Back to Journals » Clinical Ophthalmology » Volume 16
Class II Human Leukocyte Antigen (HLA) and Susceptibility to Polypoidal Choroidal Vasculopathy in Afro-Caribbean Descent
Authors Merle H, Béral L, Rocher M, Pierre M, Jean-Charles A, Béra O, Rosamont LA ![]() , Robert PY, Lézin A
, Robert PY, Lézin A
Received 1 September 2021
Accepted for publication 13 December 2021
Published 6 April 2022 Volume 2022:16 Pages 1047—1053
DOI https://doi.org/10.2147/OPTH.S337084
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Harold Merle,1 Laurence Béral,2 Maxime Rocher,3 Mitta Pierre,1 Albert Jean-Charles,1 Odile Béra,4 Laurie-Anne Rosamont,4 Pierre-Yves Robert,3 Agnes Lézin4
1Department of Ophthalmology, University Hospital of Martinique, Fort de France, French West Indies, France; 2Department of Ophthalmology, University Hospital of Guadeloupe, Pointe à Pitre, French West Indies, France; 3Department of Ophthalmology, University Hospital of Limoges, France; 4Department of Genetics, University Hospital of Martinique, Fort de France, French West Indies, France
Correspondence: Harold Merle, Department of Ophthalmology, University Hospital of Martinique, Hôpital Pierre Zobda Quitman, BP 632, Martinique, Fort de France, 97261 Cedex, French West Indies, France, Tel +596 596 552 251, Fax +596 596 758 447, Email [email protected]
Purpose: To evaluate how the HLA genotype is associated to the polypoidal choroidal vasculopathy (PCV) in a population of patients of Afro-Caribbean descent.
Methods: Forty-seven patients were diagnosed with PCV. The number of control patients was 457. All affected patients and control patients were of Afro-Caribbean descent and natives to Martinique. HLA typing was based on blood sample, using the polymerase chain reaction technique. Comparison of HLA alleles between the 2 groups was done using chi-2 test, odds ratio (OR) and confidence interval using Woolf’s method. The Bonferroni correction was considered significant when p-value ≤ 0.05. Alleles frequency was analyzed for DRB1 and DQB1 locus.
Results: HLA-DRB1*13 allele was significantly associated to PCV (OR = 2.02, CI = [1.3; 3.13], p = 0.003). In group DRB1, the Bonferroni correction significance threshold was < 0.004. HLA-DQB1*04 allele was significantly associated to PCV (OR = 3.5, CI = [1.48; 8.3], p = 0.006). In group DQB1, the Bonferroni correction significance threshold was < 0.006.
Conclusion: Two HLA alleles are positively associated to PCV. The possible association between PCV and certain alleles suggest HLA implication in PCV pathogeny, most likely by modeling the immune system response.
Keywords: polypoidal choroidal vasculopathy, major histocompatibility complex, human leucocyte antigen, genetic predisposition
Introduction
Polypoidal choroidal vasculopathy (PCV) is characterized by an abnormal branching vascular network (BVN), of which some ramifications are the set of aneurysms or polypoidal dilatations. Its evolution is characterized by the onset of recurring serous or hemorrhagic detachments of the retinal pigment epithelium (RPE) or retina, often with hard exudates, drusen and under retinal fibrosis.1 PCV diagnosis is based on indocyanine green angiography which allows the visualization of the polyps, in the shape of rounded hyper fluorescent lesions, from the early stages. BVN finding is not constant. Swept-source imaging often shows an increased choroidal thickness (> 300µm) associated with pachyvessels.2 OCT angiography confirms the set of polyps and BVN to be located between the RPE and the Bruch membrane.3 PCV is a chronic disease of which the multiple exudative or hemorrhagic macular recurrences can lead to severe loss of visual function.4
PCV’s etiology is unknown, nevertheless certain clinical elements, such as an overwhelming feminine predominance, higher prevalence among Black or Asian patients, different repartition of polyps depending on ethnic origin, and several familial observations suggest a genetic origin.5–9 A recent meta-analysis of Asian patients identified 31 susceptibility single nucleotide polymorphisms (SNPs) (for 10 genes/loci) linked to PCV.10
Human leucocyte antigen (HLA) system is the major histocompatibility complex (MHC). It is at the heart of the immune response. HLA molecules of class I are HLA-A, -B and -C. HLA molecules of class II are HLA-DR, -DQ and -DP. Class I molecules have a ubiquitous distribution while class II molecules have a more restricted distribution on cells presenting antigens. Class I and II molecules are normally present in the retina’s glial cells. Vascular endothelium, particularly ocular, are rich in molecules of class II.11 HLA genes which code for the HLA system are located on the short arm of chromosome 6. The HLA region contains the highest quantity of polymorphs genes of the whole human genome. More than 15.000 alleles have been described (http:/www.ebi.ac.uk/imgt/hla/). Alleles’ frequency varies between ethnic population.12,13 The HLA system is involved in the age-related macular degeneration (AMD) physiopathology, for which