")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Childhood Asthma and Parental Antidepressant Use in a Nationwide Danish Cohort
Authors Cabrera Guerrero S, Håkansson KEJ , Backer V , Ulrik CS , Rastogi D
Received 1 June 2023
Accepted for publication 3 August 2023
Published 8 August 2023 Volume 2023:16 Pages 821—831
DOI https://doi.org/10.2147/JAA.S421169
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Silvia Cabrera Guerrero,1,* Kjell Erik Julius Håkansson,2,* Vibeke Backer,3 Charlotte Suppli Ulrik,1,4 Deepa Rastogi1,5
1Division of Pulmonary and Sleep Medicine, Children’s National Health System, Washington, DC, USA; 2Department of Respiratory Medicine, Copenhagen University Hospital - Hvidovre, Hvidovre, Denmark; 3Department of Otorhinolaryngology, Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark; 4Institute of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark; 5Pediatrics, Genomics and Precision Medicine, George Washington University School of Medicine and Health Sciences, Washington, DC, USA
*These authors contributed equally to this work
Correspondence: Kjell Erik Julius Håkansson, Respiratory Research Unit, Department of Respiratory Medicine, Copenhagen University Hospital – Hvidovre, Hvidovre, 2650, Denmark, Email [email protected]
Background: Paediatric asthma is associated with caregiver depression, which in turn is associated with poor asthma control. Although sociodemographic risk factors are associated with parental depression among children with asthma, the contribution of these factors to caregiver depression in free-to-access universal healthcare settings is unknown.
Methods: The association between childhood asthma and parental antidepressant use was investigated in a Danish nationwide cohort of children aged 2– 17 years that redeemed inhaled corticosteroids in 2015. The odds of antidepressant use were estimated in comparison to control families that were matched 1:1 on the number of siblings, residence, income, and education.
Results: Among the families of 28,595 children with actively treated asthma, 12% of mothers and 6.2% of fathers were on antidepressant therapy, compared to 9.3% and 5.3% in controls (p< 0.001). Paediatric asthma was associated with increased odds of parental antidepressant use (OR 1.29 (1.23– 1.35)), even after adjusting for parental asthma. Poor asthma control, but not higher asthma severity, was associated with higher odds of antidepressant use (1.43 (1.31– 1.56)). Compared with the controls, families with two or more children with asthma had higher OR (1.42 (1.29– 1.56)) than those with a single child (OR 1.27 (1.21– 1.34)). Low socioeconomic status was associated with parental antidepressant use.
Conclusion: Caregiver depression in a Danish cohort is more prevalent among mothers than among fathers and is associated with poor asthma control in children. Antidepressant use among caregivers was associated with total family asthma burden and was independent of socioeconomic status.
Keywords: pediatric asthma, mental health, quality of life, pharmacoepidemiology
Introduction
Asthma is the most common chronic illness among children.1 Caregivers are responsible for symptom monitoring and medication administration,2 which places a significant physical and emotional burden, and adversely affects caregivers’ mental health.3 Caregivers of children with asthma experience higher rates of depression and anxiety, and the prevalence correlates with offspring’s asthma severity.4 However, the association between parental mental health and childhood asthma burden, including severity, exacerbation burden, comorbidities, or multiple offspring with asthma, remains poorly understood.
Conversely, families’ mental health impacts family dynamics and child well-being.5 Maternal depressive symptoms are inversely correlated with asthma control, school attendance,6 asthma knowledge, and medication adherence7 among under-resourced populations. Furthermore, caregiver depression and inadequate emotional environment contribute to offspring depression,8 which has been implicated in paediatric asthma morbidity9 and mortality.10
Most studies on parental depression and childhood asthma have focused on the mothers of the affected children.11,12 Treatment of maternal depression leads to improved asthma management and reduced asthma costs.13 Fathers of children with asthma usually comprise less than 10% of the caregiver sample in studies that investigated caregiver mental illness,14 and the effect of paternal depression management on offspring asthma control is not known.
Mental health problems among parents of children with asthma have been associated with lower family socioeconomic status (SES) family. Low SES is a social determinant of health and is independently associated with a higher disease burden.15 However, the extent to which lower SES and parental mental health independently contribute to children’s asthma burden, particularly in universal healthcare systems, has not yet been well elucidated. In the present study, we investigated the association between caregiver depression and childhood asthma, and the contribution of SES in a Danish cohort comprising of children with actively treated asthma.
