Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Chronic Obstructive Pulmonary Disease in Singapore: Current Perspectives on Prevalence, Disease Burden, and Treatment
Authors Yii A ![]() , Maldonado Sanchez Y, Lai Q, Chen W
, Maldonado Sanchez Y, Lai Q, Chen W ![]()
Received 12 December 2025
Accepted for publication 23 May 2026
Published 18 June 2026 Volume 2026:21 588581
DOI https://doi.org/10.2147/COPD.S588581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Anthony Yii,1 Yerson Maldonado Sanchez,2 Qiuwen Lai,2 Wenjia Chen3
1Department of Respiratory and Critical Care Medicine, Changi General Hospital, Singapore; 2Immunology Medical Department, Sanofi, South Beach Tower, Singapore, Singapore; 3Saw Swee Hock School of Public Health, National University of Singapore, Singapore
Correspondence: Anthony Yii, Department of Respiratory and Critical Care Medicine, Changi General Hospital, 2 Simei St 3, 529889, Singapore, Email [email protected]
Abstract: Chronic obstructive pulmonary disease (COPD) represents a significant global health challenge, affecting millions worldwide, with an estimated prevalence of 5.9% specifically for Singapore, and a projected increase driven by population aging. Despite comprehensive healthcare infrastructure, COPD remains underdiagnosed and undertreated in Singapore. Real-world evidence indicates that most patients present with moderate-to-severe disease and exhibit high rates of comorbidities, including cardiovascular disorders, diabetes, and bronchiectasis, which complicate COPD management and increase healthcare utilization. Smoking remains the predominant risk factor, although non-smoking phenotypes linked to prior tuberculosis, biomass exposure, and environmental allergens are increasingly recognized. COPD imposes a significant economic burden, primarily driven by hospitalizations, and disproportionately affects certain ethnic groups, underscoring the need for culturally tailored interventions. Current treatment strategies for moderate-to-severe COPD emphasize smoking cessation, pulmonary rehabilitation, and inhaled bronchodilator therapy; however, substantial gaps persist, with frequent exacerbations despite triple therapy (long-acting β 2-agonists and long-acting muscarinic antagonists along with inhaled corticosteroids) and inappropriate oral corticosteroid use contributing to adverse outcomes. Recent advances in biologic therapies targeting type 2 inflammation, notably dupilumab, approved in Singapore in 2025 offer promising options for patients with uncontrolled COPD characterized by elevated blood eosinophils. Emerging biomarkers, such as fractional exhaled nitric oxide, may further refine patient selection for precision therapy. This review focuses on the current evidence on COPD epidemiology, clinical characteristics, risk factors, treatment patterns, and evolving therapeutic approaches in Singapore, highlighting opportunities to optimize patient care through early diagnosis and adoption of novel biologics to improve outcomes in this heterogeneous population.
Keywords: COPD, real-world evidence, COPD management strategies, dupilumab, mepolizumab
Introduction
Chronic obstructive pulmonary disease (COPD) is a complex, heterogeneous lung condition characterized by persistent and progressive airflow obstruction and chronic respiratory symptoms, resulting from abnormalities in both airways and alveoli.1,2 COPD is a common respiratory condition in the Asia-Pacific region, including Singapore.3 However, the actual burden of the disease is likely underestimated due to underdiagnosis and undertreatment across many Asian countries.3,4 This is largely attributed to insufficient disease awareness, limited access to diagnostic tools, and underutilization of pulmonary function tests.3,4 The Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2026 emphasizes the importance of early detection and appropriate assessment of the severity of COPD based on symptoms and lung function status.1,5
Additionally, the misuse of inhalers and overreliance on oral corticosteroids (OCSs) are major therapeutic challenges. Such prescribing patterns are often driven by cost constraints, limited availability, and entrenched clinical practices. Environmental factors further complicate COPD management in Asia.4 Furthermore, the clinical profile of COPD in Asia is influenced by unique regional factors, such as a higher prevalence of bronchiectasis, tuberculosis-related lung damage, biomass smoke exposure, atopy, environmental fungal sensitization, and parasitic infections.4,6,7 These characteristics necessitate management strategies tailored to the specific needs of Asian populations. The healthcare landscape of Singapore offers a unique opportunity to improve COPD management. This multiethnic nation, operating with a universal healthcare system, serves as a representative model for the Asian region.8 However, challenges in timely and accurate diagnosis persist and must be addressed to ensure appropriate and effective COPD management.
Current COPD management strategies combine essential non-pharmacological approaches (smoking cessation, pulmonary rehabilitation, and comorbidity management) with pharmacological interventions. Despite administration of a triple fixed dose of inhaled long-acting bronchodilators (long-acting β2-agonists [LABAs] and long-acting muscarinic antagonists [LAMAs]) along with inhaled corticosteroids (ICSs), many patients remain symptomatic and continue to face exacerbations.1,9,10 OCSs are commonly used to treat COPD exacerbations; however, one in four patients was dispensed unsafe cumulative doses (≥1000 mg prednisolone-equivalent) within just 12 months, raising concerns about long-term adverse effects.11 This persistent burden led to the investigation of biologic therapies targeting inflammatory pathways in COPD. Advances in the understanding of type 2 inflammation and epithelial alarmins have facilitated the clinical evaluation of monoclonal antibodies against tumor necrosis factor alpha and various interleukins (ILs), representing a promising therapeutic strategy under active investigation. Despite limited progress in COPD pharmacotherapy, dupilumab (anti-IL-4Rα) and mepolizumab (IL-5 antagonist) improve key outcomes in eosinophilic COPD, whereas other agents, such as tezepelumab, have shown minimal clinical benefit.12,13
In Singapore, although COPD management has traditionally relied on bronchodilators and ICS, the treatment landscape is evolving. Dupilumab and mepolizumab are approved by the US Food and Drug Administration (US FDA) as an add-on maintenance treatment for adult patients with inadequately controlled COPD and an eosinophilic phenotype.14,15 However, only dupilumab is available in Singapore as an add-on maintenance treatment for patients with uncontrolled COPD characterized by type 2 high inflammation, who are administered a stable combination of ICS, LABA, and LAMA, or LABA and LAMA if ICS is inappropriate.16 Ongoing clinical trials are investigating other biologics, such as benralizumab, itepekimab, tozorakimab, astegolimab, and tezepelumab, which target type 2 inflammation and alarmin pathways.17
This landscape review discusses the available evidence on COPD in Singapore, examining its epidemiology, clinical characteristics, disease progression patterns, treatment approaches, and outcomes. Focusing on the Singaporean context, we aim to provide healthcare professionals with relevant insights to optimize COPD management strategies and identify critical areas for future research and healthcare policy development for this high-burden disease.
Methods
We conducted a literature search to synthesize evidence on the epidemiology, risk factors, clinical characteristics, management, and healthcare burden of COPD in Singapore. A narrative approach was chosen to integrate the limited number of epidemiological and population-based studies from Singapore and the heterogeneous data sources. Literature search was based on keywords related to both COPD (“chronic obstructive pulmonary disease”, “COPD”, “chronic bronchitis”, “emphysema”) and geography (“Singapore”) and included all publications up to June 2025. Titles and abstracts were screened for relevance, followed by screening of full text. Articles related to the scope of the review were included in the narrative review and comprised of observational studies, clinical trials, registry analyses, population-based studies, real world evidence and health services of economic evaluations. Case reports were excluded. We further included literature from Singapore health agencies and additional relevant studies based on authors’ knowledge of published evidence.
Findings were synthesized qualitatively and organized into predefined domains: (1) prevalence, (2) demographic and clinical characteristics such as age, gender and ethnicity, (3) smoking patterns, (4) severity, (5) comorbidities, (6) disease burden, quality of life and economic costs, (7) hospitalization and morbidity burden, (8) evolution of COPD management in Singapore summarized based on real-world evidence, current treatment landscape and implementation of guidelines, (9) emerging therapeutic approaches and future directions, and (10) treatment adherence in patients with COPD from Singapore. Where relevant, Singapore data were contextualized against global literature.
