Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Chronic Obstructive Pulmonary Disease and Associated Factors in Arba Minch Health and Demographic Surveillance Site, 2020
Authors Agedew E ![]() , Boda B
, Boda B ![]() , Kanko T
, Kanko T ![]() , Estifanos W
, Estifanos W ![]() , Shibiru T
, Shibiru T ![]()
Received 26 May 2021
Accepted for publication 12 October 2021
Published 28 October 2021 Volume 2021:16 Pages 2953—2962
DOI https://doi.org/10.2147/COPD.S319721
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Eskezyiaw Agedew,1 Belay Boda,2 Tesfaye Kanko,2 Wubshet Estifanos,3 Tamiru Shibiru4
1Department of Public Health, College of Health Sciences, Debre Markos University, Debre Markos, Ethiopia; 2Department of Biomedical Sciences, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 3School of Nursing, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 4School of Medicine, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia
Correspondence: Belay Boda PO Box: 021 Tel +251 916 27 84 53
Fax +251 46881-4264
Email [email protected]
Introduction: Chronic obstructive pulmonary disease (COPD) is a worldwide public health problem. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) defines COPD as a common, preventable and treatable disease characterized by progressive airflow limitation. Nowadays, COPD has become the third leading cause of death and fourth cause of mortality in the world.
Objective: To assess chronic obstructive pulmonary disease and associated factors in Arba Minch – Health and Demographic Surveillance Site (AMU-HDSS) of Arba Minch University.
Methods: A community-based cross-sectional study was conducted in AMU-HDSS among 615 individuals who were > 15 years of age. Study participants were selected randomly by the lottery method. Spirometer device was used to measure lung function. Binary logistic regression analysis was computed to assess the crude association between dependent and independent variables. Finally, variables which showed association in binary logistic regression analysis and have a P-value less than 0.3 were entered into multivariable logistic regression model to identify significant factors.
Results: The prevalence of spirometry diagnosed COPD was 10.6%. Highland residence showed higher proportion of COPD case which accounts 63.8% compared to 36.2% in lowland residence. Study participants who were in advanced age > 41 years adjusted odd ratio (AOR) 3.65 (1.83, 7.28), living in highland area AOR 1.71 (1, 2.92), those who are elementary education level 2.45 (1.13, 5.28), who had no separate house for domestic animals AOR 2.84 (1.38, 5.85), having house which had no windows AOR 3.05 (5.79, 1.12) and living in traditional hut (tukulu), AOR 5.92 (1.19, 29.42) were significantly associated with chronic obstructive pulmonary disease in the study area.
Conclusion and Recommendation: Chronic obstructive pulmonary disease was one of respiratory illnesses in people who live in highland and traditional house lacking windows for air circulation. Improving housing condition of traditional hut by constructing window, separating domestic animals house from humans and minimizing animal dung smoke exposure is necessary to reduce the respiratory illness.
Keywords: spirometer, housing condition, air pollution, Arba Minch University
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by lower airway inflammation and damage that impairs airflow. COPD is the fourth leading cause of death worldwide resulting in chronic diffuse irreversible airflow obstruction mainly in small airways. It also defined as a low ratio of forced expiratory volume in one second (FEV1) to forced vital capacity (FVC).1,2 It is a growing cause of morbidity, disability, and mortality both in developed and developing countries that can be related to environmental exposures, smoking and respiratory infectious diseases.3,4
The main causes of COPD in high-income countries are tobacco smoke and occupational exposure, but in low-income and middle-income countries use of biomass fuel (wood, dung, crop residues, and charcoal) for cooking and domestic heating is a major cause of COPD and childhood respiratory infections.5,6 Chronic obstructive pulmonary disease (COPD), once regarded as a disease of high-income countries, is now recognized as common in low-income and middle-income countries.1,5 The World Health Organization (WHO) has estimated that about 65 million people suffer from moderate to severe COPD worldwide. A striking issue with COPD is that the condition is often underestimated by the patient, largely under diagnosed and undertreated in African countries.7
Previously published studies evaluating the prevalence of COPD have provided a range of estimates across different countries. The prevalence of COPD diagnosed by spirometry ranged from 37 per 1000 (United Arab Emirates) to 240 per 1000 (in Netherlands).8 Low- and middle-income countries share the greatest proportion of COPD worldwide. More than half of those with COPD live in low and middle income countries.2 It has a major impact on health-care expenditure and can impose a substantial economic burden on patients and health-care service providers. In addition, COPD has a major negative impact on the daily lives of patients, as it impairs individual well-being, functional status and work production.9 One of the major affects of COPD is that it causes high economic impact. The estimated total annual cost of COPD for 2010 was $49.9 billion.8
According to WHO, around three billion people in the world still cook and heat their homes using dirty solid fuels (such as waste wood, charcoal, coal, dung, crop wastes) on open fireplaces, cooking stoves, which generates a large amount of air pollutants (such as SO2, NO2, CO, and PM). These air pollutants may accumulate in the indoor environment if not well ventilated, which seriously affects the health of the inhabitants.10,11
The Ethiopian government gives advice on control of common communicable respiratory diseases like tuberculosis and pneumonia as one of the primary health-care services, but chronic non-communicable respiratory disease has not been given due attention in spite of a large number of people suffering from COPD and asthma both in urban and rural areas. The problem of COPD alarmingly increasing, there is no planned public health intervention at country level due to lack sufficient evidence on prevalence and contributing factors for COPD in Ethiopia. The current study would provide valuable information for the community at large, decision makers, health-care planners, evaluators, and medical practitioners for promoting better health, quality of life, and the prevention of disability in from COPD.
