Back to Journals » Infection and Drug Resistance » Volume 12
Clarithromycin-Susceptible But Virulent Helicobacter pylori Strains Infecting Iranian Patients’ Stomachs
Authors Khani S, Talebi Bezmin Abadi A ![]() , Mohabati Mobarez A
, Mohabati Mobarez A ![]()
Received 17 July 2019
Accepted for publication 24 October 2019
Published 1 November 2019 Volume 2019:12 Pages 3415—3420
DOI https://doi.org/10.2147/IDR.S223602
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Shadiyeh Khani, Amin Talebi Bezmin Abadi, Ashraf Mohabati Mobarez
Department of Bacteriology, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran
Correspondence: Amin Talebi Bezmin Abadi
Department of Bacteriology, Faculty of Medical Sciences, Tarbiat Modares University, Tehran 14115-111, Iran
Tel +98 21 8288 4883
Email [email protected]
Introduction: Helicobacter pylori was discovered first in the stomachs of patients with gastritis and ulcers by Marshall and Warren in 1982. This discovery majorly affected many research areas of gastroenterology. Since then, the main aim has been to eradicate this microaerophilic bacterium from the stomachs of infected subjects.
Methods: We studied symptomatic cases by endoscopic surgery and examined the prevalence of cagA–vacA genotypes among the H. pylori isolates. H. pylori isolated from antral biopsies of patients with gastritis and duodenal ulcer were subjected to antimicrobial susceptibility testing and PCR genotyping by using routine bacterial cultures. Clarithromycin-susceptibility profiling was done by the E-test. DNA was extracted using standard manufacturer protocols with minor modifications and cagA and vacA genotyping was done PCR.
Results: In our study, all strains identified as H. pylori in culture (61/81) were confirmed by PCR by amplifying a fragment of the glmM gene. Totally, 61 patients were confirmed to be positive for H. pylori and they were included in the genotyping and antibiotic-susceptibility testing. Thirteen H. pylori strains were determined to be resistant to clarithromycin.
Discussion: Current accumulating data indicate that both clarithromycin-resistant and susceptible isolates of H. pylori need to be screened and tracked in populations.
Keywords: antibiotic susceptibility, cagA, clarithromycin, E-test, Helicobacter pylori, genotypes, PCR, vacA
Introduction
Helicobacter pylori is a well-known bacteria, colonization of which inevitably causes gastroduodenal diseases, including chronic and atrophic gastritis, peptic ulcer disease, mucosa-associated lymphoid tissue lymphoma, and gastric adenocarcinoma.1–3 Because the incidence of digestive diseases associated with H. pylori can vary in different geographical regions, we may postulate that reported cases are dictated by other factors such as bacterial virulence. Virulent strains of H. pylori are generally accepted to cause severe digestive diseases and potentially genetically carry virulence factors.4–6
Furthermore, the discovery that peptic ulcers and acute gastritis can be treated efficiently by antibiotics was an important breakthrough in this century.7,8 Therefore, finding the best effective antibiotic therapy for H. pylori isolates specific to various regions is highly desirable.9 The recent Maastricht guideline was calling for treating all symptomatic H. pylori-infected individuals.10 Broadly defined, three main reasons affect the efficacy of the recommended antibiotics therapies against this persistent bacterium; these include high bacterial load, poor patient compliance, and emergence of antibiotics resistance.11 Among them, emergence of antibiotics resistance is an undeniable factor.12,13 Proton-pump inhibitors (PPI)-clarithromycin containing triple therapy without prior susceptibility testing should be abandoned when the clarithromycin resistance rate in the region is more than 15%. In areas of high (>15%) clarithromycin resistance, bismuth quadruple or non-bismuth quadruple, concomitant (PPI, amoxicillin, clarithromycin and a nitroimidazole) therapies are recommended.14 In areas of high dual clarithromycin and metronidazole resistance, bismuth quadruple therapy (BQT) is the recommended first-line treatment. In the case of allergic reactions, metronidazole can substitute amoxicillin. Moreover, clarithromycin resistance reportedly decreases the efficacy of therapy by more than 80%.15–17 In reality, clarithromycin is a pivotal component in the treatment of H. pylori infection, but the probability of therapeutic failure is relatively high if the resistance rate is more than 15% in the population.17,18 In addition, clarithromycin is readily available as a proposed treatment to eradicate H. pylori efficiently in symptomatic individuals.19 The global resistance rate to clarithromycin has become alarming, and the World Health Organization (WHO) has warned against uncontrolled application of this key antibiotic under clinical settings.20 The main purpose of our survey is to determine the prevalence of certain virulence factors (cagA and vacA) among clarithromycin-susceptible and clarithromycin-resistant H. pylori strains obtained from symptomatic Iranian patients and to investigate likely significant associations.