immune or inflammatory origin is suspected. Several studies of the HLA system were conducted among AMD patients in search for predisposition or resistance factors. All were conducted among Caucasian patients suffering from atrophic or neovascular AMD and allowed to demonstrate a positive or negative association with several alleles.11,14,15 Through the course of AMD, there is a subretinal accumulation of microglial cells and macrophages. Chronic inflammatory reaction, by altering the Bruch membrane and modifying the functioning of the RPE, would favor neovessels appearing. Several pro inflammatory proteins are found in high quantity in drusen (immunoglobulins, protein C reactive, C5 complement activation, C5b-9, C3b …). Immunoreactivity increase of class II HLA molecules on the retina’s vessels is noted in case of pigmentary alterations or drusen.11
PCV and AMD are complex genetic diseases and the identification of patients at risk of progression is crucial. Given their close phenotype, most genes studied for AMD (complement factor H (CFH), age-related maculopathy susceptibility 2 (ARMS2), high-temperature requirement factor A1 (HTRA1) …) are also studied for PCV.10 Nevertheless, no study regarding the HLA system has been done for PCV. We report the genotype results of DRB1 and DQB1 patients of Afro-Caribbean descent suffering from PCV.
Methods
This prospective study was completed in the University Hospital of Martinique from January 1st, 2018 to December 31st, 2019. This study was approved by the institutional review board of the University Hospital of Martinique. Patients’ and controls’ informed consent were obtained for inclusion in the study. This study was conducted in accordance with the Declaration of Helsinki.
For each patient, we collected previous medical and surgical history as well as the history of the disease. Ocular exam consisted of best-corrected visual acuity (measured in Snellen and in Early Treatment Diabetic Retinopathy Study (ETDRS)), dilated fundus examination, color fundus photography, fundus autofluorescence imaging, fluorescein and indocyanine green angiography and OCT. Retinal imaging was done using the Spectralis HRA-OCT (Heidelberg Engineering, Heidelberg, Germany). Using clinical data and imaging results, the PCV diagnosis was given by ophthalmologists who specialize in retinal diseases. We included all our patients that matched the diagnostic criteria of the Japanese Study Group of Polypoidal Choroidal Vasculopathy.16,17 PCV diagnosis relied on presence of hyper subretinal fluorescence in the beginning of indocyanine green angiography associated with at least one of the following criteria: presence of nodular lesion(s) at fundus exam, halo hypo fluorescent around the polyp, abnormal BVN, throbbing filling of the polyp, subretinal nodule marching the hypercyanescence and hemorrhagic macular lesion. Patients of Asian or Caucasian descent were excluded.
Case control patients’ group was composed of voluntary blood or organ donors of the University Hospital of Martinique. All case control patients (n=457) were from Martinique and representative of the population, descendants of melanodermas Africans and Caucasian French subjects. We excluded Caucasian and Asian subjects. Case control patients were not related and without previous medical or surgical history.19
HLA typing was determined using blood sample and polymerase chain reaction technique (PCR). After DNA extraction, HLA typing of class II was established with PCR-Sequence Specific Oligonucleotide using typing test LABType®XR and CWD (One Lambda, CA 91303–2801 USA). Target DNA (20ng/µL) was amplified in amplificator ABI Applied Biosystems® Thermocycleur 9700 (Fisher Scientific SAS, France) using a mix of amerces with HLA specific sites (amplification amerces), D-mix (mix of amplification tampon solution) and Taq polymerase (OLI TAQ30, TAQ50 and TAQ75, One Lambda, CA 91303–2801 USA). A separation on electrophoresis gel was done to verify the proper functioning of the amplification. The PCR product was biotinylated, allowing to detect it with streptavidin along with phycoerythrin-R pigment (Fisher Scientific SAS, France). It was then denatured and neutralized using adapted tampon solutions. DNA was then hybrid with complementary sondes conjugate with coded fluorescent microspheres. Revelation was done through measure and analysis of the intensity of the pigment phycoerythrin-PE fluorescence fixed to each microsphere by cytometry of flux LABScan 3D® (One Lambda, CA 91303–2801 USA) with analysis software (HLA Fusion 4.0). An allele is designed by the locus to which it belongs followed by an asterisk (*) then by 2 numbers to designate allelic specificity.18
In each group, we calculated the number and frequency of alleles. The comparison of HLA alleles frequencies between the 2 groups was done using chi-2 test, Odds Ratio (OR) and confidence interval with Woolf’s method. Significant threshold for p-values was ≤ 0.05.20 The Bonferroni correction was considered significant when p-value ≤ 0.05.
