Back to Journals » Vascular Health and Risk Management » Volume 19
Chronic Limb-Threatening Ischemia in Patients with Type 2 Diabetes: Revascularization Index as a Predictor for Primary Endovascular Intervention Outcome
Authors Shatnawi NJ, Al-Zoubi NA, Al-Bakkar LA ![]() , Abu-Baker AM
, Abu-Baker AM ![]() , Khader YS
, Khader YS ![]() , Al-Omari M, El-Heis MA
, Al-Omari M, El-Heis MA ![]()
Received 4 November 2022
Accepted for publication 21 June 2023
Published 31 July 2023 Volume 2023:19 Pages 495—504
DOI https://doi.org/10.2147/VHRM.S394521
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Harry Struijker-Boudier
Nawaf J Shatnawi,1 Nabil A Al-Zoubi,1 Lujain A Al-Bakkar,1 Ammar M Abu-Baker,1 Yousef S Khader,2 Mamoon Al-Omari,3 Mowafeq A El-Heis3
1Department of Surgery, Jordan University of Science and Technology, Irbid, Jordan; 2Department of Community Medicine, Public Health and Family Medicine, Jordan University of Science and Technology, Irbid, Jordan; 3Department of Radiology, Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Nawaf J Shatnawi, Department of Surgery, Jordan University of Science and Technology, P.O. Box 3030, Irbid, 22110, Jordan, Tel + 962 795576267, Email [email protected] Nabil A Al-Zoubi, Department of General Surgery/Vascular Surgery, Jordan University of Science and Technology, P.O. Box 3030, Irbid, 22110, Jordan, Tel + 962 795774637, Email [email protected]
Purpose: Chronic limb-threatening ischemia in patients with diabetes is associated with a high risk of adverse outcomes. The associated co-morbidities, the heterogeneity of foot presentation and the distribution of atherosclerotic lesions led to the emergence of multiple revascularization strategies and scoring systems to improve management outcomes. This study aimed to introduce a new index, the revascularization index (RI), and to assess its predictive value for the outcomes of primary endovascular intervention in patients with type 2 diabetes presenting with chronic limb-threatening ischemia.
Patients and Methods: A retrospective electronic medical records review was conducted for patients with type 2 diabetes presenting with chronic limb-threatening ischemia managed at King Abdullah University Hospital by primary endovascular interventions between January 2014 and August 2019. The RI was analyzed for its predictive value for the treatment outcomes.
Results: A total of 187 patients were included in this study, with a major lower limb amputation rate of 19.3%. The performance of the RI was excellent in predicting secondary revascularization (AUC = 0.80, 95% CI: 0.73– 0.86, p-value < 0.001), good to predict major amputation (AUC = 0.76, 95% CI: 0.67– 0.85, p-value = 0.047), and poor in predicting death (AUC = 0.46, 95% CI: 0.40– 0.55, p-value = 0.398). RI of < 1.21 was significantly associated with a higher risk of major lower limb amputation (HR = 5.8, 95% CI: 1.25– 26.97, p-value < 0.025), and RI of < 1.3 was associated with a higher risk for secondary revascularization.
Conclusion: The RI can be used to predict major adverse lower limb events (MALE). It might be used as a guide for the extent of endovascular interventions for diabetic chronic limb-threatening ischemia with multi-level outflow atherosclerotic disease.
Keywords: chronic limb-threatening ischemia, diabetes mellitus, angioplasty, amputation, revascularization index
Introduction
Peripheral arterial disease (PAD) is a common disease among patients with diabetes mellitus.1,2 The relative risk for PAD increases with the increasing duration of diabetes.3 Patients with both diabetes and PAD are at increased risk for adverse outcomes due to multiple co-morbidities, heterogeneous foot presentation, and multi-segmental and multi-level disease.4,5
Chronic limb-threatening ischemia (CLTI) is defined by clinical findings (rest pain and tissue loss) attributed to PAD.6,7 Diabetes mellitus is associated with a 2–4-fold increased risk of CLTI.7,8 Computed tomography angiography (CTA) is an adequate diagnostic tool for evaluation of and management planning for CLTI.9,10 Management of CLTI entails multidisciplinary approaches.7,11 Endovascular interventions became an accepted modality to treat CLTI in patients with type 2 diabetes in many centers.7,12
Revascularization for CLTI should be decided based on the patient’s risk assessment, foot clinical finding and the complexity of the occlusive lesions.7,8 The goal of surgical or endovascular revascularization for CLTI is to provide in-line blood flow to the foot through at least one patent artery.7,13 The angiosome concept was implied in the literature regarding the revascularization of an ischemic limb, but its value is still debated.7,12–14 The evidence is in favor of targeting more than one infra-genicular artery to improve endovascular revascularization outcomes for CLTI.15
Many classifications were described in the literature to assess PAD. Some classifications depend on clinical findings such as Fontaine and Rutherford classifications.6,7 In contrast, other systems have been developed based on the location and severity of atherosclerotic lesions using imaging modalities, such as the TASC II classification16 and the Bollinger angiographic score.17 Recently, the Society for Vascular Surgery (SVS) has proposed a new classification system for CLTI, based on the three main factors that increase the risk of amputation; Wound (W), Ischemia (I) and foot Infection (“fI”), called the SVS WIfI classification system. This system stratifies patients, predicts the risk of amputation and covers diabetic patients excluded from the definition of critical limb ischemia.7,18,19 However, none of the current classification systems address the appropriate extent of targeted lesions for endovascular revascularization, especially in multi-segmental outflow diseases.
The need for several systems to stratify diabetic patients with CLTI is justified by the heterogeneity of foot presentation, the presence of multiple modifiable and non-modifiable risk factors, and the different distributions of multi-segmental atherosclerotic lesions encountered in such patients.5–8 Therefore, its crucial to have an inclusive system for this heterogeneous clinical condition. We hypothesis that development of a new index, we called it the revascularization index (RI), can be of value in predicting the outcomes. This index is defined as the ratio of atherosclerotic severity before and after an endovascular intervention.
