Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Chronic Stress in Bipolar Disorders Across the Different Clinical States: Roles of HPA Axis and Personality
Authors Zhang M, Zhao S, Chen Y, Zhang X, Li Y, Xu P, Huang Y, Sun X
Received 3 May 2022
Accepted for publication 8 August 2022
Published 12 August 2022 Volume 2022:18 Pages 1715—1725
DOI https://doi.org/10.2147/NDT.S372358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Manxue Zhang,1,2 Shengnan Zhao,1 Yuexin Chen,1 Xu Zhang,1 Yuwei Li,1 Peiwei Xu,1 Yi Huang,1,3 Xueli Sun1
1Mental Health Center, West China Hospital of Sichuan University, Chengdu, People’s Republic of China; 2The Second Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 3Brain Research Center, West China Hospital of Sichuan University, Chengdu, People’s Republic of China
Correspondence: Xueli Sun, Department of Psychiatry, Mental Health Center, West China Hospital of Sichuan University, No. 37 Guo Xue Xiang, Chengdu, 610041, People’s Republic of China, Tel +86 28 8542 2023, Fax +862885582944, Email [email protected]
Introduction: Chronic stress has been linked to the pathophysiology of bipolar disorder (BD); however, the underlying mechanism remains unclear. In BD patients, hypothalamic-pituitary-adrenal (HPA) axis activity is associated with stress. This study aimed to examine the relationship between HPA axis activity and BD symptoms in various clinical states, as well as how personality influences the process.
Methods: This study investigated the differences in HPA axis activity among four BD states. We enrolled 813 BD patients in an 8-week longitudinal study to examine the relationship between HPA axis activity and symptom trajectories using dynamic temporal warping (DTW) analysis and an unsupervised machine learning technique. Furthermore, using mediation analyses, the relationship between the HPA axis, personality, and BD symptoms was investigated.
Results: Analysis of variance (ANOVA) analysis showed that glucocorticoid cortisol (CORT) and adrenocorticotropin (ACTH) did not differ significantly among the four clinical states of BD. The DTW integrating clustering analysis revealed that the two clusters were optimal, with cluster 1 characterized by severe manic symptoms, which then improved, and cluster 2, characterized by milder manic severity, which also improved. The two clusters showed different ACTH levels (t = 2.289, p = 0.022), and logistic regression analysis revealed a slight positive association between ACTH levels and cluster 1. Furthermore, the mediation analysis indicated that ACTH influences curative efficacy via conscientiousness (βc =0.103, p=0.001).
Discussion: In conclusion, we found that a higher level of ACTH is associated with severe manic symptoms, indicating a chronic stress response in BD patients. Additionally, the ACTH levels affect short-term BD curative efficacy via the mediation of conscientiousness, providing a psychotherapeutic strategy direction for BD.
Keywords: bipolar disorder, hypothalamic–pituitary–adrenal axis, personality, dynamic time warping analysis, mediation analysis
Introduction
Bipolar disorder (BD) is a category of affective disorders characterized by depressive episodes and hypomanic or manic episodes,1 with a global incidence rate of about 2%.2 According to statistics, the total cost of BD in the United States is estimated to be $81,559 per patient per year.3 Previous studies have reported that individuals with BD experience more negative and stressful life events than the general population.4,5 A better understanding of the underlying pathophysiology may aid in improving diagnostic accuracy and patient treatment stratification;6 however, the pathophysiology mechanism of BD remains unclear.
Concerning the pathophysiology of BD, one intriguing finding in mice is that exposure to unpredictable chronic mild stress has been associated with BD pathogenesis.7 Chronic stress is a critical etiologic factor of affective disorders;8,9 and individuals with BD are exposed to a substantial accumulated stress load over their lifetimes.10 We hypothesize that chronic stress should be adequately managed to alleviate BD symptoms. Stress activates the hypothalamic-pituitary-adrenal (HPA) axis, which then releases glucocorticoid hormones.11 The pathway is initiated by the individual’s stress response in the central nervous system, and a signal is relayed to the hypothalamus, which then activates the corticotropin-releasing hormone (CRH). CRH diffuses to the anterior pituitary gland to release adrenocorticotropin (ACTH) secretion into the circulation, which then travels down to the adrenal cortex to release the glucocorticoid cortisol (CORT). Cortisol suppresses its own production by inhibiting both CRH and ACTH secretion, resulting in a closed loop.12 Several investigations have demonstrated that stress stimulates the HPA axis and increases cortisol secretion.13 The role of HPA axis activity in the pathology of BD needs to be further clarified so that we can explore the association between stress and BD symptoms changing trajectory.
Patients with BD exhibit vulnerability to stress, resulting in aberrant HPA axis activation. It indicates that HPA axis activity might be a biomarker of the disorder.14–18 However, the HPA axis activity mechanism in BD is more complex than previously thought, as both hyperactivity and hypoactivity of the HPA axis are associated with affective disorders.16,19 The hypothesis could explain the phenomenon that stress is initially manifested as hypercortisolism at the beginning but is believed to, over time, contribute to the development of hypocortisolism.20,21 Previous studies have shown that abnormal HPA axis activity in BD may vary depending on the state of the disease.16,22–24 While abnormal HPA axis activity remained in clinical remission and euthymic stage,25 this suggests that HPA axis abnormality is an endophenotype of the illness rather than an epiphenomenon. Previous studies compared manic and depressive episodes. There has been no study comparing HPA axis hormone levels in BD patients at different clinical stages such as mania, depression, mixed, and remission.
