Back to Journals » Journal of Pain Research » Volume 18
Chronic Post-Surgical Pain After Hip and Knee Arthroplasty: An Update on Mechanisms, Risk Factors, and Interventional Treatment Modalities
Authors Banks DW ![]() , Park H
, Park H ![]() , Oehlermarx W
, Oehlermarx W ![]() , Suarez M
, Suarez M ![]() , Broachwala M, D'Souza RS
, Broachwala M, D'Souza RS ![]() , Reddy R
, Reddy R
Received 19 June 2025
Accepted for publication 4 November 2025
Published 20 November 2025 Volume 2025:18 Pages 6205—6219
DOI https://doi.org/10.2147/JPR.S546617
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jinlei Li
Dylan W Banks,1 Hannah Park,1 Whitman Oehlermarx,1 Michael Suarez,2 Mustafa Broachwala,3 Ryan S D’Souza,4 Rajiv Reddy3
1Department of Physical Medicine and Rehabilitation, New York University, New York, NY, USA; 2Department of Physical Medicine and Rehabilitation, Johns Hopkins Medicine, Baltimore, MD, USA; 3Department of Anesthesiology and Pain Medicine, University of California San Diego, San Diego, CA, USA; 4Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN, USA
Correspondence: Rajiv Reddy, Department of Anesthesiology and Pain Medicine, University of California San Diego, 3350 La Jolla Village Drive, San Diego, CA, 92161, USA, Email [email protected]
Abstract: In the United States, hip and knee arthroplasties are amongst the most frequently performed elective surgeries. While generally effective, a subset of patients develop chronic post-surgical pain (CPSP) in the affected joint. The management of CPSP is an incredibly important area of ongoing research, as the prevalence of individuals with arthroplasties continues to climb. Currently, there is a lack of best practice guidelines dedicated to CPSP of the hip and knee following arthroplasty. While conservative modalities including physical rehabilitation, pharmacologics, and psychological interventions remain the cornerstone of management of CPSP, this review aims to fill an important knowledge gap by providing an overview of the existing interventional treatment modalities. Procedures discussed include radiofrequency ablation (RFA), pulsed radiofrequency (PRF), peripheral nerve stimulation (PNS), spinal cord stimulation (SCS), dorsal root ganglion (DRG) stimulation, and intrathecal drug delivery systems (IDDS). Moreover, it explores other emerging therapies. To date, RFA for CPSP has the most supporting evidence, with strong support for cooled RFA. However, neuromodulation techniques including PRF, PNS, SCS and DRG stimulation each may offer promising results in treating CPSP of the hip and knee. Ultimately, without comparative analyses, the decision regarding which to pursue relies upon shared decision-making with the patient focused on tailoring treatments to the presumed underlying mechanism in line with resource availability and associated costs.
Keywords: chronic pain, arthroplasty, total joint replacement, radiofrequency ablation, neuromodulator, spinal cord stimulation
Introduction
Hip and knee osteoarthritis are prominent sources of pain and disability.1 In response, total hip arthroplasty (THA) and total knee arthroplasty (TKA) rank amongst the most commonly performed elective procedures, with an estimated 1 million arthroplasties performed annually in the United States (US). As of 2010, there were an estimated 2.5 million and 4.7 million US individuals who had undergone a THA or TKA, respectively.2 These numbers continue to increase as the demand for improved function and quality of life increases with an aging population.2 Regression modeling of Centers for Medicare and Medicaid Services data projects that by 2040, the annual number of THAs will increase by 176% to 719,364 procedures and TKAs will increase by 139% to 1,982,099.3
While THAs and TKAs are generally considered effective in improving pain and functional levels, there remains a subset of patient with chronic post-surgical pain (CPSP) in their affected joint.4 The estimated rate of CPSP varies depending on study criteria, with some literature reporting it may be as high as 26–58% for THAs and 28–30% for TKAs.1,5,6 There is a greater amount of literature discussing post-TKA interventions, likely in part due to a higher prevelance.2 CPSP contributes to suboptimal functional recovery and thus adversely impacting quality of life.7 Moreover, CPSP may increase the risk of persistent postoperative opioid use.8
While conservative modalities including physical rehabilitation, pharmacologics, and psychological interventions remain the cornerstone CPSP management, there is a growing interest and need for interventional techniques to manage symptoms for individuals who have failed conservative modalities and are either not candidates for or do not desire additional surgery. While guidelines exist on the general treatment of painful joints, there is a lack of consensus best practice guidelines specifically related to the treatment of CPSP.9 Given the variability in study designs, patient populations and outcomes, this narrative review aims to synthesize the available evidence for interventional techniques, namely radiofrequency ablation (RFA), pulsed radiofrequency (PRF), peripheral nerve stimulation (PNS), spinal cord stimulation (SCS), dorsal root ganglion (DRG) stimulation, and intrathecal drug delivery systems (IDDS) in the setting of CPSP. This will supplement and expand upon existing reviews, which focus on acute postoperative pain management, conservative modalities, TKAs alone, or on individual treatment modalities.7,10–12 While best practice guidelines remain an extraordinarily important area of future research, this narrative review offers a synthesis of existing interventional techniques to inform clinical practice. It seeks to answer the following research questions: (1) What procedural interventions are being utilized to manage CPSP following hip and knee arthroplasty? (2) What is the level of evidence supporting their utilization? (3) What gaps exist for future studies?
Mechanisms of Chronic Post-Surgical Pain
The International Association for the Study of Pain defines CPSP as a chronic secondary pain condition that is characterized by pain that develops or increases following a surgical procedure and persists beyond 3 months. The pain is localized to the surgical site or referred to an innervation territory of a surrounding nerve, with pain not better explained by pre-existing conditions. Sub-diagnoses, such as chronic pain after arthroplasty, are further classified under the ICD-11.13
The basis of CPSP is likely multifactorial. Peripheral sensitization arises in the setting of surgical injury, leading to hyperexcitability of nociceptors via direct nerve damage and the release of inflammatory mediators. This is mediated by the increased expression of pro-nociceptive ion channels such as transient receptor potential channels, acid-sensing ion channels, transient receptor potential cation channels subfamily V member 1, mechanistic target of rapamycin, and Nav1.7 sodium channels in the DRG, which all lend to amplify signal transmission.14–16 Prolonged nociceptive input can result in spinal neurons that have become sensitized which is mediated by N-methyl-D-aspartate (NMDA) and α-amino-3-hydroxy-5-methyl-4-isoxazoleproprionic acid receptors, brain-derived neurotrophic factor, as well as activation of glial cells. These glial cells release pro-inflammatory cytokines and chemokines further increasing neuronal excitability and maintenance of the sensitized state.14,15 Additional mechanisms include maladaptive neuroplastic changes, impaired descending inhibition, and persistent activation of the innate immune system by way of the cyclic guanosine monophosphate synthase stimulation of the interferon genes pathway.17 There are also a variety of psychological and genetic factors, such as anxiety, depression, somatization, sleep disturbance, catastrophizing, resilience, social factors, and gene polymorphisms that contribute to CPSP susceptibility.18,19
Risk Factors for Developing Refractory Chronic Post-Surgical Pain
The risk factors for developing CPSP following THAs and TKAs remain inconsistent across studies and an important area of investigation. A meta-analysis by Ghoshal et al including 171,354 patients found that higher anxiety and depression scores were associated with increased risk of CPSP following TKA.20 This is suspected to be due to shared neural circuitry between pain and emotional regulation.21 Interestingly, Ghoshal et al did not find any consistent risk factors for CPSP following THA, which raises the question of potentially different mechanisms contributing to the two CPSP conditions. Other possible risk factors reported by Ghoshal et al, though with limited consistency across studies, include female sex, younger age, higher body mass index, and pre-existing psychiatric conditions such as depression and anxiety.20 A systematic review by Li et al including 18,792 patients who underwent TKA reported 10 variables as strongly associated with CPSP including age, body mass index, comorbidities, preoperative pain, chronic widespread pain, preoperative adverse health beliefs, preoperative sleep disorders, central sensitization, preoperative anxiety, and preoperative function.22 A review by Zhang et al found the most consistent risk factors for developing CPSP following THA included worse preoperative pain and function in addition to more severe comorbid diseases and psychiatric conditions.23 Taken together, it is challenging to identify consistent risk factors for the development of CPSP following arthroplasty. These findings highlight the importance of a holistic approach to understanding and managing CPSP following arthroplasty.
Non-Interventional Treatment Modalities
The optimal approach to managing CPSP involves a patient-centered multimodal strategy. This includes physical therapy and rehabilitation, pharmacologic therapy, psychosocial interventions including cognitive behavioral therapy, followed by interventional therapies if indicated.24
Physical therapy and rehabilitation remain the cornerstone of post-arthroplasty recovery. It remains the standard for improving range of motion and reducing postoperative fibrosis and scar tissue formation. Because of this, postoperative therapy is critical for optimizing functional recovery and pain control. While a significant degree of heterogeneity exists between TKA and THA therapy protocols, systematic reviews comparing protocols found no significant differences in pertinent outcomes including pain reduction, strength recovery, activities of daily living, or quality of life.24,25
Pharmacologic management also plays a critical role in post-arthroplasty pain control. Adequate pain relief in the early postoperative stage often promotes early ambulation and can correlate with long-term pain control.26 Multimodal pharmacologic management is often recommended, including topical medications, acetaminophen, nonsteroidal anti-inflammatory drugs, and opioids as indicated.27 Given that central and peripheral sensitization are implied in CPSP, often manifesting with a neuropathic component to pain manifestation, consideration of neuropathic analgesic adjuncts should also be explored as part of a multimodal analgesic strategy. These analgesic adjuncts may include gabapentinoids, tricyclic antidepressants, and selective norepinephrine reuptake inhibitors.