Results
All affected patients were of Afro-Caribbean descent and natives to Martinique. Forty-seven patients suffering from PCV were selected. Average age was 78.8 ± 7.5 years old. Patients were as follow: 50–59 years old: 1, 60–69 years old: 9, 70–79 years old: 15, 80–89 years old: 20, >90 years old: 2. Average follow up time was 10 ± 3 years. There were 30 women and 17 men, for a sex ratio women/men of 1.8. The number of studied eyes was 94. Forty-two eyes (44.68%) had visual acuity lower than 20/200, 29 eyes (30.85%) between 20/200 and 20/40 and 23 eyes (24.47%) superior to 20/40. Twenty-three patients (85.7%) had bilateral involvement. In all cases, 47 patients (94 eyes) showed polyps outside of the macular area in both indocyanine green angiography and OCT. Polyps were interpapillomacular in 11 eyes (12%), peripapillary in 50 eyes (53%), peripheric in 29 eyes (31%). They were extramacular in 77 eyes (81%) and extramacular and macular in 17 eyes (19%). None of the patients had strong myopia or hypermetropia of more than 6 diopter counts. Thirteen (27%) were diabetic and 12 (25%) had hypertension. None of the patients smoked. Five (5.3%) eyes had been treated with intravitreal anti-vascular endothelial growth factor therapy. Fifteen (16%) eyes had been treated with thermal laser photocoagulation. Five (5%) had been treated with intravitreal anti-vascular endothelial growth factor therapy and photodynamic therapy. Seventy (74%) eyes had not been treated.
Our PCV population had 3 familial observations: 2 sisters suffering on both eyes aged 72 and 80 years old, and 2 brothers suffering on both eyes aged 77 and 79 years old. The third observation was among 2 brothers suffering on both eyes aged 78 and 82 years old, the clinical characteristics were reported in a previous publication on the first described familial observation of PCV.6
Alleles frequency was analyzed for DRB1 and DQB1 locus. Results of the DRB1 association are shown in Table 1. HLA-DRB1*13 allele was significantly associated to PCV (OR=2.02, CI=[1.3; 3.13], p=0.003). In the DRB1 group, the Bonferroni correction significance threshold was <0.004. Results of the DQB1 association are shown in Table 2. HLA-DQB1*04 allele was significantly associated to PCV (OR=3.5, CI=[1.48; 8.3], p=0.006). In the DQB1 group, the Bonferroni correction significance threshold was <0.006.
