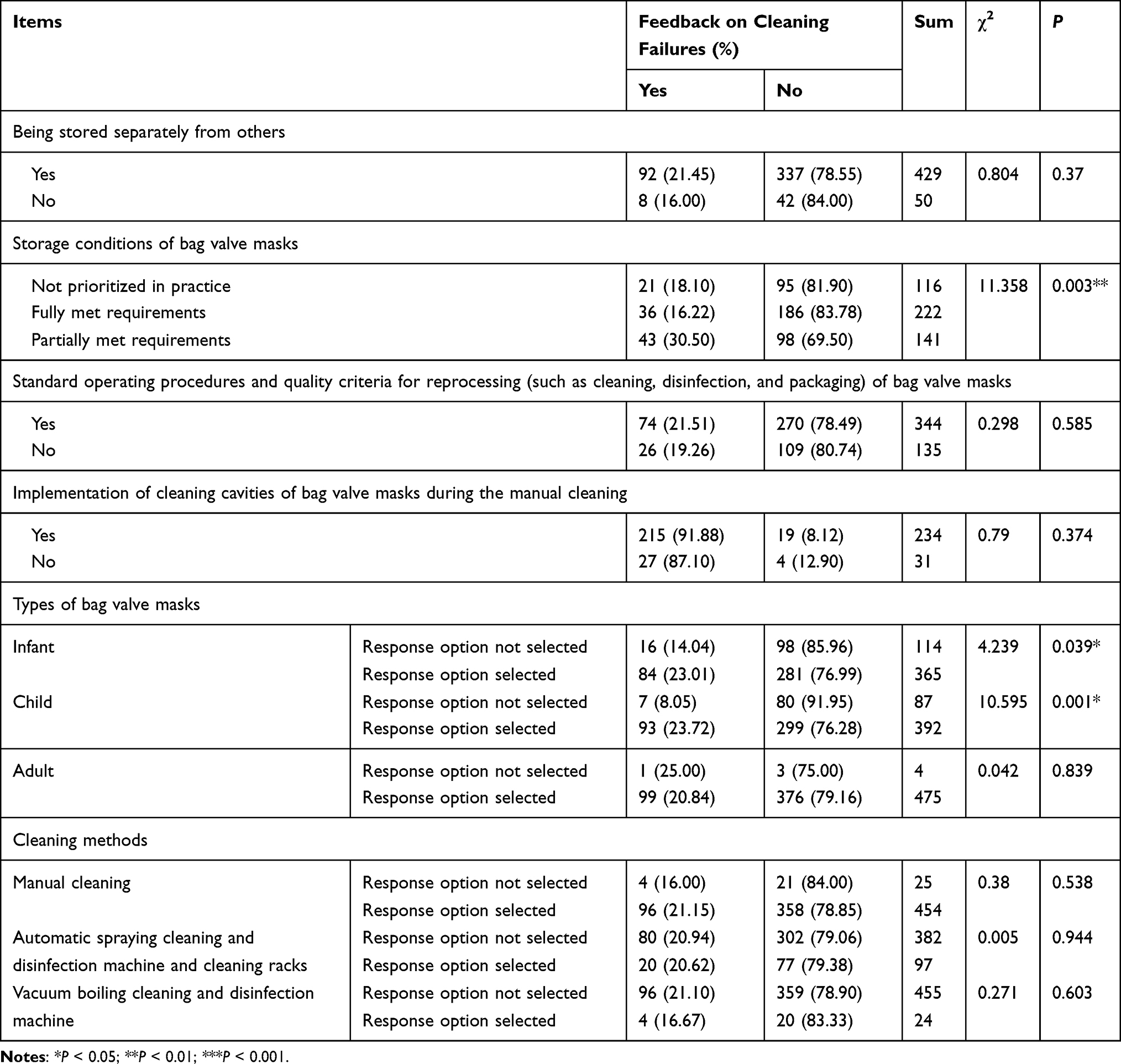 |
Table 4 Chi-Square Test Results for Factors Associated with Cleaning Failures in Bag Valve Masks |
Differential Analysis of Incidences of Malfunctions
Table 5 shows that the incidence of malfunctions in BVMs which were not stored separately from other items, was 60%, significantly higher than that in separate storage (43.82%) (χ2 = 4.726, P < 0.05). The incidence of malfunctions under storage conditions fully meeting requirements was 39.19%, significantly lower than under storage conditions partially meeting requirements (54.61%) and under storage conditions not prioritized in practice (46.55%) (χ2 = 8.336, P < 0.05). The incidence of malfunctions in infant BVMs was 48.77%, significantly higher than in non-infant BVMs (35.09%) (χ2 = 6.555, P < 0.05). The incidence of malfunctions in BVMs reprocessed using moist heat disinfection was 37.89%, significantly lower than using other disinfection methods (49.37%) (χ2 = 5.683, P < 0.05). The incidence of malfunctions in BVMs reprocessed using high-level chemical disinfection was 48.80%, significantly higher than using other disinfection methods (38.10%) (χ2 = 4.704, P < 0.05). For drying methods, the incidence of malfunctions in BVMs using high-temperature drying cabinets was 50.55%, significantly higher than using other drying methods (38.73%) (χ2 = 6.598, P < 0.05). For functional testing methods, the incidence of malfunctions in BVMs adopting function tests for exhalation valves was 41.32%, significantly lower than adopting function tests for other components (57.45%) (χ2 = 4.274, P < 0.05).
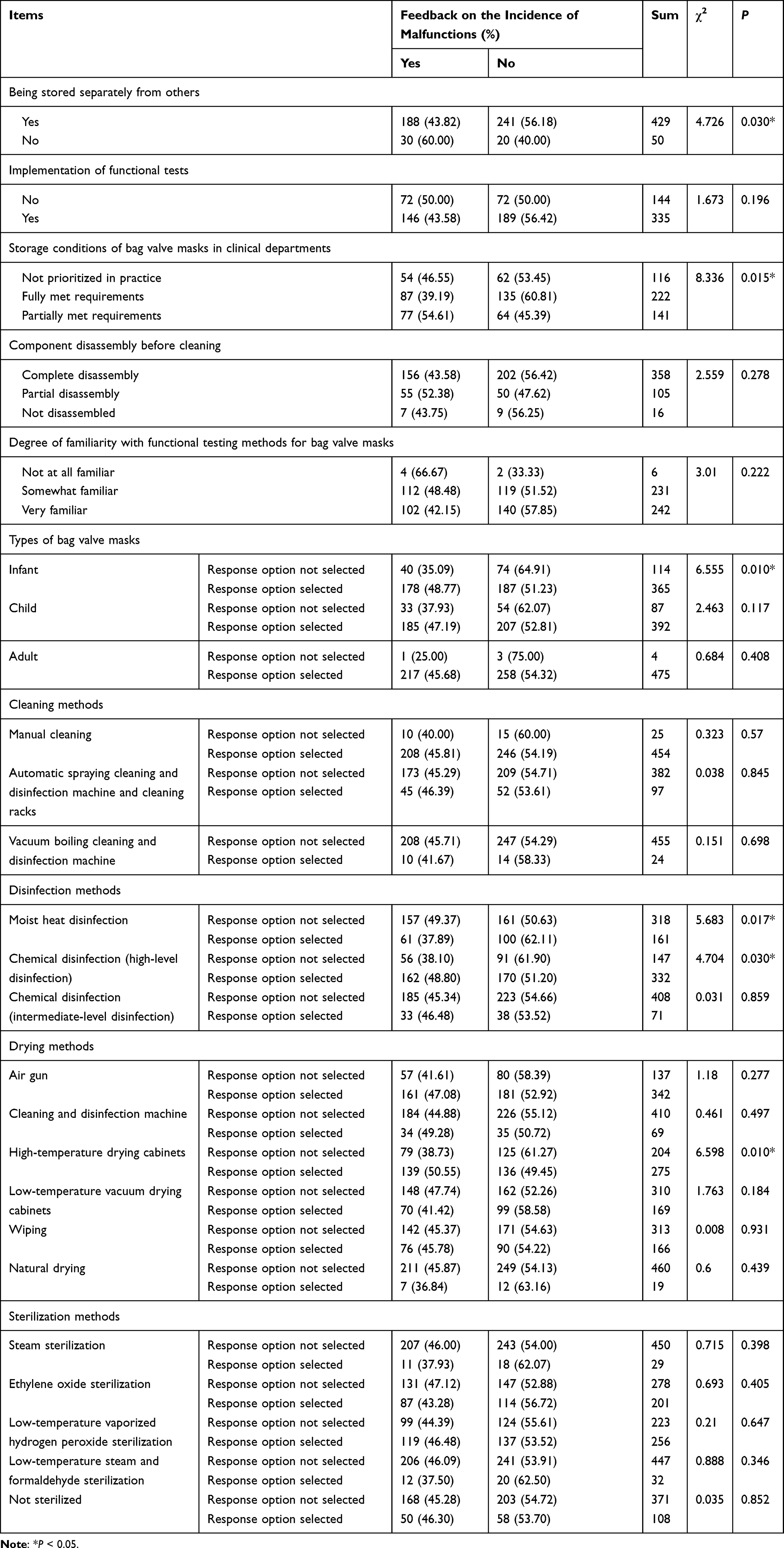 |
Table 5 Chi-Square Test Results for Factors Associated with Malfunctions in Bag Valve Masks |
Logistic Regression Analysis of Factors Associated with Cleaning Failures and Malfunctions
The Chi-square test was performed to investigate the significant differences in the incidences of cleaning failures and malfunctions under various conditions. The binary logistic regression analysis was then performed using the variables showing differences as independent variables to analyze how these variables affect the incidences of cleaning failures and malfunctions.
Binary Logistic Regression Analysis of Factors Associated with Cleaning Failures
Based on the above-mentioned results, a statistically significant difference was found in the incidence of cleaning failures between infant BVMs and child BVMs and between different storage conditions of BVMs. In order to investigate the specific impact of these three variables on cleaning failures, a binary logistic regression analysis was performed. The formula for this model is: ln(p/1-p) = −1.972+0.156*BVM type_Infant + 1.155*BVM type_children −0.635* Storage conditions_Not prioritized in practice −0.802* Storage condition_Fully met requirements (where p represents the probability of failures in cleaning and 1-p represents the probability of no failures in cleaning).
Table 6 and Figure 2 show that the probability of failures in cleaning child BVMs was 3.175 times that of non-child BVMs (odds ratio (OR): 3.175, 95% confidence interval (CI): 1.31–7.692). The probability of failures in cleaning when the BVM storage conditions fully meeting requirements was 0.448 times that of storage conditions partially meeting requirements (OR: 0.448, 95% CI: 0.269–0.748). When storage conditions were not prioritized in practice, the probability of failures in cleaning was 0.53 times that of storage conditions partially meeting requirements (OR: 0.530, 95% CI: 0.291–0.966). The BVMs with storage conditions partially meeting requirements, and the child BVMs received higher probabilities of the occurrence of cleaning failures.
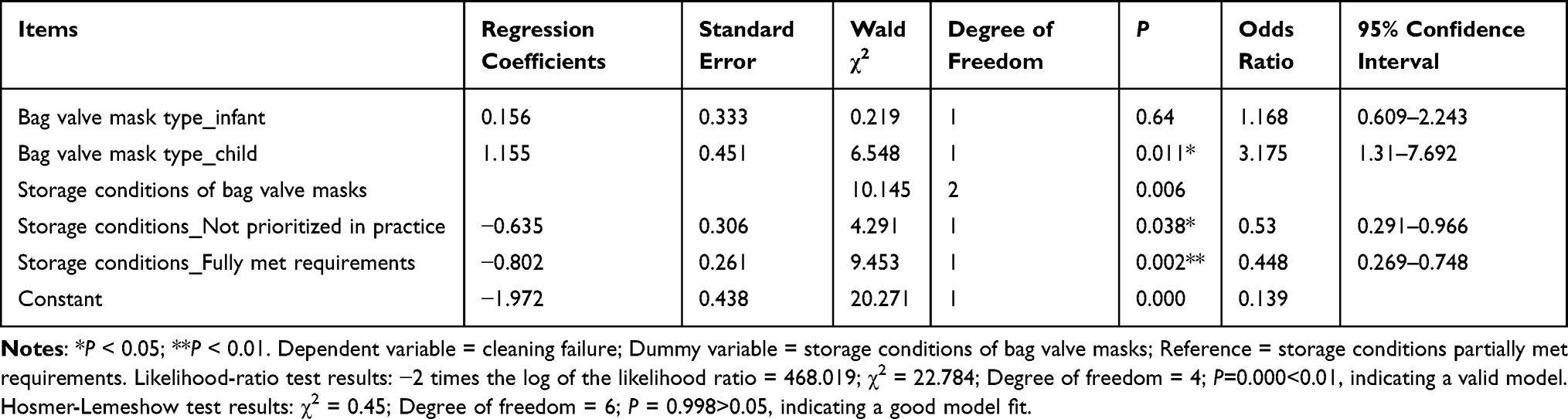 |
Table 6 Logistic Regression Analysis Results for Factors Associated with Cleaning Failures |
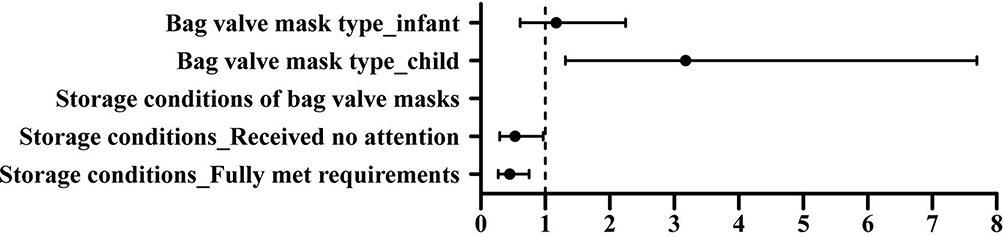 |
Figure 2 Forest plot of logistic regression analysis of factors associated with cleaning failures. |
Binary Logistic Regression Analysis of Factors Associate with Malfunctions
The above-mentioned results show that statistically significant differences were found in the incidences of malfunctions under separate storage, BVM storage conditions, infant BVMs, moist heat disinfection, high-level chemical disinfection, and drying using high-temperature drying cabinets. A binary logistic regression analysis was performed to investigate these six variables’ impact on malfunctions. The formula for this model is: ln(p/1-p) = −1.187+0.564*BVM type_Infant −0.386*Disinfection methods_Moist heat disinfection+0.225*Disinfection methods_Chemical disinfection (high-level disinfection) + 0.439)*Drying methods_High-temperature drying cabinets + 0.556*whether it was stored separately from others −0.289*Store conditions_Not prioritized in practice-0.556*Store conditions_Fully met the requirements (where p represents the probability of failures in cleaning and 1-p represents the probability of no failures in cleaning).
Table 7 and Figure 3 show that the probability of failures in cleaning infant BVMs was 1.757 times that of non-infant BVMs (OR: 1.757, 95% CI: 1.123–2.75). The probability of failures in cleaning when the BVMs were dried using high-temperature drying cabinets was 1.551 times that of other drying methods (OR: 1.551, 95% CI: 1.058–2.274). When storage conditions fully met requirements, the probability of failures in cleaning was 0.573 times that of storage conditions partially met requirements (OR: 0.573, 95% CI: 0.37–0.889). The BVMs using high-temperature drying cabinets, and infant BVMs had higher probabilities of the occurrence of cleaning failures.
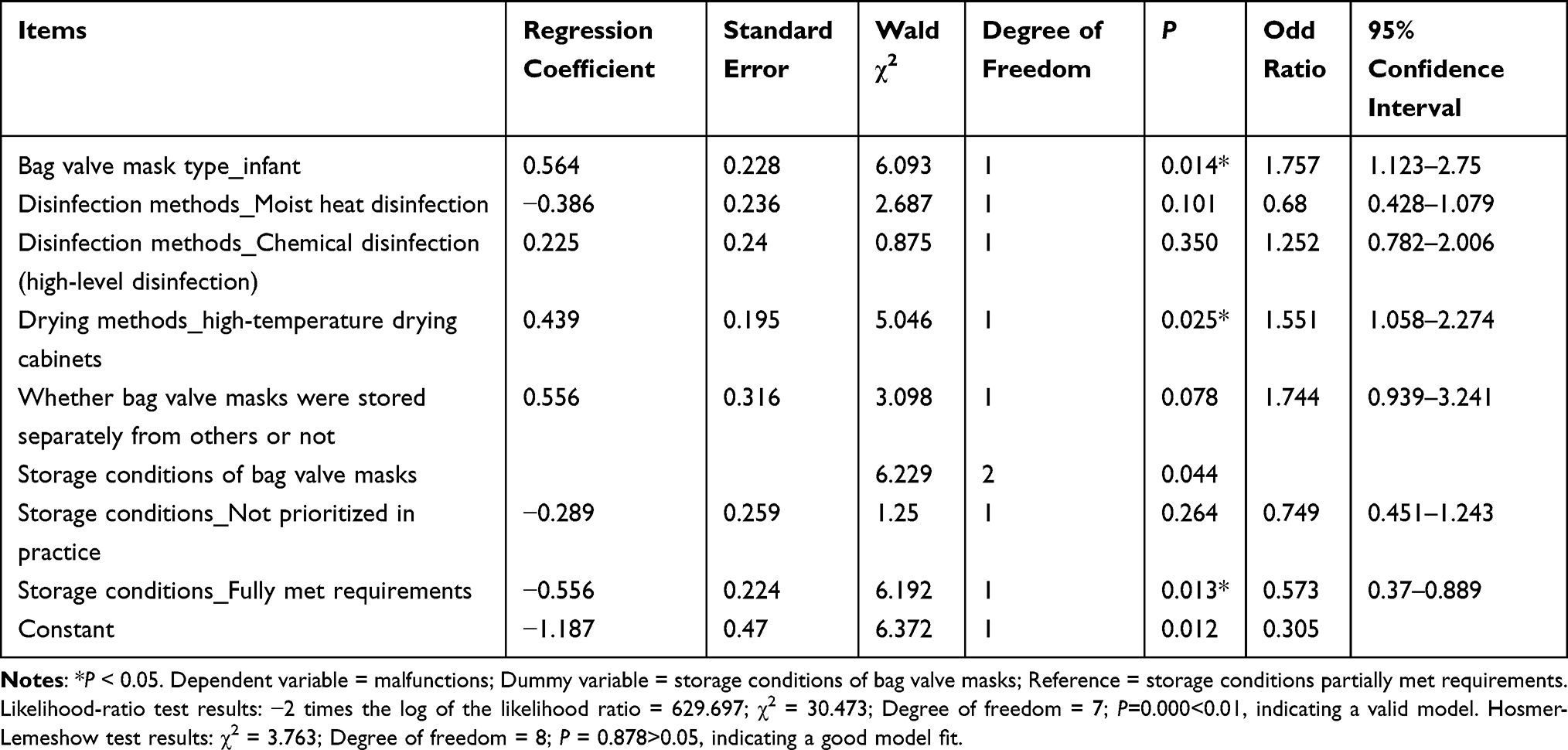 |
Table 7 Logistic Regression Analysis Results for Factors Associated with Malfunctions |
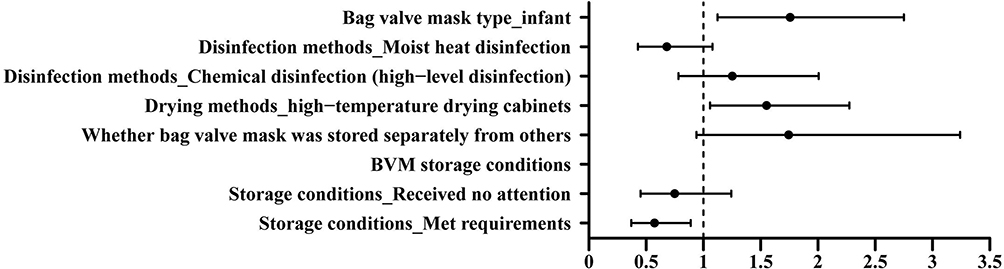 |
Figure 3 Forest plot of logistic regression analysis of factors associated with malfunctions. |
Discussion