As anxiety and depression are commonly reported risk factors for developing CPSP, psychological interventions are also an essential cornerstone in CPSP management. The value psychological interventions offer has been well supported by prior reviews examining all forms of CPSP as well as CPSP specifically following arthroplasty.28,29 These reviews have demonstrated decreased post-surgical pain and disability, improved patient satisfaction, quality of life, and reduction of healthcare costs.29 In light of this, psychiatric treatment remains essential prior to consideration of subsequent procedural interventions.
Ultimately, if conservative modalities fail to provide adequate analgesic relief and further surgical intervention is either not indicated or desired, interventional therapies can be considered.
Interventional Techniques
Radiofrequency Ablation
RFA is a minimally invasive procedure that treats pain by using radiofrequency energy to generate heat, creating a thermal lesion on the targeted nerve to interrupt pain signal transmission. RFA is particularly effective for chronic pain conditions such as knee and hip osteoarthritis, facet joint pain, and chronic migraines. Similarly, cooled RFA (CRFA) is a subtype of RFA that uses internally cooled electrodes, which allows for the creation of larger and more spherical lesions compared to standard RFA that can be advantageous in targeting complex nerve innervations and providing more extensive pain relief.30,31
The common nerves targeted by RFA at the knee are typically the genicular nerves, which provide innervation to the majority of the knee. Multiple studies and reviews have described the efficacy of RFA for knee pain, especially when targeting the superomedial (SM), superolateral (SL), and inferomedial (IL) genicular nerves. Reviews have demonstrated high rates of success in alleviating chronic nonsurgical knee pain through 12 months by targeting these genicular nerves.32,33 The American Society of Pain and Neuroscience recommended targeting the SM, SL, and IM genicular nerves for RFA in their 2021 guidelines, citing consistent efficacy in reducing pain and improving function.34
Several studies highlight the efficacy of RFA for post-TKA pain (Table 1). Shi et al found comparable success rates between post-TKA and osteoarthritic knee pain following RFA, supporting the broad applicability of this technique.35 Moreover, a study by Khan et al involving 19 post-TKA patients treated with CRFA showed significant improvements in Knee Injury and Osteoarthritis Outcome Scores as well as visual analog scale (VAS) at a mean follow-up of 10.2 months.36 Additionally, a 2022 systematic review which included 11 studies with 265 patients noted a 63% success rate, defined as at least 30% pain relief lasting three months or more, among post-TKA patients treated with CRFA.37 These findings suggest CRFA as a strong option for patients with persistent post-TKA pain who have failed conservative management strategies.
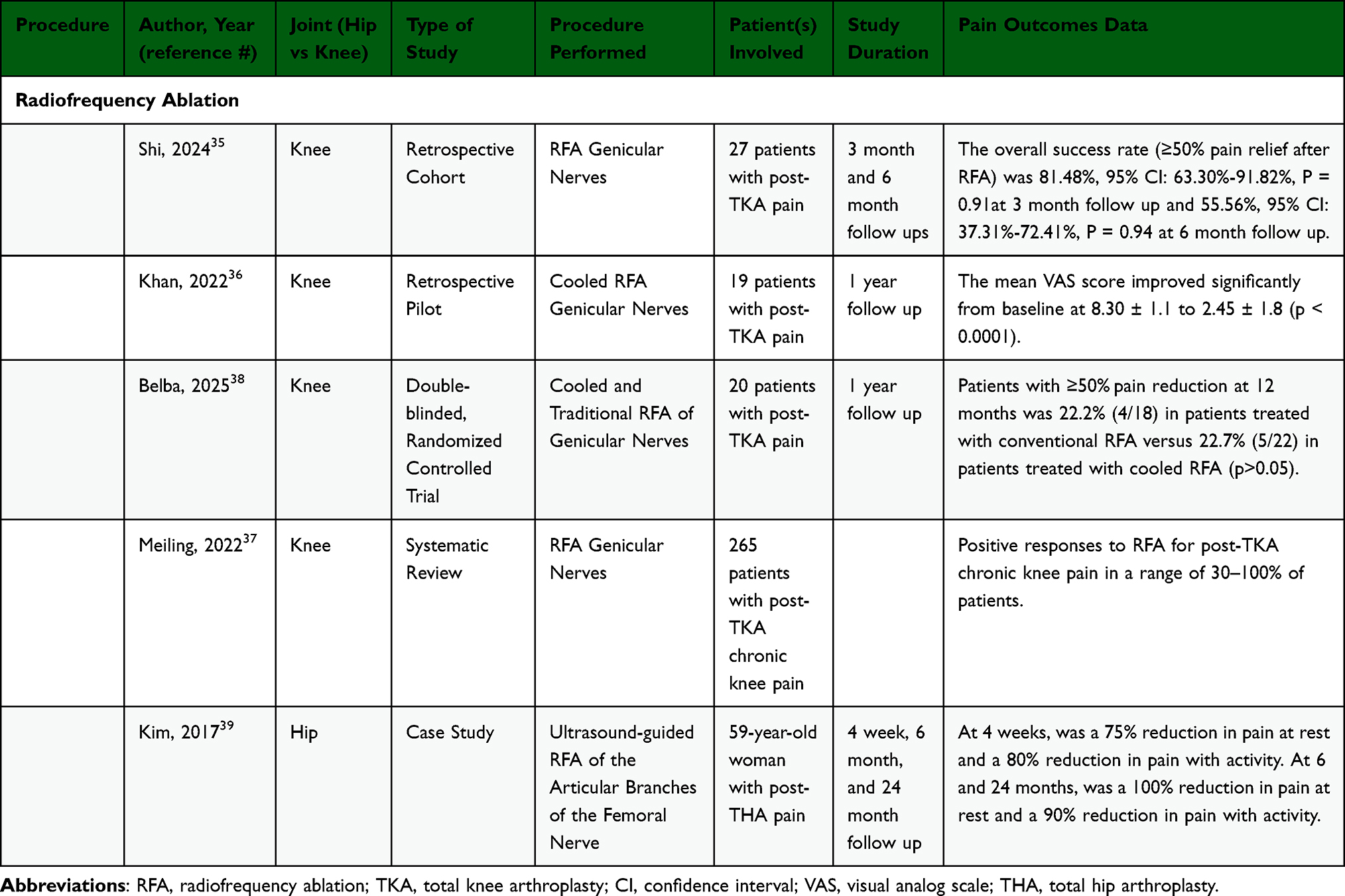 |
Table 1 Data Summary of Radiofrequency Ablation for Chronic Post Hip and Knee Arthroplasty Pain |
Comparative studies between CRFA and traditional RFA suggest differences in outcomes based on timing and patient needs. Wu et al found that RFA may offer superior short-term pain relief through 6 months post-procedure, with significant pain relief reported by 79% of RFA patients versus 59% of CRFA patients.40 However, long-term outcomes at 12 months were comparable between modalities. The COCOGEN Trial further examined CPSP after TKA, finding that CRFA-treated patients achieved statistically significant higher rates of at least 30% pain reduction at 12 months in comparison to traditional RFA. Additionally, CRFA was found to be more cost-effective in CPSP management, likely due to its ability to create larger lesions that better target the altered anatomy and neuropathic components associated with TKA-related pain.38
The primary nerves involved in hip pain, and thus common targets for RFA or CRFA, are the articular branches of the obturator nerve, femoral nerve, and to a lesser extent, the sciatic nerve.34 The obturator nerve primarily innervates the anteromedial aspect of the hip joint, while the femoral nerve innervates the anterior and SL aspects of the hip capsule. The sciatic nerve contributes to posterior innervation. These nerves are frequently implicated in chronic hip pain, including post-arthroplasty pain, and targeting their articular branches has repeatedly shown promise in pain relief.39,41 A recommended location to place the RFA probe is at the anterior IM aspect of the hip capsule, where these nerves converge. However, variability in nerve anatomy and the presence of additional articular branches from other nerves, such as the superior gluteal and quadratus femoris nerves, may limit complete pain resolution.42,43 Diagnostic nerve blocks are best used to confirm the involvement of these nerves prior to RFA.
Current literature demonstrates significant efficacy of RFA in reducing nonsurgical chronic hip pain, primarily for pain due to osteoarthritis. Studies report osteoarthritic hip pain relief ranging from 30% to >80% at follow-up durations of 3 months to 3 years. For instance, Rivera et al observed a 38% reduction in mean VAS scores at 6 months in 18 patients with hip pain treated with RFA.44 Kapural et al reported that 69% of patients experienced >50% osteoarthritic pain relief at 6 months and 52% at 12 months. In another cohort of 52 patients with osteoarthritic pain undergoing CRFA, Kapural et al found that pain scores improved significantly (P < 0.01).41 Lastly, Cheney et al summarized nine studies showing 30–80% pain reduction with durable relief for up to 36 months.45
Data specific to post-THA patients, however, remain limited. A case report was identified, which described a case of a 59-year-old woman with chronic post-arthroplasty hip pain treated with CRFA of the articular branches of the femoral nerve. The patient reported significant pain relief at 24-month follow-up.39 While RFA and CRFA show promise for treating chronic hip pain, data specific to post-THA pain is sparse and thus further research is needed to establish the efficacy and safety of these interventions in this patient population.
Overall, both RFA and CRFA are viable options for managing chronic post-TKA pain, however there is significantly limited data examining post-THA pain limiting its current application. For post-TKA pain, studies show that RFA may offer superior short-term relief, while CRFA provides comparable or superior long-term outcomes with potential advantages in treating persistent or neuropathic pain due to larger lesion creation and better cost-effectiveness.38,40 Further large-scale, long-term studies are warranted to optimize patient selection, refine procedural techniques, and quantify outcomes.
Pulsed Radiofrequency
In contrast to RFA, which utilizes high temperatures and results in local tissue destruction, PRF is a form of neuromodulation which uses short, high-voltage bursts, which alters the neuronal membrane, affects gene expression, and influences cytokine release.46 The target tissue temperature is 42°C, resulting in no permanent tissue damage.