Prevalence
In 2020, the estimated global prevalence of COPD was 10.6%, equating to 480 million affected people, with a projected increase to 592 million people by 2050.18 Considering the aging populations and neglect of key risk factors, patients are likely to face an increasing health burden. The rising prevalence of COPD will intensify the impact of the disease through significant healthcare costs for both patients and healthcare systems, resulting in a growing global economic burden.1,19 In 2015, the overall estimated prevalence of COPD was 6.2% in the Asia-Pacific region and 5.9% specifically for Singapore.3 However, these figures may underestimate the actual burden of the disease as COPD remains considerably underdiagnosed and undertreated across many Asian countries. COPD is the fourth leading cause of death worldwide, resulting in 3.5 million deaths in 2021, ie, approximately 5% of all global deaths. COPD is the eighth leading cause of poor health worldwide as measured by disability-adjusted life years.20
In 2023, COPD was the 10th leading cause of death in Singapore.21 The burden of COPD in Singapore is expected to increase over time. By 2030, it is projected that one in four Singaporeans will be aged ≥65 years, potentially leading to a higher COPD prevalence.22 The Regional COPD Working Group reported that COPD affects approximately 3.5% of Singaporeans aged ≥30 years. However, this figure likely underestimates the actual prevalence because of underdiagnosis, particularly in early stages of the disease.23,24
Overview of Clinical Studies
Epidemiological and population-based studies on COPD in Singapore are limited, posing a significant challenge to the accurate assessment of disease burden within the local population. To bridge this knowledge gap, we reviewed the limited number of available observational and real-world studies involving Singaporean patients with COPD. Although these studies primarily focused on treatment outcomes rather than epidemiological trends, they offer valuable insights into the demographic and clinical characteristics of Singaporean patients with COPD. Table 1 summarizes key research conducted on COPD in Singapore, highlighting study designs, patient populations, and primary research objectives.3,25–30
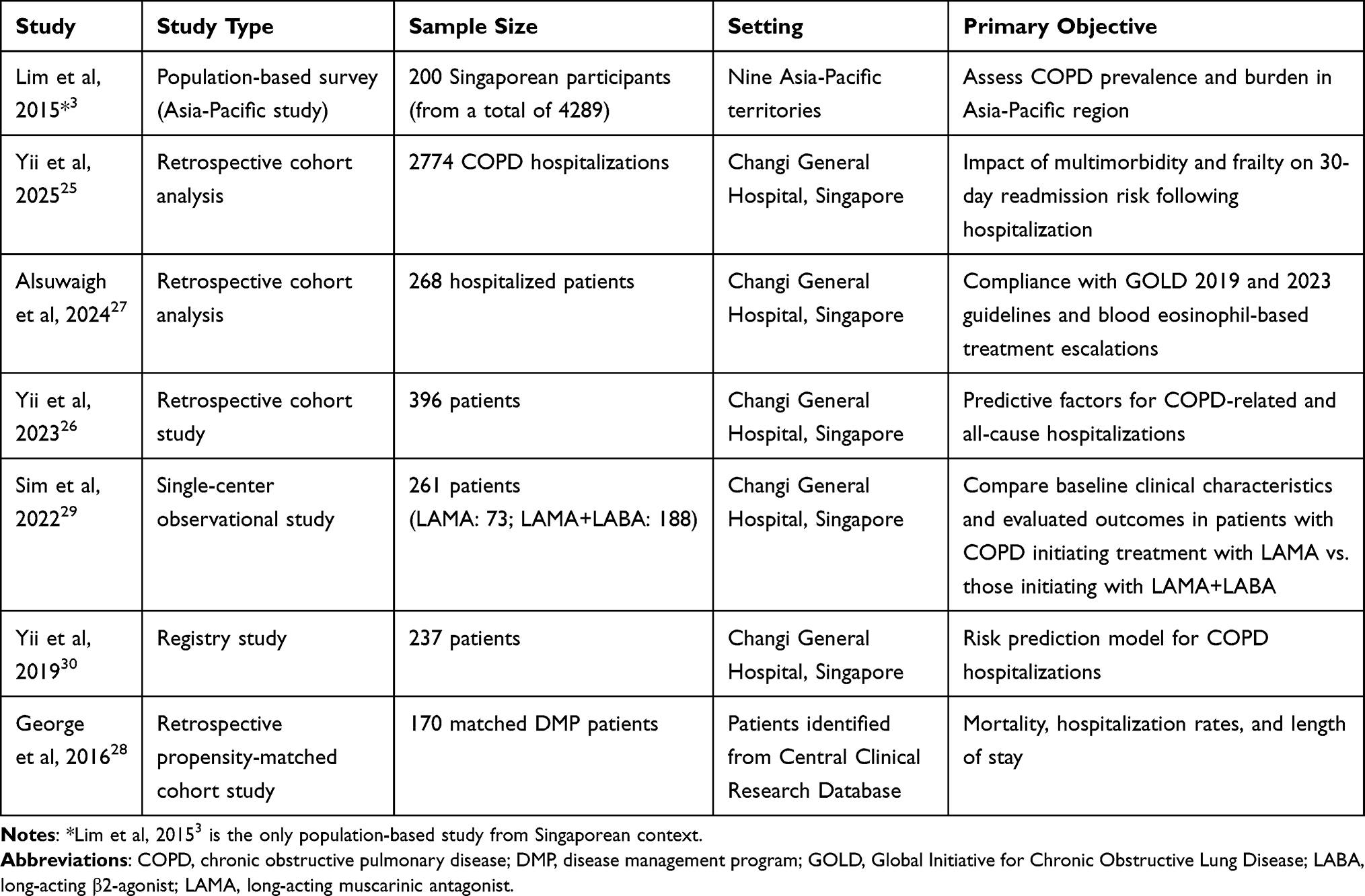 |
Table 1 Summary of Key Studies on COPD in Singapore |
Demographic and Clinical Characteristics
Age, Gender, and Ethnicity
Recent studies demonstrated a distinctive age distribution pattern among patients with COPD, with a mean age of >72 years, reflecting the predominantly elderly patient population.27,29,30 However, the disease burden significantly affects the working-age population, with Lim et al reporting that approximately only 34% of patients with COPD were aged >65 years.3 A more detailed age stratification by George et al revealed increasing COPD prevalence with age, with 20.9% of patients affected in the 55–64 years age group, 29.6% in the 65–74 years age group, and 34.8% aged ≥75 years (Table 2).31 The substantial proportion of working-age patients with COPD suggests significant economic implications through productivity loss.
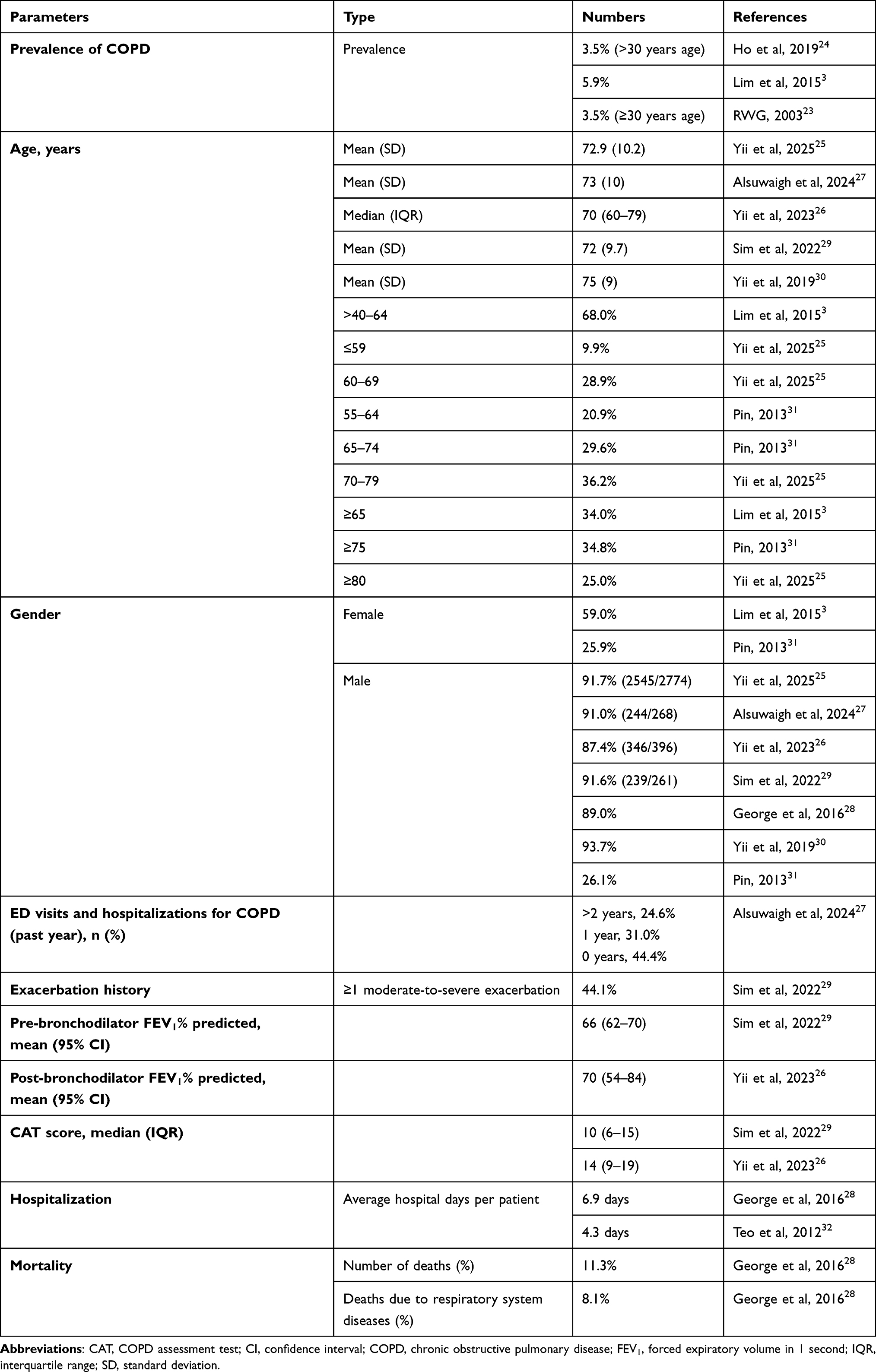 |
Table 2 Prevalence of COPD and Characteristics of Patients with COPD |
A comprehensive meta-analysis of 194 studies revealed a global COPD prevalence of 9.23% in male patients and 6.16% in female patients, with a narrower gender gap in developed countries, wherein the prevalence in female patients almost matched that in male patients. COPD burden was particularly high in the Asian region, with the South-east Asian region showing the highest prevalence of 11.34% in male patients and 5.02% in female patients. However, there is a concerning lack of high-quality epidemiological data from this region;33 therefore, current evidence from Singapore remained controversial.
Several cohort studies have consistently demonstrated a pronounced predominance among male patients with COPD. Sim et al reported that 91.6% of patients were male, while Alsuwaigh et al and George et al observed similar trends, with 91% and 89% male representation, respectively.27–29 Yii et al provided additional evidence of predominance in male patients, reporting rates of 87.4% and 91.7% male representation in 2023 and 2025, respectively.25,26 However, Lim et al observed a more balanced distribution, with 59% of patients being female.3 Moreover, the COPD Gene study revealed notable gender-related and age-related differences in COPD presentation and outcomes. Female patients demonstrated a concerning pattern of increased vulnerability, with a higher prevalence of early onset COPD (66% female predominance in patients aged <55 years), more severe dyspnea and airflow limitation, and 1.53 fold higher odds of exacerbations compared to male patients.34 Further evidence is required to understand potential factors leading to gender imbalance in COPD prevalence.