In this study, we aimed to introduce the RI and assess its predictive value for the outcomes of primary endovascular intervention (major lower limb amputation and secondary revascularization).
Materials and Methods
This is a retrospective review of medical records of patients with type 2 diabetes presenting with CLTI at King Abdullah University Hospital (KAUH). In KAUH, patients with type 2 diabetes presenting with CLTI who need hospital admission were admitted under the care of a vascular surgeon and handled by a multidisciplinary team for evaluation and management. This study included patients who had primary endovascular interventions in KAUH during the period from January 2014 to August 2019.
The study was approved by the Institutional Review Board of Jordan University of Science and Technology (26/108/2017). Consent to review patients’ medical records was not required by the Institutional Review Board of Jordan University of Science and Technology because the research involves minimal risk to the subjects and obtaining individual consent is not feasible. Measures were taken to ensure the confidentiality and privacy of patients’ data in accordance with the principles outlined in the Declaration of Helsinki.
After obtaining administrative and ethical approvals, the electronic medical records of included patients were reviewed. The following information was obtained from the records: demographic data (age and gender), history of co-morbidities (hypertension, end-stage renal disease on regular dialysis, hyperlipidemia, ischemic heart diseases), smoking status, clinical foot characteristics at presentation (SVS WIfI clinical stages), diagnostic CTA images and post endovascular interventional angiographic images. The dates of primary endovascular intervention, secondary revascularization, amputation, death and last follow-up were also extracted also from the medical records.
Patients were included in the study if they met the inclusion criteria: patients with type 2 diabetes presenting with symptoms of CLTI who are older than 40 years of age with ankle-brachial index (ABI) of ≤0.59 (SVS WIfI system ischemic grade 2 and 3). CTA (abdomen, pelvic and lower limb) was used for the diagnosis of PAD. Patients were included if they had endovascular intervention as the mean for primary revascularization. A total of 139 patients with type 2 diabetes with foot problems and ABI of ≥0.6 (grade 0 and 1 ischemia of SVS WIfI system) were excluded. As well, 85 patients with ABI of <0.59 were excluded for the following reasons: had no option for endovascular interventions (13 patients), underwent bypass (59 patients), had primary amputation (6 patients) as the primary treatment and had weakness of the affected lower limb due to stroke (7 patients).
Diagnostic CTA images and post primary endovascular interventional images were reviewed and scored by senior interventional vascular radiologists and senior vascular surgeons. CTA (abdomen, pelvic and lower limb angiography) images were created by multi-slice CTA scans using a 128-slice CT scanner (Ingenuity 128; Philips, Healthcare, Best, The Netherlands). Pre and post endovascular revascularization images were created by a bi-plane interventional X-ray system (Philips AlluraXper FD10/10 biplane system; Philips, Eindhoven, the Netherlands). Pre and post interventional angiogram images were transferred automatically to the picture archiving and communication system (PACS; Fuji, Japan) for interpretation and analysis.
The pre-revascularization atherosclerotic severity score (Pre-ASS) was calculated by summing the individual arterial atherosclerotic lesions scores depending on diagnostic CTA as shown below:
- A fully patent artery with smooth lining (Score 0)
- An artery with 1–30% diameter reduction (Score 1)
- An artery with 31–49% diameter reduction (Score 2)
- An artery with 50–99% diameter reduction (Score 3)
- A totally occluded artery (Score 4)
Each artery is scored in accordance with its most severe atherosclerotic lesion (highest score), whether it is single, multiple, short or long. Any artery with a score of 3 or 4 is considered to have hemodynamic relevant atherosclerotic lesion (HRAL) which was assessed for feasibility of endovascular interventions guided by TASC II classification. Primary endovascular interventions were tried in all TASC II grade A, B and C. Patients with high risk TASC II grade D were offered an attempt of primary endovascular option as well.
The post revascularization score (Post-ASS) was calculated by summing individual arterial diagnostic CTA scores of non-targeted lesions and the sum of the scores of post vascularized targeted lesions according to post interventional images. The Post-ASS for targeted arteries was calculated by reviewing the post revascularization images in the following way:
- An artery with successful intervention (Score 1).
- An artery with successfully treated dissection or with residual narrowing of less than 50% diameter reduction following intervention (Score 2)
- A HRAL which failed to be treated retains its pre-ASS.
- Any artery/arteries which developed occlusion as a complication of the endovascular intervention is scored 4 for each if not treated, otherwise it is scored accordingly.
The RI was calculated by dividing the Pre-ASS by the Post-ASS (RI = pre-ASS / post-ASS).
A hemodynamic successful endovascular intervention is defined as an improved ABI by ≥0.15 on the next day following the procedure and the clinical success is defined by the main outcome parameters in the follow-up period. All patients receive intravenous therapeutic heparin for 24 hours post intervention and anti-platelets lifelong.
The main outcome parameters for primary endovascular interventions were: secondary endovascular/conventional revascularization, major amputation, and patient death during the follow-up period. Secondary revascularization was defined as any revascularization procedure after the primary endovascular intervention regardless whether due to recurrence at the targeted lesion, progression of atherosclerotic disease of any artery and to deal with untargeted outflow lesions at the primary endovascular intervention. Any amputation that preserved an intact weight bearing heel was considered minor.
Statistical analysis was performed using IBM SPSS Version 24. Data were described using means and percentages. Kaplan–Meier survival analysis was used to calculate 6-month, 1-year, 2-year and 5-year rates of secondary angioplasty, major amputation and death. The Receiver Operating Characteristic (ROC) curve was used to assess the predictive power of RI and to calculate the area under the curve which is equivalent to C-Statistics. Cox regression analysis was conducted to determine the association between study outcomes and RI and Pre-ASS after adjusting for age, gender, hypertension and hyperlipidemia. The RI and Pre-ASS were categorized to be tested in Cox regression analysis. A p-value of less than 0.05 was considered statistically significant.