Materials and Methods
Study Setting and Design
A community-based cross-sectional study was conducted from August 2019 to February 2020 in the Arba Minch demographic and health surveillance system sites (AM-HDSS). Arba Minch, the capital city of Gamo zone, is found at an altitude of 130 m above sea level with the average temperature of 29°C. Based on the 2014 data, this district has a total population of 164,529, of whom 82,199 are men and 82,330 women. Arba Minch Zuria district has a total of 31 kebeles with three different climatic zones, highland, midland and lowland, among which nine kebeles are under HDSS. According to HDSS report, there are total populations of 74, 157 in the surveillance site.
Population
Randomly selected individuals who are >15 years old and live in AM-HDSS during the study period are the study population.
Inclusion and Exclusion Criteria
Individuals who lived in the HDSS for at least six months were included and those who are known asthmatic and tuberculosis cases were excluded from the study.
Sample Size Determination
The sample size for prevalence of COPD is determined by using single population proportion formula by taking prevalence (P) of COPD in Uganda 16.2% [12], 95% confidence level (Z) and margin of error (D) 3%.

By adding 10% non-response rate the final sample size for the study 638 (the sample size for factors affecting COPD were considered after calculating by using Epi Info™ version 7).
Sampling Technique
First, from nine kebeles under HDSS three sites from highland and other three from lowland climatic zone were selected randomly by lottery methods. The sampling frame was prepared by taking a list of households from HDSS of Arba Minch University. Then sample sized was allocated proportionally based on the number of households in the selected HDSS site, finally the study sample was selected by simple random method and then house-to-house interviews and measurements were conducted.
Study Variables
Dependent variable: chronic obstructive pulmonary disease (yes, no).
Independent variables: sociodemographic characteristics (age, sex, religion, educational status, occupation, income), housing condition like number of rooms, number of windows and ventilation, smoking, indoor air pollution, biomass fuel utilization, and respiratory symptoms (cough, wheezing, shortness of breath).
Operational Definition
- Chronic obstructive pulmonary disease (COPD): it is a preventable and treatable disease state characterized by air flow limitation that is not fully reversible. The main criterion for COPD is a FEV1 /FVC ratio <70%.
- FVC: The volume of air that can forcibly be blown out after maximum inspiration (30, 32).
- FEV1: This is the speed of air forcibly expelled from the lungs in the first one second from maximal inspiration.
Data Collection Tools and Procedure
A structured pretested questionnaire was used for the collection of sociodemographic data, clinical manifestations related to COPD, housing conditions and other factors. Spirometer device was used in accordance with the American Thoracic Society and European Respiratory Society recommendations: at least three measurements were taken every five minutes. The final largest values for both forced vital capacity (FVC) and forced expiratory volume in one second (FEV1) within 150 mL or no more than 5% difference; the largest values for FVC and FEV1 were considered the best and used for analysis. Spirometer was calibrated every morning. The housing conditions data were also collected by using observational check list. Four experienced MSc physiologist and 12 clinical nurses were used for data collection.
Data Quality Assurance
To ensure data quality, two days training was given for data collectors on how to measure lung function status and interview study participants. Before actual data collection, pretest was done on 5% of the sample out of the study site of AM-HDSS. Frequent calibration of spirometer was undertaken before conducting the actual recording.
Data Analysis
Data were collected by an open data kit data collection application and transferred to SPSS version 20 for analysis. Data collected by spirometer were exported to computer for further analysis. Before the actual data analysis, the data were checked for its completeness, outliers and missing values by conducting univariate analysis. Descriptive statistics like cross tabulation were calculated to describe the study population in relation to relevant variables. Exploratory data analysis was done to check potential outliers and the normality distribution for continuous variables. Binary logistic regression analysis was conducted to assess the crude association between dependent and independent variables. Finally, variables which show association in binary logistic regression analysis and have a P-value less than 0.3 were entered into multivariable logistic regression model to identify significant factors. The significant factors was identified based on adjusted odds ratio (AOR) with 95% confidence level and P≤0.05.
Ethical Consideration
The study was conducted according to the Declaration of Helsinki as a statement of ethical principles for medical research involving human subjects. Ethical clearance was obtained from the institutional review committee of College of Medicine and Health Science, Arba Minch University. The study was conducted only by individuals with the appropriate ethics and scientific education, training and qualifications. The investigators had taken every precaution to protect the life, health, dignity, integrity, right to self-determination, privacy, and confidentiality of personal information of research subjects. During data collection, the purpose, method, anticipated benefits and potential risks of the study was clearly explained to the participants and informed written consent was obtained from each study participant. Finally, study participants with impaired respiratory function who have COPD and asthma were linked to the health facility for medical treatment.