The ethnic composition of patients with COPD in Singapore, as demonstrated in five recent studies,25–29 reflects multicultural demographics while highlighting important considerations for clinical practice. The ethnic distribution across these five studies showed a consistent pattern, with Chinese participants comprising the majority in all investigations. The proportion of Chinese participants ranged from 52.9% to 76.4%. Malay participants constituted the second-largest ethnic group across all studies, with proportions ranging from 13.3% to 28.4%.27,28 Indian participants represented a smaller proportion, ranging from 6.0% to 9.7% across these single-center studies.25–29 The detailed ethnic distribution data are illustrated in Figure 1. The consistent representation of multiple ethnic groups across these studies emphasizes the need for culturally sensitive healthcare delivery in the COPD management framework of Singapore. The demographic findings from observational studies in clinical cohorts align closely with the results from the Singapore’s national health administrative databases.35 Two cohorts were created retrospectively from this database for asthma and COPD patients followed from their index date to the earliest occurring event: death, loss to follow-up or the study end date of December 31, 2019. In the COPD cohort, patients had a mean age of 68.7 (SD 11.2) years, and were predominantly male population (82.9%) with 80.4% of the patients being of Chinese ethnicity followed by Malay (10.2%), Indian (5.4%) and others (4.0%).35 This ethnic distribution is consistent with the racial composition of the Singapore resident population as reported in the 2020 consensus of Singapore population.36
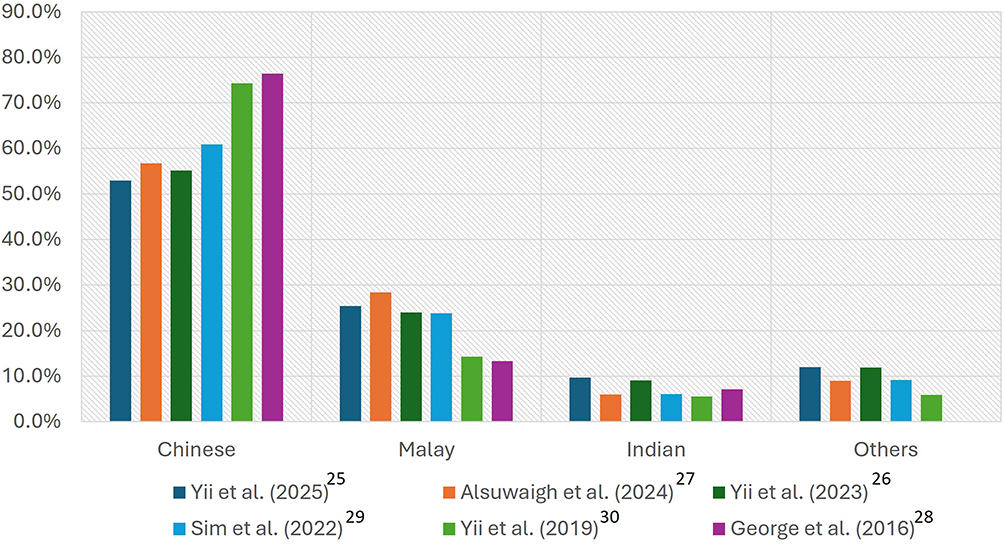 |
Figure 1 Ethnic distribution of patients with COPD in Singapore. Abbreviation: COPD, chronic obstructive pulmonary disease. |
While we see differences in ethnic distribution of COPD, it is important to note that factors like particulate matter pollution, smoking, and occupational exposure to pollutants with varying contribution across regions, were the main risk factors for COPD in Asia37 which might play a role in the disease prevalence or severity together with the socioeconomic status.1
Smoking Patterns
Recent studies on smoking patterns among patients with COPD in Singapore showed high rates of continued tobacco use despite a COPD diagnosis. The studies reveal current smoking rates ranging from 40.9% to 50.4%.27,29 Despite the well-established causal relationship between smoking and COPD, a significant proportion of patients use tobacco following diagnosis. Ministry of Health reports that, Singapore exhibits a comparatively lower national smoking prevalence than that of other Asian countries, with rates declining from 13.9% in 2010 to 10.1% in 2020. This is attributed to the comprehensive tobacco control measures implemented by the Ministry of Health, Singapore.38 This trend emphasizes the effectiveness of public health interventions at the population level, although individual-level cessation remains a challenge in COPD cohorts. The current GOLD guidelines emphasize smoking cessation as a crucial intervention in COPD management, as cessation at any disease stage can reduce progression, alleviate daily symptoms, and decrease exacerbation risk.1
COPD affects 3–10% of non-smokers, emphasizing the importance of non-smoking risk factors. These include biomass fuel use, occupational exposures, past pulmonary tuberculosis, chronic asthma, childhood respiratory infections, air pollution, and low socioeconomic status. The Singapore Longitudinal Ageing Studies confirm similar prevalence and risk patterns in non-smokers.39 Recent evidence from the 2020 National Health Interview Survey shows that female participants who never smoked had almost twice the COPD prevalence of non-smoking male participants (3.2% vs. 1.7%), with female participants having a 62% higher risk of COPD among non-smokers. This gender disparity persisted across all age groups, suggesting that factors beyond smoking contribute significantly to the COPD risk in female patients.40
These outcomes highlight two critical priorities for COPD management strategies in Singapore: strengthening smoking cessation support programs for the large population of current smokers and investigating non-smoking COPD phenotypes that may require alternative preventive, diagnostic, and therapeutic approaches. The urban environment of Singapore contributes additional risk factors including occupational exposure and ambient air pollution.41,42
Severity
The GOLD guidelines have recently introduced the ABE classification system for COPD, which simplifies the disease categories as follows: A (mild), B (moderate), and E (exacerbator). This system focuses on the symptom burden and exacerbation history to guide treatment decisions (Table 3).1
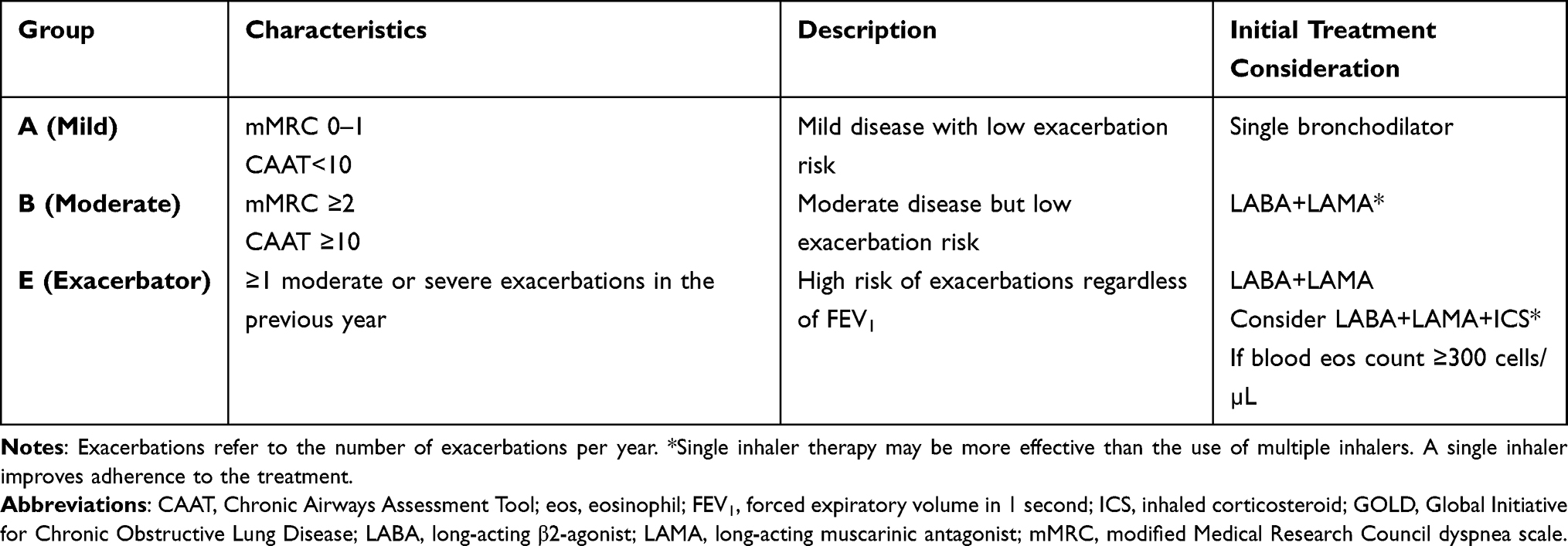 |
Table 3 ABE Classification for the Initial Treatment Consideration as per the GOLD 2026 Guidelines1 |
The severity distribution of COPD in Singapore, as classified by the GOLD staging criteria, demonstrates a remarkable consistency across multiple observational studies.3,25–27,29 Figure 2 illustrates moderate disease (GOLD Stage II) as the predominant presentation, accounting for 28.7–49.3% of patients across all studies. Mild disease (GOLD Stage I) represents approximately 21.7–29.0% of cases, whereas severe disease (GOLD Stage III) exhibits some variation between studies (13.5–23.3%). Very severe COPD (GOLD Stage IV) consistently comprises the smallest proportion of patients (0.8–4.0%).3,25–27,29 The substantial proportion of patients with moderate-to-severe disease suggests opportunities for targeted interventions to prevent progression to more severe stages of disease. Meanwhile, the relatively small but substantial population with very severe disease likely requires intensive healthcare resources and specialized management approaches, such as pulmonary rehabilitation or long-term oxygen therapy. Dupilumab or mepolizumab (not yet approved in Singapore at the time of writing) may be considered as a treatment option for patients with COPD with blood EOS ≥300 cells/µL who continue experiencing frequent exacerbations despite triple therapy.1 Dupilumab has demonstrated efficacy in reducing exacerbation rates, which is crucial since exacerbations are associated with lung function decline and increased mortality risk.15,16
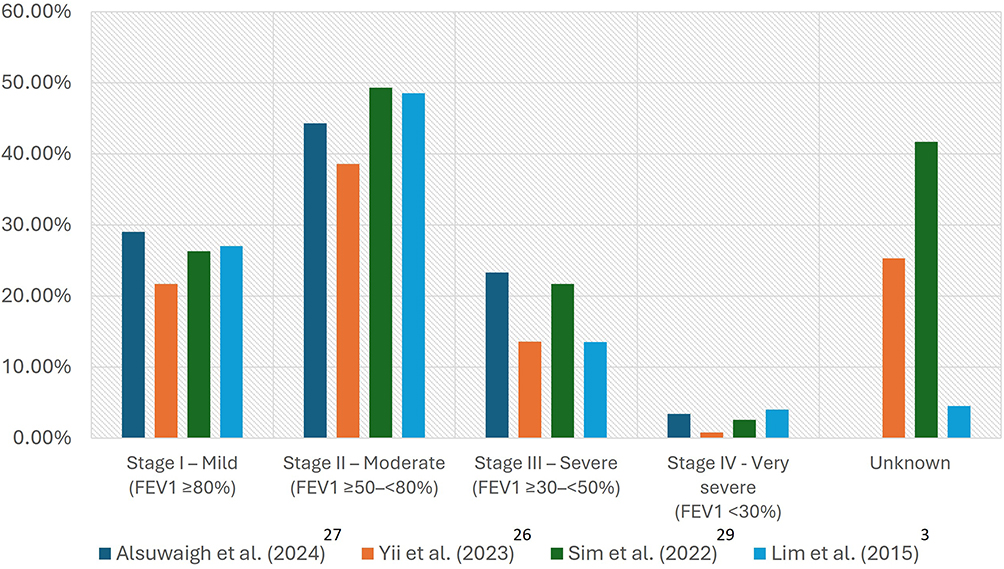 |
Figure 2 GOLD stages of severity in Singapore. Abbreviations: FEV1, forced expiratory volume in 1 second; GOLD, Global Initiative for Chronic Obstructive Lung Disease. |
The consistency of these findings across different periods and patient cohorts strengthens their reliability and highlights the need for a comprehensive COPD management strategy that addresses the full spectrum of disease severity, with particular emphasis on early intervention for the large population with moderate-to-severe disease.