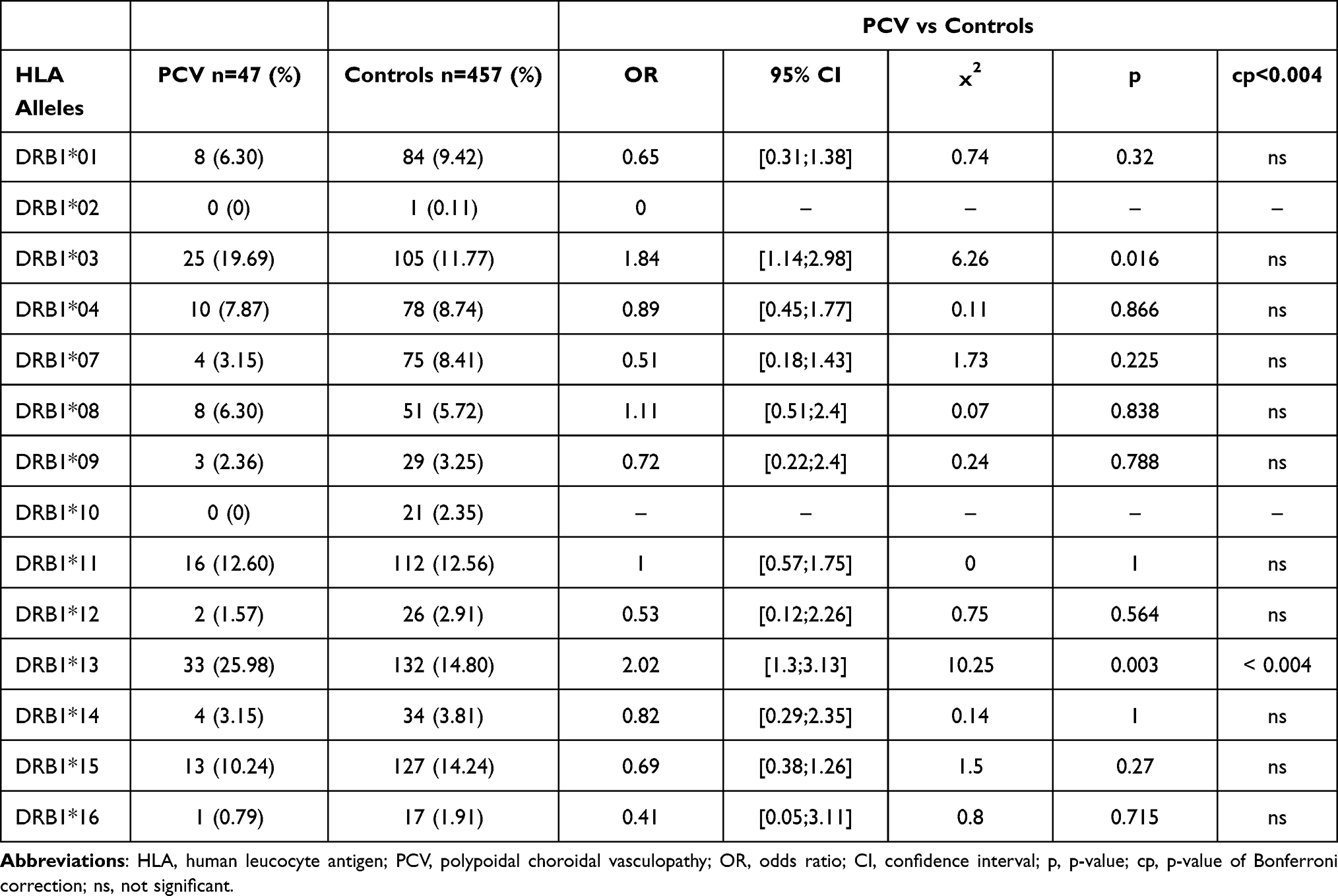 |
Table 1 Frequency and Measure of DRB1 Allele Association |
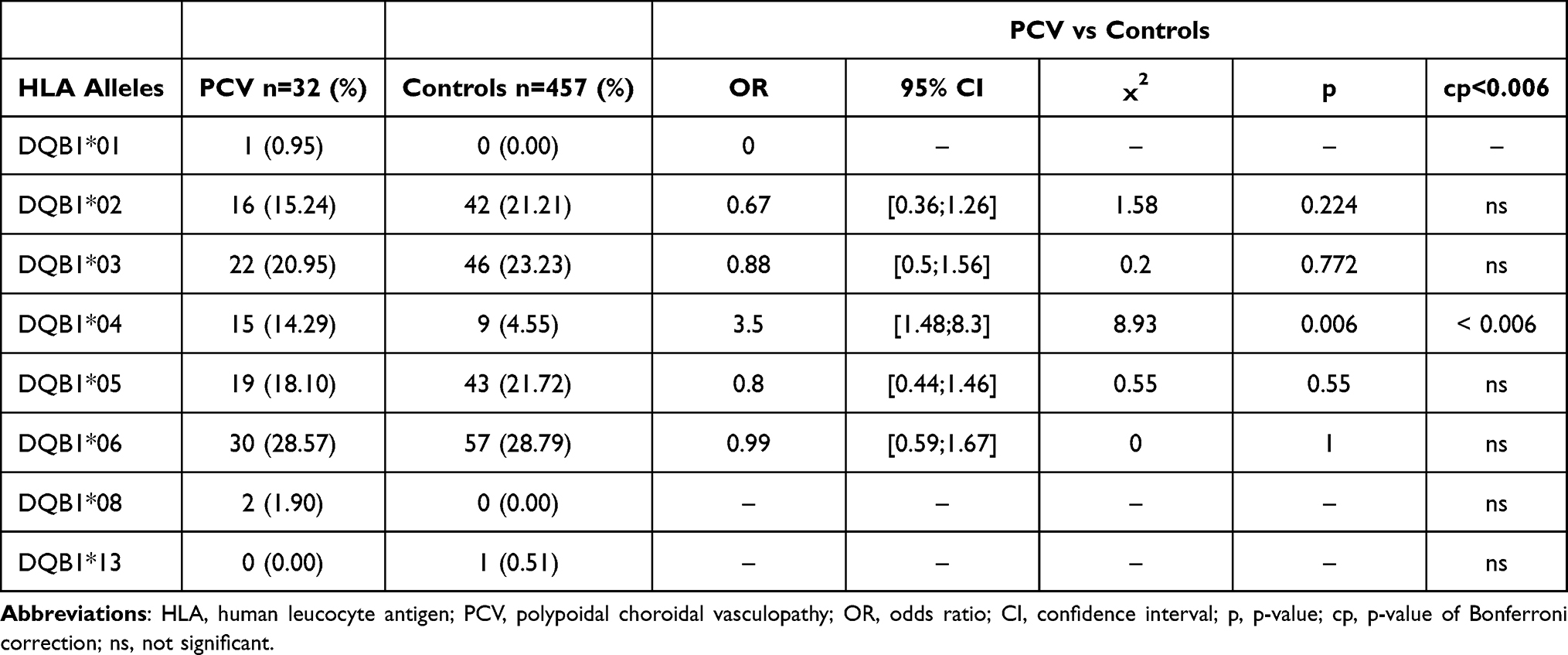 |
Table 2 Frequency and Measure of DQB1 Allele Association |
Discussion
This is the first study of the HLA system among PCV patients. Our study pertains to a homogeneous population of Afro-Caribbean descent, both from a clinical and ethnic standpoint. We found 2 alleles positively associated to PCV: allele HLA-DRB1*13 and allele HLA-DQB1*04.
Our study does not include a control group with neovascular AMD patients, because the number of neovascular AMD in Martinique is really small. Martinique has a population of about 368,000 inhabitants, descendants of various populations, American Indian, African, European, and Indian that have lived in the area throughout history. At least 80% of the population is of African descent. Percentage of Caucasian population in the Caribbean is between 8 and 10%. AMD prevalence (atrophic and neovascular) in Caucasian population 60 and over is estimated to be 2.6%, it is much less in melanoderma population, about 0.3%.21
We were careful to only include in our PCV population patients which polyps’ location would not lead to confusion with neovascular type 1 AMD. Matter of fact, in all cases, the 47 patients (94 eyes) showed polyps outside of the macular area with both indocyanine green angiography and OCT. PCV in melanoderma population is for us a separate disease from AMD. Besides the disposition of the polyps outside of the macular area, the centripetal evolution of retinal detachment and/or of the RPE lead to a functional deficit much more severe than what is usually observed in AMD.4
The AMD, which shares several semiology elements with PCV, has been the subject of several studies of the HLA system in search for predisposition or resistance factors. In a study done in Spain, which pertained to 75 patients suffering from neovascular AMD, Villegas Becerril et al found a positive association with allele HLA-B27 (OR=2.9, p=0.0113). Like in our study, HLA-DRB1*13 was the most frequent allele (13.33%) but did not increase significantly. There was not in this population of Hispanic origin a linkage between alleles HLA-B27 and HLA-Cw0701.22 Jorgenson et al study was done on a population of Caucasian origin and not Hispanic. Total cohort numbers were 4841 cases, of which 987 atrophic AMD, 1148 neovascular AMD and 2796 undefined. HLA-DQB1*02 (OR=1.22, p=3.9x10−10) allele was associated to the overall studied population (4841 cases). HLA-DQB1*0202 (OR=1.26, p=3.8x10−3) allele was associated to atrophic AMD (987 cases). HLA-DRB1*03 (OR=1.31, p=3.1x10−4) allele was associated to neovascular AMD (1148 cases). Thus, among the same population, different clinical forms of AMD were not tied to the same