A case series by Vas et al was the first to describe the use of PRF in two patients with chronic pain after TKA (Table 2). A combination of dry needling and ultrasound-guided PRF to the saphenous, tibial, and common peroneal nerves was used. This combination treatment was selected due to a new theory that post-TKA pain is a neuromyopathic phenomenon involving both sensory and motor neuropathy. Both patients reported 50–60% pain relief immediately and improved feeling of stiffness.47 A retrospective study describing the use of PRF to the L4 DRG demonstrated improvement in VAS, reduction in neuropathy scales, and higher satisfaction rate compared to transcutaneous electrical nerve stimulation (TENS) and exercise alone in patients who were at least 2 months after TKA with persistent pain.48 Lastly, a large retrospective study by Chen et al including 265 patients, 140 of which were post-TKA, underwent RFA, CRFA, or PRF for knee pain.49 Target nerves were the genicular nerves, nerves to vastus medialis, intermedium, and lateralis, recurrent fibular nerve, and infrapatellar branch of the saphenous nerve. Overall, 63% of patients had at least 30% decrease in average knee pain lasting at least 3 months. Higher success rates were noted with CRFA versus PRF or RFA (67.5% success in the CRFA group versus 54.5% in the RFA group and 42.9% in the PRF group). Though the study did not isolate post-TKA patients, this large study supported the efficacy of all types of radiofrequency in patients with chronic knee pain both with and without surgical intervention.49 In summary, PRF is a promising treatment technique being studied both peripherally on nerves innervating the knee and centrally at the DRG. Across these studies, there has been consistent improvement in reports of pain and some improvements in functional outcomes for patients who had symptoms after TKA.
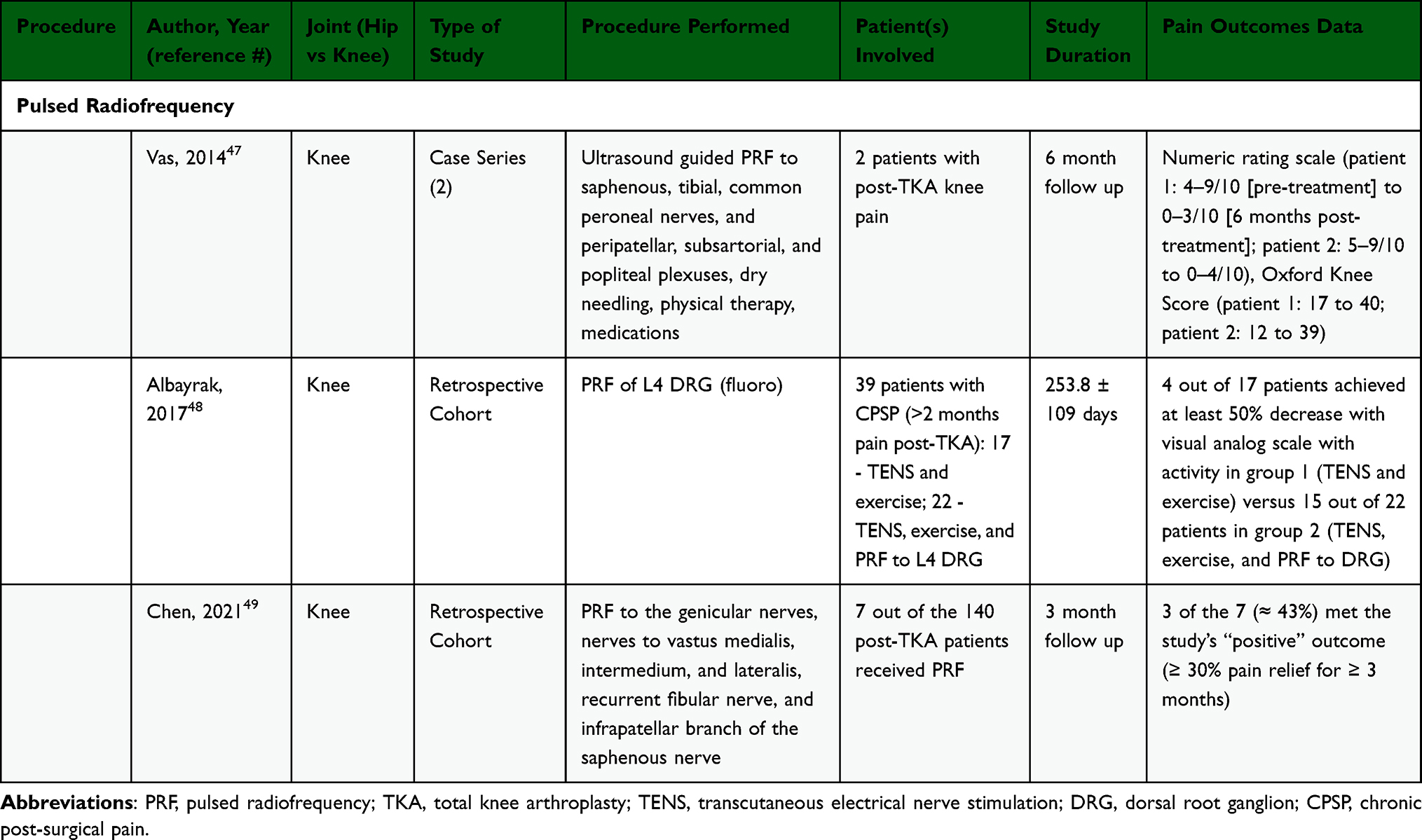 |
Table 2 Data Summary of Pulsed Radiofrequency for Chronic Post Hip and Knee Arthroplasty Pain |
There are no studies specifically assessing PRF for post-THA pain; however, the efficacy of PRF for osteoarthritic hip pain is well supported. As an example, Tinnirello et al utilized PRF of the femoral and obturator nerves and found >50% pain reduction through 6 months follow-up.50 Ultimately, the potential role of PRF in managing post-THA pain warrants further investigation.
Peripheral Nerve Stimulation
PNS is a technique that involves the placement of electrical leads onto large, myelinated afferent peripheral nerve fibers, thus interfering with transmission of pain signals from small pain fibers via the gate control theory.51 PNS previously required surgery for placement and removal, but with the development of smaller leads, placement became possible under ultrasound guidance. Another benefit is the ability to stimulate larger nerve trunks rather than distal branches, allowing for fewer leads further from the surgical site to cover areas of pain.52
The first case report describing PNS for chronic post-TKA pain was in 2010, in which two patients more than one year post-arthroplasty were provided periarticular PNS with significant improvement in their pain and function.53 Subsequent literature includes two case reports, two case studies, and two prospective studies, all of which demonstrated subjective improvement in pain and functional improvements (Table 3).52,54–56 Chauhan et al described the use of wireless PNS to the SM genicular nerve for a patient who had failed genicular nerve RFA. The patient reported over 80% improvement in their knee pain and had weaned off opioid medications at six-month follow-up.55 Recently, a randomized control study by Goree et al comparing 20 patients receiving PNS with 21 patients who received sham stimulation demonstrated greater pain relief and distances on the six minute walk test in the PNS group.57 Common targets for PNS in post-TKA patients are the femoral, saphenous, and sciatic nerves. Anterior and posterior knee pain can be targeted by the femoral and sciatic nerves respectively, and medial knee pain can be addressed with the saphenous nerve, a sensory branch of the femoral nerve.52,54,55,57 One case report also described targeting the SL genicular nerve with fluoroscopic guidance.54 Placing two leads provides more robust stimulation than one lead alone. Two leads may be inserted on the same nerve if one nerve provides adequate pain control.56 No significant adverse effects were noted in the studies.
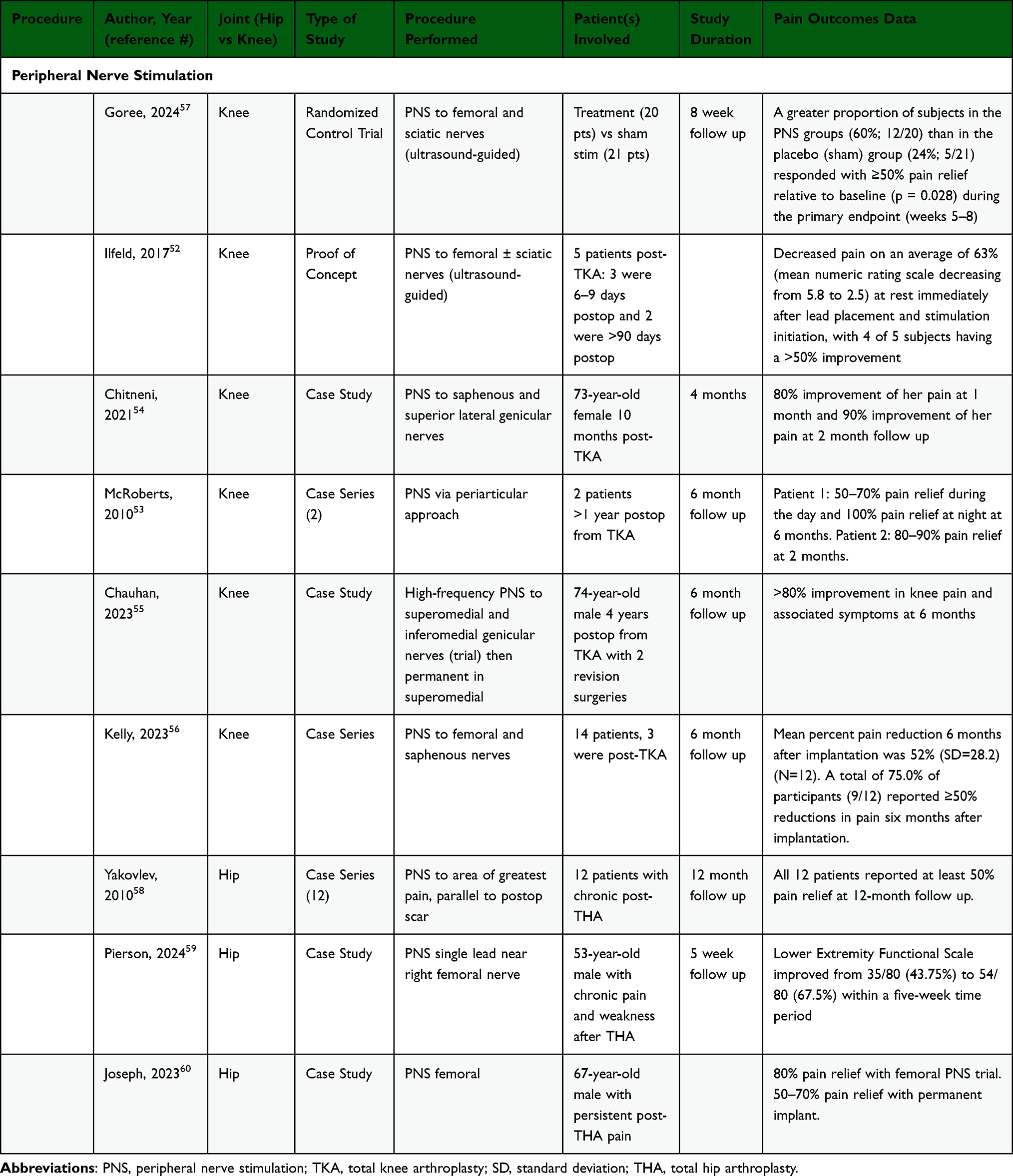 |
Table 3 Data Summary of Peripheral Nerve Stimulation for Chronic Post Hip and Knee Arthroplasty Pain |
Few studies have described the use of PNS in post-THA patients, specifically two case reports and one case series. The two case reports described stimulating the femoral nerve while the case series described placement of the leads over the greatest area of pain, parallel to the postoperative scar over the affected upper lateral thigh.58–60 Though there is a lack of randomized trials involving PNS use in patients with chronic hip pain after THA, the few studies described demonstrate improvement of pain after PNS with some improvements in functional outcomes.