Comorbidities
Comorbidities play a crucial role in the clinical presentation, management, and outcomes of patients with COPD in Singapore. As illustrated in Table 4, several studies have documented the prevalence of various comorbid conditions among patients with COPD, revealing a complex landscape of multimorbidity.3,26–30 Patients with COPD have comorbidities, such as cardiovascular disease, diabetes, hypertension, osteoporosis, lung cancer, and mental health issues, either directly linked with inflammation underlying COPD, associated with treatment (eg, osteoporosis from steroid use), or linked to shared risk factors such as smoking.43,44
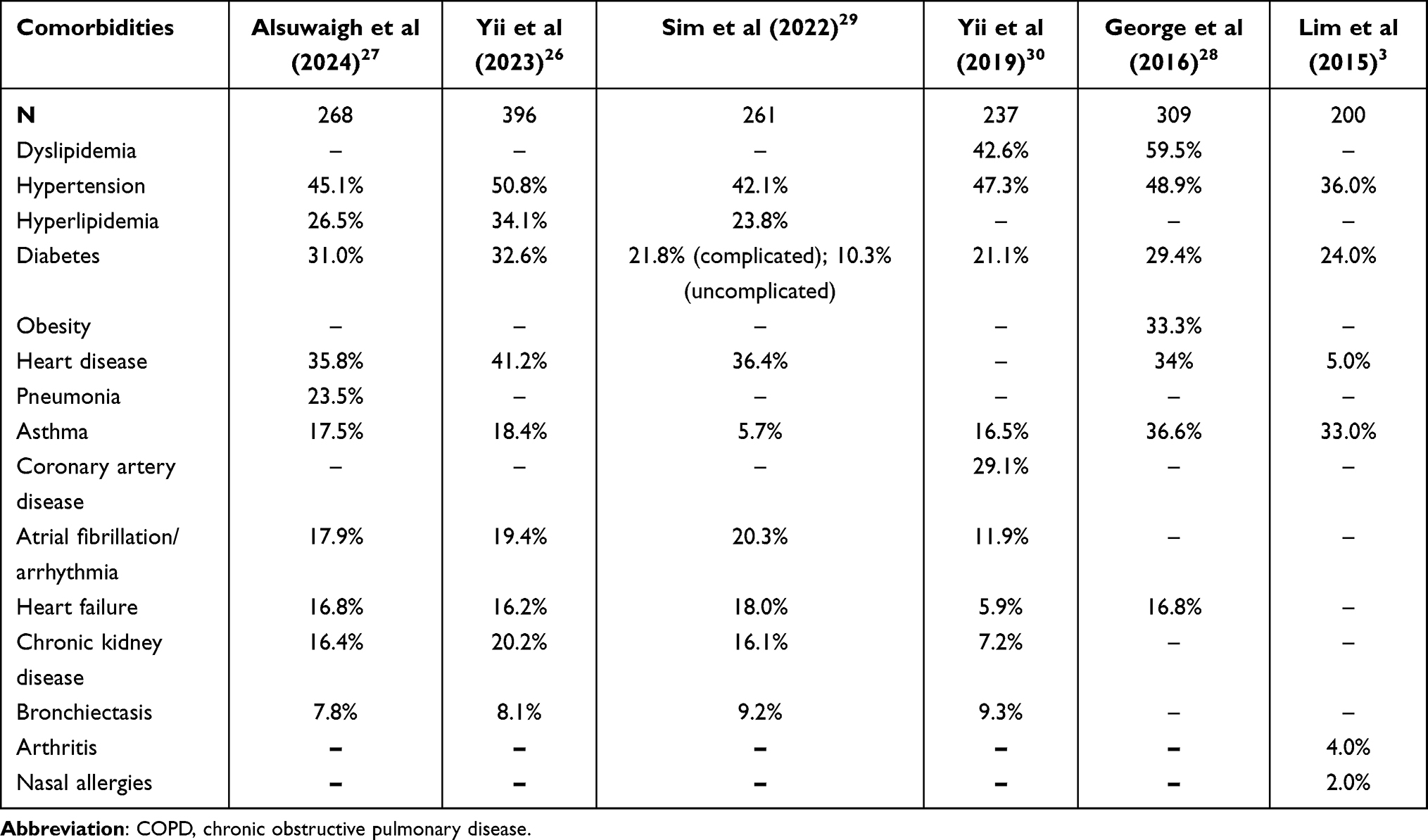 |
Table 4 Comorbid Conditions Among Patients with COPD in Singapore |
Hypertension consistently emerges as the most prevalent comorbidity, affecting 36% to 50.8% of patients across studies. Diabetes mellitus is also prominent, with prevalence rates ranging from 10.3% to 32.6%, highlighting the interplay between metabolic disorders and COPD. Cardiovascular comorbidities are notably common, with heart disease reported in 5% to 41.2% of patients and heart failure in 5.9% to 18%.3,27–30 Patients with COPD have a 2- to 5-fold increased risk of developing ischemic heart disease, heart failure, arrhythmias, or peripheral vascular disease. The coexistence of COPD and cardiovascular disease complicates the diagnostic process. Soriano et al reported that COPD was underdiagnosed in 60% of patients with cardiovascular disease and in 87% of those with ischemic heart disease.45,46 The coexistence of asthma and COPD shows considerable variation across studies (6.0–36.6%), possibly reflecting differences in diagnostic criteria or study populations. The concern regarding inappropriate or prolonged use of OCSs in the absence of appropriate disease diagnosis is particularly higher in cases of undiagnosed patients with COPD or those misdiagnosed with asthma.47,48 Other significant comorbidities include hyperlipidemia/dyslipidemia (23.8–59.5%), chronic kidney disease (7.2–16.4%), and bronchiectasis (7.8–9.3%).3,27–30 Moreover, 25% of prevalence was recorded in patients with COPD presenting with mild cognitive impairment.49
A long-term study revealed that patients treated with OCSs faced substantially increased disease risks compared with those not exposed to OCS: 26% higher for cardiovascular complications, 80% for osteoporosis and fractures, and 44% for type 2 diabetes.48 These findings align with research identifying distinct “high-risk” clusters among Chinese patients with COPD in Southeast Asia (Singapore, Malaysia, and Hong Kong), particularly the cardiovascular and ex-tuberculosis clusters, which demonstrate the highest mortality and complex cytokine networks.50
The high prevalence of these comorbidities emphasizes the need for a comprehensive, multidisciplinary approach to COPD management in Singapore. Such an approach, beginning with a simple spirometry analysis for diagnosis, involves collaboration among various healthcare professionals, including pulmonologists, cardiologists, endocrinologists, and primary care physicians. This integrated care model ensures a comprehensive assessment and treatment of both respiratory and comorbid conditions, improving patient outcomes, and a simple spirometry analysis to rule out COPD. Clinicians must be vigilant in screening for and managing these concurrent conditions as they can significantly impact COPD symptoms, exacerbation rates, and overall prognosis. Furthermore, the complex interplay between COPD and its comorbidities necessitates tailored treatment strategies that consider potential drug interactions and cumulative treatment burdens.
Disease Burden, Quality of Life, and Economic Costs
COPD significantly impacts the quality of life (QoL) of patients and imposes economic burden on these patients in Singapore. Multidimensional questionnaires are recommended to assess the broader impact of COPD on patients beyond dyspnea.1
In a single-center observational study, 51% of patients lacked COPD Assessment Test (CAT) scores and 42% had no lung function data; however, the available data suggested that patients were moderately symptomatic (median CAT score: 10), with mild/moderate lung function impairment (GOLD grade I: 26%; GOLD grade II: 49%).29 This pattern of underassessment was further confirmed in a study of 268 patients hospitalized for COPD exacerbations, wherein only 65.7% of patients had recorded lung function tests and 74.6% had documented CAT scores. Among those patients with available data, the median CAT score was 12 (interquartile range [IQR]: 7–17), indicating moderate symptom burden, with 65.5% of patients scoring ≥10, which suggested clinically significant symptoms.27 Lung function tests revealed a median post-bronchodilator forced expiratory volume in 1 s (FEV1) of 63% predicted, with 44.3% of patients classified as GOLD grade II (moderate airflow limitation). Patients prescribed LAMA+LABA combination therapy demonstrated a significantly worse QoL, with higher CAT scores and worse lung function (median FEV1 55% predicted) than those prescribed LAMA monotherapy (72% predicted) or ICS+LABA (68% predicted).27,29 These findings from single-center studies underscore the critical need for a routine QoL assessment using validated tools to guide appropriate treatment decisions and optimize patient outcomes.