Results
This study included 187 patients (140 males and 47 females) with a mean (±SD) age of 63.37 (±11.3) years. The mean (SD) duration of diabetes was 12.23 (4.07) years and the mean (SD) HbA1c was 8.68% (2.05%) Table 1. A total of 133 patients (71.1%) had history of hypertension, 125 patients (66.8%) were smokers and 43.3% of patients had SVS WIfI clinical stage 4 (high risk stage). Smoking was significantly associated with amputation (p < 0.002) and secondary revascularization. The outcome measures according to comorbidities and WIfI clinical stages of patient’s feet are shown in Table 2.
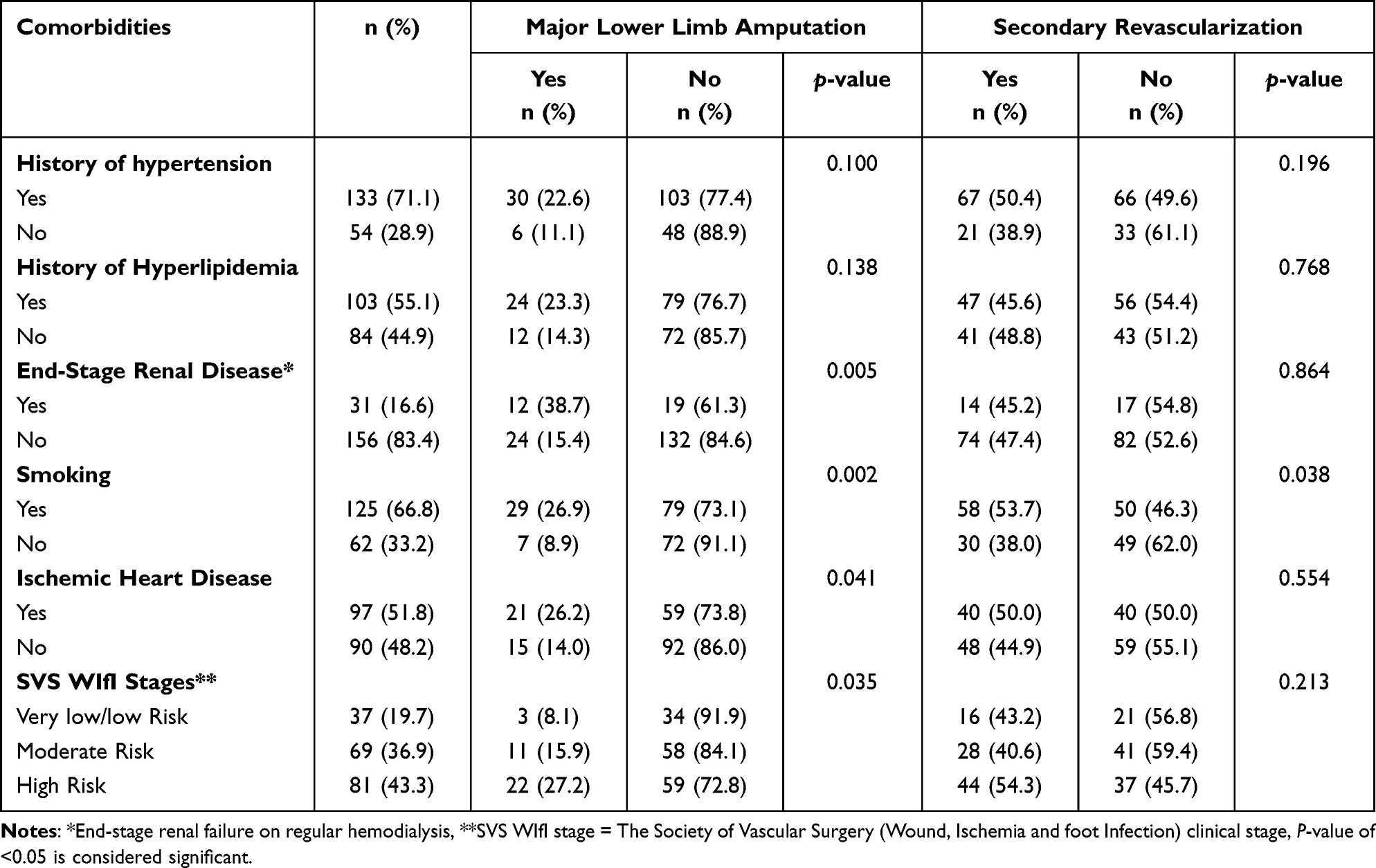 |
Table 1 Major Lower Limb Amputation and Secondary Revascularization According to Co-Morbidities and WIfI Clinical Stages |
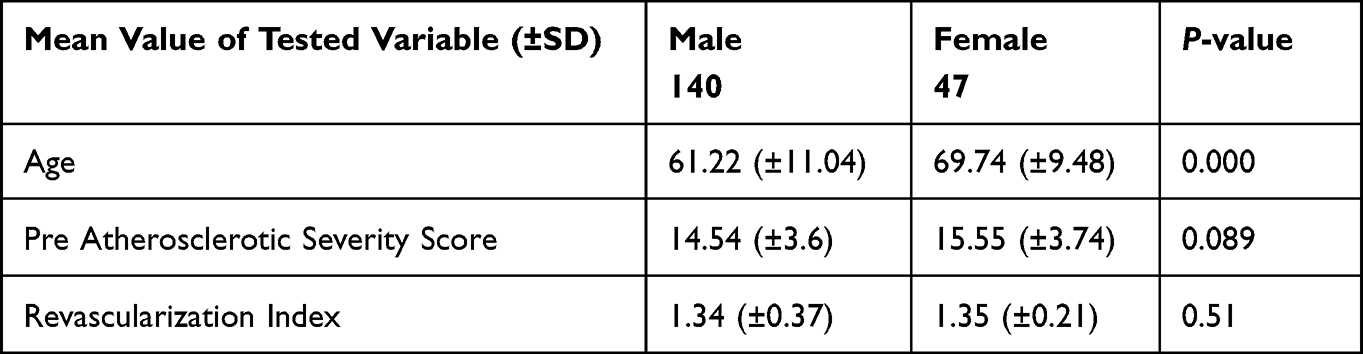 |
Table 2 Gender Variations in Relation to the Mean Values of Age, Pre-Atherosclerotic Severity Scores and the Revascularization Index |
The anatomical distribution of HRAL showed multi-segmental disease with a distal pattern. Involvement of the distal segment (distal to adductor hiatus) was found in 41.2% of patients, involvement of the proximal segment (proximal to adductor hiatus) was found in 11.7% of patients, and both distal and proximal segments were involved in 47.1% of patients.
