Back to Journals » Orthopedic Research and Reviews » Volume 11
Chondrosarcoma: the impact of comorbidity – 30 years of experience from a population-based database including 199 consecutive chondrosarcoma patients
Authors Aggerholm-Pedersen N ![]() , Maretty-Nielsen K, Baerentzen S, Jørgensen PH
, Maretty-Nielsen K, Baerentzen S, Jørgensen PH ![]() , Hansen BH, Baad-Hansen T
, Hansen BH, Baad-Hansen T ![]() , Keller J, Safwat A
, Keller J, Safwat A ![]()
Received 19 February 2019
Accepted for publication 23 July 2019
Published 3 September 2019 Volume 2019:11 Pages 109—116
DOI https://doi.org/10.2147/ORR.S205953
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Ninna Aggerholm-Pedersen1,2, Katja Maretty-Nielsen3, Steen Baerentzen3, Peter Holmberg Jørgensen4, Bjarne Hauge Hansen4, Thomas Baad-Hansen4, Johnny Keller4, Akmal Safwat1
1Department of Oncology, Sarcoma Centre of Aarhus University Hospital, Aarhus, Denmark; 2Department of Experimental Clinical Oncology, Sarcoma Centre of Aarhus University Hospital, Aarhus, Denmark; 3Department of Orthopaedic Surgery, Sarcoma Centre of Aarhus University Hospital, Aarhus, Denmark; 4Department of Pathology, Sarcoma Centre of Aarhus University Hospital, Aarhus, Denmark
Correspondence: Ninna Aggerholm-Pedersen
Department of Oncology, Sarcoma Centre of Aarhus University Hospital, Palle Juul-Jensensens Boulevard 99, Aarhus N 8200, Denmark
Email [email protected]
Background: Adjustment for comorbidity when investigating potential prognostic factors, especially in elderly cancer patients, is imperative. Patients diagnosed with chondrosarcoma are elderly and more comorbidity is expected for these patients. Demographic changes are awaited in the future resulting in more and more elderly patients with comorbidity. The aims of this study were to characterize patients with chondrosarcoma treated at a single institute and to evaluate various prognostic factors for survival adjusted for comorbidity.
Material and methods: Between 1979 and 2008, 199 patients were treated at the Sarcoma Centre of Aarhus University Hospital, for chondrosarcoma. The incidence was calculated as a WHO age-standardized incidence rate (IR) per million per year. The endpoints were overall mortality and disease-specific mortality. Possible prognostic factors were analyzed for patients with intermediate/high-grade localized tumors by the uni- and multivariate Cox-proportional hazard method.
Results: The WHO age-standardized IR in western Denmark in the period 1979–2008 was 2.4/million inhabitants/year (95% CI: 2.2;2.6). The 5-year overall and disease-specific mortality for the 199 patients were 29% (95% CI: 23;36) and 22% (95% CI: 16;27), respectively. The 5-year disease-specific mortality for patients with metastatic disease was significantly higher than for patients with localized disease. The median time to relapse was 2.0 years. Patients who relapse within 1 year after the primary diagnosis have a significantly higher 5-year overall mortality compared to patients who relapse after 1 year. The presence of comorbidity and high-grade tumors were independent prognostic factors for both the overall mortality and the disease-specific mortality of chondrosarcoma patients.
Conclusion: Patients with comorbidity had a significantly increased overall mortality and disease-specific mortality. We found that adjusting for comorbidity is important when investigating a cohort of elderly patients.
Keywords: chondrosarcoma, comorbidity, prognostic factors
Introduction
Chondrosarcoma is a rare cancer with an age-standardized incidence rate (IR) of about 2/million inhabitants/year.1,2 Even though the prognosis for chondrosarcoma patients is good, nearly 6% of the patients will present with distant metastasis at the time of diagnosis3–5 and about 25% will experience local relapse.4,6,7 At some point, either after local recurrence or as primary progression, 10–30% of the patients will develop distant metastasis.6,7 Therefore, it is important to categorize patients into risk groups according to different patients, tumor, and treatment-related factors to optimize treatment modalities for those patients with the worst prognosis.