The economic burden of COPD in Singapore represents a significant public health concern. Earlier estimates by Teo et al indicated that COPD cost major public health clusters in Singapore approximately US$ 9.9 million annually between 2005 and 2009, with inpatient hospitalizations being the major cost driver, accounting for 73% of total expenditures. The study revealed that hospitalization costs averaged US$ 7.2 million per year, whereas outpatient care, emergency department (ED) visits, and primary care contributed to 17%, 5%, and 3% of the overall costs, respectively.32 Woo et al later estimated the annual societal cost per capita for COPD in Singapore at US$ 2700, which included both direct medical costs and indirect costs such as productivity losses. The direct healthcare costs were primarily driven by inpatient hospitalizations (68%) followed by ED visits (32%).32,51
Hospitalization and Mortality Burden
The data on COPD hospitalization rates in Singapore are limited. However, recent data from Alsuwaigh et al provided important insights into healthcare utilization patterns, particularly regarding ED visits and subsequent hospitalizations. The study revealed a distinct pattern: 24.6% of patients required multiple (>2 folds) ED visits leading to hospitalization due to exacerbations, indicating a subset of patients with more severe or poorly controlled disease. Additionally, 31% of patients experienced a single ED visit requiring hospitalization, whereas 44.4% of patients managed their condition without requiring hospitalization.27 These findings are complemented by earlier data from the Asia-Pacific region from Lim et al, who reported that 19% of patients were hospitalized in the previous 12 months due to their condition.3
Yii et al analyzed 2774 COPD admissions in Singapore, reporting a 30-day readmission rate of 27%, which declined from 31% (2017–18) to 21% (2022–23). Key predictors included a higher Charlson Comorbidity Index score (CCI: 2–3 vs. 1, odds ratio [OR]: 1.50; CCI: ≥4 vs. 1, OR: 2.00) and an elevated Hospital Frailty Risk Score (HFRS: ≥5 vs. <5, OR: 1.29). After adjusting for multimorbidity and frailty, the odds of readmission fell by 32% to 35% in 2021–23 compared with those in 2017–18—an improvement masked in unadjusted analyses. These findings underscore the need to account for patient complexity when evaluating COPD care performance.25
The impact of physical frailty on hospitalization and mortality outcomes was particularly noteworthy, as demonstrated in a longitudinal study of 1116 patients over 8.2 years. Prefrailty or frailty was independently associated with a 1.8-fold increase in the mortality risk (adjusted hazard ratio [HR]: 1.83; 95% confidence interval [CI]: 1.24–2.68) compared with that in robust patients with COPD. This risk was further amplified when frailty co-occurred with poor lung function (FEV1 <80%) or dyspnea, resulting in a 2.4-fold to 3.25-fold increase in mortality risk. Notably, patients in the highest risk category of a combined prognostic index (incorporating physical frailty, FEV1 <80%, and dyspnea) showed up to an 8.96-fold increase in mortality risk despite adjusting for confounding factors.39 The Integrated Care Pathway (ICP) for COPD, developed by Wu et al,52 is a structured, multidisciplinary program ensuring coordinated care across primary, hospital, and home settings. The ICP aims to improve outcomes through evidence-based care while reducing hospitalizations. By year 2, the ICP reduced COPD-related hospitalizations by 27% and bed days by 22%, whereas compliance with the all-or-none care bundle rose from 28% to 54%.52 A CGH study evaluated a multidisciplinary telehealth program for 845 high-risk patients with COPD (mean age: 77.9 years). The intervention group showed greater reductions in both COPD-related and all-cause admissions compared to the control group, with 26 fewer COPD-related and 38 fewer all-cause admissions per 100 patients over 12 months.53 Two recent population-based studies highlighted the substantial economic burden of COPD utilizing Singapore’s national health administrative data.35,54 Juang et al54 reported average direct medical costs of SGD 5291 per patient/year among 18866 COPD patients, predominantly driven by hospitalization (70.1%). Only one-third of costs are directly attributable to COPD, while two-thirds stem from comorbidities particularly other respiratory (15%), circulatory (14.9%), and metabolic (7.8%) diseases. Authors35 report the 20-year projection of cost burden in patients with COPD to be $2.4 billion (2024–2043) mainly due to outpatient visit costs (54.8%). Metabolic (17.4%), circulatory (17.0%), and other respiratory diseases (9.8%) are major cost contributors alongside COPD (20.3%), disproportionately affecting elderly patients and adult males.35
A significantly higher all-cause mortality was seen in patents with COPD versus non-COPD individuals (HR, 1.80; 95% CI: 1.40–2.30), which worsened with increasing severity.55 In this meta-analysis based on 286,314 patients worldwide, Zhao et al reported that smoking, coexisting respiratory diseases (HR, 3.64; 95% CI: 3.10–4.27), cardiovascular diseases (HR, 1.29; 95% CI: 1.10–1.50) and cancers - especially lung cancer (HR, 2.57; 95% CI: 2.04–3.24) were independent determinants of COPD-related mortality.55 The mortality landscape of COPD in Singapore has shown notable historical trends. From 1991 to 1998, COPD mortality decreased remarkably by 43.7%, continuing a steady downward trend observed since the 1970s. This decline was evident across genders, although mortality rates in male patients was approximately four folds higher than those in female patients. Ethnic variations in mortality reduction were significant, with Chinese and Indian patients experiencing substantial decreases of 47.6% and 65.0%, respectively, whereas Malay patients showed a less pronounced reduction of only 12.2%.56 During the 1988–99 period, the mean COPD mortality rate was 303.1 per 100,000 population, with the highest burden among Chinese and Malay patients, and the lowest among Indian patients. Notably, although a majority of the ethnic groups showed declining mortality trends, Malay male patients exhibited an 11% increase in mortality during this period. These ethnic variations appear to correlate with smoking prevalence, which was the highest among Malay patients (23.5%), followed by Indian (15.9%) and Chinese (13.6%) patients.57 These apparent ethnic variations may be due to multiple confounders, such as smoking behaviour, socioeconomic status, and access to care.
Studies report a 17% 1-year mortality rate after COPD-related hospital discharge. Risk factors included male gender, duration of disease >5 years, and poor lung function (FEV1 <50% predicted). Mortality estimates are likely underestimated because of underdiagnosis, especially in the elderly, with COPD often recorded as a contributory factor rather than the primary cause of death.31
The duration of hospital stays also reflects disease severity and mortality risk of patients with complications spending an average of 7.7 days in hospitals 79% longer than the average of 4.3 days for patients without complications. This extended hospitalization correlates with an increased mortality risk and healthcare burden.52 Intervention programs has demonstrated promising effects on reducing COPD mortality in Singapore. Disease management programs, which include disease-related education, optimization of evidence-based medications, support from case managers, self-management principles, and timely treatment for exacerbations, have been associated with lower all-cause mortality than standard care.28 These outcomes highlight the critical role of allied health professionals, such as nurses, pharmacists, and respiratory therapists, in delivering comprehensive COPD care, which is a key component that contributes to improved survival and QoL. These findings highlight the complex nature of COPD mortality in Singapore, influenced by smoking prevalence, healthcare interventions, and diagnostic challenges.
Evolution of COPD Management in Singapore: Real-World Evidence and Treatment Patterns
Diagnostic Tools
Spirometry is essential to ensure accurate diagnosis and appropriate management, and serves as the gold standard for COPD diagnosis.1,58 The international GOLD standard for COPD recommends the use of spirometry as a benchmark for the accurate and repetitive measurement of lung function.1 However, access to spirometry is often limited in general practice. In Singapore, most general practice clinics do not offer the spirometry services necessary for early diagnosis and staging of COPD to facilitate appropriate disease care.52 However, Singapore polyclinics are now progressively establishing spirometry services, which should be further strengthened.
