Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Circulating Complement C1q as a Novel Biomarker is Associated with the Occurrence and Development of COPD
Authors Zhang K, Han K ![]() , Liu H, Zheng C
, Liu H, Zheng C
Received 8 November 2021
Accepted for publication 9 February 2022
Published 23 February 2022 Volume 2022:17 Pages 395—404
DOI https://doi.org/10.2147/COPD.S347607
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Ke Zhang, Kangkang Han, Hui Liu, Chunyan Zheng
Department of General Practice, Qilu Hospital, Cheeloo College of Medicine, Shandong University, Jinan, Shandong, 250012, People’s Republic of China
Correspondence: Chunyan Zheng, Department of General Practice, Qilu Hospital, Cheeloo College of Medicine, Shandong University, Jinan, Shandong, 250012, People’s Republic of China, Email [email protected]
Purpose: Increasing evidence has shown that the immune response interacts with the chronic inflammatory response and gives rise to the occurrence and development of COPD. Complement component 1q (C1q), as a subcomponent of the C1 complex, could be involved in innate and adaptive immunity. Our study aimed to investigate the relationship between C1q and the clinical characteristics of COPD subjects.
Patients and Methods: Serum C1q levels were measured in 203 COPD subjects and 191 non-COPD controls. Correlations between C1q and the characteristics of COPD were analyzed using Spearman’s rho. Receiver operating curve (ROC) analysis was used to evaluate the threshold value in differentiating disease status. All 203 COPD subjects were followed up for 1 year for future acute exacerbations.
Results: There were significant reductions in serum C1q levels in COPD subjects compared to non-COPD controls. Moreover, serum C1q levels were obviously positively correlated with the FEV1/FVC ratio and predicted FEV1% but had a weakly negative correlation with the %LAA-950 and the percentage of neutrophils in peripheral blood. Using a cutoff value of 137.150 mg/l as the boundary in ROC analysis, the sensitivity and specificity were 65.9% and 76.0%, respectively. The 1-year follow-up results showed that C1q levels less than 137.150 mg/l were negatively related to the time to the next severe exacerbation and the time to death.
Conclusion: Circulating C1q levels may be a novel biomarker not only related to the pulmonary function of COPD but also having great potential to predict the risk of COPD deterioration in the future. However, further prospective trials are needed to clarify the influences of C1q on the pathogenesis of COPD.
Keywords: complement component 1q, chronic obstructive pulmonary disease, pulmonary function, exacerbations, future risk
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic disease characterized by airflow restriction and persistent respiratory symptoms and is caused by airway and/or alveolar abnormalities.1 Cigarette smoking is the most common risk factor for the development of COPD.1 Chronic airway inflammation and pulmonary emphysema are the main pathological features of COPD.2 However, the exact pathogenesis of COPD is not fully understood. A large body of literature3,4 has tested the hypothesis that COPD may be related to chronic inflammation, oxidative stress, protease antiprotease imbalance and other factors. Recent studies5,6 have proposed that in addition to the above mechanisms, the immune response is also involved in COPD. Innate immunity,7 acquired immunity,7 T cell-mediated immune imbalance8,9 and autoimmunity10 play an important role in the pathogenesis of COPD. Therefore, the investigation of immune factors and immune genes may further elucidate the pathogenesis of COPD, which would provide a theoretical basis for finding new targets for the prevention and treatment of COPD.
Complement component 1q (C1q), as a subcomponent of the C1 complex participating in the classical pathway of complement activation, could be involved in innate and adaptive immunity.11 Studies have shown that C1q is associated with a variety of autoimmune diseases,12,13 several cancers,14 active pulmonary tuberculosis15 and other diseases. In 2019, Yuan et al16 found that upon exposure to cigarettes, C1q produced by antigen presenting cells (APCs) is the crucial mediator of the differentiation of regulatory T cells (Tregs) and Th17 cells. Cigarette smoke can induce proinflammatory cytokines such as IL-1β. These cytokines can inhibit the expression of C1q produced by APCs, reduce the induction of Tregs, and further increase the proliferation and expression of cytokines (such as interferon γ and interleukin 17a) in Th17 cells, thereby aggravating pulmonary inflammation and emphysema. It is suggested that complement C1q is of great significance in the occurrence and development of COPD. However, the study of serum C1q levels and their potential roles in COPD have not been reported. Therefore, a case–control study was performed to observe the levels of serum C1q in COPD subjects and further analyzed its relationship with the pulmonary function, emphysema index, acute exacerbations, and smoking history to provide a theoretical basis for revealing the roles of C1q in COPD.