Methods
Study Cohort
Children aged 2–17 years with actively treated asthma, defined as the redemption of ≥2 canisters of ICS during 2015, were enrolled in the REASSESS Youth cohort, a nationwide Danish paediatric asthma cohort with data provided by Statistics Denmark, the Danish National Prescription Database and the National Patient Registry as previously described.16 Families with children with actively treated asthma were matched 1:1 by Statistics Denmark to control families based on the number of siblings, size of the city of residence, families’ disposable income, families’ highest education level, and the mother’s age. All matches were unique. Data was collected from the date of the first ICS redemption (“index date”) in 2015 for a prospective period of 730 days.
Study approval was granted by the Capital Region of Copenhagen’s Data Safety Board (ref. P-2021-602). As per Danish law, access to patient journals does not require informed consent if granted by the Capital Region of Copenhagen’s Data Safety Board. According to Danish law, access to patient journals does not require informed consent, if granted by the Capital Region of Copenhagen’s Data Safety Board. This study was conducted in accordance with the principles of the Declaration of Helsinki. All data and supporting materials are available through Statistics Denmark upon application; however, approval from data sources may be required as per Danish law.
Caregivers were defined as the adult(s) residing with a case child on the index date. A family was defined as co-residing adults, biological and non-biological siblings, and the case child. Biological parents were defined as the individuals registered in birth records as biological mothers or fathers. Children without known caregivers, those with less than 365 days of ICS treatment data, and those belonging to families without a suitable match were excluded (Figure 1).
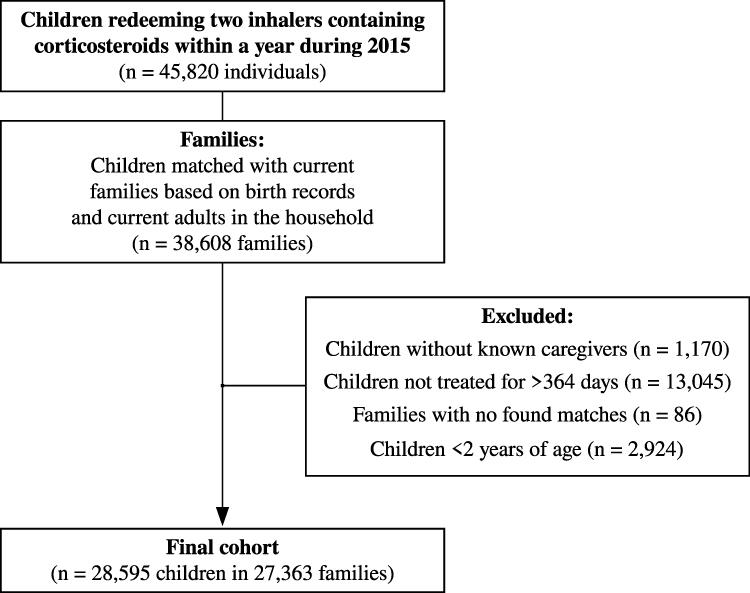 |
Figure 1 Flowchart of study inclusion and exclusion criteria in a nationwide cohort of childhood asthma. |
Asthma Definitions and Classifications
Based on medication redemption in 730 prospective days from the index date, the GINA 2020 Treatment Steps were used to classify the asthma severity for each child.17 ICS treatment was calculated as the average daily dose (calculated as beclomethasone standard particle dose equivalents) during the observation period as previously described18 and stratified according to the age-appropriate GINA 2020 dosing chart.17
Possible severe asthma was defined based on GINA 2020 Step 3 or 4 with either two moderate or one severe or near-fatal exacerbation for individuals aged 2–11 years, and GINA Step 4 with exacerbation frequency as detailed above, or GINA Step 5 regardless of exacerbations for individuals aged 12+ years.
Disease control was defined based on short-acting β2-agonist (SABA) use quantified by annualised redeemed doses during the observation period. Excessive SABA use was defined as twice the acceptable control criteria for children aged 2–11 years (2 daily puffs at least two days a week, totalling 400 annual doses) or 600 (ages 12+)) annual redeemed doses of SABA.17,19
Exacerbations were defined as moderate when they were associated with the redemption of at least 37.5 mg of prednisolone for 5 days, severe when associated with hospitalisation (ICD-10 codes DJ45, DJ46, DJ96, DJ960 or DJ969), and near-fatal exacerbations when hospitalisation was to an intensive care unit with or without supplemental ventilation. Re-exacerbations within ± 14 days were considered treatment failures and were not counted as an additional exacerbation.
Socioeconomic Definitions
The variables used to define SES include family workforce attachment defined as the highest SES at the index date, ranked in the following order: Employed (or self-employed), Currently undergoing education, Transfer income recipient (Main source of income stemming from welfare transfers) and Retiree or Unclassifiable. Additional socioeconomic variables included family residence classified based on the number of inhabitants in the municipality of residence at the index date and family disposable income adjusted for the number of cohabiting individuals to correct for the economics of scale,20 family highest attained education level ranked as higher education (Bachelor’s degree or higher), vocational education (at least two years of vocational studies in addition to mandatory schooling) or basic education (ca. 12 years of mandatory schooling).
Antidepressant Use and Comorbidity Definitions
Parental antidepressant use was defined based on the redemption of >1 prescription belonging to the N06A ATC-code group after the birth of the child.
Comorbidities were included as covariates and were defined as the non-respiratory Charlson score, with updated weights by Quan et al,21 used either as the total household score, or individual (maternal/paternal) scores depending on the outcome.
Statistical Analyses
Descriptive statistics on demographic variables are presented as median (interquartile range, IQR). Wilcoxon rank-sum test or χ2 -test was used depending on continuous or categorical data for groupwise comparisons.
Logistic multivariate regression was used to investigate the impact of childhood asthma (yes/no; none/mild-to-moderate/possible severe), childhood asthma control (controlled/uncontrolled; exacerbating/non-exacerbating) and total family childhood asthma burden (one/multiple children with asthma) on the odds of caregiver antidepressant use. Analyses were adjusted for child age, family disposable income quartile, highest attained family education level, city of residence size, family workforce attachment and comorbidity (Charlson score).
R 4.1.3 (The R Foundation, AU) was used for statistical analyses and Ggplot2 was used for creating figures.
Results
We identified 38,608 families for the 45,820 children with actively treated asthma in 2015. After excluding children below 2 years of age, those without known caregivers, those with episodic ICS treatment, and those without found matches, the final cohort comprised 28,595 children and their families (Figure 1). The median age of the children was 8 years, and 59% of the children were boys. The 28,595 children and their families were 1:1 matched with control families with children without asthma, such that the case and control families did not differ in median child age, maternal and paternal age, number of siblings, or socioeconomic variables (Table 1 and Table 2). Within the cases, the prevalence of uncontrolled asthma was 16% and 4.8% of children had possible severe asthma. In terms of exacerbations, 7.8% of children experienced at least one asthma exacerbation, either moderate or severe (Table 1).
 |
Table 1 Demographics Characteristics of the Children with Actively Treated Asthma, of Their Families, and of the Control Families in a Nationwide Danish Cohort |
 |
Table 2 Socioeconomic Characteristics of Families with Children with Actively Treated Asthma and of Control Families |
Prevalence of Caregiver Depression
The overall prevalence of caregiver antidepressant use was higher among case families as compared to controls (17% versus 14%, respectively). Maternal antidepressant use was seen in 12% of case families as compared to 9.3% of the control families (p<0.001). Paternal antidepressant use was also higher in case (6.2%) compared to control families (5.3%, p<0.001), although the difference was smaller than that observed in the mothers (Table 1).
Determinants of Caregiver Depression
Odds of caregiver antidepressant use were higher in the case families compared to controls (OR 1.29 (1.23–1.35)), with slightly higher odds among mothers than fathers. There were higher odds of caregiver antidepressant use among cases with uncontrolled asthma compared to controlled asthma (OR 1.43 (1.31–1.56) vs 1.26 (1.20–1.33)).
After adjusting for family asthma burden, defined as either parental asthma or additional children with asthma, the odds of caregiver depression in case families remained increased compared to controls, with trends towards lower odds among those with parental asthma and higher odds of antidepressant use among those with more than one child with asthma. Intriguingly, the odds of caregiver antidepressant use were higher among families with children who had had no exacerbations compared to children who experienced at least one exacerbation during the study period. There was no significant association between caregiver antidepressant use and asthma severity (Figure 2).
 |
Figure 2 Odds for antidepressant use in families of children with actively treated asthma and 1:1 matched control families. Analyses adjusted for matching variables, children’s age, and family non-respiratory Charlson score. |
Positive predictors of caregiver antidepressant use among families with children with actively treated asthma included welfare recipiency, residence outside of the capital region and higher Charlson scores. Conversely, higher parental education level and higher disposable income were protective factors against the use of antidepressants among caregivers. (Table 3 and Figure 2).
