Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Child Vaccination Coverage, Trends and Predictors in Eastern Ethiopia: Implication for Sustainable Development Goals
Authors Dheresa M ![]() , Dessie Y, Negash B, Balis B
, Dessie Y, Negash B, Balis B ![]() , Getachew T
, Getachew T ![]() , Mamo Ayana G
, Mamo Ayana G ![]() , Merga BT
, Merga BT ![]() , Regassa LD
, Regassa LD ![]()
Received 14 July 2021
Accepted for publication 7 September 2021
Published 21 September 2021 Volume 2021:14 Pages 2657—2667
DOI https://doi.org/10.2147/JMDH.S325705
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Merga Dheresa,1 Yadeta Dessie,2 Belay Negash,2 Bikila Balis,1 Tamirat Getachew,1 Galana Mamo Ayana,2 Bedasa Taye Merga,2 Lemma Demissie Regassa2
1School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Bedasa Taye Merga
School of Public Health, College of Health and Medical Sciences, Haramaya University, P.O.Box: 235, Harar, Ethiopia
Tel +251917723961
Email [email protected]
Background: Every year, immunization prevents about 4– 5 million child fatalities from vaccine preventable morbidities. Conversely, in Ethiopia, achieving full coverage of vaccination has continued to be challenging. Socio-demographic, caregivers and child related factors determine vaccination coverage. Therefore, this study aimed to find out recent coverage, trends in coverage, and its predictors in eastern Ethiopia.
Methods: A population-based longitudinal study design was conducted among 14,246 children aged 12– 24 months from 2017 to 2021 in Kersa Health and Demographic Surveillance System site (KHDSS). The data were collected from caregivers of the child by face to face interview. Multinomial logistic regressions were used to identify predictors of vaccination. The association between vaccination coverage and its predictors was presented by adjusted odds ratio with 95% confidence interval. A p-value of < 0.05 was used to establish statistical significance.
Results: From the 14,198 included children, only 39% of children were fully vaccinated, with highest proportion in 2020 (45%) and lowest proportion in 2019 (32%). In comparison to fully vaccinated, being partially vaccinated was positively associated with older maternal age, rural residence, unemployment, rich wealth index, no antenatal care, facility delivery, and birth order whereas negatively associated with semi-urban residence. In compared to fully vaccinated, being not vaccinated was positively associated with older maternal age, rural residence, maternal education, unemployment, and no antenatal care whereas negatively associated with semi-urban residence, poor wealth index, multipara, grand multipara, and facility delivery.
Conclusion: Less than two-fifths of children aged 12 to 24 months were fully vaccinated. Socio-demographic factors and maternity care utilization were found to be predictors of vaccination coverage. Therefore, strategies that emphasize women’s empowerment in terms of education, economy, and employment status, and enhancing maternal healthcare utilization may improve vaccination coverage.
Keywords: immunization, vaccination, coverage, trends, Kersa HDSS, Ethiopia
Introduction
Immunization is a cost-effective public health program in reducing burden of under-five child morbidity and mortality attributed to vaccine preventable diseases: measles, diphtheria, influenza, tetanus, and pertussis.1 The launching of Expanded Program of Immunization (EPI) in 1974 which targeted strengthening of routine immunization coverage,2,3 has resulted in significant reduction of vaccine preventable causes of child death across the globe.4,5
Every year, immunization averts an estimate of 4–5 million under five child deaths.1,6 Nevertheless, in 2020 19.7 million infants did not receive basic vaccines across the world; sixty percent of them were from 10 developing countries.6,7 Survey from 2010 to 2016 conducted in sub-Saharan countries indicated the average of full vaccination coverage in under-five children was 58.9%; which ranges from 24.2% in Nigeria to 81.3% in Burkina Faso.8
In a 2019 analysis, the pooled full vaccination coverage among children of 12–23 months age was 47% in Ethiopia. The complete vaccination coverage varies across administrative regions ranging from 21% in the Afar regional state to 89% in Amhara regional state.9 Since 2019 Ethiopia is providing 10 antigens targeting major causes of morbidity and mortality during childhood.10
Despite promising improvements in child vaccination coverage in Ethiopia since 2011,11,12 due to its large size population, the country still has a large number of unvaccinated children and there are huge variations in immunization coverage across regions.12 The Ethiopian Demographic Health Survey (EDHS) 2016 report showed that nearly two out of five children aged 12–23 months (39%) received all basic vaccinations at some time, and 22% were vaccinated by the appropriate age.12
Improving vaccination coverage has been challenged due to factors such as quality of services, local and regional inequalities,13,14 competing health priorities, inadequate monitoring and evaluation, resource limitations, and socio-behavioral variables.13–16 Socio-demographic factors,17 maternal health services utilizations during antenatal, delivery and postnatal period,18 were found to be predictors for child vaccination.19 Poor perception toward vaccination and lack of awareness were deterring caregivers from seeking vaccination for their children.20,21
Universal immunization coverage is among health related targets of sustainable development goals (SDGs) by 2030.7 In addition to sharing the SDGs, Ethiopia has set a national five year health sector transformation plan to increase the full vaccination coverage to 95% by 2020.22
Tracking the progress of vaccination, and identifying the hurdles that deter child from taking vaccine is crucial to plan and reorient tailored strategies. However, the evidences generated from health management information systems (HMIS)22,23 and/or cross sectional surveys,12,24 do not reflect the true features of vaccination coverage. Thus, this study aimed at finding out recent vaccination coverage, trends and its predictors among children prospectively followed in Kersa HDSS, Eastern Ethiopia.
Methods
Study Setting and Period
We enrolled 12 to 24 month old children from Kersa Health Demographic Surveillance System (HDSS) field site of Eastern Ethiopia from January 1, 2017 to April 29, 2021. Kersa HDSS was established in 2007, initial census included 12 kebeles (small administrative unit in Ethiopia) of Kersa district.25 HDSS field site was extended to Harari region (Harar town) in 2012 and operates among 6 kebeles. The HDSS continuously collects data related to socio-demography, health and observes demographic changes in the designated population. Currently, the HDSS includes 41,056 households and a total population of 197,268 in 36 kebeles (24 kebeles from Kersa districts, and 12 kebeles from Harar town).26
Study Design and Population
Kersa HDSS employs an open dynamic cohort design which longitudinally follows individuals living within a specific geographic area. The main variables include migration, membership/relation to the head of household, birth, death, pregnancy observation and birth outcome were collected regularly and updated every six months. Among the other add-on variables, vaccination variables updated every year on the first round of data collection period. Children whose age was 12 to 24 months (12 and 24 months are inclusive lower and upper bounds) were extracted from Kersa HDSS database system during June 1–20, 2021. The extracted information contains child name, household name, household ID, individual ID, and residents Kebele. Data collectors interviewed the care takers/mother of the child about their immunization status each year at the first round data collection period.
This study included a total of 14,246 children aged 12–24 months old who were assessed from January 1, 2017 through April 29, 2021. We included all the households in the surveillance site which had eligible children.
Data Collection Procedure
Data collection was conducted by trained HDSS staff through face to face interviews using Open Data Kit (ODK) application. Trained supervisors supervised data collection in the field and checked data quality before it was sent to the database system. