Back to Journals » Advances in Medical Education and Practice » Volume 16
Classrooms to Clinics: A Capstone Preclinical Course Designed from Educational, Social, and Developmental Perspectives on the Transition to Clerkship
Received 4 March 2025
Accepted for publication 4 July 2025
Published 23 July 2025 Volume 2025:16 Pages 1281—1286
DOI https://doi.org/10.2147/AMEP.S523459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Mary Kate Worden,1 Megan J Bray2
1Department of Medical Education, Center for Medical Education Research and Scholarly Innovation, University of Virginia School of Medicine, Charlottesville, VA, USA; 2Department of Obstetrics and Gynecology, Department of Medical Education, Center for Medical Education Research and Scholarly Innovation, University of Virginia School of Medicine, Charlottesville, VA, USA
Correspondence: Mary Kate Worden, Department of Medical Education, University of Virginia School of Medicine, P.O. Box 800382, 200 Jeannette Lancaster Way, Charlottesville, VA, 22903, USA, Tel +1 434 924 7042, Email [email protected]
Introduction: Transitions to clerkship courses aim to alleviate medical students’ concerns about preparing for clerkship rotations. Most focus on reviewing medical knowledge and clinical skills from an educational perspective. However, few are designed from social or developmental perspectives that emphasize self-regulation and social learning habits. This is unfortunate because learners who are unaware of the social and developmental aspects of learning may struggle to transition from a structured classroom environment to a complex and unpredictable clinical learning environment.
Approach: The two-week Classrooms to Clinics (C2C) course at the University of Virginia School of Medicine serves as a capstone to the preclinical curriculum that helps ease students’ transition to the clerkship year. From the educational perspective, it incorporates case discussions that permit review of key concepts and clinical reasoning skills taught in earlier preclinical courses. From the developmental perspective, C2C challenges students to perform workplace tasks authentic to the clinical environment and to recognize best practices for identifying and leveraging learning opportunities within the clinical workflow. From a social perspective, C2C policies encourage students to nurture relationships with peers to facilitate learning and co-learning on clerkships.
Outcomes: Evidence from course evaluations and analysis of students’ commentary on the most recent iteration of C2C shows that students recognize and appreciate the educational, developmental, and social perspectives on making a successful transition to clerkships.
Next Steps: As next steps, we will address student feedback about Classrooms to Clinics by clarifying how and why it differs from a traditional transitions course in its emphasis on developmental and social learning strategies that facilitate life-long learning. We will also enable clerkship students (and their coaches) to retrospectively review the reflective essays they wrote in C2C so that students can monitor their progress in developing self-regulated learning habits that facilitate a successful transition to the clinical workplace.
Keywords: social learning, clerkship readiness, medical student, curriculum, clinical preparedness
Introduction
Many medical students approach the start of their clinical rotations with some degree of trepidation, uncertain whether their preclinical studies in the classroom have adequately prepared them for the experience of full-time patient care in the clinics.1 Given that each clinic has its own organizational culture and practices and learning opportunities are variable in clinical settings,2 learners may never be fully prepared for the transition to the clinical environment. Nevertheless, many medical schools attempt to bolster students’ confidence and competence by offering “transitions to clerkships” courses that review preclinical concepts, introduce clerkship-specific practices and policies, and address student well-being. Designed from an educational perspective that foregrounds mastery of medical knowledge and clinical skills, relatively few transition courses feature social or developmental conceptual perspectives on the transition from the classroom to the clinical learning environment.3
This is problematic because one of the key challenges for students making the transition to full-time patient care is effectively and proactively engaging in work-based learning. Proactivity is critical, because of the three factors that influence the quality of the learning experience in the clinical environment (student proactivity, clinical engagement, and the availability of clinical learning activities),2 only proactivity is under the control of the learner. The developmental perspective on the transition to clerkship empowers students to reflect and take ownership of their learning experiences while developing a professional identity as a medical practitioner. Self-regulated learners who are proactive in identifying their own resources and assessing their own progress have more success in making the transition to clerkships.4
In contrast, a social perspective on the transition to full-time patient care emphasizes the importance of engaging in meaningful interactions with others, including staff, peers, and near-peers. Students in a nurturing medical learning environment are more likely to engage in clinical tasks and teamwork. Engaging with a community of peers while on clerkship rotations decreases student isolation and enhances clinical and professional learning.5,6 Professional socialization that enables colleagues to share perspectives and fill in knowledge gaps is important throughout a career in medicine.5,7
Approach
To leverage all three complementary ideas on how to ease a medical student’s transition between the classroom and the clinical learning environment, we designed an innovative preclinical capstone course called “Classrooms to Clinics” (C2C). Scheduled just prior to a “transition to clerkships” course that focuses more narrowly on procedural skills and clerkship requirements, C2C has been a two-week required course for ~160 second-year medical students since 2019. Enrollment is mandatory for all medical students who have completed the eighteen-month undergraduate medical education preclinical curriculum at our school of medicine.
C2C incorporates an educational perspective by requiring students to diagnose undifferentiated patients in clinical vignettes, explain the pathophysiology underlying their disease/disorder, and justify plans for their management and treatment. Class discussion of these patient cases allows for a review of key clinical concepts and clinical reasoning skills taught in the preclinical courses. To incorporate a developmental perspective that fosters self-regulated learning in a clinical environment, Classrooms to Clinics also provides anticipatory guidance on the “best practices for learning” on clerkships and highlights the importance of proactively seeking out learning opportunities while engaged in patient care. Finally, and from a social perspective, C2C includes both formal and informal teamwork exercises that encourage students to anticipate the benefits of working with peers to accomplish clinical workplace tasks.
Although fourth-year capstone courses for medical students have been described previously, to our knowledge this is the first preclinical capstone course described in the medical education literature.
Course Design from an Educational Perspective
To provide a capstone experience for preclinical medical students that promotes consolidation of medical knowledge and refinement of clinical reasoning skills, C2C includes twelve clinical cases of undifferentiated patients who present with symptoms that are most likely to be encountered by students on clerkships (Box 1). Each case requires that students recall and apply concepts from multiple preclinical courses to reason through the diagnosis, pathophysiology, and management/treatment. To ensure that multiple clinical perspectives are represented in each case discussion, each C2C session is team-taught. Course faculty represent fourteen different departments in the health system. Learning objectives for each case are replicates of those taught and assessed in earlier courses in the eighteen-month preclinical curriculum and are released to students after class ends, so as not to provide inadvertent clues to the diagnosis. This practice contrasts with that in prior preclinical courses, in which learning objectives for each class session are released prospectively to help students prepare for class.
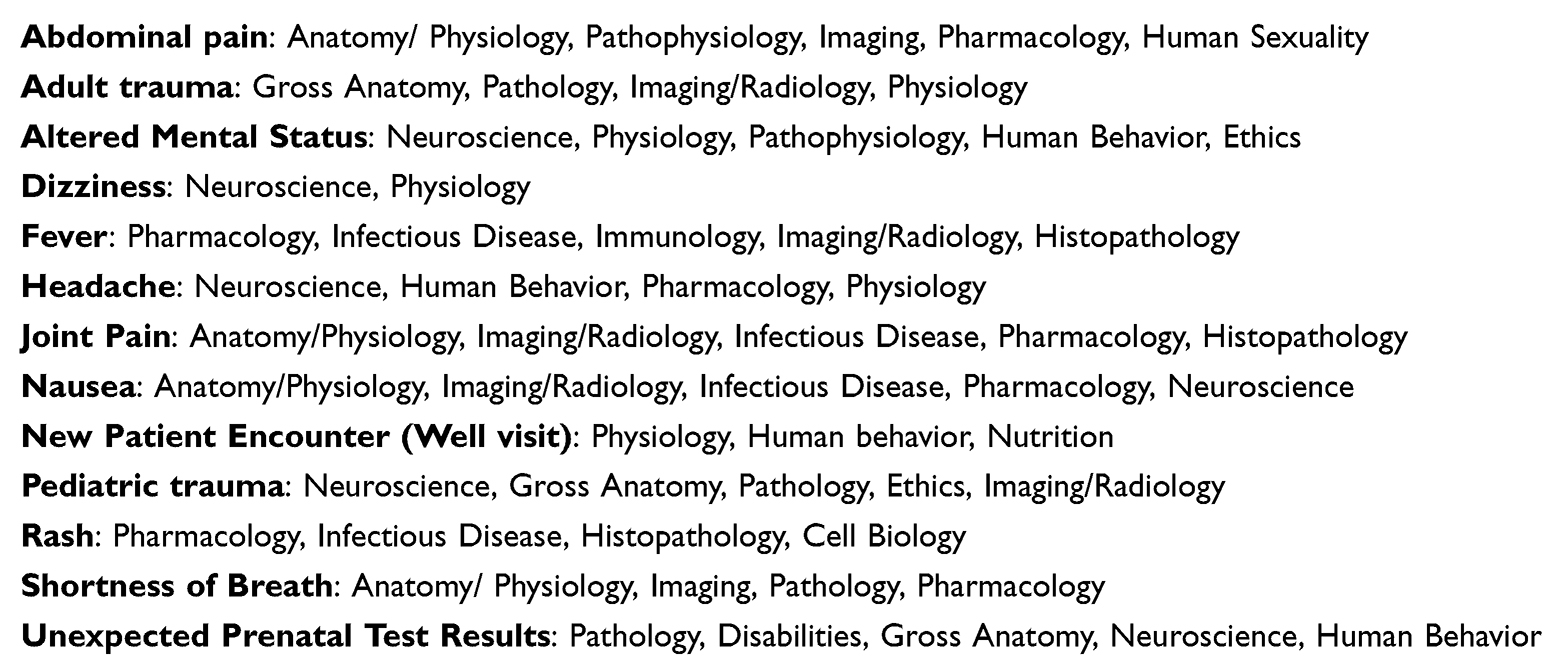 |
Box 1 Clinical case vignettes in Classrooms to Clinics: Presenting symptom in the patient and curricular disciplines addressed |
Presenting clinical reasoning challenges in the context of undifferentiated patients heightens the diagnostic challenge for our preclinical students because diseases and disorders are taught in the context of specific organs in our organ systems-based preclinical curriculum. In clinical vignettes taught in the preclinical cardiovascular system course, for example, any patient who presents with fatigue is very likely to have a diagnosis of cardiovascular disease. Similarly, the diagnosis of a patient with fatigue is more likely to be mood disorder in the course that includes psychiatry, pregnancy in the reproductive system course, and malnutrition in the gastrointestinal system course. Coming to premature closure on diagnosis is a diagnostic error,8 however an organ-system-based preclinical curriculum might inevitably facilitate that error. In Classrooms to Clinics, there is no single organ system as a central focus, which more closely mimics the reality of family medicine or internal medicine clerkships, in which any (or multiple) organ system(s) must be considered in a differential diagnosis.
Course Design from a Developmental Perspective
To help students anticipate how learning opportunities may present themselves in the clinical environment, the most recent iteration of C2C includes several exercises that are authentic to the clerkship experience (see Table 1). Several clerkship rotations include journal club activities, therefore C2C requires students to present a journal article in a teamwork format that gives students insight into how their peers interpret the biomedical literature, communicate research findings to others, and give and receive feedback that is specific, measurable, achievable, relevant and time-bound (SMART).9 As ethical missteps might occur in any patient case during clerkships, another C2C exercise challenges students to collaborate on an ethical analysis of an authentic patient experience as relayed in a complex medical record.
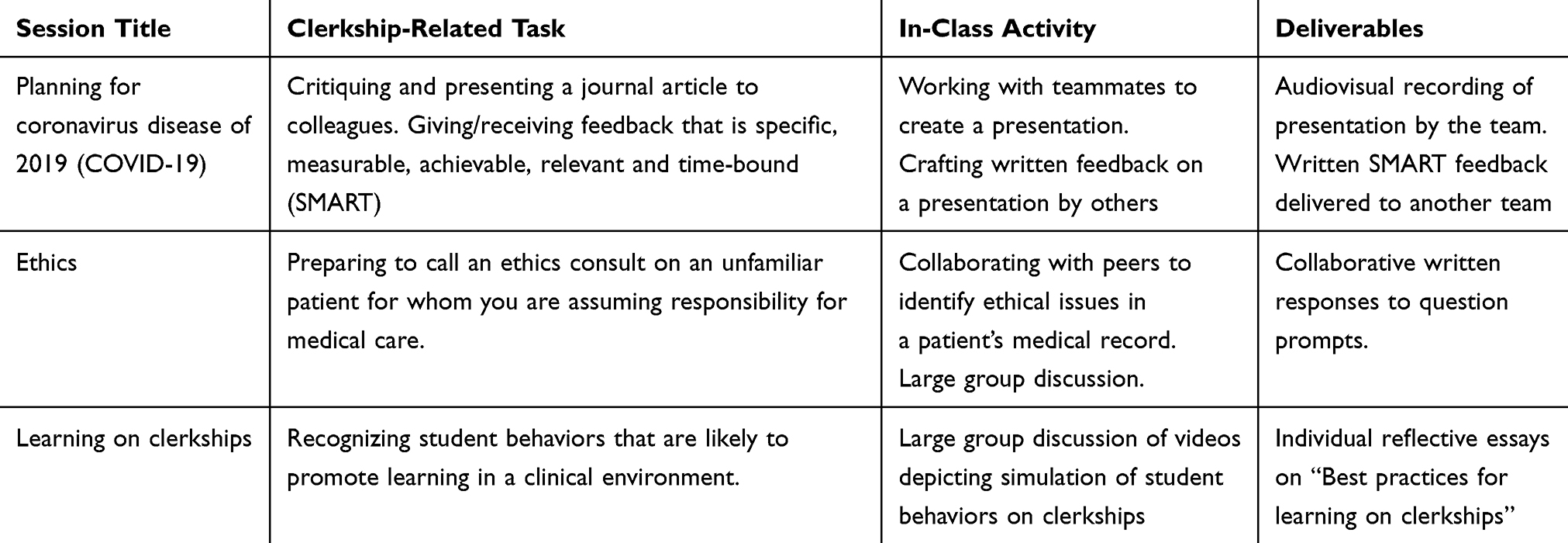 |
Table 1 Classrooms to Clinics Sessions Designed from a Developmental Perspective |
C2C also includes a session that explicitly prompts students to anticipate how learning opportunities might arise during the clinical workflow. In this session, students discuss videos in which actors simulate poor learner behaviors in a clerkship setting, identify missteps and missed opportunities, and role-play with instructors what the actors/students should have done differently. After this session, each student submits a written reflection on “best practices for learning on clerkships”.
Course Design from a Social Perspective
Course policies for C2C are informed by a social perspective that highlights the importance of joint engagement in learning activities with others that promotes co-regulation, and therefore self-regulation, of learning in clinical settings.7 Each C2C class session incorporates active learning in the form of a large or small group discussion or a hands-on activity in alignment with the theory of social constructivism. Student attendance at all C2C class sessions is mandated to encourage students to strengthen working and learning relationships with peers. This policy differs from that in the prior preclinical courses, in which attendance is generally not required.