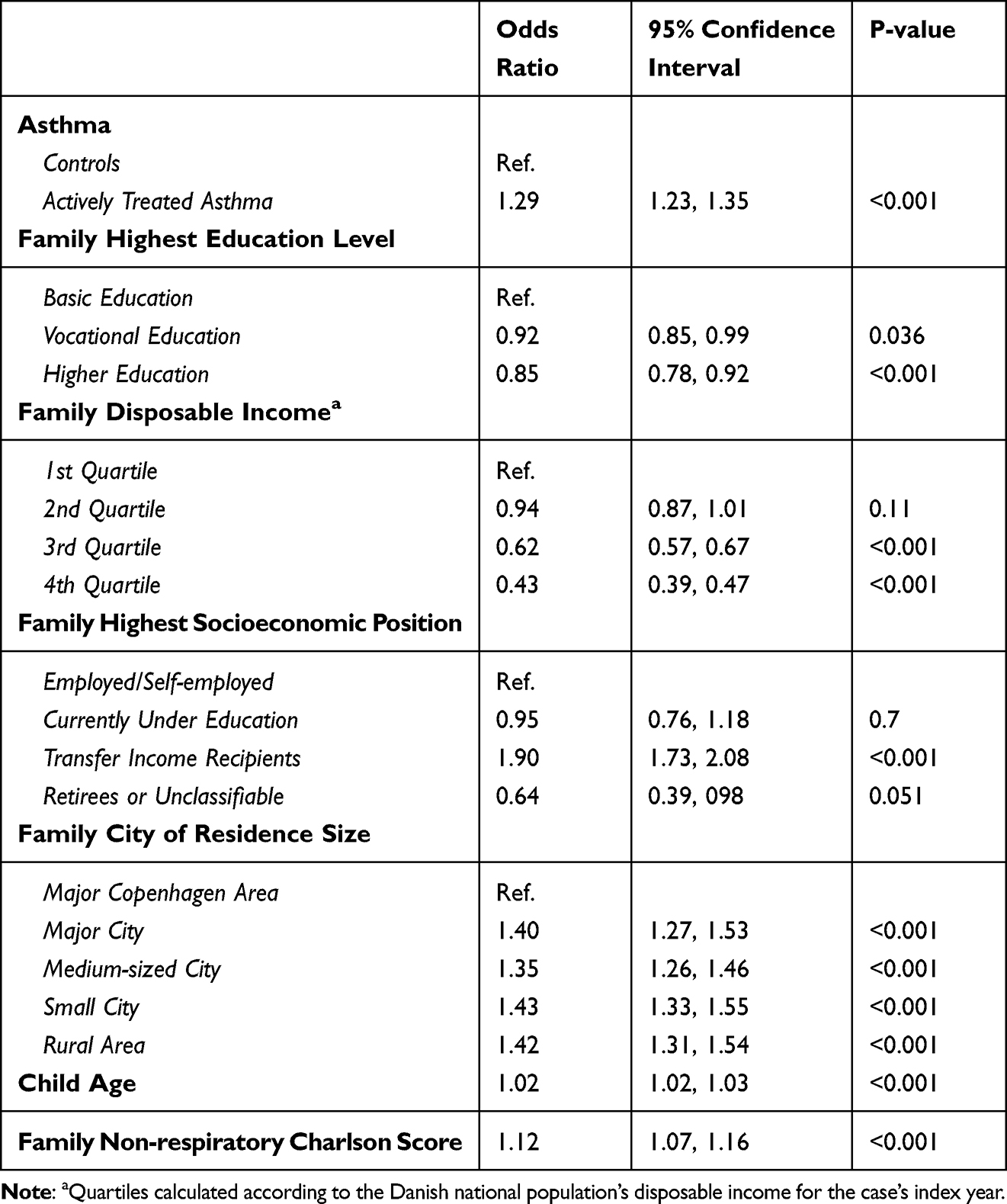 |
Table 3 Predictors of Caregiver Antidepressant Use in Families of Children with Actively Treated Asthma Compared to Control Families |
Association Between Caregiver Depression and Childhood Asthma Outcomes
The odds for adverse childhood asthma outcomes dependent on the caregiver's use of antidepressants was investigated after adjusting for socioeconomic covariates (Figure 3). The odds of poor asthma control were higher among families with caregiver antidepressant use. The odds of possible severe asthma were lower in families with caregiver antidepressant use. No significant association between asthma exacerbations and antidepressant use was observed. Additionally, we found that caregiver antidepressant use was not associated with their child’s ongoing ICS doses (Table 4).