HPA axis activity is influenced by genetics and early negative life events.26,27 In BD patients, an abnormal HPA axis is associated with elevated manic mood symptoms.24 It is noteworthy that BD patients with abnormal HPA-axis activity have a higher frequency of affective episodes and a lower quality of life than those with normally functioning HPA-axis.16 Age, age of onset of BD, number of episodes, and mood stabilizers are found to predict HPA axis activity in BD.28,29 Chronic stress appears to dysregulate HPA axis activation, increasing the risk of disease onset or relapse.30 Stress management can improve BD prognosis by eliminating factors that impact HPA activation. Stress can be of various types and associated with personality features;31 for instance, personality dimensions, such as low conscientiousness and high neuroticism, can make people vulnerable to environmental stress. However, we did not address how personality influences the relationship between HPA axis activity and BD symptoms.
This study aimed to investigate the relationship between HPA axis activity and BD symptoms using a longitudinal study design. We hypothesize that HPA axis hyperactivity would predict BD symptoms’ changing trajectory. Furthermore, this study attempted to investigate how personality traits influence the relationship between HPA axis activity and BD symptoms, with the mediation effect of personality expected to be found in BD patients.
Methods
Participants
This study was conducted at West China Hospital of Sichuan University (outpatient department) from December 2018 to December 2019. The study included 813 patients with BD who met Diagnostic and Statistical Manual of Mental Disorders IV (DSM-IV) criteria, aged 18–65 years, and completed the study procedure, which included four clinical states: manic episode (N = 227), depressive episode (N = 466), mixed state (N = 80), and remission state (N = 40). Exclusion criteria included a history of substance abuse within the previous three months, unstable or severe physical disease, metabolic or endocrine disease, and pregnant or lactating women. All 813 patients received at least one mood stabilizer; additional medications were atypical antipsychotics, antidepressants, and benzodiazepines. Every participant signed an informed consent form following a detailed description of the study. The study conformed to the principles of the Declaration of Helsinki and was approved by the Institutional Ethics Board of the Chinese Clinical Trial Registry (The registration number is ChiECTR-20180187).
Procedures
Expert psychiatrists performed all experimental procedures (see participant flowchart in Figure 1). At baseline, general demographic information, clinical evaluation, NEO Five-Factor Inventory (NEO-FFI) assessments, and hormone determination were conducted. The optimum treatment strategy was then selected by the researchers based on their evaluation of the patients’ symptoms. The following three major categories were employed to evaluate the medication treatment models: 1. Triple-therapy Group: Combination of three types of drugs (mood stabilizer (MS) + antidepressants (AD) + atypical antipsychotics (AA)); 2. Double-therapy Group: Combination of either two of the aforementioned medications (eg, MS + AA, MS + AD); and 3. Monotherapy Group (MS). Follow-up visits were scheduled for weeks 4 and 8, respectively. At each visit, the clinical assessments were performed by expert psychiatrists. Unscheduled follow-up visits were offered if requested by the patients.
 |
Figure 1 Flow chart of the study design. |
Clinical Assessment
Current and lifetime diagnostic status was confirmed with Structured Clinical Interview for DSM‐IV Axis I disorders (SCID-I),32 the official diagnostic tool for the diagnostic and statistical manual of psychiatric disorders.1 The duration of the SCID-I is 30–90 minutes. Demographic data included age, gender, family history, the age of BD onset, duration time for diagnosis, and the number of affective episodes. Clinical assessment and symptom evaluation were conducted at baseline, week 4 and week 8, via administration of the Montgomery Asberg Depression Rating Scale (MADRS),33 Young Mania Rating Scale (YMRS),34 and Clinical Global Impression (CGI).35 A trained member of staff completed the clinical assessments to measure the current mood state.
NEO Five-Factor Inventory (NEO-FFI)
The personality traits were evaluated using the NEO-FFI, a commonly used test in clinical psychology. The Chinese version of the inventory showed good reliability and validity.36 It describes personality in terms of five board factors: neuroticism, extroversion, openness, agreeableness, and conscientiousness according to an individual’s response to a set of 60 questions, with each subscale comprising 12 items scored on a 5-point scale. In our study, only 170 participants completed NEO-FFI.
Hormone Determination
The CORT and ACTH levels were measured when the subject was included in our study at a single time point (8:00 AM–9:00 AM). As there is significant variation in the literature in the timing of blood draws for CORT and ACTH, to deal with this limitation, the blood samples for serum analyses in this study were collected between 8:00 and 9:00 Am, when hormone levels peaked in the diurnal cycle.37 According to the manufacturer’s instructions, plasma CORT and ACTH levels were measured using the chemiluminescence immunoassay kit (AutoLumo A2000). The normal range level for CORT was 147.3–609.3 nmol/L, and a range for healthy subjects of 5.0–78 ng/L was used for ACTH. The West China Hospital of Sichuan University, which performs these assays regularly, provided all of the normal ranges of the above hormones for healthy subjects.