Results
Sociodemographic Characteristics
The data were collected from 615 study participants with a 96.4% response rate. Among study participants 53.8% were male. The median age of the study participants were 38 years and 58% of the study participants were above 40 years. Regarding the educational status of study participants 69.4% had no formal education and 67.8% of them were farmers in their occupation. From all study participants 87.3% were married and 46.5% of households had a family size above six (Table 1).
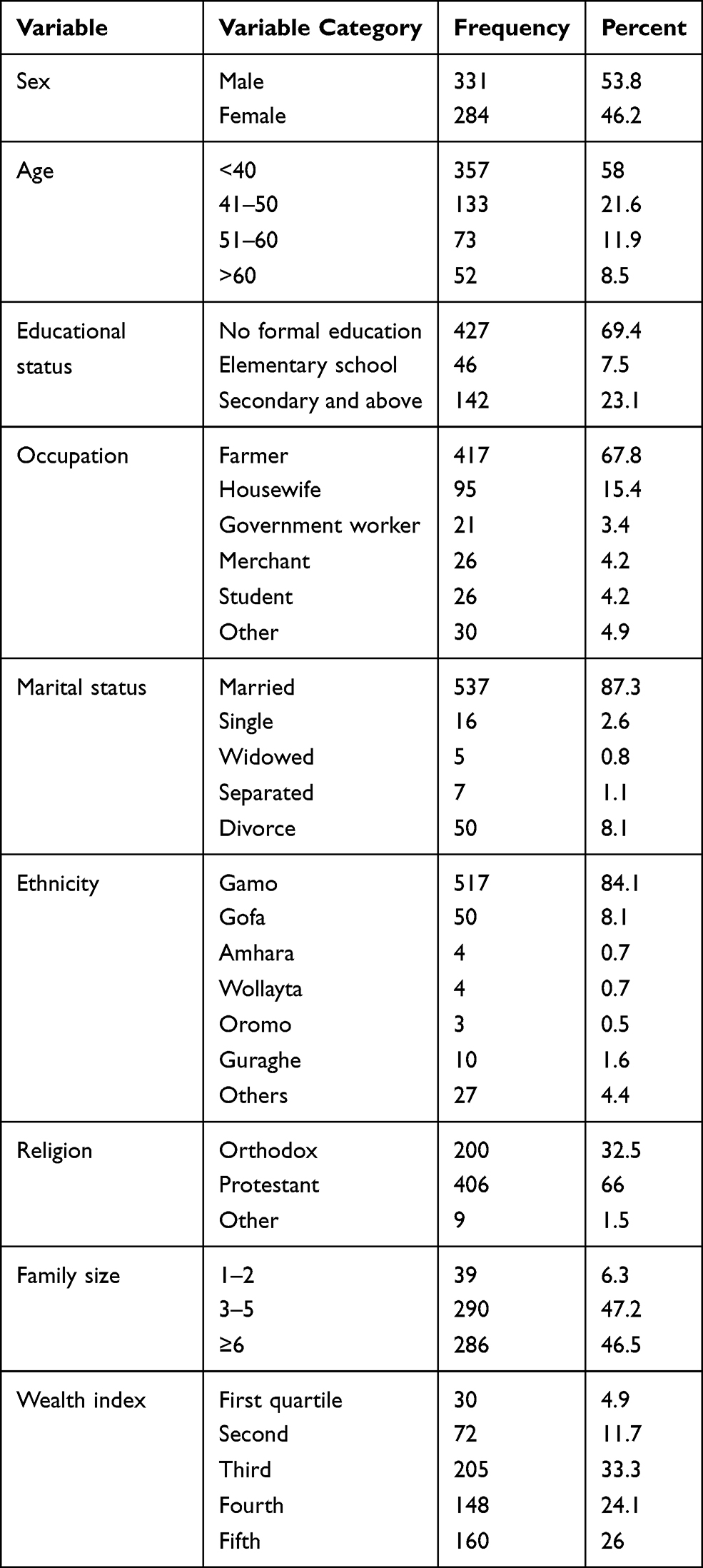 |
Table 1 Sociodemographic Characteristics of Study Participants in AM-HDSS, Southern Ethiopia, 2020 |
Housing Conditions
Among 615 households included in the study, 58.7% of houses were traditional hut (tukulu), 37.9% were constructed from iron sheets and mud. Only 3.4% of house were constructed from iron sheets and cemented materials. Among the houses, 64.2% have only one room, 31.4% of them have 2–3 rooms and the rest have more than four rooms.
Regarding the number of windows and rooms, 84.55% houses constructed from iron sheets and cement materials have more than two rooms and 64.38% have more than three windows. In contrast from 361 traditional hut (tukulu) 347 (96.12%) have no windows (Figure 1).