The posterior tibial artery (PTA) was involved with HRAL in 103 patients (55.1%), while the superficial femoral artery (SFA) was involved in 84 patients (44.9%). Primary endovascular intervention targeted the superficial femoral artery in 76 patients (40.6%), and the popliteal artery was targeted in 65 patients (34.8%). Of the 187 patients, 64 patients (34.2%) had their endovascular interventions for proximal segment only, and 78 patients (41.7%) had their endovascular interventions for distal segment only, while 45 patients (24.1%) had intervention for both proximal and distal segments. The distribution of arterial atherosclerotic lesions and frequency of intervention in each artery are shown in Table 3.
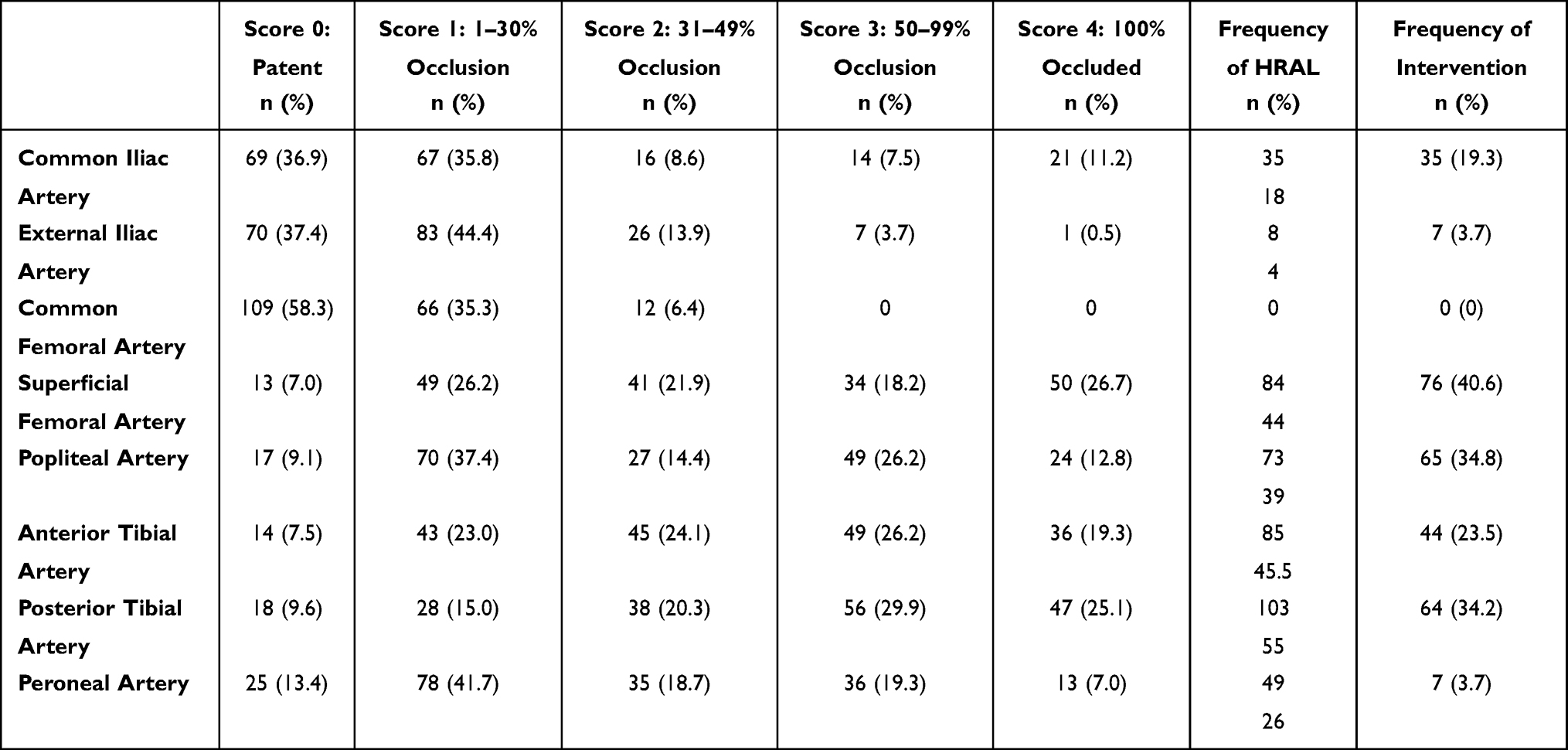 |
Table 3 Distribution of Atherosclerotic Lesions in the Arteries and the Frequency of Intervention in Each Artery |
The range of follow-up duration was 5 to 67 months. The mean (SD) follow-up duration was 24.1 (13.8) months for secondary revascularization, 27.1 (13.7) months for major amputation and 29.7 (12.7) months for patient’s death. Almost 47.1% of patients needed secondary revascularization, 19.3% underwent major amputation and 21.9% of patients died during the follow-up period.