HLA alleles.23 A study, done in the United Kingdom on a Caucasian population by Goverdhan et al, had 200 AMD cases of which 35% were neovascular AMD. In the total population, the authors found a positive association to HLA-Cw*0701 (OR=1.85, p=0.036) allele, and a negative association with HLA-B*4001 (OR=0.39, p=0.027) allele and HLA-DRB1*1301 (OR=0.31, p=0.009) allele.24 Contrary to Goverdhan et al, Pappas et al did not find a negative association with HLA-DRB1*1301 in a cohort of women of European origin treated in the United States.25
The role of genetics in PCV pathogeny is finalized by highlighting the multiple associated variants. Meta-analysis of Ma et al retains 31 polymorphisms for 10 genes/loci significantly associated to PCV.10 These genes are related to extracellular matrix, basement membrane, complement cascade, lipid metabolism, cellular apoptosis, and inflammation. Collected results come for the most part from Asian series essentially Japanese and Chinese. A variant can be associated in the Asian population and not be found in the Caucasian population.25 The 3 main SNPs associated with PCV are rs800292 from the CFH, rs10490924 from ARMS2 and rs11200638 from HTRA1. For rs10490924, OR for homozygotes and heterozygotes was respectively 4.9 and 1.74, suggesting a cumulative genetic effect. Compared to other non-genetic risk factors such as high blood pressure (OR=0.73, p=0.047) or high HDL cholesterol (OR=1.84, p=0.045), the variants’ influence seemed more important with a higher OR (ARMS2: OR=2.53, p<0.001).26–29 HTRA1 transgenic mice developed polypoidal lesions, BVNs, as well as severe degeneration of the elastic laminae and tunica media of choroidal vessels typical of PCV.30
HLA molecules sometimes play a preponderant role of genetic factor of either susceptibility or resistance to several pathologies (Behcet’s disease, birdshot chorioretinopathy, anterior uveitis …). Diseases tied to the HLA system result from several genes interactions with environmental factors.31 Same as with AMD, possible association between PCV and some alleles suggest the implication of the HLA in PCV pathogeny. Indeed, several cellular types (vascular endothelium, uvea, microglial cells …) express HLA molecules that can favor an immune reaction, inflammatory reaction, and the apparition of neovessels, as it was shown throughout the presumed ocular histoplasmosis syndrome.32,33
Recently, several studies have shown that the systemic C-reactive protein (CRP) was elevated among patients suffering from PCV (OR 3.05, 95% CI: 1.56–5.98, p=0.0011), reinforcing the hypothesis of immunitary factor in PCV etiology.34 Thus, Lafaut et al and Terasaki et al described an infiltration of lymphocytes and macrophages around polyps and in the choroid.35,36 In a murine experimental model, Kumar et al showed the presence in the choroid of elastin degradation as well as an exudative reaction tied to complement activation and immune cells activation (Kumar et al).37