Materials and Methods
Selection of Participants
We performed a retrospective study using the clinical data of Qilu Hospital, Shandong University, Jinan, People’s Republic of China. COPD patients admitted to the Respiratory Department in Qilu Hospital of Shandong University from July 2018 to February 2021 were involved. All COPD subjects met the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines1 by the following criteria: 1) patients with dyspnea, chronic cough or expectoration, and/or a history of exposure to risk factors; 2) the ratio of the forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) (FEV1/FVC ratio) <70% after inhalation of bronchodilator; and 3) excluding other diseases that may cause persistent airflow restriction. Patients who lacked sufficient information, such as lung function test results and imaging pictures, were excluded. Subjects with rheumatic diseases such as systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA); the presence of significant respiratory disease other than COPD such as active tuberculosis and pulmonary fibrosis caused by various reasons; and other diseases such as unstable cardiovascular disease, malignant tumor, and end-stage renal and liver diseases within 12 weeks before recruitment were excluded. All subjects have complete inpatient medical records, and if multiple hospitalizations occurred, only the first one was included. Meanwhile, non-COPD control group was randomly selected from the general population in the Health Examination Center. The non-COPD group also met the above exclusion criteria. Data on age, sex, body mass index (BMI), smoking history, and comorbidities were carefully collected for all subjects in the study. All data used in this study, such as serum C1q, pulmonary function test data and chest CT images, were obtained during routine hospitalization process. This study complies with the principles of the Declaration of Helsinki and was approved by the Medical Ethics Committee of Qilu Hospital of Shandong University (KYLL-202107-005). The Ethics Committee of our hospital agreed that for the retrospective study, written informed consent from participants was not required.
Pulmonary Function Tests and CT Scan Acquisition
Pulmonary function test (PFTs) data were exported from the MasterLab system (Jaeger, Höchberg, Germany). The FEV1/FVC ratio and the percentage of the predicted FEV1 (predicted FEV1%) were specially selected from all PFT data. According to the GOLD criteria,1 subjects with a FEV1/FVC ratio after a postbronchodilator less than 0.70 had COPD. The status of GOLD was measured by simple ranges of predicted FEV1% values: GOLD1 (≥80%), GOLD2 (50–79%), GOLD3 (30–49%), and GOLD4 (<30%).
To quantitatively evaluate emphysema, chest CT images with a slice thickness of 1.5 mm were obtained from all CT scans, and ratio of low attenuation areas(%LAA) was calculated according to the area and thickness of every slice on each lung segmented manually by 3D slicer 4.11 (http://www.slicer.org/).17 Then, we defined the lung field as an area with a CT scan density <–200 Hounsfield units (HU)18 and defined the threshold between the LAA and normal lung density as –950 HU. The %LAA-950 was measured as (number of LAA pixels in all slices)/(total lung area)×100 (%).
Laboratory Measurements
Within 24 hours of admission, serum C1q of all subjects was measured as one of routine examinations of hospitalized patients in our hospital by professional medical laboratory staff under the same conditions (Beckman Kurt (au5800), USA). The serum leukocyte count, the percentage of neutrophils, D-dimer level, and erythrocyte sedimentation rate (ESR) were detected by an automatic blood cell counter in the blood laboratory. There were no repeated freeze–thaw cycles for any serum analyzed. Venous blood samples were collected from all subjects for standardized laboratory tests under the same conditions. The technicians who conducted the test were blinded to the details of the subjects.
