Back to Journals » Veterinary Medicine: Research and Reports » Volume 10
Chronic Enteropathy In Canines: Prevalence, Impact And Management Strategies
Authors Dandrieux JRS, Mansfield CS
Received 22 March 2019
Accepted for publication 8 September 2019
Published 6 December 2019 Volume 2019:10 Pages 203—214
DOI https://doi.org/10.2147/VMRR.S162774
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Young Lyoo
Video abstract of 'Chronic enteropathy in canines' [ID 162774]
Views: 578
Julien Rodolphe Samuel Dandrieux , Caroline Sarah Mansfield
Department of Veterinary Clinical Sciences, Melbourne Veterinary School, Faculty of Veterinary and Agricultural Sciences, University of Melbourne, Werribee, Victoria, Australia
Correspondence: Julien Rodolphe Samuel Dandrieux
Department of Veterinary Clinical Sciences, Melbourne Veterinary School, Faculty of Veterinary and Agricultural Sciences, University of Melbourne, Werribee, Victoria, Australia
Email [email protected]
Abstract: In this article, the studies about the prevalence of chronic enteropathy are reviewed as well as the information regarding short- and long-term prognosis for dogs treated with the three most common therapies; these include dietary modification, antibiotics, and immunosuppressants. Although the data available are limited, most studies support a good to excellent long-term response in dogs that have a successful food trial, whereas the response is poor with antibiotics or on-going treatment is required to retain remission. There is a risk of antimicrobial resistance developing with inappropriate use of antimicrobials such as in these situations. The published information highlights the need for alternative strategies to antibiotic treatment to manipulate the GI microbiome, and in the final part of this article studies on the use of probiotic for the treatment of chronic enteropathy are reviewed.
Keywords: chronic enteropathy, inflammatory bowel disease, dog, treatment, probiotic, diet
Plain Language Summary
Chronic vomiting and diarrhoea are common clinical signs in dogs, but as we review in this article, there is little information on how frequent this problem really is both in general or referral veterinary practice.
Furthermore, of the three main treatment options, including change of diet, treatment with antibiotics or immune suppressive drugs, only dogs responding to a diet change have a long-term response. This highlights the need for new strategies to treat dogs not responding to a diet change.
In the last part of this article, we review the information for the use of probiotics as an alternative treatment to antibiotics. We highlight that there is currently not enough information on probiotics to determine how useful they can be and future research in their use is needed.
Introduction
Chronic enteropathy (CE) is a term used for gastro-intestinal diseases present for a duration of 3 weeks or longer, when extra-intestinal diseases or intestinal disease such as parasitic disease or neoplastic disease are ruled out.1 Clinically, CE is further classified according to treatment response as food-responsive enteropathy (FRE), antibiotic-responsive enteropathy (ARE), and immunosuppressant-responsive enteropathy (IRE). The term steroid-responsive enteropathy is also used for IRE and is the closest entity to the human Crohn’s disease, a variant of inflammatory bowel disease (IBD). The term idiopathic IBD is also used in veterinary medicine interchangeably with IRE in cases not responding to diet or antibiotic trial, and where intestinal inflammation is present on histology. Dogs not responding to treatment are categorized as having non-responsive enteropathy (NRE).
Although CE in dogs is perceived to be a common presentation in referral centres, there are few data about the true prevalence of this disease both at referral and general practice levels. In this review, we will summarize the evidence available about the prevalence of gastrointestinal disease, and more specifically CE where available.
Treatment trials remain the main tool to differentiate between the different clinical categories of CE as clinical history, biomarkers, endoscopic or histological changes have not been proven sufficient to do so at this point in time.2 For this reason, in most situations, a diet trial is performed in the first instance as studies have reported a response in a majority of dogs that is maintained for a long duration.3,4 In view of the good response to diet alone, endoscopy is typically performed at a later stage in the diagnostic work-up, as similar intestinal histological findings are expected in both FRE and IRE dogs, except if the clinical signs are severe or negative prognostic factors such as hypoalbuminaemia are present.1 Although antibiotic and corticosteroid trials, respectively, have often been used as next steps in dogs with CE, there is sparse information on long-term response to these treatment modalities.4 In the second part of this review, we will assess the evidence for short-term (less than 3 months median follow-up), mid-term (3 to 6 months median follow-up), and long term (over 6 months median follow-up) response to either diet, antibiotic, or immunosuppressant trial.
Although one of the clinical classifications of CE is antibiotic-responsive, there has been little evaluation apart from tylosin, which has been extensively studied in dogs from Finland as well as the UK.5–8 The long-term outcome in these dogs has been reported to be poor, and there is a growing concern of antibiotic resistance as described in human patients.4,9,10 For this reason, there is a need for evaluating alternative treatments for dogs with CE failing a diet trial.
The gastrointestinal microbiota have been recognized as a major player in intestinal health, and there is accumulating information about their role in dogs with CE.11,12 In view of these results, strategies to alter the microbiota are of much interest. Strategies to manipulate the microbiome beyond antibiotics include prebiotics, probiotics, and faecal microbiota transplant, whereby faecal contents from a healthy donor are administered to a dog with CE in view of re-implanting a healthy microbiota.13,14 The evidence for the use of probiotics will be reviewed in this article. There is currently not enough evidence to review the use of faecal microbiota transplant, however this will likely change in the future.
Materials And Methods
There is currently no literature assessing specifically the prevalence of CE in dogs in the general population. For this reason, articles describing a population of dogs from an insurance database or other large database were reviewed for pertinent information on the proportion of dogs with gastrointestinal disease.
To assess short and long-term outcome of dogs treated for CE, articles describing different treatment combination including diet manipulation, antibiotic treatment, and immunosuppressive treatment with follow-up information were considered. Relevant papers were retrieved with two searches. The following key words were included in PubMed, Web of Science, and Google Scholar databases for the first search: “Dog or canine” and “Chronic enteropathy or IBD”. For the second search, the following keywords were included: “chronic” and “diarrhea or vomiting” and “dog or canine”.
From the first search, 744 articles were retrieved; 492 were excluded as they were either not relevant, or described a single case report or one breed of dog. Out of the 252 articles remaining in English, 51 were found to be relevant after reading the abstract or the paper and were included. From the second search an additional 2 articles were identified that were not retrieved with the first search. In summary, 53 articles were included to review for outcome information. The results are descriptive only to capture the data available and no attempt at stratifying the evidence level has been done.
Each study was evaluated to include only dogs with CE after ruling out extra-intestinal disease and treatment with either diet, antibiotic, immunosuppressant, or a combination thereof. Histology was not required to be included, in order to reflect the fact that many dogs will be treated without biopsies in the general practice clinic. Studies without inclusion of outcome data or follow time were excluded. A definition for response, partial response, or no response was required. If not clearly defined, the cases were defined as response vs no response. Studies were divided by their follow-up time into short-term (3 months or less median follow-up), mid-term (3 to 6 months median follow-up), and long-term (over 6 months median follow-up) response.
To evaluate probiotic usage in dogs with CE, PubMed, Web of Science, and Google Scholar databases were searched for the terms (“canine” or “dog”) and (“probiotic”). A total of 142 entries were retrieved, excluding duplicates and reviews. Following exclusion of non-dog, non-diarrhoea, and non-CE/IBD (including parasitic disease, studies in shelters and studies in acute diarrhoea) entries, a total of 9 were then evaluated.
Prevalence Of Chronic Enteropathy
There is a lack of information on the prevalence of dogs with CE and it is difficult to obtain reliable data. All studies to date are retrospective and include one of the following strategies:
- Questionnaires sent to owners, breeders, or veterinarians.