To enhance student perception of C2C as a social and nurturing learning environment, there are no high-stakes assessments. Instead, to ensure that students master the key teaching points, each C2C class session includes a low stakes graded exercise on which students are permitted to collaborate. Students engage in formal teamwork for a journal club exercise that includes the exchange of peer feedback,9 and for a session on Altered Mental Status that uses Team Based Learning (TBL) pedagogy to leverage the power of teamwork in problem-solving.
Outcomes
Data from 80 students who completed the 2023 Classroom to Clinics course evaluation show that over 70% agree that the course provided opportunities to diagnose patient cases and explain pathophysiology (58/80 students), and to justify plans for the management and treatment of patients (57/80 students). Conventional content analysis of course evaluations from the most recent iteration of Classrooms to Clinics identified three main themes in student commentary on the “greatest strengths” of the course: case-based learning, the effective review of key topics from prior preclinical courses and working with peers in a positive (low stress) learning environment. Student teams provided reflective commentary on the teamwork aspect of the journal club exercise that revealed their appreciation of peers who effectively collaborated, communicated, and organized the work of the teams.9 Students also reported that having the assistance of peers in interpreting the medical record and identifying ethical quandaries proved valuable, as they had not seen authentic and complex patient notes prior to the C2C Ethics exercise. Therefore, from the educational and social perspectives, we are satisfied that C2C serves as an effective capstone to the preclinical curriculum.
Students’ written reflections on “best practices for learning on clerkships” demonstrate the effectiveness of C2C from the developmental conceptual perspective. The five most prominent themes in these reflective essays are shown in Table 2 and identify several best practices, including advance preparation (reviewing patient cases and the day’s schedule beforehand), and being open/receptive to feedback (seeking feedback to learn from mistakes). Both strategies enhance the quality of learning in clinical settings and scaffold learner success throughout a clerkship. Students of C2C also listed as best practices seeking out learning opportunities (taking advantage of learning opportunities whenever possible), active engagement with patients and the healthcare team (asking questions of residents and attendings), and asking questions at appropriate times (situational awareness concerning patient care).