Table 4 shows 6-month, 1-year, 2-year and 5-year rates of secondary revascularization, major amputation, and death. The median (95% CI) time to death was 52.0 months (95% CI: 44.5–59.5), to major amputation was 50.2 months (95% CI: 46.2–54.2), and to secondary revascularization was 34.0 months (95% CI: 26.2–41.8). The need for secondary revascularization was 8.1%, 15.7% and 86.4% at 6 months, 1 year and 5 years, respectively. The major amputation rate was 5.9%, 8.6% and 45.1% at 6 months, 1 year and 5 years, respectively. The five-year mortality rate was 73.2%.
 |
Table 4 The 6 Month, 1-Year, 2-Year, and 5-Year Rates of Secondary Revascularization, Major Amputation, and Death |
Patients who underwent secondary revascularization had a significantly lower revascularization index (RI) mean compared to those who did not need secondary revascularization (1.25 ± 0.14 vs 1.45 ± 0.25, p < 0.001). Moreover, patients with major amputation had a significantly lower RI mean (1.25 ± 0.21) compared to those without major amputation (1.39 ± 0.22). Patients who died within the follow-up period had an RI mean of 1.36 ± 0.23, and patients who survived during the follow-up period had an RI mean of 1.36 ± 0.19.
To assess the predictive power of the RI, the ROC curve was used to calculate the AUC. The performance of RI was excellent in predicting secondary revascularization (AUC = 0.80, 95% CI: 0.73–0.86, p-value < 0.001), good to predict major amputation (AUC = 0.76, 95% CI: 0.67–0.85, p-value = 0.047), and poor in predicting death (AUC = 0.46, 95% CI: 0.40–0.55, p-value = 0.398).
Table 5 shows the association of the RI and Pre-ASS with the studied outcome parameters in the Cox proportional-hazards model. The RI was not significantly associated with death. The hazard of amputation for patients with RI <1.21 was 6 times higher than that for patients with revascularization index ≥1.5 (HR = 5.8, 95% CI: 1.25–26.97, p = 0.025). Decreased RI was significantly associated with increased hazards of secondary revascularization. Having a pre-ASS score of 12–13.9 was associated with decreased hazards of amputation by 79% when compared to a score ≥17.
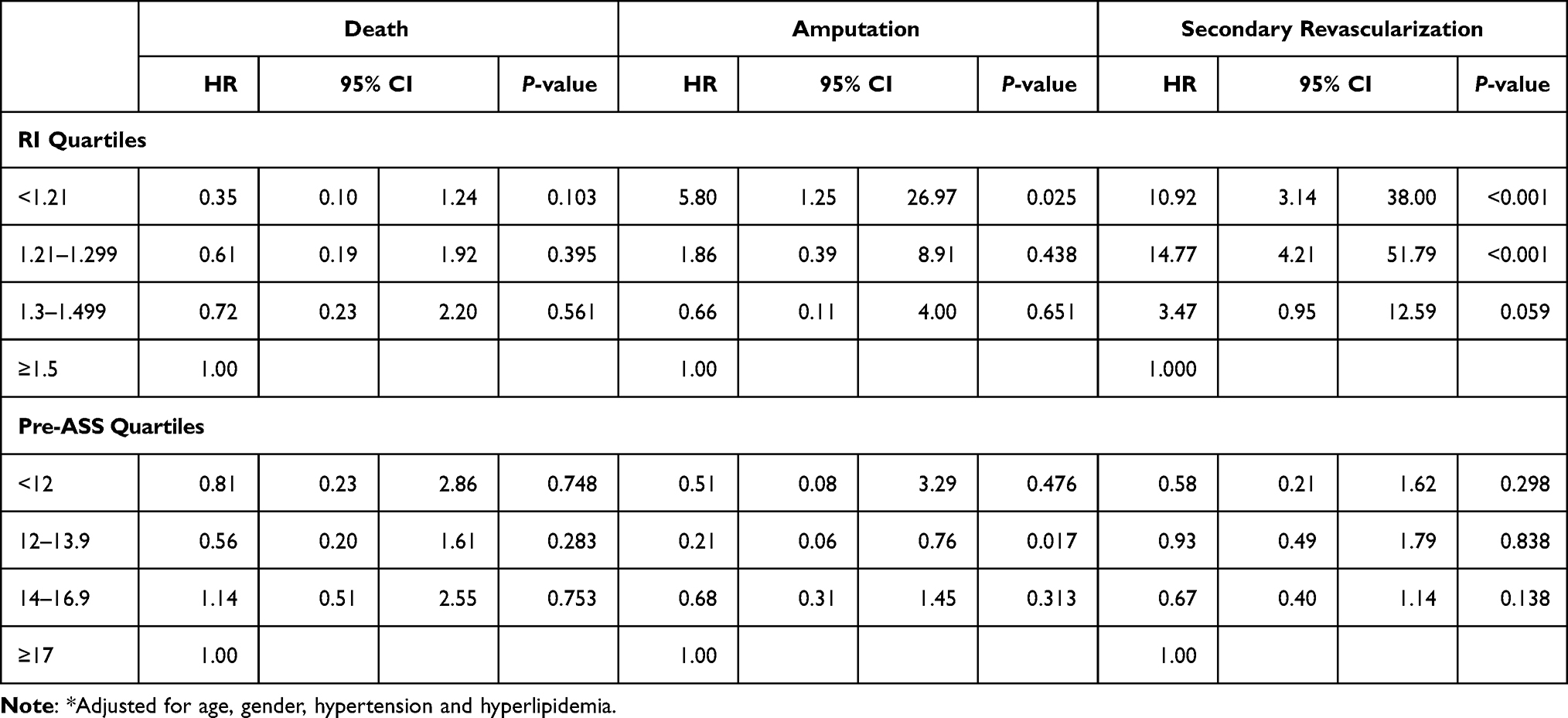 |
Table 5 The Association of Revascularization Index (RI) and Pre-Revascularization Atherosclerotic Severity Score (Pre-ASS) with the Outcome Parameters in the Cox Proportional-Hazards Model* |
Discussion
In this study group, the majority of patients were males who were significantly younger than the females. This is consistent with global data that symptomatic PAD presents more commonly and earlier in males. PAD presents in females at older age with severe ischemic symptoms, due to the protective hormonal and metabolic effects in the pre-menopausal stage.2,20–22 The majority of patients in this study had one or more other co-morbidities. It is well established that diabetes mellitus with PAD is associated with other cardiovascular complications due to the common shared risk factors.6–8
Smoking was frequent in this study group, with a significant association between smoking and amputation and secondary revascularization. Smoking increases the risk of PAD by several-fold.1,23 In a recent meta-analysis, smoking was found to increase the risk of diabetic foot amputation (OR=1.65, 95% CI, 1.09–2.50, P< 0.0001) compared with the non-smoking population.24 End-stage renal disease on regular dialysis had a significant association with the risk of major amputation; consistent with previous evidence that end-stage renal diseases with concurrent diabetes mellitus increases the risk of amputation.25,26 There was a significant association between major amputations and increasing SVS WIfI clinical stage. An increased rate of amputation was reported with increased clinical stage of SVS WIfI classification system.7,18,27
The distribution of diseased vessels before endovascular interventions shows a more distal predominance, consistent with the fact that the diabetic patients have a pattern of extended infra-genicular disease, often associated with SFA lesions (inflow disease).28 It is known that diabetes mellitus is most strongly associated with femoral-popliteal and tibial (below the knee) PAD.7,29