- Use of data from insurance companies.
- Use of veterinary records from general practice or on occasion referral centres.
Each of these strategies has its own limitations, which leads to bias in the population selected (especially with insurance data and pedigree information) and recall of information (questionnaires). Scant information is available on prevalence of CE diseases and little more information on causes of death.
Additionally, most of these studies do not report the prevalence of CE, but rather gastrointestinal signs overall (i.e. summation of acute and chronic causes of different aetiologies). For this review, not only the information on prevalence of gastrointestinal disease in general practice and referral practice has been summarized, but also the information of gastrointestinal disease as a cause for death or euthanasia. The information from studies about prevalence is summarized in Table 1.
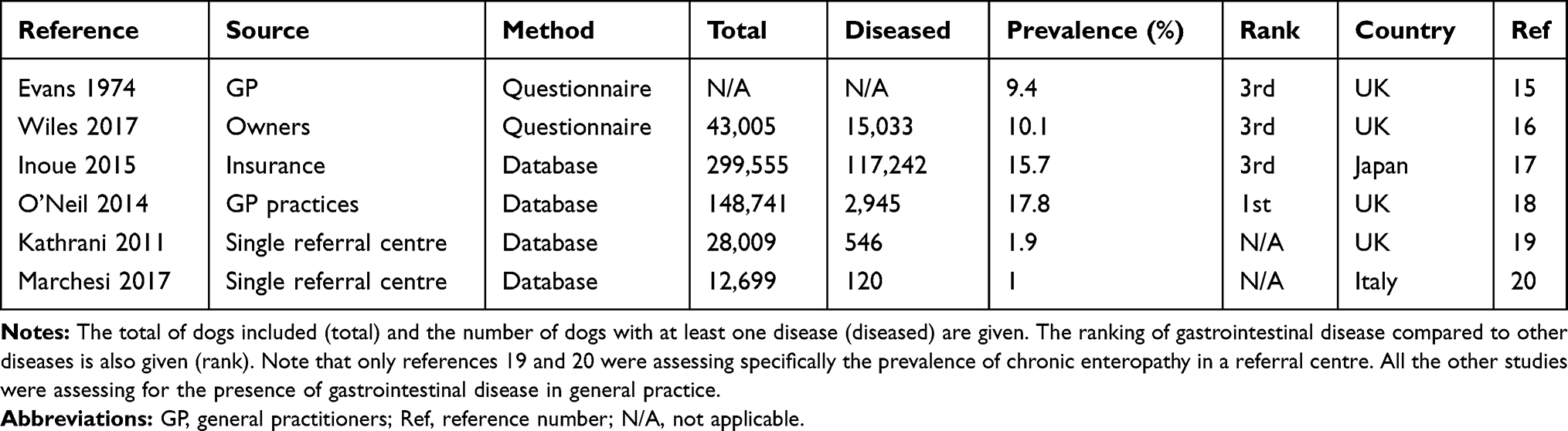 |
Table 1 Prevalence Of Gastrointestinal Disorders In Different Studies |
The oldest study assessing prevalence of gastrointestinal signs in dogs in general veterinary practice is a survey published in 1974. A questionnaire was developed and used to assess 61 companion animal veterinary surgeons practising in England, Scotland, and Wales.15 Taking into account the survey results, the authors report that 9.4% of dogs seen will have signs of gastrointestinal disease in general practice. The data collected did not enable the distinction between chronic and acute gastrointestinal disease to be made.
Another study from the UK assessed the prevalence of disease in pedigree dogs using a questionnaire filled by the owners.16 The questionnaire was open for 2 months in 2014 and 546,836 invitations were sent to owners of UK Kennel Club registered dogs. Only dogs alive at the time of the study were included. Data from 43,005 individual dogs across 187 breeds were obtained. The owners reported a total of 27,035 incidents from 752 distinct disease terms throughout their pet lives. Overall 35% of dogs had at least one disease or condition. The three most reported body systems included integument (skin, hair, and coat) with 36.2%, motor system (muscle, bone, and joint) with 16.9%, and digestive system with 10.1%. Prevalence of specific diseases reported included colitis (0.84%, confidence interval (CI): 0.76–0.93), food allergy (0.86%, CI: 0.78–0.95), inflammatory bowel disease (IBD, 0.35%, CI: 0.30–0.41), persistent diarrhoea (0.49%, CI: 0.43–0.56), persistent vomiting (0.16%, CI: 0.13–0.20), persistent vomiting and diarrhea (0.24%, CI: 0.20–0.29), overall equating to 2.1 to 2.9% of dogs showing signs consistent with CE (with or without the colitis category). The data reported do not allow to determine if several of these signs were present in the same dog.
One Japanese study assessed the prevalence of diseases in dogs included in an insurance policy database over a 1-year period (2010 to 2011).17 A total of 299,555 dogs were included and 177,242 dogs had at least one claim. Gastrointestinal disease was the third most frequent cause for an insurance claim with an annual prevalence of 15.7% (CI: 15.5–15.9); male dogs had a small, albeit significant, increased annual prevalence (16.4%, CI: 16.2–16.6) compared with female dogs (15.7%, CI: 15.5–15.9) in this category. The five breeds with the highest annual prevalence for gastrointestinal disease included French bulldog (22.0%, CI: 21.0–23.0), cavalier King Charles spaniel (21.0%, CI: 19.9–22.0), Yorkshire terrier (19.4%, CI: 18.7–20.2), golden retriever (18.6%, CI: 17.8–19.4), and Pembroke Welsh corgi (17.9%, CI: 16.8–18.9).
A recent study from the UK reported disorder prevalence amongst 3,884 dogs randomly selected from 148,741 dogs attending 93 clinics in central and southeastern England between September 2009 and March 2013.18 Data were obtained from the information entered by the veterinarian at the time of consultation. A total of 2,945 dogs (75.8%) had at least one disorder documented during the study period. Gastrointestinal disease was the most prevalent (17.8%, CI: 16.0–19.6), followed by dermatological disease (15.5%, CI: 13.9–17.1), then musculoskeletal disease (11.8%, CI: 10.6–12.9). These were from a range of breeds, gender, and ages.
Although gastrointestinal disease is frequently reported in these different studies, it is impossible to determine the true incidence of CE or IBD, both due to the retrospective nature of the studies, but also due to the recent changes in terminology and failure in many instances to complete a full work-up in general practice.
In the referral setting, one study specifically assessed at-risk breeds for CE in a single institution in the UK.19 The authors reviewed all dogs admitted over a 5.5-year period (2003 to 2009); a total of 546 dogs were diagnosed with CE after a thorough work up accounting for 86 breeds (including mix-breed). During the same period, 27,463 dogs of the same breeds were admitted to this hospital. This suggests that 2% of overall cases seen in this referral centre were dogs with CE. Breeds at significantly higher risk of developing CE than mix-breed dogs in this study included weimaraner, rottweiler, German shepherd, border collie, and boxer. Another Italian referral centre reports only 120 dogs with signs consistent with CE out of 12,699 cases admitted during 1 year.20 This represent 0.9% of the cases seen in this centre.
The data do not allow to determine whether the difference in these 2 studies reflects a geographical difference in the prevalence of CE, or a difference in the referral caseload. A larger study of referral practices (private and university-based, and secondary or tertiary) is necessary to determine the worldwide distribution of this disease.