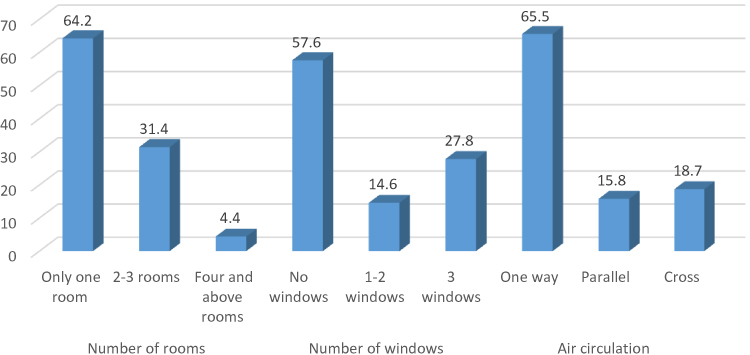 |
Figure 1 Major housing characteristics distribution in AM-HDSS, Southern Ethiopia, 2020. |
Households Smoke Exposure, Ventilation and Illumination
All households utilized biomass fuel as energy sources for food preparation. The common utilized biomass fuel was firewood, animal dung, and crop residues. Among the respondents, 11.5% smoke cigarettes and 8.3% of them smoke more than three times per day. More than half of houses in the study did not have a window and 90% of them had no enclosed area/built structure for the kitchen. More than half of the houses 64.2% have only one room; the remaining 35.8% houses have more than two rooms. Among the houses, 58% have separated kitchen while 42% have kitchen connected with main house or inside the house.
Mean Lung Function Parameters in Relation Factors
The lung function test parameters had lower mean score in females and in those who are in advanced age study participants. According to the test, FEV1/PRE 1 is lower among females and greater than 41 year old participants (Table 2).
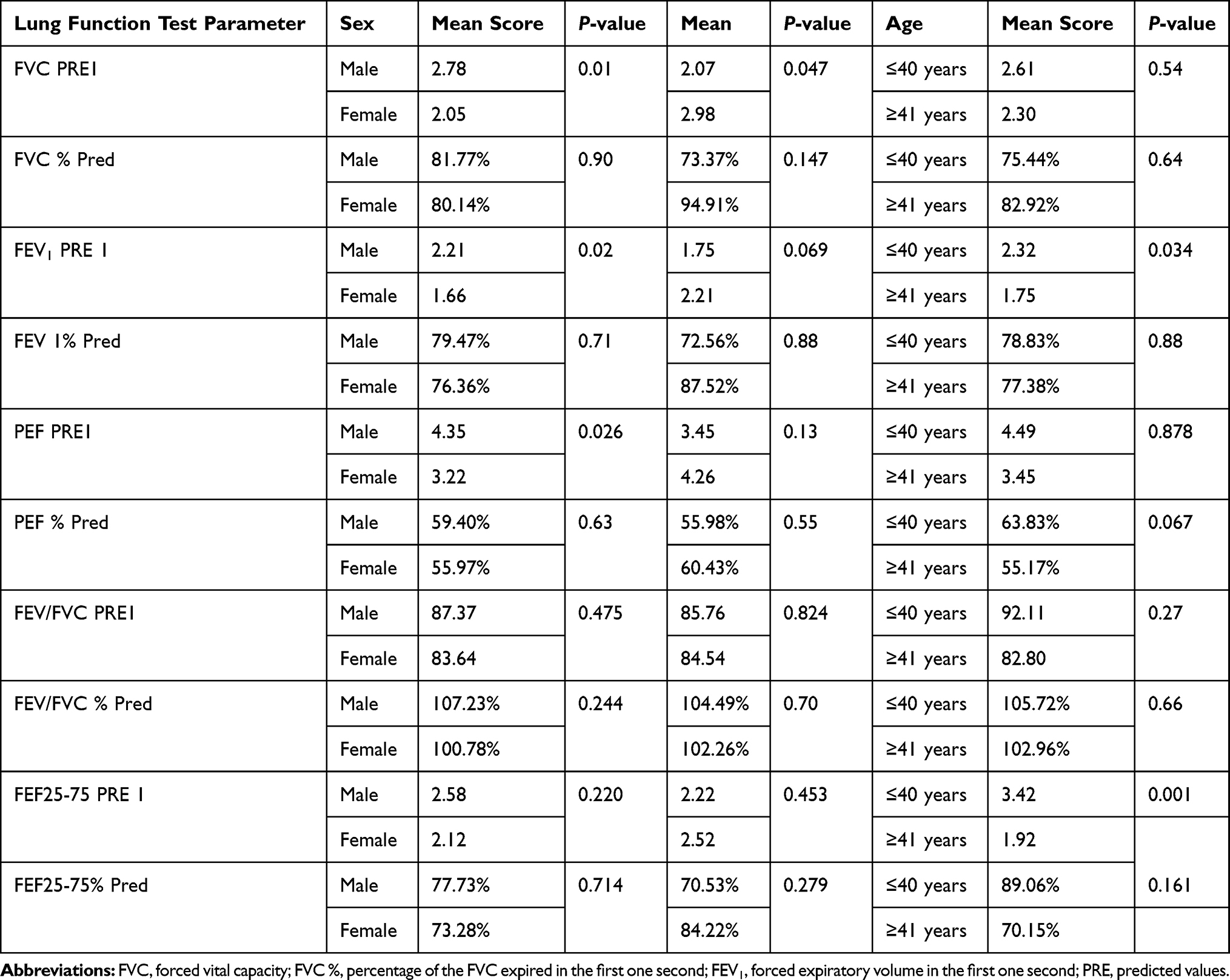 |
Table 2 The Mean Lung Function Parameters in Relation to Age and Sex Factors in AM-HDSS, Southern Ethiopia, 2020 |
Prevalence of Chronic Obstructive Pulmonary Disease
Among study participants 10.6% had chronic obstructive pulmonary disease. Among the participants who have cough 60.3% had duration of chronic cough less than 4 years, 29.31% had 4–10 years and rest had above 11 years. Of study participants who had chronic cough 62.1% had sputum and the rest 37.9% had dry cough. Coughing was worsens at night time which accounts for 32.76%, while 23.28% their cough worsened in day time. Among study participants 6% of them had shortness of breath and half of them had two years duration of shortness of breath (Table 3).