The need for secondary revascularization in the first 6 months in our sample was 8.1%. The CLTI recurrence rate is emphasized in recent literature. The secondary revascularization rate following primary endovascular intervention for CLTI is variable depending on the targeted segment and the modality of treatment.30–32 Faglia et al reported in a prospective study that 8.8% of patients needed secondary revascularization after primary endovascular intervention for CLTI.33 Meloni et al reported that 24.3% of patients had clinical recurrence that mandates secondary revascularization in a median time of 3.5±0.6 months. They concluded that poor glycemic control and end-stage renal disease are independent predictors for relapse of CLTI after PTA.26 Others reported a recurrence rate of 9.6% for clinical CLTI which needed secondary revascularization within 20 months.34
According to our study, the major lower limb amputation rate was 5.9% in the first 6 months, compared with a reported major amputation rate of 27% in the first 6 months following infra-popliteal intervention for CLTI in diabetic patients.34 This low 6-month amputation rate might be explained by the high proportion of proximal segment intervention in the study group (34.2%). The five-year mortality rate was 73.2%, consistent with the fact that patient mortality rate increases yearly upon diagnosis of CLTI, typically exceeding 50% after 5 years.35 The relatively high 5-year mortality in our patients is explained by the existing comorbidities and poor diabetic control. Patients with type 2 diabetes presenting with CLTI are often elderly, suffer from multiple co-morbidities and they have more severe atherosclerotic multi-segmental disease.4,5,35
Due to high prevalence of below-the-knee disease in diabetic patients, some studies reported worse outcome for endovascular interventions in diabetic patients with CLTI.36 However, other studies have suggested that diabetic patients with adequate distal runoff appear to have patency rates comparable to that of non-diabetic individuals.26,29,33,37 Thus, and due to the heterogeneity and complexity of disease distribution and presentation, the approach for revascularization in CLTI in diabetic patients has always been a debate. However, an “endovascular first approach” is an accepted modality in treating CLTI in many centers.7,12,31 Taylor and Palmer were the first to emphasize the role of the angiosome concept in plastic and reconstructive field.38 The utility of angiosome in management of ischemic diabetic foot has been demonstrated, especially in diabetic patients with CKD.30,39–41 However, recent studies demonstrated the superiority of revascularization for CLTI using venous conduit.42
Direct revascularization of the ischemic angiosome should be considered whenever possible.43 On the other hand, Faglia et al stated that angioplasty in diabetic patients with infra-genicular lesions with poor run-off at the foot and/or high surgical risk can be treated with endovascular modality, achieving an acceptable outcome.44,45
Our study showed an excellent and good predictive power for the RI to predict secondary revascularization and major lower limb amputation, respectively. Our study showed a significant association between RI <1.21 and the risk of major lower limb amputation (HR 5.80, 95% CI 1.25–26.97, p < 0.025). RI <1.30 was also significantly associated with the need for secondary revascularization in diabetic patients with CLTI undergoing primary angioplasty. The RI reflects endovascular radiological success, the more arteries that had successful revascularization will result in a higher index, in contrast, more HRAL of outflow arteries left with no interventions leads to lower RI. Bear in mind that successful endovascular revascularizations of more than one infra-genicular arterial lesion were associated with superior outcomes.15 Based on the above-mentioned evidence, there are multiple strategies for CLTI managements, however, currently there is no single scientific evidence to indicate which strategy is ideal for treating CLTI associated with multi-segmental disease including infra-genicular involvement.7,30,41
Current classification systems help in grading severity of foot problem in diabetic patients rather than aiding in planning revascularization.6,7 The WIfI classification predicts the risk of amputation and the need for revascularization, but tells little about the appropriate extent of targeted outflow arteries for endovascular interventions in diabetic patients.7,41 The global anatomic staging system (GLASS) assesses the severity of hemodynamic relevant atherosclerotic lesions of the femoro-popliteal and crural (infra-genicular) segments to achieve continuous in-line blood flow to the ankle through targeting the least disease infra-genicular artery for endovascular interventions.7 The impact of this classification system in clinical practice has to be evaluated.