Outcome
A study from the UK assessed the causes of mortality in purebred dogs by surveying owners contacted through the UK Kennel Club.21 During 2004 a total of 58,863 questionnaires were sent out and data were collected on all dogs that had died within the previous 10 years. The response rate was 24% (13,741 questionnaires returned) with information on 15,881 deaths during this time. In this study, gastrointestinal disease was the 7th cause of death with a frequency of 4.1%; over 50% of these deaths were due to a gastric dilation or volvulus. The specific diagnoses for the remaining GI causes of death were not documented.
In a similar study, questionnaires were sent to breeders in Denmark.22 A response rate of 20.5% was obtained, with information collected for 2,928 dogs. Gastrointestinal disease was reported as cause of death in 65 dogs (2.2%, CI: 1.7–2.8) and was the 9th most frequent cause of death out of 14 (after removing the category “old age”). Both studies, by design, only assessed the incidence of death in pedigree or purebred dogs. Genetic predisposition is strongly linked to CE and idiopathic IBD in dogs, with some breeds developing severe disease with a poorer prognosis.23,24 Therefore, it is likely that in the wider dog population, gastrointestinal disease as a cause of death is lower than in pedigree dogs.
One study assessed causes for mortality in over 222,000 insured Swedish dogs and reported gastrointestinal disease to be the 7th out of 18 causes.25 The data of the insurer cover over 30% of the dog population in Sweden and for this reason results can likely be extrapolated to the Swedish dog population as a whole.26 This study was published in 1997, and it is unlikely that the findings would be equally applicable in 2019.
The same group also assessed disease patterns more specifically in German shepherd dogs using the same insured population. A total of 32,486 German shepherd dogs (7.3% of the whole database) were included in this retrospective study from 1995 to 2006. Gastrointestinal disease of any type was the third most common reason for presentation for veterinary care and accounted for 267.1 cases per 10,000 dog years at risk (DYAR).
Another study from Japan studied the cause for 4,169 deaths among a population study of 278,411 insured dogs.27 Gastrointestinal disease was reported as the 4th cause of death with a percentage of 5.9% in this population.
Some data are also available on mortality causes for dogs in the UK.28 In this study, the authors reviewed clinical health data from 102,609 dogs from 86 first opinion veterinary practices in central and southeast England between January 2009 and December 2011. During this period, 5,095 dogs died or were euthanized. Gastrointestinal disease was the 3rd cause of death (6.5%) and dogs euthanized had a median age of 10.5 years (interquartile range 5.0 to 13.7). A bi-modal distribution in death was noted with peaks in year 1 and year 14. The top three causes for dogs younger than 3 years old included behaviour abnormality (14.7%), gastrointestinal disease (14.5%), or no cause recorded (13.3%), whereas for dogs older than 3 years old these were neoplastic disease (18.2%), no cause recorded (13.0%), or musculoskeletal disease (12.4%).
