Back to Journals » Clinical Ophthalmology » Volume 20
Choroidal Detachment After Baerveldt Glaucoma Implant Surgery: Incidence and Risk Factors
Authors Iwasaki K, Katsuo A, Arimura S, Takamura Y, Inatani M
Received 31 March 2026
Accepted for publication 11 June 2026
Published 15 June 2026 Volume 2026:20 611424
DOI https://doi.org/10.2147/OPTH.S611424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sotiria Palioura
Kentaro Iwasaki, Ayami Katsuo, Shogo Arimura, Yoshihiro Takamura, Masaru Inatani
Department of Ophthalmology, Faculty of Medical Sciences, University of Fukui, Yoshida, Fukui, Japan
Correspondence: Masaru Inatani, Department of Ophthalmology, Faculty of Medical Sciences, University of Fukui, 23-3 Shimoaizuki, Matsuoka, Eiheiji, Yoshida, Fukui, 910-1193, Japan, Tel +81-776-61-8400, Fax +81-776-61-8131, Email [email protected]
Purpose: To investigate the incidence and risk factors for postoperative choroidal detachment (CD) following Baerveldt glaucoma implant (BGI) surgery.
Patients and Methods: We conducted a retrospective cohort study including adult patients who underwent BGI surgery using a 350-mm2 endplate at Fukui University Hospital between April 2012 and March 2025. We excluded patients who had eyes with no light perception, prior tube-shunt surgery, postoperative follow-up of ˂3 months, or additional intraocular surgery within 3 months. CD was diagnosed by fundoscopy using B-scan ultrasonography when fundus visualization was limited. The clinical characteristics and postoperative intraocular pressure (IOP) were compared between eyes with and without CD. Multivariable logistic regression analysis was performed to identify independent risk factors for CD, and exploratory analyses were conducted to compare early- and delayed-onset CD. For these exploratory analyses, early-onset CD was defined as occurring within 10 days after surgery and delayed-onset CD as occurring 30 days or later.
Results: We analyzed the data of 261 eyes, and postoperative CD developed in 48 eyes (18.4%). Eyes with CD were significantly older and showed lower postoperative day 1 IOP and the lowest postoperative IOP within 7 days compared with those without CD. Multivariable analysis revealed that older age (odds ratio [OR] 1.06 per year, P < 0.01) and greater postoperative IOP reduction (OR 1.08 per mmHg, P < 0.01) were independently associated with CD. Among the eyes with CD, 37 were classified as early onset and 11 as delayed onset. Exploratory analyses suggested that early-onset CD tended to be associated with a greater number of previous intraocular surgeries, longer axial length, differences in tube insertion site, and lower postoperative day 1 IOP compared with delayed-onset CD.
Conclusion: Older age and greater postoperative IOP reduction were independently associated with CD after BGI surgery, suggesting that rapid postoperative IOP reduction may play an important role in CD pathogenesis. Early- and delayed-onset CD may reflect different postoperative mechanisms of aqueous humor dynamics following BGI surgery.
Keywords: glaucoma drainage device, intraocular pressure reduction, postoperative complications, postoperative hypotony
Introduction
Choroidal detachment (CD) is a common early complication of glaucoma filtering surgery.1 It is typically associated with ocular hypotony, excessive aqueous outflow, and postoperative inflammation. Many cases resolve spontaneously; however, severe or persistent CD may lead to a shallow anterior chamber, hypotonic maculopathy, or visual deterioration, which negatively affect surgical outcomes.2–4
Previous studies investigating trabeculectomy with mitomycin C identified several risk factors for postoperative CD, including advanced age, exfoliation glaucoma (ExG), large postoperative IOP reduction, low early postoperative IOP, and smaller central corneal thickness.5–7 This suggests that preoperative ocular characteristics and early postoperative IOP dynamics play important roles in CD development.
In recent years, tube-shunt surgery using the Baerveldt glaucoma implant (BGI) or Ahmed glaucoma valve (AGV) has been increasingly adopted worldwide to manage refractory glaucoma.8–11 Contrary to trabeculectomy, which relies on subconjunctival filtration, glaucoma drainage devices divert the aqueous humor into an endplate reservoir through a tube inserted into the eye. The AGV incorporates a mechanical valve designed to restrict excessive aqueous outflow and reduce the risk of early postoperative hypotony. Contrarily, the BGI is a non-valved drainage device that requires temporary tube ligation at the time of surgery to prevent early postoperative hypotony. Aqueous outflow is restored only after the spontaneous dissolution of the ligature, leading to characteristic postoperative IOP fluctuations. Consequently, the mechanism and timing of postoperative hypotony after BGI surgery differ from those observed after trabeculectomy or AGV implantation. These differences in aqueous outflow control may influence the incidence and mechanisms of postoperative complications such as CD.