1-Year Follow-Up
COPD subjects were followed up regularly for 1 year by monthly telephone communication. During the telephone follow-up, we obtained oral informed consent from all patients. They all received optimal treatment according to the GOLD criteria,1 including drug treatment, oxygen therapy as required, and antibiotics according to the Anthonisen criteria.19 To determine the impact of serum C1q levels on patient outcomes, we examined the monthly frequency of acute exacerbations, the time to the next exacerbation and death events in COPD subjects. The severity of the exacerbations was stratified according to the GOLD criteria:1 mild (the clinical symptoms are present but no change in treatment), moderate (changes in medication such as the use of antibiotics and systemic corticosteroids), and severe (requiring hospitalization). We mainly collected information about severe exacerbations during the 1-year follow-up.
Statistical Analysis
Numerical variables are expressed as the mean ± SD, whereas categorical variables are presented as n (%). For comparisons between groups, the chi square test was used to test categorical data (such as COPD subjects and non-COPD subjects), and the t-test or Mann–Whitney U-test were used for normally distributed or skewed value data, respectively. As the data for the FEV1/FVC ratio, the predicted FEV1%, the %LAA-950, inflammatory parameters and the smoking time were skewed and could not be normalized after logarithmic conversion, the influence of these variables on serum C1q levels was investigated by Spearman’s rho. A receiver operating characteristic (ROC) curve was constructed to determine the best cutoff value of serum C1q levels to distinguish COPD status. The times to next new exacerbation and death, according to the best cutoff value of C1q, were evaluated with Kaplan–Meier survival curves and Log rank tests. Multiple stepwise linear regression analysis was performed to determine the risk factors for serum C1q levels in COPD subjects. P values <0.05 were considered to be statistically significant. All tests were two-tailed. Data and graphs were analyzed and created using SPSS 26.0 and R.4.0.3.
Results
Subject Characteristics
All the demographic data and other clinical variables of the study are summarized in Table 1. Through rigorous screening process, 203 COPD subjects, consisting of 35 with stable COPD and 168 with an acute exacerbation of COPD (AECOPD), were enrolled in our study, and 114 COPD subjects were excluded eventually. The age of 203 COPD patients was 68.43 ± 7.96 years. In total, 181 (86.2%) were male and 178 (87.7%) were current smokers or ex-smokers. Meanwhile, 191 age- and sex-matched non-COPD subjects were involved as control group. There was no significant difference in sex, age, BMI, comorbidity-cardiovascular, comorbidity-diabetes, or comorbidity-hypertension between COPD subjects and non-COPD controls.
 |
Table 1 Characteristics of COPD Subjects and Non-COPD Controls |
Correlations of Serum C1q Levels with Pulmonary Function Parameters and Emphysema
Compared with the non-COPD controls, the serum C1q levels in COPD subjects decreased significantly (150.880 ± 29.388 vs 182.400 ± 31.600, P < 0.001) (Figure 1A). In COPD subjects, according to the GOLD criteria, 17 subjects were classified as GOLD 1, 62 subjects as GOLD 2, 76 subjects as GOLD 3 and 48 subjects as GOLD 4. Compared with the non-COPD controls, the serum C1q levels of GOLD 1–2 COPD subjects showed a downward trend (163.730 ± 25.970 vs 182.400 ± 31.600, P < 0.001) (Figure 1B). In particular, the levels of C1q in GOLD 3–4 COPD subjects decreased significantly compared with those in GOLD 1–2 subjects (142.694 ± 28.584 vs 163.730 ± 25.970, P < 0.001) (Figure 1B). Subsequently, in COPD subjects, we performed a correlation analysis between C1q and some pulmonary function parameters, which showed that the serum C1q levels were positively correlated with the FEV1/FVC ratio and predicted FEV1% (all P < 0.001) (Table 2 and Figure 1D and E).