Only one study from North America reports cause of death in a large sample of dogs in a referral setting.29 The data were obtained from the Veterinary Medical Database (VMDB) that contains abstracted records from 27 Veterinary Teaching Hospitals. Visits during which the dog died were retrospectively evaluated from 1984 to 2004, again a time that may not be readily extrapolated to current day veterinary practice. A total of 74,556 dogs were analysed, and the proportion of death attributable to gastrointestinal disease was over 15% in dogs up to a year (1st cause) and about 10% in dogs older than a year (3rd cause of death).
So, how much is CE truly a problem? As can be seen from the information summarized above, there are currently insufficient data to fully answer this question. Overall, all causes of gastrointestinal disease are a common problem in general practice with a prevalence ranging from 9.4 to 17.8% according to different studies. The only 2 studies assessing the prevalence of CE in a referral centre report a prevalence of 0.9 to 2.0% of the overall caseload, which is similar to what is reported in purebred dog studies (2.1% of chronic disease).16,19,20
Data from surveys of causes of death are more variable, and the contribution of CE to these is impossible to determine. In summary, further work is required to better understand how prevalent CE truly is both in general and referral practice, but a prevalence of at least 1–2% can be hypothesized.
Response To Treatment For Chronic Enteropathy
Although response to treatment has been reported in several studies, the follow-up period is often short and less than 3 months. For this reason, the second part of this review was to summarize the information available about long-term response in dogs with CE. The results from the different studies are summarized in Tables 2–4.
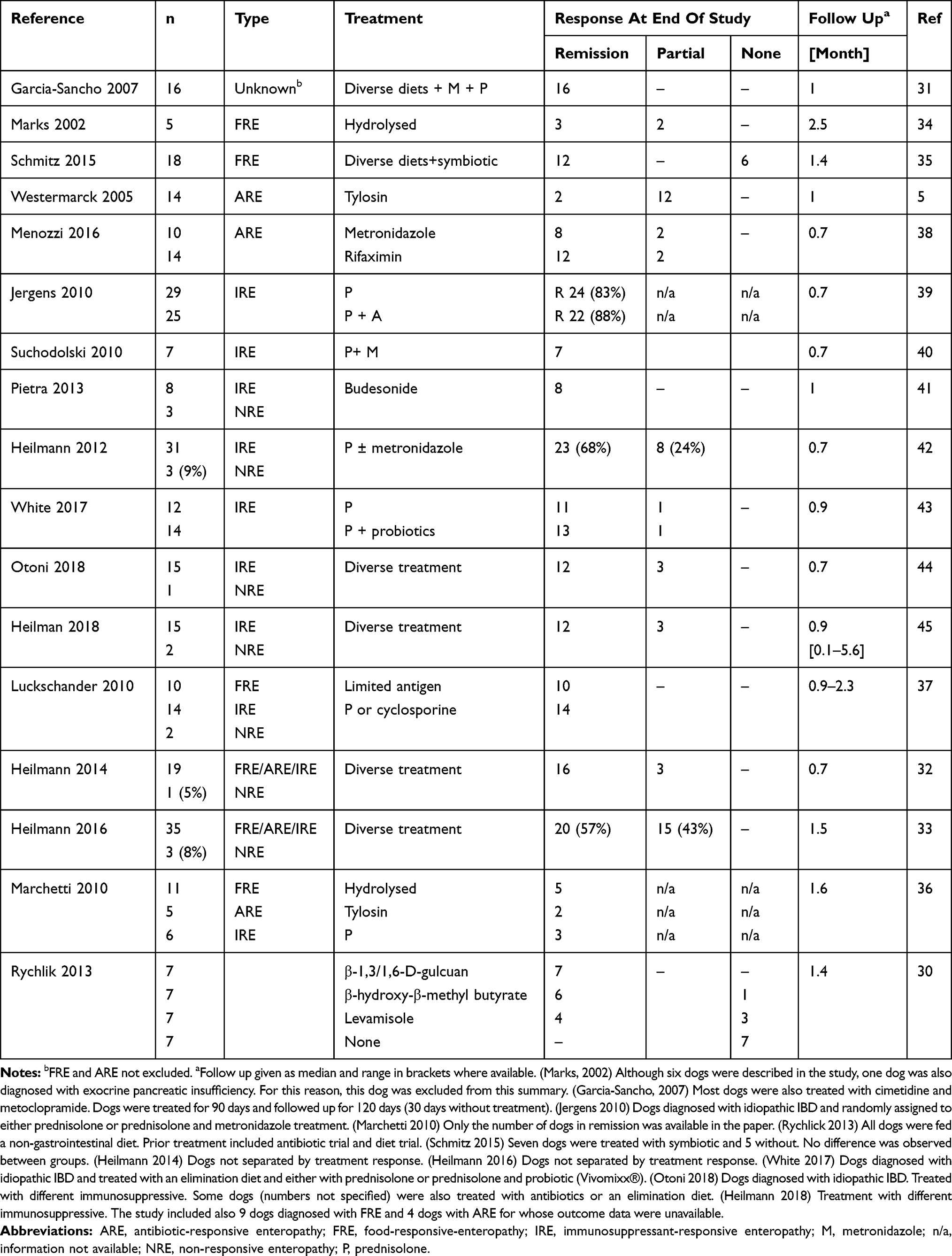 |
Table 2 Study Reporting Outcome To Different Treatments With A Median Follow Up Of Less Than 3 Months |
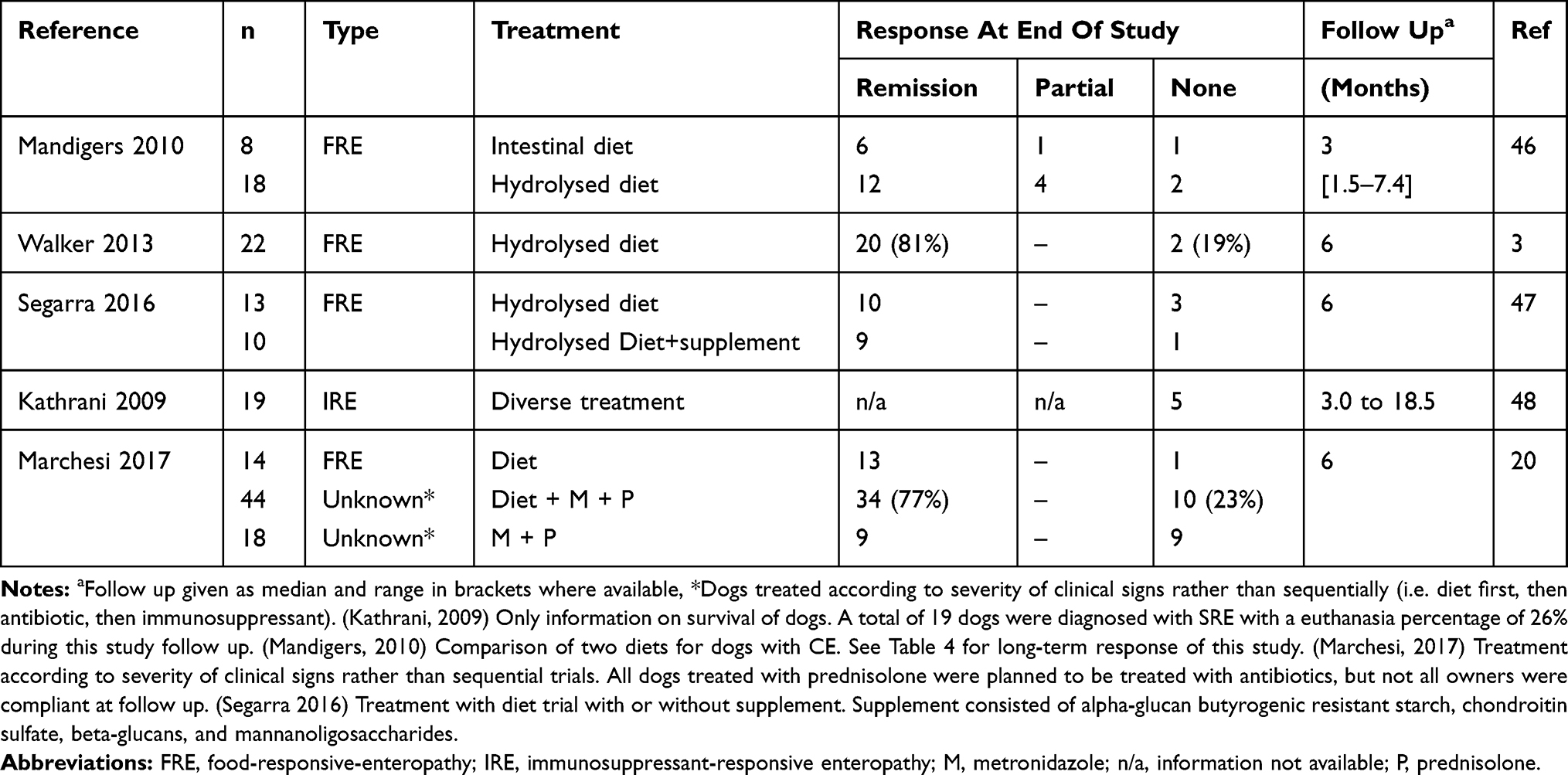 |
Table 3 Study Reporting Outcome To Different Treatments With A Median Follow Up Of 3 To 6 Months |
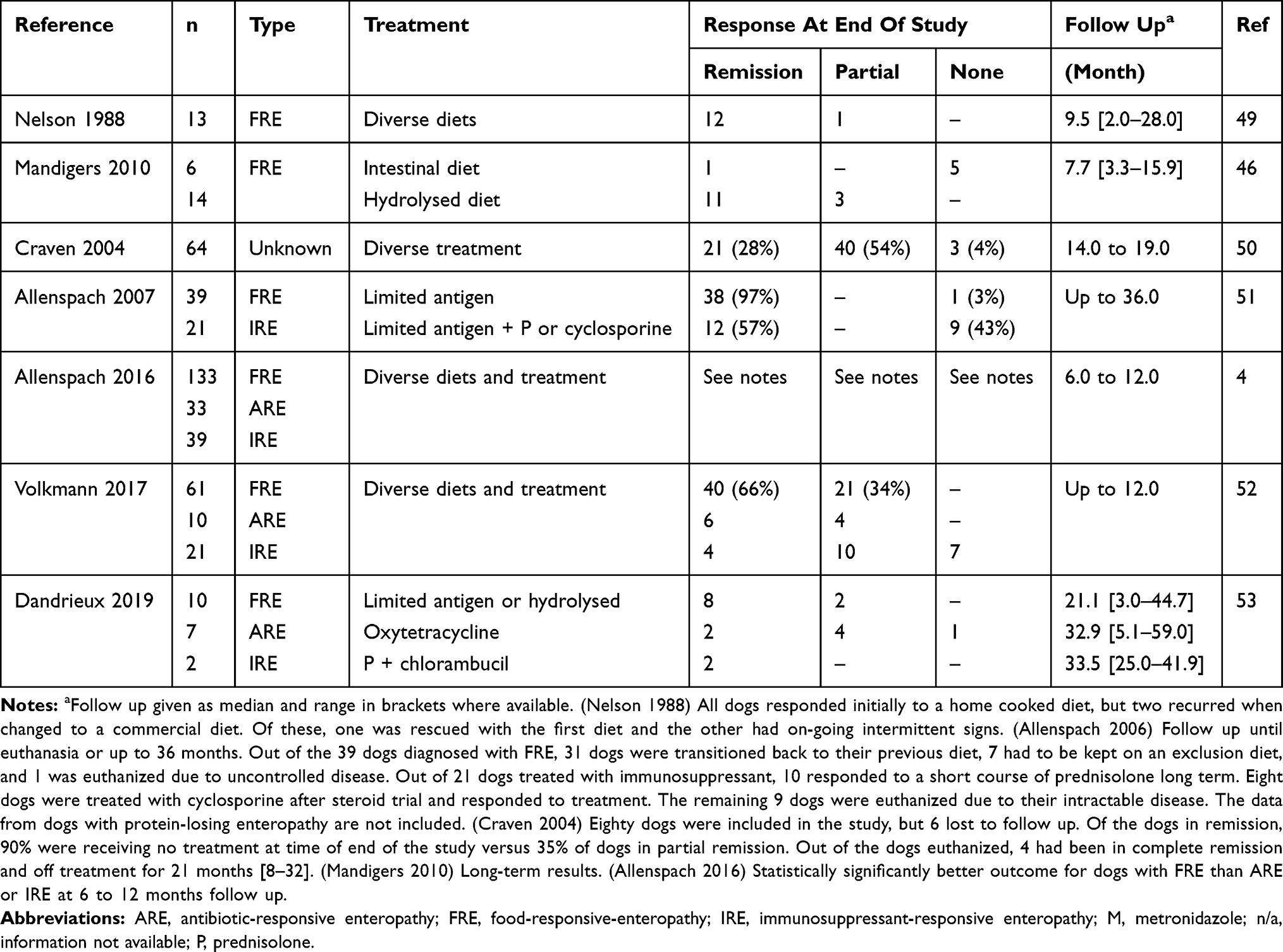 |
Table 4 Study Reporting Outcome To Different Treatments With A Median Follow Up Of More Than 6 Months |
A total of 17 studies were identified that reported the outcome of dogs treated for CE with a follow up of 3 months or less (Table 2). Except for one study assessing the effect of natural or synthetic immunomodulators, all the other studies assessed the effects of diet, antibiotics, and immunosuppressants.30 However, not all the studies had sequential treatment trials. In one study, standard treatment included the use of corticosteroids in combination with antibiotic and diet whereas for several other studies, only the overall remission (i.e. all the different subtypes) were reported.31–33 Remission in these studies varied from 57 to 100%.