Statistical Analyses
One-way analysis of variance (ANOVA) or Chi-square analysis was performed to test for differences in BD states in general demographic variables and hormone levels. A repeated-measures ANOVA with a post-hoc analysis using Bonferroni’s multiple comparisons was performed. Multiple linear regression analysis was performed to explore the elementary predictors of HPA axis activity. Analyses were performed using the Statistical Package for the Social Sciences, 26.0 (SPSS 26.0, IBM Corp., Armonk, NY, USA). The Kolmogorov–Smirnov test was used to determine the normal distribution of all variables. For comparisons between multiple means, nonparametric tests of Kruskal–Wallis were used. All statistical significance was set to a two-tailed p-value of 0.05.
We used a dynamic time warping (DTW) algorithm to demonstrate the symptoms’ trajectory. MADRS, YMRS, and CGI scores were used to record temporal changes in symptom severity at baseline, 4 weeks, and 8 weeks. We then used k-means clustering analysis with Ward linkage to identify clusters of similar symptom trajectories. The number of clusters was computed by combining four measures: Silhouette scores, the Calinski-Harabaz index, the Davies–Bouldin (DB) index, and the Dunn validity index. The above analyses were performed using python’s dtw38 and sklearn.cluster packages. Furthermore, differences between clusters were compared using the Student’s t-test or Chi-square analysis. Using logistic regression analysis, we investigated the association between HPA axis activity and the resulting symptom trajectory clusters.
Mediation analysis is ideally suited to investigating HPA axis-personality-BD symptoms relationships and has increasingly been applied to psychological data with interactions rather than functioning independently. Mediation models were performed using Analysis of Moment Structures software (AMOS, IBM SPSS Amos 21.0.0). In all the present study mediation models, HPA-axis hormone secretion was the independent variable (X). Depending on the condition, CGI, YMRS, MADRS, and YMRS changing scores representing the therapeutic efficacy were the dependent variables (Y). Personality traits were the mediators (M). The mediational effects of personality on the HPA-axis for BD symptoms were examined using causal mediation models.
Results
Demographic Characteristics of BD Across Different Clinical States
We included 813 BD patients in our study for hormone testing and 8-week follow-up visits. Of the BD patients, 227 were in the manic episode (mean age, 33.91±14.10 years), 466 were in the depressive episode (mean age 35.62±14.17 years), 80 were in the mixed state (mean age 33.65±11.96 years), and 40 were in the remission state (mean age 32.35±14.34 years). ANOVA revealed no significant differences among states of BD in age, family history, and age of onset (p > 0.05). In contrast, the female ratio of the depression episode group was higher than the other groups (χ2=46.22, p<0.001), this could be explained by the higher prevalence of depression among females. The duration time for diagnosis differed significantly among groups (F3813=4.35, p=0.005), and post-hoc t-tests with Bonferroni’s multiple comparison correction revealed that the manic group had a shorter duration time than the depression group. It indicated that clinicians would spend more time identifying the depression state of BD patients. For an overview of all demographic characteristics, see Table 1.
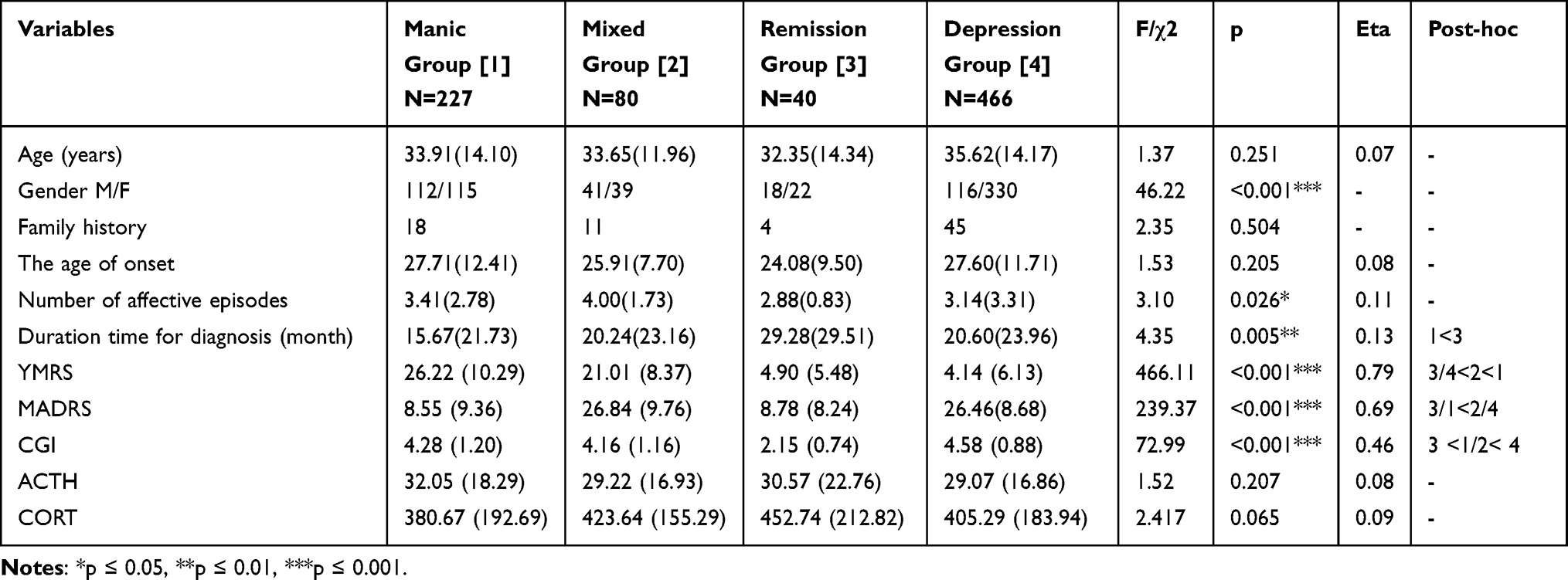 |
Table 1 Demographic Characteristics, Clinical Features, and HPA Axis of Patients with BD at Baseline (N= 813) |
Clinical Features and Hormones of BD Patients in Different Clinical States