Current Treatment Landscape and Implementation of Guidelines
COPD management in Singapore is hindered by significant challenges, particularly regarding the real-world implementation of treatment guidelines and initial bronchodilator therapy decisions.29 Real-world evidence from CGH has provided valuable insights into treatment patterns. Sim et al revealed that patients initiated on LAMA+LABA typically present with more severe COPD than those prescribed LAMA monotherapy, although similar rates of clinical worsening were observed in both groups, thereby highlighting the critical importance of early disease identification and timely treatment optimization to prevent disease progression.29 A retrospective, real-world, single center study from CGH reported the treatment regimens in various group-based trajectories numbered C1 to C4 based on moderate-to-severe COPD exacerbations. It was seen that “no treatment” was the predominant regimen at baseline in patients in the C1 trajectory, which declined over 3 years and there was an increase in proportion of patients receiving LABA+LAMA. Patients on C2 received triple therapy predominantly but LABA+LAMA was also prescribed and the patients in C3 and C4 trajectories received triple therapy for the entire follow-up period.26 Another retrospective analysis at CGH (October 2018 to April 2020) identified a significant treatment gap, with 84% of patients qualifying for treatment escalation under both GOLD 2019 and 2023 guidelines.27 This finding is particularly relevant given the evolving GOLD recommendations, which now incorporate the blood eosinophil count as a key factor in guiding treatment adjustments for high-risk patients, showing a marked shift from previous approaches that did not rely on this biomarker.27
Moreover, Keeratichananont et al highlighted the emerging role of fractional exhaled nitric oxide (FeNO) testing in COPD management.59 The strong correlation between FeNO levels and blood eosinophil counts suggests its potential as a non-invasive biomarker for eosinophilic inflammation. High FeNO levels (≥25 ppb) were linked to poorer outcomes, including increased exacerbations, hospitalizations, and mortality, indicating its value as a prognostic tool. Although larger studies are needed, FeNO testing could play a significant role in COPD management, potentially guiding decisions on the use of ICSs and overall treatment strategies.59
The translation of guidelines into clinical practice remains challenging, as evidenced by an observational study across Southeast Asia and Australasia, including three Singapore sites, which found that only 80% of ED-diagnosed patients with COPD received bronchodilator treatment.29,60 Safety considerations further complicate treatment decisions, particularly regarding the use of ICSs in combination with long-acting bronchodilators, which has been associated with up to a 39% increased relative risk of pneumonia.27
Emerging Therapeutic Approaches and Future Directions
While current management strategies in Singapore focus on optimizing bronchodilator and ICS therapies, the landscape of COPD treatment is poised for significant evolution with the advent of biologic therapies. Table 5 presents several active clinical trials investigating the effects of biologics in patients with COPD, targeting various inflammatory pathways implicated in disease progression.61–71 These include agents targeting type 2 inflammation (such as mepolizumab and benralizumab targeting IL-5, and dupilumab targeting IL-4 and IL-13) and those targeting alarmins (including itepekimab and tozorakimab targeting IL-33, astegolimab targeting ST-2, and tezepelumab targeting thymic stromal lymphopoietin [TSLP]).17
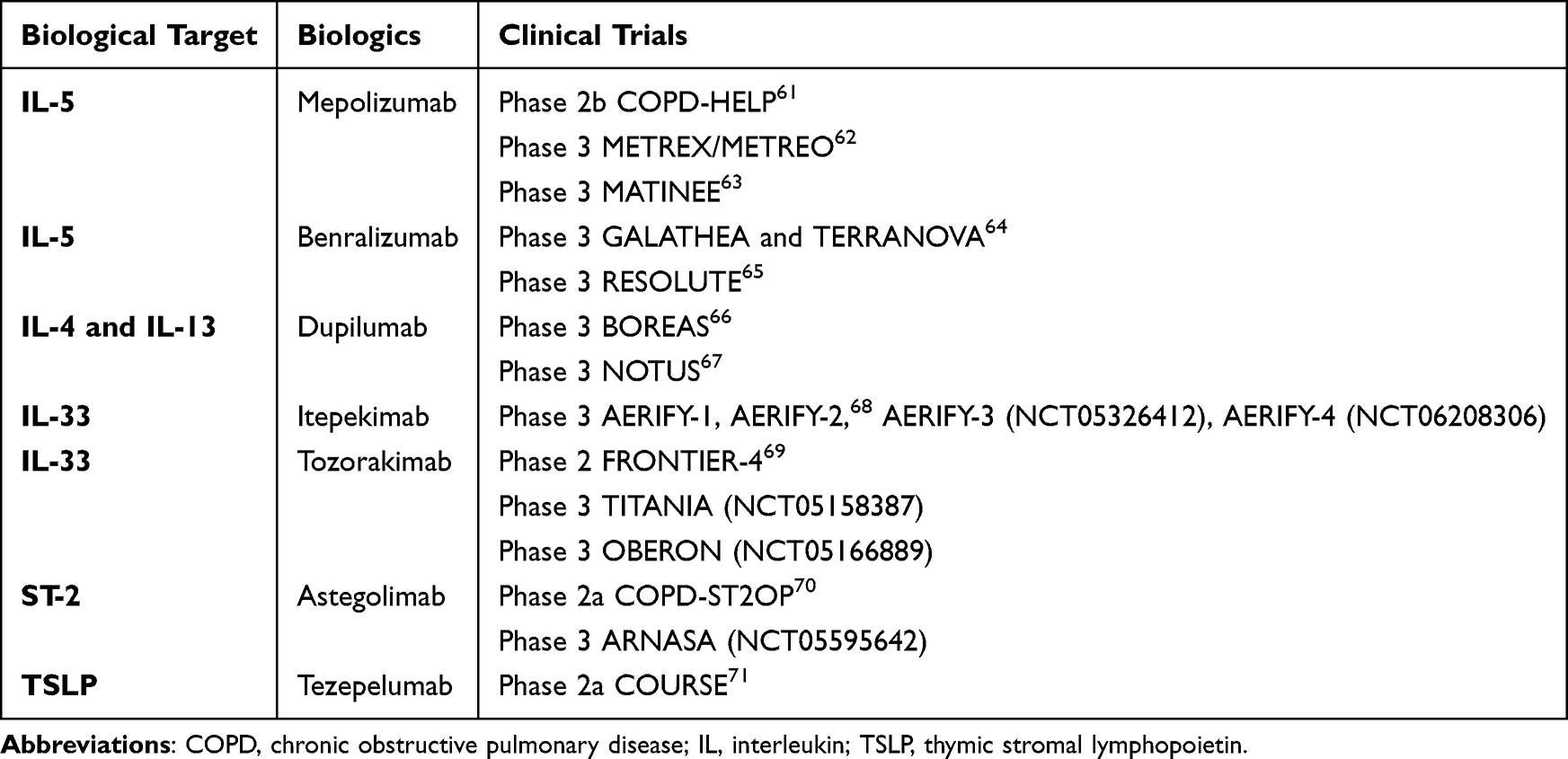 |
Table 5 Therapeutic Targets for the Biological Treatment of COPD61–71 |
The recent approval of some biologics and ongoing trials for others may herald a new era of precision medicine in COPD management, offering targeted treatment options for specific patient subgroups. The US FDA, the European Medicines Agency (EMA), and the Health Sciences Authority, Singapore have recently approved dupilumab and mepolizumab (US FDA, EMA) as an add-on maintenance treatment for uncontrolled COPD characterized by elevated blood eosinophil counts in patients who are prescribed a stable combination of an ICS, a LABA, and a LAMA, or a combination of a LABA and a LAMA in case an ICS is not appropriate.14,15 This landmark development introduces biologics targeting the type 2 inflammatory pathway, which is involved in approximately 20–40% of patients with COPD.72 The GOLD 2026 guidelines suggest that patients experiencing persistent exacerbations despite triple therapy (LABA+LAMA+ICS) with a blood eosinophil count of ≥300 cells/μL may be suitable candidates for dupilumab co-treatment.1 Although biologics for COPD have received regulatory approval, their real-world implementation in Singapore is likely to be constrained by substantial costs, uncertainty regarding cost-effectiveness, requirement for biomarker identification and careful patient selection, and insufficient integration of biologic treatment pathways within primary care settings. Collectively, these challenges likely limit the early adoption to specialized centers and carefully selected patients, emphasizing the need for locally generated effectiveness and health economic evidence.
The evolution of COPD management in Singapore necessitates a comprehensive approach to address current gaps in patient care. Establishing a nationwide integrated care program, supported by a multidisciplinary approach involving pulmonologists, primary care providers, and allied health professionals, is crucial for delivering coordinated and patient-centric care. Access to spirometry for early diagnosis represents a key potential future direction that should be implemented countrywide to facilitate timely intervention. Ongoing real-world studies utilizing routine clinical practice data, coupled with the development of robust guidelines for the selection of novel therapy, particularly biologics, will be essential. These strategic efforts will enable more personalized and effective COPD management in Singapore, while ensuring the optimal use of healthcare resources, ultimately improving patient outcomes in real-world clinical settings.
Adherence to Treatment in Singaporean Patients with COPD
Treatment adherence remains a significant challenge in COPD management, with multiple factors influencing patients’ ability to follow prescribed therapeutic regimens. Adherence is a key determinant of treatment outcomes in COPD management as non-adherence to COPD medication has been associated with poor symptom control, an increased risk of exacerbations, increased healthcare utilization and costs, decreased health-related QoL, and higher mortality rates.1,73 COPD non-adherence occurs in two forms: intentional (due to medication beliefs and concerns regarding side effects) and unintentional (due to regimen complexity and technique issues). Both types of non-adherence led to worse clinical outcomes, including increased exacerbations and disease progression.74–76
Recent research by Sim et al provides important insights into medication adherence patterns in Singapore.29 The study demonstrated a relatively high median medication dispensation rate of 0.86 (IQR: 0.56–1.00), where the dispensation rate was defined as the ratio of inhalers dispensed to inhalers prescribed during the follow-up period.29 Notably, adherence as assessed by the medication dispensation rate was high across different groups, suggesting that differences in disease severity were not related to differing rates of adherence.29
Additionally, the complexity of inhaler device usage poses a challenge to COPD treatment adherence. Up to 60% of patients commit critical inhaler technique errors, potentially reducing medication effectiveness and disease control, even with regular medication use.77 To address these challenges, successful adherence interventions must be multifaceted, incorporating patient education, simplified treatment regimens, regular technique assessment, and consideration of cultural factors.
Limitations
This narrative review provides valuable insights into the COPD prevalence, severity and management in Singapore; however, we should consider the limitations while interpreting these findings. The paucity of long-term real-world data, current uncertainties regarding patient selection and health-system considerations play a substantial role in overall COPD outcomes and management. The evidence base for the COPD landscape in Singapore is further constrained, as the current literature is predominantly derived from the studies conducted at Changi General Hospital, with very few population-based studies and few reports from the Health Ministry. Most of the interpretations in this review are consequently drawn from this limited body of evidence. While factors impacting hospitalization and risk factors for mortality appear consistent with findings reported in the international literature, lack of cause-specific mortality data for patients with COPD in Singapore remains a notable evidence gap that warrants attention in future research.
Conclusions
COPD in Singapore presents unique challenges despite reductions in age-standardized prevalence and mortality rates. This study highlights critical gaps in current practice: underutilization of diagnostic tools resulting in a substantial proportion of patients remaining inadequately assessed, substantial treatment gaps, and the need for culturally tailored approaches across diverse ethnic groups in Singapore. To address these challenges effectively, healthcare systems should enhance accessibility of spirometry in primary care settings, develop integrated care pathways, and establish clear protocols for the implementation of biologic therapy.
In particular, the patient population for dual/triple therapy typically includes those with moderate-to-severe COPD. Despite optimized inhaler triple therapy, a subset of patients continues to experience exacerbations.78,79 Dupilumab, recently approved in Singapore (2025) as the first biologic for COPD in patients with moderate-to-severe elevated eosinophils, may offer new hope to improve patient outcomes. Biologics specifically target type 2 inflammation pathways in COPD, offering precision medicine for patients with identifiable inflammatory endotypes.79,80 These focused efforts will be crucial in addressing the projected increase in COPD burden associated with population aging in Singapore, ultimately improving outcomes for this heterogeneous patient population.