Typically, response to diet was higher than 60% and reached 100% except for one study reporting a remission of clinical signs in 45% of dogs.34–37
Three studies report the outcome in dogs with ARE, and in 2 of these, remission or partial remission were achieved by all dogs.5,36,38 However, most dogs treated with tylosin relapsed within a month when the antibiotic was discontinued.
A very good outcome is reported for dogs with IRE treated with a variety of immunomodulators with remission of 65% or higher in most studies and some reporting 100% response.36,37,39–45 In one study comparing treatment with prednisolone or a combination of prednisolone and metronidazole, no difference was seen between either treatment protocols, suggesting no tangible benefit from metronidazole in the short-term.39 Similarly, no improvement was achieved when adding a probiotic to prednisolone treatment.43
Overall, these studies suggest a good short-term outcome in dogs diagnosed with FRE, ARE or IRE; whereas NRE was reported to represent 5 to 27% of the cases with the highest percentage after treatment with budesonide.41
Only 5 studies report the outcome of dogs treated for CE with follow up of 3 to 6 months (Table 3). Response to diet trial is reported most frequently (3 studies), with remission rates of over 67%.3,46–48 Additionally, 2 studies reported the short-term results of corticosteroid treatment.20,48 In these studies, a relapse in clinical signs after treatment with prednisolone was reported in 23 to 50% of cases.
Finally, 7 studies reported outcomes in dogs with CE with a follow-up period greater than 6 months (Table 4). Most studies reported a good long term outcome in dogs responding to diet with remission rates of over 66%.46,49,51–53 The effect of diet could not be assessed in one study as the diet was not changed in all dogs and additional treatment was used concomitantly.50 Interestingly, in one study, although the response was similar between hydrolysed diet and limited antigen diets when assessed at less than 6 months, there was a statistically significant improvement in response in dogs fed a hydrolysed diet after a longer follow up with a remission rate of 79% vs 12% (P<0.001).46
In comparison, partial or lack of response was observed in over 40% of dogs classified as having ARE or IRE.51 The poor long-term outcome in IRE and ARE dogs was also reported in a large study from the UK with significantly better outcome in dogs with FRE than ARE or IRE.4 Similar results are reported in a study from Australia with better outcome in dogs with FRE than ARE although the study was underpowered.53
The data suggest there is a good long-term outcome for dogs with CE that initially respond to a dietary trial. However, there are growing concerns that dogs classified as ARE and IRE when first diagnosed, will not respond longer term to the same degree. This finding suggests that strategies that manipulate the microbiome should be evaluated to improve the outcome of dogs diagnosed with CE.
Use Of Probiotics In Dogs With CE
The use of probiotics in veterinary practice has been expanding over recent years, due in part to increasing knowledge about the microbiome and in part due to reluctance to use antibiotics long term. Probiotics are defined as live microorganisms that confer a health benefit on the host when administered in adequate amounts.54 In addition, probiotics should survive gastric acid and bile to reach and adhere to the intestine, be able to proliferate and colonize the colon, modulate the intestinal immune system, be active against pathogenic microorganisms and have no carcinogenic, toxic, pathogenic or mutagenic effects. The most common types of bacteria contained in probiotics that are used in veterinary practice include Bifidobacterium, Lactobacillus, Enterococcus faecium, and the yeast Saccharomyces boulardii. There is an increasing use of probiotics in human gastroenterology, particularly in treatment of ulcerative colitis.55 In most countries, probiotics are not considered veterinary medicines, and therefore products may contain different concentrations of organisms than labelled and are not obligated to demonstrate efficacy in particular conditions.56
The studies on the use of probiotics in dogs with CE are either bench-top or clinical trials, with different products being assessed in different breeds and different forms of CE, making definitive conclusions difficult to make. Studies reviewed are summarized in Table 5.
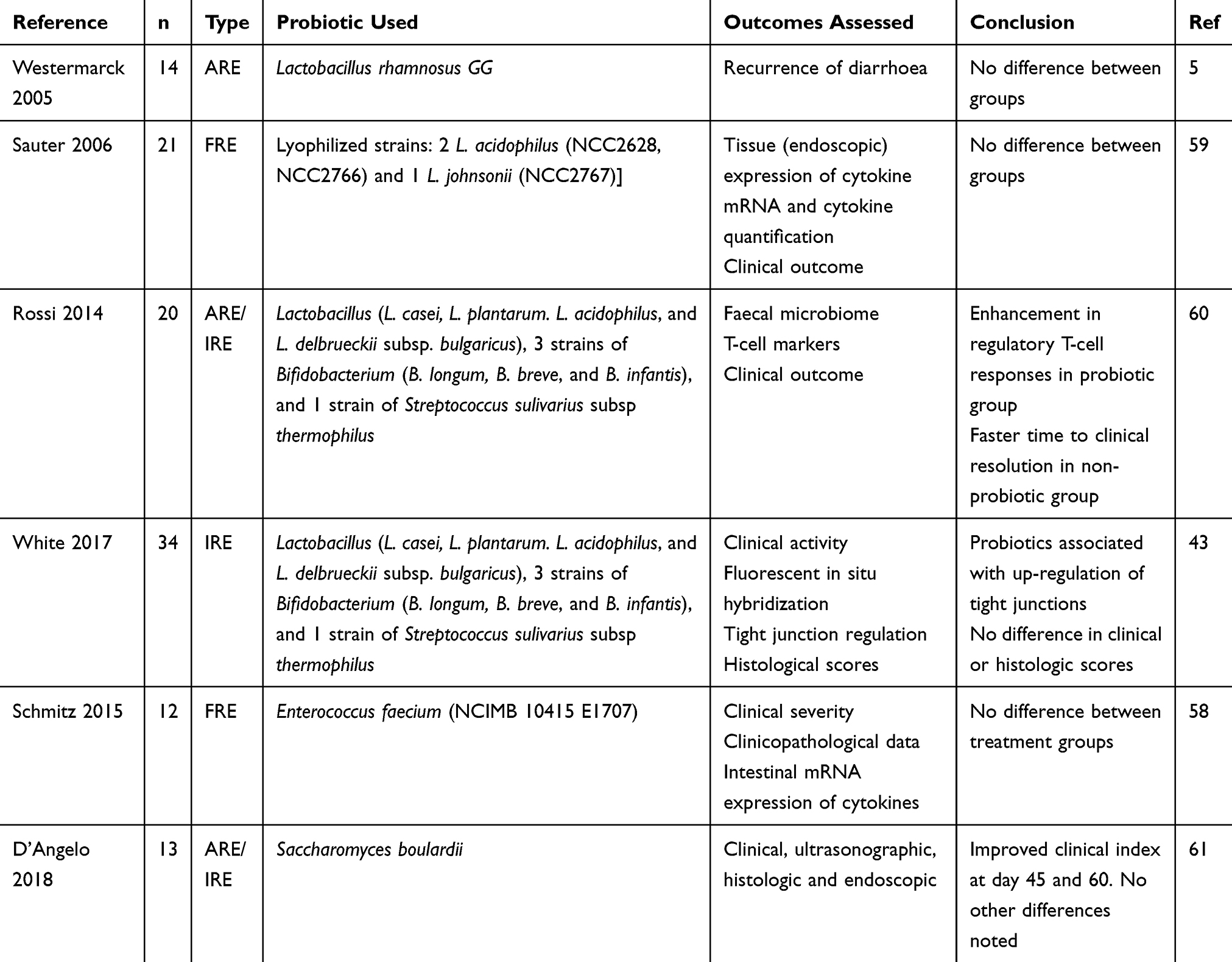 |
Table 5 Studies Reporting The Use Of Probiotic For Treatment Of Dogs With CE |