The symptom severity measured by CGI was significantly differed among groups. As shown in Table 1, the CGI scores were lower in the remission group (M=2.15, SD=0.74) than other three groups (F3813=46.31, p<0.001). Moreover, the depression group (M = 4.58, SD = 0.88) was more severe than the mixed (M = 4.16, SD = 1.16) and manic groups (M = 4.28, SD = 1.20). The difference between the manic and mixed groups was insignificant. ANOVA revealed a significant omnibus difference in YMRS scores (F3813=198.40, p<0.001) and MADRS scores (F3813=169.55, p<0.001) across four BD clinical states. Post-hoc tests revealed that the manic group (M=26.22, SD=10.29) had higher YMRS scores than the mixed (M=21.01, SD=8.37), remission (M=4.90, SD=5.48), and depression groups (M=4.14, SD=6.13); and that the mixed group had higher YMRS scores than the remission and depression groups. There was no significant difference between the remission and depression groups in YMRS scores. MARDS post-hoc tests identified that the depression (M=26.46, SD=8.68) and mixed groups (M=26.84, SD=9.76) were higher than the remission (M=8.78, SD=8.24) and manic (M=8.55, SD=9.36) groups; while there was no significant difference between depression and mixed groups or between the remission and manic groups. As shown in Table 1, CORT and ACTH levels did not differ significantly among the four clinical states associated with BD in the baseline.
Predictors of HPA-Axis Activity in BD
Table 2 presents the results from the stepwise multivariate regression analyses. Initial analyses included personality (neuroticism, extroversion, openness, agreeableness, and conscientiousness), symptom severity (YMRS scores, MADRS scores, and CGI scores), age, the age of first time to diagnose, number of affective episodes, and duration time for diagnosis. Only conscientiousness predicted ACTH levels (β = −0.271, p < 0.001); neuroticism, extroversion, and openness predicted CORT levels (neuroticism-CORT, β = −0.223, p = 0.021; extroversion -CORT, β = −0.311, p = 0.001; and openness -CORT, β = −0.163, p = 0.043, respectively). Age, number of affective episodes, and symptom severity, among others, did not qualify as potential independent predictors.
 |
Table 2 The Independent Correlates of HPA According to the Multiple Linear Regression (N=170) |
The HPA Axis Characteristics of Manic Symptom Trajectory Clusters
The Manic Symptom Trajectory Clusters
The optimal number of clusters was selected as two after calculating the Silhouette scores (0.62), the Calinski-Harabaz index (2388), the DB index (0.67), and the Dunn validity index (0.02). (Depicted in Figure 2) The findings revealed that the two clusters represented distinct symptom trajectories: cluster 1 was characterized by severe manic symptoms, which then improved; cluster 2 was characterized by milder manic severity, which also improved. Cluster 1 had higher YMRS scores and lower MADRS scores than cluster 2 at all three-time points. Chi-square analysis showed no difference between the medication treatment models of the two clusters (χ2=1.686, p= 0.430). There were no differences in CGI scores at baseline and 4 weeks, with only a slight but significant difference being identified at the 8-week follow-up visit (Depicted in Table S1 and Figure 3).
 |
Figure 2 K-means subtyping via dynamic time warping (DTW) algorithm. Notes: Green means manic symptom trajectory cluster 1; golden represents manic symptom trajectory cluster 2. |
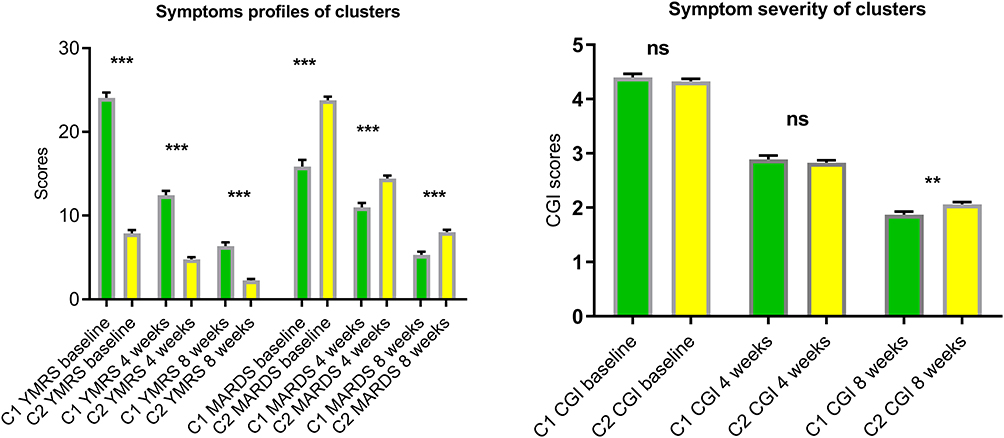 |
Figure 3 Symptom profiles of the two clusters. Notes: **p ≤ 0.01, ***p ≤ 0.001; green means cluster 1; golden represents cluster 2. |
The Association Between the HPA Axis and the Two Symptom Clusters
As shown in Table S1, cluster 1, which had higher YMRS scores, had higher ACTH levels than cluster 2 (t= 2.289, p=0.022); there was no significant difference in CORT levels between the two clusters. Furthermore, logistic regression analysis revealed a slight positive relationship between ACTH levels and cluster 1, which was characterized by severe manic symptoms before improving (β = 0.15, Ward= 7.553, p = 0.006). However, no association was found between CORT levels and clusters (p = 0.432).