Despite the growing use of tube-shunt surgery, limited information regarding the incidence and risk factors of postoperative CD is available. The incidence of CD after tube-shunt surgery ranges from 2.1 to 35.1%.12–16 ExG, older age, pseudophakia, diabetes mellitus, and systemic hypertension are known risk factors for CD after AGV implantation.12,13 In our previous study using the same cohort, we investigated risk factors for postoperative hyphema following BGI surgery.17 However, to the best of our knowledge, the risk factors for CD following BGI surgery have not yet been systematically investigated. Given the distinct aqueous humor dynamics and postoperative IOP profiles associated with this procedure, whether the risk factors identified in trabeculectomy and AGV apply to BGI remains unclear.
Therefore, we aimed to investigate the incidence of CD after BGI surgery and identify the clinical factors associated with its development.
Material and Methods
Participant Selection
This retrospective cohort study was approved by the Institutional Review Board of Fukui University Hospital (Japan) and adhered to the principles of the Declaration of Helsinki. The requirement for informed consent was waived, given the retrospective nature of the study. All data were anonymized prior to analysis, and patient confidentiality was maintained in accordance with institutional regulations.
We reviewed the data of consecutive adult patients (≥20 years) who underwent BGI surgery using a 350-mm2 endplate (BG101-350 or BG102-350; Abbott Medical Optics, Abbott Park, IL, USA) at Fukui University Hospital between April 1, 2012, and March 31, 2025. We excluded individuals whose eyes could not perceive light, with a history of tube-shunt implantation (including BGI or AGV), with a postoperative follow-up period <3 months, or who required additional intraocular surgery unrelated to postoperative CD management within 3 months of the initial procedure, including implant removal. When both eyes met the eligibility criteria, only data from the first operated eye was included to avoid inter-eye correlation. All surgeries were performed using a previously described standardized technique.16
Outcome Measures and Data Collection
We collected patient demographic, ocular, and surgical data, including sex, age, glaucoma subtype, lens status, central corneal thickness, axial length, tube insertion site, plate type and position, preoperative and postoperative IOP, number of glaucoma medications, history of previous intraocular surgery, and combined surgery status from medical records. We also recorded systemic comorbidities, including hypertension and diabetes mellitus.
The main outcome was the risk factors for CD occurrence as an early postoperative complication (within 3 months) of BGI surgery. Postoperative examinations were routinely performed at regular clinical follow-up visits, and the presence of CD was assessed based on fundoscopy by the treating glaucoma specialists and was defined as a solid-appearing elevation of the retina and choroid. When adequate fundus visualization was limited, including cases with media opacity, B-scan ultrasonography was used to assist in the diagnosis of CD.
Preoperative and postoperative IOP measurements were obtained from routine clinical examinations. We recorded the lowest postoperative IOP within 7 days of surgery, and the magnitude of postoperative IOP reduction (ΔIOP) was calculated as the difference between preoperative IOP and the lowest postoperative IOP in 7 days. Regarding the primary analysis that compared eyes with and without CD, postoperative IOP-related variables were evaluated using standardized early postoperative measurements applicable to all eyes, including the postoperative day 1 IOP and the lowest postoperative IOP within 7 days. For exploratory analyses of the eyes that developed CD, the lowest IOP before CD onset was defined as the lowest postoperative IOP recorded before or on the day of CD diagnosis. Early-onset CD was defined as CD occurring within 10 days after surgery, whereas delayed-onset CD was defined as CD occurring 30 days or later. No cases developed CD between postoperative days 10 and 29.
Statistical Analysis
Categorical variables were analyzed using the chi-squared or Fisher’s exact test, as appropriate. Continuous variables were compared using the Mann–Whitney U-test. Univariable logistic regression analyses were performed for each variable to assess associations with postoperative CD. Multivariable logistic regression analysis was subsequently performed to identify the independent factors associated with postoperative CD. Candidate covariates for the multivariable logistic regression model were selected a priori based on clinical relevance and previously published evidence, while considering the number of CD events and potential multicollinearity among variables. Statistical significance was set at P < 0.05. All statistical analyses were performed using the JMP Pro software (version 17.2.0; SAS Institute Inc., Cary, NC, USA).