Bench-top studies have demonstrated mixed results in terms of efficacy when assessing dogs with CE. An early study assessed three Lactobacilli strains, and the three combined in a cocktail in tissue culture (duodenal explants) from dogs with CE.57 This demonstrated increased expression and production of interleukin-10 (an anti-inflammatory cytokine) and decreased pro-inflammatory cytokines. A more recent study assessing treatment ex vivo of intestinal samples with E. faecium found no change in inflammatory mediator gene expression (the inflammasome) compared to placebo, in samples from both healthy dogs and dogs with CE.58 The same group of researchers performed whole blood stimulation and stimulation of duodenal explants in healthy (colony) samples and dogs with FRE.35 No differential gene expression was identified in duodenal samples with administration of the probiotic, whereas TNFα production was increased with E. faecium administration.
In clinical trials, the results have also been varied, as have the study populations and probiotics used. In a study based in Finland in 2005, dogs with tylosin-responsive diarrhoea were studied after achieving disease remission in 14 dogs.5 Discontinuation of tylosin resulted in recurrence of signs in 12 dogs, and this was not attenuated by administration of the probiotic Lactobacillus rhamnosus GG. In a 2006 study of 21 dogs with FRE, a placebo or probiotic cocktail (3 different Lactobacillus spp. strains which were all lyophilized: 2 L. acidophilus (NCC2628, NCC2766) and 1 L. johnsonii (NCC2767)) was administered along with dietary therapy.59 All dogs clinically improved, with no difference noted between groups in clinical outcome or expression of cytokine mRNA in intestinal samples, despite the probiotic bacteria being identified in the faeces of treated dogs.
Studies of the probiotic VSL#3 have also been undertaken, with one prospective study performed in dogs with CE.60 VSL #3 is a high-dose, multi-strain probiotic product containing viable lyophilized bacteria consisting of 4 strains of Lactobacillus (L. casei, L. plantarum. L. acidophilus, and L. delbrueckii subsp. bulgaricus), 3 strains of Bifidobacterium (B. longum, B. breve, and B. infantis), and 1 strain of Streptococcus sulivarius subsp thermophilus. Enrolled study dogs had failed response to dietary therapy and entered a 90-day open label trial. Recovery was more rapid in dogs treated with metronidazole and prednisolone than VSL#3, but there were changes in the inflammatory profile with probiotic treatment. A later study evaluated VSL #3 (but as a renamed commercial product) in a multi-centre study of dogs with idiopathic IBD.43 All dogs that completed the trial (n=26) were treated with elimination diet and prednisolone, but 14 of those were randomly assigned to also receive the probiotic. No adverse effects were reported during the trial, and probiotic treatment had no impact on histological scores within the intestine, or reduction of the clinical activity index. Probiotic therapy was however associated with up-regulation of tight junction proteins, although the clinical significance of this is unknown. Similarly, in a larger study of dogs with FRE, administration of E faecium failed to produce any significant benefit over treatment with diet alone.35
In a recent Italian study, 20 dogs with IRE were treated with the yeast Saccharomyces boulardii or a placebo.61 Each dog was also managed with dietary therapy (hydrolysed or limited antigen), antibiotics (tylosin or metronidazole), and immunosuppressive treatment tailored to the individual dog. The study was not sequential (i.e. not randomized), but double-blinded as to treatment group. Only 13 dogs reached the end of the study (6 in probiotic group and 7 in placebo group), and an improvement in clinical severity was noted for dogs in the probiotic group at day 45 and 60. There were no differences noted in ultrasonographic, histologic or endoscopic findings between groups at different time-points. Although this appears a promising study, the variability in other treatments as well as the inclusion of data from dogs that died during the study makes it difficult to attribute benefit entirely to the effects of the probiotic.
Conclusion
In conclusion, although CE is considered as a frequent cause of presentation to the veterinarian, there is currently a lack of studies to determine the true prevalence either at the level of general practice or referral. Future studies are necessary to answer this question.
Although there are many studies reporting short-term response to different treatment trials, there are only a few reporting long-term response and most of the studies included dogs with FRE. Although FRE dogs do have an excellent long-term response, the results are not as clear for ARE or IRE dogs. More studies are required to confirm these results, but this information suggests that other strategies than antibiotic treatment is required.
Despite the variation in types of disease and probiotics studied, there appears to be no detrimental effects reported from administration. Based on the literature to date, use of probiotics in dogs with food-responsive enteropathy does not appear to have any benefit. Likewise, the long-term impact on dogs with ARE/IRE is difficult to ascertain. Larger studies are required before any conclusions about the clinical utility of probiotics can be made.
