Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Chronic Obstructive Pulmonary Disease and Obstructive Sleep Apnea Coexistence: From Pathophysiology to Clinical Complications
Authors Wei X, Zhang X, Wang S, Jiang G, Yu H, Fu B, Bai L, Sun F, Hu S, Shi L
Received 2 July 2025
Accepted for publication 8 November 2025
Published 15 December 2025 Volume 2025:20 Pages 4031—4059
DOI https://doi.org/10.2147/COPD.S550739
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Xiaotong Wei,1 Xiaoyu Zhang,2 Siping Wang,1 Guolu Jiang,1 Hongpeng Yu,2 Bowen Fu,1 Lina Bai,1 Feng Sun,1 Shaodan Hu,2 Li Shi2
1College of Traditional Chinese Medicine, Changchun University of Chinese Medicine, Changchun, Jilin, 130117, People’s Republic of China; 2Department of Pneumology, Affiliated Hospital of Changchun University of Chinese Medicine, Changchun, Jilin, 130021, People’s Republic of China
Correspondence: Li Shi, Department of Pneumology, Affiliated Hospital of Changchun University of Chinese Medicine, 1478 Gongnong Road, Changchun, People’s Republic of China, Email [email protected] Shaodan Hu, Department of Pneumology, Affiliated Hospital of Changchun University of Chinese Medicine, 1478 Gongnong Road, Changchun, People’s Republic of China, Email [email protected]
Background: Obstructive sleep apnea (OSA) and chronic obstructive pulmonary disease (COPD) are two common chronic respiratory diseases. Their co-existence forms overlap syndrome (OVS), a distinct clinical entity that imposes a dual burden on patients due to its unique pathophysiological mechanisms and significant clinical implications.
Purpose: This narrative review describes the consequences of OVS by tracing its pathophysiological from molecular mechanisms to clinical phenotypes, including non-cardiovascular complications. The primary aim is to synthesize this knowledge into a conceptual framework to guide future therapeutic development.
Methods: We searched electronic databases including Pubmed, Web of Science and Google Scholar for relevant studies and academic articles discussing OSA-COPD overlap.
Results: OVS demonstrates a high population prevalence, with distribution influenced by factors such as gender, age, COPD-specific phenotypes, and OSA severity. Pathogenically, factors including smoking and obesity collectively contribute to significant airflow limitation (AFL) through impaired respiratory control, reduced ventilatory drive, and multi-level airway narrowing. The characteristic chronic hypoxia and persistent AFL drive disease progression by triggering systemic inflammation, oxidative stress, and autonomic dysfunction. Consequently, the clinical presentation of OVS is more complex and severe than that of either disease alone, characterized by profound hypoxemia and prevalent hypercapnia. Beyond the core respiratory impairments, which predispose patients to major cardiovascular events, OVS drives a range of extrapulmonary manifestations. These include metabolic derangements, hematological alterations, neuropsychiatric complications, Vitamin D Deficiency, osteoporosis, retinal vascular tortuosity, erectile dysfunction (ED), and postural control, potentially fueled by persistent systemic inflammation and chronic hypoxia. This multisystem involvement. This multisystem involvement collectively contributes to a significantly worsened clinical prognosis.
Conclusion: Understanding the progression from localized AFL to systemic injury is essential for clarifying the full burden of OVS, particularly as it relates to its various comorbidities. Current evidence offers a basis for improving early identification and diagnosis of both the primary condition and its associated comorbid states. Future research should prioritize the development of personalized management strategies that address the specific risks of different comorbidities.
Keywords: obstructive apnea syndrome, chronic obstructive pulmonary disease, overlap syndrome, metabolic disease, vitamin D deficiency, retinal vascular tortuosity
Introduction
Chronic obstructive pulmonary disease (COPD), characterized by irreversible and progressive airflow limitation (AFL) due to chronic airway inflammation, and obstructive sleep apnea (OSA), defined by recurrent apnea and hypopnea episodes, represent two prevalent yet distinct respiratory disorders. Their coexistence, termed overlap syndrome (OVS).1 However, insufficient recognition of disease overlap by clinicians and patients frequently results in diagnostic and therapeutic oversight in clinical practice,2 thereby resulting in OVS manifesting elevated incidence rates and disproportionately high mortality that surpass those characteristics of isolated COPD or OSA presentations. Experimental evidence further corroborates these clinical observations; animal models simulating coexisting COPD and OSA through intermittent hypoxia and smoking exposure reveal characteristic pathological alterations via electron microscopy, including alveolar collapse, inflammatory cell infiltration, and immune cell damage.3 These findings collectively underscore the imperative to enhance diagnostic precision and mechanistic comprehension of sleep-disordered breathing for mitigating comorbidity-associated health burdens.
Ventilatory restriction serves as the primary pathophysiological catalyst, initiating maladaptive cellular/molecular cascades that include sympathetic hyperactivity, systemic inflammation, and oxidative stress. Crucially, these mechanisms demonstrate comorbidity-specific dominance patterns. For instance, the significantly elevated hypertension and coronary heart disease incidence observed in OVS patients compared to isolated OSA or COPD cases primarily results from exacerbated vascular endothelial damage and impaired cellular immune responses.4 Another study revealed that rodent models subjected to the combined insults of chronic intermittent hypoxia and cigarette smoke exposure-which induce characteristic pathologies including inflammatory cell infiltration and alveolar destruction-exhibit accelerated bone destruction. This effect was mechanistically linked to the resulting dysregulated systemic inflammation rather than mechanical stress alone.5 Together, these insights highlight the need for multidimensional investigation into the pathobiology of OVS.
This review aims to systematically elucidate the pathophysiological continuum of OVS from molecular mechanisms to clinical phenotypes. In addition to the conventional focus on cardiovascular complications, emerging evidence indicates that OVS is associated with a broader spectrum of multi-system complications. These encompass metabolic disturbances, neurocognitive dysfunction, psychiatric comorbidities such as depression and anxiety, as well as critical extrapulmonary manifestations including vitamin D deficiency and osteoporosis. Furthermore, less frequently recognized conditions such as impaired postural stability, erectile dysfunction (ED), and retinal vascular tortuosity have also been linked to OVS. These findings highlight the systemic nature of OVS and underscore the urgent need for enhanced early recognition and systematic clinical management. Beyond raising diagnostic awareness, it is crucial to elucidate the underlying mechanisms of these complications. To address current knowledge gaps, this review aims to establish a novel theoretical framework focused on delineating the scope of systemic complications in OVS, thereby advancing precision medicine strategies for complex respiratory multimorbidity.
Epidemiology of OSA and COPD
COPD affects more than 400 million people worldwide and ranks as the third leading cause of death. Its prevalence is strongly linked to smoking, yet notable geographic and gender disparities exist. Low- and middle-income countries bear the greatest burden, and projections indicate a rising prevalence among women- attributed to slower declines in tobacco use and greater exposure to biomass fuels-while rates among men are expected to fall.6 In parallel, OSA is highly prevalent, affecting approximately 24% of men and 9% of women aged 30–60 years. Obesity serves as a core driver of OSA, and given the ongoing increase in global obesity rates, the true prevalence of OSA is likely higher than current estimates suggest. 7 The high prevalence and serious health implications of both COPD and OSA underscore the urgent need for effective prevention and early diagnosis strategies. When it comes to patients with OVS, epidemiological investigations demonstrate variable prevalence patterns of OVS across clinical populations. While the general population exhibits an OVS prevalence of approximately 2%, this rate diverges substantially in cohorts with isolated OSA or COPD. Specifically, COPD prevalence ranges from 10.8% to 74.2% in OSA populations,8–13 whereas OSA occurs in 3.6% to 68.18% of COPD patients.14–29 Notably, individuals with cardiovascular or metabolic comorbidities show elevated OVS prevalence.30 The observed heterogeneity in epidemiological data likely arises from methodological variations, including inconsistent diagnostic criteria (eg, FEV1/FVC thresholds for AFL), differing hypoxemia definitions (eg, oxygen desaturation index cutoffs), and disparities in sleep monitoring approaches (portable devices versus laboratory polysomnography (PSG)).
Further analysis of existing prevalence data reveals distinct epidemiological characteristics of OVS. Among these, advanced age (>60 years) constitutes a clinically significant risk factor, as evidenced by a prospective observational study reporting an OVS prevalence of 41.3% in the study cohort, with advanced age (>60 years) identified as an independent risk factor strongly correlated with diminished pulmonary function parameters.31 This age-dependent association has been further corroborated by subsequent investigations.32–36 Supporting this observation, studies reveals that patients aged ≥60 years account for over 50% of reported OVS cases.11,18,37 Critically, this age-related distribution does not imply inherent biological predisposition in elderly populations. Rather, it underscores age as a contributing factor to OVS clinical manifestation, potentially mediated through cumulative exposure to shared risk factors (eg, chronic airway inflammation) and age-related physiological decline in respiratory compensatory mechanisms.
Apart from age-related influences, gender-specific disparities emerge as critical modifiers of OVS epidemiology. For instance, a comprehensive evaluation and meta-analysis by Chinese researchers revealed that the prevalence of COPD combined with OSA reached 29.1% (95% CI 27.2%-30.9%). Notably, males were identified as the predominant group in this context (OR 1.631, 95% CI: 1.231–2.161).38 And similar findings have been reported by researchers from various countries.9,14,18,19,37,39 However, a matched study from Israel showed that OSA prevalence was associated with higher rates of COPD, with a more pronounced effect in females.40 Therefore, current evidence indicates that gender-related differences represent a key factor influencing the epidemiology of OVS. More precisely, gender differences may modulate the intensity of pro-inflammatory responses and differentially affect upper airway physiology in obstructive lung diseases.40 These physiological variations likely contribute to the sex-specific clinical manifestations seen in overlapping syndromes such as COPD-OSA. In male patients, COPD typically manifests with a distinct symptom profile characterized by prominent airway symptoms such as cough and sputum, often accompanied by systemic manifestations including fatigue and sleep disturbances.41 This clinical presentation shares pathophysiological similarities with the upper airway collapse observed in OSA, suggesting a potential mechanistic interaction between the two disorders. In OSA, male patients generally display greater disease severity, as indicated by higher apnea-hypopnea index (AHI), which measures OSA severity by calculating the average number of apnea and hypopnea events per hour of sleep, and oxygen desaturation index (ODI) values, along with a stronger correlation between disease severity and body mass index (BMI) compared to females.42 These findings suggest that OSA in males is not only more severe but also more closely linked to obesity, a well-established shared risk factor for COPD-OSA overlap. Together, these male-predominant clinical features of COPD and OSA appear to form a synergistic risk profile that favors their co-occurrence.43 In contrast, potential protective effects of female reproductive hormones on respiratory function and sleep architecture may partly explain the lower prevalence of OVS in women.44 It should be noted that these proposed mechanisms require further validation, as the current understanding remains constrained by a limited number of studies specifically examining sex-related factors in the pathogenesis of OVS. Further research focused on gender differences in OVS is needed to clarify the underlying mechanisms.
In addition to demographic determinants, such as age and gender, the prevalence of OVS is associated with distinct phenotypes or progression stages of OSA and COPD. Research findings demonstrate a 47% prevalence of COPD comorbidity in patients with moderate-to-severe OSA, whereas 58% of COPD patients without OSA symptoms exhibited concurrent OVS development.37,39 Furthermore, the incidence of OVS differs between COPD phenotypes: patients with chronic bronchitis maintained a higher prevalence of OSA even after adjusting for BMI and lung function discrepancies, whereas emphysema patients demonstrated a lower OSA prevalence.45 This review reveals that OVS prevalence demonstrates bidirectional associations with the severity of underlying diseases (OSA/COPD) and is modulated by COPD phenotype-specific factors.
In conclusion, this study demonstrates that OVS exhibits elevated prevalence in both community-based populations and patients with OSA/COPD, suggesting multifactorial pathogenesis involving age, sex, and phenotypic variations. Therefore, establishing consensus on standardized diagnostic criteria is essential. How to enhance the accuracy of epidemiological assessments of OVS remains an important question worthy of further consideration (Table 1).
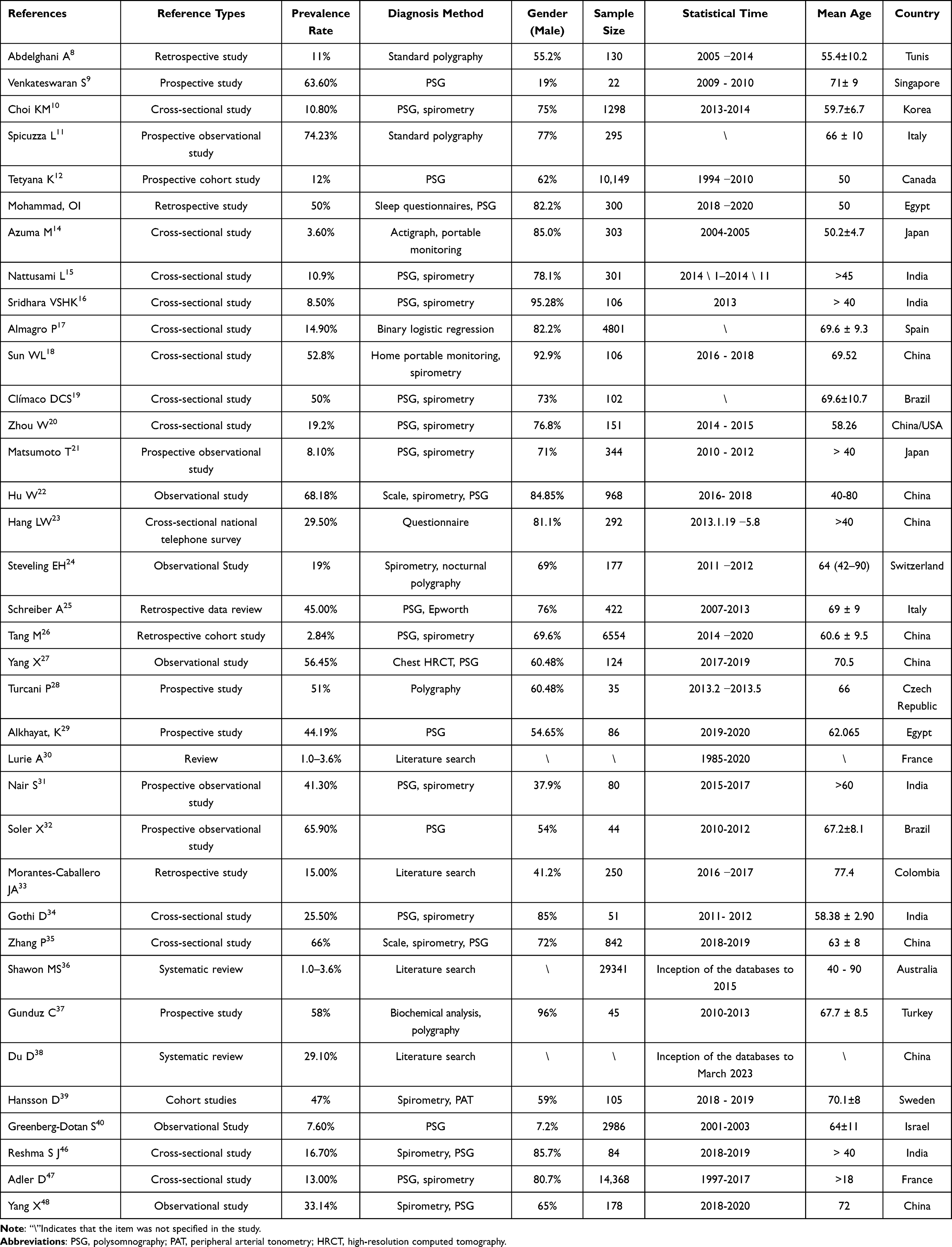 |
Table 1 Epidemiological Insights: Trends and Observations |
Common Risk Factors and Pathogenesis of COPD and OSA
The risk factors predisposing OSA patients to COPD and COPD patients to OSA demonstrate substantial overlap, with smoking, obesity, systemic inflammation,49 and advanced age representing core shared elements.50 Smoking stands as the most well-established common risk factor, not only directly damaging the lower airways to cause COPD but also contributing to upper airway inflammation and collapse, thereby promoting the development of OSA.51 Obesity, particularly central adiposity and increased neck circumference, participates in the pathogenesis of both OSA and COPD through mechanical compression of the upper airway and restriction of lung volume.52 Furthermore, OSA exacerbates airway inflammation in COPD patients, leading to markedly elevated inflammatory markers.53 The systemic inflammation associated with COPD, combined with intermittent hypoxia and oxidative stress resulting from OSA, can mutually influence the structure and function of both upper and lower airways, establishing a self-perpetuating pathological cycle.49 As previous scholars have comprehensively summarized and visualized these interactions, they will not be elaborated in detail here.54 Beyond these established factors, emerging evidence has revealed the crucial involvement of neurorespiratory control mechanisms in OVS pathophysiology.55 Consequently, the considerable overlap and bidirectional nature of these risk factors provide a fundamental explanation for the frequent coexistence of COPD and OSA as an “OVS”. The following sections will elaborate on the various elements contributing to the pathogenesis of this complex clinical entity (Figure 1).