The BVM is a critical device for emergency treatment and life support. The quality of its disinfection and the integrity of its function are paramount. The CSSD is responsible for reprocessing all reusable medical devices within a healthcare institution. The standardization, quality, and efficiency of CSSD procedures directly impact the quality of clinical diagnosis and emergency treatment. If BVMs are not thoroughly cleaned and disinfected or if functional testing is not conducted properly, it may endanger patients’ lives.
Functional Testing Gaps
The findings of this study indicate that BVM reprocessing has not received adequate attention from hospitals across all levels in China. Moreover, functional tests were not performed on BVMs, and tests on some components were conducted inappropriately. A BVM consists of multiple components, such as a face mask, intake valve, air-inlet reservoir and air-out valves, pop-off valve, oxygen in-let tubing, and oxygen reservoir bag. Each component has its own specific function. For example, the pop-off valve can automatically adjust pressure. If the pressure inside the self-inflating bag reaches 60cm H2O for adults and 40cm H2O for children and infants, the pop-off valve will automatically open to protect the lungs from high-pressure damage. CSSD staff shall correctly and carefully inspect the components of BVMs during BVM reprocessing. This ensures that BVMs are safely and effectively used to rescue patients. The reasons for functional tests not being implemented or being implemented inappropriately may be because CSSD staff did not have an adequate understanding of the role of each component of BVM or because they received improper training.
It is recommended that the safety awareness of CSSD staff of hospitals across all levels in China be enhanced. They should prioritize the use and reprocessing of emergency medical equipment. Clear standard operating procedures for BVM reprocessing should be established. CSSD staff require additional professional training and should only be permitted to work after passing an assessment to ensure their competence in BVM reprocessing. This ensures an effective supply of BVMs and supports seamless clinical diagnosis and treatment.