Abbreviations
ARE, antibiotic-responsive enteropathy; CE, chronic enteropathy; FRE, food-responsive enteropathy; IBD, inflammatory bowel disease; IRE, immunosuppressant-responsive enteropathy.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dandrieux JRS. Inflammatory bowel disease versus chronic enteropathy in dogs: are they one and the same? J Small Anim Pract. 2016;57(11):589–599. doi:10.1111/jsap.2016.57.issue-11
2. Heilmann RM, Steiner JM. Clinical utility of currently available biomarkers in inflammatory enteropathies of dogs. J Vet Intern Med. 2018;32(5):1495–1508. doi:10.1111/jvim.15247
3. Walker D, Knuchel-Takano A, McCutchan A, et al. A comprehensive pathological survey of duodenal biopsies from dogs with diet-responsive chronic enteropathy. J Vet Intern Med. 2013;27:862–874. doi:10.1111/jvim.12093
4. Allenspach K, Culverwell C, Chan D. Long-term outcome in dogs with chronic enteropathies: 203 cases. Vet Rec. 2016;178(15):
5. Westermarck E, Skrzypczak T, Harmoinen J, et al. Tylosin-responsive chronic diarrhea in dogs. J Vet Intern Med. 2005;19:177–186. doi:10.1111/j.1939-1676.2005.tb02679.x
6. Kilpinen S, Rantala M, Spillmann T, Björkroth J, Westermarck E. Oral tylosin administration is associated with an increase of faecal enterococci and lactic acid bacteria in dogs with tylosin-responsive diarrhoea. Vet J. 2015;205(3):369–374. doi:10.1016/j.tvjl.2015.03.021
7. Kilpinen S, Spillmann T, Westermarck E. Efficacy of two low-dose oral tylosin regimens in controlling the relapse of diarrhea in dogs with tylosin-responsive diarrhea: a prospective, single-blinded, two-arm parallel, clinical field trial. Acta Vet Scand. 2014;56:43. doi:10.1186/1751-0147-56-4
8. Kilpinen S, Spillmann T, Syrja P, Skrzypczak T, Louhelainen M, Westermarck E. Effect of tylosin on dogs with suspected tylosin-responsive diarrhea: a placebo-controlled, randomized, double-blinded, prospective clinical trial. Acta Vet Scand. 2011;53:26. doi:10.1186/1751-0147-53-26
9. Makielski K, Cullen J, O’Connor A, Jergens AE. Narrative review of therapies for chronic enteropathies in dogs and cats. J Vet Intern Med. 2019;33(1):11–22. doi:10.1111/jvim.15345
10. Nguyen GC. Tip of the iceberg?: the emergence of antibiotic-resistant organisms in the IBD population. Gut Microbes. 2012;3(5):434–436. doi:10.4161/gmic.20870
11. Suchodolski JS, Markel ME, Garcia-Mazcorro JF, et al. The fecal microbiome in dogs with acute diarrhea and idiopathic inflammatory bowel disease. PLoS One. 2012;7:e51907. doi:10.1371/journal.pone.0051907
12. Minamoto Y, Otoni CC, Steelman SM, et al. Alteration of the fecal microbiota and serum metabolite profiles in dogs with idiopathic inflammatory bowel disease. Gut Microbes. 2015;6:33–47. doi:10.1080/19490976.2014.997612
13. Schmitz S, Suchodolski J. Understanding the canine intestinal microbiota and its modification by pro-, pre- and synbiotics - what is the evidence? Vet Med Sci. 2016;2:71–94. doi:10.1002/vms3.17
14. Chaitman J, Jergens AE, Gaschen F, et al. Commentary on key aspects of fecal microbiota transplantation in small animal practice. Vet Med Auckl. 2016;7:71–74.
15. Evans JM, Lane DR, Hendy PG. The profile of small animal practice. J Small Anim Pract. 1974;15(10):595–608. doi:10.1111/j.1748-5827.1974.tb06504.x
16. Wiles BM, Llewellyn-Zaidi AM, Evans KM, O’Neill DG, Lewis TW. Large-scale survey to estimate the prevalence of disorders for 192 Kennel Club registered breeds. Canine Genet Epidemiol. 2017;4. doi:10.1186/s40575-017-0053-5
17. Inoue M, Hasegawa A, Hosoi Y, Sugiura K. Breed, gender and age pattern of diagnosis for veterinary care in insured dogs in Japan during fiscal year 2010. Prev Vet Med. 2015;119(1–2):54–60. doi:10.1016/j.prevetmed.2015.02.010
18. O′Neill DG, Church DB, McGreevy PD, Thomson PC, Brodbelt DC. Prevalence of disorders recorded in dogs attending primary-care veterinary practices in England. PLoS One [Internet]. 2014 [cited February 12, 2019];9(3). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3942437/.
19. Kathrani A, Werling D, Allenspach K. Canine breeds at high risk of developing inflammatory bowel disease in the south-eastern UK. Vet Rec. 2011;169:635. doi:10.1136/vr.d5380
20. Marchesi MC, Timpano CC, Busechian S, Pieramati C, Rueca F. The role of diet in managing inflamatory bowel disease affected dogs: a retrospective cohort study on 76 cases. Vet Ital. 2017;6:297–302.
21. Adams VJ, Evans KM, Sampson J, Wood JLN. Methods and mortality results of a health survey of purebred dogs in the UK. J Small Anim Pract. 2010;51(10):512–524. doi:10.1111/j.1748-5827.2010.00974.x
22. Proschowsky HF, Rugbjerg H, Ersbøll AK. Mortality of purebred and mixed-breed dogs in Denmark. Prev Vet Med. 2003;58(1–2:63–74. doi:10.1016/S0167-5877(03)00010-2
23. Breitschwerdt EB, Ochoa R, Barta M, Barta O, McClure J, Waltman C. Clinical and laboratory characterization of Basenjis with immunoproliferative small intestinal disease. Am J Vet Res. 1984;45(2):267–273.
24. Littman MP, Dambach DM, Vaden SL, Giger U. Familial protein-losing enteropathy and protein-losing nephropathy in Soft Coated Wheaten Terriers: 222 cases (1983–1997). J Vet Intern Med. 2000;14:68–80.
25. Bonnett BN, Egenvall A, Olson P, Hedhammar A. Mortality in insured Swedish dogs: rates and causes of death in various breeds. Vet Rec. 1997;141(2):40–44. doi:10.1136/vr.141.2.40
26. Egenvall A, Nødtvedt A, Penell J, Gunnarsson L, Bonnett BN. Insurance data for research in companion animals: benefits and limitations. Acta Vet Scand. 2009;51(1):42. doi:10.1186/1751-0147-51-42
27. Inoue M, Hasegawa A, Hosoi Y, Sugiura K. A current life table and causes of death for insured dogs in Japan. Prev Vet Med. 2015;120(2):210–218. doi:10.1016/j.prevetmed.2015.03.018
28. O’Neill DG, Church DB, McGreevy PD, Thomson PC, Brodbelt DC. Longevity and mortality of owned dogs in England. Vet J. 2013;198(3):638–643. doi:10.1016/j.tvjl.2013.09.020
29. Fleming JM, Creevy KE, Promislow DEL. Mortality in North American Dogs from 1984 to 2004: an investigation into age-, size-, and breed-related causes of death. J Vet Intern Med. 2011;25(2):187–198. doi:10.1111/j.1939-1676.2011.0695.x
30. Rychlik A, Nieradka R, Kander M, Nowicki M, Wdowiak M, Kolodziejska-Sawerska A. The effectiveness of natural and synthetic immunomodulators in the treatment of inflammatory bowel disease in dogs. Acta Vet Hung. 2013;61:297–308. doi:10.1556/AVet.2013.015
31. Garcia-Sancho M, Rodriguez-Franco F, Sainz A, Mancho C, Rodriguez A. Evaluation of clinical, macroscopic, and histopathologic response to treatment in nonhypoproteinemic dogs with lymphocytic-plasmacytic enteritis. J Vet Intern Med. 2007;21:11–17. doi:10.1111/j.1939-1676.2007.tb02922.x
32. Heilmann RM, Otoni CC, Jergens AE, Grützner N, Suchodolski JS, Steiner JM. Systemic levels of the anti-inflammatory decoy receptor soluble RAGE (receptor for advanced glycation end products) are decreased in dogs with inflammatory bowel disease. Vet Immunol Immunopathol. 2014;161(3–4):184–192. doi:10.1016/j.vetimm.2014.08.003
33. Heilmann RM, Volkmann M, Otoni CC, et al. Fecal S100A12 concentration predicts a lack of response to treatment in dogs affected with chronic enteropathy. Vet J. 2016;215:96–100. doi:10.1016/j.tvjl.2016.03.001
34. Marks SL, Laflamme DP, McAloose D. Dietary trial using a commercial hypoallergenic diet containing hydrolyzed protein for dogs with inflammatory bowel disease. Vet Ther. 2002;3:109–118.