A classification system that homogenizes the atherosclerotic burden and predicts the outcome of intervention is needed. The RI gives weight to all atherosclerotic lesions at different levels, measures the degree of success of intervention, and predicts the outcome of revascularization. In addition, it might guide vascular surgeons and interventional radiologists in selecting the targeted arteries for endovascular interventions in multi-level disease in order to achieve a higher revascularization index that might improve the outcome. The Pre-ASS and the RI might also be used to assess severity of atherosclerotic disease and compare the degree of success of endovascular interventions in different patient series, especially with concomitant inflow and outflow disease.
Limitations
This is a retrospective study which might be liable to confounding and misclassification bias. We also did not consider the length of HRAL and the multiplicity of HRAL in each artery in the calculation process of the RI. Giving a score of 3 for lesions with a range of (50–99%) narrowing might be wide. The retrospective nature of the study makes difficult to assess the relation of the RI to wound healing time.
Conclusions
The RI can predict major adverse lower limb events (MALE). It might be used as a guide for the extent of endovascular interventions for diabetic CLTI with multi-level outflow atherosclerotic disease. We propose calculating the RI before performing endovascular interventions for CLTI in type 2 diabetic patients presenting with inflow and outflow diseases. This might help the surgeons and interventional radiologists to target several outflow arteries for endovascular interventions to achieve a higher revascularization index. Further prospective analysis and studies are needed.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Song P, Rudan D, Zhu Y, et al. Global, regional and national prevalence and risk factors for peripheral artery disease in 2015: an updated systematic review and analysis. Lancet Glob Health. 2019;7(8):e1020–e1030. doi:10.1016/S2214-109X(19)30255-4
2. Chase-Vilchez AZ, Chan IHY, Sanne AE, Peters SAP, Woodward M. Diabetes as a risk factor for incident peripheral arterial disease in women compared to men: a systematic review and meta-analysis. Cardiovasc Diabetol. 2020;19:151.
3. Al-Delaimy WK, Merchant AT, Rimm EB, Willett WC, Stampfer MJ, Hu FB. Effect of type 2 diabetes and its duration on the risk of peripheral arterial disease among men. Am J Med. 2004;116(4):236–240. doi:10.1016/j.amjmed.2003.09.038
4. Marso SP, Hiatt WR. Peripheral arterial disease in diabetic patients. J Am Coll Cardiol. 2006;47(5):921–929. doi:10.1016/j.jacc.2005.09.065
5. Davies MG. Critical limb ischemia: epidemiology. Methodist DebakeyCardiovasc J. 2012;8(4):
6. Hardman RL, Jazaeri O, Yi J, Smith M, Gupta R. Overview of classification systems in peripheral artery disease. SeminIntervent Radiol. 2014;31(4):378–388.
7. Conte MS, Bradbury AW, Kolh P, et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. Eur J Vasc Endovasc Surg. 2019;58(1):s109–s133.
8. Barnes JA, Eid MA, Creager MA, Goodney PP. Epidemiology and risk of amputation in patients with diabetes mellitus and peripheral artery disease. Arterioscler Thromb Vasc Biol. 2020;40(8):1808–1817. doi:10.1161/ATVBAHA.120.314595
9. Met R, Bipat S, Legemate DA, Reekers JA, Koelemay MJ. Diagnostic performance of computed tomography angiography in peripheral arterial disease: a systematic review and meta-analysis. JAMA. 2009;301(4):415–424. doi:10.1001/jama.301.4.415
10. Firnhaber J, Powell CS. Lower extremity peripheral artery disease diagnosis and treatment. Am Fam Physician. 2019;99(6):362–369.
11. Topfer LA, Spry C. New technologies for the treatment of peripheral artery disease. 2018 April 1. In: CADTH Issues in Emerging Health Technologies. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2016:172. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519606/.
12. Kinlay S. Management of Chronic limb-threatening ischemia. Circ Cardiovasc Interv. 2016;9(2):e001946.
13. Gerhard-Herman MD, Gornik HL, Barrett C, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2017;135(12):e686–e725. doi:10.1161/CIR.0000000000000470
14. Van den Berg JC. Angiosome perfusion of the foot: an old theory or a new issue? Semin Vasc Surg. 2018;31(2–4):56–65. doi:10.1053/j.semvascsurg.2018.12.002
15. Biagioni RB, Biagioni LC, Nasser F, et al. Infra popliteal angioplasty of one or more than one artery for critical limb ischemia: a randomized clinical trial. Eur J Vasc Endo Vascular Surg. 2018;55(4):518–527. doi:10.1016/j.ejvs.2017.12.022
16. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG; TASC II Working Group. Inter-Society Consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007;45(Suppl S):S5–S67. doi:10.1016/j.jvs.2006.12.037
17. Bollinger A, Breddin K, Hess H, et al. Semi quantitative assessment of lower limb atherosclerosis from routine angiographic images. Atherosclerosis. 1981;38(3–4):339–346. doi:10.1016/0021-9150(81)90050-2
18. Cerqueira LO, Duarte Júnior EG, Barros ALS, Cerqueira JR, Araújo WJB. WIfI classification: the Society for Vascular Surgery lower extremity threatened limb classification system, a literature review. J Vasc Bras. 2020;19:e20190070. doi:10.1590/1677-5449.190070
19. Mills JL Sr, Conte MS, Armstrong DG, et al. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: risk stratification based on wound, ischemia, and foot infection (WIfI). J Vasc Surg. 2014;59:220–234.e1–2.
20. Srivaratharajan K, Abramason B. Women and peripheral arterial disease: a review of sex differences in epidemiology, clinical manifestations and outcome. Can J Cardiol. 2018;34:356–361.
21. Stefanska A, Sypniewskay G, Senterkiewicz L. Inflammatory markers and cardiovascular risk in healthy Polish women across the menopausal transition. Clin Chem. 2005;51(10):1893–1895. doi:10.1373/clinchem.2005.052191
22. Teodorescu VJ, Vavra AK, Kibbe MR. Peripheral arterial disease in women. J Vasc Surg. 2013;57(4):18s–26s. doi:10.1016/j.jvs.2012.10.115
23. Lu JT, Creager MA. The relationship of cigarette smoking to peripheral arterial disease. Rev Cardiovasc Med. 2004;5(4):189–193.