Acknowledgments
Medical writing and editorial support were provided by Pankaj Kothavade, PhD, and Phani Tejasvi Gundu, MPharm, from Sanofi.
Disclosure
Anthony Yii received grants/honoraria paid through his institution from Sanofi, GlaxoSmithKline, and AstraZeneca; Wenjia Chen declared no conflicts of interest; and Yerson Maldonado Sanchez and Qiuwen Lai are employees of Sanofi and may hold stocks and/or stock options in the company. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for prevention, diagnosis and management of COPD: 2026 report. Available from: https://goldcopd.org/wp-content/uploads/2025/11/GOLD-REPORT-2026-v1.2-20Nov2025_WMV.pdf.
2. Decramer M, Janssens W, Miravitlles M. Chronic obstructive pulmonary disease. Lancet. 2012;379(9823):1341–17. doi:10.1016/s0140-6736(11)60968-9
3. Lim S, Lam DC-L, Muttalif AR, et al. Impact of chronic obstructive pulmonary disease (COPD) in the Asia-Pacific region: the EPIC Asia population-based survey. Asia Pacific Fam Med. 2015;14(1):4. doi:10.1186/s12930-015-0020-9
4. Rhee CK, Chau NQ, Yunus F, Matsunaga K, Perng DW. Management of COPD in Asia: a position statement of the Asian Pacific society of respirology. Respirology. 2019;24(10):1018–1025. doi:10.1111/resp.13633
5. Dirven JA, Tange HJ, Muris JW, van Haaren KM, Vink G, van Schayck OC. Early detection of COPD in general practice: implementation, workload and socioeconomic status. A mixed methods observational study. Prim Care Respir J. 2013;22(3):338–343. doi:10.4104/pcrj.2013.00071
6. Tiew PY, Ko FWS, Pang SL, et al. Environmental fungal sensitisation associates with poorer clinical outcomes in COPD. Eur Respir J. 2020;56(2):2000418. doi:10.1183/13993003.00418-2020
7. Fattahi F, ten Hacken NH, Löfdahl CG, et al. Atopy is a risk factor for respiratory symptoms in COPD patients: results from the EUROSCOP study. Respir Res. 2013;14(1):10. doi:10.1186/1465-9921-14-10
8. How CH, Fock KM. Healthcare in Singapore: the present and future. Singapore Med J. 2014;55(3):126–127. doi:10.11622/smedj.2014027
9. Nici L, Mammen MJ, Charbek E, et al. Pharmacologic management of chronic obstructive pulmonary disease. an official American thoracic society clinical practice guideline. Am J Respir Crit Care Med. 2020;201(9):e56–e69. doi:10.1164/rccm.202003-0625ST
10. Chen S, Small M, Lindner L, Xu X. Symptomatic burden of COPD for patients receiving dual or triple therapy. Int J Chron Obstruct Pulmon Dis. 2018;13:1365–1376. doi:10.2147/copd.S163717
11. Burge AT, Cox NS, Dal Corso S, Jones AW, Faqih FM, Holland AE. Cumulative dispensing of oral corticosteroids over 12 months in people with COPD. Int J Chron Obstruct Pulmon Dis. 2025;20:149–158. doi:10.2147/copd.S491654
12. Pitre T, Lupas D, Mah J, et al. Biologic therapies for chronic obstructive pulmonary disease: a systematic review and network meta-analysis of randomized controlled trials. Copd. 2025;22(1):2449889. doi:10.1080/15412555.2025.2449889
13. McCann MR, Kosloski MP, Xu C, Davis JD, Kamal MA. Dupilumab: mechanism of action, clinical, and translational science. Clin Transl Sci. 2024;17(8):e13899. doi:10.1111/cts.13899
14. Prescribing Information: NUCALA (mepolizumab) for injection, for subcutaneous use, Revised: 05/2025. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/125526s007lbl.pdf.
15. Prescribing Information: DUPIXENT® (dupilumab) injection, for subcutaneous use, Revised: 06/2025. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/761055s070lbl.pdf.
16. Prescribing Information, dupixent (dupilumab) 200/300 mg solution for injection in a pre-filled syringe, 2025, health sciences authority (HSA), Singapore. 2025 Available from: https://www.ndf.gov.sg/about-drugs/product-information/sin17291p/
17. Kersul AL, Cosio BG. Biologics in COPD. Open Respir Arch. 2024;6(2):100306. doi:10.1016/j.opresp.2024.100306
18. Boers E, Barrett M, Su JG, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
19. Chen S, Kuhn M, Prettner K, et al. The global economic burden of chronic obstructive pulmonary disease for 204 countries and territories in 2020-50: a health-augmented macroeconomic modelling study. Lancet Glob Health. 2023;11(8):e1183–e1193. doi:10.1016/s2214-109x(23)00217-6
20. World Health Organization (WHO). 2024 COPD fact sheet: chronic obstructive pulmonary disease. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-%28copd%29.
21. Ministry of Health Singapore. Principal causes of death. 2023. Available from: https://www.moh.gov.sg/others/resources-and-statistics/principal-causes-of-death/.
22. Ministry of Health Singapore. Action plan for successful ageing 2023. 2024. Available from: https://www.moh.gov.sg/others/resources-and-statistics/action-plan-for-successful-ageing.
23. COPD Working Group R; RWG. COPD prevalence in 12 Asia–Pacific countries and regions: projections based on the COPD prevalence estimation model. Respirology. 2003;8(2):192–198. doi:10.1046/j.1440-1843.2003.00460.x
24. Ho T, Cusack RP, Chaudhary N, Satia I, Kurmi OP. Under- and over-diagnosis of COPD: a global perspective. Breathe. 2019;15(1):24–35. doi:10.1183/20734735.0346-2018
25. Yii A, Fong I, Loh SCH, Koh JM, Tee A. Chronic obstructive pulmonary disease 30-day readmission metric: risk adjustment for multimorbidity and frailty. Ann Acad Med Singap. 2025;54(7):419–427. doi:10.47102/annals-acadmedsg.202524
26. Yii A, Xu X, Loh CH, et al. Year-to-year trajectories of hospital utilisation rates among patients with COPD: a real-world, single-centre, retrospective cohort study. BMJ Open. 2023;13(9):e072571. doi:10.1136/bmjopen-2023-072571
27. Alsuwaigh R, Yii A, Loh CH, et al. A comparison of GOLD 2019 and 2023 recommendations to contemporaneous real-world inhaler treatment patterns for chronic obstructive pulmonary disease management in Singapore. J Thorac Dis. 2024;16(2):847–861. doi:10.21037/jtd-22-1769
28. George PP, Heng BH, Lim TK, et al. Evaluation of a disease management program for COPD using propensity matched control group. J Thorac Dis. 2016;8(7):1661–1671. doi:10.21037/jtd.2016.06.05
29. Sim M, Yii A, Xu X, et al. Characteristics of patients with chronic obstructive pulmonary disease treated with long-acting bronchodilators in a real-world setting in Singapore: a single-center observational study. Int J Chron Obstruct Pulmon Dis. 2022;17:1349–1363. doi:10.2147/copd.S357820
30. Yii ACA, Loh CH, Tiew PY, et al. A clinical prediction model for hospitalized COPD exacerbations based on “treatable traits”. Int J Chron Obstruct Pulmon Dis. 2019;14:719–728. doi:10.2147/copd.S194922
31. Pin NT. Epidemiology of chronic obstructive pulmonary disease (COPD). Singapore Family Physician. 2013;39(2):8–10.
32. Teo W-SK, Tan W-S, Chong W-F, et al. Economic burden of chronic obstructive pulmonary disease. Respirology. 2012;17(1):120–126. doi:10.1111/j.1440-1843.2011.02073.x
33. Ntritsos G, Franek J, Belbasis L, et al. Gender-specific estimates of COPD prevalence: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2018;13:1507–1514. doi:10.2147/copd.S146390
34. Maselli DJ, Bhatt SP, Anzueto A, et al. Clinical epidemiology of COPD: insights from 10 years of the COPDGene study. Chest. 2019;156(2):228–238. doi:10.1016/j.chest.2019.04.135
35. Juang YR, Lim LHM, Chotirmall SH, et al. Projecting the 20-year healthcare resource burden of asthma and COPD multimorbidity: insights from Singapore for integrated chronic respiratory care in South-East Asia. NPJ Prim Care Respir Med. 2026. doi:10.1038/s41533-026-00502-9
36. Singapore census of population. 2020. Available from: https://www.singstat.gov.sg/files/b80ab730-e972-42cf-979b-f16546c0b515.pdf.
37. Wu Z, Zhang X, Zhang P, et al. The burden and risk factors of chronic obstructive pulmonary disease in Asia and its countries from 1990 to 2021: a systematic analysis based on the 2021 global burden of disease study. Front Med Lausanne. 2025;12:1641719. doi:10.3389/fmed.2025.1641719
38. Ministry of Health, Singapore. Smoking prevalence in S’pore population dropped from 13.9% in 2010 to 10.1% in 2020. Available from: https://www.moh.gov.sg/newsroom/smoking-prevalence-in-s’pore-population-dropped-from-139-in-2010-to-101-in-2020.
39. Lee SY, Nyunt MSZ, Gao Q, et al. Co-occurrence of physical frailty and COPD and association with disability and mortality: singapore longitudinal ageing study. Chest. 2022;161(5):1225–1238. doi:10.1016/j.chest.2021.12.633
40. Steinberg AW, Ozga JE, Tang Z, Stanton CA, Sargent JD, Paulin LM. Gender, tobacco and chronic obstructive pulmonary disease: analysis of the 2020 national health interview survey. BMJ Open Respiratory Res. 2025;12(1):e002462. doi:10.1136/bmjresp-2024-002462
41. Aik J, Ang L, Gunther SH, Tang C, Lee JKW, Seow WJ. Climate change and population health in Singapore: a systematic review. Lancet Regional Health – Western Pacific. 2023;40:100947. doi:10.1016/j.lanwpc.2023.100947
42. D’Amato G, Cecchi L, D’Amato M, Liccardi G. Urban air pollution and climate change as environmental risk factors of respiratory allergy: an update. J Investig Allergol Clin Immunol. 2010;20(2):95–102. quiz following 102.