Results
Patient Characteristics
We included the data of 261 eyes of Japanese patients. Postoperative CD developed in 48 eyes (18.4%); 16 of these had hypotony-related shallow or flat anterior chambers requiring anterior chamber reformation using viscoelastic material, and the remaining cases resolved without additional surgery. Baseline characteristics of eyes with and without postoperative CD are summarized in Table 1. Patients who developed CD were significantly older than those who did not (74.2 ± 11.5 vs. 66.0 ± 13.2 years, P < 0.01). The distribution of glaucoma subtypes also differed significantly between the two groups (P = 0.014), with ExG being more common in eyes with CD. Eyes with CD had a significantly higher prevalence of previous glaucoma filtration surgery (54.2% vs. 37.1%, P = 0.035), a lower prevalence of pars plana vitrectomy (18.8% vs. 39.4%, P < 0.01), significantly shorter axial length (24.1 ± 2.0 mm vs. 24.9 ± 2.3 mm, P = 0.015), significantly lower postoperative day 1 IOP (14.5 ± 13.9 mmHg vs. 22.6 ± 12.5 mmHg, P < 0.01), lower postoperative IOP within 7 days (6.3 ± 5.4 mmHg vs. 14.7 ± 6.8 mmHg, P < 0.01), and a significantly greater ΔIOP (24.1 ± 9.2 mmHg vs. 17.8 ± 11.6 mmHg, P < 0.01) than those without CD.
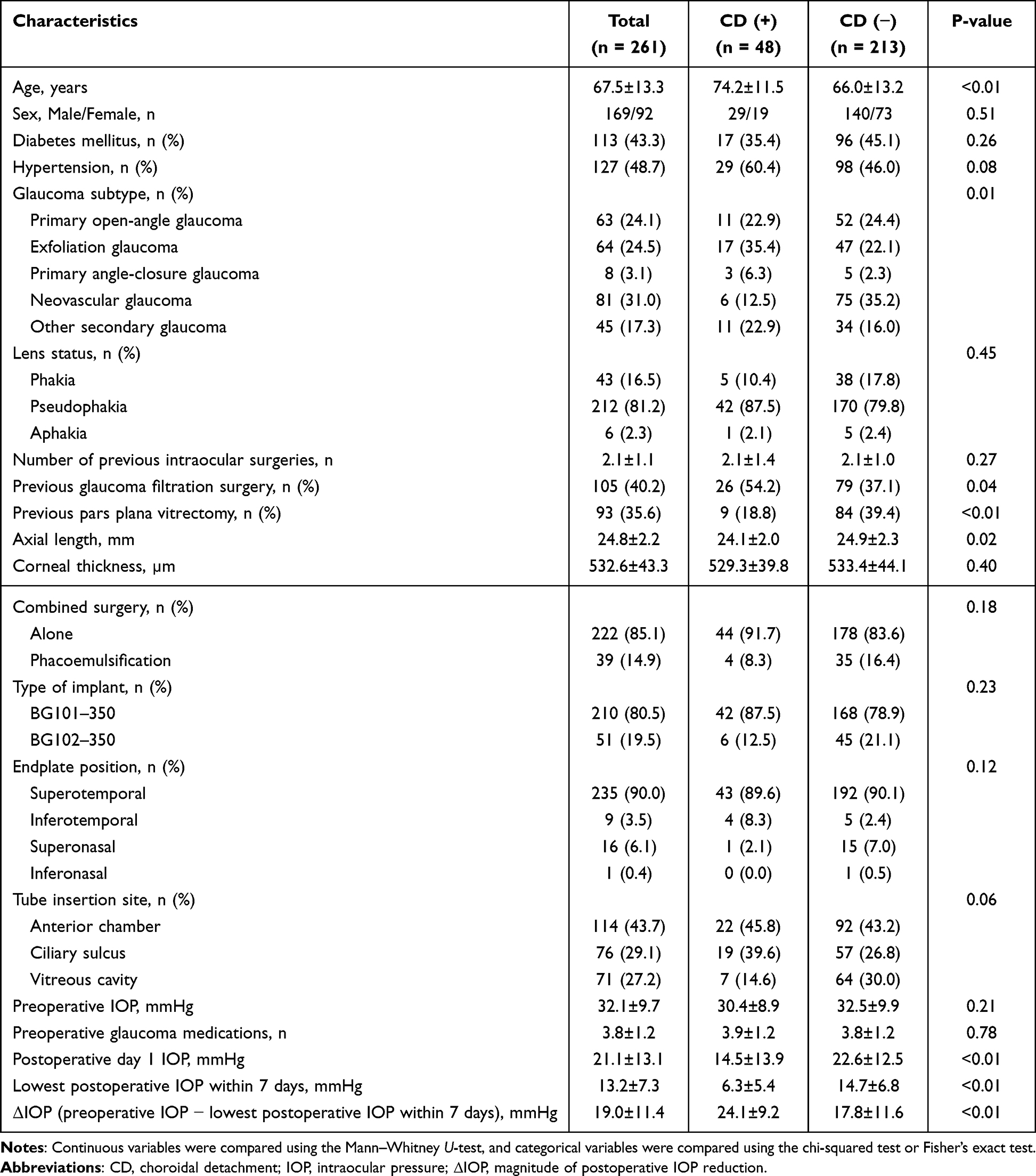 |
Table 1 Baseline and Perioperative Characteristics of Eyes with and without Postoperative CD |
Risk Factors for Postoperative CD
Univariable logistic regression analyses for factors associated with postoperative CD are summarized in Supplementary Table 1. Multivariable logistic regression analysis was performed to identify independent factors associated with postoperative CD (Table 2). Patient