Spinal Cord Stimulation
SCS is a treatment modality for chronic pain with on-label indications for persistent spinal pain syndromes (type I and II), painful diabetic neuropathy, and complex regional pain syndrome (CRPS). SCS therapy is associated with improved analgesia, physical function, emotional function, patient satisfaction, quality of life, along with a reduction in analgesic use with potential cost saving implications, though long-term outcomes remain an important area of ongoing investigation.61,62 It is proposed that SCS works by way of the gate control theory delivering electrical impulses to large sensory fibers in the dorsal column.63,64 While SCS has had many applications in various pain conditions, there appears to be a paucity of literature surrounding the use of SCS in post-TKA and post-THA pain.
SCS for post-TKA pain was first mentioned in 2010 in a case report by Lowry and Simopoulos, followed by a case series by Gillis et al in 2007.65,66 Of the literature reviewed, including one case series, two case reports, and two abstracts, all patients underwent a myriad of treatment options from oral analgesics, therapy, nerve blocks, and RFA, to revision surgeries to treat their post-TKA pain before trialing SCS (Table 4).65–69 SCS had a variable but positive impact on all patients reported. Lowry and Simopoulos describe a patient who underwent SCS implantation and subsequently experienced less pain with activity and significant improvement in her Oxford Knee Score over 1 year.65 Gillis et al published a case series describing 3 patients who found relief with SCS. All three cases demonstrated significant pain relief, functional improvement, and reduction or cessation of oral analgesic medication.66 Urits et al report a patient with complete resolution of pain and opioid use at 6 months post-implant.67 Reeves and Torres published an abstract where their patient experienced >80% relief during SCS trial and underwent subsequent implantation.68 Patel and Nicholson reported >75% relief in their patient after SCS.69
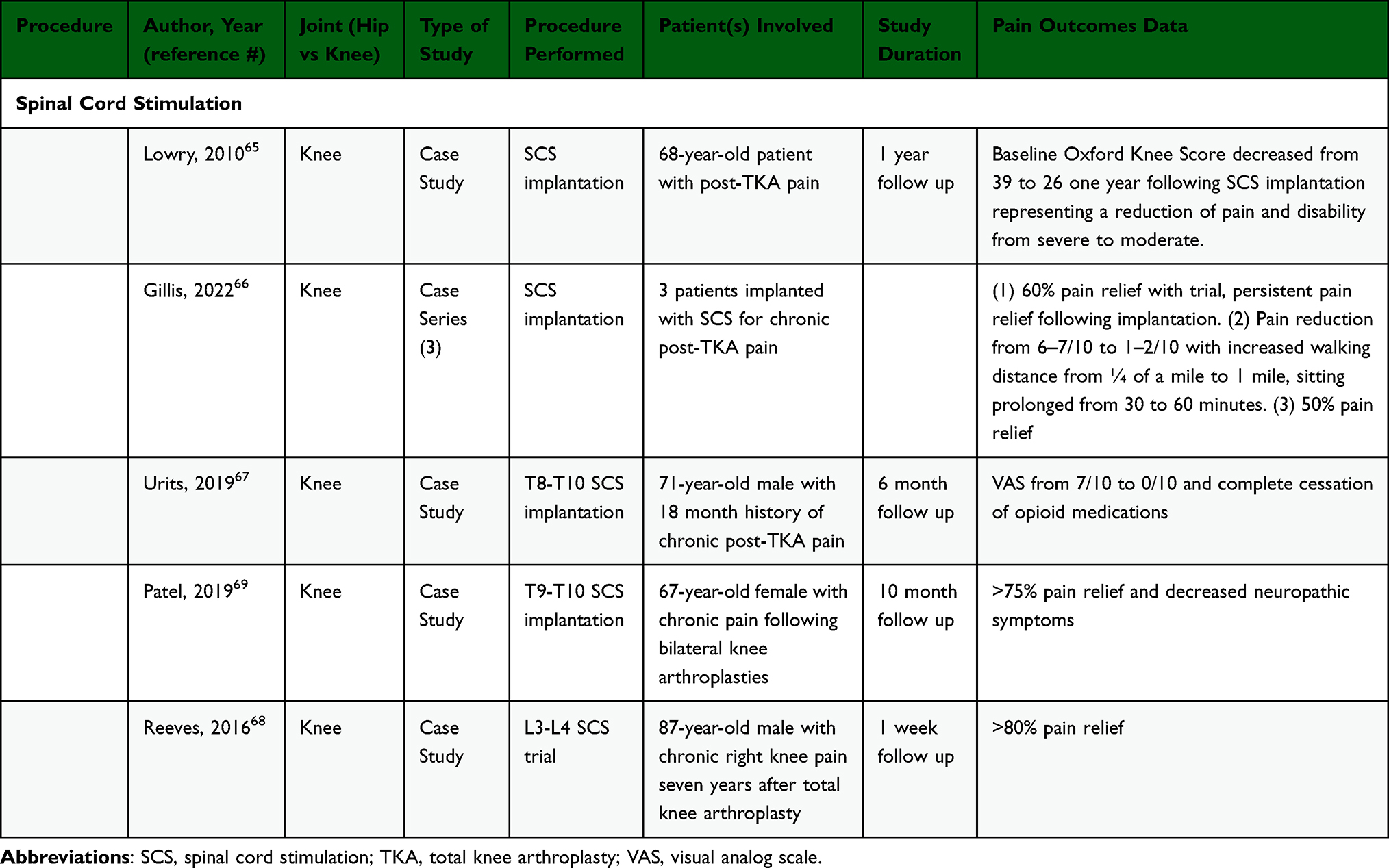 |
Table 4 Data Summary of Spinal Cord Stimulation for Chronic Post Hip and Knee Arthroplasty Pain |
There was no reference to SCS used in post-THA pain found in the literature. There is evidence to support that patients have developed CRPS post-THA.70,71 SCS has been utilized, and demonstrated efficacy in treating CRPS.61,72,73 It is then plausible that SCS could provide relief to this patient population if they fail to respond to more conservative measures.
Although there is a lack of high-quality evidence in the use of SCS in post-TKA pain and an absence of evidence for post-THA pain, the literature that does exist shows significant pain relief in these patients and warrants further research to optimize its use in these populations.