Materials And Methods
Sample Collection
This is a cross-sectional study conducted from August 2017 to August 2018. All patients, who were referred for upper gastrointestinal endoscopy at Imam-Hossein Hospital, Tehran, Iran, were enrolled. Three antral biopsy samples were taken from each patient for further analysis. The first biopsy sample was sent for histopathological examination; the second one was used for urease assay (Bahar-Azma, Tehran, Iran); and the last sample was placed in a small 1.5-mL tube containing the thioglycollate broth medium and kept at 4°C for bacterial culturing. The last biopsy samples were processed for bacterial culturing within 4 h of endoscopy. Exclusion criteria included age under 17 or over 80 years, severe cardiovascular diseases, antibiotic therapy against H. pylori 2 months before endoscopy, pregnancy, bleeding problems, history of abdominal surgery a year before endoscopy, alcohol consumption 2 months before biopsy, and consumption of 1) nonsteroidal anti-inflammatory drugs 2) proton-pump inhibitors (PPI), or 3) bismuth a month before enrolment in the study. The study was first presented to, and approved by, the ethics committee of Tarbiat Modares University, Tehran, Iran (IR.TMU.REC. 1397.071), and all patients gave their written informed consent forms to participate before participation. Patients were free to join or leave the study at any time. Additionally, all documents about patients’ endoscopic findings and pathology results were codified and kept confidential.
Bacterial Isolation
All biopsy specimens were first mixed by a vortex for 50 s, and then 150 µl of homogenized suspension was streaked on Brucella agar plates enriched with 10% fetal bovine serum, 8% defibrinated caprine blood, and antibiotics (Selectab, MAST, UK). Plates were incubated at 37°C for 7–12 days under microaerophilic conditions (5% O2, 10% CO2, and 85% N2).21,22 After incubation, translucent, grey and small colonies grew and confirmed by biochemical tests (for oxidase, urease, and catalase) to positively identify H. pylori. Moreover, microscopy was used to confirm the bacterial identity by observing typical characteristics, including curved rods and Gram-negative staining.23,24 After confirming the identification, typical colonies were harvested and stored at −80°C in brain heart infusion growth medium containing 20% glycerol until further analysis.25
Antimicrobial Susceptibility Tests
In this assay, clarithromycin-susceptibility profile of confirmed H. pylori stocks was determined by using the E‐test (AB Biodisk, Sweden). First, we have checked that the new plates did not have any contamination and then we placed an E-test strip on the surface of a plate.23 Following 5–7 days of incubation at microaerophilic conditions at 37°C and with 95% humidity, we rechecked plates to determine zones of inhibited growth. The minimum inhibitory concentration (MIC) for clarithromycin was determined by the E-test following the manufacturer’s instructions but with minor modifications. Strains were considered resistant when MIC was >0.05 μg/mL for clarithromycin.23 Randomly, 10% of all isolates were selected for double-checking the first reported findings by a second operator.
DNA Extraction And Genotyping
Typical H. pylori colonies were carefully harvested, and DNA was extracted using a commercial kit according to the manufacturer’s instructions (CinnaGen, Tehran, Iran). Extracted DNA was stored at −20°C for further analysis. glmM was used for genetic confirmation of H. pylori besides previous biochemical tests.26 To determine the genotype of the resistant or susceptible strains, we used previously reported primers with minor changes.27 Table 1 shows the primer sets used for PCR; distilled water was used as the negative control replacing the DNA template. To determine the positive or negative results, we subsequently subjected the PCR products (at least 4 μl) to electrophoresis on 1% agarose gels (Sina-clon, Tehran, Iran), and visualized the PCR products by a UV transilluminator (Biometra, Germany).