Factors Associated with Cleaning Failures and Malfunctions
This study found that the types of BVMs and the methods of cleaning, disinfection, drying, and storage conditions could affect the cleaning quality or functional integrity of BVMs. BVMs are categorized into adult, child, and infant types with similar materials and structures. However, negative feedback regarding the cleaning quality of non-adult BVMs was more frequent than for adult BVMs in practice. This suggests that greater attention should be paid to reprocessing small and precise components during the cleaning process. Finely controlled pressure is particularly critical for infant and child BVMs, as infants and young children have immature lungs, high airway resistance, and are vulnerable to barotrauma. This highlights the need for a greater emphasis on the functional testing of BVMs. This study found that some CSSD staff did not clean the BVM cavity during the manual cleaning. The results of Li et al21 have shown that when patients have excessive respiratory bleeding or secretions (such as sputum) and choking cough, blood and secretions can flow back into the face mask or cavity of the self-inflating bag of the BVM, thereby polluting the cavity. Incomplete disassembly and ineffective cleaning is one of the important factors that may cause respiratory infections in patients.12 Therefore, a BVM should be disassembled into its smallest components before cleaning and disinfection, and the internal and external surfaces of the self-inflating bag and other components should be thoroughly reprocessed.
According to China’s Hygienic Standard for Disinfection in Hospitals (GB 15982–2012),22 the United States’ Chemical Sterilization and High-level Disinfection in Health Care Facilities (ANSI/AAMI ST58),23 and the World Health Organization’s Infection Prevention and Control of Epidemic-and Pandemic Prone Acute Respiratory Infections in Health Care,24 devices that come into direct or indirect contact with mucous membranes are classified as moderately hazardous items. They should undergo high-level or medium-level disinfection before use. Reusable oxygen humidifier bottles, suction bottles, water bottles for infant incubators, and heated humidifier tanks require high-level disinfection. A BVM contacts skin and mucous membranes during use, making it a moderately hazardous item and requires high-level disinfection. Moist heat disinfection and chemical disinfection can meet high-level disinfection requirements. Zhang’s findings25 indicate that when chlorine-containing disinfectants are used for soaking, disinfection may be incomplete due to the volatility of their aqueous solutions, insufficient coverage of the disinfectant on the BVM’s inner surface, or the formation of an organic biofilm on the inner wall that hinders disinfectant penetration.
This study found that BVMs disinfected with moist heat had a lower incidence of malfunctions, suggesting that chemical disinfection may negatively affect their materials and structures. For disinfection efficacy and functional testing, moist heat disinfection appears to be a better option than chemical disinfection. For drying methods, BVMs using high-temperature drying cabinets had a higher incidence of malfunctions, according to the feedback from clinical department staff. A BVM has multiple components - the components can be made of high-polymer materials, such as polyvinyl chloride and polyethylene. Different components may have different heat resistance. Non-standard treatment is prone to cause changes in physical properties, such as aging and deformation. For storage methods and conditions, BVMs, which were stored separately from other items and were stored under conditions fully meeting the requirements, received a lower incidence of malfunctions. This suggests that CSSDs should obtain the product manuals from the BVM manufacturers before receiving BVMs, be familiar with the characteristics of structure and different components, correctly disassemble the BVMs, and choose the proper disinfection and drying methods. Clinical departments using BVMs and CSSDs should regularly monitor storage conditions and prevent damage by ensuring that BVMs are stored separately from other items. CSSDs should develop standardized reprocessing procedures for different BVM types and create detailed illustration diagrams for BVMs with different model numbers, which are prone to confusion.
Needs for Technical Standardization
This study explored the needs and preferences of CSSD staff for improving BVM reprocessing procedures, quality criteria, and technical guidelines. It revealed that some CSSDs lacked standard operating procedures or quality criteria for BVM reprocessing. Most investigated CSSD staff expressed a need for unified technical guidelines for BVM reprocessing. The aforementioned factors may negatively impact BVMs and are related to CSSD operations. Therefore, unified technical guidelines are essential for standardizing the reprocessing of BVMs. It is hoped that these issues can be addressed through the development of unified technical guidelines and the implementation of systematic training.
Limitations
This study had a small sample size, and demographic data of BVM reprocessing personnel were not collected. Future studies should increase the sample size, include more primary and private hospitals, and collect BVM reprocessing personnel’ demographic data (such as age, length of service, and qualification). This will enable a more comprehensive analysis and yield robust conclusions. Future studies should evaluate BVM performance post-standardized reprocessing protocols in a controlled trial.
Conclusions
A CSSD serves as a hospital’s “heart” and is responsible for cleaning, disinfecting, sterilizing, and supplying sterile reusable diagnostic and treatment instruments, utensils, and articles. It plays an important role in preventing and controlling nosocomial infections.26–28 Therefore, CSSDs should prioritize the standardized management of reusable medical devices. Given its complex structure and critical role as a first aid and life support tool, a BVM must remain in optimal condition for immediate use. CSSDs play a vital role throughout the entire lifecycle of a BVM. Standardizing cleaning and disinfection procedures for BVMs and ensuring their functional integrity is crucial to guarantee the safety and availability of these devices in emergency care.