Surgery is the primary treatment modality for chondrosarcoma and neither chemotherapy nor radiation therapy has any documented effect on recurrence rate. Age has been shown to be an important prognostic factor in some studies,8,9 whereas in other studies the age is not important regarding the prognosis.10,11
We have previously shown the importance of comorbidity for survival in bone sarcoma patients.12 Because chondrosarcoma affects elderly patients, more comorbidity is expected, and when looking at potential prognostic factors it is imperative that adjustments are made for comorbidity. Demographic changes are awaited in the future resulting in more and more elderly patients with comorbidity.13
In this study, we have investigated all patients treated at a single institution, servicing the population of western Denmark from 1979 to 2008 with the aims of characterizing patients with chondrosarcoma and evaluating various prognostic factors for disease-specific survival adjusted for potential confounders such as comorbidity.
Materials and methods
Patient selection
Patients diagnosed with either conventional or dedifferentiated chondrosarcoma of the bone, treated at the Aarhus Sarcoma Centre, between January 1979 and December 2008, were included in this study. Exclusion of 15 patients with borderline or uncertain malignancy grade resulted in a study cohort of 199 patients. For the incidence calculation, additional 19 patients were included. For these 19 patients, the hospital records could not be retrieved. Patients with low-grade chondrosarcoma, as well as patients whom we could not retrieve the hospital records, were not included in the survival analyses. The study cohort for the survival analysis comprised 108 patients. Only patients with intermediate/high-grade localized tumors who underwent curative intended surgery were included in the multivariate analysis. This study cohort included 92 patients. The patients included in this study have previously been part of a publication on comorbidity in bone sarcoma patients.12
Data sources
Clinical data were obtained from the validated population-based Aarhus Sarcoma Registry,14 which contains comprehensive clinical information on each sarcoma patient from 1979 to 2008 in a well-defined geographic area of Denmark. The low-grade chondrosarcomas and enchondromas are problematic. However, all pathology reports were done by a pathologist specialized in sarcoma. The primary differentiation between low-grade chondrosarcoma and enchondromas was made by the growth pattern of the tumor cells in combination with the appearance on the radiological examinations. Enchondromas were defined as well-defined radiologic and without permeate/infiltrative growth pattern. Low-grade chondrosarcomas were defined as radiologic destructive and histological permeate/infiltrative growth pattern. The National Patient Registry15 was used to obtain data on comorbidity. All discharge diagnoses from January 1, 1977, until the date of sarcoma diagnosis were used. Diagnoses within 30 days and all cancer diagnoses within 90 days prior to the primary diagnosis of sarcoma were excluded. The vital status and cause of death were registered through linkage to the Central Population Registry16 and Cause of Death Registry.17 Linkage between the different registries was done on an individual level by the 10-digit civil personal registration number which since 1968 has been assigned to all Danish citizens.
Data analysis and statistics
The incidence was calculated as an overall age-standardized IR18 using the WHO standard population and data from StatBank Denmark.19 The endpoints were overall mortality and disease-specific mortality, timed from date of diagnosis until death with sarcoma, as death from other causes was regarded as a competing event when analyzing disease-specific mortality. The study ended on October 9, 2013, and patients who were alive at this date were censored. The cumulative incidence function was reported for disease-specific mortality. Crude and adjusted analyses were performed using the Cox-proportional hazard mode. Based on the result of literature review and number of events, the following variables were included in the adjusted analysis: age, comorbidity, size of the primary tumor, histological type, grade, margin, and soft tissue extension. Directed acyclic graphs (DAGs) by DAGitty software20 were used to determine the relations between potential explanatory variables (Figure S1). Based on the DAG, comorbidity was adjusted for age, margin, soft tissue extension, and size. Soft tissue extension was adjusted for age, comorbidity, margin, and size. Histological types were adjusted for age, size, and grade. Size was adjusted for age, comorbidity, histological type, soft tissue extension, grade, and margin. Grade was adjusted for size and histological type. Margin was adjusted for age, comorbidity, soft tissue extension, and size. All variables were analyzed as categorical variables based on the literature except age. The categorization of age did not meet the assumption of proportional hazard, and therefore age was regarded as a time-dependent variable. Comorbidity was assessed using the Charlson Comorbidity Index and categorized into no comorbidity or comorbidity (Table S1). Size was categorized into ≤8/>8 cm. Margin was categorized into wide, marginal, and intralesional; the margin was defined as wide if the tumor was resected in toto surrounded by 1–2 mm of healthy tissue. Histological types were categorized into classic and dedifferentiated chondrosarcoma; in the classic group, one patient with myxoid and two patients with mesenchymal chondrosarcomas were included. Soft tissue extension was categorized into yes/no. For all analyses, a 5% level of significance was used in this study. The software program STATA 13 was used.
