Back to Journals » Psychology Research and Behavior Management » Volume 15
Chinese Translation and Psychometric Testing of the Simplified Version of Social Support Scale for Physical Activity
Authors Mao X, Mao X, Yu Y ![]() , Guo J
, Guo J ![]()
Received 9 March 2022
Accepted for publication 7 July 2022
Published 22 September 2022 Volume 2022:15 Pages 2691—2700
DOI https://doi.org/10.2147/PRBM.S365639
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Xia Mao,1 Xianhua Mao,1 Yu Yu,2 Jia Guo3
1Department of Nursing, Yueyang Vocational Technical College, Yueyang, People’s Republic of China; 2Department of Psychiatry, Yale School of Medicine, New Haven, CT, USA; 3Department of Clinical Nursing, Xiangya School of Nursing, Central South University, Changsha, People’s Republic of China
Correspondence: Jia Guo, Department of Clinical Nursing, Xiangya School of Nursing, Central South University, Changsha, People’s Republic of China, Tel +86 13875947418, Fax +86 0731-82650266, Email [email protected]
Purpose: Sallis et al’s social support scale for physical activity (SSSPH) is one of the most widely used scales to measure exercise-related social support yet has never been translated and validated in Chinese. The current study aims to simplify, translate, and validate a short form of SSSPH in a Chinese population.
Patients and Methods: A simplified Chinese version of the SSSPH (SSSPH-SC) retaining 6 items was achieved after the translation and back-translation process, which showed good content validity. The scale was then assessed among a convenience sample of 266 Chinese adults from various backgrounds. Internal consistency was tested by calculating Cronbach’s α. The a priori two-factor structure was tested with confirmatory factor analysis (CFA). Concurrent validity was examined by investigating the correlation of the SSSPH-SC with general social support, quality of life, and self-rated health.
Results: The SSSPH-SC full scale and subscales showed good internal consistency with Cronbach’s alpha ranging from 0.87 to 0.92. The CFA supported the a priori two-factor structure: family support and friend support, with χ 2/df=2.93, CFI = 0.98, TLI = 0.98, RMSEA = 0.07, SRMR = 0.035. The concurrent validity of the SSSPH-CS was further supported by its significant positive correlations with social support (r=0.26, p< 0.001), quality of life (r=0.25, p< 0.001), and self-rated general health depression (r=0.23, p< 0.001).
Conclusion: The SSSPH-SC had good reliability and validity and could be used as a simple and effective tool for assessing social support for physical activity in Chinese adults. The scale can be used as an effective tool to guide future health promotion programs as well as an evaluation tool to assess intervention effects.
Keywords: short form, reliability, validity, confirmatory factor analysis
Plain Language Summary
It has been well-known that physical activity is beneficial to population health and social support is an important protective factor for physical activity. A good measurement tool is thus needed to better understand and evaluate social support for physical activity. The Sallis’ social support scale for physical activity (SSSPA) has been widely used and validated in many other countries but not in China yet. Our study is the first to simplify the 20-item SSSPA into 6 items and translate it into a Chinese version—the Simplified Chinese version of SSSPA (SSSPA-SC), and test it among the Chinese population. Our results showed that the SSSPA-SC was both reliable and valid in assessing social support for physical activity, with two dimensions: family support and friend support. In addition, the SSSPA-SC is more applicable for quick screening on busy occasions due to its short item number and minimization of respondent burden. Introducing this scale into mainland China could ensure the standardized evaluation of social support for physical activity as well as a guide for further intervention program evaluation.