 |
Figure 1 Anatomical and non-structural determinants interact to impair pulmonary ventilation and gas exchange, leading to systemic hypoxia. This condition predisposes individuals to increased risks of inflammation, oxidative stress, and altered autonomic nervous activity, which may subsequently contribute to the pathogenesis of disorders in other organ systems. |
Non-Anatomical Factors
Obesity
Obesity represents a critical pathophysiological link between COPD and OSA, with their interactions creating a self-reinforcing vicious cycle.56,57
Mechanistically, cervical adipose deposition in obesity compromises the structural integrity of pharyngeal soft tissues, leading to upper airway narrowing and establishing the anatomical foundation for the upper airway collapse central to OSA pathogenesis.58 Simultaneously, abdominal obesity mechanically restricts diaphragmatic excursion and acts synergistically with COPD to significantly reduce lung compliance and functional residual capacity (FRC).56 This FRC reduction facilitates small airway collapse by allowing closing volume to exceed the threshold, while simultaneously diminishing the longitudinal traction that maintains upper airway patency, thereby creating a dual compromise of both upper and lower airways. This compromised respiratory mechanics is further exacerbated in the supine position due to elevated intra-abdominal pressure, culminating in posture-dependent hypoxemia.59
Biologically, the pulmonary inflammation characteristic of COPD engages in cross-talk with the systemic inflammation and oxidative stress triggered by OSA-related intermittent hypoxia, resulting in synergistic amplification. When combined with the adipokine-mediated systemic inflammation and immune dysregulation inherent to obesity, these processes deliver a collective second hit that significantly aggravates systemic injury, cardiovascular risk, and airway hyperresponsiveness.60
Regarding gas exchange, the convergence of persistent daytime hypoxemia from COPD and severe intermittent nocturnal hypoxemia from OSA generates a nearly continuous hypoxic burden that serves as a primary driver for pulmonary hypertension (PH) and respiratory failure. Crucially, these processes form a self-perpetuating cycle wherein obesity-aggravated hypoxemia and hypercapnia stimulate further adipogenesis, while progressive pulmonary dysfunction exacerbates metabolic disturbance.61,62
Ultimately, the intricate interplay of mechanical, inflammatory, hypoxic, and metabolic dysregulations leads to substantially worse clinical outcomes in patients with the COPD-OSA-obesity-OVS, highlighting the imperative for integrated therapeutic strategies.
Cigarette Smoking
Cigarette smoking, an established pathogenic driver of COPD progression, exhibits a dual mechanistic role in OSA pathogenesis.63 Epidemiological analyses consistently demonstrate elevated smoking prevalence among OSA cohorts, with a dose-dependent correlation between smoking intensity and OSA severity.64–66 Clinically, smoking potentiates OSA-associated comorbidities including COPD, hypertension, and chronic airway inflammation through synergistic pathways.67 Mechanistically, tobacco smoke induces respiratory epithelial barrier dysfunction, impairing innate defense against inhaled pathogens and particulate matter.68,69 This is compounded by smoke-triggered oxidative stress, inflammatory cascades, and apoptotic signaling that collectively drive airway remodeling- a hallmark of COPD pathophysiology.70 Parallel neurorespiratory effects emerge through smoke-mediated suppression of central respiratory drive, manifesting as sleep-related ventilatory instability.71 While these findings position smoking as a shared etiological nexus for OSA and COPD via peripheral and central mechanisms, precise molecular pathways warrant further elucidation.
Age
Structural and functional degeneration of the respiratory system associated with aging, characterized by degradation of pulmonary elastic matrices, dilation of alveolar ducts, and compromised chest wall mechanics, progressively reduces gas exchange efficiency and ventilatory capacity.72 These senescent adaptations not only potentiate COPD symptom severity but also interact synergistically with OSA pathophysiology in elderly populations. Older OSA patients exhibit heightened susceptibility to sleep architecture fragmentation, nocturnal hypoxemia exacerbations, and cardiometabolic comorbidities, attributable in part to age-dependent deterioration of neuromodulatory control over respiratory drive stability.72,73 Crucially, cumulative environmental exposures (eg, smoking) after the fourth decade compound these vulnerabilities, amplifying risks of obstructive airway disease progression.51 Epidemiological profiles confirm OVS predominance in populations over 60, with incidence rates substantially exceeding those of younger cohorts.11,18,37 While advanced age emerges as a cardinal determinant of OVS epidemiology, precise age-stratified risk stratification remains constrained by insufficient mechanistic delineation of age-OSA-COPD interplay.
Impaired Immune Function
Immune dysregulation plays a pivotal role in the pathogenesis of chronic respiratory disorders. In COPD, aberrant lower airway immune responses manifest as lymphoid follicle formation through coordinated infiltration of innate and adaptive inflammatory cells.74 Tobacco exposure, including conventional and electronic cigarettes, suppresses respiratory tract immunity by downregulating critical immune-related gene networks while concurrently activating pro-inflammatory cascades in pulmonary structural cells.75 OSA further compounds this immune perturbation through sleep-disordered breathing-induced airway immunocompromise and amplified allergic inflammation across respiratory compartments. This dual mechanism sustains a chronic inflammatory milieu via neutrophil, macrophage, and T-lymphocyte recruitment, directly fueling disease progression and multi-organ comorbidity development in OVS.76,77 Clinically, OVS patients exhibit exacerbated immune dysfunction characterized by CD8+ T-cell predominance, CD4+ depletion, and inverted CD4+/CD8+ ratios compared to isolated OSA or COPD cohorts.4 While these findings implicate synergistic immune network disruption in OVS pathobiology, the exact molecular interplay between smoking-induced inflammation, sleep-related hypoxia, and adaptive immune exhaustion remains mechanistically undefined, necessitating further investigation through large-scale cohort studies.
Respiratory Arousal Threshold
The respiratory arousal threshold represents the ventilatory drive required to terminate apneic events during sleep, serving as a key indicator of respiratory effort modulation. Polysomnographic studies demonstrate that patients with OVS exhibiting moderate-to-severe airflow obstruction show significantly lower arousal thresholds than both patients with isolated OSA and OVS patients with mild AFL.78 Consistent findings emerge from research on functional respiratory parameters in OVS. Among 10 consecutively enrolled non-hypercapnic COPD patients, 6 demonstrated elevated loop gain, while 4 (65%) exhibited low arousal thresholds.79 Furthermore, a negative correlation exists between arousal thresholds and functional measures of pulmonary air trapping and static hyperinflation, suggesting pulmonary hyperinflation may mechanistically reduce arousal thresholds.79,80 This phenomenon likely stems from COPD-related thoracic biomechanical alterations where pulmonary hyperinflation distorts the thoracic cage, heightening mechanosensory perception of respiratory effort and consequently lowering arousal thresholds. Simultaneously, it amplifies chemoreflex sensitivity, destabilizing respiratory control. Patients with low arousal thresholds typically experience premature termination of respiratory events, triggering recurrent cortical arousals. This sleep fragmentation prevents sustained slow-wave sleep, further compromising respiratory pattern stability and impeding chemoreflex-mediated restoration of pharyngeal patency during sleep.81 These studies identify a markedly reduced arousal threshold as a key determinant of OVS severity, prompting its recent proposal as a novel clinical metric.82 Standardizing its measurement aims to establish it as a key supplementary component within the OVS diagnostic and therapeutic framework, thereby providing new perspectives for stratifying disease severity and guiding personalized treatment.
Respiratory Drive
Respiratory drive denotes the output intensity of the respiratory center, governing respiratory muscle effort.83 Brainstem interneurons regulate this drive by integrating continuous inputs from chemical, mechanical, behavioral, and emotional stimuli. The respiratory center processes these signals, with the amplitude of its neural output dictating the mechanical strength of respiratory muscles, reflected in tidal volume.84
In pathological conditions including OSA, COPD, and hypoventilation syndromes, hypoxia severity correlates with episode duration and frequency. This hypoxic stimulus activates redox-sensitive neurons within brainstem nuclei, triggering diverse physiological responses.85 During non-rapid eye movement sleep, loss of arousal-dependent descending influence establishes a hypocapnic apneic threshold. This threshold is linked to periodic breathing under conditions of high chemoreflex loop gain. Furthermore, loss of descending arousal influence reduces motor compensatory capacity, thereby increasing upper airway resistance. These impairments in arousal response and associated upper airway dysfunction markedly exacerbate apnea and hypopnea events in patients with kyphosis or thoracic neuromuscular disorders.86
Abnormal central respiratory control amplifies vulnerability to nocturnal respiratory events. COPD patients exhibit worsened nocturnal gas exchange, particularly during rapid eye movement sleep. When compounded by OSA, this impairment progresses to ventilatory failure and acute or chronic respiratory compromise.87 Collectively, these findings underscore that respiratory drive dysfunction is a central mediator of ventilatory instability in OVS patients.
Anatomical Factors
Airway Tissue
The airway functions as the primary conduit for airflow. Anatomical narrowing or obstruction from mucus accumulation or mucosal edema impedes airflow, causing hypopnea or apnea.88,89 OSA patients experience recurrent pharyngeal collapse during sleep,90,91 while COPD primarily involves lower airway pathology where AFL and bronchoconstriction disrupt sleep.92 When coexisting as OVS, these distinct anatomical pathologies interact synergistically,93 significantly increasing total airway resistance and exacerbating clinical symptoms. Upper and lower airway pathologies demonstrate interdependence. Upper airway inflammation may propagate inferiorly, inducing bronchial mucosal irritation and acute bronchospasm that elevates lower airway resistance.94–96 Concurrently, inhaled irritants like cigarette smoke damage lower airway epithelium, impairing ciliary function,97,98 reducing mucociliary clearance, and provoking hyperplasia and hypertrophy of mucus-secreting structures.99,100 This causes pathological mucus hypersecretion and physical obstruction.101,102 Crucially, upper airway pathology triggers distal functional derangements while preexisting lower airway structural damage establishes persistent occlusion substrates, collectively amplifying dysfunction. Lung volume changes exert distinct anatomical effects. In OSA, increased volume during NREM sleep generates caudal tracheal traction, stabilizing the upper airway through reduced pharyngeal compliance.103 In COPD, hyperinflation enhances parenchymal elastic recoil, increasing radial peripharyngeal traction that similarly resists collapse. Though mediated through different biomechanical pathways tracheal traction versus parenchymal recoil mediated tension both mechanisms secondarily improve upper airway stability during sleep.104 In summary, OVS involves airway caliber alterations from pharynx to bronchioles due to intrinsic factors edema, inflammation or extrinsic factors mucus, lung volume changes. These collectively obstruct airflow and compromise ventilation.
Muscle Tissues
Maintaining airway patency requires integrated neuromuscular coordination. In OVS, pathologically elevated upper airway resistance demands compensatory recruitment of pharyngeal dilator muscles, with genioglossus activation being physiologically essential.105 During normal inspiration, genioglossus contraction stabilizes collapsible airway segments against negative intraluminal pressures. When resistance exceeds compensatory thresholds, dilator muscles fail to overcome inspiratory forces. This deficit worsens with sleep-induced neuromuscular dysfunction including attenuated genioglossus responsiveness, impaired compensation, and respiratory control instability, collectively increasing collapse risk.91,106 Thoracic wall musculature such as intercostal and accessory muscles enhances airway stability through caudal traction during elevated lung volume. This action increases longitudinal airway tension and wall stiffness, generating ventral distending forces that maintain patency.107 Respiratory pump muscles including the diaphragm sustain basal ventilation. In COPD, persistent AFL overloads these muscles during sleep, causing progressive contractile dysfunction and fatigue.45 When COPD coexists with OSA, their pathophysiological convergence accelerates nocturnal hypoventilation via interdependent mechanisms where respiratory muscle fatigue reduces tidal volumes, diminished central drive impairs upper airway compensation, and hypercapnia blunts ventilatory responsiveness. These processes establish a self-amplifying cycle of ventilatory failure and accelerated disease progression.87
Pathophysiology
The chronic inflammatory response in COPD is characterized by infiltration of alveolar macrophages, neutrophils, and CD8+ T lymphocytes, accompanied by release of inflammatory mediators that induce lung tissue injury and airway remodeling, manifesting as airway wall fibrosis and luminal narrowing. Oxidative stress amplifies this inflammation and persists after exposure cessation, triggering downstream effects including NF-κB activation, impaired antiprotease defense, DNA damage, and corticosteroid resistance.108 Additionally, activated inflammatory cells release excessive proteases such as neutrophil elastase. When their activity overwhelms endogenous inhibitors like α1-antitrypsin, protease-antiprotease imbalance occurs, leading to alveolar extracellular matrix degradation and emphysema development.109 Alveolar structural destruction further diminishes small airway traction, promoting expiratory collapse. Systemic inflammation in COPD may also exacerbate extrapulmonary comorbidities such as cardiovascular disease. Thus, COPD pathogenesis involves interconnected mechanisms of chronic inflammation, oxidative stress, and protease-antiprotease imbalance.
Similarly, OSA, while originating from localized mechanical upper airway obstruction during sleep, exerts systemic effects through complex pathophysiological cascades. Its core pathophysiology involves recurrent upper airway collapse resulting from combined anatomical narrowing and impaired neuromuscular control. Wakefulness permits compensatory pharyngeal muscle activation to maintain airway patency, but sleep-induced loss of muscle tone renders the airway vulnerable to collapse under negative inspiratory pressure. Unstable respiratory control and abnormal arousal thresholds perpetuate respiratory events, whose termination often involves micro-arousals causing sleep fragmentation and subsequent daytime sleepiness, fatigue, and cognitive impairment.110,111
When COPD and OSA coexist as OVS, they create a clinically more severe condition. COPD remodels local and systemic environments, increasing susceptibility to and severity of OSA, while OSA amplifies COPD-related oxidative stress and inflammation through intermittent hypoxia. This synergistic interaction worsens ventilation and gas exchange, leading to progressive hypoxia that further triggers systemic inflammation, oxidative stress, and sympathetic activation, collectively driving heterogeneous clinical manifestations in OVS patients.
Inflammatory Response
Inflammation significantly contributes to the pathophysiology of OVS. Chronic intermittent hypoxia in OSA patients initiates pathological changes by altering allergen-induced lower airway inflammation and disrupting protease-antiprotease balance, driving lung remodeling characterized by proximal airway fibrosis and peripheral emphysema-like tissue destruction. This structural compromise ultimately causes expiratory flow limitation112 and further compounds pulmonary damage; the resulting cytokine-mediated inflammatory cascade, combined with traction lung injury, accelerates COPD progression.113 Studies confirm that OVS patients demonstrate elevated pro-inflammatory cytokines (CCL11, CD40 ligand) with concurrent reduction in anti-inflammatory cytokines (IL-10).114 Furthermore, significantly increased levels of inflammatory mediators—including TNF-α, IL-8, IL-6, and granulocyte colony-stimulating factor (G-CSF)—are observed in both serum and bronchoalveolar lavage fluid, alongside elevated neutrophil proportions.20,49,53,115 This chronic inflammatory state appears predominantly mediated by the NF-κB signaling pathway, which activates pivotal inflammatory factors during hypoxic conditions.116 Systemic inflammation biomarkers in OVS extend beyond cytokines. C-reactive protein (CRP) demonstrates conflicting patterns across studies. While individuals with OVS and COPD exhibit elevated high-sensitivity CRP (hs-CRP) relative to controls and OSA-only patients,49 other research reveals no significant CRP differences among OSA patients irrespective of COPD comorbidity.117,118 Consequently, these conflicting findings necessitate further studies to clarify CRP’s role in OVS pathogenesis. In contrast to CRP, the anti-inflammatory biomarker soluble receptor for advanced glycosylation end products (sRAGE) shows clinical promise. After adjustment for age, gender, and smoking status, plasma sRAGE levels showed no significant differences between OVS, OSA-only, and COPD-only groups.119 However, following continuous positive airway pressure treatment, sRAGE levels increased significantly in both OSA and OVS patients. This therapeutic response suggests sRAGE’s potential as an inflammatory marker for OVS.119 Collectively, inflammatory cytokines drive OVS pathogenesis through interconnected pathways.