 |
Table 4 The Distribution of Parental Antidepressant Use Based on Inhaled Corticosteroid Dosing of Children with Actively Treated Asthma |
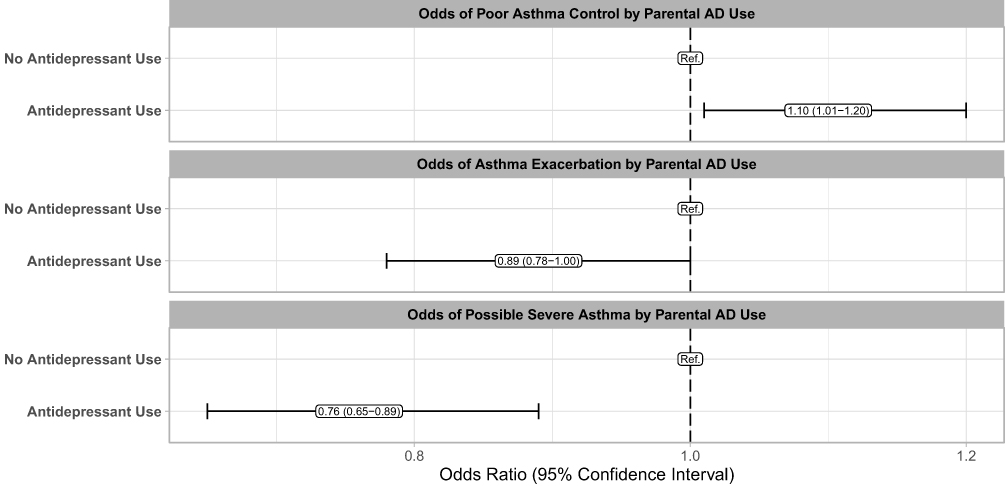 |
Figure 3 Odds for adverse asthma outcomes in children with actively treated asthma with parental antidepressant use. Analyses adjusted for size of city of residence, families’ disposable income, families’ highest education, children’s age, and family non-respiratory Charlson score. |
Discussion
In the present study, we demonstrated that caregiver antidepressant use was higher among families with children actively treated for asthma compared to families with children without known and treated asthma, even after adjusting for socioeconomic factors. The association between caregiver antidepressant use and childhood asthma was stronger in mothers than in fathers. Higher parental education and family income were protective against antidepressant use among caregivers with children with asthma. Although poor asthma control in children was more prevalent among families with caregiver antidepressant use than among non-antidepressant users, there was no association with asthma severity.
Although the link between caregiver depression and childhood asthma has been examined22 to the best of our knowledge, this is the first study to show a positive association between caregiver depression and childhood actively treated asthma, using medication retrieval rather than symptom questionnaires, independent of socioeconomic status in a large nationwide cohort. Our findings are consistent with those of a meta-analysis14 and support a recent nationwide Danish study23 which reported an increased risk of asthma in children whose parents had mental health conditions. In this study, we built on the work of Heuckendorff et al,23 and report not only higher odds of childhood asthma, but also higher odds of poorly controlled asthma among children with caregivers on antidepressant use, independent of SES.
The prevalence of antidepressant use by caregivers in families with children actively treated for asthma was lower than the 25% prevalence reported in a Spanish study.24 A Danish nationwide study estimated a 39% prevalence of caregiver mental health conditions among parents of children, irrespective of their health status.25 These differences are explained by our stringent inclusion of children with continuous ICS use and of active antidepressant use in a system in which antidepressants are not the first-in-line treatment, and lower symptom reporting has been observed among adults in Denmark.26 Irrespective of these differences, our study and prior published data highlight the burden of caregiver depression among children with asthma and identify the necessity of addressing parental needs in the clinical management of childhood asthma, which is likely not addressed during caregivers’ medical visits.