Introduction
The global pandemic of the Coronavirus disease 2019 (COVID-19) and the lockdown policy have significantly reduced people’s physical activity, which plays an essential role in the prevention and treatment of certain diseases and maintenance of well-being.1 Physical inactivity due to sustained quarantine and social distancing can significantly impair the body’s immunity and increase the risk of viral infection, respiratory disease, cardiovascular disease, musculoskeletal disease, etc.1 Lack of physical activity has been a rampant issue challenging population health all over the world. According to the World Health Organization,2 1 in 4 adults, and over 80% of adolescents do not meet the global recommended levels of physical activity. This situation was further aggravated by the COVID-19 pandemic. It is thus both urgent and essential to identify determinants of physical activity to develop and implement effective intervention programs to improve physical activity.3,4 Among various factors, social support has been demonstrated as one of the most important and modifiable factors for physical activity.3,4
Social support refers to the “help or care received in personal relations and interpersonal exchanges”, which can be further categorized into various types (emotional, instrumental, informative, and evaluative) and sources (family and friends).5 Social support is especially important during the COVID-19 pandemic as it may serve as a buffer against psychological distress caused by the pandemic, which helps people to cope better with the health challenges and maintain well-being. Social support for physical activity is characterized by the assistance received from different social groups (such as family and friends) to assist in the behaviors of physical activity.5 The positive effect of social support in promoting physical activity during the pandemic has been well understood, with consistent evidence showing social support as a significant indicator and predictor of physical activity and thus promotes health.3,4,6 Several literature reviews have suggested a positive association between social support and physical activity among people of various ages such as adolescents,7 college students,8 and the elderly;9 as well as people with various health conditions such as people living with HIV/AIDS,10 mental disorders,11 and cancers.12 In addition, social support has also been widely associated with a wide range of health outcomes, such as quality of life and general health.13–15
Although there have been a large number of various measures developed to assess social support, most attempt to measure general social support, which may be different from specific social support targeted at physical activity.16 In 1987, Sallis et al16 developed a social support scale for physical activity (SSSPA), which has now been one of the most widely used scales for physical activity social support assessment. This scale was developed in 2 stages that started with structured in-depth interviews to identify physical activity-related interpersonal behavior items, followed by item analysis, reliability, and validity testing.16 Finally, a 20-item scale was developed comprising two subscales: the friend support subscale (5 items) and the family support subscale (15 items).16 The SSSPA has shown good reliability and validity both in the original study and in the following validation studies that translated the scale into other languages.16–19
However, the SSSPA has never been translated into Chinese and validated in a Chinese population. In addition, the item number of the scale is unbalanced between its two subscales, with much more items on the family support scale than on the friend support scale. In a recent review conducted by Morgado et al,20 item limitation has been listed among the top ten major limitations of scale development, with unbalanced item numbers among factors being a potential limitation that may weaken the psychometric properties of the scale and restrict its generalizability and future applicability. Furthermore, the original 20 items of the scale may be too lengthy for use in quick rapid assessment among a large population. In light of these limitations, the current study was conducted to simplify the Sallis’s SSSPA into a short version; translate it into Chinese, and validate it for a Chinese population.
Materials and Methods
The Simplified Chinese Version of the SSSPH (SSSPH-SC)
We obtained the approval for simplification and translation of the Sallis’ SSSPH from the original developer of the scale. For simplification of the scale, we removed the 10 additional items that only exist in the family subscale but not in the friend subscale to keep the same item number and weight between the two subscales. Among the remaining 5 similar items in each subscale, we kept the following 3 items: “offered to exercise with me”, “exercised with me”, and “gave me encouragement to stick with my exercise program” since they represent a gradual process of behavior changes: intention—action—maintenance. As a result, a final 6-item short version of the SSSPH (SSSPH-S) was extracted.
The 6-item SSSPH was translated into Mandarin Chinese based on Brislin’s (1986)21 adapted translation model that includes forward translation, back translation, and practical application. This process aimed to achieve semantic and conceptual equivalence between the Chinese version of the SSSPH-S and the original version of the SSSPH-S. The forward translation was completed by two nurse researchers who were native Chinese speakers and proficient in English. The first Chinese version of the SSSPH-S through forward translation was then translated back into English by a professional translator who was completely blinded to the original version of the instrument. The back-translation was then sent to the developer of the original scale for discussion of further revision, leading to a final version: the Simplified Chinese version of the Social Support Scale for Physical Activity (SSSPH-SC).
Content validity of the SSSPH-SC was performed among an expert committee of 7 clinical nurses to assess their agreement on relevance and intelligibility. This process aimed to identify any conceptually or culturally inappropriate items and make further item modifications. The committee was asked to rate each item on a four-point Likert scale from “1” = not relevant to “4” = highly relevant. Two forms of content validity index (CVI) were calculated: CVI for the item (I-CVI) and CVI for scale (S-CVI). I-CVI was calculated by dividing the number of experts in agreement by the number of total experts, while the S-CVI was calculated by averaging the I-CVI scores across all items.22 Items with I-CVI <0.78 were further revised accordingly.22 After several rounds of discussion and revision, the SSSPH-SC achieved good content validity with I-CVI >0.80, and S-CVI = 0.86.