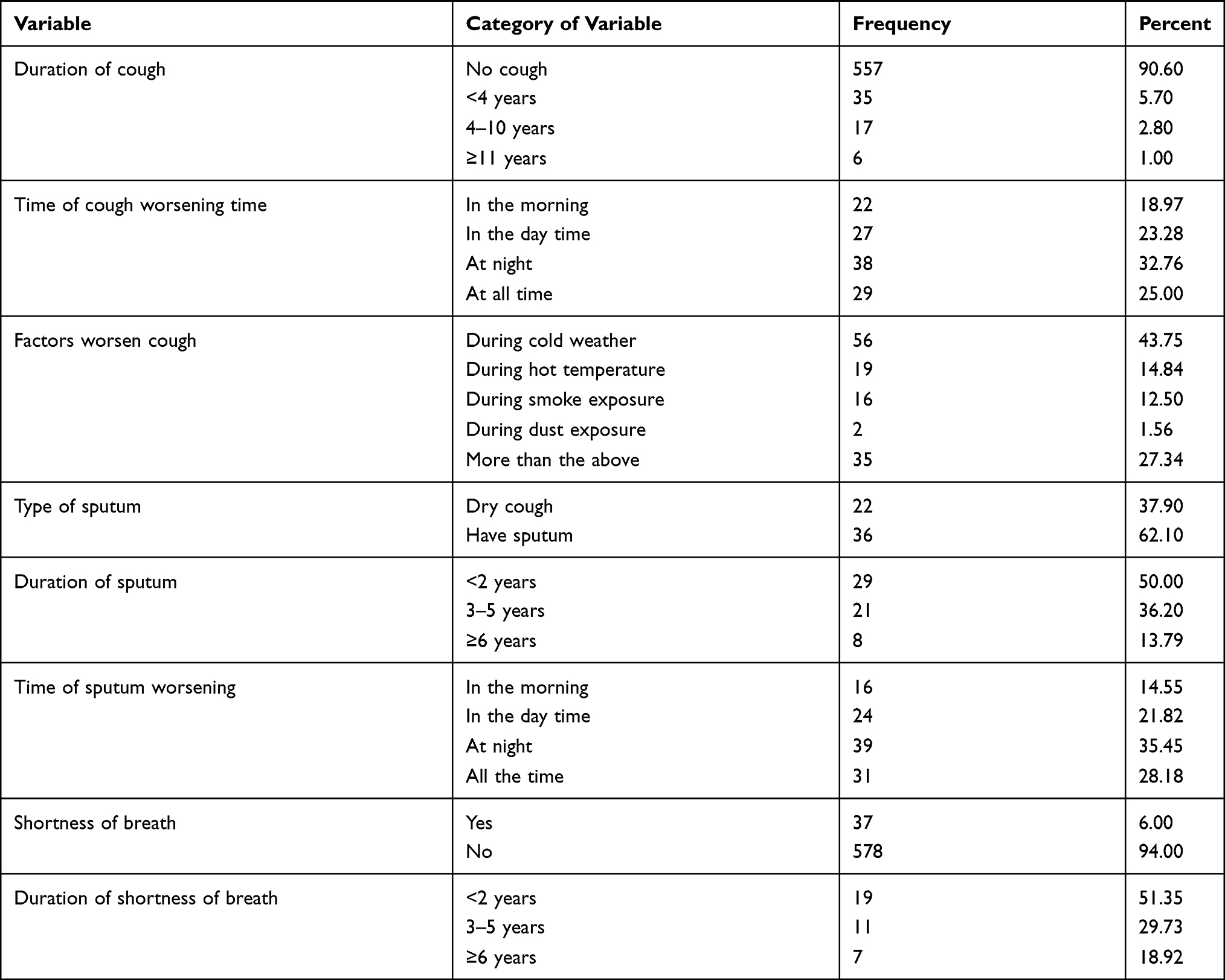 |
Table 3 Cough and its Characteristics Among Study Participants in AM-HDSS, Southern Ethiopia, 2020 |
Chronic Obstructive Pulmonary Disease and Housing Conditions
Relatively higher proportions of COPD cases existed in highland residence, which accounts for 63.8% compared to 36.2% lowland residence. In the case of housing type, 65.5% of COPD cases live in a traditional hut (tukulu). In addition, houses with no windows and one room had a relatively higher number of COPD cases compared to those which had windows and more than one room (Figure 2).