characteristics, including age, glaucoma type, previous glaucoma filtration surgery, previous pars plana vitrectomy, axial length, and ΔIOP (preoperative IOP − lowest postoperative IOP within 7 days), were assessed as potential determinants of postoperative CD. For regression analysis, glaucoma subtype was categorized as ExG versus non-ExG because previous studies have identified ExG as a potential risk factor for postoperative CD. Multivariable logistic regression analysis revealed that older age was significantly associated with an increased risk of CD (odds ratio [OR] 1.06, 95% confidence interval [CI] 1.03–1.11, P < 0.01). Additionally, a greater reduction in IOP was independently associated with CD (OR 1.08, 95% CI 1.04–1.12, P < 0.01). Other variables were not independently associated with CD after adjustment.
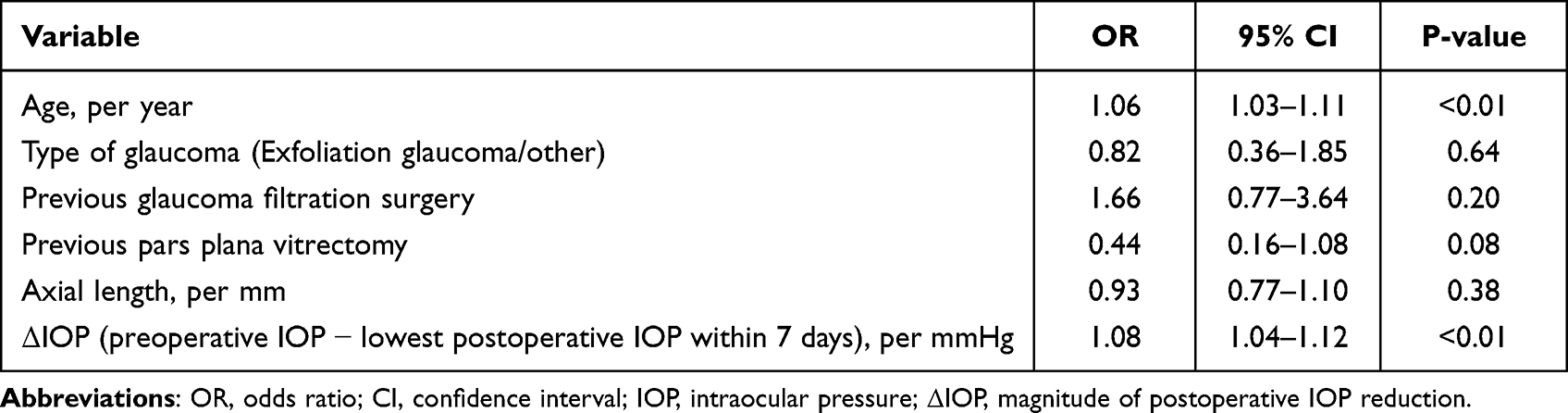 |
Table 2 Multivariable Logistic Regression Analysis for Postoperative CD After BGI Surgery |
Exploratory Analysis of Early- and Delayed-Onset CD
Among the 48 eyes that developed CD, 37 were classified as early-onset and 11 as delayed-onset CD (Supplementary Table 2). No cases developed CD between postoperative days 10 and 29. The mean time to CD onset was 3.8 ± 1.7 days (range 1–9 days) in the early-onset group and 48.4 ± 9.5 days (range 38–67 days) in the delayed-onset group. Eyes with early-onset CD had a significantly higher number of previous intraocular surgeries and longer axial lengths than those with delayed-onset CD. Additionally, the distribution of the tube insertion sites differed significantly between the two groups. The IOP on postoperative day 1 was significantly lower in the early onset CD group.