The effects of childhood asthma on caregiver depression are linked to psychosocial influences of life stressors. Caregivers of children with chronic illnesses are exposed to greater stress than caregivers of healthy children.27 Asthma knowledge,28 medication adherence,28 and mitigation of dust mite exposure29 are associated with less parental stress, while Everhart et al30 found that paediatric asthma-related stressors such as asthma severity and SES, had a cumulative negative impact on caregiver quality of life. The age of disease onset is also important since parents of younger children assume more responsibility for asthma management than parents of older children,2 whereas asthma control and knowledge tend to improve with age.31,32 In light of these associations, addressing barriers to parental asthma knowledge could facilitate better paediatric asthma control and improvement in parental mental health.
There is an additive interaction between maternal mental illness and disadvantaged SES on childhood asthma.23 Indeed, Freeman et al33 demonstrated that the risk of depression was inversely correlated with SES in the European adult population. In our study, we found that antidepressant use among caregivers of children with persistent asthma was positively correlated with lower SES.
Our observed association between poor asthma control and caregiver antidepressant use is consistent with the known negative effect of caregiver depression on childhood asthma outcomes34 and on school attendance, with higher absenteeism.6 One possible explanation is the link between depression severity and altered cognitive function including compromised memory, processing speed and executive functioning,35 which could contribute to ineffective asthma management and a higher likelihood of exposing children to potential triggers such as tobacco exposure.36 In fact, depressed caregivers of children with asthma endorsed lower confidence during their interactions with the child’s medical providers and described more unmet needs.37 Notably, a recent study found that caregiver depression remission improved childhood asthma outcomes, which was partially mediated by improvements in the severity of children’s depressive symptoms.38
Limitations
The present study was strengthened by data obtained from nationwide registries providing a powerful statistical analysis, a strict definition of parental depression and a matched control group. However, we acknowledge that there are several limitations to our observational study related to study design and availability of data. First, the inclusion criteria are based on the redemption of ICS and thus exclude SABA-only treated children. Second, using the outcome of antidepressant use, we exclude many individuals with depression who are receiving active antidepressant therapy. Third, the study is limited to two years of annualised data, yet asthma is a variable disease with a burden changing over time. Despite these limitations, we would like to highlight the strengths of the REASSESS Youth cohort, which include a high degree of data completeness, universal linkage between children and parents, and a robust non-biased data capture due to legal requirements to submit data to Statistics Denmark from the various sources used. Our family-based match allowed robust comparisons and is also a strength of the study.
Conclusion
In this nationwide study of 28,595 children with actively treated asthma, we found that caregiver antidepressant use was more prevalent in families with children with asthma than in control families, independent of socioeconomic factors. Parental antidepressant use was associated with poor asthma control in children, even after adjusting for socioeconomic status, signalling that caregiver mental health can have an impact on childhood asthma.
Funding
The present work was funded by Børnelungefonden, Trial Nation Denmark Respiratory, the Respiratory Research Unit, Hvidovre Hospital and SanofiGenzyme. All grants were unrestricted research grants and grantors had no involvement in any aspects pertinent to planning, conducting, analyzing or presenting the present study results.
Disclosure
KEJH has received personal fees from AstraZeneca, Chiesi, GSK, Sanofi and TEVA. DR declares no conflicts of interest but does serve on DSMBs for the National Institute of Health. CSU has received personal fees from AstraZeneca, GSK, TEVA, Chiesi, Sanofi Genzyme, Boehringer-Ingelheim, Orion Pharma, Novartis, ALK-Abello, Mundipharma, Covis Pharma, TFF Pharmaceuticals, Pfizer, Berlin Chemie and Actelion. VB has received personal fees from AstraZeneca, GSK, TEVA, Sanofi Genzyme, MSD, Chiesi, Boehringer-Ingelheim, Novartis, ALK-Abello, Mundipharma and Pharmaxis. The authors report no other conflicts of interest in this work.