Ethics
The study has been approved by the Ethics Committee of Denmark and the Danish Agency of Data Protection.
Results
Incidence of chondrosarcoma in western Denmark
The 199 patients included in this study corresponded to 91% of all chondrosarcoma patients in western Denmark from 1979 to 2008. Only 30 additional patients were found in the Danish Cancer Registry. Of these patients, 11 had uncertain diagnoses and the diagnosis could not be verified in the Pathology Registry. The hospital records of the remaining 19 patients could not be retrieved, and all these patients were treated outside the center or had their diagnosis postmortem. The WHO age-standardized IR in western Denmark in the period 1979–2008 was 2.4/million inhabitants/year (95% CI: 2.2;2.6) including these extra 19 patients.
Patients and tumor characteristics
The median age at diagnosis was 54 years (range 2–86 years), with 57% being males. The most frequent site of the tumor was the lower extremities (n=96) and axial/pelvis region (n=73). Only 10% of the patients had the histological type dedifferentiated chondrosarcoma (n=19). At the time of diagnosis, 11 (6%) of the patients had metastatic disease. Most patients underwent resection (n=138) or amputation (n=44) of the primary tumor. The percentages of limp-sparing procedures and amputations were not significantly different between the different year groups. The only difference in surgery procedures during this period was an increased use of rotations skin graft in the last 10 years. Yet, 17 patients were not treated with surgery at any time. Of these patients, six patients had metastatic disease; two patients received radiation therapy, and the rest were aged 77–83 and had either low-grade tumors or comorbidity.
Radiation therapy was given to 15 patients. For most patients as a palliative treatment, four patients were treated with curative intent without prior surgery, and these patients were treated with a total dose from 45 to 64 Gy. The remaining patients were treated with adjuvant radiation therapy after surgery, and the total dose given was 50 or 60 Gy.
Chemotherapy was used for four patients as palliative treatment and for three patients as adjuvant treatment to surgery. Of these patients, one had a mesenchymal chondrosarcoma and two had other traditional chondrosarcomas.
At the end of the primary treatment 169 patients (85%) were without evidence of disease and 29 (15%) patients were not primarily cured. A total of 56 (33%) patients did experience relapse. The patient, tumor, and treatment characteristics are shown in Table 1.