Oxidative Stress
Beyond inflammation, oxidative stress significantly contributes to OVS pathophysiology. This process originates from an imbalance between reactive oxygen species (ROS) production and antioxidant defenses. ROS generation occurs in inflammatory cells (neutrophils, macrophages) and damaged airway epithelial cells activated by hypoxia, inflammation, and metabolic stimuli. Intermittent hypoxia-reoxygenation cycles during apneic events amplify oxidative stress in airway epithelium and pulmonary vascular endothelium. Clinical evidence demonstrates elevated oxidative stress markers in OVS. Patients with combined COPD and OSA exhibit higher exhaled carbon monoxide levels—a recognized oxidative stress biomarker—compared to non-smoking OSA patients.120 Moreover, studies report increased lipid peroxidation and reduced paraoxonase activity in both OSA patients and non-apneic COPD patients with nocturnal desaturation.121 Collectively, these findings associate hypoxia, irrespective of its temporal pattern, with oxidative stress exacerbation in OVS.
Autonomic Nervous System
Complementing these mechanisms, autonomic nervous system (ANS) dysregulation significantly contributes to OVS pathophysiology. Recurrent hypoxia, hypercapnia, and apnea during sleep activate chemoreceptors, triggering compensatory hyperventilation that paradoxically exacerbates tissue oxygen fluctuations.122 This response directly heightens sympathetic tone.123 Heart rate variability analyses reveal distinct ANS alterations in OVS. Compared to isolated COPD or OSA patients, OVS subjects exhibit significantly reduced high-frequency (HF) power (indicating impaired parasympathetic activity) and elevated low-frequency (LF) power (reflecting sympathetic dominance).124,125 A direct correlation between the elevated LF/HF ratio and increased residual volume further suggests lung hyperinflation potentiates sympathetic drive.124 This systemic sympathetic overactivity is corroborated by cross-sectional studies showing greater sympathetic activation during respiratory sinus arrhythmia in COPD-OSA overlap patients than in COPD-alone groups.126 Furthermore, as a neural component of this dysregulation, muscle sympathetic nerve activity is markedly increased in OVS, serving as a compensatory mechanism to maintain blood pressure through elevated systemic vascular resistance.127,128 Collectively, ANS dysfunction critically influences OVS progression, exacerbating functional impairment and adverse cardiometabolic outcomes.129
Thus, inflammatory cascades, oxidative stress, and ANS dysfunction collectively represent shared pathogenic mechanisms in both COPD and OSA.130 These pathways interweave and mutually amplify, forming a self-perpetuating cycle that drives progressive multi-organ dysfunction. However, the traditional theoretical framework centered on inflammation, oxidative stress, and autonomic regulation has proven insufficient to fully explain the complex clinical manifestations of OVS. Research perspectives are gradually shifting toward exploring novel mechanisms underlying the diverse clinical symptoms in affected patients. Endothelial dysfunction serves as a critical bridge connecting pulmonary pathology with cardiovascular comorbidities, driving pathological vascular remodeling.131 Simultaneously, the “gut-lung axis” hypothesis reveals how gut microbiota dysbiosis drives systemic inflammation from a microorganism-host interaction perspective, providing a new dimension for understanding multi-organ damagez.51 These interconnected mechanisms constitute a more profound pathophysiological network. Although most mechanisms remain under investigation, they provide crucial insights for systematically interpreting disease complexity, poor prognosis, and treatment resistance, while also pointing toward future directions for developing targeted therapeutic strategies.
Clinical Outcomes
Hypoxemia and Hypercapnia in OVS Pathophysiology
Ventilatory limitation, driven by both anatomical and non-anatomical factors, leads to impaired gas exchange and hypoxia, primarily manifesting as hypoxemia and hypercapnia. These abnormalities represent one of the most significant sleep-related disturbances in OVS. Under physiological conditions, a mild decrease in the arterial oxygen partial pressure (PaO2) predominantly stimulates peripheral chemoreceptors such as the carotid bodies, whereas an elevation in the arterial carbon dioxide partial pressure (PaCO2) primarily activates central chemoreceptors located in the medulla. Together, they synergistically increase respiratory drive to maintain blood gas homeostasis. However, this compensatory mechanism is frequently disrupted in chronic respiratory diseases.
In COPD, the initial dominant mechanism is ventilation/perfusion (V/Q) mismatch, characterized by small airway disease creating low V/Q regions and emphysema forming high V/Q areas. As alveolar destruction progresses, diffusion impairment becomes increasingly significant. In advanced disease stages, respiratory muscle fatigue and blunted central drive result in alveolar hypoventilation, collectively resulting in persistent and progressive hypoxemia and hypercapnia.132,133 In contrast, OSA is characterized by an intermittent pattern of hypoxemia driven by the repeated collapse of the upper airway during sleep. This collapse causes apnea or hypopnea, leading to a cessation of alveolar ventilation and an absolute shunt effect, which precipitates a rapid decline in blood oxygen levels. This continues until arousal triggered by hypoxia or hypercapnia restores upper airway patency, allowing transient recovery of ventilation and oxygenation. The recurring “obstruction-hypoxia-arousal-recovery” cycle throughout the night produces a characteristic sawtooth pattern in oxygen saturation, accompanied by transient hypercapnia during apneic episodes.7
When COPD and OSA coexist, forming OVS, the resulting pathophysiology is not a simple summation of the two disorders but involves a synergistic amplification. The pre-existing compromise in gas exchange capacity in COPD patients limits their ability to compensate for the recurrent nocturnal episodes of acute hypoxia and hypercapnia characteristic of OSA. A “dual inhibition of ventilatory drive” arises from the combination of OSA-related central chemosensitivity depression134 and the inherently blunted ventilatory drive in advanced COPD. Simultaneously, the sleep-related reduction in FRC in the supine position and during REM sleep further compromises gas exchange on the background of emphysema.135 Together, these factors create a vicious cycle, transforming the nocturnal hypoxemia in OVS from the intermittent pattern seen in pure OSA into a more severe and sustained pattern, evidenced by prolonged periods of SpO2 below 90% and delayed recovery.135–138 Hypercapnia (PaCO2 ≥45 mmHg) also becomes more pronounced and refractory.139,140 These persistently deranged blood gas levels are consequently associated with multisystem clinical comorbidities (Figure 2).
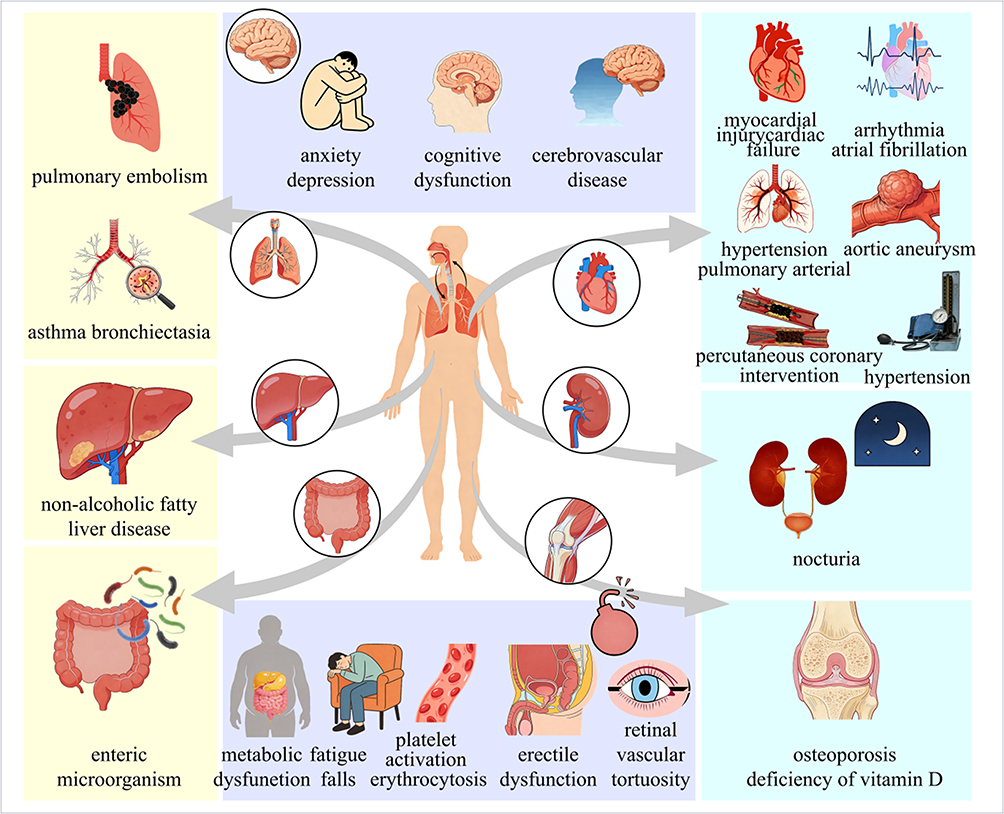 |
Figure 2 Patients with overlap syndrome present with a spectrum of distinct clinical outcomes. |
Cardiovascular Disease
Pulmonary Hypertension
PH is a primary clinical outcome in patients with OVS. These patients consistently exhibit PH manifestations both at rest and during physical exertion,141,142 while also demonstrating an elevated respiratory event index.143 This elevated respiratory event index reflects underlying ventilatory dysfunction including ventilation-perfusion (V/Q) mismatch and reduced diffusing capacity,18,46 indicating severely compromised respiratory mechanics. Regarding PH pathogenesis in OVS, sustained hypoxia likely plays a central role through multiple pathways. More specifically, it may induce prolonged pulmonary arteriolar vasoconstriction or alter ion channel activity in pulmonary vascular smooth muscle cells. Additionally, persistent hypoxia can trigger hypertrophy and proliferation of vascular smooth muscle cells and fibroblasts. These pathological changes culminate in structural remodeling characterized by wall thickening and luminal narrowing, consequently elevating vascular pressure.144 However, further experimental studies are needed to elucidate the underlying mechanisms.
Cardiac Failure
Heart failure represents another major clinical outcome in patients with OVS.145 Compared to patients with COPD or OSA alone, OVS patients demonstrate greater impairment in left ventricular diastolic function and higher risks of developing congestive heart failure and coronary artery disease.146 This correlation is further supported by Prakash Banjade et al.147 Persistent hypoxemia drives right ventricular remodeling,148 significantly elevating the risk of right heart failure.149 Collectively, these mechanisms establish that OVS patients face dual risks of both left-sided and right-sided cardiac failure. Critically, OVS-associated cardiac impairment directly exacerbates sleep-related ventilatory dysfunction. These patients exhibit significantly increased risk of airway narrowing during supine sleep,93 which further compromises ventilation and aggravates hypoxia—establishing a self-perpetuating cycle of cardiopulmonary deterioration. Such evidence underscores the pathological complexity of heart failure in OVS, though further investigation is required to elucidate specific risk factors.
Atherosclerosis
Atherosclerosis demonstrates significantly elevated prevalence in patients with OVS.121 This condition manifests through increased pulse wave velocity and brachial-ankle pulse wave velocity values,19,118 with higher measurements directly indicating greater arterial stiffness and more severe vascular damage.19 Beyond these vascular abnormalities, clinical focus extends to post-revascularization outcomes. Studies establish that OVS patients experience poorer clinical prognosis and reduced quality of life following percutaneous coronary intervention.150 Similarly, OVS patients undergoing coronary artery bypass grafting show significantly higher rates of non-routine discharge, acute kidney injury, and respiratory failure requiring prolonged mechanical ventilation.151 These adverse outcomes may involve OVS-specific oxidative stress mechanisms, such as elevated serum lipid peroxidation and decreased paraoxonase activity,121 which may exacerbate vascular injury and impair tissue recovery. Nevertheless, the precise pathogenic pathways linking these biochemical alterations to clinical manifestations require further investigation.
Cardiac Arrhythmia
Cardiac arrhythmia refers to irregularities in heart rate or rhythm stemming from conduction system abnormalities. In clinical studies, this condition affects 18.5% of patients with OSA, with the risk of tachyarrhythmia rising significantly when OSA coexists with COPD. Notably, COPD itself and bronchodilator use constitute independent risk factors for such rhythm disturbances in this population.152 This aligns with evidence showing that arrhythmia prevalence rises with worsening AFL severity in COPD patients.22 Atrial fibrillation is notably prevalent in OSA patients, with risk escalating upon COPD comorbidity.153 In particular, patients with OSA exhibit AF incidence rates of 21%–24%,154,155 substantially exceeding rates in isolated COPD (10%) and OSA (6%) groups. Those with OVS and AF typically present with advanced age, elevated prevalence of hypertension, cardiac disease, diabetes mellitus, increased hospitalization frequency, and higher mortality. Concurrent deterioration in sleep parameters is observed, including significant prolongation of AHI, arousal index, and percentage of sleep time with oxygen saturation below 90%.155 Hypoxemia burden and comorbidity severity are established as core drivers of AF development in this population,155 potentially mediated by sympathetic overactivation triggered by hypoxia.126 Furthermore, recent studies demonstrate that patients with OVS face a significantly increased risk of new-onset atrial fibrillation, defined as the first ECG- or rhythm-monitoring-confirmed episode irrespective of duration or symptoms. Analysis of a rigorously matched cohort showed OVS patients had a higher lifetime new-onset atrial fibrillation incidence compared to those with OSA or COPD alone. This elevated risk persisted throughout the first five years post-diagnosis. These findings underscore the need for enhanced rhythm monitoring and targeted interventions in OVS management to mitigate arrhythmia risk.156
Myocardial Injury
Ventricular wall stress serves as a fundamental hemodynamic parameter modulating myocardial oxygen demand and ventricular afterload. This mechanical stress initiates compensatory hypertrophy through physiological feedback mechanisms to preserve cardiac homeostasis.157 When such adaptive responses become maladaptive, myocardial injury occurs. This pathological process is biochemically evidenced by elevated levels of specific biomarkers including N-terminal pro-B-type natriuretic peptide, which reflects ventricular wall stress, and high-sensitivity cardiac troponin, indicating cardiomyocyte damage. In patients with OVS, significantly increased high-sensitivity cardiac troponin concentrations (14.2 pg/mL vs 6.5 pg/mL in isolated OSA patients, p < 0.001) and NT- N-terminal pro-B-type natriuretic peptide levels (93.1 pg/mL vs 19.2 pg/mL, p < 0.001) demonstrate subclinical cardiac impairment.158 The persistence of elevated biomarker levels signifies ongoing myocardial injury, thereby increasing CVD risk. Consequently, integrating cardiac biomarker assessment with evaluation of ventricular wall stress provides essential insights into early cardiac remodeling processes in OVS patients.
Aortic Aneurysm
Aortic aneurysm, characterized by localized or diffuse dilation of the aortic wall, may compress adjacent organs and progressively expand over time. Complications such as rupture or dissection can lead to catastrophic outcomes. A cohort study investigating the association between OVS and aortic aneurysm risk employed a 1:4 propensity score matching strategy based on key baseline characteristics. After several years of follow-up in 31274 patients with OSA, the analysis revealed no significant difference in cumulative aortic aneurysm risk between the matched cohorts with and without OSA. Multivariable risk assessment confirmed that OSA itself was not an independent risk factor. Instead, significant risk factors identified within the OSA population included male sex, advanced age, diabetes mellitus, COPD, and coronary artery disease. Notably, the subgroup of OSA patients with comorbid COPD exhibited a significantly higher aneurysm risk compared to matched non-OSA controls.159 These findings position aortic aneurysm as an independent cardiovascular risk specifically in the OVS population, warranting vigilant monitoring despite the overall null association with OSA alone.
Hypertension
Based on current evidence, OVS demonstrates a significant association with hypertension. Studies consistently show markedly elevated hypertension prevalence in OVS patients compared to those with either COPD or OSA alone. A clinical investigation comprising 968 subjects revealed substantially higher hypertension rates in the OVS group relative to COPD-only patients. Furthermore, hypertension prevalence exhibited a positive correlation with OSA severity among COPD patients, with OSA confirmed as an independent risk factor for hypertension.22 These observations are reinforced by a meta-analysis of 17 studies, which confirmed significantly increased hypertension risks in OVS patients versus COPD-only (OR 1.94, 95% CI 1.49–2.52) and OSA-only groups (OR 2.05, 95% CI 1.57–2.68). Collectively, these findings substantiate the consistent relationship between OVS and heightened hypertension risk, underscoring the importance of intensified blood pressure monitoring and management strategies in this patient population to mitigate cardiovascular complications.160
Accumulating evidence from literature reviews indicates that patients with OVS frequently experience cardiovascular comorbidities including heart failure, arrhythmias, and PH. Nevertheless, despite extensive investigation of cardiovascular manifestations in this population, significant knowledge gaps persist regarding specific cardiovascular entities such as aortic aneurysm pathogenesis, clinical outcomes following coronary revascularization, patterns of subclinical myocardial injury, and ventricular wall stress dynamics. The current scarcity of dedicated studies examining these cardiovascular aspects in OVS underscores the imperative for rigorously designed research to elucidate their pathophysiological relationships with this complex syndrome.