Participants and Procedure
This cross-sectional study was conducted from May 2020 to August 2020 among healthy adults recruited in Yueyang city, Hunan province, China. In order to get a general population sample that is as diverse as possible, a convenience sampling method was adopted to recruit participants from the following three different research sites: the Yueyang Vocational Technical College, the Yueyang Baling Petrochemical Company, and the Shiying village, Huarong County of Yueyang City. Participants included farmers, civil servants, business people, and college students and teachers. Participants were included in the study if they were aged 18 years or older and were able to read and communicate. Those who were currently hospitalized and receiving medical treatment, those who had substantial physiological defects or major diseases that prevented them from engaging in normal daily life; and those with cognitive impairment were excluded from the study. There is no strict rule of sample size requirement for psychometric testing, and the past literature recommends a minimal sample size ranging from 3 to 20 times the number of items and absolute ranges from 100 to over 1000.23 In the current study, the N of 266 satisfies the minimal sample size requirement by these recommendations to conduct a factor analysis.23 The study was approved by the Ethics Committee of Xiangya School of Nursing, Central South University (No.2018028). Eligible participants were identified and recruited from the three research sites by our investigators of college students. After providing written informed consent, each participant was invited to complete a questionnaire by face-to-face interview with our investigators in a quiet room at the research site. The answers were checked by a quality control person to ensure that there were no inconsistencies or missing items.
Measurements
Social Support for Physical Activity
The 6-item Simplified Chinese version of Social Support for Physical Activity (SSSPH-SC) was used to evaluate social support for physical activity in two domains: family support (items 1, 2 and 3), and friend support (items 4, 5 and 6). The items of the SSSPH-SC were as follows: “My family/friends offered to exercise with me”, “My family/friends exercised with me”, and “My family/friends gave me encouragement to stick with my exercise program”. Each item is rated on a 5-point scale from 1 (none) to 5 (very often). The total score ranges from 6 to 30, with a higher score indicating a higher level of social support for physical activity.
Social Support
The 10-item Social Support Rating Scale (SSRS) was used to assess general social support among the Chinese population in three domains: subjective support (3 items), objective support (4 items), and support-seeking behavior (3 items).24 The total score ranges from 12 to 66, with a higher score indicating better perceived social support. The scale was originally developed in Chinese and has been widely used in Chinese populations with good validity and reliability.24,25 In the current study, the SSRS showed good internal consistency, with a Cronbach’s alpha of 0.69.
Quality of Life
The World Health Organization Quality of Life-brief version (WHOQOL-BREF) was used to assess the quality of life in various domains.26 It contains 26 questions with the first 2 questions asking about the overall quality of life and overall perception of their own health status. The next 24 questions ask about individuals’ perceived health in 4 domains: physical health (7 items), psychological health (6 items), social relationships (3 items), and environment (8 items). Each item is rated on a 5-point scale ranging from 1 = “low, negative perception” to 5 = “high, positive perception”. The total score ranges from 26 to 130, with a higher score indicating better quality of life. In the current study, the WHOQOL-BREF demonstrated good internal consistency, with a Cronbach’s α coefficient of 0.89.
Self-Rated General Health
One self-designed question was used to assess the self-rated general health by the following question: “How do you rate your general health status”. The optional answers ranged from 1 “very poor” to 5 “very bad”, with a higher score indicating better self-rated general health.
Statistical Analyses
Sample characteristics were examined using descriptive statistics including mean and standard deviation for continuous variables and frequencies and percentages for categorical variables. Internal consistency was tested by calculating Cronbach’s α, with a recommended level of 0.70 or above indicating good internal consistency based on the criterion by Nunnally.27 Factorial validity was evaluated by confirmatory factor analysis (CFA). In CFA, model fit was assessed using a combination of fit indices including relative Chi-square (χ2/df), comparative fit index (CFI), Tucker–Lewis Index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). Relative chi-square is the ratio of chi-square to degrees of freedom, with a recommended level of <3 for acceptable model fit.28 Values for CFI and TLI range between 0 and 1, with values closer to 1 or >0.90 indicative of data fitness.29 An RMSEA ranging from 0.08 to 0.10 shows a moderate fit and below 0.08 indicates a good fit.30,31 The acceptable value for SRMR is <0.10, with values <0.08 indicating adequate fit, and values below 0.05 indicating good fit.30,31 Concurrent validity of the SSSPH-SC was tested using Pearson’s Correlations with expected significant positive correlations with general social support, quality of life, and self-rated general health based on past studies showing positive associations between them.13–15 All data were analyzed using STATA version 16. Values of p less than 0.05 were considered statistically significant (two-tailed test).