References
1. Thomsen SF, Ulrik CS, Larsen K, Backer V. Change in prevalence of asthma in Danish children and adolescents. Anna Allergy Asthma Immunol. 2004;92(5):506–511. doi:10.1016/S1081-1206(10)61757-7
2. McQuaid EL. Medication adherence in pediatric asthma: reasoning, responsibility, and behavior. J Pediatr Psychol. 2003;28(5):323–333. doi:10.1093/jpepsy/jsg022
3. Frankel K, Wamboldt MZ. Chronic childhood illness and maternal mental health--why should we care? J Asthma. 1998;35(8):621–630. doi:10.3109/02770909809048964
4. Leão LL, Zhang L, Sousa PLR, et al. High prevalence of depression amongst mothers of children with asthma. J Asthma. 2009;46(4):388–391. doi:10.1080/02770900802444237
5. Sales J, Fivush R, Teague GW. The role of parental coping in children with asthma’s psychological well-being and asthma-related quality of life. J Pediatr Psychol. 2008;33(2):208–219. doi:10.1093/jpepsy/jsm068
6. Rodríguez EM, Kumar H, Alba-Suarez J, Sánchez-Johnsen L. Parental coping, depressive symptoms, and children’s asthma control and school attendance in low-income, racially, and ethnically diverse urban families. J Asthma. 2017;54(8):833–841. doi:10.1080/02770903.2016.1274402
7. Bartlett SJ, Krishnan JA, Riekert KA, Butz AM, Malveaux FJ, Rand CS. Maternal depressive symptoms and adherence to therapy in inner-city children with asthma. Pediatrics. 2004;113(2):229–237. doi:10.1542/peds.113.2.229
8. Wood B, J L, Miller BD, et al. Testing the biobehavioral family model in pediatric asthma: pathways of effect. Fam Process. 2008;47(1):21–40. doi:10.1111/j.1545-5300.2008.00237.x
9. Waxmonsky J, Wood B, Stern T, et al. Association of depressive symptoms and disease activity in children with asthma: methodological and clinical implications. J Am Acad Child Adolesc Psychiatry. 2006;45(8):945–954. doi:10.1097/01.chi.0000222789.34229.21
10. Miller BD. Circumstances surrounding the deaths of children due to asthma. Am J Dis Child. 1989;143(11):1294. doi:10.1001/archpedi.1989.02150230052022
11. Alcala CS, Orozco Scott P, Tamayo-Ortiz M, et al. Longitudinal assessment of maternal depression and early childhood asthma and wheeze: effect modification by child sex. Pediatr Pulmonol. 2023;58(1):98–106. doi:10.1002/ppul.26164
12. Ramratnam SK, Lockhart A, Visness CM, et al. Maternal stress and depression are associated with respiratory phenotypes in urban children. J Allergy Clin Immunol. 2021;148(1):120–127. doi:10.1016/j.jaci.2021.03.005
13. Perry CD. Does treating maternal depression improve child health management? The case of pediatric asthma. J Health Econ. 2008;27(1):157–173. doi:10.1016/j.jhealeco.2007.03.005
14. Easter G, Sharpe L, Hunt C. Systematic review and meta-analysis of anxious and depressive symptoms in caregivers of children with asthma. J Pediatr Psychol. 2015;40(7):623–632. doi:10.1093/jpepsy/jsv012
15. Pearce A, Dundas R, Whitehead M, Taylor-Robinson D. Pathways to inequalities in child health. Arch Dis Child. 2019;104(10):998–1003. doi:10.1136/archdischild-2018-314808
16. Håkansson KEJ, Guerrero SC, Backer V, Ulrik CS, Rastogi D. Burden and unmet need for specialist care in poorly controlled and severe childhood asthma in a Danish nationwide cohort. Respir Res. 2023;24(1):173. doi:10.1186/s12931-023-02482-7
17. Bateman ED, Hurd SS, Barnes PJ, et al.; GINA. Global strategy for asthma management and prevention. Europ Res J. 2008;31(1):143–178. doi:10.1183/09031936.00138707
18. Håkansson KEJ, Backer V, Suppli Ulrik C. Socioeconomic biases in asthma control and specialist referral of possible severe asthma. Eur Respir J. 2021;58:2100741. doi:10.1183/13993003.00741-2021
19. Nwaru BI, Ekström M, Hasvold P, Wiklund F, Telg G, Janson C. Overuse of short-acting β2 -agonists in asthma is associated with increased risk of exacerbation and mortality: a nationwide cohort study of the global SABINA programme. Eur Respir J. 2020;55(4):1901872. doi:10.1183/13993003.01872-2019
20. TIMES variabel - FAMDISPONIBEL_13. Statistics Denmark; 2023. Available from: https://www.dst.dk/da/Statistik/dokumentation/Times/familieindkomst/famdisponibel-13.