Respiratory System
COPD manifests as two distinct airway remodeling phenotypes: intrathoracic tracheal stenosis and tracheal dilatation.161 The interplay between these COPD phenotypes and OSA yields divergent clinical outcomes. Chronic bronchitis drives persistent inflammation-mediated pathological changes—including tissue congestion, edema, mucus hypersecretion, and adipose deposition—that collectively exacerbate airway obstruction. This AFL intensifies nocturnal respiratory compromise, explaining why chronic bronchitis patients with peripheral edema and elevated BMI exhibit heightened OSA susceptibility.162 In contrast, the emphysema phenotype demonstrates relative protection against OSA progression. Lung hyperinflation characteristic of emphysema, frequently associated with lower BMI, enhances upper airway stability through critical closing pressure reduction during sleep.163,164 This protective mechanism operates via increased tracheal traction forces that mitigate pharyngeal collapsibility. These phenotype-specific relationships highlight the imperative for stratified analyses to decode pathophysiological interactions within OVS.
Bronchiectasis
Bronchiectasis, a chronic inflammatory disorder characterized by purulent inflammation, fibrosis, and destruction of bronchial walls and surrounding lung parenchyma, results in irreversible bronchial dilation and distortion. Crucially, patients with COPD-OSA OVS demonstrated a significantly higher prevalence of bronchiectasis (42.86%, 30/70) compared to COPD patients without OSA (18.52%, 10/54) identified by PSG. Moreover, this COPD-OSA group exhibited a more severe disease profile, including significantly elevated AHI, increased time with nocturnal oxygen saturation below 90%, higher CRP levels, and lower CD4/CD8 ratios. Focusing specifically on the COPD-OSA patients with bronchiectasis, correlation analysis revealed significant associations between the severity of their bronchiectasis (Bhalla score), its anatomical extent (Smith score), CD8+T-cell counts, and CD4/CD8 ratios. These immunological associations suggest that CD8+ T-cells and CD4/CD8 imbalance likely contribute to the pathophysiology driving bronchiectasis development and progression within the OVS. Collectively, these findings indicate that OVS patients who develop bronchiectasis experience more severe respiratory compromise, nocturnal oxygen desaturation, systemic inflammation, and immune imbalance compared to those without OSA.27
Pulmonary Embolism
Pulmonary embolism, characterized by thrombotic obstruction of pulmonary arteries causing perfusion deficits, exhibits elevated incidence in OVS. Epidemiological data identify male sex and age >58 years as independent risk factors for PE in this population.165 Notably, inhaled glucocorticoid therapy (utilized by 83.7% of OVS patients versus 69.4% of COPD-only patients in clinical cohorts) constitutes an additional modifiable risk factor,166 consistent with established mechanisms of glucocorticoid-induced hypercoagulability.167 This confluence of demographic and iatrogenic risk factors underscores the necessity for heightened clinical vigilance regarding PE in OVS patients. Prospective studies are required to validate these associations and optimize risk stratification protocols.
Lung Transplantation
Lung transplantation serves as a definitive intervention for end-stage respiratory diseases including COPD, idiopathic pulmonary fibrosis, and cystic fibrosis. A cross-sectional PSG analysis of 77 clinically stable transplant recipients demonstrated a substantial prevalence of OSA, affecting 61% of patients transplanted for COPD and 52% for idiopathic pulmonary fibrosis. Crucially, pre-transplant COPD emerged as an independent predictor of post-transplant OSA development (adjusted OR 3.21, 95% CI 1.78–5.92).168 These findings establish a significant association between pre-transplant pulmonary pathology and post-transplant OSA. Future research must prioritize elucidating the bidirectional pathophysiological interplay between OSA and pre-transplant COPD in lung transplant recipients, particularly its impact on graft survival, acute rejection incidence, and long-term patient mortality.
Neurological/Psychiatric Disorders
Cerebrovascular Disease
Patients with OVS exhibit a significantly elevated risk of vascular events, including ischemic stroke. Carotid atherosclerotic plaque represents an established biomarker for stroke risk stratification in this population.169 Notably, 79% of OVS patients develop atherosclerotic plaques within the left carotid artery, demonstrating significantly higher mean plaque volumes compared to COPD patients without OSA. Multivariate analysis identifies age, current smoking status, and the AHI as independent predictors of left carotid atherosclerosis in COPD patients. In contrast, neither plaque prevalence nor volume differs significantly in the right carotid artery between groups. This anatomical asymmetry underscores the specific clinical relevance of left carotid plaque assessment as a marker for stroke risk in OVS patients.170 Mechanistically, severe stenosis or occlusion of the common carotid artery likely compromises cerebral perfusion, potentially triggering cerebrovascular events such as stroke. Collectively, these findings establish OVS as a significant cerebrovascular risk entity, necessitating heightened clinical vigilance through routine carotid monitoring and targeted research into plaque weakness mechanisms.
Cognitive Disorder
Hypoxemia and hypercapnia directly impair the central nervous system in patients with OVS, leading to widespread cognitive deficits encompassing attention, memory, executive function, and language abilities.171–174 Cross-sectional studies confirm the prevalence of this impairment, demonstrating that mild cognitive impairment (MCI) occurs in 40.6% to 78% of OVS patients. Furthermore, Luels et al specifically noted significant slowing in processing speed, a key aspect of executive function, within this patient population.175 Critically, patients with OVS face a higher risk of dementia compared to those with COPD alone. Evidence supporting this risk difference comes from subgroup analysis. Among COPD patients, those with moderate-to-severe OSA (AHI ≥30 events/hour) exhibit significantly lower Mini-Mental State Examination (MMSE) scores than those with no or mild OSA (AHI <15 events/hour).176 This clearly demonstrates an inverse correlation between OSA severity (measured by AHI) and the degree of cognitive decline (measured by MMSE score), further reinforcing OSA as a key factor exacerbating cognitive impairment and dementia risk in OVS.
Multiple studies suggest this association may relate to the hypoxic state in OVS. For instance, neuropsychological testing indicates that patients with OSA exhibit cognitive deficits similar to those with COPD on tasks sensitive to hypoxia and sleep disruption.174 OSA severity, measured by the ODI, is an independent risk factor for MCI in COPD, particularly during REM sleep. The time spent with oxygen saturation below 90% (T<90%) may serve as an indicator of hypoxia-related cognitive impairment.177,178 These studies collectively highlight the significant role of hypoxia in OVS. However, further studies are warranted to elucidate the specific impact of OSA on cognitive domains in COPD patients with OVS and to determine the therapeutic implications.
Anxious Depression
Beyond cognitive deficits, patients with OVS demonstrate an elevated risk of anxiety, depression, or psychiatric conditions. Reported prevalence rates reach 54% for depression and 77% for anxiety within the OVS population. Independent risk factors for depression include chest pain, higher COPD Assessment Test scores, and the presence of OVS itself.179 Comparative studies in Korean populations indicate that the prevalence of anxiety and depression is approximately 2.5 times higher among individuals with COPD-OSA overlap compared to those with COPD alone.175 A documented case report described recurrent mental and behavioral alterations over six months in a male patient with no prior psychiatric history but concurrently diagnosed with COPD and OSA. Blood gas analysis suggested that the patient likely experienced hypoxemia and hypercapnia, potentially contributing to his acute manic episodes and other clinical manifestations.180 Notably, some researchers propose that fatigue symptoms appear more prominent than drowsiness, anxiety, or depression in OVS patients and the impairment persisted after 3 months of CPAP treatment.181 Given these complex and potentially distinct presentations, the characteristics and underlying mechanisms of anxiety and depression in OVS remain incompletely understood and merit further investigation.
Metabolic Disease
Metabolic dysfunction is highly prevalent in OVS, with bidirectional pathophysiological interactions observed between diabetes and respiratory impairment. While diabetes independently damages pulmonary structure and function,182 coexisting COPD and OSA substantially elevates type 2 diabetes (T2D) risk in specific subpopulations. A retrospective analysis of 1939 patients demonstrated significant age- and sex-stratified associations between OVS and T2D risk. Specifically, OVS conferred an 8.45-fold increased T2D risk in patients aged <58 years (95% CI 1.46–65.90; P=0.018) and a 4.39-fold increase in female patients (95% CI 1.04–22.50; P=0.044). No significant association was observed in males or patients aged ≥58 years.183 Despite this risk stratification, conclusive evidence demonstrating that OVS treatment reduces incident metabolic disorders or prevents diabetic complications remains lacking.183 Furthermore, metabolic syndrome affects 38% of OVS patients, with abdominal obesity universally present in the studied cohort, representing its most consistent manifestation.184 Contributing metabolic factors include advanced age, elevated BMI, increased bedtime systolic pressure, and recumbent angiotensin II levels, aligning with cross-sectional epidemiological data.20 Collectively, diabetes-induced pulmonary damage and OVS-driven T2D risk establish a bidirectional pathophysiological link between metabolic and respiratory dysfunction, forming a self-perpetuating cycle that requires targeted interventions.
Other Related Diseases
Beyond its established associations with cardiovascular, respiratory, and metabolic disorders, OVS demonstrates significant links to additional systemic comorbidities. A comprehensive literature review confirms non-alcoholic fatty liver disease (NAFLD), nocturia, and secondary erythrocytosis as clinically relevant manifestations.
NAFLD
The pathogenesis of NAFLD in patients with OSA and COPD is primarily mediated by the overactivation of inflammatory and oxidative pathways.185,186 Hepatic steatosis represents the hallmark manifestation, with a meta-analysis of 2120 OSA patients showing a prevalence of approximately 75%.187 The risk of steatosis increases with coexisting COPD, an AHI >5 events/hour, a BMI >26 kg/m2, and advanced age. This risk becomes particularly elevated when an AHI >30 events/hour coincides with stage 1 COPD.187 Elevated AHI values indicate a greater apnea-hypopnea burden, and the coexistence of OSA and COPD exacerbates hypoventilation severity. This pathophysiological synergy worsens hypoxemia and systemic inflammation, substantially amplifying the risk of steatosis through the potentiation of disease severity. Consequently, clinical monitoring of lipid metabolism is recommended for these patients.
Nocturia
Nocturia is notably prevalent and clinically significant in OVS. A cross-sectional study of 2098 patients revealed that 63.5% of individuals with OVS exhibited nocturia, significantly higher than the 58.0% prevalence in OSA patients (p<0.01).47 Nocturia incidence correlates with OSA severity, particularly among patients with comorbid COPD, diabetes, or hypertension,188 and significantly compromises sleep quality.189 In OVS, nocturnal airway obstruction and oxygen desaturation may induce blood gas alterations (eg, hypercapnia or hypoxia), thereby modifying renal perfusion. This process triggers vasoactive system activation, promoting renal vasoconstriction and subsequent increased urine production.190 However, the precise pathophysiological link between OVS and nocturia remains unclear.
Platelet Activation and Erythrocytosis
Emerging evidence indicates platelet activation in OSA and COPD patients, prompting our evaluation of mean platelet volume (MPV) and platelet distribution width (PDW) in OVS patients. Analysis of 485 patients undergoing PSG and pulmonary function testing revealed significantly elevated MPV in OVS patients (10.7 ± 1.0 fL) versus both controls (10.0 ± 0.9 fL; P<0.001) and OSA patients (10.3 ± 1.2 fL; P=0.002), demonstrating stepwise MPV elevation across disease severity strata. Similarly, PDW was higher in OVS (13.8 ± 2.3 fL; P=0.008) and OSA groups (13.6 ± 1.9 fL; P=0.007) compared to controls (12.9 ± 2.0 fL).191 Concurrently, chronic hypoxic stimulation in OVS drives compensatory erythropoiesis, manifesting as higher erythrocytosis prevalence than COPD alone.192 This risk is independently predicted by nocturnal hypoxemia severity (percentage of sleep time with SaO2<90%), with significantly increased erythrocytosis in OSA patients with GOLD 1–2 COPD versus GOLD 3–4 patients (P<0.05)193 - a discrepancy potentially attributable to age, nutritional status, and long-term oxygen therapy effects on hematopoiesis in advanced COPD. Critically, both hematological perturbations - platelet activation indicated by MPV/PDW elevation and hypoxia-induced erythrocytosis - are mitigated by oxygen supplementation,194 collectively demonstrating that respiratory dysfunction represents the primary driver of hematological abnormalities in OVS, warranting targeted oxygen therapy to attenuate these complications.
Fatigue and Exercise Impairment
Fatigue represents a more prevalent symptom than anxiety or depression in OVS patients, with limited treatment efficacy observed.181 Notably, comorbid OSA and COPD correlate with significantly reduced mean oxygen saturation, increased daytime hypoxemia, and impaired exercise tolerance. These patients demonstrate pronounced exercise limitations and exercise-induced desaturation.195 Objective exercise capacity metrics reveal critical associations: The 6-minute walk distance (6MWD) shows positive correlations with AHI, ODI, nocturnal SpO2, resting PaO2, and mean exercise SpO2. Conversely, 6MWD exhibits negative correlations with duration of nocturnal SpO2 <90%, mean nocturnal desaturation, and arterial PaCO2 (p<0.001).195 This evidence collectively indicates that OSA-COPD comorbidity substantially reduces physical capacity. Mechanistic studies further demonstrate that OVS patients exhibit elevated inflammatory markers (including CRP and IL-6) and engage in significantly reduced daily physical activity—averaging 672 fewer steps than COPD-only patients. Critically, every 1000-step reduction in daily activity associates with a 0.875 ng/mL increase in IL-6 levels.196 These findings implicate systemic inflammation as a key contributor to motor dysfunction in OVS, underscoring the necessity for comprehensive exercise capacity assessment and therapeutic management in this population.
Given the central role of exercise intolerance in OVS, interventions aimed at improving physical capacity are of paramount importance. A prospective randomized controlled single-blind trial demonstrated that in OVS patients adhering to positive airway pressure therapy, the addition of moderate-intensity aerobic exercise for 20 weeks led to significant improvements in 6MWD, Barthel index, and modified Medical Research Council score compared to controls (p < 0.05), alongside improvements in body composition and nocturnal oxygenation.197 Complementing this long-term exercise approach, another study found that even short-term CPAP therapy (two nights) could enhance walking capacity in OVS patients, with incremental shuttle walk distance increasing significantly from 226.4 ± 95.3 m to 288.6 ± 94 m (p < 0.05).197 Collectively, these studies validate that combining positive airway pressure with structured physical activity-whether as a sustained rehabilitation program or as a facilitator of initial improvement-constitutes an effective strategy for mitigating motor dysfunction in OVS.
Enteric Microorganism
The bidirectional lung-gut axis plays a significant role in respiratory diseases, with evidence demonstrating that fecal microbial transfer (FMT) attenuates inflammation, alveolar destruction, and lung function impairment in COPD.198 Clinical studies and animal models indicate that smoking-induced COPD and pulmonary inflammation subsequently drive gut dysbiosis. Interventions targeting microbial restoration – including probiotics, prebiotics, short-chain fatty acids (SCFAs), and FMT – show therapeutic potential for COPD through gut microbiota modulation.199 Parallel mechanisms exist in OSA, where apnea/hypopnea-induced hypoxia correlates with specific alterations in gut microbiota composition and function.200 This pathophysiological overlap suggests that probiotic administration, SCFA supplementation, and FMT may constitute promising therapeutic approaches for OSA.201 Collectively, current evidence indicates that prebiotics, probiotics, SCFAs, and FMT could ameliorate intestinal dysbiosis resulting from shared COPD-OSA pathogenesis. These interventions likely exert beneficial effects by enhancing intestinal barrier integrity and stimulating production of immunomodulatory metabolites, thereby alleviating systemic pathophysiology. However, robust clinical validation of these mechanisms remains limited.