 |
Table 2 Factors Correlated with Serum C1q in COPD Subjects |
 |
Figure 1 Serum C1q showed a downward trend in COPD subjects (A), especially in GOLD 3–4 (B) and severe emphysema (C). Serum C1q was obviously positively correlated with the FEV1/FVC ratio and predicted FEV1% in COPD (D and E) but had a weakly negative correlation with the %LAA-950 (F). *P < 0.05, **P < 0.01, ***P < 0.001. Abbreviations: ns, not significant; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; %LAA, ratio of low attenuation areas. |
In COPD subjects, to evaluate the relationship between C1q and the severity of emphysema, we conducted a correlation analysis between C1q and the %LAA-950, which showed a weakly negative correlation between them (P < 0.001) (Table 2 and Figure 1F). Then, we classified the %LAA-950 into three subgroups based on its thresholds defined in the literature:20,21 no emphysema (%LAA-950 <6), moderate emphysema (%LAA-950 ≥6 and <14) and severe emphysema (%LAA-950 ≥14). The study found that severe emphysema (n = 122), compared with moderate emphysema (n = 48) and no emphysema (n = 33), had lower levels of C1q in peripheral blood (144.548 ± 27.015 vs 162.156 ± 30.015, P < 0.01; 144.548 ± 27.015 vs 157.894 ± 31.222, P < 0.05) (Figure 1C). Furthermore, the %LAA-950 was significantly negatively correlated with the predicted FEV1% and the FEV1/FVC ratio (rho = −0.521, P < 0.001; rho = −0.523, P < 0.001).
Correlations of Serum C1q Levels with the State of COPD and Inflammatory Parameters
Compared with 35 stable COPD subjects, 168 subjects with AECOPD had significantly lower serum C1q levels (146.087 ± 27.595 vs 173.891 ± 27.059, P < 0.001) (Figure 2A). In all 203 COPD subjects, C1q was only weakly negatively correlated with the percentage of neutrophils in peripheral blood (P = 0.027) (Table 2 and Figure 2B). Unexpectedly, in our study, no significant difference in the ESR, D-dimer level, leukocyte count or the percentage of neutrophils was observed in AECOPD subjects compared with stable COPD subjects. (all P > 0.05) (Supplementary Figure 1A–D). Furthermore, no correlation was observed between C1q and the ESR, D-dimer level, or leukocyte count in the peripheral blood of COPD subjects (all P > 0.05) (Table 2 and Supplementary Figure 1E–G).
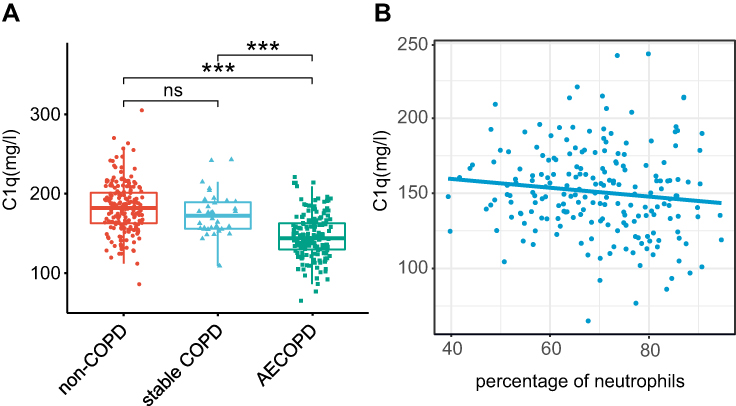 |
Figure 2 Serum C1q decreased in AECOPD subjects compared with stable COPD and non-COPD (A). Serum C1q was weakly negatively correlated with the percentage of neutrophils in peripheral blood in COPD subjects (B). ***P < 0.001. Abbreviation: ns, not significant. |
Serum C1q and Severe Exacerbators
During the 1-year follow-up period of all 203 COPD subjects, 59 subjects were excluded because they were followed up for less than 1 year before the beginning of statistical analyses, suffered from excluded diseases such as cancers, had interrupted telephone contact and so on. A total of 144 subjects were recorded completely during the 1-year follow-up, including 44 subjects who experienced severe exacerbations (30.6%) (ie, requiring hospitalization) and 12 deaths (8.3%) (Table 3).