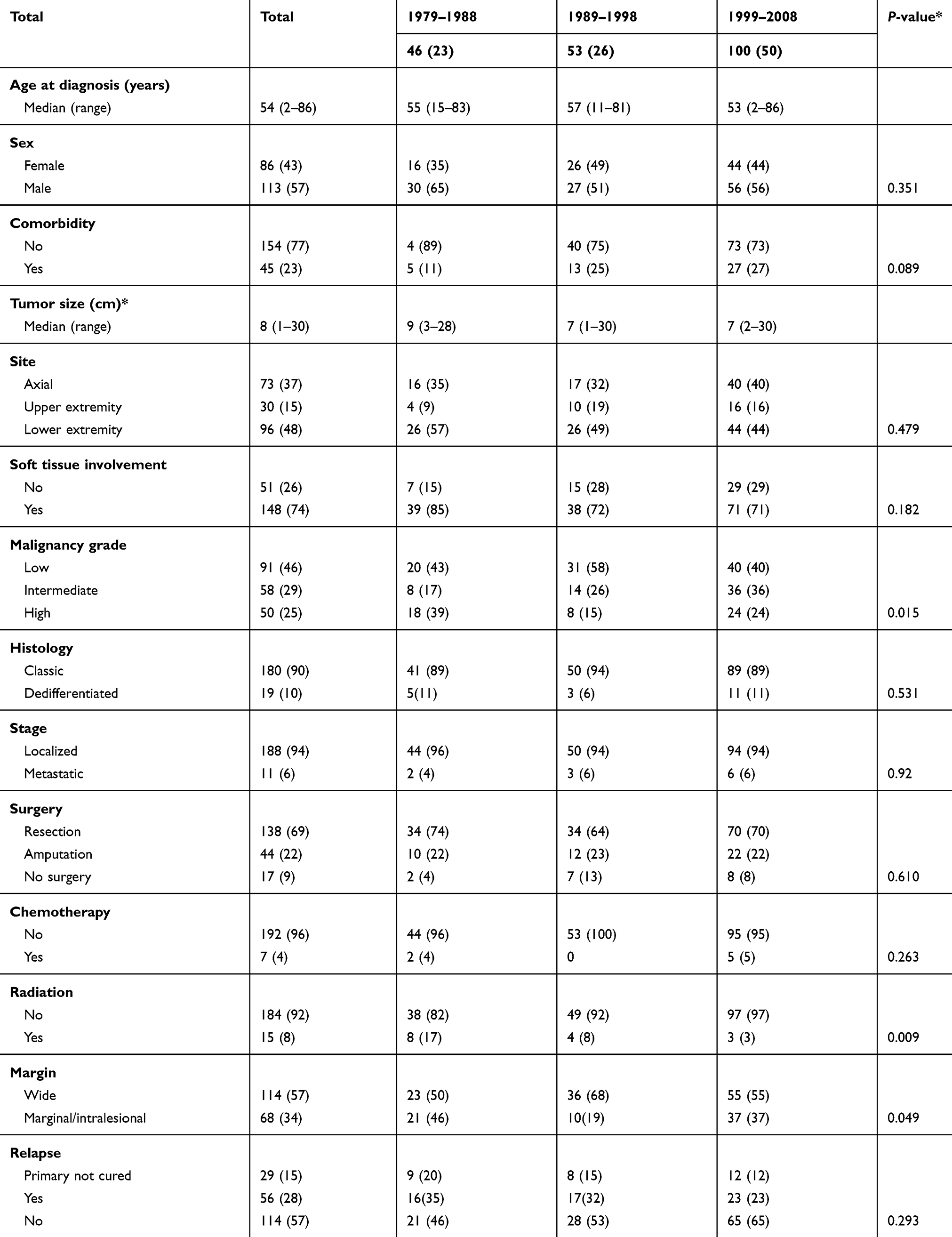 |
Table 1 Patient, tumor, and treatment characteristics of patients treated for chondrosarcoma (N=199) according to year of diagnosis. The values are number (%) |
Overall mortality
The 5-year overall mortality for the whole cohort of 199 patients was 29% (95% CI: 23;36); for patients with metastatic disease, the 5-year overall mortality was 91% (95% CI: 67;99) which was significantly higher than for patients with localized disease, 26% (95% CI: 20;33). Patients with intermediate/high-grade localized tumors who underwent curative intended surgery were included in the rest of the analysis (n=92) of overall survival. Fifty-one patients died during follow-up. The overall 5-year mortality was 35% (95% CI: 26;46). The cumulative incidence function of overall mortality for the 92 patients is shown in Figure 1.