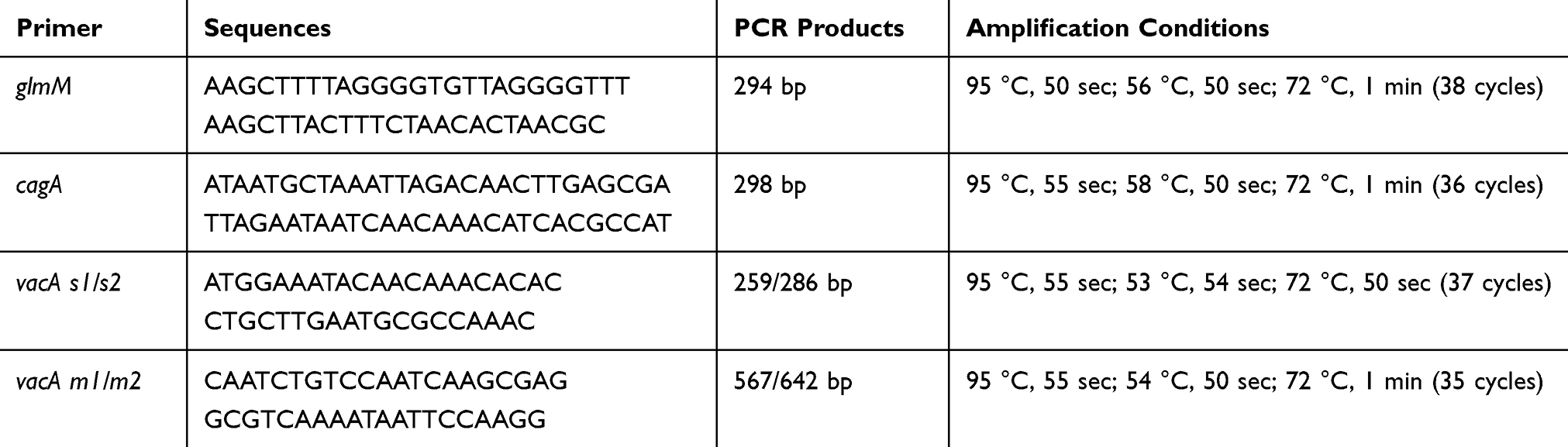 |
Table 1 Primer Sequences And Associated Amplification Conditions |
Statistical Analyses
A chi-square test was used to analyze the possible association between resistance status and particular genotypes (cagA and vacA). All measurements of significance were two-tailed with P < 0.05.
Results
Twenty-eight men and 33 women, with a mean age of 56.8 years (range, 21–73) were included. No statistically significant differences were found between age and gender of patients with H. pylori antibiotic resistance (P < 0.05). In our study, clarithromycin resistance rate was 21% (n = 13/61). Sixty-one out of 81 patients with duodenal ulcer, gastric ulcer and gastritis were recognized to be infected with H. pylori strains. Indeed, we discard the 20 samples due to lack of enough data from patients, or their disapproval to participate. Nevertheless, positive routine bacterial cultures, classic biochemical tests, and PCR amplification of glmM were used to identify the 61 positive cases. Generally, PCR for glmM detected 61 out of the 61 (100%) confirmed culture samples, indicating reliability and consistency of the two approaches.
Distribution Of H. pylori cagA And vacA
In total, 65% (n = 40/61) of the H. pylori strains were cagA-positive. The prevalence of vacA alleles were s1/m1 at 40% (n = 25/61), s1/m2 at 21% (n = 13/61), s2/m1 at 14% (n = 9/61), s2/m2 at %22 (n = 14/61). No statistical association was found between vacA alleles and gastroduodenal diseases (P > 0.05). The current genotyping on all the 61 H. pylori strains demonstrated that vacAS1M1 (the most virulent genotype based on vacA) was the predominant genotype in our study with no significant statistical discrepancy observed among the different disease diagnoses (P > 0.05). Distribution of the combined cagA and vacA genotypes of H. pylori among different diagnoses are summarized in Table 2.