Vitamin D Deficiency and Osteoporosis
Vitamin D, a fat-soluble vitamin essential for bone integrity, neuromuscular function, and immune regulation, demonstrates anti-inflammatory and immunomodulatory properties.202–204 Patients with OVS exhibit significantly lower serum 25-hydroxyvitamin D [25(OH)D] levels compared to those with OSA and non-apneic controls. Both the AHI and FEV1 independently predict 25(OH)D concentrations, with OVS patients displaying the most severe vitamin D deficiency at higher AHI and lower FEV1 values.205 This metabolic disturbance impairs calcium homeostasis, directly compromising bone mineralization and contributing to osteoporosis development—a pathological trajectory particularly relevant to OVS patients. Animal models provide mechanistic insights into OVS-related bone loss. OVS-exposed rats exhibit greater bone volume percentage than smoke-exposed controls but reduced trabecular and cortical thickness compared to intermittent hypoxia groups. Concurrent elevations in IL-6 and TNF-α levels suggest that synergistic inflammatory pathways in OVS may independently exacerbate bone microarchitectural damage.5
Clinically, correcting nocturnal hypoxia through CPAP therapy appears to ameliorate vitamin D deficiency in OVS. A one-year clinical study demonstrated that CPAP treatment significantly increased serum vitamin D levels in OVS patients from 21.3±8.4 ng/mL to 23.8±8.7 ng/mL (p=0.001), with adherent patients achieving higher levels (25.8±7.6 ng/mL) than those with poor adherence (20.4±9.6 ng/mL, p=0.038).206 While these preclinical and clinical findings highlight potential inflammatory and therapeutic mechanisms, comprehensive models of bone disease pathophysiology in OVS require further human studies that integrate the interplay between nutritional status (such as vitamin D levels), systemic inflammation, and the effects of therapeutic interventions.
Postural Control
Postural control, defined as the ability to maintain functional stability during both static and dynamic tasks,207 is frequently impaired in patients with COPD, contributing to their elevated fall risk.208 Emerging evidence suggests a bidirectional relationship between respiratory disorders and balance control, as impaired daytime postural stability may exacerbate sleep disordered breathing while OSA itself can disrupt balance through multiple physiological pathways including vestibular system, visual acuity and cognitive function.209,210 A clinical investigation examining this interaction enrolled 70 patients with moderate-to-severe COPD, revealing that those with comorbid moderate-to-severe OSA demonstrated significantly impaired postural stability on objective force platform assessment. These patients exhibited increased postural sway with compensatory rapid adjustments and experienced more recurrent falls during follow-up. Interestingly, these objective balance deficits were not reflected in standard clinical balance scales, physical activity levels, or psychological assessments.211 These findings establish moderate-to-severe OSA as an independent risk factor for balance impairment and increased fall risk in COPD patients, while highlighting the dissociation between laboratory-measured postural control and conventional clinical metrics. This underscores the necessity of incorporating objective balance assessment and OSA management into the comprehensive care of OVS patients. Systematic screening and treatment of sleep-disordered breathing may represent a crucial strategy for reducing fall risk and preserving functional independence in this vulnerable population.
Erectile Dysfunction
Our review identifies a male predominance among patients with OVS. A study conducted in male OVS patients with erectile dysfunction (ED) demonstrated that after six months of standardized respiratory therapy (continuous positive airway pressure combined with bronchodilators), although overall erectile function scores showed significant improvement, only one-quarter of patients met the clinical threshold for meaningful improvement (defined as an increase of ≥5 points in ED intensity scores). It is noteworthy that among those who achieved therapeutic benefit, one-third remained dissatisfied with the degree of improvement. The extent of ED improvement was positively correlated with patient age and the AHI, and negatively correlated with the duration of ED. These findings suggest that while respiratory therapy can partially ameliorate erectile function in OVS patients, adjunctive targeted ED treatment is necessary to achieve satisfactory outcomes for the majority of individuals.212
Retinal Vascular Tortuosity
Retinal vascular tortuosity represents a compensatory structural adaptation to chronic hypoxic conditions. In a comparative study evaluating retinal vascular morphology across patients with OVS, OSA alone, COPD alone, and healthy controls (15 subjects per group, total n=60), OVS patients demonstrated the most pronounced degree of retinal vascular tortuosity. The tortuosity severity exhibited a significant negative correlation with partial pressure of oxygen (PO2) and oxygen saturation, while showing positive correlations with partial pressure of carbon dioxide (PCO2), AHI, and ODI. This pathological alteration likely originates from the distinctive dual hypoxia mechanism characteristic of OVS, where persistent hypoxia from COPD synergistically interacts with intermittent hypoxia induced by OSA, compounded by concomitant systemic inflammatory responses and hemodynamic abnormalities collectively affecting the microvascular system. These findings suggest that retinal vascular assessment could represent a potential non-invasive biomarker for detecting systemic microvascular impairment in OVS patients.213
Discussion
Current epidemiological studies reveal significant variations in the reported prevalence of the OVS between COPD and OSA, necessitating critical examination from multiple perspectives. Although OVS has been documented in general populations, OSA patients, and COPD cohorts, with incidence rates reaching up to 58% even among asymptomatic OSA patients, particularly in overweight or obese subgroups.37 Yet, these substantial fluctuations across studies indicate marked heterogeneity and instability in available evidence. These discrepancies primarily stem from inconsistent OVS definitions, variations in sample inclusion criteria and sizes, and the fact that many studies were not primarily designed to assess incidence, thereby introducing notable classification biases and methodological heterogeneity.
It should be emphasized that OVS should not be simply regarded as the coexistence of two diseases, but rather as a unique clinical phenotype characterized by bidirectional pathological amplification. This essential distinction demands more refined epidemiological frameworks. Currently, most studies lack standardized diagnostic criteria, often rely on limited sample sizes vulnerable to selection bias, and fail to systematically incorporate essential assessments such as pulmonary function testing. Given that some COPD patients may present with atypical symptoms while OSA patients rarely undergo routine pulmonary function evaluation, these diagnostic limitations further constrain the accuracy of prevalence estimates. Consequently, current understanding of OVS epidemiology is marked by significant “post-test uncertainty”, highlighting the urgent need for large-scale, multicenter, prospective studies employing standardized diagnostic protocols to address these limitations.
Beyond epidemiological challenges, the pathophysiological investigation of OVS confronts several critical questions. The interplay of hypoxia-induced sympathetic activation, systemic inflammation, and oxidative stress collectively underpins multi-organ damage, with these mechanisms likely acting synergistically to drive complications across various organ systems. Clinically, OVS exhibits substantial multi-system involvement. It is not only strongly associated with cardiovascular disorders, such as heart failure, arrhythmias, and PH, but also exerts effects on the respiratory system that extend beyond the simple additive burden of COPD and OSA. These include an elevated risk of PE, accelerated progression of bronchiectasis, and poorer outcomes following lung transplantation. Notably, current research on OVS clinical outcomes is unevenly distributed across organ systems. Although cardiovascular complications have been relatively well characterized, investigations into other systemic comorbidities remain limited. For example, the pathophysiological basis of frequent clinical manifestations such as nocturia, secondary polycythemia, and ED remains inadequately elucidated. Compounding this, a substantial knowledge gap exists regarding the management of these manifestations. Such limitations in evidence directly impede a comprehensive assessment and effective management of systemic risks in OVS patients.
From the perspective of evidence quality, current research predominantly relies on cross-sectional surveys and retrospective cohort analyses, while prospective studies and randomized controlled trials remain clearly insufficient. This methodological imbalance limits most findings to associative relationships, making it difficult to establish robust causal inferences. Moreover, the depth and scope of mechanistic investigations are still inadequate. Critical scientific questions concerning the interactions between COPD and OSA at molecular and cellular levels, such as the specificity of shared inflammatory pathways and epigenetic regulatory networks, have not yet been systematically addressed. In light of these evidence gaps, future research should prioritize elucidating OVS-specific molecular mechanisms and validating targeted therapies through innovative clinical trial designs. More specifically, efforts are needed to clarify the distinct biological pathways responsible for different organ injuries. In parallel, interventions targeting key pathological processes in OVS should be developed, and the synergistic potential of existing treatment strategies for multi-organ protection ought to be further optimized.
Future Research Perspective
With advances in multi-omics technologies,214 organoid models,215 and artificial intelligence analytical methods,214 we anticipate achieving more systematic understanding of OVS pathophysiology in the future. However, this will require interdisciplinary collaboration and well-designed studies. By establishing multidimensional biomarker integration systems, conducting in-depth analyses of clinical phenotypes, and implementing biomarker-based clinical trial designs, we can advance OVS management from symptomatic treatment to targeted therapy addressing underlying causes, ultimately opening new avenues for precise prevention and control of this disease.
Limitation
While providing a comprehensive overview of current OVS research, we must acknowledge the methodological limitations of this review. Our analysis primarily incorporated research literature from the past decade. Since methodological standards and diagnostic tools used in earlier studies differ substantially from contemporary approaches, many historically valuable findings may not have been included in our analysis. Although this temporal limitation helps ensure methodological comparability among included studies, it may inevitably omit some important early mechanistic explorations and clinical observations, potentially affecting our complete understanding of the disease trajectory.
Strength
A key strength of this article lies in its comprehensive synthesis of both epidemiological and pathophysiological aspects of OVS. Building on this foundation, the work provides a detailed characterization of cardiovascular and pulmonary complications, while also giving due attention to less widely recognized extra-pulmonary manifestations. These include not only classic examples such as cognitive impairment, NAFLD, and nocturia, but also less frequently discussed sequelae like secondary polycythemia, osteoporosis, ED, and retinal vessel tortuosity. This broad scope underscores that OVS not only confers significant intrinsic risk but also exerts multi-system adverse effects, thereby highlighting the importance of a holistic approach to disease management.
Conclusion
In summary, epidemiological data reveal significant heterogeneity in the prevalence of OVS across different populations, largely attributable to inconsistent diagnostic criteria and assessment methods. Clinically, OVS is associated with systemic comorbidities that extend beyond the well-recognized cardiovascular manifestations, significantly impacting patients’ quality of life and prognosis. However, research in this area remains limited. There is an urgent need to adopt a systems biology perspective and establish a mechanism-oriented framework supported by multi-omics approaches. By integrating existing evidence and identifying critical knowledge gaps, we may ultimately address these unresolved clinical challenges.
Abbreviations
OSA, obstructive sleep apnea; COPD, chronic obstructive pulmonary disease; OVS, overlap syndrome; AFL, airflow limitation; PSG, polysomnography; FRC, functional residual capacity; CRP, c-reactive protein; sRAGE, soluble receptor for advanced glycosylation end products; ROS, reactive oxygen species; ANS, autonomic nervous system; HF, high-frequency; LF, low-frequency; PaO2, oxygen partial pressure; PaCO2, carbon dioxide partial pressure; PH, pulmonary hypertension; V/Q, ventilation-perfusion; AHI, apnea-hypopnea index; MMSE, Mini-Mental State Examination; ODI, oxygen desaturation index; BMI, body mass index; T2D, type 2 diabetes; NAFLD, non-alcoholic fatty liver disease; MPV, mean platelet volume; PDW, platelet distribution width; 6MWD, 6-minute walk distance; FMT, fecal microbial transfer; SCFAs, short-chain fatty acids; ED, erectile dysfunction.
Data Sharing Statement
Due to its nature as a review article, all references are published articles.
Funding
This work was supported by the Jilin Provincial Science and Technology Development Plan (Grant No. 20230203189SF).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Flenley DC. Sleep in chronic obstructive lung disease. Clin Chest Med. 1985;6(4):651–661. doi:10.1016/S0272-5231(21)00402-0
2. D’Cruz RF, Murphy PB, Kaltsakas G. Sleep disordered breathing and chronic obstructive pulmonary disease: a narrative review on classification, pathophysiology and clinical outcomes. J Thorac Dis. 2020;12(Suppl 2):S202–S216. doi:10.21037/jtd-cus-2020-006
3. Liu D, Wang Z, Zhuang Y, et al. Chronic breathlessness in obstructive sleep apnea and the use of lymphocyte parameters to identify overlap syndrome among patients. J Clin Med. 2023;12(3):936. doi:10.3390/jcm12030936
4. Wang J, Li X, Hou WJ, Dong LX, Cao J. Endothelial function and T-lymphocyte subsets in patients with overlap syndrome of chronic obstructive pulmonary disease and obstructive sleep apnea. Chin Med J. 2019;132(14):1654–1659. doi:10.1097/CM9.0000000000000312
5. Zhuang Y, Yan Y, Yang X, Cao J. Osteoporosis in a rat model co-exposed to cigarette smoke and intermittent hypoxia. Int J Chron Obstruct Pulmon Dis. 2020;15:2817–2825. doi:10.2147/COPD.S276913
6. de Oca MM, Perez-Padilla R, Celli B, et al. The global burden of COPD: epidemiology and effect of prevention strategies. Lancet Respir Med. 2025;13(8):709–724. doi:10.1016/S2213-2600(24)00339-4
7. Lv R, Liu X, Zhang Y, et al. Pathophysiological mechanisms and therapeutic approaches in obstructive sleep apnea syndrome. Signal Transduct Target Ther. 2023;8(1):218. doi:10.1038/s41392-023-01496-3
8. Abdelghani A, Benzarti W, Ben salem H, et al. Adherence to treatment with continuous positive airway pressure in the obstructive sleep apnea syndrome. Tunis Med. 2016;94(8–9):551–562.