 |
Figure 1 Cumulative incidence of localized chondrosarcoma treated with surgery by overall mortality and disease-specific mortality (solid lines) with 95% CI (dash lines), n=92. |
 |
Figure 2 Adjusted cumulative incidence of disease-specific mortality according to comorbidity (A), soft tissue extension (B), histological type (C), size (D), grade (F), and margin (G) using competing risk model. Comorbidity was adjusted for age, size, soft tissue extension, and margin. Soft tissue extension was adjusted for size, age, comorbidity, and margin. Histological type was adjusted for age, size, and grade. Size was adjusted for age, comorbidity, histological type, soft tissue extension, grade, and margin. Grade was adjusted for size and histological type. Margin was adjusted for age, comorbidity, soft tissue extension, and size. |
The presence of comorbidity and high grade of the tumor were independent adverse prognostic factors for overall mortality. The crude and adjusted analyses of potential prognostic factors for overall mortality are shown in Table 2. There were no significant difference regarding the site of the tumor.
 |
Table 2 Crude and adjusted analysis of potential prognostic factor for overall and disease-specific mortality for patients with localized high-grade disease and treated with surgery. N=92 |
Disease-specific mortality
The 5-year disease-specific mortality rate for the 199 patients was 22% (95% CI: 16;27); for patients with metastatic disease, the 5-year disease-specific mortality was 91% (74;108) which was significantly higher than patients with localized disease, 18% (95% CI: 13;23). Patients with high-grade tumors had a significantly higher 5-year disease-specific mortality of 36% (95% CI: 21;51) compared to 8% (95% CI: 3;13) for patients with low- or intermediate-grade tumors. In the rest of the disease-specific mortality analysis, patients with intermediate/high-grade localized disease treated with curative intended surgery were included resulting in 92 patients. Twenty-six (28%) patients died with sarcoma during follow-up. This corresponded to a 5-year disease-specific mortality of 23% (95% CI: 14;32). Figure 1 shows the cumulative incidence function of disease-specific mortality.
High grade and comorbidity were independent prognostic factors associated with a high disease-specific mortality see Figure 2. The crude and adjusted analyses of potential prognostic factors for disease-specific mortality are shown in Table 2.
Patients with relapse
The median time to relapse was 2.1 years. Patients who relapsed within 1 year after the primary diagnosis had a significantly higher 5-year overall mortality compared to patients who relapsed after 1 year, 96% (95% CI: 84;100) and 70% (95% CI: 54;85), respectively. The 5-year overall mortality for patients who experienced relapse within 2 years after the primary diagnosis was 86% (95% CI: 73;94).
Discussion
This study is, to the best of the authors’ knowledge, the first study to assess the problem of comorbidity in chondrosarcoma patients when reporting prognostic factors for this rare cancer. Many patients with chondrosarcoma have an excellent prognosis after adequate surgery and for most patient’s relapse will not occur after primary surgery. We found that 68% of primarily cured patients did not experience local or distant relapse.
This retrospective study shows that the overall and disease-specific mortality for patients with intermediate/high-grade localized disease are different. This interesting finding could be a consequence of an elderly patient’s cohort dying from other causes than chondrosarcoma. Only patients with high-grade localized chondrosarcoma were included in the survival analysis, resulting in a total cohort of 92 patients over a period of 30 years.
The overall mortality and the disease-specific mortality reported were comparable to the findings of other studies.3,5–7,21,22 Disease-specific mortality is dependent on correct evaluation of the causes of death. This is particularly important for chondrosarcoma patients who, in general, are elderly patients, and death due to other causes matters. It has been reported that 70% of the chondrosarcoma patients are over the age of 40.3 In the present study, 78% of the patients diagnosed with chondrosarcoma were over the age of 40, which shows the importance of reporting the disease-specific mortality rather than the overall mortality when analyzing possible prognostic factors because many patients will die from other causes than chondrosarcoma. The major strengths of this investigation are the population-based cohort and the possibility of individual linkage to national registries resulting in detail about comorbidity and cause of death. Furthermore, in this study, we have a complete follow-up until the date of analysis for all patients who are included.