21. Quan H, Li B, Couris CM, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173(6):676–682. doi:10.1093/aje/kwq433
22. Szabó A, Mezei G, Kővári É, Cserháti E. Depressive symptoms amongst asthmatic children’s caregivers. Pediat Allerg Immunol. 2009;21(2):e667–73. doi:10.1111/j.1399-3038.2009.00896.x
23. Heuckendorff S, Johansen MN, Overgaard C, Johnsen SP, Kelly Y, Fonager K. Parental mental health, socioeconomic position and the risk of asthma in children—a nationwide Danish register study. Eur J Public Health. 2022;32(1):14–20. doi:10.1093/eurpub/ckab205
24. Morillo-Vanegas D, Sanchez-Salcedo P, Sebastián Ariño AF. Relationship between pediatric asthma and psychosocial status of caregivers. Respir Med. 2020;174:106187. doi:10.1016/j.rmed.2020.106187
25. Christesen AMS, Knudsen CK, Fonager K, Johansen MN, Heuckendorff S. Prevalence of parental mental health conditions among children aged 0–16 years in Denmark: a nationwide register-based cross-sectional study. Scand J Public Health. 2022;50(8):1124–1132. doi:10.1177/14034948211045462
26. Kessing LV, Pedersen BK, Jespersen NZ, Kristensen JK, Øgard CG. Lægehåndbogen Sundhed.dk. Lægehåndbogen – depression; 2021.
27. Cousino MK, Hazen RA. Parenting stress among caregivers of children with chronic illness: a systematic review. J Pediatr Psychol. 2013;38(8):809–828. doi:10.1093/jpepsy/jst049
28. Celano M, Klinnert MD, Holsey CN, McQuaid EL. validity of the family asthma management system scale with an urban African-American sample. J Pediatr Psychol. 2011;36(5):576–585. doi:10.1093/jpepsy/jsp083
29. Joseph KE, Adams CD, Cottrell L, Hogan MB, Wilson NW. Providing dust mite-proof covers improves adherence to dust mite control measures in children with mite allergy and asthma. Ann Allergy Asthma Immunol. 2003;90(5):550–553. doi:10.1016/S1081-1206(10)61849-2
30. Everhart RS, Fiese BH, Smyth JM. A cumulative risk model predicting caregiver quality of life in pediatric asthma. J Pediatr Psychol. 2008;33(8):809–818. doi:10.1093/jpepsy/jsn028
31. Orrell-Valente JK, Jarlsberg LG, Hill LG, Cabana MD. At what age do children start taking daily asthma medicines on their own? Pediatrics. 2008;122(6):e1186–92. doi:10.1542/peds.2008-0292
32. Ekim A, Ocakci AF. Perceptions of parents and children regarding asthma management responsibilities. J Special Pediat Nurs. 2013;18(4):289–296. doi:10.1111/jspn.12037
33. Freeman A, Tyrovolas S, Koyanagi A, et al. The role of socio-economic status in depression: results from the COURAGE (aging survey in Europe). BMC Public Health. 2016;16(1):1098. doi:10.1186/s12889-016-3638-0
34. Wood BL, Brown ES, Lehman HK, Khan DA, Lee MJ, Miller BD. The effects of caregiver depression on childhood asthma: pathways and mechanisms. Ann Allergy Asthma Immunol. 2018;121(4):421–427. doi:10.1016/j.anai.2018.06.031
35. McDermott LM, Ebmeier KP. A meta-analysis of depression severity and cognitive function. J Affect Disord. 2009;119(1–3):1–8. doi:10.1016/j.jad.2009.04.022
36. Orton S, Jones LL, Cooper S, Lewis S, Coleman T. Predictors of children’s secondhand smoke exposure at home: a systematic review and narrative synthesis of the evidence. PLoS One. 2014;9(11):e112690. doi:10.1371/journal.pone.0112690
37. Fagnano M, Berkman E, Wiesenthal E, Butz A, Halterman JS. Depression among caregivers of children with asthma and its impact on communication with health care providers. Public Health. 2012;126(12):1051–1057. doi:10.1016/j.puhe.2012.08.007
38. Brown ES, Palka JM, Lehman HK, et al. The impact of caregiver depression on child asthma outcomes: pathways and mechanisms. J Allergy Clin Immunol Pract. 2023;11(1):200–209. doi:10.1016/j.jaip.2022.09.016
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.