35. Schmitz S, Glanemann B, Garden OA, et al. A prospective, randomized, blinded, placebo‐controlled pilot study on the effect of enterococcus faecium on clinical activity and intestinal gene expression in canine food‐responsive chronic enteropathy. J Vet Intern Med. 2015;29(2):533–543. doi:10.1111/jvim.12542
36. Marchetti V, Lubas G, Lombardo A, Corazza M, Guidi G, Cardini G. Evaluation of erythrocytes, platelets, and serum iron profile in dogs with chronic enteropathy. Vet Med Int. 2010. 2010;1–5. doi:10.4061/2010/716040
37. Luckschander N, Hall JA, Gaschen F, et al. Activation of nuclear factor-kappaB in dogs with chronic enteropathies. Vet Immunol Immunopathol. 2010;133:228–236. doi:10.1016/j.vetimm.2009.07.015
38. Menozzi A, Dall’Aglio M, Quintavalla F, Dallavalle L, Meucci V, Bertini S. Rifaximin is an effective alternative to metronidazole for the treatment of chronic enteropathy in dogs: a randomised trial. BMC Vet Res. 2016;12. doi:10.1186/s12917-016-0813-6
39. Jergens AE, Crandell J, Morrison JA, et al. Comparison of oral prednisone and prednisone combined with metronidazole for induction therapy of canine inflammatory bowel disease: a randomized-controlled trial. J Vet Intern Med. 2010;24:269–277. doi:10.1111/j.1939-1676.2009.0447.x
40. Suchodolski JS, Xenoulis PG, Paddock CG, Steiner JM, Jergens AE. Molecular analysis of the bacterial microbiota in duodenal biopsies from dogs with idiopathic inflammatory bowel disease. Vet Microbiol. 2010;19(142):394–400. doi:10.1016/j.vetmic.2009.11.002
41. Pietra M, Fracassi F, Diana A, et al. Plasma concentrations and therapeutic effects of budesonide in dogs with inflammatory bowel disease. Am J Vet Res. 2013;74:78–83. doi:10.2460/ajvr.74.1.78
42. Heilmann RM, Jergens AE, Ackermann MR, Barr JW, Suchodolski JS, Steiner JM. Serum calprotectin concentrations in dogs with idiopathic inflammatory bowel disease. Am J Vet Res. 2012;73:1900–1907. doi:10.2460/ajvr.73.12.1900
43. White R, Atherly T, Guard B, et al. Randomized, controlled trial evaluating the effect of multi-strain probiotic on the mucosal microbiota in canine idiopathic inflammatory bowel disease. Gut Microbes. 2017;3(8):451–466. doi:10.1080/19490976.2017.1334754
44. Otoni CC, Heilmann RM, García‐Sancho M, et al. Serologic and fecal markers to predict response to induction therapy in dogs with idiopathic inflammatory bowel disease. J Vet Intern Med. 2018;32(3):999–1008. doi:10.1111/jvim.15123
45. Heilmann RM, Berghoff N, Mansell J, et al. Association of fecal calprotectin concentrations with disease severity, response to treatment, and other biomarkers in dogs with chronic inflammatory enteropathies. J Vet Intern Med. 2018;32(2):679–692. doi:10.1111/jvim.15065
46. Mandigers PJ, Biourge V, van Den Ingh TS, Ankringa N, German AJ. A randomized, open-label, positively-controlled field trial of a hydrolyzed protein diet in dogs with chronic small bowel enteropathy. J Vet Intern Med. 2010;24:1350–1357. doi:10.1111/j.1939-1676.2010.0632.x
47. Segarra S, Martinez-Subiela S, Cerda-Cuellar M, et al. Oral chondroitin sulfate and prebiotics for the treatment of canine Inflammatory Bowel Disease: a randomized, controlled clinical trial. BMC Vet Res. 2016;10(12):49. doi:10.1186/s12917-016-0676-x
48. Kathrani A, Steiner JM, Suchodolski J, et al. Elevated canine pancreatic lipase immunoreactivity concentration in dogs with inflammatory bowel disease is associated with a negative outcome. J Small Anim Pr. 2009;50:126–132. doi:10.1111/jsap.2009.50.issue-3
49. Nelson RW, Stookey LJ, Kazacos E. Nutritional management of idiopathic chronic colitis in the dog. J Vet Intern Med. 1988;2(3):133–137. doi:10.1111/j.1939-1676.1988.tb02809.x
50. Craven M, Simpson JW, Ridyard AE, Chandler ML. Canine inflammatory bowel disease: retrospective analysis of diagnosis and outcome in 80 cases (1995–2002). J Small Anim Pr. 2004;45:336–342. doi:10.1111/j.1748-5827.2004.tb00245.x
51. Allenspach K, Wieland B, Grone A, Gaschen F. Chronic enteropathies in dogs: evaluation of risk factors for negative outcome. J Vet Intern Med. 2007;21:700–708. doi:10.1111/j.1939-1676.2007.tb03011.x
52. Volkmann M, Steiner JM, Fosgate GT, Zentek J, Hartmann S, Kohn B. Chronic diarrhea in dogs – retrospective study in 136 cases. J Vet Intern Med. 2017;31(4):1043–1055. doi:10.1111/jvim.2017.31.issue-4
53. Dandrieux JRS, Lopez LM, Prakash N, Mansfield CS. Treatment response and long term follow up in nineteen dogs diagnosed with chronic enteropathy in Australia. Aust Vet J. 2019;97(9):301–307. doi:10.1111/avj.12846
54. Ciorba MA. A gastroenterologist’s guide to probiotics. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc [[Internet]. 2012 [cited March 12, 2019];10(9):960–968. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3424311/.
55. Bai A-P, Ouyang Q, Xiao X-R, Li S-F. Probiotics modulate inflammatory cytokine secretion from inflamed mucosa in active ulcerative colitis. Int J Clin Pract. 2006;60(3):284–288. doi:10.1111/j.1368-5031.2006.00833.x
56. Weese JS. Microbiologic evaluation of commercial probiotics. J Am Vet Med Assoc. 2002;220(6):794–797. doi:10.2460/javma.2002.220.794
57. Sauter SN, Allenspach K, Gaschen F, Grone A, Ontsouka E, Blum JW. Cytokine expression in an ex vivo culture system of duodenal samples from dogs with chronic enteropathies: modulation by probiotic bacteria. Domest Anim Endocrinol. 2005;29:605–622. doi:10.1016/j.domaniend.2005.04.006
58. Schmitz S, Werling D, Allenspach K. Effects of ex-vivo and in-vivo treatment with probiotics on the inflammasome in dogs with chronic enteropathy. PloS One. 2015;10(3):e0120779. doi:10.1371/journal.pone.0120779
59. Sauter SN, Benyacoub J, Allenspach K, et al. Effects of probiotic bacteria in dogs with food responsive diarrhoea treated with an elimination diet*. J Anim Physiol Anim Nutr. 2006;90(7–8):269–277. doi:10.1111/j.1439-0396.2005.00595.x
60. Rossi G, Pengo G, Caldin M, et al. Comparison of microbiological, histological, and immunomodulatory parameters in response to treatment with either combination therapy with prednisone and metronidazole or probiotic VSL#3 strains in dogs with idiopathic inflammatory bowel disease. PLoS One. 2014;9:e94699. doi:10.1371/journal.pone.0094699
61. D’Angelo S, Fracassi F, Bresciani F, et al. Effect of Saccharomyces boulardii in dogs with chronic enteropathies: double-blinded, placebo-controlled study. Vet Rec. 2018;182(9):258. doi:10.1136/vr.k93
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.