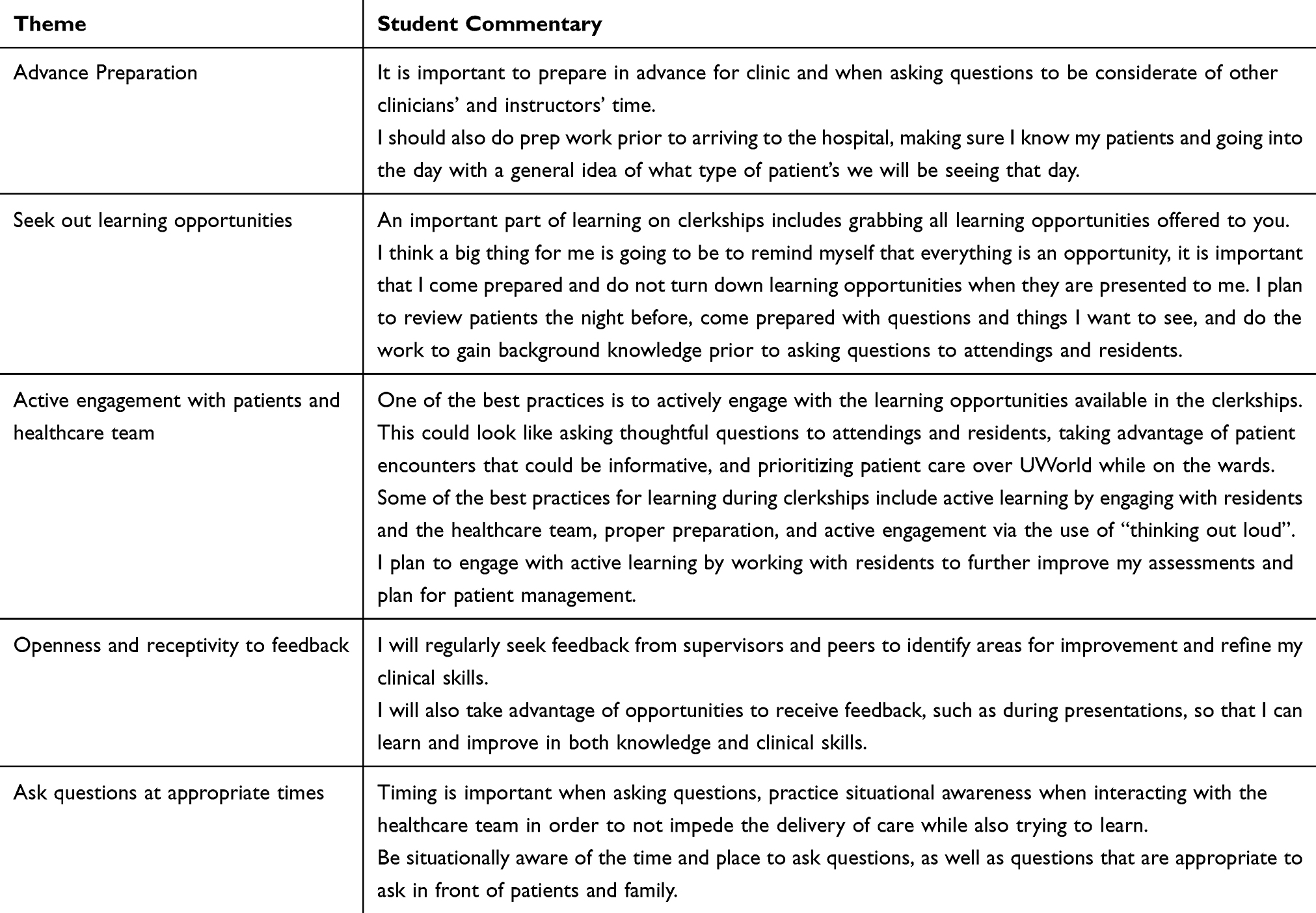 |
Table 2 Five Most Frequent Themes in Student Reflective Essays (n=132) on “Best Practices for Learning on Clerkships” |
On C2C course evaluations, some medical students expressed disappointment that C2C did not offer comprehensive details about the clinical environments through which students will rotate on clerkships. As this information will be presented to students in the subsequent “Clerkship Readiness” course, this feedback represents a misunderstanding of the nature and intent of the Classroom to Clinics course.
Although we had hoped that the Classrooms to Clinics course might help students feel more prepared for clerkships, only 53% (42/80 students) agreed it had. Other authors have pointed out that students’ perceptions of a transitions course are unlikely to be a reliable indicator for outcomes,3,10 given students’ uncertainty about their future experiences in the complex environment of the clinics.