Discussion
In this retrospective cohort study, postoperative CD developed in 18.4% of the eyes following BGI surgery. Multivariable analysis showed that older age and greater postoperative IOP reduction were independently associated with CD. Additionally, exploratory analysis within the CD group suggested that early- and delayed-onset CD may have different clinical characteristics, and early-onset CD was associated with a greater number of previous intraocular surgeries, longer axial length, posterior tube placement, and lower postoperative day 1 IOP. The present study is distinct from our previous report focusing on postoperative hyphema,17 as it specifically investigates the incidence and risk factors of choroidal detachment following BGI surgery.
Postoperative CD is a known complication of glaucoma surgery that is generally associated with ocular hypotony, excessive aqueous outflow, and postoperative inflammation. The pathophysiology of CD involves inflammation and an acute reduction in IOP, resulting in a sudden shift in hydrostatic pressure. Consequently, serum transudates across the choriocapillaris and accumulates in the suprachoroidal space.18,19 The incidence of postoperative CD in this study (18.4%) falls within the range reported in previous studies on glaucoma drainage device surgery. This relative frequency underscores the need for careful postoperative observation after BGI implantation. Clinicians should note that CD may develop during the immediate and later postoperative periods following changes in tube resistance and aqueous outflow.
One of our main findings was that greater postoperative IOP reduction was independently associated with CD. This finding suggests that absolute postoperative hypotony and the magnitude of postoperative IOP reduction may play an important role in the pathogenesis of CD after BGI surgery. A rapid decrease in IOP may alter the trans-scleral and trans-choroidal pressure gradients, thereby facilitating the expansion of the choroid and the accumulation of suprachoroidal fluid. This observation was consistent with that of a previous report on trabeculectomy.7 In BGI surgery, such changes may be particularly relevant because the aqueous outflow is initially restricted by tube ligation and may increase abruptly as the ligature loosens or dissolves. Therefore, our findings suggest that dynamic postoperative IOP change may play an important role in the development of CD after BGI surgery. Because postoperative IOP-related variables were measured during the early postoperative period, particularly in early-onset cases, these findings should be interpreted as associations rather than definitive predictive factors. Although the tube is usually completely ligated during BGI surgery to prevent early postoperative hypotony, early IOP reduction may still occur in some eyes20 due to aqueous leakage through the Sherwood slit, leakage around the tube insertion site, and incomplete or loosened tube ligation. Contrarily, delayed IOP reduction is most likely related to spontaneous dissolution of the absorbable ligature, resulting in a sudden increase in aqueous outflow. Therefore, delayed-onset CD may be a postoperative event associated with restoration of aqueous flow after BGI surgery.
Consistent with findings of previous reports on postoperative CD following glaucoma surgery, older age was identified as an independent risk factor for CD.6,7,12,13 Age-related changes in scleral rigidity, choroidal vascular permeability, and ocular tissue compliance may make older eyes more susceptible to choroidal expansion in response to a sudden IOP reduction. Therefore, older patients undergoing BGI surgery may require closer postoperative monitoring, particularly when a marked IOP reduction is observed.
In univariable analysis, ExG, previous glaucoma filtration surgery, shorter axial length, absence of previous pars plana vitrectomy, and ciliary sulcus tube insertion were associated with postoperative CD. However, these factors were no longer significant after adjusting for covariates, suggesting that their effects may be partly mediated through postoperative IOP behavior rather than representing fully independent mechanisms. Eyes with previous filtration surgery or ExG may be more prone to unstable aqueous dynamics after surgery, which could ultimately result in greater postoperative IOP reduction and subsequent CD formation. Previous studies on trabeculectomy and AGV implantation have also identified ExG as a risk factor for postoperative CD.7,12 Similarly, vitreous cavity tube insertion may be associated with different postoperative aqueous humor dynamics compared with anterior chamber or ciliary sulcus insertion. However, tube insertion site was not included in the final multivariable model because of potential collinearity with previous pars plana vitrectomy and concerns regarding model stability given the limited number of CD events.