Dorsal Root Ganglion Stimulation
DRG stimulation is another form of neuromodulation with increasing utilization, though similar to SCS, long-term outcomes remain an important area of ongoing investigation. In comparison to SCS, DRG stimulation offers advantages such as greater spatial selectivity and reduced sensitivity to positional changes.63,74,75 DRG stimulation has evidence supporting its use in treating chronic focal neuropathic pain and CRPS.76 DRG stimulation is thought to impart pain relief in a variety of mechanisms including modulating action potentials at the DRG, reducing hypersensitivity of sensory neurons, influencing cellular ion and chemical activity, and reducing inflammation.77
Shulthesis et al published a prospective observational study including 11 patients with post-TKA pain (Table 5). All patients underwent a L3-L4 nerve block and if experienced ≥50% pain relief then selected for implantation at that level, if <50% relief or area of pain not covered additional roots were blocked, and if ≥50% pain relief with additional root then underwent implantation. All subjects underwent implantation. Average VAS decreased from 8.6 to 3.0. Knee range of motion improved by 24.5 degrees and walking distance dramatically increased from 125 to 1481 meters. Cessation of opioids, antidepressants, and/or anticonvulsants in 73% of patients.78 Gravius et al conducted a two-part clinical trial where they followed 24 patients, 12 who have post-TKA pain and diagnosed CRPS who underwent selective L4 DRG stimulation. Ten patients responded with ≥50% pain relief and moved to implantation where they experienced statistically significant decreases in VAS. At 3 months follow-up they reported a 61.3% reduction in pain with 60% of participants noting at least 50% decrease in pain. Interestingly, they also reported these patients with CRPS displayed a pro-inflammatory molecular pattern in serum and following DRG stimulation showed a decrease in serum IL-10 and increase in salivary oxytocin, providing insight into the mechanism surrounding neuroimmune modulation.79,80
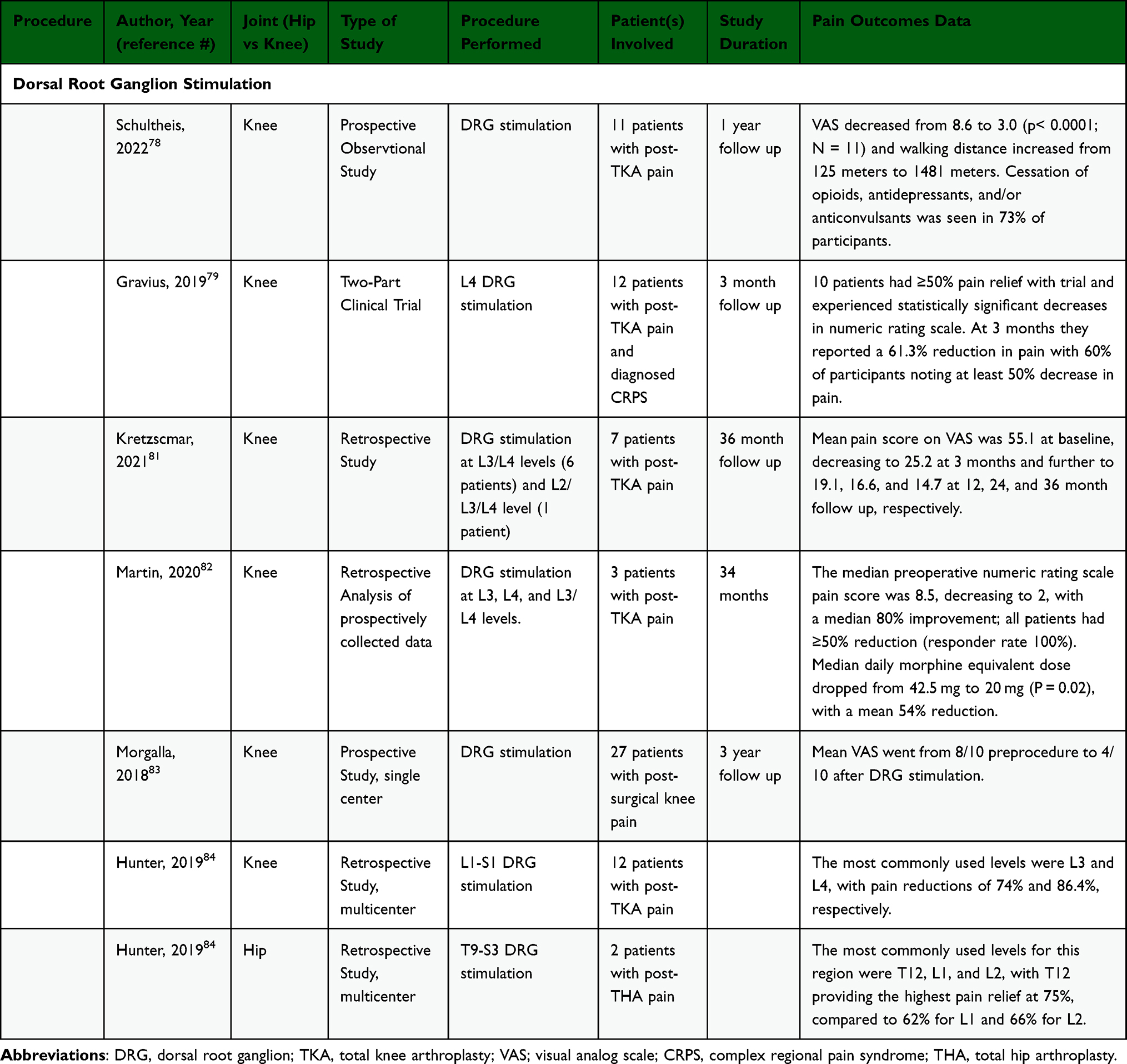 |
Table 5 Data Summary of Dorsal Root Ganglion Stimulation for Chronic Post Hip and Knee Arthroplasty Pain |
There is also a collection of literature where post-TKA patients make up a subset of the patients implanted with DRG stimulation. Kretzscmar et al conducted a retrospective study including 21 patients who received DRG stimulation, 7 of which with post-TKA pain. Of the 7 patients, 6 received DRG stimulation at L3/L4 levels and 1 patient at L2/L3/L4 level. For the entire cohort, at 36 month follow up, they reported significant pain relief, mental and physical improvement, increase in quality of life, and 20 patients were completely opioid free.81 Martin et al conducted a retrospective analysis of prospectively collected data on 14 patients undergoing DRG stimulation for chronic knee pain, 3 of which had post-TKA pain. Twelve patients underwent implantation. For the 3 post-TKA pain patients, DRG leads were placed at L3, L4, and L3/L4 levels. For the entire cohort, they reported median pain improvement score of 80%, median coverage of 85%, and all but 1 patient had reduced need for opioid medication over a mean 34 month follow-up.82 Morgalla et al completed a prospective, single-center investigation on a cohort of 62 patients, 27 of which were implanted with DRG stimulation for post-surgical knee pain, however it is unclear how many were post-TKA specifically. Of the starting 27, 16 were followed for three years with an average improvement in VAS by 69.2% in this group.83 Within a larger cohort of patients, Hunter et al included 12 patients with post-TKA pain treated with DRG stimulation. The average number of leads implanted was two and trial stimulation resulted in approximately 70% pain relief overall with subsequent implantation in 8 patients. These authors recommended ipsilateral L3 and L4 DRG stimulation for this patient population.63,84 No discrete data was found for post-THA pain however, Hunter et al also included 2 post-THA pain patients reporting T12, L1, and L2 DRG stimulation in the larger subset of groin/hip patients with T12 showing the highest percentage of pain relief.63,84
There appears to be a growing body of evidence to suggest the efficacy of DRG stimulation in the use of post-TKA pain. While the literature is lacking for post-THA pain, the available evidence points to a positive result. While DRG stimulation can be considered for patients with post-TKA and post-THA pain, more high-quality research is needed to solidify its use in this population.
Intrathecal Drug Delivery
Only one case was found describing the use of IDDS in a patient with post-THA pain (Table 6). Dahm et al describe a 77-year-old woman who underwent THA and subsequently developed refractory nociceptive-neuropathic pain located at ventral and dorsal aspects of the left hip. Intrathecal treatment bupivacaine and buprenorphine provided 85–100% pain relief for a follow-up period of 6 years.85
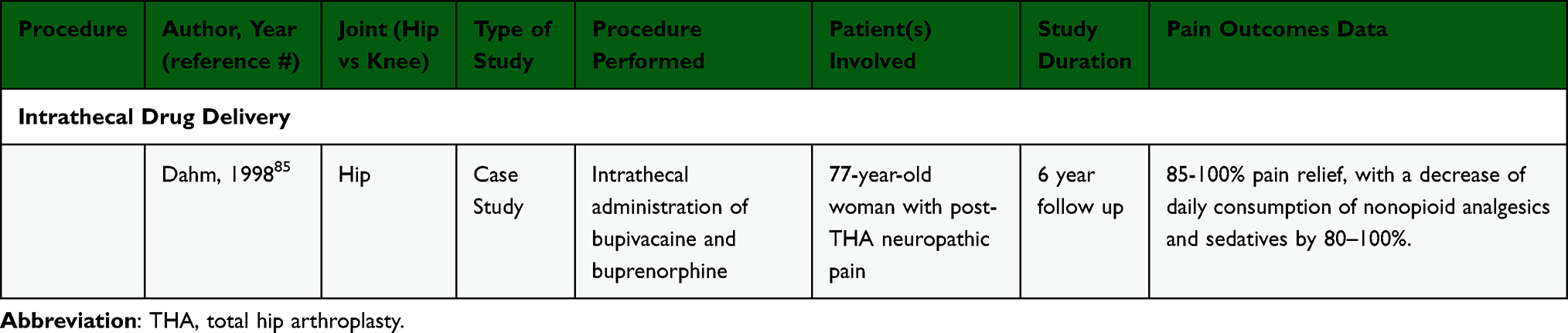 |
Table 6 Data Summary of Intrathecal Drug Delivery Systems for Chronic Post Hip and Knee Arthroplasty Pain |
Emerging Therapies
Genicular artery embolization is emerging as a possible intervention to address post-TKA CPSP. Currently, there is a lack of substantial evidence, however the first randomized control trial is underway. These researchers will take up to 112 patients with post-TKA pain and will provide either microparticle genicular artery knee embolization or sham saline. Outcomes that will be assessed include changes in pain, mobility, use of pain medications, duration of improvement, and adverse effects.86
Cryoanalgesia, or cryoneurolysis, is an intervention which has been utilized for decades for both acute and chronic pain management, notably with variable evidence, but has recently been studied for post-TKA CPSP. Cryoanalgesia relies upon the application of extremely low temperature (−78°F) to targeted nerves, ultimately creating Wallerian degeneration within the axon without disrupting surrounding connective tissue structure. In earlier applications, cryoneurolysis was applied to the infrapatellar branch of the saphenous nerve for knee osteoarthritis with improved pain, and has also been utilized perioperatively with knee arthroplasty with notable reduction of hospital length and opioid use.87,88 More recently, Bianco et al applied cryoanalgesia to the genicular nerves of patients with chronic knee pain, including some with post-TKA CPSP, and found statistically significant and impactful improvements of pain, neuropathic symptoms, and quality of life up to 9 months. A slow trend towards baseline was noted over time.89 Ultimately, this is a promising modality for CPSP management warranting further investigation.