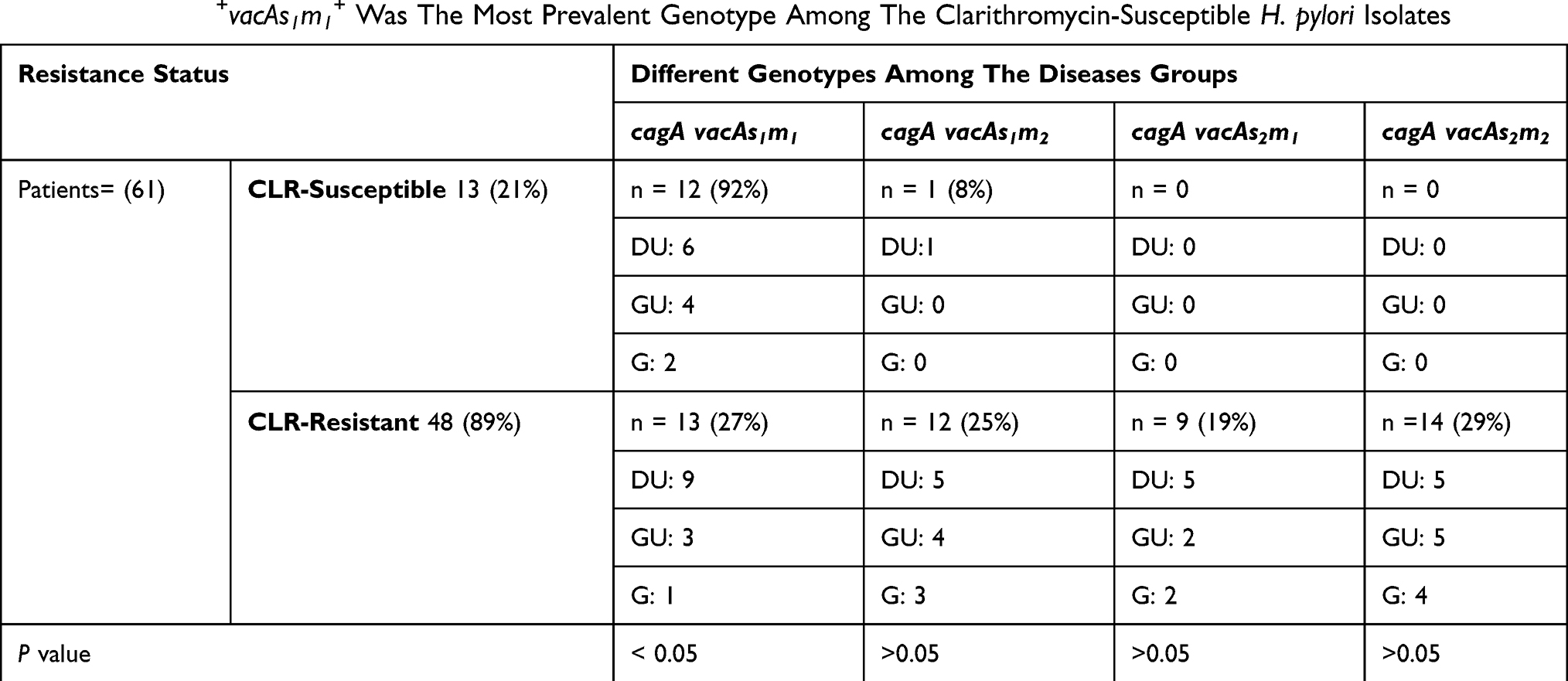 |
Table 2 The cagA+vacAs1m1+ Was The Most Prevalent Genotype Among The Clarithromycin-Susceptible H. pylori Isolates |
Combination Of Susceptibility Profile With H. pylori cagA-vacA Genotypes
As shown in Table 2, clarithromycin-susceptible H. pylori isolates carried the cagA+ vacAs1m1+ genotype; this association was statistically significant (P < 0.05). The H. pylori cagA− vacAs1m2− genotype, as the less virulent strain, did not associate with the resistance phenotype (P > 0.05).