CSSD staff should communicate with clinical departments, consult BVM manufacturers’ manuals, adhere to national and industry standards, refine standard operating procedures, participate in cross-department training provided by CSSD, the Emergency Department, and the Intensive Care Unit, standardized pre-treatment procedures (such as disassembling reusable BVMs and keeping them moist immediately after use), strength professional training, collect ongoing feedback from clinical departments on BVM performance, optimize cleaning, disinfection, inspection, and sterilization procedures, and implement dynamic quality control and continuous quality improvement. This ensures the effective reprocessing of BVMs and prevents the transmission of nosocomial infections. The results of BVM reprocessing reflect the level of medical device management and CSSD operations.
This baseline survey reveals that no established standard operating procedures or quality criteria exist for BVM reprocessing, highlighting the need for unified technical guidelines, which is highly significant for ensuring patient safety. The design of clinical diagnostic and treatment devices should fully consider the effectiveness of their reprocessing procedures. Therefore, this study can serve as a design reference for BVM manufacturers, encouraging greater focus on the operability and quality of BVM reprocessing, such as cleaning and disinfection, in product design. It also provides data support for further studies on quantifying key factors associated with the cleaning quality and functional testing of BVMs.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This cross-sectional survey does not involve patients or their private information. This study can not trigger any risks for patients’ treatment and the use of BVMs. BVMs with defects, such as cleaning failures and malfunctions, were returned to the CSSDs for reprocessing, which did not affect patients’ use. All research methods were implemented in accordance with relevant guidelines and regulations, as well as the Declaration of Helsinki. Ethical approval of this study was obtained from the Biomedical Ethics Committee of West China Hospital, Sichuan University [2024 Nian Shen (2578)]. Waiver of informed consent was approved by the Biomedical Ethics Committee of West China Hospital, Sichuan University.
Funding
No funding was obtained for this study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Qin G. Comparison of the effects of laryngeal mask airway and endotracheal intubation in pre hospital care. J Clin Med Lit. 2017;4(7):1241–1244. doi:10.3877/j.issn.2095-8242.2017.07.045
2. Jänig C, Wenzel J, König J, Piepho T. Airway management techniques in a restricted-access situation: a manikin study. Eur J Emerg Med. 2016;23(4):286–291. doi:10.1097/MEJ.0000000000000273
3. Simon M, Wachs C, Braune S, de Heer G, Frings D, Kluge S. High-flow nasal cannula versus bag-valve-mask for preoxygenation before intubation in subjects with hypoxemic respiratory failure. Respir Care. 2016;61(9):1160–1167. doi:10.4187/respcare.04413
4. Groombridge C, Chin CW, Hanrahan B, Holdgate A. Assessment of common preoxygenation strategies outside of the operating room environment. Acad Emerg Med. 2016;23(3):342–346. doi:10.1111/acem.12889
5. Lindsay HL, Humar MJ, Anderson DJ, Meadley BN. Optimizing preoxygenation for prehospital emergency anesthesia and air medical transport: a comparative study of bag refill valve and reservoir bag. Air Med J. 2025.
6. Malinverni S, Wilmin S, de Longueville D, et al. A retrospective comparison of mechanical cardio-pulmonary ventilation and manual bag valve ventilation in non-traumatic out-of-hospital cardiac arrests: a study from the Belgian cardiac arrest registry. Resuscitation. 2024;199:110203. doi:10.1016/j.resuscitation.2024.110203
7. Culbreth RE, Gardenhire DS. Manual bag valve mask ventilation performance among respiratory therapists. Heart Lung. 2021;50(3):471–475. doi:10.1016/j.hrtlng.2020.10.012
8. Zeng Q, Tan L, Yang X, Luo Y, Wang B, Yan J. Application of the novel bag respirator assisted ventilation device in postoperative transport under general anesthesia with laryngeal mask. J Chongqing Med Univ. 2025;50(5):682–687. doi:10.13406/j.cnki.cyxb.003736
9. Hua F, Wang X, Wang K, et al. Effect of oxygen therapy using new type of simple face mask on patients with severe or critical COVID-19. J Clin Anesthesiol. 2020;36(5):487–489. doi:10.12089/jca.2020.05.016
10. Zhu Y, Fu H. Decentralized management and centralized management of simple respirator: a comparative study on quality. Chin J Nosocomiol. 2013;23(2):416–417.