Lastly, the use of transcranial magnetic stimulation (TMS) in the management of chronic pain is an area of emerging interest. Early studies have demonstrated that TMS may reduce acute postoperative opioid requirements following TKA.90,91 It is suspected that chronic pain may stem from maladaptive brain changes fundamental to pain perception, and thus reversal of these areas via neuromodulation may serve an important role in chronic pain reduction. Currently, there is an ongoing randomized control trial looking at theta burst TMS to improve centrally mediated osteoarthritic knee pain.92 While still requiring significantly more investigation, TMS may serve a role in chronic post-arthroplasty pain management in the future.
Conclusion
Chronic post-arthroplasty pain is an increasingly prevalent condition that is often challenging to manage and has significant negative impacts on quality of life.2 If conservative measures fail, interventional therapies serve an important role. To date, the best supported interventional approach for chronic post-TKA pain is RFA.36,37 Moreover, while traditional RFA offers superior short-term relief, CRFA provides comparable or superior long-term outcomes likely due to larger lesions.38 While the utilization of RFA or CRFA for post-THA pain remains a potential future consideration, additional research is required to demonstrate its efficacy. In the realm of neuromodulation, PRF is an important tool for post-arthroplasty pain. Both peripheral nerve and DRG PRF have established efficacy for post-TKA pain.49 The potential role of PRF for post-THA pain remains a viable option, considering the proven efficacy in management of osteoarthritic hip pain, though it requires further investigation.50 The role of PNS for post-TKA pain is well supported.52,57 The benefits of PNS for post-THA pain remain less certain, though the existing case reports do provide support.58–60 Lastly, while the early literature is supportive of SCS for CPSP, there has been a shift in recent focus to DRG stimulation.65,66,70,71 DRG stimulation for post-TKA pain has promising results in early studies.78,83 However, the use of DRG stimulation for post-THA pain remains a small subset of larger studies, thus warranting further investigation.84
Taken together, the management of post-arthroplasty pain remains an exciting area of development with many promising interventional modalities. Numerous areas for future directions exist. Randomized control trials are an important area of future research, with an emphasis on assessing both the clinical efficacy and cost effectiveness of each modality. There also tends to be a lack of research in post-hip arthroplasty patients compared to post-knee arthroplasty patients. Comparative analyses between the different interventions are also necessary to help elucidate which patient populations would benefit most from each type of intervention. In line with this, a better understanding of the underlying mechanisms is needed to help guide targeted management. Each of the above will play a critical role in the development of best practice guidelines and a more standardized approach to the management of CPSP following hip or knee arthroplasty. Currently, the choice of which modality to pursue is based upon patient-centered discussions with a focus on tailoring treatments to the presumed underlying mechanism. Moreover, practical barriers must also be considered, including cost and resource availability. For instance, although advanced neuromodulatory techniques are associated with higher initial costs than modalities such as RFA or CRFA, their long-term cost-effectiveness in the treatment of CPSP warrants further investigation.62
This review has several limitations to address. Firstly, the findings are shaped by the limited and heterogenous literature available in many of the domains discussed, affecting the generalizability of findings. Additionally, the lack of controls and retrospective nature of many of the reported studies also limits the generalizability of the findings. Lastly, as this was a narrative review, it lacks a more standardized review approach thus limiting replicability and increasing variability and the potential impact of bias. Future studies may focus on a more systematic approach to decrease these risks.
Abbreviations
US, United States; THA, total hip arthroplasty; TKA, total knee arthroplasty; CPSP, chronic post-surgical pain; RFA, radiofrequency ablation; PRF, pulsed radiofrequency; PNS, peripheral nerve stimulation; SCS, spinal cord stimulation; DRG, dorsal root ganglion; IDDS, intrathecal drug delivery systems; VAS, visual analog scale; CRFA, cooled radiofrequency ablation; NMDA, N-methyl-D-aspartate; SM, superomedial; SL, superolateral; IL, inferomedial; TENS, transcutaneous electrical nerve stimulation; CRPS, complex regional pain syndrome; TMS, transcranial magnetic stimulation.
Disclosure
RSD receives investigator-initiated grant funding paid to his institution from Nevro Corp and Saol Therapeutics; he is also a part of the speakers’ bureau for Vertex Pharmaceuticals. The remaining authors have no disclosures for this work.
References
1. Edwards RR, Campbell C, Schreiber KL, et al. Multimodal prediction of pain and functional outcomes 6 months following total knee replacement: a prospective cohort study. BMC Musculoskelet Disord. 2022;23(1):302. doi:10.1186/s12891-022-05239-3
2. Maradit Kremers H, Larson DR, Crowson CS, et al. Prevalence of total hip and knee replacement in the United States. J Bone Joint Surg Am. 2015;97(17):1386–1397. doi:10.2106/JBJS.N.01141
3. Shichman I, Roof M, Askew N, et al. Projections and epidemiology of primary hip and knee arthroplasty in medicare patients to 2040-2060. JB JS Open Access. 2023;8(1):
4. Jones CA, Beaupre LA, Johnston DWC, Suarez-Almazor ME. Total joint arthroplasties: current concepts of patient outcomes after surgery. Rheum Dis Clin North Am. 2007;33(1):71–86. doi:10.1016/j.rdc.2006.12.008
5. Erlenwein J, Müller M, Falla D, et al. Clinical relevance of persistent postoperative pain after total Hip replacement - a prospective observational cohort study. J Pain Res. 2017;10:2183–2193. doi:10.2147/JPR.S137892
6. Hasegawa M, Tone S, Naito Y, Wakabayashi H, Sudo A. Prevalence of persistent pain after total knee arthroplasty and the impact of neuropathic pain. J Knee Surg. 2019;32(10):1020–1023. doi:10.1055/s-0038-1675415
7. Luo D, Fan Z, Yin W. Chronic post-surgical pain after total knee arthroplasty: a narrative review. Perioper Med. 2024;13(1):108. doi:10.1186/s13741-024-00466-9
8. Ramo S, Frangakis S, Waljee JF, Bicket MC. Risk factors for persistent postoperative opioid use: an entity distinct from chronic postsurgical pain. Reg Anesth Pain Med. 2025;50(2):121–128. doi:10.1136/rapm-2024-105599
9. Hunter CW, Deer TR, Jones MR, et al. Consensus guidelines on interventional therapies for knee pain (STEP Guidelines) from the American society of pain and neuroscience. JPR. 2022;15:2683–2745. doi:10.2147/JPR.S370469
10. De Souza DN, Lorentz NA, Charalambous L, Galetta M, Petrilli C, Rozell JC. Comprehensive pain management in total joint arthroplasty: a review of contemporary approaches. JCM. 2024;13(22):6819. doi:10.3390/jcm13226819
11. Wei S, Li L, Yang X, Li X, Jiang Q. Psychological interventions in the pain management after Hip and knee arthroplasty: a mini review. Ann Joint. 2020;5. doi:10.21037/aoj.2019.12.06
12. Urits I, Markel M, Vij N, et al. Use of spinal cord stimulation for the treatment of post total knee arthroplasty pain. Best Pract Res Clin Anaesthesiol. 2020;34(3):633–642. doi:10.1016/j.bpa.2020.07.006
13. Schug SA, Lavand’homme P, Barke A, et al. The IASP classification of chronic pain for ICD-11: chronic postsurgical or posttraumatic pain. Pain. 2019;160(1):45–52. doi:10.1097/j.pain.0000000000001413
14. Tassou A, Richebe P, Rivat C. Mechanisms of chronic postsurgical pain. Reg Anesth Pain Med. 2025;50(2):77–85. doi:10.1136/rapm-2024-105964
15. Richebé P, Capdevila X, Rivat C. Persistent postsurgical pain: pathophysiology and preventative pharmacologic considerations. Anesthesiology. 2018;129(3):590–607. doi:10.1097/ALN.0000000000002238
16. Liu BW, Zhang J, Hong YS, et al. NGF-induced nav1.7 upregulation contributes to chronic post-surgical pain by activating SGK1-dependent nedd4-2 phosphorylation. Mol Neurobiol. 2021;58(3):964–982. doi:10.1007/s12035-020-02156-1
17. Chen Y, Hu Y, He X, et al. Activation of mitochondrial DNA-mediated cGAS-STING pathway contributes to chronic postsurgical pain by inducing type I interferons and A1 reactive astrocytes in the spinal cord. Int Immunopharmacol. 2024;127:111348. doi:10.1016/j.intimp.2023.111348
18. Murphy J, Pak S, Shteynman L, et al. Mechanisms and preventative strategies for persistent pain following knee and hip joint replacement surgery: a narrative review. Int J Mol Sci. 2024;25(9):4722. doi:10.3390/ijms25094722