Our study’s main limit is that it only concerns HLA DRB1 and DQB1 and that all patients are of Afro-Caribbean descent. Our statistical analysis only includes the Bonferroni correction. We did not use sample replication technique. Furthermore, case control patients were not physically assessed and could suffer from PCV. However, in that case, the association we found between PCV and HLA could be underestimated. Further studies, in other population are require to confirm our results. Like the 3 SNPs tied to PCV (CFH, ARMS2 and HTRA1), our results contributed to identify the genetic basis on which PCV develops.
PCV is a rare disease and on top of that traditional genetic studies are limited because of the late onset of the disease. Indeed, when PCV is diagnosed, patients are often already deceased.38 Two HLA alleles are positively associated to PCV: allele HLA-DRB1*13 and allele HLA-DQB1*04. Besides contributing hypotheses on PCV’s physiopathology, the association between PCV and HLA would allow the definition of at-risk population most likely to develop the disease. In this at-risk population, a regular ocular exam could be performed. Our results cannot alone prove the genetic origin of PCV. Nevertheless, in our opinion they constitute, like the different clinical and epidemiologic characteristics depending on populations, the reveal of associated variants, and the familial observations, an important argument in favor of a genetic component of PCV.
Author Contributions
All authors attest they meet the current ICMJE criteria for Authorship. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article was submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
No funding or grant support.
Disclosure
The authors report no conflicts of interest for this work and have no financial disclosures, financial interest, or conflicting relationship regarding the subject of this paper.
References
1. Yannuzzi LA, Sorenso J, Spaide RF, Lipson B. Idiopathic polypoidal choroidal vasculopathy. Retina. 1990;10:1–8. doi:10.1097/00006982-199010010-00001
2. Dansingani KK, Balaratnasingam C, Naysan J, Freund KB. En face imaging of pachychoroid spectrum disorders with swept-source optical coherence tomography. Retina. 2016;36:499–516. doi:10.1097/IAE.0000000000000742
3. Wang M, Zhou Y, Gao SS, et al. Evaluating polypoidal choroidal vasculopathy with optical coherence tomography angiography. Invest Ophthalmol Vis Sci. 2016;57:526–532. doi:10.1167/iovs.15-18955
4. Palkar AH, Khetan V. Polypoidal choroidal vasculopathy: an update on current management and review of literature. Taiwan J Ophthalmol. 2019;9:72–92.