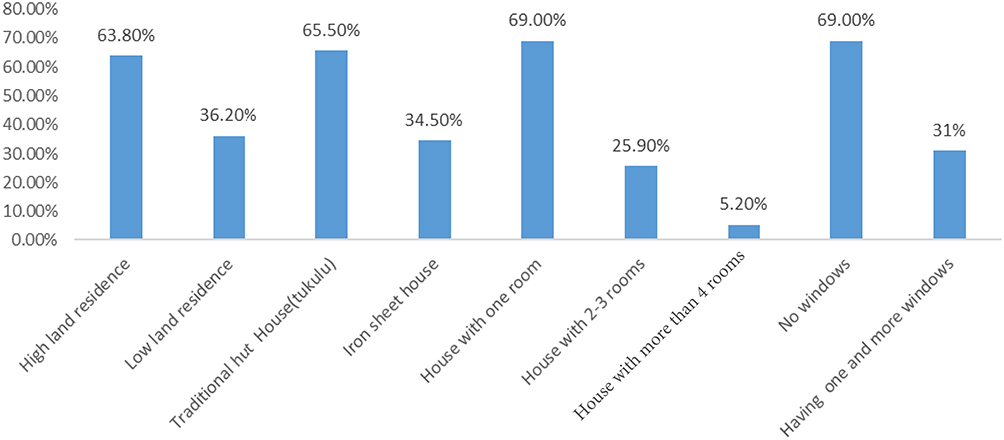 |
Figure 2 The relationship between housing condition and area of residence with COPD case, AM-HDSS, Southern Ethiopia, 2020. |
Factors Affecting Chronic Obstructive Pulmonary Disease
In binary logistic analysis factors like age ≥41 years COR 2.82 (1.65, 4.83), living in highland area 1.71 (1, 2.92), those who are elementary education 2.45 (1.13, 5.28), those who shares the house with domestic animals COR 2.34 (1.28, 4.28) and having a house that had no windows COR 1.75 (1.01, 3.05) were associated with chronic obstructive pulmonary disease.
Variables which have association in binary logistic analysis which had a P-value <0.3 were candidates for multivariable analysis. Finally, multivariable logistic regression analysis indicated that age ≥41 years AOR 3.65 (1.83, 7.28), living in highland area 1.71 (1, 2.92), those with elementary education level 2.45 (1.13, 5.28), who had no separate house for domestic animals AOR 2.84 (1.38, 5.85), having a house that had no windows AOR 3.05 (5.79, 1.12) and living in traditional hut (tukulu) AOR 5.92 (1.19, 29.42) were significantly associated with chronic obstructive pulmonary disease in the study area (Table 4).
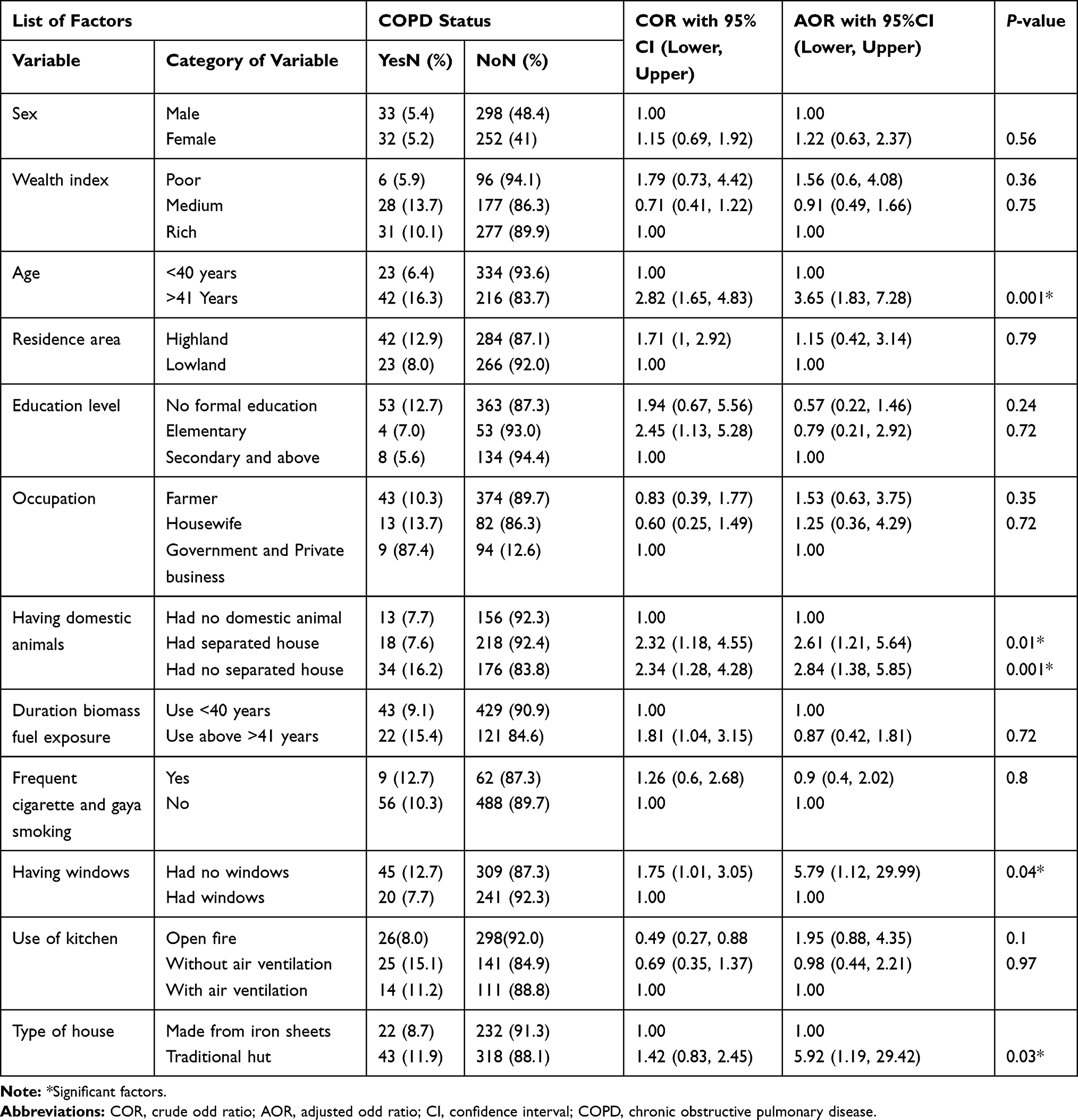 |
Table 4 Factors Associated with COPD AM-HDSSS, Southern Ethiopia, 2020 |
Discussion
In this study, the prevalence of spirometry-defined chronic obstructive pulmonary disease was 10.6%. This finding is comparable with previous studies conducted in Nepal (8.5%) and China (8%).13,14 The prevalence reported in this study is lower than the estimate from Ethiopia (17.8%) and Uganda (16.2%).9,12 The inconsistency in the prevalence estimates could be explained by the variation in the methods of estimation. This study defined COPD together with airflow obstruction and the presence of symptoms, while earlier studies defined COPD depending on airflow obstruction only and could be due to variations in study population, sample size, and differences in health-care systems.
Relatively the prevalence of COPD in participants who live in the highland area was 12.8% whereas it was 7.9% in the lowland area. This indicated that COPD is one of the chronic illnesses which cause respiratory morbidity in the study area especially in highland agro-ecology. This result is in line with a population-based observational study conducted in Kyrgyzstan and among pooled representative samples of adults in well-defined administrative areas worldwide.15,16 This may be due to the fact that the study participants who lived in a highland area utilized biomass fuel for long durations to heat the house. This biomass smoke exposure put the individuals at risk of developing COPD.17,18