Mediation Effect Analysis of Personality on the HPA Axis–BD Symptom Relationship
Mediation analysis quantifies how a variable termed mediator influences the effects of an independent variable on a dependent variable. In an 8-week follow-up, we tested the personality for mediation in the association between HPA-axis activity and therapeutic efficacy in BD patients. In our study, mediation analysis was present when: (i) HPA-axis hormone secretion correlated with personality trait scores (βa); (ii) personality trait scores were correlated with BD symptom severity changing scores (βb); (iii) personality trait scores were correlated with BD symptom severity changing scores without adjusting the model for the mediator (βc); and (iv) the model provided good fitness (p < 0.05). Figure 4 depicts one mediation model with good fitness (CMIN/DF=5.843, p=0.001; RMSEA=0.169). According to the ACTH-Conscientiousness-CGI changing scores mediation model, ACTH was mediated by conscientiousness to CGI changing scores (βc = 0.103, p = 0.001) but not directly related to CGI changing scores (βc = 0.065, p = 0.411). ACTH was found to be inversely related to conscientiousness (βa = −0.264, p < 0.001). Conversely, conscientiousness was negatively and directly related to YMRS scores (βb = −0.147, p = 0.041). The indirect effect of ACTH on CGI changing scores through conscientiousness was significant, accounting for 37.86% of the total effect (See Figure 4). In an 8-week follow-up, we tested the hypothesis that the mediator personality trait could explain part of the association between HPA axis activity and therapeutic efficacy in BD patients.
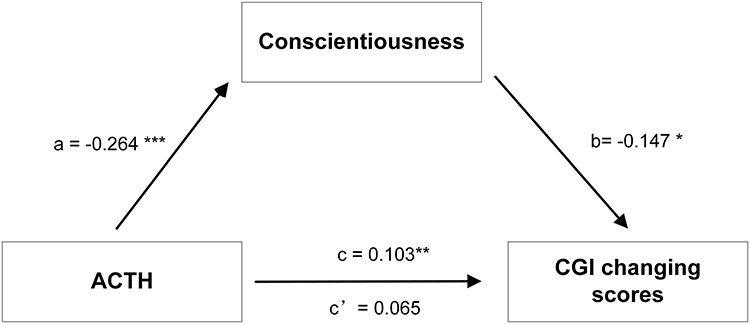 |
Figure 4 Mediation effects of personality on the relationship between ACTH levels and symptoms (N = 170). Notes: *P<0.05, **P<0.01, ***P<0.001. The ACTH – Conscientiousness – CGI changing scores mediation model showed good model fit index: CMIN/DF=5.843, p=0.001; RMSEA=0.169. ACTH was negatively related to conscientiousness (βa=−0.264, p<0.001). In turn, conscientiousness was negatively related to CGI changing scores (βb=−0.147, p=0.041). Indirect effect of ACTH on therapeutic efficacy measured by CGI changing scores through conscientiousness (ab)= 0.039, direct effect (c’) = 0.065 (p=0.411), total effect (c) = 0.103 (p=0.001). |
Discussions
The present study examined the association between the HPA axis activity and BD symptoms in different states. Furthermore, the role of personality in the relationship between the HPA axis activity and symptoms was explored. We found no significant difference in CORT and ACTH plasma levels among the four clinical states. The current longitudinal study achieved two clusters with distinct manic symptom trajectories over 8 weeks using DTW analysis and unsupervised machine learning technique, and ACTH levels varied between the two clusters. The higher the level of ACTH, the more severe the manic symptoms, indicating a correlation between the HPA axis activity and short-term BD curative efficacy. Multiple regression analysis revealed that conscientiousness predicted higher levels of ACTH. Furthermore, using an 8-week follow-up prospective cohort study design, the ACTH-Conscientiousness-CGI changing scores mediation model was established, indicating that conscientiousness mediated the relationship between ACTH and BD symptoms.