 |
Table 3 Differences in the COPD Subjects Outcomes During 1-Year Follow-Up According to the Levels of Serum C1q on Admission |
In the 144 follow-up subjects, our data showed that in 44 severe exacerbators, serum C1q levels on admission were lower than those in non-severe exacerbators (130.872 ± 22.079 vs 158.794 ± 31.157, P < 0.001) (Figure 3A). ROC analysis of the 144 subjects showed that the AUC of C1q, which was 0.762 (95% CI, 0.682–0.842), could be used to discriminate severe exacerbations (Figure 3B). The cutoff value was set to 137.150 mg/L. The sensitivity was 65.9%, and the specificity was 76.0%. Using the cutoff value (137.150 mg/L) of ROC analysis as the boundary, we observed that C1q levels <137.150 mg/l were negatively correlated with the time to the next new severe exacerbation after discharge (P < 0.001) and the time to death (P = 0.026; Log rank test) (Figure 3C and D). In addition, 114 subjects were divided into C1q < 137.150 mg/L group and C1q ≥ 137.150 mg/L group. We observed that subjects with C1q < 137.150 mg/L group had a higher number of severe exacerbations and deaths after discharge than C1q ≥ 137.150 mg/L group. The detailed events are shown in Table 3.
 |
Figure 3 Serum C1q levels were downregulated in 44 follow-up severe exacerbators (A). Diagnostic accuracy of serum C1q to differentiate severe exacerbations in 144 follow-up COPD subjects (B). Area under the curves (AUC) was 0.762, and the cutoff value was set to 137.150 mg/L. Differences between subjects with low and high C1q levels in time to the next severe exacerbation (C) and time to death (D). ***P < 0.001. |
Serum C1q and Smoke
The study found that in COPD subjects, compared with never-smokers (n = 25), smokers (n = 178) had relatively lower C1q levels (149.147 ± 28.915 vs 163.228 ± 30.366, P = 0.037) (Figure 4A). However, no correlation was found between C1q levels and pack years in COPD subjects (P > 0.05) (Table 2 and Supplementary Figure 2A). Interestingly, in non-COPD control group, there was no difference in C1q levels between smokers (n = 59) and never-smokers (n = 132) (P > 0.05) (Supplementary Figure 2B). Furthermore, we divided all 394 participants (203 COPD subjects and 191 non-COPD controls) into two groups: smokers (n = 237) and never-smokers (n = 157). Results showed that the C1q levels of smokers were relatively lower than those of never-smokers (157.881 ± 32.038 vs 178.659 ± 33.869, P < 0.001) (Figure 4B).
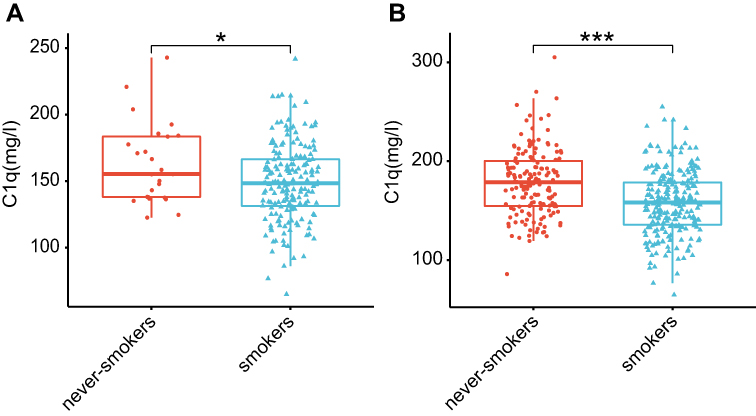 |
Figure 4 C1q levels of smokers were lower than those of never-smokers, whether in COPD subjects (A) or all 394 subjects (B). *P < 0.05, ***P < 0.001. |
Factors Associated in a Multivariate Model
In COPD subjects, we evaluated the combined effects of independent variables that might be related to C1q. After adjusting for potential confounding factors (ie, age, sex, BMI, comorbidity-cardiovascular, comorbidity-diabetes, and comorbidity-hypertension), predicted FEV1% was an independent factor associated with serum C1q levels by stepwise multiple linear regression (Supplementary Table 1).