Results
Sample Characteristics
Table 1 shows the socio-demographic characteristics of the sample. The participants had a mean age of 37.54 years (SD = 15.39, range = 21–76), with the largest proportion lying in the 18–29 age group (43.98%). Most were female (69.92%) and approximately half were married (50.75%). Nearly sixty percent of the participants were employed (58.27%) and had an educational level of college and above (57.52%). For family income, the largest proportion was in the 3001–4500 yuan/month group (28.57%), followed by the >6000 yuan/month group (22.56%).
 |
Table 1 Socio-Demographic Characteristics of the Sample |
Internal Consistency Reliability
Cronbach’s alpha coefficient was 0.82 for the total score of the SSSPH-SC, 0.80 for the subscale of family support, and 0.84 for the subscale of friend support. All these results indicate good internal consistency reliability.
Factorial Validity
A CFA was conducted to test the a priori two-factor structure of the SSSPH-SC and compare it with a single-factor model. Table 2 shows a comparison of the model fit indices between the two-factor structure and single-factor structure of the SSSPH-SC. The results generally supported the a priori specified two-factor structure, and the goodness-of-fit indices of the two-factor model were better than the single-factor structural model. For the two-factor model, the relative Chi-squares (χ2/df=2.45) were lower than 3, indicating the fitness of the model;32 the values of CFI (0.98) and TLI (0.97) were close to 1, also showing goodness-of-fit for the data;29 an RMSEA value of lower than 0.08 (0.074) and an SRMR value of lower than 0.04 (0.033) further supported a good fit.30,31 For the single-factor model, only the SRMR met the criteria. In sum, all the fit indices revealed a good model fit for the two-factor SSSPH-SC.
 |
Table 2 Comparison of Model Fit Statistics of Single-Factor Model and Two-Factor Model of the SSSPH-SC by Confirmatory Factor Analysis# |
Table 3 displays the means, standard deviations, and factor loadings of all 6 items by the CFA. All items loaded well in their respective domains, with factoring loading ranging from 0.71 to 0.83 for the subscale of family support, and 0.74–0.87 for the subscale of friend support. The correlation of 0.60 between the two subscales of family support and friend support indicated a large effect size.
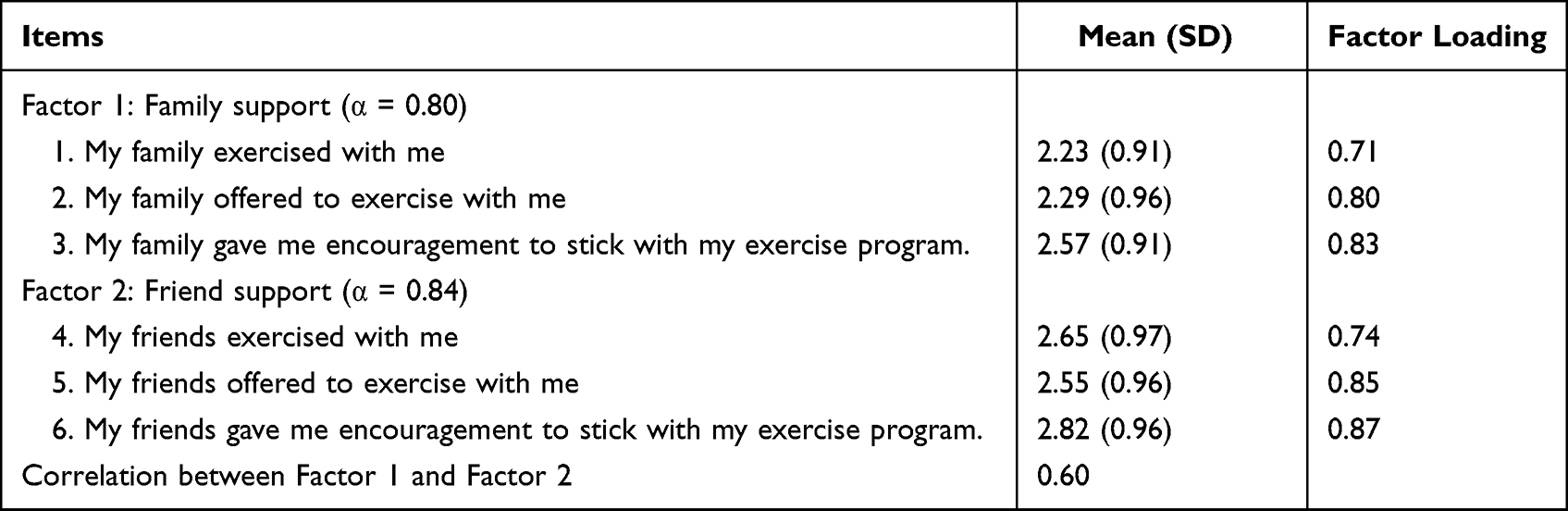 |
Table 3 Descriptive Statistics and Factor Loadings of All 6 Items of the SSSPH-SC by Confirmatory Factor Analysis |
Concurrent Validity
Drawing on the existing literature, social support in physical activity was positively associated with general social support, quality of life, and self-rated health. The correlations between the SSSPH-SC and SSRS, WHOQOL-BREF, and one item self-rated general health were calculated to determine the concurrent validity. As shown in Table 4, the total scale of SSSPH-SC and its two subscales were all positively and significantly related to general social support (r ranging from 0.20 to 0.26, p<0.001), quality of life (r ranging from 0.16 to 0.26, p<0.05), and self-rated health (r=0.13–0.25, p<0.05). All these results further corroborated the concurrent validity of the SSSPH-SC.