The sex of the patients has been investigated in previous studies, and no significance regarding the prognosis has been shown;5,10,11 therefore we did not investigate the prognostic value of sex. In another study, age has been shown to be an independent prognostic factor for overall survival. However, when analyzing the prognostic value of age using disease-specific mortality as in the present study, age did not meet the assumption about proportional hazard and was included as a time-dependent variable and used for adjustment. The prognostic value of the surgical margin has been investigated numerous times, and some papers have reported that inadequate surgical margin is associated with a poorer overall survival.4,6,8,23 Our results also found surgical margin to be a prognostic factor for overall survival as well as disease-specific survival.
The most common site of the primary tumor in the present study was the long bones of the lower limp followed by the pelvic bones which also has been reported elsewhere.3 The prognostic role of site for overall survival has previously been investigated,24 and no association has been found. Therefore, tumor site was not included in this analysis. Corresponding to our findings, size has not been shown to have an impact on overall survival.7,25 However, even though the result was not significant, there was a tendency toward a higher mortality when the tumor was >5 cm.
The importance of tumor grade in our study was previously seen in a large study by Giuffrida et al5 including 2890 chondrosarcoma patients with both localized and metastatic disease at the time of diagnosis, which reported that only stage and grade of the tumor were independent prognostic factors for disease-specific survival. Similarly, Fiorenza et al found that extra compartmental spread of localized chondrosarcoma and the grade of the tumor were independent prognostic factors for chondrosarcoma patients.7
In conclusion, in patients treated surgically for localized intermediate/high-grade chondrosarcoma, the presence of comorbidity and high-grade tumors were independent prognostic factors for overall mortality and disease-specific mortality. We found that adjusting for comorbidity is important when investigating a cohort of elderly patients.
Acknowledgment
The study was supported by a scholarship from Aarhus University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stiller CA, Bielack SS, Jundt G, Steliarova-Foucher E. Bone tumours in European children and adolescents, 1978-1997. Report from the automated childhood cancer information system project. Eur J Cancer. 2006;42(13):2124–2135. doi:10.1016/j.ejca.2006.05.015
2. Whelan J, McTiernan A, Cooper N, et al. Incidence and survival of malignant bone sarcomas in England 1979-2007. Int J Du Cancer. 2012;131(4):E508–17. doi:10.1002/ijc.26426
3. Damron TA, Ward WG, Stewart A. Osteosarcoma, chondrosarcoma, and Ewing’s sarcoma: National Cancer Data Base Report. Clin Orthop Relat Res. 2007;459:40–47. doi:10.1097/BLO.0b013e318059b8c9
4. Lee FY, Mankin HJ, Fondren G, et al. Chondrosarcoma of bone: an assessment of outcome. J Bone Joint Surg Am. 1999;81(3):326–338. doi:10.2106/00004623-199903000-00004
5. Giuffrida AY, Burgueno JE, Koniaris LG, Gutierrez JC, Duncan R, Scully SP. Chondrosarcoma in the United States (1973 to 2003): an analysis of 2890 cases from the SEER database. J Bone Joint Surg Am. 2009;91(5):1063–1072. doi:10.2106/JBJS.H.00416
6. Bjornsson J, McLeod RA, Unni KK, Ilstrup DM, Pritchard DJ. Primary chondrosarcoma of long bones and limb girdles. Cancer. 1998;83(10):2105–2119.