Discussion
Our study demonstrated that the serum C1q levels in COPD subjects were significantly downregulated compared to those in non-COPD controls. In addition, the decline in C1q levels was obviously related to a decrease in pulmonary function and the state of COPD. During the 1-year follow-up period, C1q levels less than 137.150 mg/l were negatively related to the time to next new severe exacerbation and the time to death. After adjusting for potential confounding factors, predicted FEV1% was an independent factor associated with C1q levels. Decreased serum C1q levels in COPD may have potential as a biomarker for predicting the risk of COPD deterioration in the future.
In the present study, we observed that the reduction in serum C1q in GOLD 3–4 subjects was more obvious than that in GOLD 1–2 subjects, implying that C1q may be related to a decline in pulmonary function. To further test this hypothesis, correlation analysis showed that C1q was positively correlated with the FEV1/FVC ratio and predicted FEV1%, further indicating that C1q may have significant associations with the development of airflow obstruction and the severity of pulmonary function. Moreover, multiple linear regression proposed that predicted FEV1% was an independent factor related to C1q levels, which was consistent with the above standpoints. In addition, although C1q varied among the severity of emphysema, there were weakly negative correlations between C1q and the %LAA-950. Our observations suggest that the decrease in C1q, although related to lung function, may not be a clinically relevant predictive biomarker of emphysema severity. We know that the pulmonary function damage in patients is inevitably affected by the anatomical distribution of emphysema. Compared with subjects with lower lobe-predominant emphysema, subjects with mostly upper-lobe predominance emphysema had less severe lung function impact.22 Our study implied that further investigations about the relationship between C1q and the anatomical distribution of emphysema in the whole lung field are needed.
Some studies suggested that the neutrophil count,23 ESR,24 D-dimer level,25 and leukocyte count26 were related to AECOPD. Surprisingly, no difference was found in the ESR, D-dimer level, leukocyte count or percentage of neutrophils between subjects with stable COPD and AECOPD in our study. We conjecture the more likely reason may be that most patients with acute exacerbation have received initial therapy including antibiotics before admission in our hospital. Noticeably, although our result did not show the association with AECOPD and the ESR, D-dimer level, leukocyte count and percentage of neutrophils, C1q still decreased significantly in AECOPD, which may suggest that C1q was more valuable as a biomarker of AECOPD. Although the underlying mechanisms require further validation, we still cannot rule out the possibility of the association between C1q and inflammation in COPD.
COPD patients always experience repeated exacerbations, which result in decreased pulmonary function27 and an increased risk of death.28 Therefore, prevention of exacerbation is a vital goal in the management of COPD patients. Exacerbations of COPD are characterized by continuous deterioration beyond daily symptoms, which include dyspnea, increased sputum volume and purulence, and the requirement to change routine medication.1 The current diagnostic basis of exacerbations mainly depends on the above characteristics, and specific biomarkers are still lacking. We found that serum C1q was downregulated in severe exacerbators (requiring hospitalization) of COPD during the 1-year follow-up, implying that the risk of COPD deterioration may be related to lower C1q levels to some extent. When the cutoff value was set at 137.150 mg/l in the ROC analysis, C1q had good specificity for the presence of severe exacerbations. Using 137.150 mg/l as the boundary, we observed that C1q levels less than 137.150 mg/l were negatively related to the next new severe exacerbation and the time to death after discharge. Therefore, serum C1q might have great potential to act as a biomarker for the prediction of new severe exacerbations.