11. Fu G, Jia X, Wei X. The relationship between the respirator pneumonia and the disinfection cycle period of respirator. Chin J Prac Nurs. 2006;22(14):14–15. doi:10.3760/cma.j.issn.1672-7088.2006.14.008
12. Yan X, Peng Q, Zhou Y, Hu W. Effect analysis of centralized management of bag valve masks in central sterile supply department. Chin Clin Nurs. 2022;14(6):370–372. doi:10.3969/j.issn.1674-3768.2022.06.011
13. Rutala WA, Weber DJ. Guideline for disinfection and sterilization in healthcare facilities, 2008.
14. Dai X, Wang Q, Ni L. Effect of cleaning bag valve mask resuscitators. Chin J Nurs. 2011;46(6):596–597. doi:10.3761/j.issn.0254-1769.2011.06.025
15. Zemitis S, Harman M, Hargett Z, Weinbrenner D. Single-use bag valve masks: evaluation of device design and residual bioburden analytical methods. J Biomed Sci Eng. 2018;11(9):235–246. doi:10.4236/jbise.2018.119019
16. National Health and Family Planning Commission of the People’s Republic of China. Guidelines (WS 310.1-2016) for health sector of the People’s Republic of China - Central sterile supply department (CSSD) - Part 1: management standard. 2016. Available from: https://www.nhc.gov.cn/ewebeditor/uploadfile/2017/01/20170105090443523.pdf.
17. National Health and Family Planning Commission of the People’s Republic of China. Guidelines (WS 310.2-2016) for health sector of the People’s Republic of China - Central sterile supply department (CSSD) - Part 2: standard for operating procedure of cleaning, disinfection and sterilization. 2016. Available from: http://www.nhc.gov.cn/ewebeditor/uploadfile/2017/01/20170105090606684.pdf.
18. National Health and Family Planning Commission of the People’s Republic of China. Guidelines (WS 310.3-2016) for health sector of the People’s Republic of China - Central sterile supply department (CSSD) - Part 3: surveillance standard for cleaning, disinfection and sterilization. 2016. Available from: https://www.nhc.gov.cn/ewebeditor/uploadfile/2017/01/20170105090648964.pdf.
19. Ministry of Health of the People’s Republic of China. Guidelines (WS/T 367-2012) for health sector of the People’s Republic of China - Regulation of disinfection technique in healthcare setting. 2012. Available from: https://www.nhc.gov.cn/wjw/s9496/201204/54510/files/1739782203873_68673.pdf.
20. China Food and Drug Administration. Guidelines (YY 0600.4-2013/ISO 10651-4:2002) for pharmaceutical sector of the People’s Republic of China - Lung ventilators for medical use - Particular requirements for basic safety and essential performance - Part 4: operator-powered resuscitators. 2013. Available from: https://www.cmde.org.cn/hbpdf/YY0600.4-2013.pdf.
21. Li Q, He S, Ye G. Effect of using bag valve masks to remove air bag retention on ventilator-associated lower respiratory tract infection. Clin Med. 2009;29(10):124–125. doi:10.3969/j.issn.1003-3548.2009.10.083
22. General Administration of Quality Supervision, Inspection and Quarantine of The People’s Republic of China, National Standardization Administration. National Standard of the People’s Republic of China (GB 15982-2012) - Hygienic standard for disinfection in hospitals. 2012. Available from: http://c.gb688.cn/bzgk/gb/showGb?type=online&hcno=4DA7977F7EFBF4B3181E3EE674DC82C8.
23. American National Standards Institute, Inc, Association for the Advancement of Medical Instrumentation. Chemical sterilization and high-level disinfection in health care facilities. ANSI/AAMI ST58. 2005.
24. World Health Organization. Infection Prevention and Control of Epidemic-and Pandemic Prone Acute Respiratory Infections in Health Care. World Health Organization; 2014:156.
25. Zhang H. Effects of two methods of cleaning and disinfection of simple respirators. Mod Clinl Nurs. 2013;12(9):64–66. doi:10.3969/j.issn.1671-8283.2013.09.020
26. Shi J, Li X, Gao L. Construction of high-quality nursing evaluation indexes system in disinfection supply center. Nurs Pract Res. 2020;17(21):1–3. doi:10.3969/j.issn.1672-9676.2020.21.001
27. Zheng Y, Bian Z. Exploration and practice of centralized utilization in CSSD. Health Vocat Educ. 2011;29(12):139–141. doi:10.3969/j.issn.1671-1246.2011.12.082
28. Lu J. Construction and development of disinfection supply centers in our country. Chin Hosp Arch Equip. 2023;24(4):15–17. doi:10.3969/j.issn.1671-9174.2023.04.002
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.