A limitation of this report is that it reports outcomes from a single iteration of C2C at a single institution. We intend to repeat the Classrooms to Clinics course in future years to confirm the outcomes observed. Four previous iterations of C2C (from 2019 to 2022) included only the educational and social perspectives on the transition to clerkship; the developmental perspective was introduced in the fifth iteration.
Next Steps
In future iterations of C2C, we plan to clarify for students how the goals of this capstone course differ from those of the transitions course that follows it on the schedule. The goal of C2C is to review preclinical concepts while emphasizing the importance of developing self-regulatory and social learning habits that facilitate life-long learning. In contrast, the subsequent “Clerkship Readiness” course is more narrowly focused on the specifics of clerkship policies, on required activities such as mask-fitting and basic lifesaving skills, and on maintaining “wellness” during the rigors of clinical rotations.
Another next step is to capture the students’ written reflections on “best practices for learning on clerkships” within each student’s educational portfolio. This step would make the essays available to the coaches who meet with students to co-create individualized learning plans during the clerkship year. In addition, we will keep the content of C2C current by re-evaluating the list of patient cases (see Box 1) and focusing the journal club exercise (see Table 1) on an emerging topic in medicine, rather than on epidemiology of the coronavirus disease of 2019 (COVID-19) pandemic.
Finally, our next steps include surveying students about their perceptions of Classrooms to Clinics after they have completed their first clerkship rotation, instead of when the course concludes. We anticipate that students with substantial clerkship experience might have better insight into the degree to which Classrooms to Clinics meets its goals for facilitating our students’ successful transition to clerkships from an educational, developmental, and social perspective.
Ethics Approval and Informed Consent
The University of Virginia Institutional Review Board for the Social and Behavioral Sciences approved this project and waived the requirement for ethics consent, including consent of students per the institution’s “Use of Student Data” policy (Protocol # 6544).
Acknowledgments
The authors gratefully acknowledge Johanna Craig PhD and Aniseh Burtner for help with thematic analysis and Donna Chen MD and Elizabeth Bradley PhD for helpful discussions. We are also grateful for the contributions of all the instructors who helped design and lead the Classrooms to Clinics course.
Author Contributions
Both authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The University of Virginia School of Medicine provided funding for the administration of the Classrooms to Clinics course.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Malau-Aduli BS, Roche P, Adu M, et al. Perceptions and processes influencing the transition of medical students from pre-clinical to clinical training. BMC Med Educ. 2020;20(1):279. doi:10.1186/s12909-020-02186-2
2. Taylor AWR, Anderson ES, Gay S. ‘It’s a gamble’: a phenomenological exploration of medical students’ learning experiences as newcomers to clinical communities of practice. Clin Teach. 2023;21(4):e13708. doi:10.1111/tct.13708
3. Atherley A, Dolmans D, Hu W, et al. Beyond the struggles: a scoping review on the transition to undergraduate clinical training. Med Educ. 2019;53(6):559–570. doi:10.1111/medu.13883
4. White CB. Smoothing out transitions: how pedagogy influences medical students’ achievement of self-regulated learning goals. Adv Health Sci Educ. 2007;12(3):279–297. doi:10.1007/s10459-006-9000-z
5. Bransen D, Driessen EW, Sluijsmans DMA, Govaerts MJB. How medical students co-regulate their learning in clinical clerkships: a social network study. BMC Med Educ. 2022;22(1):193. doi:10.1186/s12909-022-03259-0
6. Chou CL, Teherani A. A foundation for vital academic and social support in clerkships: learning through peer continuity. Acad Med. 2017;92(7):951–955. doi:10.1097/ACM.0000000000001661
7. Chou CL, Teherani A, Masters DE, et al. Workplace learning through peer groups in medical school clerkships. Med Educ Online. 2014;19(1):25809. doi:10.3402/meo.v19.25809
8. Redelmeier DA, Shafir E. The fallacy of a single diagnosis. Med Decis Making. 2023;43(2):183–190. doi:10.1177/0272989X221121343
9. Worden MK. Is that SMART? Leveraging collaboration and peer feedback to enable practice in appraising and presenting journal articles. Med Sci Educ. 2024;35(1):5–7. doi:10.1007/s40670-024-02188-5
10. Yardley S, Westerman M, Bartlett M, et al. The do’s, don’t and don’t knows of supporting transition to more independent practice. Perspect Med Educ. 2018;7(1):8–22. doi:10.1007/S40037-018-0403-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.