Discussion
Reportedly, H. pylori has colonized 50% of the world population.28 The capacity of H. pylori to cause successful infections is affected by certain elements, which include carrying virulence factors, emergence of antibiotics resistance, and genetic vulnerability in the host.29 Despite identification of H. pylori as the causative agent of various gastritis, designing the best standard therapy to eradicate this bacterium is still in infancy stages.30 From a biological point of view, the antibiotics-resistant H. pylori strains may have a higher chance to survive and propagate in human gastric microniches; hence, expecting certain virulence types among those pathogenic strains is plausible.31,32 The main rationale for this research was based on this phenomenon that humans may harbor some H. pylori strains that carry virulence elements while they are also resistant to antibiotics. Among the Iranian population, H. pylori clarithromycin resistance is almost as high as 21%, which agrees with other parallel analyses.33–35 However, a fundamental discord exists regarding the positivity of cagA and vacA alleles among the H. pylori strains. Our investigation for the first time has shown that clarithromycin-susceptible H. pylori strains carried the most virulent profile (cagA+vacAs1m1+). Importantly, some studies, such as that by Alarcón-Millán et al conducted in Mexico, reported no association between any virulence genotypes and clarithromycin-susceptibility patterns.36 However, this major difference can be explained by geographical differences between Iran and Mexico. Moreover, we have found that 65% of the H. pylori strains are cagA-positive. The H. pylori cagA-positivity rate agrees with the rates reported in other studies, at least in Iran.37–40 Little is known about any association between this virulence factor and clarithromycin susceptibility. Here, we showed, for the first time, that all most-virulent H. pylori strains are not clarithromycin-resistant, a report which should be seriously considered by gastroenterologists for better insight into treating this persistent microorganism. A multicenter study, including patients from different geographical regions, should be conducted to confirm our findings.
The main aim now is to eradicate this bacterium from the stomachs of symptomatic individuals; however, little is known about symptomatic patients likely infected by strains with antibiotics-susceptible profile. Such virulent strains (e.g., cagA and vacA) are more capable to induce acute inflammation with increased chance of causation of severe gastroduodenal diseases. In other words, we expect that H. pylori isolates representing the resistance genotypes have a higher chance to survive (according to the natural selection phenomena); thus, basically, they should have a quite different profile of virulence in comparison with antibiotics-susceptible isolates. Our study’s limitations include: 1) relatively small number of subjects for antibiotic resistance analysis and 2) short period of time to investigate the clarithromycin susceptibility among H. pylori isolates. Indeed, we had only 1 year to analyze the subjects and assess the two virulent genotypes among both susceptible and resistant H. pylori isolates. Another basic limitation of our study is that we have not checked other virulence factors that may be associated with resistance. However, Alarcón-Millánet al used babA2 as another possible virulence factor, but they have found no statistically significant association between resistance and cagA genotypes. At last, we were unable to check treatment failure among the patients who utilized clarithromycin within different therapeutic regimens. Indeed, more studies with larger sample sizes could facilitate thorough investigation of the relationship between virulent strains and susceptible H. pylori strains.
Conclusion
We found that some clarithromycin-susceptible H. pylori strains carry the virulent genotype, cagA+vacAs1m1+, and this can exacerbate the management of this persistent microorganism. Cumulative data indicate that both clarithromycin-resistant and clarithromycin-susceptible isolates of H. pylori need to be screened and tracked in regional populations. Thus, even the clarithromycin-susceptible H. pylori isolates should not be underestimated in the clinics.
Ethics
Our study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
This study was financially supported by research deputy of Tarbiat Modares University, Tehran, Iran. We would like to thank Dr Farid Rahimi (The Australian National University) for constructive comments and help with English editing of this manuscript.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Suerbaum S, Michetti P. Helicobacter pylori infection. N Engl J Med. 2002;347(15):1175–1186. doi:10.1056/NEJMra020542
2. Uemura N, Okamoto S, Yamamoto S, et al. Helicobacter pylori infection and the development of gastric cancer. N Engl J Med. 2001;345(11):784–789. doi:10.1056/NEJMoa001999
3. Yamaoka Y. Mechanisms of disease: helicobacter pylori virulence factors. Nat Rev Gastroenterol Hepatol. 2010;7(11):629. doi:10.1038/nrgastro.2010.154
4. Brennan DE, Dowd C, O’Morain C, McNamara D, Smith SM. Can bacterial virulence factors predict antibiotic resistant Helicobacter pylori infection? World J Gastroenterol. 2018;24(9):971. doi:10.3748/wjg.v24.i9.971
5. Crabtree J, Wessler S. Special Issue “H. pylori Virulence Factors in the Induction of Gastric Cancer. Multidisciplinary Digital Publishing Institute; 2018.
6. Kabamba ET, Yamaoka Y. Helicobacter pylori and related virulence factors for gastrointestinal diseases. Gastr Cancer (Springer). 2019;31–50.