24. Liu M, Zhang W, Yan Z, Yuan X. Smoking increase the risk of diabetic foot amputation: a meta-analysis. ExpTher Med. 2018;15(2):1680–1685.
25. Gilhotra RA, Rodrigues BT, Vangaveti VN, Malabu UH. Prevalence and risk factors of lower limb amputation in patients with end-stage renal failure on dialysis: a systematic review. Int J Nephrol. 2016;ID 4870749:7. doi:10.1155/2016/4870749
26. Meloni M, Izzo V, Giurato L, et al. Recurrence of chronic limb-threatening ischemia after endovascular intervention in patients with diabetic foot ulcers. Adv Wound Care. 2018;7(6):171–176. doi:10.1089/wound.2017.0778
27. Darling JD, McCallum JC, Soden PA, et al. Predictive ability of the SVS WIfI classification system following first-time lower extremity revascularizations. J Vasc Surg. 2017;65(3):695–704. doi:10.1016/j.jvs.2016.09.055
28. Aboyansa V, Riccoa J-B, Bartelinka MLEL. 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2018;55:305–368.
29. Thiruvoipati T, Kielhorn CE, Armstrong EJ. Peripheral artery disease in patients with diabetes: epidemiology, mechanisms, and outcomes. World J Diabetes. 2015;6(7):961–969. doi:10.4239/wjd.v6.i7.961
30. Gutierrez MI, Vicente S, Criado F, et al. Below-the-Knee revascularization of critical limb ischemia in diabetic patients. Vasc Dis Manag. 2020;17(7):e150–e154.
31. Meecham L, Bate G, Patel S, Bradbury AWA. Comparison of clinical outcomes following femoropopliteal bypass or plain balloon angioplasty with selective bare metal stenting in the bypass versus angioplasty in severe ischemia of the limb (BASIL). Trial Eur J Vasc Endovasc Surg. 2019;58:52–59.
32. Biscetti F, Nardella E, Rando MM, et al. Review outcomes of lower extremity endovascular revascularization: potential predictors and prevention strategies. Int J Mol Sci. 2021;2002. doi:10.3390/ijms22042002
33. Faglia E, Paola LD, Clerici G, et al. Peripheral angioplasty as the first-choice revascularization procedure in diabetic patients with critical limb ischemia: prospective study of 993 consecutive patients hospitalized and followed between 1999 and 2003. Eur J Vasc Endovasc Surg. 2005;29(6):620–627. doi:10.1016/j.ejvs.2005.02.035
34. Spreen MI, Martens JM, Hansen BE, et al. Percutaneous transluminal angioplasty and drug eluting stents for infrapopliteal lesions in critical limb ischemia (PADI) trial. Circ Cardiovasc Interv. 2016;9(2):e002376. doi:10.1161/CIRCINTERVENTIONS.114.002376
35. Duff S, Mafilios MS, Bhounsule P, Hasegawa JT. The burden of chronic limb-threatening ischemia: a review of recent literature. Vasc Health Risk Manag. 2019;15:187–208. doi:10.2147/VHRM.S209241
36. Sumpio BE, Forsythe RO, Ziegler KR, van Baal JG, Lepantalo MJA, Hinchliffe RJ. Clinical implications of the angiosome model in peripheral vascular disease. J Vasc Surg. 2013;58(3):814–826. doi:10.1016/j.jvs.2013.06.056
37. Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis: epidemiology, pathophysiology, and management. JAMA. 2002;287(19):2570–2581. doi:10.1001/jama.287.19.2570
38. Taylor GI, Palmer JH. The vascular territories (angiosomes) of the body: experimental study and Clinical applications. Br J Plast Surg. 1987;40(2):113–141. doi:10.1016/0007-1226(87)90185-8
39. Attinger CE, Evans KK, Bulan E, Blume P, Cooper P. Angiosomes of the foot and ankle and clinical implications for limb salvage: reconstruction, incisions, and revascularization. Plast Reconstr Surg. 2006;117(suppl 7):261S–293S. doi:10.1097/01.prs.0000222582.84385.54
40. Uccioli L, Meloni M, Izzo V, Giurato L, Merolla S, Gandini R. Critical limb ischemia: current challenges and future prospects. Vasc Health Risk Manag. 2018;2018:14 63–74.
41. Biancari F, Juvonen T. Angiosome-targeted lower limb revascularization for ischemic foot wounds: systematic review and meta-analysis. Eur J VascEndovasc Surg. 2014;47(5):517–522. doi:10.1016/j.ejvs.2013.12.010
42. Farber A, Menard MT, Conte MS, et al. Surgery or endovascular therapy for chronic limb-threatening ischemia. N Engl J Med. 2022;387(25):2305–2316. doi:10.1056/NEJMoa2207899
43. ShKabra A, Suresh KR, Vivekanand V. Outcomes of angiosome and non-angiosome targeted revascularization in critical lower limb ischemia. J Vasc Surg. 2013;57(1):44–49. doi:10.1016/j.jvs.2012.07.042
44. Faglia E, Clerici G, Scatena A, et al. Severity of demographic and clinical characteristics, revascularization feasibility, major amputation, and mortality rate in diabetic patients admitted to a tertiary diabetic foot center for critical limb ischemia: comparison of 2 cohorts recruited at a 10-year distance. Ann Vas Surg. 2014;28(7):1729–1736.
45. Uccioli L, Gandini R, Giurato L, et al. Long-term outcomes of diabetic patients with critical limb ischemia in diabetic foot patients followed in a tertiary referral diabetic foot clinic. Diabetes Care. 2010;33(5):977–982. doi:10.2337/dc09-0831
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.