When comparing early- and delayed-onset CD, we found that early-onset CD was associated with lower IOP on postoperative day 1, suggesting immediate postoperative hypotony as an important mechanism in early-onset CD. Contrarily, delayed-onset CD may reflect a different process related to postoperative changes in aqueous outflow after spontaneous ligature dissolution. Since BGI surgery involves temporary tube occlusion with absorbable suture material, CD may occur in the immediate postoperative period and after the re-establishment of aqueous flow. This temporal variability may be characteristic of CD following BGI surgery. Interestingly, early-onset CD was also associated with a greater number of previous intraocular surgeries, longer axial lengths, and differences in the tube insertion site. These findings suggest that the structural vulnerability of the operated eye, altered intraocular fluid dynamics, and surgical complexity contribute to the timing of CD onset. Eyes that have undergone multiple intraocular surgeries may have altered ocular biomechanics or postoperative inflammatory responses, making them more susceptible to early postoperative hypotony-related changes. Similarly, posterior tube placement is a more complex surgery, causing different fluid dynamics in the eyes. However, as this subgroup analysis was exploratory and based on a limited number of cases, the findings should be interpreted with caution.
This study has some limitations. First, its retrospective design inherently introduced selection bias and unmeasured confounding factors. Second, the diagnosis of CD was primarily based on clinical findings. Wide-field imaging modalities, such as ultra-widefield fundus photography, were not used; therefore, small or peripheral CD may have been under-detected. Additionally, adequate fundus visualization is occasionally difficult in patients with an anterior chamber hyphema or vitreous hemorrhage. Although B-scan ultrasonography was performed when necessary, subtle CD may not have been fully captured, potentially leading to an underestimation of its true incidence. Third, the severity or extent of CD was not quantitatively graded using a standardized scoring system. Therefore, we were unable to analyze the risk factors according to CD severity. Fourth, postoperative management during the early postoperative period was not fully standardized and was left to the surgeon’s discretion. Variations in medical therapy or the timing of clinical interventions may have influenced postoperative IOP fluctuations and CD development. Finally, although all tubes were occluded with absorbable sutures at the time of surgery, early postoperative hypotony was observed in some eyes that subsequently developed CD. This finding suggests that subtle technical differences in ligation tightness or intraoperative aqueous dynamics may have influenced the early IOP behavior, which could not be fully quantified in this study. In addition, the exploratory comparison between early- and delayed-onset CD involved a relatively small number of delayed-onset cases, which may have limited the statistical power of this subgroup analysis. Moreover, this single-center study was conducted in the Japanese population, which may have limited the generalizability of our findings. Further prospective multicenter studies with standardized imaging protocols and severity grading systems are warranted to validate our results.
Conclusion
Postoperative CD after BGI surgery was associated with older age and greater postoperative IOP reduction. These findings suggest that rapid IOP reduction may play an important role in CD development after BGI surgery. Furthermore, the clinical differences observed between early- and delayed-onset CD may suggest that multiple mechanisms contribute to CD development in this setting. Careful postoperative monitoring, particularly in older patients and eyes with marked early IOP reduction, may help facilitate earlier detection and management of this complication.
Abbreviations
BGI, Baerveldt glaucoma implant; AGV, Ahmed glaucoma valve; CD, Choroidal detachment; IOP, Intraocular pressure.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Institutional Review Board of Fukui University Hospital in Japan (approval number: 20250191) and was conducted in accordance with the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective nature of the study. All patient data were anonymized before analysis, and patient confidentiality was strictly maintained in accordance with institutional and ethical guidelines.
Author Contributions
All authors made a significant contribution to the work reported, either in the conception, study design, execution, acquisition of data, analysis, or interpretation; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Lamping KA, Bellows AR, Hutchinson BT, et al. Long-term evaluation of initial filtration surgery. Ophthalmology. 1986;93(1):91–8. doi:10.1016/S0161-6420(86)33771-0
2. Costa VP, Arcieri ES. Hypotony maculopathy. Acta Ophthalmol Scand. 2007;85(6):586–597. doi:10.1111/j.1600-0420.2007.00910.x
3. Migdal C, Hitchings R. Morbidity following prolonged postoperative hypotony after trabeculectomy. Ophthalmic Surg. 1988;19(12):865–867.