7. Walsh JH, Peterson WL. The treatment of Helicobacter pylori infection in the management of peptic ulcer disease. N Engl J Med. 1995;333(15):984–991. doi:10.1056/NEJM199510123331508
8. den Hoed CM, Kuipers EJ Helicobacter pylori infection. Hunter’s Tropical Medicine and Emerging Infectious Diseases: Elsevier; 2020:476–480.
9. Goderska K, Pena SA, Alarcon T. Helicobacter pylori treatment: antibiotics or probiotics. Appl Microbiol Biotechnol. 2018;102(1):1–7. doi:10.1007/s00253-017-8535-7
10. Malfertheiner P, Megraud F, O’Morain CA, Gisbert JP. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut. 2017;66(1):6–30.
11. Uotani T, Miftahussurur M, Yamaoka Y. Effect of bacterial and host factors on Helicobacter pylori eradication therapy. Expert Opin Ther Targets. 2015;19(12):1637–1650. doi:10.1517/14728222.2015.1073261
12. Thung I, Aramin H, Vavinskaya V, et al. the global emergence of Helicobacter pylori antibiotic resistance. Aliment Pharmacol Ther. 2016;43(4):514–533. doi:10.1111/apt.13497
13. Graham DY. Antibiotic resistance in Helicobacter pylori: implications for therapy. Gastroenterology. 1998;115(5):1272–1277. doi:10.1016/S0016-5085(98)70100-3
14. Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG clinical guideline: treatment of Helicobacter pylori infection. Am J Gastroenterol. 2017;112(2):212. doi:10.1038/ajg.2016.563
15. Fischbach L, Evans E. Meta‐analysis: the effect of antibiotic resistance status on the efficacy of triple and quadruple first‐line therapies for Helicobacter pylori. Aliment Pharmacol Ther. 2007;26(3):343–357. doi:10.1111/apt.2007.26.issue-3
16. Rimbara E, Fischbach LA, Graham DY. Optimal therapy for Helicobacter pylori infections. Nat Rev Gastroenterol Hepatol. 2011;8(2):79. doi:10.1038/nrgastro.2010.210
17. Broutet N, Tchamgoue S, Pereira E, Lamouliatte H, Salamon R, Megraud F. Risk factors for failure of Helicobacter pylori therapy—results of an individual data analysis of 2751 patients. Aliment Pharmacol Ther. 2003;17(1):99–109. doi:10.1046/j.1365-2036.2003.01396.x
18. Malfertheiner P, Megraud F, O’Morain CA, et al. Management of Helicobacter pylori infection—the Maastricht IV/Florence consensus report. Gut. 2012;61(5):646–664. doi:10.1136/gutjnl-2012-302084
19. Federico A, Gravina AG, Miranda A, Loguercio C, Romano M. Eradication of Helicobacter pylori infection: which regimen first? World J Gastroenterol. 2014;20(3):665. doi:10.3748/wjg.v20.i3.665
20. Asokan GV, Vanitha A. WHO global priority pathogens list on antibiotic resistance: an urgent need for action to integrate one health data. Perspect Public Health. 2018;138(2):87–88. doi:10.1177/1757913917743881
21. Miyachi H, Miki I, Aoyama N, et al. Primary levofloxacin resistance and gyrA/B mutations among Helicobacter pylori in Japan. Helicobacter. 2006;11(4):243–249. doi:10.1111/hel.2006.11.issue-4
22. Mendonça S, Ecclissato C, Sartori M, et al. Prevalence of Helicobacter pylori resistance to metronidazole, clarithromycin, amoxicillin, tetracycline, and furazolidone in Brazil. Helicobacter. 2000;5(2):79–83. doi:10.1046/j.1523-5378.2000.00011.x
23. Mégraud F, Lehours P. Helicobacter pylori detection and antimicrobial susceptibility testing. Clin Microbiol Rev. 2007;20(2):280–322. doi:10.1128/CMR.00033-06
24. Tanih NF, McMillan M, Naidoo N, Ndip LM, Weaver LT, Ndip RN. Prevalence of Helicobacter pylori vacA, cagA and iceA genotypes in South African patients with upper gastrointestinal diseases. Acta Trop. 2010;116(1):68–73. doi:10.1016/j.actatropica.2010.05.011
25. Kusters JG, van Vliet AH, Kuipers EJ. Pathogenesis of Helicobacter pylori infection. Clin Microbiol Rev. 2006;19(3):449–490. doi:10.1128/CMR.00054-05
26. Jafari F, Shokrzadeh L, Dabiri H, et al. vacA genotypes of Helicobacter pylori in relation to cagA status and clinical outcomes in Iranian populations. Jpn J Infect Dis. 2008;61(4):290.