19. Schreiber KL, Wilson JM, Chen YYK. Recognizing pain phenotypes: biopsychosocial sources of variability in the transition to chronic postsurgical pain. Reg Anesth Pain Med. 2025;50(2):86–92. doi:10.1136/rapm-2024-105602
20. Ghoshal A, Bhanvadia S, Singh S, Yaeger L, Haroutounian S. Factors associated with persistent postsurgical pain after total knee or Hip joint replacement: a systematic review and meta-analysis. Pain Rep. 2023;8(1):e1052. doi:10.1097/PR9.0000000000001052
21. Yoshino A, Okamoto Y, Doi M, et al. Regional brain functions in the resting state indicative of potential differences between depression and chronic pain. Sci Rep. 2017;7(1):3003. doi:10.1038/s41598-017-03522-1
22. Li J, Guan T, Zhai Y, Zhang Y. Risk factors of chronic postoperative pain after total knee arthroplasty: a systematic review. J Orthop Surg Res. 2024;19(1):320. doi:10.1186/s13018-024-04778-w
23. Zhang B, Rao S, Mekkawy KL, et al. Risk factors for pain after total Hip arthroplasty: a systematic review. Arthroplasty. 2023;5(1):19. doi:10.1186/s42836-023-00172-9
24. Konnyu KJ, Thoma LM, Cao W, et al. Rehabilitation for total knee arthroplasty: a systematic review. Am J Phys Med Rehabil. 2023;102(1):19–33. doi:10.1097/PHM.0000000000002008
25. Konnyu KJ, Pinto D, Cao W, et al. Rehabilitation for total hip arthroplasty: a systematic review. Am J Phys Med Rehabil. 2023;102(1):11–18. doi:10.1097/PHM.0000000000002007
26. Willinger ML, Heimroth J, Sodhi N, et al. Management of refractory pain after total joint replacement. Curr Pain Headache Rep. 2021;25(6):42. doi:10.1007/s11916-021-00956-1
27. Parvataneni HK, Shah VP, Howard H, Cole N, Ranawat AS, Ranawat CS. Controlling pain after total Hip and knee arthroplasty using a multimodal protocol with local periarticular injections: a prospective randomized study. J Arthroplasty. 2007;22(6 Suppl 2):33–38. doi:10.1016/j.arth.2007.03.034
28. Nicholls JL, Azam MA, Burns LC, et al. Psychological treatments for the management of postsurgical pain: a systematic review of randomized controlled trials. Patient Relat Outcome Meas. 2018;9:49–64. doi:10.2147/PROM.S121251
29. Rojas Marcos C, Schiller N, Braun S, et al. Psychosocial interventions to reduce post operative pain in total knee arthroplasty: a systematic review. HSS J. 2024:15563316241260717. doi:10.1177/15563316241260717
30. Kapural L, Nageeb F, Kapural M, Cata JP, Narouze S, Mekhail N. Cooled radiofrequency system for the treatment of chronic pain from sacroiliitis: the first case-series. Pain Pract. 2008;8(5):348–354. doi:10.1111/j.1533-2500.2008.00231.x
31. Kallas ON, Nezami N, Singer AD, et al. Cooled radiofrequency ablation for chronic joint pain secondary to hip and shoulder osteoarthritis. Radiographics. 2022;42(2):594–608. doi:10.1148/rg.210074
32. Bhatia A, Peng P, Cohen SP. Radiofrequency procedures to relieve chronic knee pain: an evidence-based narrative review. Reg Anesth Pain Med. 2016;41(4):501–510. doi:10.1097/AAP.0000000000000414
33. Hong T, Wang H, Li G, Yao P, Ding Y. Systematic review and meta-analysis of 12 randomized controlled trials evaluating the efficacy of invasive radiofrequency treatment for knee pain and function. Biomed Res Int. 2019;2019:9037510. doi:10.1155/2019/9037510
34. Lee DW, Pritzlaff S, Jung MJ, et al. Latest Evidence-Based Application for Radiofrequency Neurotomy (LEARN): best Practice Guidelines from the American Society of Pain and Neuroscience (ASPN). J Pain Res. 2021;14:2807–2831. doi:10.2147/JPR.S325665
35. Shi W, Vu TN, Annaswamy T, et al. Effectiveness comparison of genicular nerve ablation for knee osteoarthritic versus post-total knee arthroplasty pain. Interv Pain Med. 2024;3(1):100390. doi:10.1016/j.inpm.2024.100390
36. Khan FM, Tran A, Wong PKW, et al. Management of uncomplicated total knee arthroplasty chronic pain and stiffness utilizing cooled radiofrequency ablation: a single institution pilot study. Skeletal Radiol. 2022;51(6):1215–1223. doi:10.1007/s00256-021-03944-z
37. Meiling JB, Barndt BS, Ha CT, et al. The therapeutic effect of genicular nerve radiofrequency for chronic knee pain after a total knee arthroplasty: a systematic review. Interv Pain Med. 2022;1(1):100072. doi:10.1016/j.inpm.2022.100072
38. Belba A, Vanneste T, Kallewaard JW, et al. Cooled versus conventional radiofrequency treatment of the genicular nerves for chronic knee pain: 12-month and cost-effectiveness results from the multicenter COCOGEN trial. Reg Anesth Pain Med. 2025;50(1):36–45. doi:10.1136/rapm-2023-105127
39. Kim DJ, Shen S, Hanna GM. Ultrasound-guided radiofrequency lesioning of the articular branches of the femoral nerve for the treatment of chronic post-arthroplasty hip pain. Pain Physician. 2017;20(2):E323–E327.
40. Wu BP, Grits D, Foorsov V, Xu J, Tankha P, Bolash RB. Cooled and traditional thermal radiofrequency ablation of genicular nerves in patients with chronic knee pain: a comparative outcomes analysis. Reg Anesth Pain Med. doi:10.1136/rapm-2022-103693
41. Kapural L, Jolly S, Mantoan J, Badhey H, Ptacek T. Cooled radiofrequency neurotomy of the articular sensory branches of the obturator and femoral nerves - combined approach using fluoroscopy and ultrasound guidance: technical report, and observational study on safety and efficacy. Pain Physician. 2018;21(3):279–284. doi:10.36076/ppj.2018.3.279
42. Tomlinson J, Ondruschka B, Prietzel T, Zwirner J, Hammer N. A systematic review and meta-analysis of the Hip capsule innervation and its clinical implications. Sci Rep. 2021;11(1):5299. doi:10.1038/s41598-021-84345-z
43. Locher S, Burmeister H, Böhlen T, et al. Radiological anatomy of the obturator nerve and its articular branches: basis to develop a method of radiofrequency denervation for Hip joint pain. Pain Med. 2008;9(3):291–298. doi:10.1111/j.1526-4637.2007.00353.x
44. Rivera F, Mariconda C, Annaratone G. Percutaneous radiofrequency denervation in patients with contraindications for total Hip arthroplasty. Orthopedics. 2012;35(3):e302–305. doi:10.3928/01477447-20120222-19
45. Cheney CW, Ahmadian A, Brennick C, et al. Radiofrequency ablation for chronic hip pain: a comprehensive, narrative review. Pain Med. 2021;22(Suppl 1):S14–S19. doi:10.1093/pm/pnab043
46. Chua NHL, Vissers KC, Sluijter ME. Pulsed radiofrequency treatment in interventional pain management: mechanisms and potential indications-a review. Acta Neurochir. 2011;153(4):763–771. doi:10.1007/s00701-010-0881-5
47. Vas L, Khandagale N, Pai R. Successful management of chronic postsurgical pain following total knee replacement. Pain Med. 2014;15(10):1781–1785. doi:10.1111/pme.12508
48. Albayrak I, Apiliogullari S, Dal CN, Levendoglu F, Ozerbil OM. Efficacy of pulsed radiofrequency therapy to dorsal root ganglion adding to TENS and exercise for persistent pain after total knee arthroplasty. J Knee Surg. 2017;30(2):134–142. doi:10.1055/s-0036-1583268
49. Chen Y, TNH V, Chinchilli VM, et al. Clinical and technical factors associated with knee radiofrequency ablation outcomes: a multicenter analysis. Reg Anesth Pain Med. 2021;46(4):298–304. doi:10.1136/rapm-2020-102017
50. Tinnirello A, Todeschini M, Pezzola D, Barbieri S. Pulsed radiofrequency application on femoral and obturator nerves for hip joint pain: retrospective analysis with 12-month follow-up results. Pain Physician. 2018;21(4):407–414.
51. Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965;150(3699):971–979. doi:10.1126/science.150.3699.971
52. Ilfeld BM, Grant SA, Gilmore CA, et al. Neurostimulation for postsurgical analgesia: a novel system enabling ultrasound-guided percutaneous peripheral nerve stimulation. Pain Pract. 2017;17(7):892–901. doi:10.1111/papr.12539
53. McRoberts WP, Roche M. Novel approach for peripheral subcutaneous field stimulation for the treatment of severe, chronic knee joint pain after total knee arthroplasty. Neuromodulation. 2010;13(2):131–136. doi:10.1111/j.1525-1403.2009.00255.x
54. Chitneni A, Berger AA, Orhurhu V, Kaye AD, Hasoon J. Peripheral nerve stimulation of the saphenous and superior lateral genicular nerves for chronic pain after knee surgery. Orthop Rev. 2021;13(2):24435. doi:10.52965/001c.24435
55. Chauhan G, Srinivasan SK, Khanduja S. Wireless high-frequency peripheral nerve stimulation for chronic refractory knee pain post-total knee replacement. Cureus. 2023;15(3):e35759. doi:10.7759/cureus.35759
56. Kelly TD, Pazzol ML, Rahimi Darabad R. Peripheral nerve stimulation in chronic knee pain: a case series. Cureus. 2023;15(12):e50127. doi:10.7759/cureus.50127
57. Goree JH, Grant SA, Dickerson DM, et al. Randomized placebo-controlled trial of 60-day percutaneous peripheral nerve stimulation treatment indicates relief of persistent postoperative pain, and improved function after knee replacement. Neuromodulation. 2024;27(5):847–861. doi:10.1016/j.neurom.2024.03.001
58. Yakovlev AE, Resch BE, Karasev SA. Treatment of intractable Hip pain after THA and GTB using peripheral nerve field stimulation: a case series. WMJ. 2010;109(3):149–152.