In our study, four different groups were subdivided based on the clinical states of BD: results showed no difference in CORT or ACTH levels among the four states, suggesting that HPA axis activity abnormality persisted in all forms of BD. Previous studies comparing HPA axis activity in different states of BD yielded inconclusive results: patients with depression have hyperactivity of the HPA axis compared to BD patients;23 manic symptoms predicted higher CORT levels than depression;22 a meta analysis revealed that the manic state yielded the largest effect sizes when compared to depression and euthymic conditions.14 The reasons for this inconsistency might lie in the clinical heterogeneity that characterizes BD and the opposite patterns of HPA axis activity.24 Moreover, the molecular mechanisms of HPA axis function in BD patients were associated with impaired intracellular signaling, and similar alterations were identified in first-degree relatives of BD patients.15 It indicated that HPA axis activity was the phenotype of BD rather than an epiphenomenon of the affective episodes.
The current study used DTW analysis and an unsupervised machine learning technique to identify two distinct manic symptom trajectory clusters: cluster 1, which had more severe manic symptoms over the 8 weeks, had a higher ACTH level than cluster 2, which had milder manic symptoms. Moreover, the logistic regression analysis revealed that ACTH was a short-term predictor of manic symptom trajectory. Consistent with evidence that long-term CORT levels were higher in BD and were related to the number of manic episodes.39 Conscientiousness has been associated with medication adherence in several mental diseases.40 Therefore the association observed here between ACTH and symptoms improvement could also be explained by a better medication adherence in these individuals. Moreover, HPA axis activity activates biological pathways in the brain and body, promoting adaptation to a stressful environment. Previous research has linked chronic stress to the etiology of BD,8,9 and BD patients are likely to be exposed to chronic stress throughout their lives.10 We proposed that HPA axis activity could be a marker of BD patients’ stress response. Stress responses to physiology and behavior depend highly on the stimulus types and categorize stress into physical and psychogenic. Psychogenic stressors such as affective symptoms and an unstable environment activate neurons in the caudal region of the dorsomedial medulla and the medial amygdala, which then activate the HPA.41 Although we have not fully elucidated the physiological and behavioral mechanisms by which the HPA axis functions in stress resilience, personality may contribute to the response strategy. We found that conscientiousness was associated with ACTH levels in patients with BD. While this personality trait has previously been linked to CORT but not ACTH in posttraumatic stress disorder.42 This implies that the results obtained may be unique to BD.
Furthermore, this is the first study to investigate how personality influences the relationship between the HPA axis activity and BD symptoms, and our findings revealed that an ACTH-Conscientiousness-CGI changing scores mediation model was established, indicating conscientiousness personality traits mediated the effect of ACTH on BD curative efficacy over 8 weeks. Previous studies have shown that BD patients’ personality profiles differ from the healthy controls, with higher openness to experience and neuroticism.43,44 According to one study, personality traits can distinguish between depression and manic states of BD, and a shared genetic etiology has been proposed for both BD and personality traits.43 Conscientiousness was associated with depressive symptoms, whereas manic symptoms were associated with increased extraversion and decreased agreeableness.43 Extensive reviews have highlighted amygdala, hippocampus, and cortical prefrontal alteration in BD patients.45–47 However, some studies have suggested that the conscientiousness personality trait is also associated with amygdala activity.48,49 Recent reviews have linked chronic stress disorders to structural and functional abnormalities in the amygdala, cingulate, and hippocampal regions.50,51 Therefore, we can hypothesize that HPA axis activation affects BD symptoms via the same neural circuit that includes the amygdala, and the association is mediated by personality traits that make people vulnerable to chronic stress.
Limitations
Following are the limitation of our study. First, the hormone levels were determined at a single point in time, although ACTH and CORT levels may vary due to circadian variation. The ideal method of establishing the reliability of hormone levels is to collect data at multiple time points throughout the day, which is difficult for the real-world study design. To address this limitation, we collected the blood samples for hormone determination between 8:00–9:00 AM, as this is when HPA axis hormone levels are at their peak in the diurnal cycle. Another limitation was that we did not evaluate the impact of pharmacologic therapies on clinical outcomes; however, there was no significant difference in the medication treatment model between the two trajectory clusters. Future prospective randomized controlled trials may enable the comparative investigation of the effect of HPA axis activity on the therapeutic efficacy of a specific treatment option. Finally, our study adopted a short-term follow-up design, limiting our ability to explore the long-term influence of personality and the HPA axis BD symptoms. Nevertheless, long-term follow-up will be continued with multiple measurements of HPA axis hormones.
Conclusions
We found that a higher level of ACTH is associated with more severe manic symptoms, indicating a chronic stress response in BD patients. Additionally, ACTH levels affect short-term BD curative efficacy via the mediation of conscientiousness, providing evidence that psychotherapeutic interventions targeting personality to improve the stress response would favor clinical outcome prediction.
Abbreviations
BD, bipolar disorders; HPA, hypothalamic–pituitary–adrenal; CORT, glucocorticoid cortisol; ACTH, adrenocorticotropin; NEO-FFI, NEO Five-Factor Inventory; MADRS, Montgomery Asberg Depression Rating Scale; YMRS, Young Mania Rating Scale; CGI, Clinical Global Impression; DTW, dynamic time warping.
Data Sharing Statement
We guarantee the authenticity of the data, but do not disclose the data, if necessary, you can email [email protected] to obtain the data.
Ethics Approval
The study conformed to the principles of the Declaration of Helsinki and was approved by the Institutional Ethics Board of the Chinese Clinical Trial Registry (The registration number is ChiECTR-20180187).