27. Chomvarin C, Namwat W, Chaicumpar K, et al. Prevalence of Helicobacter pylori vacA, cagA, cagE, iceA and babA2 genotypes in Thai dyspeptic patients. Int J Infect Dis. 2008;12(1):30–36. doi:10.1016/j.ijid.2007.03.012
28. Zamani M, Ebrahimtabar F, Zamani V, et al. Systematic review with meta‐analysis: the worldwide prevalence of Helicobacter pylori infection. Aliment Pharmacol Ther. 2018;47(7):868–876. doi:10.1111/apt.14561
29. Miftahussurur M, Yamaoka Y, Graham DY. Helicobacter pylori as an oncogenic pathogen, revisited. Expert Rev Mol Med. 2017;19.
30. Lee Y-C, Chen T-H-H, Chiu H-M, et al. The benefit of mass eradication of Helicobacter pylori infection: a community-based study of gastric cancer prevention. Gut. 2013;62(5):676–682. doi:10.1136/gutjnl-2012-302240
31. Ansari S, Yamaoka Y. Survival of Helicobacter pylori in gastric acidic territory. Helicobacter. 2017;22(4):e12386. doi:10.1111/hel.2017.22.issue-4
32. Knorr J, Ricci V, Hatakeyama M, Backert S. Classification of Helicobacter pylori virulence factors: is CagA a toxin or not? Trends Microbiol. 2019;27:731–738. doi:10.1016/j.tim.2019.04.010
33. Khashei R, Dara M, Bazargani A, et al. High rate of A2142G point mutation associated with clarithromycin resistance among Iranian Helicobacter pylori clinical isolates. Apmis. 2016;124(9):787–793. doi:10.1111/apm.2016.124.issue-9
34. Mahmoudi S, Mamishi S, Banar M, et al. Antibiotic susceptibility of Helicobacter pylori strains isolated from Iranian children: high frequency of A2143G point mutation associated with clarithromycin resistance. J Glob Antimicrob Resist. 2017;10:131–135. doi:10.1016/j.jgar.2017.04.011
35. Pourakbari B, Mahmoudi S, Parhiz J, Sadeghi R, Monajemzadeh M, Mamishi S. High frequency of metronidazole and clarithromycin-resistant Helicobacter pylori in formalin-fixed, paraffin-embedded gastric biopsies. Br J Biomed Sci. 2018;75(2):61–65. doi:10.1080/09674845.2017.1391466
36. Alarcón-Millán J, Fernández-Tilapa G, Cortés-Malagón EM, et al. Clarithromycin resistance and prevalence of Helicobacter pylori virulent genotypes in patients from Southern México with chronic gastritis. Infect Genet Evol. 2016;44:190–198. doi:10.1016/j.meegid.2016.06.044
37. Bagheri N, Azadegan-Dehkordi F, Rafieian-Kopaei M, Rahimian G, Asadi-Samani M, Shirzad H. Clinical relevance of Helicobacter pylori virulence factors in Iranian patients with gastrointestinal diseases. Microb Pathog. 2016;100:154–162. doi:10.1016/j.micpath.2016.09.016
38. Gilani A, Razavilar V, Rokni N, Rahimi E VacA and cagA genotypes of Helicobacter pylori isolated from raw meat in Isfahan province, Iran. Paper presented at: Veterinary Research Forum 2017.
39. Ranjbar R, Khamesipour F, Jonaidi‐Jafari N, Rahimi E. Helicobacter pylori isolated from Iranian drinking water: vacA, cagA, iceA, oipA and babA2 genotype status and antimicrobial resistance properties. FEBS Open Bio. 2016;6(5):433–441. doi:10.1002/2211-5463.12054
40. Bachir M, Allem R, Tifrit A, et al. Primary antibiotic resistance and its relationship with cagA and vacA genes in Helicobacter pylori isolates from Algerian patients. Braz J Microbiol. 2018;49(3):544–551. doi:10.1016/j.bjm.2017.11.003
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.