9. Venkateswaran S, Tee A. Overlap syndrome between chronic obstructive pulmonary disease and obstructive sleep apnoea in a Southeast Asian teaching hospital. Singapore Med J. 2014;55(9):488–492. doi:10.11622/smedj.2014117
10. Choi K-M, Thomas RJ, Kim J, Lee SK, Yoon DW, Shin C. Overlap syndrome of COPD and OSA in Koreans. Medicine. 2017;96(27):e7241. doi:10.1097/MD.0000000000007241
11. Spicuzza L, Campisi R, Crimi C, Frasca E, Crimi N. Prevalence and determinants of co-morbidities in patients with obstructive apnea and chronic obstructive pulmonary disease. Eur J Intern Med. 2019;69:e15–e16. doi:10.1016/j.ejim.2019.08.020
12. Kendzerska T, Leung RS, Aaron SD, Ayas N, Sandoz JS, Gershon AS. Cardiovascular outcomes and all-cause mortality in patients with obstructive sleep apnea and chronic obstructive pulmonary disease (overlap syndrome). Ann Am Thoracic Society. 2019;16(1):71–81. doi:10.1513/AnnalsATS.201802-136OC
13. Mohammad OI, Elgazzar AG, Mahfouz SM, Elnaggar ME. Prevalence of obstructive sleep apnea among patients with chronic obstructive pulmonary disease. Egypt J Bronchol. 2021;15(1):46. doi:10.1186/s43168-021-00093-8
14. Azuma M, Chin K, Yoshimura C, et al. Associations among chronic obstructive pulmonary disease and sleep-disordered breathing in an urban male working population in Japan. Respiration. 2014;88(3):234–243. doi:10.1159/000366064
15. Nattusami L, Hadda V, Khilnani GC, et al. Co-existing obstructive sleep apnea among patients with chronic obstructive pulmonary disease. Lung India. 2021;38(1):12–17. doi:10.4103/lungindia.lungindia_169_20
16. Sridhara VSHK, Acharya V. Comorbidities of chronic obstructive pulmonary disease and their affect on hospitalization of patients in a tertiary care hospital. J Community Hosp Intern Med Perspect. 2021;11(1):120–123. doi:10.1080/20009666.2020.1843823
17. Almagro P, Soler-Cataluña JJ, Huerta A, González-Segura D, Cosío BG. CLAVE Study Investigators. Impact of comorbidities in COPD clinical control criteria. The CLAVE study. BMC Pulm Med. 2024;24(1):6. doi:10.1186/s12890-023-02758-0
18. Sun WL, Wang JL, Jia GH, et al. Impact of obstructive sleep apnea on pulmonary hypertension in patients with chronic obstructive pulmonary disease. Chin Med J. 2019;132(11):1272–1282. doi:10.1097/CM9.0000000000000247
19. Clímaco DCS, Lustosa TC, de FP MV, et al. Is obstructive sleep apnea associated with increased arterial stiffness in patients with COPD? Sleep Breath. 2023;27(2):765–770. doi:10.1007/s11325-022-02635-w
20. Zhou W, Li CL, Cao J, Feng J. Metabolic syndrome prevalence in patients with obstructive sleep apnea syndrome and chronic obstructive pulmonary disease: relationship with systemic inflammation. Clin Respir J. 2020;14(12):1159–1165. doi:10.1111/crj.13253
21. Matsumoto T, Murase K, Tachikawa R, et al. Microalbuminuria in patients with obstructive sleep apnea-chronic obstructive pulmonary disease overlap syndrome. Ann Am Thorac Soc. 2016;13(6):917–925. doi:10.1513/AnnalsATS.201510-655OC
22. Hu W, Zhao Z, Wu B, et al. Obstructive sleep apnea increases the prevalence of hypertension in patients with chronic obstructive disease. COPD. 2020;17(5):523–532. doi:10.1080/15412555.2020.1815688
23. Hang LW, Hsu JY, Chang CJ, et al. Predictive factors warrant screening for obstructive sleep apnea in COPD: a Taiwan national survey. Int J Chron Obstruct Pulmon Dis. 2016;11:665–673. doi:10.2147/COPD.S96504
24. Steveling EH, Clarenbach CF, Miedinger D, et al. Predictors of the overlap syndrome and its association with comorbidities in patients with chronic obstructive pulmonary disease. Respiration. 2014;88(6):451–457. doi:10.1159/000368615
25. Schreiber A, Cemmi F, Ambrosino N, Ceriana P, Lastoria C, Carlucci A. Prevalence and predictors of obstructive sleep apnea in patients with chronic obstructive pulmonary disease undergoing inpatient pulmonary rehabilitation. COPD. 2018;15(3):265–270. doi:10.1080/15412555.2018.1500533
26. Tang M, Wang Y, Wang M, Tong R, Shi T. Risk for cardiovascular disease and one-year mortality in patients with chronic obstructive pulmonary disease and obstructive sleep apnea syndrome overlap syndrome. Front Pharmacol. 2021;12:767982. doi:10.3389/fphar.2021.767982
27. Yang X, Tang X, Cao Y, et al. The bronchiectasis in COPD-OSA overlap syndrome patients. Int J Chron Obstruct Pulmon Dis. 2020;15:605–611. doi:10.2147/COPD.S243429
28. Turcani P, Skrickova J, Pavlik T, Janousova E, Orban M. The prevalence of obstructive sleep apnea in patients hospitalized for COPD exacerbation. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2015;159(3):422–428. doi:10.5507/bp.2014.002
29. Alkhayat K, Hussein MT, Mohammed OA, Mohammadien HA. Prevalence of obstructive sleep apnea in patients with chronic obstructive pulmonary disease. Egypt J Chest Dis Tuberc. 2021;70(4):441–446. doi:10.4103/ecdt.ecdt_12_21
30. Lurie A, Roche N. Obstructive sleep apnea in patients with chronic obstructive pulmonary disease: facts and perspectives. COPD. 2021;18(6):700–712. doi:10.1080/15412555.2021.1950663
31. Nair S, Paul T, Mehta AA, Haridas N, Kunoor A, Sudhakar N. Prevalence of overlap syndrome in patients with obstructive sleep apnea in a quaternary care center of Kerala. Indian J Public Health. 2022;66(Supplement):S12–S16. doi:10.4103/ijph.ijph_1085_22
32. Soler X, Gaio E, Powell FL, et al. High prevalence of obstructive sleep apnea in patients with moderate to severe chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2015;12(8):1219–1225. doi:10.1513/AnnalsATS.201407-336OC
33. Morantes-Caballero JA, Fajardo Rodriguez HA. Effects of air pollution on acute exacerbation of chronic obstructive pulmonary disease: a descriptive retrospective study (pol-AECOPD). Int J Chron Obstruct Pulmon Dis. 2019;14:1549–1557. doi:10.2147/COPD.S192047
34. Gothi D, Gupta SS, Kumar N, Sood K. Impact of overlap syndrome on severity of acute exacerbation of chronic obstructive pulmonary disease. Lung India. 2015;32(6):578–583. doi:10.4103/0970-2113.168132
35. Zhang P, Chen B, Lou H, et al. Predictors and outcomes of obstructive sleep apnea in patients with chronic obstructive pulmonary disease in China. BMC Pulm Med. 2022;22(1):16. doi:10.1186/s12890-021-01780-4
36. Shawon MSR, Perret JL, Senaratna CV, Lodge C, Hamilton GS, Dharmage SC. Current evidence on prevalence and clinical outcomes of co-morbid obstructive sleep apnea and chronic obstructive pulmonary disease: a systematic review. Sleep Med Rev. 2017;32:58–68. doi:10.1016/j.smrv.2016.02.007
37. Gunduz C, Basoglu OK, Tasbakan MS. Prevalence of overlap syndrome in chronic obstructive pulmonary disease patients without sleep apnea symptoms. Clin Respir J. 2018;12(1):105–112. doi:10.1111/crj.12493
38. Du D, Zhang G, Xu D, et al. Prevalence and clinical characteristics of sleep disorders in chronic obstructive pulmonary disease: a systematic review and meta-analysis. Sleep Med. 2023;112:282–290. doi:10.1016/j.sleep.2023.10.034
39. Hansson D, Andersson A, Vanfleteren LEGW, et al. Clinical impact of routine sleep assessment by peripheral arterial tonometry in patients with COPD. ERJ Open Res. 2023;9(2):00458–02022. doi:10.1183/23120541.00458-2022
40. Greenberg-Dotan S, Reuveni H, Tal A, et al. Increased prevalence of obstructive lung disease in patients with obstructive sleep apnea. Sleep Breath. 2014;18(1):69–75. doi:10.1007/s11325-013-0850-3
41. Zhang H, Wu F, Yi H, et al. Gender differences in chronic obstructive pulmonary disease symptom clusters. Int J Chron Obstruct Pulmon Dis. 2021;16:1101–1107. doi:10.2147/COPD.S302877
42. Fabozzi A, Pasqualotto F, Laguardia M, et al. Gender differences in obstructive sleep apnea syndrome: a pilot study. Sleep Breath. 2024;28(4):1645–1650. doi:10.1007/s11325-024-03052-x
43. Saraç S, Afşar GÇ, Saraç S, Afşar GÇ. Comorbidity of obstructive sleep apnea syndrome, cronic obstructive lung disease and asthma chronic airway diseases and sleep apnea. Turkish J Sleep Med. 2017. doi:10.4274/jtsm.18209
44. Han MK, Arteaga-Solis E, Blenis J, et al. Female sex and gender in lung/sleep health and disease. increased understanding of basic biological, pathophysiological, and behavioral mechanisms leading to better health for female patients with lung disease. Am J Respir Crit Care Med. 2018;198(7):850–858. doi:10.1164/rccm.201801-0168WS
45. van Zeller M, McNicholas WT. Sleep disordered breathing: OSA-COPD overlap. Expert Rev Respir Med. 2024;18(6):369–379. doi:10.1080/17476348.2024.2373790
46. Reshma SJ, George S, SK P. Pulmonary hypertension in newly diagnosed obstructive sleep apnea-chronic obstructive pulmonary disease overlap syndrome patients attending a tertiary care centre-a cross-sectional analysis. Ir J Med Sci. 2024. doi:10.1007/s11845-024-03657-x
47. Adler D, Bailly S, Benmerad M, et al. Clinical presentation and comorbidities of obstructive sleep apnea-COPD overlap syndrome. PLoS One. 2020;15(7):e0235331. doi:10.1371/journal.pone.0235331
48. Yang X, Han X, Liang M, Wang Y, Zhang J, Cao J. The role of neutrophil to lymphocyte ratio in patients with COPD-OSA overlap syndrome. Sleep Breath. 2024. doi:10.1007/s11325-024-03013-4
49. Sanchez-Azofra A, Gu W, Masso-Silva JA, et al. Inflammation biomarkers in OSA, chronic obstructive pulmonary disease, and chronic obstructive pulmonary disease/OSA overlap syndrome. J Clin Sleep Med. 2023;19(8):1447–1456. doi:10.5664/jcsm.10600
50. Jen R, Li Y, Owens RL, Malhotra A. Sleep in chronic obstructive pulmonary disease: evidence gaps and challenges. Can Respir J. 2016;2016:7947198. doi:10.1155/2016/7947198
51. Brennan M, McDonnell MJ, Walsh SM, Gargoum F, Rutherford R. Review of the prevalence, pathogenesis and management of OSA-COPD overlap. Sleep Breath. 2022;26(4):1551–1560. doi:10.1007/s11325-021-02540-8
52. Oțelea MR, Trenchea M, Rașcu A, et al. Smoking obstructive sleep apnea: arguments for a distinctive phenotype and a personalized intervention. J Pers Med. 2022;12(2):293. doi:10.3390/jpm12020293
53. Wang Y, Hu K, Liu K, et al. Obstructive sleep apnea exacerbates airway inflammation in patients with chronic obstructive pulmonary disease. Sleep Med. 2015;16(9):1123–1130. doi:10.1016/j.sleep.2015.04.019
54. Ioachimescu OC, McNicholas WT. Chronic obstructive pulmonary disease-obstructive sleep apnea overlap: more than a casual acquaintance. Am J Respir Crit Care Med. 2022;206(2):139–141. doi:10.1164/rccm.202204-0695ED
55. He BT, Lu G, Xiao SC, et al. Coexistence of OSA may compensate for sleep related reduction in neural respiratory drive in patients with COPD. Thorax. 2017;72(3):256–262. doi:10.1136/thoraxjnl-2016-208467
56. Brock JM, Billeter A, Müller-Stich BP, Herth F. Obesity and the lung: what we know today. Respiration. 2020;99(10):856–866. doi:10.1159/000509735
57. Ioachimescu OC, Teodorescu M. Integrating the overlap of obstructive lung disease and obstructive sleep apnoea: OLDOSA syndrome. Respirology. 2013;18(3):421–431. doi:10.1111/resp.12062
58. Kuvat N, Tanriverdi H, Armutcu F. The relationship between obstructive sleep apnea syndrome and obesity: a new perspective on the pathogenesis in terms of organ crosstalk. Clin Respir J. 2020;14(7):595–604. doi:10.1111/crj.13175
59. Parameswaran K, Todd DC, Soth M. Altered respiratory physiology in obesity. Can Respir J. 2006;13(4):203–210. doi:10.1155/2006/834786
60. Mancuso P. Obesity and lung inflammation. J Appl Physiol. 2010;108(3):722–728. doi:10.1152/japplphysiol.00781.2009
61. Carneiro-Barrera A, Amaro-Gahete FJ, Guillén-Riquelme A, et al. Effect of an interdisciplinary weight loss and lifestyle intervention on obstructive sleep apnea severity: the INTERAPNEA randomized clinical trial. JAMA Network Open. 2022;5(4):e228212. doi:10.1001/jamanetworkopen.2022.8212
62. Kikuchi R, Tsuji T, Watanabe O, et al. Hypercapnia accelerates adipogenesis: a novel role of high CO2 in exacerbating obesity. Am J Respir Cell Mol Biol. 2017;57(5):570–580. doi:10.1165/rcmb.2016-0278OC
63. Yang Y, Wu J, Li S, et al. Smoking, coffee consumption, alcohol intake, and obstructive sleep apnea: a mendelian randomization study. Curr Neurovasc Res. 2023;20(2):280–289. doi:10.2174/1567202620666230627145908
64. Zeng X, Ren Y, Wu K, et al. Association between smoking behavior and obstructive sleep apnea: a systematic review and meta-analysis. Nicotine Tob Res. 2023;25(3):364–371. doi:10.1093/ntr/ntac126
65. Esen AD, Akpinar M. Relevance of obstructive sleep apnea and smoking: obstructive sleep apnea and smoking. Fam Pract. 2021;38(2):181–186. doi:10.1093/fampra/cmaa112
66. Zhu HM, Yi HL, Guan J, et al. Relationship between smoking and the severity of OSA. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2019;33(9):862–865;869. doi:10.13201/j.issn.1001-1781.2019.09.016
67. Shao C, Qi H, Fang Q, Tu J, Li Q, Wang L. Smoking history and its relationship with comorbidities in patients with obstructive sleep apnea. Tob Induc Dis. 2020;18:56. doi:10.18332/tid/123429
68. Aghapour M, Raee P, Moghaddam SJ, Hiemstra PS, Heijink IH. Airway epithelial barrier dysfunction in chronic obstructive pulmonary disease: role of cigarette smoke exposure. Am J Respir Cell Mol Biol. 2018;58(2):157–169. doi:10.1165/rcmb.2017-0200TR
69. Guillot L, Nathan N, Tabary O, et al. Alveolar epithelial cells: master regulators of lung homeostasis. Int J Biochem Cell Biol. 2013;45(11):2568–2573. doi:10.1016/j.biocel.2013.08.009
70. Dang X, He B, Ning Q, et al. Alantolactone suppresses inflammation, apoptosis and oxidative stress in cigarette smoke-induced human bronchial epithelial cells through activation of Nrf2/HO-1 and inhibition of the NF-κB pathways. Respir Res. 2020;21(1):95. doi:10.1186/s12931-020-01358-4
71. Lei F, Wang W, Fu Y, Wang J, Zheng Y. Mitochondrial KATP channels contribute to the protective effects of hydrogen sulfide against impairment of central chemoreception of rat offspring exposed to maternal cigarette smoke. PLoS One. 2020;15(10):e0237643. doi:10.1371/journal.pone.0237643
72. Lalley PM. The aging respiratory system--pulmonary structure, function and neural control. Respir Physiol Neurobiol. 2013;187(3):199–210. doi:10.1016/j.resp.2013.03.012
73. Shao C, Wang H, He Y, Yu B, Zhao H. Clinical phenotype of obstructive sleep apnea in older adults: a hospital-based retrospective study in China. Ir J Med Sci. 2023;192(5):2305–2312. doi:10.1007/s11845-023-03290-0
74. Caramori G, Ruggeri P, Di Stefano A, et al. Autoimmunity and COPD: clinical implications. Chest. 2018;153(6):1424–1431. doi:10.1016/j.chest.2017.10.033
75. Martin EM, Clapp PW, Rebuli ME, et al. E-cigarette use results in suppression of immune and inflammatory-response genes in nasal epithelial cells similar to cigarette smoke. Am J Physiol Lung Cell Mol Physiol. 2016;311(1):L135–144. doi:10.1152/ajplung.00170.2016
76. Bhat TA, Panzica L, Kalathil SG, Thanavala Y. Immune dysfunction in patients with chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2015;12 Suppl 2(Suppl 2):S169–175. doi:10.1513/AnnalsATS.201503-126AW
77. Gong LZ, Ping LT, Ye H, Feng Y, Qing LD. Immune function changes in patients with obstructive sleep apnea hypopnea syndrome. Nan Fang Yi Ke Da Xue Xue Bao. 2011;31(6):1003–1005.
78. Yamaguchi Y, Shiota S, Kusunoki Y, et al. Polysomnographic features of low arousal threshold in overlap syndrome involving obstructive sleep apnea and chronic obstructive pulmonary disease. Sleep Breath. 2019;23(4):1095–1100. doi:10.1007/s11325-019-01786-7
79. Messineo L, Lonni S, Magri R, et al. Lung air trapping lowers respiratory arousal threshold and contributes to sleep apnea pathogenesis in COPD patients with overlap syndrome. Respir Physiol Neurobiol. 2020;271:103315. doi:10.1016/j.resp.2019.103315
80. Raphelson J, Sanchez-Azofra A, Orr JE, et al. Obstructive sleep apnea severity and pathophysiological traits in overlap syndrome: insights from the SNOOzzzE cohort. Physiol Rep. 2025;13(13):e70438. doi:10.14814/phy2.70438
81. El-Solh AA, Lawson Y, Wilding GE. Impact of low arousal threshold on treatment of obstructive sleep apnea in patients with post-traumatic stress disorder. Sleep Breath. 2021;25(2):597–604. doi:10.1007/s11325-020-02106-0
82. Wang D, Zhang Y, Gan Q, et al. Arousal threshold score: a new indicator for examining the relationship between obstructive sleep apnea and overlap syndrome - a retrospective study. NAT SCI SLEEP. 2025;17:1945–1956. doi:10.2147/NSS.S551944
83. de Vries H, Jonkman A, Shi ZH, Spoelstra-de Man A, Heunks L. Assessing breathing effort in mechanical ventilation: physiology and clinical implications. Ann Transl Med. 2018;6(19):387. doi:10.21037/atm.2018.05.53
84. Del negro CA, Funk GD, Feldman JL. Breathing matters. Nat Rev Neurosci. 2018;19(6):351–367. doi:10.1038/s41583-018-0003-6
85. Neubauer JA, Sunderram J. Oxygen-sensing neurons in the central nervous system. J Appl Physiol. 2004;96(1):367–374. doi:10.1152/japplphysiol.00831.2003
86. Remmers JE. Sleeping and breathing. Chest. 1990;97(3 Suppl):77S–80S. doi:10.1378/chest.97.3_supplement.77s
87. Olson EJ, Simon PM. Sleep-wake cycles and the management of respiratory failure. Curr Opin Pulm Med. 1996;2(6):500–506.