Acknowledgment
We gratefully acknowledge the participants of this study for generously donating their time. We would like to thank the research staff for their dedication to this project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the West China Psychiatric Association, China. Grant ID: WCPASX-2016. It provided the fund for the investigation, editing and the subject’s allowance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Association AP. Diagnostic and statistical manual of mental disorders, Fourth Edition (DSM-IV). Am Psych Ass. 2009;42:275.
2. Merikangas KR, Jin R, He JP, et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch Gen Psychiatry. 2011;68(3):241–251.
3. Cloutier M, Greene M, Guerin A, Touya M, Wu E. The economic burden of bipolar I disorder in the United States in 2015. J Affect Disord. 2018;226:45–51.
4. Hosang GM, Korszun A, Jones L, et al. Adverse life event reporting and worst illness episodes in unipolar and bipolar affective disorders: measuring environmental risk for genetic research. Psychol Med. 2010;40(11):1829–1837.
5. Romero S, Birmaher B, Axelson DA, et al. Negative life events in children and adolescents with bipolar disorder. J Clin Psychiatry. 2009;70(10):1452–1460.
6. Vieta E, Salagre E, Grande I, et al. Early Intervention in Bipolar Disorder. Am J Psychiatry. 2018;1:854.
7. Liu Y, Yang N, Hao W, et al. Dynamic proteomic analysis of protein expression profiles in whole brain of Balb/C mice subjected to unpredictable chronic mild stress: implications for depressive disorders and future therapies. Neurochem Int. 2011;58(8):904–913.
8. Hammen C. Stress and depression. Annu Rev Clin Psychol. 2005;1(1):293–319.
9. Paykel ES. Life events and affective disorders. Acta Psychiatr Scand Suppl. 2003;108(418):61–66.
10. Hammen C. Stress and depression. Annu Rev Clin Psychol. 2005;1:293–319.
11. Adinoff B, Junghanns K, Kiefer F, Krishnan-Sarin S. Suppression of the HPA axis stress-response: implications for relapse. Alcohol Clin Exp Res. 2005;29(7):1351–1355.
12. Kim LU, D’Orsogna MR, Chou T. Onset, timing, and exposure therapy of stress disorders: mechanistic insight from a mathematical model of oscillating neuroendocrine dynamics. Biol Direct. 2016;11(1):13.
13. Hill EE, Zack E, Battaglini C, Viru M, Viru A, Hackney AC. Exercise and circulating cortisol levels: the intensity threshold effect. J Endocrinol Invest. 2008;31(7):587–591.
14. Belvederi Murri M, Prestia D, Mondelli V, et al. The HPA axis in bipolar disorder: systematic review and meta-analysis. Psychoneuroendocrinology. 2016;63:327–342.
15. Fries GR, Vasconcelos-Moreno MP, Gubert C, et al. Hypothalamic-pituitary-adrenal axis dysfunction and illness progression in bipolar disorder. Int j Neuropsychopharmacol. 2014;18(1):84.
16. Maripuu M, Wikgren M, Karling P, Adolfsson R, Norrback KF. Relative hypo- and hypercortisolism are both associated with depression and lower quality of life in bipolar disorder: a cross-sectional study. PLoS One. 2014;9(6):e98682.
17. Leszczyńska-Rodziewicz A, Maciukiewicz M, Szczepankiewicz A, Pogłodziński A, Hauser J. Association between OPCRIT dimensions and polymorphisms of HPA axis genes in bipolar disorder. J Affect Disord. 2013;151(2):744–747.
18. Schreuder MM, Vinkers CH, Mesman E, Claes S, Nolen WA, Hillegers MH. Childhood trauma and HPA axis functionality in offspring of bipolar parents. Psychoneuroendocrinology. 2016;74:316–323.
19. Heim C, Ehlert U, Hellhammer DH. The potential role of hypocortisolism in the pathophysiology of stress-related bodily disorders. Psychoneuroendocrinology. 2000;25(1):1–35.
20. Heim C, Ehlert U, Hanker JP, Hellhammer DH. Psychological and endocrine correlates of chronic pelvic pain associated with adhesions. J Psychosom Obstet Gynaecol. 1999;20(1):11–20.
21. Miller GE, Chen E, Zhou ES. If it goes up, must it come down? Chronic stress and the hypothalamic-pituitary-adrenocortical axis in humans. Psychol Bull. 2007;133(1):25–45.
22. Jabben N, Nolen WA, Smit JH, Vreeburg SA, Beekman AT, Penninx BW. Co-occurring manic symptomatology influences HPA axis alterations in depression. J Psychiatr Res. 2011;45(9):1208–1213.
23. Feng G, Kang C, Yuan J, et al. Neuroendocrine abnormalities associated with untreated first episode patients with major depressive disorder and bipolar disorder. Psychoneuroendocrinology. 2019;107:119–123.
24. Valiengo LL, Soeiro-de-Souza MG, Marques AH, et al. Plasma cortisol in first episode drug-naïve mania: differential levels in euphoric versus irritable mood. J Affect Disord. 2012;138(1–2):149–152.
25. Cheng Y, Li Z, He S, Tian Y, He F, Li W. Elevated heat shock proteins in bipolar disorder patients with hypothalamic pituitary adrenal axis dysfunction. Medicine. 2018;97(27):e11089.