 |
Table 4 Correlations of SCESS-6 and Its Two Subscales with Other Variables |
Discussion
The current study is the first to simplify the 20-item SSSPA into a 6-item SSSPA-S by retrieving 3 similar items from each of the original two domains: family support and friend support; translate it into a Chinese version of SSSPA-S (SSSPA-SC) using forward translation, back translation, and content validation; and test its psychometric performance among a diverse sample of Chinese general population. We tested internal consistency reliability, factorial validity, and concurrent validity, and our findings showed that the SSSPA-SC full scale and subscales were psychometrically sound. Overall, the SSSPA-SC showed good internal consistency, and the confirmatory factor analysis supported the a priori two-factor structure with favorable factor loadings and model fit indices. Concurrent validity was also supported by its significant positive correlations with genera social support, quality of life, and self-rated general health. Thus, the SSSPA-SC demonstrated psychometrically sound properties for assessing social support for physical activity among the general Chinese population. Compared with the original 20-item SSSPA, the 6-item SSSPA-SC demonstrates unique advantages due to its ease of administration, minimization of respondent burden, and quick screening ability on busy occasions with an average completion time of 3 minutes. Introducing this scale into mainland China could ensure the standardized evaluation of social support for physical activity as well as a guide for further intervention program evaluation.
Cronbach’s alpha coefficients for the total scale and its two subscales exceeded 0.80, indicating high internal consistency reliability of the SSSPA-SC. This finding is consistent with previous validation studies of the non-Chinese version showing Cronbach’s alphas ranging from 0.61 to 0.91 for the full SSSPA scale and two subscales in other populations. Although Cronbach’s alpha coefficients are sensitive to the number of items and may decrease with reduced items.33 We observed generally comparable Cronbach’s alpha coefficients in the 6-item SSSPA-SC as in the full 20-item SSSPA, further demonstrating the item homogeneity and internal consistency of the selected 6 items from the original SSSPA. This result also justifies our original simplification of the full SSSPA by removing items that exist in the friend subscale but not in the family subscale. As some studies have shown that friend support plays an even more, if not equally important role in promoting physical activity than family support.34 Also, in the validation of the original SSSPA by Sallis,16 the subfactor of “rewards and punishment” that exists in the family subscale but not the friend subscale shows relatively low internal consistency with a Cronbach’s alpha coefficient of 0.61, compared to the 0.84 for the “exercising together” in the friend subscale and 0.91 for the “participation and involvement” in the family subscale. In general, the internal consistency of the SSSPA-SC in the current study demonstrates the appropriateness of the item simplification and the reliability of the scale.
The confirmatory factor analysis confirmed the a priori two-factor structure of the SSSPA-SC: family support (items 1, 2 and 3) and friend support (items 4, 5 and 6) with generally good model fit indices. This finding resonates with the original factor analysis of the SSSPA scale that includes the two conceptually-distinguishable domains and shows the robustness of the factor structure of the SSSPA-SC even with shorter item numbers.16 It also aligns the bulk of past literature showing the importance of different sources of social support such as family, friends, and coworkers in providing different types of support in promoting physical activity such that it is necessary to distinguish between these sources.35–38 In general, the two-factor structure of the SSSPA-SC is in accordance with our theoretical hypothesis that social support for physical activity covers the two most important sources: family and friends.