The present study identified some factors which are strongly associated with COPD. Participants who are in advanced age >41 years (AOR 3.65; 1.83, 7.28) had more than 3.6 times developed COPD compared to those in the age range <40 years. This finding is consistent with the result of other studies,7 which reported that the frequency of COPD had a tendency to increase with age and old age is considered a risk factor for developing COPD.19,20 The effect of age with COPD may due more exposure to risk factors like biomass fuel, smoking and physiological decrease in respiratory function with age which begins around the age of 30–40 years.9,18 Study participants who had domestic animals and lack separate housing conditions (AOR 2.84) more likely developed COPD compared to those who had no domestic animals (AOR 1.38, 5.85). This effect is due to animal dung utilization for household food preparation and associated exposure to smoke and this leads to lung irritation and subsequently development of COPD.9,21
Residence who live in a highland area had (AOR 1.71; 1, 2.92) 1.7 times more likely developed COPD compared to those who live in a lowland area. This is due to the fact that study participants who live in a highland area almost all live in traditional huts and this housing type lacks windows for air circulation. As indicated in this study, participants who lived in traditional huts (tukulu) and who lack windows had significant contributing factors for development of COPD. The housing environment influences the physical and mental health of the inhabitants. Poor ventilation may increase exposure to smoke, which can lead to COPD. Indoor exposure to nitrogen dioxide (from poorly functioning combustion appliances) is the major factor affecting COPD.17,18
Conclusion and Recommendation
Chronic obstructive pulmonary disease (COPD) was one of the public health preventive respiratory illness in people who live in highland and traditional house who lack windows for air circulation. The identified contributing factors for COPD are modifiable factors such as lack of windows, those sharing houses with domestic animals and living in traditional huts (tukulu) and un-modifiable factor such as advanced age was also a significant contributing factor in the study area.
Therefore, improving housing condition of traditional huts by constructing windows for air circulation should be taken as a public health measure. In addition constructing separate a house for domestic animals and minimizing animal dung smoke exposure by improving air circulation in the house is mandatory to reduce respiratory illness. Due attention for individuals who are in advanced age should be given to avoid household smoke exposure.