26. Feng X, Wang L, Yang S, et al. Maternal separation produces lasting changes in cortisol and behavior in rhesus monkeys. Proc Natl Acad Sci U S A. 2011;108(34):14312–14317.
27. Duffy A, Lewitzka U, Doucette S, Andreazza A, Grof P. Biological indicators of illness risk in offspring of bipolar parents: targeting the hypothalamic-pituitary-adrenal axis and immune system. Early Interv Psychiatry. 2012;6(2):128–137.
28. Manenschijn L, Spijker AT, Koper JW, et al. Long-term cortisol in bipolar disorder: associations with age of onset and psychiatric co-morbidity. Psychoneuroendocrinology. 2012;37(12):1960–1968.
29. Maripuu M, Wikgren M, Karling P, Adolfsson R, Norrback KF. Hyper- and hypocortisolism in bipolar disorder - A beneficial influence of lithium on the HPA-axis? J Affect Disord. 2017;213:161–167.
30. Holtzman CW, Trotman HD, Goulding SM, et al. Stress and neurodevelopmental processes in the emergence of psychosis. Neuroscience. 2013;249:172–191.
31. Vollrath M, Torgersen S. Personality types and coping. Pers Individ Dif. 2000;29(2):367–378.
32. Wittchen H, Wittchen HU, Wunderlich U, Gruschwitz S, Zaudig M, Wittchen H. SKID-I: strukturiertes Klinisches Interview für DSM-IV, Achse I. Psychische Störungen. 1997;1:84.
33. Mundt JC, Katzelnick DJ, Kennedy SH, Eisfeld BS, Bouffard BB, Greist JH. Validation of an IVRS version of the MADRS. J Psychiatr Res. 2006;40(3):243–246.
34. Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: reliability, validity and sensitivity. Br j Psychiatry. 1978;133:429–435.
35. Jones RM, Patel K, Moscovici M, McMaster R, Glancy G, Simpson AIF. Adaptation of the Clinical Global Impression for Use in Correctional Settings: the CGI-C. Front Psychiatry. 2019;10:687.
36. Yao R, Liang L. Analysis of the Application of Simplified NEO-FFI to Undergraduates. Chin J Clin Psychol. 2010;5:89.
37. Hucklebridge F, Hussain T, Evans P, Clow A. The diurnal patterns of the adrenal steroids cortisol and dehydroepiandrosterone (DHEA) in relation to awakening. Psychoneuroendocrinology. 2005;30(1):51–57.
38. Giorgino T. Computing and Visualizing Dynamic Time Warping Alignments in R: the dtw Package. J Stat Softw. 2009;31:87.
39. van den Berg MT, Wester VL, Vreeker A, et al. Higher cortisol levels may proceed a manic episode and are related to disease severity in patients with bipolar disorder. Psychoneuroendocrinology. 2020;119:104658.
40. Kirchner S, Lauseker M, Adorjan K, et al. Medication Adherence in a Cross-Diagnostic Sample of Patients From the Affective-to-Psychotic Spectrum: results From the PsyCourse Study. Front Psychiatry. 2021;12:713060.
41. Herman JP, Figueiredo H, Mueller NK, et al. Central mechanisms of stress integration: hierarchical circuitry controlling hypothalamo-pituitary-adrenocortical responsiveness. Front Neuroendocrinol. 2003;24(3):151–180.
42. Savic D, Knezevic G, Damjanovic S, Spiric Z, Matic G. The role of personality and traumatic events in cortisol levels–where does PTSD fit in? Psychoneuroendocrinology. 2012;37(7):937–947.
43. Barnett JH, Huang J, Perlis RH, et al. Personality and bipolar disorder: dissecting state and trait associations between mood and personality. Psychol Med. 2011;41(8):1593–1604.
44. Schouws SN, Paans NP, Comijs HC, Dols A, Stek ML. Coping and personality in older patients with bipolar disorder. J Affect Disord. 2015;184:67–71.
45. Berens AE, Jensen SKG, Nelson CA
46. Herzberg MP, Gunnar MR. Early life stress and brain function: activity and connectivity associated with processing emotion and reward. NeuroImage. 2020;209:116493.
47. Blond BN, Fredericks CA, Blumberg HP. Functional neuroanatomy of bipolar disorder: structure, function, and connectivity in an amygdala-anterior paralimbic neural system. Bipolar Disord. 2012;14(4):340–355.
48. Kunisato Y, Okamoto Y, Okada G, et al. Personality traits and the amplitude of spontaneous low-frequency oscillations during resting state. Neurosci Lett. 2011;492(2):109–113.
49. Morawetz C, Kirilina E, Baudewig J, Heekeren HR. Relationship between personality traits and brain reward responses when playing on a team. PLoS One. 2014;9(1):e87277.
50. Weis CN, Webb EK, Huggins AA, et al. Stability of hippocampal subfield volumes after trauma and relationship to development of PTSD symptoms. NeuroImage. 2021;236:118076.
51. Misquitta KA, Miles A, Prevot TD, et al. Reduced anterior cingulate cortex volume induced by chronic stress correlates with increased behavioral emotionality and decreased synaptic puncta density. Neuropharmacology. 2021;190:108562.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.