Concurrent validity of the SSSPA-SC was demonstrated by its significant positive correlations with general social support, quality of life, and self-rated general health. In Sallis’ original validation study, no significant correlation was found between social support for physical activity and general social support.16 However, our study showed a small to a medium positive association between SSSPA-SC and SSRS, indicating that social support for physical activity belongs to general social support but carries unique characteristics that distinguish itself from the general social support. While the general social support scale mostly focuses on the assessment of general emotional items that buffer life stress (eg, who can you count on when you are upset?), social support for physical activity is more targeted at specific activities (eg, my family exercised with me). This finding further justifies that it is both necessary and important to measure social support for a specific activity such as physical activity using a specific social support scale instead of the general social support scale. The positive associations between social support for physical activity with the quality of life and self-rated general health were consistent with the extensive literature showing the positive effect of social support in enhancing the quality of life and promoting well-being.13–15 Individuals with a higher level of social support also enjoy a better quality of life and are more satisfied with their general health. In general, all these results corroborate the concurrent validity of the SSSPA-SC.
Several limitations need to be noted when interpreting the study results. First, our study sample was recruited from healthy adults in Hunan Province of China and may not represent other populations, such as people with chronic conditions, or people from other areas of China. Future research may consider validating the SSSPA-SC in other populations and in other areas. Second, a re-test has not been done on this sample, so the test-retest reliability of the SSSPA-SC cannot be evaluated. Future validation studies should add a re-test on a selected large sample to get a robust test-retest reliability. Third, the cross-sectional descriptive design makes it more difficult to test sensitivity to change in the SSSPA-SC. Future research should fill in this gap by conducting longitudinal studies to see whether SSSPA-SC is sufficiently sensitive to reflect changes after interventions and over time. Fourth, we did not assess participants’ physical activities, which may be an essential indicator to examine concurrent validity, future studies should consider collecting these data such as time and frequency of physical activities for concurrent validity. Fifth, in order to get a short and easy-to-administer SSSPH short form with the equal item and weight between its two subscales, the original 20-item SSSPH was simplified by removing 10 additional items that only exist in the family subscale but not in the friend subscale, which might cause some information loss and lead to potential bias. Future studies in modifying the SSSPH may consider adding similar items in the friend subscale from the family subscale to get more comprehensive information.
Despite these limitations, our study still provides important clinical and research implications. The 6-item SSSPA-SC provides a short, effective, and reliable tool that can be used to screen social support for physical activity in the general population in China. The scale can be used as an effective screening tool as well as an evaluation tool to understand people’s physical activity-related social support so as to guide targeted physical activity promotion interventions.
Conclusion
This is the first study to simplify Sallis’ 20-item social support scale for physical activity (SSSPA) into a 6-item short form, translate it into Chinese, and further validate it for a Chinese population. Our results confirmed the internal consistency, factorial validity, and concurrent validity of the 6-item SSSPA short form (SSSPA-SC) among the general population in China. The SSSPA-SC may be useful as a reliable and valid self-report measure of social support for physical activity. The validation of SSSPA-SC enables its usage as an alternative for the full SSSPA as a rapid assessment tool in busy clinical and research settings.
Abbreviations
CFI, comparative fit index; CVI, content validity index; EFA, exploratory factor analysis; CFA, confirmatory factor analysis; I-CVI, content validity index for item; RMSEA, root mean square error of approximation; S-CVI, CVI for scale for scale; SRMR, standardized root mean square residual; SSRS, Social Support Rating Scale; SSSPA, social support scale for physical activity; SSSPH-S, short version of the social support scale for physical activity; SSSPH-SC, simplified Chinese version of the social support scale for physical activity; TLI, Tucker–Lewis Index; WHOQOL-BREF, World Health Organization Quality of Life-brief version.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to data protection from the organization but are available from the corresponding author on reasonable request.
Ethical Approval and Informed Consent
Ethical approval was obtained from the Ethics Committee of Xiangya School of Nursing, Central South University (No.2018028). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from all individual participants included in the study.
Acknowledgments
The authors would like to thank all the participants we interviewed during the study for openly sharing their feelings and experiences.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Huxiang Youth Talent of Technology and Research Award (No.: 2019RS2006).
Disclosure
The authors have no relevant financial or non-financial interests to disclose in this work.