4. Benson SE, Mandal K, Bunce CV, et al. Is post-trabeculectomy hypotony a risk factor for subsequent failure? A case control study. BMC Ophthalmol. 2005;5(1):7. doi:10.1186/1471-2415-5-7
5. Jampel HD, Musch DC, Gillespie BW, et al. Perioperative complications of trabeculectomy in the collaborative initial glaucoma treatment study (CIGTS). Am J Ophthalmol. 2005;140(1):16–22. doi:10.1016/j.ajo.2005.02.013
6. Haga A, Inatani M, Shobayashi K, et al. Risk factors for choroidal detachment after trabeculectomy with mitomycin C. Clin Ophthalmol. 2013;7:1417–1421. doi:10.2147/OPTH.S46375
7. Iwasaki K, Kakimoto H, Arimura S, et al. Prospective cohort study of risk factors for choroidal detachment after trabeculectomy. Int Ophthalmol. 2020;40(5):1077–1083. doi:10.1007/s10792-019-01267-6
8. Arora KS, Robin AL, Corcoran KJ, et al. Use of various glaucoma surgeries and procedures in medicare beneficiaries from 1994 to 2012. Ophthalmology. 2015;122(8):1615–1624. doi:10.1016/j.ophtha.2015.04.015
9. Vinod K, Gedde SJ, Feuer WJ, et al. Practice preferences for glaucoma surgery: a survey of the American Glaucoma Society. J Glaucoma. 2017;26(8):687–693. doi:10.1097/IJG.0000000000000720
10. Iwasaki K, Arimura S, Takamura Y, et al. Clinical practice preferences for glaucoma surgery in Japan: a survey of Japan Glaucoma Society specialists. Jpn J Ophthalmol. 2020;64(4):385–391. doi:10.1007/s10384-020-00749-w
11. Iwasaki K, Arimura S, Takamura Y, et al. Clinical practice preferences for glaucoma surgery in Japan in 2024. J Clin Med. 2025;14(6):2039. doi:10.3390/jcm14062039
12. Shin DY, Jung KI, Park HYL, et al. Risk factors for choroidal detachment after Ahmed valve implantation in glaucoma patients. Am J Ophthalmol. 2020;211:105–113. doi:10.1016/j.ajo.2019.10.035
13. Jin SW, Heo JW, Ahn HB. Comparison of choroidal detachment with and without hypotony after Ahmed valve implantation. Jpn J Ophthalmol. 2025;69(1):110–115. doi:10.1007/s10384-024-01138-3
14. Ying S, Coulon SJ, Lidder AK, et al. Choroidal effusions after glaucoma drainage implant surgery: risk factors and surgical management. Ophthalmol Glaucoma. 2023;6(5):530–540. doi:10.1016/j.ogla.2023.03.002
15. Iwasaki K, Kojima S, Wajima R, et al. Surgical outcomes of baerveldt glaucoma implant versus ahmed glaucoma valve in neovascular glaucoma: a retrospective multicenter study. Adv Ther. 2025;42(4):1745–1759. doi:10.1007/s12325-025-03128-4
16. Iwasaki K, Komori R, Arimura S, et al. Long-term outcomes of Baerveldt glaucoma implant surgery in Japanese patients. Sci Rep. 2023;13(1):14312. doi:10.1038/s41598-023-41673-6
17. Iwasaki K, Katsuo A, Arimura S, et al. Risk factors for postoperative hyphema following baerveldt glaucoma implant surgery: a Retrospective Cohort Study. J Clin Med. 2026;15(6):2247. doi:10.3390/jcm15062247
18. Bakir B, Pasquale LR. Causes and treatment of choroidal effusion after glaucoma surgery. Semin Ophthalmol. 2014;29(5–6):409–413. doi:10.3109/08820538.2014.959200
19. Schrieber C, Liu Y. Choroidal effusions after glaucoma surgery. Curr Opin Ophthalmol. 2015;26(2):134–142. doi:10.1097/ICU.0000000000000131
20. Iwasaki K, Kanamoto M, Arimura S, et al. Filtering blebs after baerveldt glaucoma implantation using magnetic resonance imaging: a prospective investigation. Ophthalmol Glaucoma. 2020;3(3):221–224. doi:10.1016/j.ogla.2020.01.003
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.