7. Fiorenza F, Abudu A, Grimer RJ, et al. Risk factors for survival and local control in chondrosarcoma of bone. J Bone Joint Surg Br. 2002;84(1):93–99. doi:10.1302/0301-620X.84B1.11942
8. Daugaard S, Myhre-Jensen O, Schiodt T, et al. Clinical and histopathological prognostic factors in chondrosarcomas. Sarcoma. 1997;1(1):47–54. doi:10.1080/13577149778470
9. Duchman KR, Lynch CF, Buckwalter JA, Miller BJ. Estimated cause-specific survival continues to improve over time in patients with chondrosarcoma. Clin Orthop Relat Res. 2014;472:2516–2525. doi:10.1007/s11999-014-3600-3
10. Marcove RC, Mike V, Hutter RV, et al. Chondrosarcoma of the pelvis and upper end of the femur. An analysis of factors influencing survival time in one hundred and thirteen cases. J Bone Joint Surg Am. 1972;54(3):561–572. doi:10.2106/00004623-197254030-00009
11. Pritchard DJ, Lunke RJ, Taylor WF, Dahlin DC, Medley BE. Chondrosarcoma: a clinicopathologic and statistical analysis. Cancer. 1980;45(1):149–157. doi:10.1002/1097-0142(19800101)45:1<149::aid-cncr2820450125>3.0.co;2-a
12. Aggerholm-Pedersen N, Maretty-Nielsen K, Keller J, Baerentzen S, Safwat A. Comorbidity in adult bone sarcoma patients: a population-based cohort study. Sarcoma. 2014;2014:690316. doi:10.1155/2014/690316
13. Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74(11):2913–2921. doi:10.1158/0008-5472.CAN-14-0155
14. Maretty-Nielsen K, Aggerholm-Pedersen N, Keller J, Safwat A, Baerentzen S, Pedersen AB. Population-based Aarhus Sarcoma Registry: validity, completeness of registration, and incidence of bone and soft tissue sarcomas in western Denmark. Clin Epidemiol. 2013;5:45–56. doi:10.2147/CLEP.S41835
15. Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health. 2011;39(7 Suppl):30–33. doi:10.1177/1403494811401482
16. Storm HH, Michelsen EV, Clemmensen IH, Pihl J. The Danish Cancer Registry–history, content, quality and use. Dan Med Bull. 1997;44(5):535–539.
17. Helweg-Larsen K. The Danish register of causes of death. Scand J Public Health. 2011;39(7 Suppl):26–29. doi:10.1177/1403494811399958
18. Ahmad O, Boschi-Pinto C, Lopex A, et al. Age standardization of rates: a new WHO standard. GPE Discussion Paper Series: No.31 EIP/GPE/EBD Geneva: World Health Organization; 2001.
19. Statistic Denmark, Population Denmark; 2013. Available from: https://www.dst.dk/en/Statistik/emner/befolkning-og-valg/befolkning-og-befolkningsfremskrivning/folketal. Accessed November 2, 2018.
20. Textor J, Hardt J, Knuppel S. DAGitty: a graphical tool for analyzing causal diagrams. Epidemiology (Cambridge, Mass). 2011;22(5):745. doi:10.1097/EDE.0b013e318225c2be
21. Evans HL, Ayala AG, Romsdahl MM. Prognostic factors in chondrosarcoma of bone: a clinicopathologic analysis with emphasis on histologic grading. Cancer. 1977;40(2):818–831. doi:10.1002/1097-0142(197708)40:2<818::aid-cncr2820400234>3.0.co;2-b
22. Sanerkin NG, Gallagher P. A review of the behaviour of chondrosarcoma of bone. J Bone Joint Surg Br. 1979;61-B(4):395–400. doi:10.1302/0301-620X.61B4.500746
23. Rizzo M, Ghert MA, Harrelson JM, Scully SP. Chondrosarcoma of bone: analysis of 108 cases and evaluation for predictors of outcome. Clin Orthop Relat Res. 2001;391:224–233. doi:10.1097/00003086-200110000-00025
24. Puri A, Shah M, Agarwal MG, Jambhekar NA, Basappa P. Chondrosarcoma of bone: does the size of the tumor, the presence of a pathologic fracture, or prior intervention have an impact on local control and survival? J Cancer Res Ther. 2009;5(1):14–19.
25. Jakobsen KR, Paulsen BS, Baek R, Varming K, Sorensen BS, Jorgensen MM. Exosomal proteins as potential diagnostic markers in advanced non-small cell lung carcinoma. J Extracell Vesicles. 2015;4:26659. doi:10.3402/jev.v4.26659
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.