References
1. Polero P, Rebollo-Seco C, Adsuar JC, et al. Physical activity recommendations during COVID-19: narrative review. Int J Environ Res Public Health. 2021;18(1):65. doi:10.3390/ijerph18010065
2. Krupchanka D, Kruk N, Sartorius N, Davey S, Winkler P, Murray J. Experience of stigma in the public life of relatives of people diagnosed with schizophrenia in the Republic of Belarus. Soc Psychiatry Psychiatr Epidemiol. 2017;52(4):493–501. doi:10.1007/s00127-017-1365-1
3. Anderson ES, Wojcik JR, Winett RA, Williams DM. Social-cognitive determinants of physical activity: the influence of social support, self-efficacy, outcome expectations, and self-regulation among participants in a church-based health promotion study. Health Psychol. 2006;25(4):510–520. doi:10.1037/0278-6133.25.4.510
4. Glozah FN, Pevalin DJ. Perceived social support and parental education as determinants of adolescents’ physical activity and eating behaviour: a cross-sectional survey. Int J Adolesc Med Health. 2015;27(3):253–259. doi:10.1515/ijamh-2014-0019
5. Glanz KLF, Rimer BK, editors. Health Behavior and Health Education: Theory, Research, and Practice.
6. Zimmer C, McDonough MH. Social support and physical activity in older adults: identifying predictors using data from the Canadian longitudinal study on aging. J Aging Phys Act. 2021;4:1–12.
7. Mendonca G, Cheng LA, Melo EN. Physical activity and social support in adolescents: a systematic review. Health Educ Res. 2014;29(5):822–839. doi:10.1093/her/cyu017
8. Van Luchene P, Delens C. The influence of social support specific to physical activity on physical activity among college and university students: a systematic review. J Phys Act Health. 2021;18(6):737–747. doi:10.1123/jpah.2020-0713
9. Lindsay Smith G, Banting L, Eime R, O’Sullivan G, van Uffelen JGZ. The association between social support and physical activity in older adults: a systematic review. Int J Behav Nutr Phys Act. 2017;14(1):56. doi:10.1186/s12966-017-0509-8
10. Mabweazara SZ, Ley C, Leach LL. Physical activity, social support and socio-economic status amongst persons living with HIV and AIDS: a review. Afr J AIDS Res. 2018;17(2):203–212. doi:10.2989/16085906.2018.1475400
11. Quirk H, Crank H, Harrop D, Hock E, Copeland R. Understanding the experience of initiating community-based physical activity and social support by people with serious mental illness: a systematic review using a meta-ethnographic approach. Syst Rev. 2017;6(1):214. doi:10.1186/s13643-017-0596-2
12. McDonough MH, Beselt LJ, Kronlund LJ, et al. Social support and physical activity for cancer survivors: a qualitative review and meta-study. J Cancer Surviv. 2021;15(5):713–728. doi:10.1007/s11764-020-00963-y
13. Snowden MB, Steinman LE, Carlson WL, et al. Effect of physical activity, social support, and skills training on late-life emotional health: a systematic literature review and implications for public health research. Front Public Health. 2014;2:213. doi:10.3389/fpubh.2014.00213
14. Kruithof WJ, van Mierlo ML, Visser-Meily JM, van Heugten CM, Post MW. Associations between social support and stroke survivors’ health-related quality of life–a systematic review. Patient Educ Couns. 2013;93(2):169–176. doi:10.1016/j.pec.2013.06.003
15. Tajvar M, Fletcher A, Grundy E, Arab M. Social support and health of older people in Middle Eastern countries: a systematic review. Australas J Ageing. 2013;32(2):71–78. doi:10.1111/j.1741-6612.2012.00639.x
16. Sallis JF, Grossman RM, Pinski RB, Patterson TL, Nader PR. The development of scales to measure social support for diet and exercise behaviors. Prev Med. 1987;16(6):825–836. doi:10.1016/0091-7435(87)90022-3
17. Treiber FA, Baranowski T, Braden DS, Strong WB, Levy M, Knox W. Social support for exercise: relationship to physical activity in young adults. Prev Med. 1991;20(6):737–750. doi:10.1016/0091-7435(91)90068-F
18. Noroozi A, Ghofranipour F, Heydarnia AR, Nabipour I, Shokravi,FA. Validity and reliability of the social support scale for exercise behavior in diabetic women. Asia Pac J Public Health. 2011;23(5):730–741. doi:10.1177/1010539509357342
19. Reis MS, Reis RS, Hallal PC. Validity and reliability of a physical activity social support assessment scale. Rev Saude Publica. 2011;45(2):294–301. doi:10.1590/S0034-89102011000200008
20. Morgado FFR, Meireles JFF, Neves CM, et al. Scale development: ten main limitations and recommendations to improve future research practices. Psicol Refl Crít. 2018;30(3):1–20.