Yuan et al16 certified that C1q plays an essential role as an immune response regulator in the cigarette-smoke-mediated inflammatory response and that this procedure promotes the occurrence and development of COPD. Meanwhile, we confirmed that smokers had significantly lower C1q levels than never-smokers in all 394 subjects and in the COPD group. However, there was no significant difference in C1q levels between smokers and never-smokers in the non-COPD controls. We speculate that the reason may be that the pack years of smoking in the non-COPD controls are far less than those in COPD subjects which causing a nonsignificant difference in C1q levels, and most non-COPD controls have quit smoking for more than decades. We believe that the potential relationship between C1q and cigarette smoke is unclear. Further researchers with larger sample sizes are needed to replicate these preliminary findings.
There are several limitations for this study. Our inclusion criteria were so strict that only 203 COPD subjects who met the clinical criteria were enrolled. Therefore, it is necessary to verify our study in a large number of subjects in future clinical trials. Moreover, it is preferable to collect various sample types (such as lung tissue, sputum, and bronchoalveolar lavage fluid (BALF)) to further investigate the association between circulating C1q and COPD.
Conclusion
We have demonstrated that circulating C1q levels may be a novel biomarker not only related to the pulmonary function of COPD subjects but also having great potential to predict the risk of COPD deterioration in the future. However, further prospective trials are needed to clarify the influences of C1q on the pathogenesis of COPD.
Acknowledgments
This work was supported by grants of The National Key Research and Development Program of China (No. 2016YFC1304601). The funders had no role in research design, data collection or analysis, and writing manuscripts.
Author Contributions
Ke Zhang, Chunyan Zheng designed this research, and all authors made a great contribution to acquisition of data, statistical analysis, drafting, revising and critically reviewing the article, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
All authors declare no conflicts of interest related to this work.
References
1. Global initiative for chronic obstructive lung disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2021. Available from: https://goldcopd.org/.
2. Barnes PJ, Burney PG, Silverman EK, et al. Chronic obstructive pulmonary disease. Nat Rev Dis Primers. 2015;1:15076. doi:10.1038/nrdp.2015.76
3. Cosio MG, Saetta M, Agusti A. Immunologic aspects of chronic obstructive pulmonary disease. N Engl J Med. 2009;360(23):2445–2454. doi:10.1056/NEJMra0804752
4. Brusselle GG, Joos GF, Bracke KR. New insights into the immunology of chronic obstructive pulmonary disease. Lancet. 2011;378(9795):1015–1026. doi:10.1016/S0140-6736(11)60988-4
5. Hsu AT, Gottschalk TA, Tsantikos E, Hibbs ML. The role of innate lymphoid cells in chronic respiratory diseases. Front Immunol. 2021;12:733324. doi:10.3389/fimmu.2021.733324
6. Lourenco JD, Ito JT, Martins MA, Tiberio I, Lopes F. Th17/Treg imbalance in chronic obstructive pulmonary disease: clinical and experimental evidence. Front Immunol. 2021;12:804919. doi:10.3389/fimmu.2021.804919
7. Halper-Stromberg E, Yun JH, Parker MM, et al. Systemic markers of adaptive and innate immunity are associated with chronic obstructive pulmonary disease severity and spirometric disease progression. Am J Respir Cell Mol Biol. 2018;58(4):500–509. doi:10.1165/rcmb.2017-0373OC
8. Urbanowicz RA, Lamb JR, Todd I, Corne JM, Fairclough LC. Altered effector function of peripheral cytotoxic cells in COPD. Respir Res. 2009;10:53. doi:10.1186/1465-9921-10-53
9. Tang Y, Li X, Wang M, et al. Increased numbers of NK cells, NKT-like cells, and NK inhibitory receptors in peripheral blood of patients with chronic obstructive pulmonary disease. Clin Dev Immunol. 2013;2013:721782. doi:10.1155/2013/721782