59. Pierson CJ, Velez N, Jain NB, Konda C. Changing stimulation frequency improves implanted peripheral nerve stimulator effects after posttraumatic total hip arthroplasty: a case report. Am J Phys Med Rehabil. 2024;103(6):e67–e70. doi:10.1097/PHM.0000000000002411
60. Joseph C, Parkash A, Chitneni A, Kalava AID. Femoral peripheral nerve stimulator for chronic hip pain with total hip arthroplasty: a case report. Neuromodulation. 2023;26(4):S240. doi:10.1016/j.neurom.2023.04.432
61. Taylor RS. Spinal cord stimulation in complex regional pain syndrome and refractory neuropathic back and leg pain/failed back surgery syndrome: results of a systematic review and meta-analysis. J Pain Symptom Manage. 2006;31(4 Suppl):S13–19. doi:10.1016/j.jpainsymman.2005.12.010
62. Mekhail N, Deer TR, Poree L, et al. Cost-effectiveness of dorsal root ganglion stimulation or spinal cord stimulation for complex regional pain syndrome. Neuromodulation. 2021;24(4):708–718. doi:10.1111/ner.13134
63. Deer TR, Levy RM, Kramer J, et al. Comparison of paresthesia coverage of patient’s pain: dorsal root ganglion vs. spinal cord stimulation. An ACCURATE study sub-analysis. Neuromodulation. 2019;22(8):930–936. doi:10.1111/ner.12920
64. Karcz M, Abd-Elsayed A, Chakravarthy K, et al. Pathophysiology of pain and mechanisms of neuromodulation: a narrative review (a neuron project). J Pain Res. 2024;17:3757–3790. doi:10.2147/JPR.S475351
65. Lowry AM, Simopoulos TT. Spinal cord stimulation for the treatment of chronic knee pain following total knee replacement. Pain Physician. 2010;13(3):251–256.
66. Gillis J, Southerland WA, Kaye AD, Eskander JP, Pham AD, Simopoulos T. Spinal cord stimulation for post total knee replacement pain: a case series. Orthop Rev. 2022;14(3):33835. doi:10.52965/001c.33835
67. Urits I, Osman M, Orhurhu V, et al. A case study of combined perception-based and perception-free spinal cord stimulator therapy for the management of persistent pain after a total knee arthroplasty. Pain Ther. 2019;8(2):281–284. doi:10.1007/s40122-019-00136-5
68. Reeves C, Benito T. Persistent post-surgical knee pain treated with stimulation at L3-L4 level accessed via the s1 foramen. In. 2016.
69. Patel E, Nicholson B. Successful spinal cord stimulation in chronic knee pain: do we have it all wrong? In. 2019.
70. Zanotti G, Slullitel PA, Comba FM, Buttaro MA, Piccaluga F. Three cases of type-1 complex regional pain syndrome after elective total Hip replacement. SICOT J. 2017;3:52. doi:10.1051/sicotj/2017038
71. Adam MF, Khalifa AA, Abdelaal AM. Complex regional pain syndrome after multiple revision total Hip arthroplasty surgeries. Bull Natl Res Cent. 2023;47(1):21. doi:10.1186/s42269-023-00994-2
72. Mattie R, Lin AB, Bhandal H, et al. Spinal cord stimulation for the treatment of complex regional pain syndrome: a systematic review of randomized controlled trials. Interv Pain Med. 2024;3(4):100527. doi:10.1016/j.inpm.2024.100527
73. Stanton-Hicks M. Complex regional pain syndrome: manifestations and the role of neurostimulation in its management. J Pain Symptom Manage. 2006;31(4 Suppl):S20–24. doi:10.1016/j.jpainsymman.2005.12.011
74. Rigoard P, Roulaud M, Goudman L, et al. Comparison of spinal cord stimulation vs. dorsal root ganglion stimulation vs. association of both in patients with refractory chronic back and/or lower limb neuropathic pain: an international, prospective, randomized, double-blinded, crossover trial (BOOST-DRG Study). Medicina. 2021;58(1):7. doi:10.3390/medicina58010007
75. Deer TR, Levy RM, Kramer J, et al. Dorsal root ganglion stimulation yielded higher treatment success rate for complex regional pain syndrome and causalgia at 3 and 12 months: a randomized comparative trial. Pain. 2017;158(4):669–681. doi:10.1097/j.pain.0000000000000814
76. Deer TR, Hunter CW, Mehta P, et al. A systematic literature review of dorsal root ganglion neurostimulation for the treatment of pain. Pain Med. 2020;21(8):1581–1589. doi:10.1093/pm/pnaa005
77. Abd-Elsayed A, Vardhan S, Aggarwal A, Vardhan M, Diwan SA. Mechanisms of action of dorsal root ganglion stimulation. Int J Mol Sci. 2024;25(7):3591. doi:10.3390/ijms25073591
78. Schultheis BC, Ross-Steinhagen N, Jerosch J, Breil-Wirth A, Weidle PA. The impact of dorsal root ganglion stimulation on pain levels and functionality in patients with chronic postsurgical knee pain. Neuromodulation. 2024;27(1):151–159. doi:10.1016/j.neurom.2022.10.057
79. Gravius N, Chaudhry SR, Muhammad S, et al. Selective L4 dorsal root ganglion stimulation evokes pain relief and changes of inflammatory markers: part i profiling of saliva and serum molecular patterns. Neuromodulation. 2019;22(1):44–52. doi:10.1111/ner.12866
80. Kinfe TM, Asif M, Chakravarthy KV, et al. Unilateral L4-dorsal root ganglion stimulation evokes pain relief in chronic neuropathic postsurgical knee pain and changes of inflammatory markers: part II whole transcriptome profiling. J Transl Med. 2019;17(1):205. doi:10.1186/s12967-019-1952-x
81. Kretzschmar M, Reining M, Schwarz MA. Three-year outcomes after dorsal root ganglion stimulation in the treatment of neuropathic pain after peripheral nerve injury of upper and lower extremities. Neuromodulation. 2021;24(4):700–707. doi:10.1111/ner.13222
82. Martin SC, Macey AR, Raghu A, et al. Dorsal root ganglion stimulation for the treatment of chronic neuropathic knee pain. World Neurosurg. 2020;143:e303–e308. doi:10.1016/j.wneu.2020.07.102
83. Morgalla MH, Fortunato M, Lepski G, Chander BS. Dorsal root ganglion stimulation (drgs) for the treatment of chronic neuropathic pain: a single-center study with long-term prospective results in 62 cases. Pain Physician. 2018;21(4):E377–E387. doi:10.36076/ppj.2018.4.E377
84. Hunter CW, Sayed D, Lubenow T, et al. DRG FOCUS: a multicenter study evaluating dorsal root ganglion stimulation and predictors for trial success. Neuromodulation. 2019;22(1):61–79. doi:10.1111/ner.12796
85. Dahm PO, Nitescu PV, Appelgren LK, Curelaru ID. Six years of continuous intrathecal infusion of opioid and bupivacaine in the treatment of refractory pain due to intrapelvic extrusion of bone cement after total Hip arthroplasty. Reg Anesth Pain Med. 1998;23(3):315–319. doi:10.1016/s1098-7339(98)90061-x
86. Roux C. Efficacy of microparticle geniculate artery embolization in total knee prosthesis patients with pain resistant to medical treatment. a prospective randomized controlled trial (EPROGE). Available from: https://clinicaltrials.gov/study/NCT06466330?cond=chronic%20pain%20total%20hip%20arthroplasty&page=2&rank=14#more-information.
87. Radnovich R, Scott D, Patel AT, et al. Cryoneurolysis to treat the pain and symptoms of knee osteoarthritis: a multicenter, randomized, double-blind, sham-controlled trial. Osteoarthritis Cartilage. 2017;25(8):1247–1256. doi:10.1016/j.joca.2017.03.006
88. Dasa V, Lensing G, Parsons M, Harris J, Volaufova J, Bliss R. Percutaneous freezing of sensory nerves prior to total knee arthroplasty. Knee. 2016;23(3):523–528. doi:10.1016/j.knee.2016.01.011
89. Bianco GL, D’angelo FP, Dos Santos GF, et al. Genicular nerve ultrasound-guided cryoanalgesia for the treatment of chronic knee joint pain: an observational retrospective study. Pain Ther. 2025;14(3):985–998. doi:10.1007/s40122-025-00727-5
90. Borckardt JJ, Reeves ST, Robinson SM, et al. Transcranial direct current stimulation (tDCS) reduces postsurgical opioid consumption in total knee arthroplasty (TKA). Clin J Pain. 2013;29(11):925–928. doi:10.1097/AJP.0b013e31827e32be
91. Khedr EM, Sharkawy ESA, Attia AMA, Ibrahim Osman NM, Sayed ZM. Role of transcranial direct current stimulation on reduction of postsurgical opioid consumption and pain in total knee arthroplasty: double randomized clinical trial. Eur J Pain. 2017;21(8):1355–1365. doi:10.1002/ejp.1034
92. Drabek M, Hodkinson D, Horvath S, et al. B rain connectivity-guided, optimised theta burst transcranial magnetic stimulation to improve central pain modulation in knee osteoarthritis pain (BoostCPM): protocol of a pilot randomised clinical trial in a secondary care setting in the UK. BMJ Open. 2023;13(10):e073378. doi:10.1136/bmjopen-2023-073378
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Radiofrequency Ablation for Chronic Lumbar Zygapophyseal Joint Pain Using a V-Shaped Active Tip Needle: An Observational Retrospective Study
Lo Bianco G, Misseri G, Stogicza AR, Cesare G, Li S, Day M, Kennedy DJ, Schatman ME
Journal of Pain Research 2023, 16:1243-1255
Published Date: 11 April 2023
Pain and Transcranial Direct Current Stimulation: A Bibliometric Analysis
Chiriac VF, Leucuța DC, Moșoiu DV
Journal of Pain Research 2023, 16:3655-3671
Published Date: 1 November 2023
Spinal Cord Stimulation for Intractable Visceral Pain Originating from the Pelvic and Abdominal Region: A Narrative Review on a Possible New Indication for Patients with Therapy-Resistant Pain
Bieze M, van Haaps AP, Kapural L, Li S, Ferguson K, de Vries R, Schatman ME, Mijatovic V, Kallewaard JW
Journal of Pain Research 2024, 17:691-736
Published Date: 19 February 2024
Transforming Chronic Pain Management: Integrating Neuromodulation with Advanced Technologies to Tackle Cognitive Dysfunction – A Narrative Review
Green M, Hayley A, Gunnersen JM, Nazemian V, Cabble A, Thompson S, Chakravarthy K
Journal of Pain Research 2025, 18:2497-2507
Published Date: 16 May 2025