21. Brislin RW. The wording and translation of research instruments. In: Lonner WL, Berry JW, editors. Field Methods in Cross-Cultural Research. Newbury Park, CA: Sage Publications; 1986:137–164.
22. Yusoff MSB. ABC of content validation and content validity index calculation. Edu Med J. 2019;11(2):49–54. doi:10.21315/eimj2019.11.2.6
23. Mundfrom DJ, Shaw DG, Ke TL. Minimum sample size recommendations for conducting factor analyses. Int J Testing. 2005;5(2):159–168. doi:10.1207/s15327574ijt0502_4
24. Xiao S. The theoretical basis and applications of Social Support Rating Scale (SSRS). (in Chinese). J Clinical Psychiatry. 1994;02:98–100.
25. Wang XD, Ma H. Rating scales for mental health: social support rating scale. J Chin Psychol Press, China, Beijing. 1999;4:56.
26. The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med. 1998;28(3):551–558. doi:10.1017/S0033291798006667
27. Nunnally JC. Psychometric Theory.
28. Nunnally JC. Psychometric Theory.
29. Kline RB. Principles and Practice of Structural Equation Modeling.
30. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. 1999;6(1):1–55. doi:10.1080/10705519909540118
31. Bollen KA, Long JS. Testing Structural Equation Models. Thousand Oaks, CA: Sage Publications; 1993.
32. Munro BH, Duffy ME, Brancato V, Newton S, Talbot L. Statistical Methods for Health Care Research.
33. Sijtsma K. On the use, the misuse, and the very limited usefulness of cronbach’s alpha. Psychometrika. 2009;74(1):107–120. doi:10.1007/s11336-008-9101-0
34. Reimers AK, Jekauc D, Mess F, Mewes N, Woll A. Validity and reliability of a self-report instrument to assess social support and physical environmental correlates of physical activity in adolescents. BMC Public Health. 2012;12:705. doi:10.1186/1471-2458-12-705
35. Yusuf RA, Mont DF, Lin WH, Chen HJ. Adolescents’ physical activity and the association with perceived social support of parents and peers in Indonesia. Asia Pac J Public Health. 2021;33(4):388–395. doi:10.1177/1010539521997255
36. Sarkar S, Taylor WC, Lai D, Shegog R, Paxton RJ. Social support for physical activity: comparison of family, friends, and coworkers. Work. 2016;55(4):893–899. doi:10.3233/WOR-162459
37. Prado CV, Lima AV, Fermino RC, Anez CR, Reis RS. Apoio social e prática de atividade física em adolescentes da rede pública de ensino: qual a importância da família e dos amigos? [Social support and physical activity in adolescents from public schools: the importance of family and friends]. Cad Saude Publica. 2014;30(4):827–838. Portuguese. doi:10.1590/0102-311X00014313
38. Duncan SC, Duncan TE, Strycker LA. Sources and types of social support in youth physical activity. Health Psychol. 2005;24(1):3–10. doi:10.1037/0278-6133.24.1.3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Validation of the Connor-Davidson Resilience Scale-10 in South Africa: Item Response Theory and Classical Test Theory
Pretorius TB, Padmanabhanunni A
Psychology Research and Behavior Management 2022, 15:1235-1245
Published Date: 16 May 2022
Validity and Reliability of the Thai Version of the 19-Item Compliance-Questionnaire-Rheumatology
Panichaporn S, Chanapai W, Srisomnuek A, Thaweeratthakul P, Katchamart W
Patient Preference and Adherence 2022, 16:2149-2158
Published Date: 17 August 2022
Psychometric Properties of the Montreal Cognitive Assessment (MoCA) to Detect Major Neurocognitive Disorder Among Older People in Ethiopia: A Validation Study
Daniel B, Agenagnew L, Workicho A, Abera M
Neuropsychiatric Disease and Treatment 2022, 18:1789-1798
Published Date: 22 August 2022
Validation of the Spanish Activity Questionnaire in COPD (SAQ-COPD) in Patients with Chronic Obstructive Pulmonary Disease
Soler-Cataluña JJ, Puente Maestu L, Román Rodríguez M, Esteban C, Gea J, Bernabeu Mora R, Pleguezuelos Cobo E, Ancochea J, García-Río F
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2835-2846
Published Date: 5 November 2022
Research and Evaluation of a Cyberchondria Severity Scale in a Chinese Context
Wang D, Sun L, Shao Y, Zhang X, Maguire P, Hu Y
Psychology Research and Behavior Management 2023, 16:4417-4429
Published Date: 1 November 2023