88. Iannella G, Magliulo G, Greco A, et al. Obstructive sleep apnea syndrome: from symptoms to treatment. Int J Environ Res Public Health. 2022;19(4):2459. doi:10.3390/ijerph19042459
89. Gleadhill IC, Schwartz AR, Schubert N, Wise RA, Permutt S, Smith PL. Upper airway collapsibility in snorers and in patients with obstructive hypopnea and apnea. Am Rev Respir Dis. 1991;143(6):1300–1303. doi:10.1164/ajrccm/143.6.1300
90. Abbasi A, Gupta SS, Sabharwal N, et al. A comprehensive review of obstructive sleep apnea. Sleep Sci. 2021;14(2):142–154. doi:10.5935/1984-0063.20200056
91. McNicholas WT, Pevernagie D. Obstructive sleep apnea: transition from pathophysiology to an integrative disease model. J Sleep Res. 2022;31(4):e13616. doi:10.1111/jsr.13616
92. Basile M, Baiamonte P, Mazzuca E, et al. Sleep disturbances in COPD are associated with heterogeneity of airway obstruction. COPD. 2018;15(4):350–354. doi:10.1080/15412555.2018.1504015
93. McNicholas WT. Comorbid obstructive sleep apnoea and chronic obstructive pulmonary disease and the risk of cardiovascular disease. J Thorac Dis. 2018;10(Suppl 34):S4253–S4261. doi:10.21037/jtd.2018.10.117
94. Matran R, Alving K, Lundberg JM. Cigarette smoke, nicotine and capsaicin aerosol-induced vasodilatation in pig respiratory mucosa. Br J Pharmacol. 1990;100(3):535–541. doi:10.1111/j.1476-5381.1990.tb15842.x
95. Peters EJ, Morice R, Benner SE, et al. Squamous metaplasia of the bronchial mucosa and its relationship to smoking. Chest. 1993;103(5):1429–1432. doi:10.1378/chest.103.5.1429
96. Sterling GM. Mechanism of bronchoconstriction caused by cigarette smoking. Br Med J. 1967;3(5560):275–277. doi:10.1136/bmj.3.5560.275
97. Rasmussen LW, Stanford D, LaFontaine J, Allen AD, Raju SV. Nicotine aerosols diminish airway CFTR function and mucociliary clearance. Am J Physiol Lung Cell Mol Physiol. 2023;324(5):L557–L570. doi:10.1152/ajplung.00453.2021
98. Dülger S, Çapkur Ç, Gençay S, et al. The relationship between nasal mucociliary clearance time and the degree of smoking dependence in smokers with obstructive sleep apnea syndrome. Adv Respir Med. 2021;89(4):353–358. doi:10.5603/ARM.a2021.0069
99. Ramos FL, Krahnke JS, Kim V. Clinical issues of mucus accumulation in COPD. Int J Chron Obstruct Pulmon Dis. 2014;9:139–150. doi:10.2147/COPD.S38938
100. Mall MA, Danahay H, Boucher RC. Emerging concepts and therapies for mucoobstructive lung disease. Ann Am Thorac Soc. 2018;15(Suppl 3):S216–S226. doi:10.1513/AnnalsATS.201806-368AW
101. Vastag E, Matthys H, Köhler D, Gronbeck L, Daikeler G. Mucociliary clearance and airways obstruction in smokers, ex-smokers and normal subjects who never smoked. Eur J Respir Dis Suppl. 1985;139:93–100.
102. Fu C, Lu H, Wu X, et al. Chronic intermittent hypoxia decreases pulmonary clearance of 99mTc-labelled particulate matter in mice. Am J Transl Res. 2017;9(6):3060–3072.
103. Heinzer RC, Stanchina ML, Malhotra A, et al. Effect of increased lung volume on sleep disordered breathing in patients with sleep apnoea. Thorax. 2006;61(5):435–439. doi:10.1136/thx.2005.052084
104. Biselli P, Grossman PR, Kirkness JP, et al. The effect of increased lung volume in chronic obstructive pulmonary disease on upper airway obstruction during sleep. J Appl Physiol. 2015;119(3):266–271. doi:10.1152/japplphysiol.00455.2014
105. Deegan PC, McNicholas WT. Pathophysiology of obstructive sleep apnoea. Eur Respir J. 1995;8(7):1161–1178. doi:10.1183/09031936.95.08071161
106. Leiter JC, Knuth SL, Bartlett D. The effect of sleep deprivation on activity of the genioglossus muscle. Am Rev Respir Dis. 1985;132(6):1242–1245. doi:10.1164/arrd.1985.132.6.1242
107. Van de Graaff WB. Thoracic influence on upper airway patency. J Appl Physiol. 1988;65(5):2124–2131. doi:10.1152/jappl.1988.65.5.2124
108. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011
109. Parameswaran GI, Wrona CT, Murphy TF, Sethi S. Moraxella catarrhalis acquisition, airway inflammation and protease-antiprotease balance in chronic obstructive pulmonary disease. BMC Infect Dis. 2009;9:178. doi:10.1186/1471-2334-9-178
110. Younes M. Pathogenesis of obstructive sleep apnea. Clin Chest Med. 2019;40(2):317–330. doi:10.1016/j.ccm.2019.02.008
111. Kimoff RJ. Sleep fragmentation in obstructive sleep apnea. Sleep. 1996;19(9 Suppl):S61–66. doi:10.1093/sleep/19.suppl_9.s61
112. Owens RL, Macrea MM, Teodorescu M. The overlaps of asthma or COPD with OSA: a focused review. Respirology. 2017;22(6):1073–1083. doi:10.1111/resp.13107
113. Locke BW, Lee JJ, Sundar KM. OSA and chronic respiratory disease: mechanisms and epidemiology. Int J Environ Res Public Health. 2022;19(9):5473. doi:10.3390/ijerph19095473
114. Chaszczewska-Markowska M, Górna K, Bogunia-Kubik K, Brzecka A, Kosacka M. The influence of comorbidities on chemokine and cytokine profile in obstructive sleep apnea patients: preliminary results. J Clin Med. 2023;12(3):801. doi:10.3390/jcm12030801
115. Macrea M, Campbell S, Martin T, Oursler KA. The peripheral neutrophils in subjects with COPD-OSA overlap syndrome and severe comorbidities: a feasible inflammatory biomarker? Adv Clin Exp Med. 2018;27(12):1677–1682. doi:10.17219/acem/75904
116. Yu H, Shao H, Wu Q, et al. Altered gene expression of hepatic cytochrome P450 in a rat model of intermittent hypoxia with emphysema. Mol Med Rep. 2017;16(1):881–886. doi:10.3892/mmr.2017.6642
117. Shah A, Mukherjee S, McArdle N, Singh B, Ayas N. Circulating C-reactive protein levels in patients with suspected obstructive sleep apnea. J Clin Sleep Med. 2022;18(4):993–1001. doi:10.5664/jcsm.9774
118. Shiina K, Tomiyama H, Takata Y, et al. Overlap syndrome: additive effects of COPD on the cardiovascular damages in patients with OSA. Respir Med. 2012;106(9):1335–1341. doi:10.1016/j.rmed.2012.05.006
119. Marin-Oto M, Sanz-Rubio D, Santamaría-Martos F, et al. Soluble RAGE in COPD, with or without coexisting obstructive sleep apnoea. Respir Res. 2022;23(1):163. doi:10.1186/s12931-022-02092-9
120. Kis A, Meszaros M, Tarnoki DL, et al. Exhaled carbon monoxide levels in obstructive sleep apnoea. J Breath Res. 2019;13(3):036012. doi:10.1088/1752-7163/ab231d
121. Okur HK, Pelin Z, Yuksel M, Yosunkaya S. Lipid peroxidation and paraoxonase activity in nocturnal cyclic and sustained intermittent hypoxia. Sleep Breath. 2013;17(1):365–371. doi:10.1007/s11325-012-0703-5
122. Somers VK, Mark AL, Zavala DC, Abboud FM. Influence of ventilation and hypocapnia on sympathetic nerve responses to hypoxia in normal humans. J Appl Physiol. 1989;67(5):2095–2100. doi:10.1152/jappl.1989.67.5.2095
123. Somers VK, Mark AL, Zavala DC, Abboud FM. Contrasting effects of hypoxia and hypercapnia on ventilation and sympathetic activity in humans. J Appl Physiol. 1989;67(5):2101–2106. doi:10.1152/jappl.1989.67.5.2101
124. Taranto-Montemurro L, Messineo L, Perger E, et al. Cardiac sympathetic hyperactivity in patients with chronic obstructive pulmonary disease and obstructive sleep apnea. COPD. 2016;13(6):706–711. doi:10.1080/15412555.2016.1199668
125. Camargo PF, Ditomaso-Luporini L, Tinoco Areas GP, Goulart CDL, Mendes RG, Borghi-Silva A. Impact of obstructive sleep apnea on cardiac autonomic control during the respiratory sinus arrhythmia maneuver in patients with chronic obstructive pulmonary disease. Heart Mind. 2023;7(2):80–88. doi:10.4103/hm.hm_54_22
126. Zangrando KTL, Trimer R, de Carvalho LCS, et al. Chronic obstructive pulmonary disease severity and its association with obstructive sleep apnea syndrome: impact on cardiac autonomic modulation and functional capacity. Int J Chron Obstruct Pulmon Dis. 2018;13:1343–1351. doi:10.2147/COPD.S156168
127. Macefield VG. Firing patterns of muscle vasoconstrictor neurons in respiratory disease. Front Physiol. 2012;3:153. doi:10.3389/fphys.2012.00153
128. Ashley C, Burton D, Sverrisdottir YB, Sander M, McKenzie DK, Macefield VG. Firing probability and mean firing rates of human muscle vasoconstrictor neurones are elevated during chronic asphyxia. J Physiol. 2010;588(Pt 4):701–712. doi:10.1113/jphysiol.2009.185348
129. Camargo PF, Ditomaso-Luporini L, de Carvalho LCS, et al. Obstructive sleep apnea reduces functional capacity and impairs cardiac autonomic modulation during submaximal exercise in patients with chronic obstructive pulmonary disease: a follow-up study. Heart Lung. 2023;57:257–264. doi:10.1016/j.hrtlng.2022.10.007
130. Rodríguez-Pérez J, Andreu-Martínez R, Daza R, et al. Oxidative stress and inflammation in hypoxemic respiratory diseases and their comorbidities: molecular insights and diagnostic advances in chronic obstructive pulmonary disease and sleep apnea. Antioxidants. 2025;14(7):839. doi:10.3390/antiox14070839
131. Brevetti G, Silvestro A, Schiano V, Chiariello M. Endothelial dysfunction and cardiovascular risk prediction in peripheral arterial disease: additive value of flow-mediated dilation to ankle-brachial pressure index. Circulation. 2003;108(17):2093–2098. doi:10.1161/01.CIR.0000095273.92468.D9
132. Kent BD, Mitchell PD, McNicholas WT. Hypoxemia in patients with COPD: cause, effects, and disease progression. Int J Chron Obstruct Pulmon Dis. 2011;6:199–208. doi:10.2147/COPD.S10611
133. MacIntyre NR. Acute hypercapnic respiratory failure in COPD. Respir Care. 2023;68(7):973–982. doi:10.4187/respcare.10560
134. Franczuk M, Radwan L, Pływaczewski R, Sliwiński P, Boros P, Wesołowski S. Respiratory responses to CO2 stimulation in hypercapnic patients with obstructive sleep apnea syndrome. Pneumonol Alergol Pol. 2006;74(4):383–390.
135. Khatri SB, Ioachimescu OC. The intersection of obstructive lung disease and sleep apnea. Cleve Clin J Med. 2016;83(2):127–140. doi:10.3949/ccjm.83a.14104
136. Ferrer-Lluis I, Castillo-Escario Y, Glos M, Fietze I, Penzel T, Jane R. Sleep apnea & chronic obstructive pulmonary disease: overlap syndrome dynamics in patients from an epidemiological study. Annu Int Conf IEEE Eng Med Biol Soc. 2021;2021:5574–5577. doi:10.1109/EMBC46164.2021.9630515
137. Povitz M, James MT, Pendharkar SR, Raneri J, Hanly PJ, Tsai WH. Prevalence of sleep-disordered breathing in obese patients with chronic hypoxemia. a cross-sectional study. Ann Am Thorac Soc. 2015;12(6):921–927. doi:10.1513/AnnalsATS.201412-551OC
138. Resta O, Foschino Barbaro MP, Brindicci C, Nocerino MC, Caratozzolo G, Carbonara M. Hypercapnia in overlap syndrome: possible determinant factors. Sleep Breath. 2002;6(1):11–18. doi:10.1007/s11325-002-0011-6
139. Brown LK. Sleep-related disorders and chronic obstructive pulmonary disease. Respir Care Clin N Am. 1998;4(3):493–512.
140. Radwan L, Maszczyk Z, Koziorowski A, et al. Control of breathing in obstructive sleep-apnea and in patients with the overlap syndrome. Eur Resp J. 1995;8(4):542–545.
141. Hawryłkiewicz I, Cieślicki J, Koziej M, Pałasiewicz G, Zieliński J. Pulmonary hemodynamics in obstructive sleep apnea or overlap syndrome. Pol Arch Med Wewn. 1994;92(6):467–473.