Acknowledgments
The authors are grateful to Arba Minch University for providing this opportunity to conduct the research. We thank study participants for their genuine responses and participation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
2. Buist A, McBurnie M, Vollmer W, et al. International variation in the prevalence of COPD (the BOLD study): a population-based prevalence study. Lancet. 2007;370(9589):741–750. doi:10.1016/S0140-6736(07)61377-4
3. Rabe KF, Hurd S, Anzueto A, et al. Global initiative for chronic obstructive lung disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532–555. doi:10.1164/rccm.200703-456SO.
4. Ignatiev V, Titov O, Gultyaeva O. Chronic Obstructive Pulmonary Disease: Epidemiology and Economic Damage. Bulletin of St. Petersburg University; 2007:37–46.
5. Cruz AA. Global Surveillance, Prevention and Control of Chronic Respiratory Diseases: A Comprehensive Approach. World Health Organization; 2007.
6. Kurmi OP, Lam KBH, Ayres JG. Indoor air pollution and the lung in low-and medium-income countries. Eur Respiratory Soc. 2012;40(1):239–254. doi:10.1183/09031936.00190211
7. Musafiri S, van Meerbeeck J, Musango L, et al. Prevalence of atopy, asthma and COPD in an urban and a rural area of an African country. Respir Med. 2011;105(11):1596–1605. doi:10.1016/j.rmed.2011.06.013
8. Van Schayck C, Chavannes N. Detection of asthma and chronic obstructive pulmonary disease in primary care. Eur Respir J. 2003;21(39 suppl):16s–22s. doi:10.1183/09031936.03.00040403
9. Woldeamanuel GG, Mingude AB, Geta TG. Prevalence of chronic obstructive pulmonary disease (COPD) and its associated factors among adults in Abeshge District, Ethiopia: a cross sectional study. BMC Pulm Med. 2019;19(1):1–9. doi:10.1186/s12890-019-0946-z
10. Polatli M, Ben Kheder A, Wali S, et al. Chronic obstructive pulmonary disease and associated healthcare resource consumption in the Middle East and North Africa: the BREATHE study. Respir Med. 2012;106:S75–S85. doi:10.1016/S0954-6111(12)70016-1
11. Salvi S, Barnes PJ. Is exposure to biomass smoke the biggest risk factor for COPD globally? Chest. 2010;138(1):3–6. doi:10.1378/chest.10-0645
12. Van Gemert F, Kirenga B, Chavannes N, et al. Prevalence of chronic obstructive pulmonary disease and associated risk factors in Uganda (FRESH AIR Uganda): a prospective cross-sectional observational study. Lancet Glob Health. 2015;3:e44–51. doi:10.1016/S2214-109X(14)70337-7
13. Adhikari TB, Acharya P, Högman M, et al. Prevalence of chronic obstructive pulmonary disease and its associated factors in Nepal: findings from a community-based household survey. Int J Chron Obstruct Pulmon Dis. 2020;15:2319–2331. doi:10.2147/COPD.S268110
14. Zhong N, Wang C, Yao W, et al. Prevalence of chronic obstructive pulmonary disease in China: a large, population-based survey. Am J Respir Crit Care Med. 2007;176(8):753–760. doi:10.1164/rccm.200612-1749OC.
15. Brakema EA, Tabyshova A, Kasteleyn MJ, et al. High COPD prevalence at high altitude: does household air pollution play a role? Eur Respir J. 2019;53:1801193. doi:10.1183/13993003.01193-2018
16. Horner A, Soriano JB, Puhan MA, et al. Altitude and COPD prevalence: analysis of the PREPOCOL-PLATINO-BOLD-EPI-SCAN study. Respir Res. 2017;18:162. doi:10.1186/s12931-017-0643-5
17. Kanchongkittiphon W, Mendell MJ, Gaffin JM, Wang G, Phipatanakul W. Indoor environmental exposures and exacerbation of asthma: an update to the 2000 review by the Institute of Medicine. Environ Health Perspect. 2015;123(1):6–20. doi:10.1289/ehp.1307922
18. Nugmanova D, Sokolova L, Feshchenko Y, et al. The prevalence, burden and risk factors associated with bronchial asthma in commonwealth of independent states countries (Ukraine, Kazakhstan and Azerbaijan): results of the CORE study. BMC Pulm Med. 2018;18(1):110. doi:10.1186/s12890-018-0676-7
19. Sutradhar I, Das Gupta R, Hasan M, Wazib A, Sarker M. Prevalence and risk factors of chronic obstructive pulmonary disease in Bangladesh: a systematic review. Cureus. 2019;11(1):e3970. doi:10.7759/cureus.3970
20. Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet. 2007;370(9589):765–773. doi:10.1016/S0140-6736(07)61380-4
21. Behera D, Jindal SK. Respiratory symptoms in Indian women using domestic cooking fuels. Chest. 1991;100(2):385–388. doi:10.1378/chest.100.2.385
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.