43. Chatila WM, Thomashow BM, Minai OA, Criner GJ, Make BJ. Comorbidities in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008;5(4):549–555. doi:10.1513/pats.200709-148ET
44. Cavaillès A, Brinchault-Rabin G, Dixmier A, et al. Comorbidities of COPD. Eur Respir Rev. 2013;22(130):454–475. doi:10.1183/09059180.00008612
45. Soriano JB, Rigo F, Guerrero D, et al. High prevalence of undiagnosed airflow limitation in patients with cardiovascular disease. Chest. 2010;137(2):333–340. doi:10.1378/chest.09-1264
46. de Miguel-Díez J, Núñez Villota J, Santos Pérez S, et al. Multidisciplinary management of patients with chronic obstructive pulmonary disease and cardiovascular disease. Archivos de Bronconeumología. 2024;60(4):226–237. doi:10.1016/j.arbres.2024.01.013
47. Gerstein E, Bierbrier J, Whitmore GA, et al. Impact of undiagnosed chronic obstructive pulmonary disease and asthma on symptoms, quality of life, healthcare use, and work productivity. Am J Respir Crit Care Med. 2023;208(12):1271–1282. doi:10.1164/rccm.202307-1264OC
48. Tse G, Emmanuel B, Ariti C, et al. A long-term study of adverse outcomes associated with oral corticosteroid use in COPD. Int J Chron Obstruct Pulmon Dis. 2023;18:2565–2580. doi:10.2147/copd.S433326
49. Yohannes AM, Chen W, Moga AM, Leroi I, Connolly MJ. Cognitive impairment in chronic obstructive pulmonary disease and chronic heart failure: a systematic review and meta-analysis of observational studies. J Am Med Directors Assoc. 2017;18(5):451.e1–451.e11. doi:10.1016/j.jamda.2017.01.014
50. Tiew PY, Ko FWS, Narayana JK, et al. “High-Risk” clinical and inflammatory clusters in COPD of Chinese descent. Chest. 2020;158(1):145–156. doi:10.1016/j.chest.2020.01.043
51. Woo L, Smith HE, Sullivan SD. The economic burden of chronic obstructive pulmonary disease in the Asia-Pacific region: a systematic review. Value Health Regional Issues. 2019;18:121–131. doi:10.1016/j.vhri.2019.02.002
52. Wu CX, Hwang CH, Tan WS, et al. Effectiveness of a chronic obstructive pulmonary disease integrated care pathway in a regional health system: a propensity score matched cohort study. BMJ Open. 2018;8(3):e019425. doi:10.1136/bmjopen-2017-019425
53. Hnin TM. Evaluation of a multidisciplinary telehealth program for COPD patients: insights from a Singapore tertiary hospital experience, APSR 2023: AO15-1. Available from: https://onlinelibrary.wiley.com/doi/10.1111/resp.14618?msockid=3692ba99d072648b1d26afa2d1e96593.
54. Juang YR, Lim LHM, Chotirmall SH, et al. Healthcare costs and trends of multimorbidity in COPD patients: a population-based study in Singapore. Int J Chron Obstruct Pulmon Dis. 2026;21:563620. doi:10.2147/COPD.S563620
55. Zhao G, Wang L, Lei S, Li Y, Li J, Feng Z. All-cause and cause-specific mortality in chronic obstructive pulmonary disease: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2025;20:4173–4190. doi:10.2147/COPD.S563250
56. Ng TP, Niti M, Tan WC. Trends and ethnic differences in COPD hospitalization and mortality in Singapore. COPD. 2004;1(1):5–11. doi:10.1081/copd-120028702
57. Tan WC. The epidemiology and clinical management of chronic obstructive pulmonary disease in Singapore. Respirology. 2001;6(s2):S17–S20. doi:10.1046/j.1440-1843.2001.00307.x
58. Bailey KL. The importance of the assessment of pulmonary function in COPD. Med Clin North Am. 2012;96(4):745–752. doi:10.1016/j.mcna.2012.04.011
59. Keeratichananont W, Kaenmuang P, Geater SL, Denyuk R, Kanchanakanok C. Correlation of fractional exhaled nitric oxide (FeNO) and clinical outcomes in patients with chronic obstructive pulmonary disease: a prospective cohort study. Respir Med. 2024;229:107682. doi:10.1016/j.rmed.2024.107682
60. Kelly AM, Van Meer O, Keijzers G, et al. Get with the guidelines: management of chronic obstructive pulmonary disease in emergency departments in Europe and Australasia is sub-optimal. Intern Med J. 2020;50(2):200–208. doi:10.1111/imj.14323
61. Flynn C, McAuley HJC, Elneima O, et al. COPD-HELP: a randomised controlled trial of mepolizumab initiated following admission to hospital for a severe exacerbation of eosinophilic COPD [abstract]. Am J Respir Crit Care Med. 2025;211(Supplement_1):A5546. doi:10.1164/ajrccm.2025.211
62. Pavord ID, Chanez P, Criner GJ, et al. Mepolizumab for eosinophilic chronic obstructive pulmonary disease. N Engl J Med. 2017;377(17):1613–1629. doi:10.1056/NEJMoa1708208
63. Sciurba FC, Criner GJ, Christenson SA, et al. Mepolizumab to prevent exacerbations of COPD with an eosinophilic phenotype. N Engl J Med. 2025;392(17):1710–1720. doi:10.1056/NEJMoa2413181
64. Criner GJ, Celli BR, Brightling CE, et al. Benralizumab for the prevention of COPD exacerbations. N Engl J Med. 2019;381(11):1023–1034. doi:10.1056/NEJMoa1905248
65. Resolute, NCT04053634. Available from: https://clinicaltrials.gov/study/NCT04053634.
66. Bhatt SP, Christenson S, Hanania NA, et al. In the phase 3 BOREAS trial, dupilumab reduced FeNO levels over time in patients with moderate or severe severe chronic obstructive pulmonary disease with type 2 inflammation. Chest. 2024;166(4):A4835–A4839. doi:10.1016/j.chest.2024.06.2871
67. Bhatt SP, Rabe KF, Hanania NA, et al. Dupilumab for COPD with blood eosinophil evidence of Type 2 inflammation. N Engl J Med. 2024;390(24):2274–2283. doi:10.1056/NEJMoa2401304
68. Rabe KF, Martinez FJ, Bhatt SP, et al. AERIFY-1/2: two phase 3, randomised, controlled trials of itepekimab in former smokers with moderate-to-severe COPD. ERJ Open Res. 2024;10(5):00718–2023. doi:10.1183/23120541.00718-2023
69. Singh D, Guller P, Reid F, et al. A phase 2a trial of the IL-33 monoclonal antibody tozorakimab in patients with COPD: FRONTIER-4. Eur Respir J. 2025;66(1):2402231. doi:10.1183/13993003.02231-2024
70. Yousuf AJ, Mohammed S, Carr L, et al. Astegolimab, an anti-ST2, in chronic obstructive pulmonary disease (COPD-ST2OP): a phase 2a, placebo-controlled trial. Lancet Respir Med. 2022;10(5):469–477. doi:10.1016/S2213-2600(21)00556-7
71. Singh D, Brightling CE, Rabe KF, et al. Efficacy and safety of tezepelumab versus placebo in adults with moderate to very severe chronic obstructive pulmonary disease (COURSE): a randomised, placebo-controlled, phase 2a trial. Lancet Respir Med. 2025;13(1):47–58. doi:10.1016/S2213-2600(24)00324-2
72. Li S, Yi B, Wang H, Xu X, Yu L. Efficacy and safety of biologics targeting Type 2 inflammation in COPD: a systematic review and network meta-analysis. Int J Chron Obstruct Pulmon Dis. 2025;20:2143–2159. doi:10.2147/copd.S504774
73. Chen R, Gao Y, Wang H, Shang H, Xuan J. Association between adherence to maintenance medication in patients with COPD and acute exacerbation occurrence and cost in China: a retrospective cohort database study. Int J Chron Obstruct Pulmon Dis. 2020;15:963–971. doi:10.2147/copd.S234349
74. George J, Kong DC, Thoman R, Stewart K. Factors associated with medication nonadherence in patients with COPD. Chest. 2005;128(5):3198–3204. doi:10.1378/chest.128.5.3198
75. Ingebrigtsen TS, Marott JL, Nordestgaard BG, et al. Low use and adherence to maintenance medication in chronic obstructive pulmonary disease in the general population. J Gen Intern Med. 2015;30(1):51–59. doi:10.1007/s11606-014-3029-0
76. Toy EL, Beaulieu NU, McHale JM, et al. Treatment of COPD: relationships between daily dosing frequency, adherence, resource use, and costs. Respir Med. 2011;105(3):435–441. doi:10.1016/j.rmed.2010.09.006
77. Turégano-Yedro M, Trillo-Calvo E, Navarro IRF, et al. Inhaler adherence in COPD: a crucial step towards the correct treatment. Int J Chron Obstruct Pulmon Dis. 2023;18:2887–2893. doi:10.2147/copd.S431829
78. Langham S, Lewis J, Pooley N, et al. Single-inhaler triple therapy in patients with chronic obstructive pulmonary disease: a systematic review. Respir Res. 2019;20(1):242. doi:10.1186/s12931-019-1213-9
79. Kostikas K, Gogali A. Biologics in COPD: the road is still long and winding. COPD. 2025;22(1):2467657. doi:10.1080/15412555.2025.2467657
80. Gogali A, Kostikas K. Biologics in COPD: do we need a divide and conquer approach? Lung. 2025;203(1):45. doi:10.1007/s00408-025-00803-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Real-World Effectiveness of Triple Extrafine Fixed-Dose Combination with Beclomethasone/Formoterol/Glycopyrronium on Symptoms and Lung Function in COPD: A Systematic Review and Meta-Analysis
Rogliani P, Manzetti GM, Cazzola M, Calzetta L
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1723-1736
Published Date: 27 May 2025