5. Machida S, Takahashi T, Gotoh N, Yoshimura N, Fujiwara T, Kurosaka D. Monozygotic twins with polypoidal choroidal vasculopathy. Clin Ophthalmol. 2010;4:793–800. doi:10.2147/OPTH.S11003
6. Merle H, Donnio A, Richer R, Jean-Charles A. Familial bilateral polypoidal choroidal vasculopathy. Retin Cases Brief Rep. 2008;2:181–183. doi:10.1097/IAE.0b013e31802be7a3
7. Stern RM, Zakov N, Zegarra H, Gutman FA. Multiple recurrent serosanguineous retinal pigment epithelial detachments in black women. Am J Ophthalmol. 1985;100:560–569. doi:10.1016/0002-9394(85)90682-8
8. Wong CW, Wong TY, Cheung CM. Polypoidal choroidal vasculopathy in Asians. J Clin Med. 2015;4:782–821. doi:10.3390/jcm4050782
9. Yannuzzi LA, Ciardella A, Spaide RF, Rabb M, Freund KB, Orlock DA. The expanding clinical spectrum of idiopathic polypoidal choroidal vasculopathy. Arch Ophthalmol. 1997;115:478–485. doi:10.1001/archopht.1997.01100150480005
10. Ma L, Li Z, Liu K, et al. Association of genetic variants with polypoidal choroidal vasculopathy. A systematic review and updated meta-analysis. Ophthalmology. 2015;122:1854–1865. doi:10.1016/j.ophtha.2015.05.012
11. Penfold PL, Liew SC, Madigan MC, Provis JM. Modulation of major histocompatibility complex class II expression in retinas with age-related macular degeneration. Invest Ophthalmol Vis Sci. 1997;38:2125–2133.
12. Klein J, Sato A. The HLA system. First of two parts. N Engl J Med. 2000;343:702–709. doi:10.1056/NEJM200009073431006
13. Klein J, Sato A. The HLA system. Second of two parts. N Engl J Med. 2000;343:782–786. doi:10.1056/NEJM200009143431106
14. Stanton CM, Wright AF. Inflammatory biomarkers for AMD. Adv Exp Med Biol. 2014;801:251–257.
15. Hageman LPJ, Victor Chong NH, Johnson LV, Anderson DH, Mullins RF. An integrated hypothesis that considers drusen as biomarkers of immune-mediated processes at the RPE-Bruch’s membrane interface in aging and age-related macular degeneration. Prog Retin Eye Res. 2001;20:705–732. doi:10.1016/S1350-9462(01)00010-6
16. Tan CS, Ngo WK, Chen JP, Tan NW, Lim TH. Everest study report 2: imaging and grading protocol, and baseline characteristics of a randomised controlled trial of polypoidal choroidal vasculopathy. Br J Ophthalmol. 2015;99:624–628. doi:10.1136/bjophthalmol-2014-305674
17. Japanese Study Group of Polypoidal Choroidal Vasculopathy. Criteria for diagnosis of polypoidal choroidal vasculopathy. Nippon Ganka Gakkai Zasshi. 2005;109:417–427.