142. Zhen X, Moya EA, Gautane M, et al. Combined intermittent and sustained hypoxia is a novel and deleterious cardio-metabolic phenotype. Sleep. 2022;45(6):zsab290. doi:10.1093/sleep/zsab290
143. Hu BZ, Jiang C, Ding YJ, et al. The clinical and hemodynamic characteristics of pulmonary hypertension in patients with OSA-COPD overlap syndrome. Am J Med Sci. 2024. doi:10.1016/j.amjms.2024.03.014
144. Hawryłkiewicz I, Sliwiński P, Górecka D, Pływaczewski R, Zieliński J. Pulmonary haemodynamics in patients with OSAS or an overlap syndrome. Monaldi Arch Chest Dis. 2004;61(3):148–152. doi:10.4081/monaldi.2004.693
145. Kharchenko I, Krakhmalova O, Izmailova O. The relationship between the severity of obstructive sleep apnea syndrome and severity of chronic obstructive pulmonary disease (COPD) associated with coronary artery disease (CAD). Eur Resp J. 2016;48. doi:10.1183/13993003.congress-2016.PA640
146. Chen FM, Wang YL, Sun WL, Huang YW, Zhang J, Chen Y. Effects of obstructive sleep apnea hypopnea syndrome on cardiac function in patients with chronic obstructive pulmonary disease. Zhonghua Jie He He Hu Xi Za Zhi. 2022;45(2):151–157. doi:10.3760/cma.j.cn112147-20210601-00372
147. Banjade P, Kandel K, Itani A, et al. The interplay between obstructive sleep apnea, chronic obstructive pulmonary disease, and congestive heart failure: time to collectively refer to them as triple overlap syndrome? Medicina. 2023;59(8):1374. doi:10.3390/medicina59081374
148. Sharma B, Neilan TG, Kwong RY, et al. Evaluation of right ventricular remodeling using cardiac magnetic resonance imaging in co-existent chronic obstructive pulmonary disease and obstructive sleep apnea. COPD. 2013;10(1):4–10. doi:10.3109/15412555.2012.719050
149. Fletcher EC. Chronic lung disease in the sleep apnea syndrome. Lung. 1990;168 Suppl:751–761. doi:10.1007/BF02718204
150. Desai R, Sachdeva S, Jain A, et al. Comparison of percutaneous coronary intervention outcomes among patients with obstructive sleep apnea, chronic obstructive pulmonary disease overlap, and pickwickian syndrome (obesity hypoventilation syndrome). Cureus. 2022;14(5):e24816. doi:10.7759/cureus.24816
151. Yeh YL, Lai CM, Liu HP. Outcomes of coronary artery bypass grafting (CABG) in patients with OSA-COPD overlap syndrome versus COPD alone: an analysis of US Nationwide Inpatient Sample. BMC Pulm Med. 2024;24(1):171. doi:10.1186/s12890-024-02994-y
152. Olmetti F, La Rovere MT, Robbi E, Taurino AE, Fanfulla F. Nocturnal cardiac arrhythmia in patients with obstructive sleep apnea. Sleep Med. 2008;9(5):475–480. doi:10.1016/j.sleep.2007.08.015
153. Dalgaard F, North R, Pieper K, et al. Risk of major cardiovascular and neurologic events with obstructive sleep apnea among patients with atrial fibrillation. Am Heart J. 2020;223:65–71. doi:10.1016/j.ahj.2020.01.001
154. Ganga HV, Nair SU, Puppala VK, Miller WL. Risk of new-onset atrial fibrillation in elderly patients with the overlap syndrome: a retrospective cohort study. J Geriatr Cardiol. 2013;10(2):129–134. doi:10.3969/j.issn.1671-5411.2013.02.001
155. Akinnusi M, El-Masri AR, Lawson Y, El-Solh AA. Association of overlap syndrome with incident atrial fibrillation. Intern Emerg Med. 2021;16(3):633–642. doi:10.1007/s11739-020-02469-y
156. Soin S, Pham HN, Hoffer M, et al. New onset atrial fibrillation in chronic obstructive pulmonary disease, obstructive sleep apnea, and overlap syndrome: a retrospective observational study from the trinetx database. Am J Respir Crit Care Med. 2025;211(Abstracts):A5315–A5315. doi:10.1164/ajrccm.2025.211.Abstracts.A5315
157. Tsuda T. Clinical assessment of ventricular wall stress in understanding compensatory hypertrophic response and maladaptive ventricular remodeling. J Cardiovasc Dev Dis. 2021;8(10):122. doi:10.3390/jcdd8100122
158. Voulgaris A, Archontogeorgis K, Apessos I, Paxinou N, Nena E, Steiropoulos P. Is COPD the determinant factor for myocardial injury and cardiac wall stress in OSA patients? Medicina. 2023;59(10):1759. doi:10.3390/medicina59101759
159. Shih CC, Wang JC, Tsai SH, et al. Obstructive sleep apnoea and aortic aneurysm: a nationwide population-based retrospective study. J Vasc Res. 2018;55(4):235–243. doi:10.1159/000491928
160. Xu J, Wei Z, Wang X, Li X, Wang W. The risk of cardiovascular and cerebrovascular disease in overlap syndrome: a meta-analysis. J Clin Sleep Med. 2020;16(7):1199–1207. doi:10.5664/jcsm.8466
161. Stark P, Norbash A. Imaging of the trachea and upper airways in patients with chronic obstructive airway disease. Radiol Clin North Am. 1998;36(1):91–105. doi:10.1016/s0033-8389(05)70008-7
162. McNicholas WT, Hansson D, Schiza S, Grote L. Sleep in chronic respiratory disease: COPD and hypoventilation disorders. Eur Respir Rev. 2019;28(153):190064. doi:10.1183/16000617.0064-2019
163. Wells JM, Washko GR, Han MK, et al. Pulmonary arterial enlargement and acute exacerbations of COPD. N Engl J Med. 2012;367(10):913–921. doi:10.1056/NEJMoa1203830
164. McNicholas WT. Does associated chronic obstructive pulmonary disease increase morbidity and mortality in obstructive sleep apnea? Ann Am Thorac Soc. 2019;16(1):50–53. doi:10.1513/AnnalsATS.201809-628ED
165. Xie J, Li F, Wu X, Hou W. Prevalence of pulmonary embolism in patients with obstructive sleep apnea and chronic obstructive pulmonary disease: the overlap syndrome. Heart Lung. 2019;48(3):261–265. doi:10.1016/j.hrtlng.2018.11.001
166. Kalemci S, Sarıhan A, Zeybek A, Taşdemir N. Prevalence of pulmonary embolism in patients with obstructive sleep apnea and chronic obstructive pulmonary disease: the overlap syndrome. Heart Lung. 2019;48(5):465. doi:10.1016/j.hrtlng.2019.04.005
167. Johannesdottir SA, Horváth-Puhó E, Dekkers OM, et al. Use of glucocorticoids and risk of venous thromboembolism: a nationwide population-based case-control study. JAMA Intern Med. 2013;173(9):743–752. doi:10.1001/jamainternmed.2013.122
168. Sommerwerck U, Kleibrink BE, Kruse F, et al. Predictors of obstructive sleep apnea in lung transplant recipients. Sleep Med. 2016;21:121–125. doi:10.1016/j.sleep.2016.01.005
169. Saba L, Saam T, Jäger HR, et al. Imaging biomarkers of vulnerable carotid plaques for stroke risk prediction and their potential clinical implications. Lancet Neurol. 2019;18(6):559–572. doi:10.1016/S1474-4422(19)30035-3
170. Landete P, Fernández-García CE, Muñoz JM, et al. Sleep apnea-COPD overlap syndrome is associated with larger left carotid atherosclerotic plaques. Front Cardiovasc Med. 2023;10:1104377. doi:10.3389/fcvm.2023.1104377
171. Olaithe M, Bucks RS, Hillman DR, Eastwood PR. Cognitive deficits in obstructive sleep apnea: insights from a meta-review and comparison with deficits observed in COPD, insomnia, and sleep deprivation. Sleep Med Rev. 2018;38:39–49. doi:10.1016/j.smrv.2017.03.005
172. Beaudin AE, Raneri JK, Ayas NT, et al. Contribution of hypercapnia to cognitive impairment in severe sleep-disordered breathing. J Clin Sleep Med. 2022;18(1):245–254. doi:10.5664/jcsm.9558
173. Alharbi AM, Alotaibi N, Uysal ÖF, et al. Cognitive outcomes in chronic obstructive pulmonary disease (COPD)/OSA overlap syndrome compared to obstructive sleep apnea (OSA) alone: a systematic review. Sleep Breath. 2025;29(5):275. doi:10.1007/s11325-025-03426-9
174. Roehrs T, Merrion M, Pedrosi B, Stepanski E, Zorick F, Roth T. Neuropsychological function in obstructive sleep-apnea syndrome (OSAS) compared to chronic obstructive pulmonary-disease (COPD). Sleep. 1995;18(5):382–388. doi:10.1093/sleep/18.5.382
175. Luehrs RE, Moreau KL, Pierce GL, et al. Cognitive performance is lower among individuals with overlap syndrome than in individuals with COPD or obstructive sleep apnea alone: association with carotid artery stiffness. J Appl Physiol. 2021;131(1):131–141. doi:10.1152/japplphysiol.00477.2020
176. Zhang XL, Gao B, Han T, Xiang BY, Liu X. Moderate-to-severe obstructive sleep apnea and cognitive function impairment in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:1813–1822. doi:10.2147/COPD.S257796
177. Wang Y, Li B, Li P, et al. Severe obstructive sleep apnea in patients with chronic obstructive pulmonary disease is associated with an increased prevalence of mild cognitive impairment. Sleep Med. 2020;75:522–530. doi:10.1016/j.sleep.2020.05.002
178. Zhu Z, Wu Y, Qu L, et al. Evaluation of nocturnal apnea and airflow limitation as indicators for cognitive dysfunction in patients with chronic obstructive pulmonary disease/obstructive sleep apnea hypopnea syndrome overlap syndrome. Chron Respir Dis. 2024;21:14799731241236492. doi:10.1177/14799731241236492
179. Zhao Z, Zhang D, Sun H, et al. Anxiety and depression in patients with chronic obstructive pulmonary disease and obstructive sleep apnea: the overlap syndrome. Sleep Breath. 2022;26(4):1603–1611. doi:10.1007/s11325-021-02500-2
180. Kennedy K, Corby C, Noctor E. Manic-like presentation with an organic aetiology. Ir J Psychol Med. 2023;40(2):292–295. doi:10.1017/ipm.2020.76
181. Economou NT, Ilias I, Velentza L, et al. Sleepiness, fatigue, anxiety and depression in chronic obstructive pulmonary disease and obstructive sleep apnea - overlap - syndrome, before and after continuous positive airways pressure therapy. PLoS One. 2018;13(6):e0197342. doi:10.1371/journal.pone.0197342
182. Mirrakhimov AE. Chronic obstructive pulmonary disease and glucose metabolism: a bitter sweet symphony. Cardiovasc Diabetol. 2012;11:132. doi:10.1186/1475-2840-11-132
183. Xie J, Li F. Association of sleep overlap syndrome with type 2 diabetes in a cross-sectional study. Beijing Da Xue Xue Bao Yi Xue Ban. 2019;51(2):252–255. doi:10.19723/j.issn.1671-167X.2019.02.009
184. Archontogeorgis K, Voulgaris A, Papanas N, et al. Metabolic syndrome in patients with coexistent obstructive sleep apnea syndrome and chronic obstructive pulmonary disease (overlap syndrome). Metab Syndr Relat Disord. 2020;18(6):296–301. doi:10.1089/met.2019.0126
185. Mesarwi OA, Loomba R, Malhotra A. Obstructive sleep apnea, hypoxia, and nonalcoholic fatty liver disease. Am J Respir Crit Care Med. 2019;199(7):830–841. doi:10.1164/rccm.201806-1109TR
186. Viglino D, Jullian-Desayes I, Minoves M, et al. Nonalcoholic fatty liver disease in chronic obstructive pulmonary disease. Eur Respir J. 2017;49(6):1601923. doi:10.1183/13993003.01923-2016
187. Jullian-Desayes I, Trzepizur W, Boursier J, et al. Obstructive sleep apnea, chronic obstructive pulmonary disease and NAFLD: an individual participant data meta-analysis. Sleep Med. 2021;77:357–364. doi:10.1016/j.sleep.2020.04.004
188. Ayik S, Bal K, Akhan G. The association of nocturia with sleep disorders and metabolic and chronic pulmonary conditions: data derived from the polysomnographic evaluations of 730 patients. Turk J Med Sci. 2014;44(2):249–254. doi:10.3906/sag-1210-20
189. Haddad R, Decalf V, Monaghan TF, et al. Nocturia severely impairs the sleep quality of nursing home residents: results from a multi-center study. Geriatr Nurs. 2022;48:164–168. doi:10.1016/j.gerinurse.2022.09.009
190. Kilburn KH, Dowell AR. Renal function in respiratory failure. Effects of hypoxia, hyperoxia, and hypercapnia. Arch Intern Med. 1971;127(4):754–762.
191. Archontogeorgis K, Voulgaris A, Papanas N, et al. Mean platelet volume and platelet distribution width in patients with obstructive sleep apnea syndrome and concurrent chronic obstructive pulmonary disease. Clin Appl Thromb Hemost. 2018;24(8):1216–1222. doi:10.1177/1076029618788178
192. Harada T, Tsuboi I, Hirabayashi Y, et al. Decreased “ineffective erythropoiesis” preserves polycythemia in mice under long-term hypoxia. Clin Exp Med. 2015;15(2):179–188. doi:10.1007/s10238-014-0286-5
193. Zeng Z, Song Y, He X, et al. Obstructive sleep apnea is associated with an increased prevalence of polycythemia in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2022;17:195–204. doi:10.2147/COPD.S338824
194. Zhang J, DeMeo DL, Silverman EK, et al. Secondary polycythemia in chronic obstructive pulmonary disease: prevalence and risk factors. BMC Pulm Med. 2021;21(1):235. doi:10.1186/s12890-021-01585-5
195. Vitacca M, Paneroni M, Braghiroli A, et al. Exercise capacity and comorbidities in patients with obstructive sleep apnea. J Clin Sleep Med. 2020;16(4):531–538. doi:10.5664/jcsm.8258
196. Fitzgibbons CM, Goldstein RL, Gottlieb DJ, Moy ML. Physical activity in overlap syndrome of COPD and obstructive sleep apnea: relationship with markers of systemic inflammation. J Clin Sleep Med. 2019;15(7):973–978. doi:10.5664/jcsm.7874
197. Shen H, Xu Y, Zhang Y, Ren L, Chen R. Efficacy of pulmonary rehabilitation in patients with chronic obstructive pulmonary disease and obstructive sleep apnea; a randomized controlled trial. J Rehabil Med. 2024;56:jrm23757. doi:10.2340/jrm.v56.23757
198. Budden KF, Shukla SD, Bowerman KL, et al. Faecal microbial transfer and complex carbohydrates mediate protection against COPD. Gut. 2024;73(5):751–769. doi:10.1136/gutjnl-2023-330521
199. Lim EY, Song EJ, Shin HS. Gut microbiome as a possible cause of occurrence and therapeutic target in chronic obstructive pulmonary disease. J Microbiol Biotechnol. 2023;33(9):1111–1118. doi:10.4014/jmb.2301.01033
200. Baldanzi G, Sayols-Baixeras S, Theorell-Haglöw J, et al. OSA is associated with the human gut microbiota composition and functional potential in the population-based swedish cardiopulmonary bioimage study. Chest. 2023;164(2):503–516. doi:10.1016/j.chest.2023.03.010
201. Badran M, Mashaqi S, Gozal D. The gut microbiome as a target for adjuvant therapy in obstructive sleep apnea. Expert Opin Ther Targets. 2020;24(12):1263–1282. doi:10.1080/14728222.2020.1841749
202. Ma JG, Wu GJ, Xiao HL, Xiao YM, Zha L. Vitamin D has an effect on airway inflammation and Th17/Treg balance in asthmatic mice. Kaohsiung J Med Sci. 2021;37(12):1113–1121. doi:10.1002/kjm2.12441
203. Ghosh AJ, Moll M, Hayden LP, et al. Vitamin D deficiency is associated with respiratory symptoms and airway wall thickening in smokers with and without COPD: a prospective cohort study. BMC Pulm Med. 2020;20(1):123. doi:10.1186/s12890-020-1148-4
204. Bikle DD. Vitamin D regulation of immune function. Curr Osteoporos Rep. 2022;20(3):186–193. doi:10.1007/s11914-022-00732-z
205. Archontogeorgis K, Voulgaris A, Nena E, et al. Vitamin D levels in patients with overlap syndrome, is it associated with disease severity? J Pers Med. 2022;12(10):1693. doi:10.3390/jpm12101693
206. Archontogeorgis K, Voulgaris A, Chadia K, Bonelis K, Steiropoulos P. Effect of CPAP therapy on vitamin D status in patients with obstructive sleep apnea and chronic obstructive pulmonary disease overlap syndrome. Sleep Breath. 2025;29(2):162. doi:10.1007/s11325-025-03324-0
207. Shumway-Cook A, Woollacott M. Motor Control – Theory and Practical Applications.
208. Roig M, Eng JJ, Macintyre DL, Road JD, Reid WD. Postural control is impaired in people with COPD: an observational study. Physiother Can. 2011;63(4):423–431. doi:10.3138/ptc.2010-32
209. Degache F, Goy Y, Vat S, Haba Rubio J, Contal O, Heinzer R. Sleep-disordered breathing and daytime postural stability. Thorax. 2016;71(6):543–548. doi:10.1136/thoraxjnl-2015-207490
210. Stevens D, Jackson B, Carberry J, et al. The impact of obstructive sleep apnea on balance, gait, and falls risk: a narrative review of the literature. J Gerontol a Biol Sci Med Sci. 2020;75(12):2450–2460. doi:10.1093/gerona/glaa014
211. de Censo CM, Passini VV, Verri BATA, et al. Postural balance in COPD with obstructive sleep apnoea: a cross-sectional study. ERJ Open Res. 2024;10(2):00948–02023. doi:10.1183/23120541.00948-2023
212. Perimenis P, Karkoulias K, Konstantinopoulos A, et al. The impact of long-term conventional treatment for overlap syndrome (obstructive steep apnea and chronic obstructive pulmonary disease) on concurrent erectile dysfunction. Respir Med. 2007;101(2):210–216. doi:10.1016/j.rmed.2006.06.012
213. Yousif M, Wahsh RE, Ibrahim A. Retinal vascular tortuosity in patients with obstructive sleep apnea-chronic obstructive pulmonary disease overlap syndrome. Eur Respir J. 2018;52(suppl 62). doi:10.1183/13993003.congress-2018.PA2504
214. Dar MA, Arafah A, Bhat KA, et al. Multiomics technologies: role in disease biomarker discoveries and therapeutics. Brief Funct Genomics. 2023;22(2):76–96. doi:10.1093/bfgp/elac017
215. Rossi G, Manfrin A, Lutolf MP. Progress and potential in organoid research. Nat Rev Genet. 2018;19(11):671–687. doi:10.1038/s41576-018-0051-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Mechanism of Traditional Chinese Medicine and Natural Medicine in Treating Chronic Obstructive Pulmonary Disease

Li L, Liu XF, Cui ZF, Zou H, Liu SL, Wang HW
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1249-1266
Published Date: 26 April 2025