10. Zhou JS, Li ZY, Xu XC, et al. Cigarette smoke-initiated autoimmunity facilitates sensitisation to elastin-induced COPD-like pathologies in mice. Eur Respir J. 2020;56(3):2000404. doi:10.1183/13993003.00404-2020
11. Kishore U, Reid KB. C1q: structure, function, and receptors. Immunopharmacology. 2000;49(1–2):159–170. doi:10.1016/S0162-3109(00)80301-X
12. Sharma M, Vignesh P, Tiewsoh K, Rawat A. Revisiting the complement system in systemic lupus erythematosus. Expert Rev Clin Immunol. 2020;16(4):397–408. doi:10.1080/1744666X.2020.1745063
13. Liaskos C, Rentouli S, Simopoulou T, et al. Anti-C1q autoantibodies are frequently detected in patients with systemic sclerosis associated with pulmonary fibrosis. Br J Dermatol. 2019;181(1):138–146. doi:10.1111/bjd.17886
14. Mangogna A, Agostinis C, Bonazza D, et al. Is the complement protein C1q a pro- or anti-tumorigenic factor? Bioinformatics analysis involving human carcinomas. Front Immunol. 2019;10:865. doi:10.3389/fimmu.2019.00865
15. Lubbers R, Sutherland JS, Goletti D, et al. Complement component C1q as serum biomarker to detect active tuberculosis. Front Immunol. 2018;9:2427. doi:10.3389/fimmu.2018.02427
16. Yuan X, Chang CY, You R, et al. Cigarette smoke-induced reduction of C1q promotes emphysema. JCI Insight. 2019;5. doi:10.1172/jci.insight.124317
17. Fedorov A, Beichel R, Kalpathy-Cramer J, et al. 3D slicer as an image computing platform for the quantitative imaging network. Magn Reson Imaging. 2012;30(9):1323–1341. doi:10.1016/j.mri.2012.05.001
18. Ohara T, Hirai T, Muro S, et al. Relationship between pulmonary emphysema and osteoporosis assessed by CT in patients with COPD. Chest. 2008;134(6):1244–1249. doi:10.1378/chest.07-3054
19. Anthonisen NR, Manfreda J, Warren CP, Hershfield ES, Harding GK, Nelson NA. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 1987;106(2):196–204. doi:10.7326/0003-4819-106-2-196
20. Lynch DA, Austin JH, Hogg JC, et al. CT-definable subtypes of chronic obstructive pulmonary disease: a statement of the Fleischner society. Radiology. 2015;277(1):192–205. doi:10.1148/radiol.2015141579
21. Hersh CP, Washko GR, Estepar RS, et al. Paired inspiratory-expiratory chest CT scans to assess for small airways disease in COPD. Respir Res. 2013;14:42. doi:10.1186/1465-9921-14-42
22. Boueiz A, Chang Y, Cho MH, et al. Lobar emphysema distribution is associated with 5-year radiological disease progression. Chest. 2018;153(1):65–76. doi:10.1016/j.chest.2017.09.022
23. Sapey E, Stockley JA, Greenwood H, et al. Behavioral and structural differences in migrating peripheral neutrophils from patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2011;183(9):1176–1186. doi:10.1164/rccm.201008-1285OC
24. Wang L, Yang H, Gu W. Value of erythrocyte sedimentation rate and serum epo levels in evaluating the condition and prognosis of COPD in the elderly. Pak J Pharm Sci. 2021;34(1):435–439.
25. Zhang M, Zhang J, Zhang Q, et al. D-dimer as a potential biomarker for the progression of COPD. Clin Chim Acta. 2016;455:55–59. doi:10.1016/j.cca.2016.01.024
26. Sahin F, Kosar AF, Aslan AF, Yigitbas B, Uslu B. Serum biomarkers in patients with stable and acute exacerbation of chronic obstructive pulmonary disease: a comparative study. J Med Biochem. 2019;38(4):503–511. doi:10.2478/jomb-2018-0050
27. Suissa S, Dell’Aniello S, Ernst P. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67(11):957–963. doi:10.1136/thoraxjnl-2011-201518
28. Sadatsafavi M, Xie H, Etminan M, Johnson K, FitzGerald JM. Canadian respiratory research N. The association between previous and future severe exacerbations of chronic obstructive pulmonary disease: updating the literature using robust statistical methodology. PLoS One. 2018;13(1):e0191243. doi:10.1371/journal.pone.0191243
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.