18. Marsh SG, Albert ED, Bodmer WF, et al. Nomenclature for factors of the HLA system, 2004. Hum Immunol. 2005;66:571–636. doi:10.1016/j.humimm.2005.02.002
19. Béra O, Césaire R, Quelvennec E, et al. HLA class I and class II allele and haplotype diversity in Martinicans. Tissue Antigens. 2001;57:200–207. doi:10.1034/j.1399-0039.2001.057003200.x
20. Largen CE, Alper CA. The genetics of HLA-associated disease. Curr Opin Immunol. 2004;16:660–667. doi:10.1016/j.coi.2004.07.014
21. Klein R, Chou CF, Klein B, Zhang X, Meuer SM, Saaddine JB. Prevalence of age-related macular degeneration in the US population. Arch Ophthalmol. 2011;129:75–80. doi:10.1001/archophthalmol.2010.318
22. Villegas Becerril E, Gonzalez Fernadez R, Pérula Torres L, et al. HLA-B27 as predisposition factor to suffer age related macular degeneration. Cell Mol Immunol. 2009;6:303–307. doi:10.1038/cmi.2009.40
23. Jorgenson E, Melles RB, Hoffmann TJ, et al. Common coding variants in the HLA-DQB1 region confer susceptibility to age-related macular degeneration. Eur J Hum Genet. 2016;24:1049–1055. doi:10.1038/ejhg.2015.247
24. Goverdhan SV, Howell MW, Mullins RF, et al. Association of HLA class I and class II polymorphisms with age-related macular degeneration. Invest Ophthalmol Vis Sci. 2005;46:1726–1734. doi:10.1167/iovs.04-0928
25. Pappas D, Hollenbach J, Coleman AL, et al. HLA class II genotypes are not associated with age related macular degeneration in a case-control, population-based study. Hum Immunol. 2015;76:142–145. doi:10.1016/j.humimm.2015.01.010
26. Yuan D, Yang Q, Liu X, et al. Complement factor H Val62Ile variant and risk of age-related macular degeneration: a meta-analysis. Mol Vis. 2013;19:374–383.
27. Chen H, Liu K, Chen LJ, et al. Genetic associations in polypoidal choroidal vasculopathy: a systematic review and meta-analysis. Mol Vis. 2012;18:816–829.
28. Hayashi H, Yamashiro K, Gotoh N, et al. CFH and ARMS2 variations in age-related macular degeneration, polypoidal choroidal vasculopathy, and retinal angiomatous proliferation. Invest Ophthalmol Vis Sci. 2010;51:5914–5919. doi:10.1167/iovs.10-5554
29. Cheung CM, Laude A, Yeo I, et al. Systemic, ocular and genetic risk factors for age-related macular degeneration and polypoidal choroidal vasculopathy in Singaporeans. Sci Rep. 2017;7:41386. doi:10.1038/srep41386
30. Jones A, Kumar S, Zhang N, et al. Increased expression of multifunctional serine protease, HTRA1, in retinal pigment epithelium induces polypoidal choroidal vasculopathy in mice. Proc Natl Acad Sci USA. 2011;108:14578–14583. doi:10.1073/pnas.1102853108
31. Thorsby E, Lie BA. HLA associated genetic predisposition to autoimmune diseases: genes involved and possible mechanisms. Transpl Immunol. 2005;14:175–182. doi:10.1016/j.trim.2005.03.021
32. Abi-Hanna D, Wakefield D, Watkins S. HLA antigens in ocular tissues. I. In vivo expression in human eyes. Transplantation. 1988;45:610–613. doi:10.1097/00007890-198803000-00021
33. Dabil H, Kaplan HJ, Duffy BF, Phelan D, Mohanakumar T, Jaramillo A. Association of the HLA-DR15/HLA-DQ6 haplotype with development of choroidal neovascular lesions in presumed ocular histoplasmosis syndrome. Human Immunol. 2003;64:960–964. doi:10.1016/S0198-8859(03)00175-7
34. Borgersen NJ, Moller-Lorentzen T, Sorensen TL, Subhi Y. Association between C-reactive protein and polypoidal vasculopathy: a systematic review and meta-analysis. Acta Ophthalmol. 2021;99:470–477. doi:10.1111/aos.14655
35. Lafaut BA, Aisenbrey S, Van den Broecke C, Bartz-Schmidt KU, Heimann K. Polypoidal choroidal vasculopathy pattern in age-related macular degeneration: a clinicopathologic correlation. Retina. 2000;20:650–654. doi:10.1097/00006982-200011000-00010
36. Terasaki H, Miyake Y, Suzuki T, Nakamura M, Nagasaka T. Polypoidal choroidal vasculopathy treated with macular translocation: clinical pathological correlation. Br J Ophthalmol. 2002;86:321–327. doi:10.1136/bjo.86.3.321
37. Kumar S, Nakashizuka H, Jones A, et al. Proteolytic degradation and inflammation play critical roles in polypoidal choroidal vasculopathy. Am J Pathol. 2017;187:2841–2857. doi:10.1016/j.ajpath.2017.08.025
38. Yannuzzi LA, Wong DW, Sforzolini BS, et al. Polypoidal choroidal vasculopathy and neovascularized age-related macular degeneration. Arch Ophthalmol. 1999;117:1503–1510. doi:10.1001/archopht.117.11.1503
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.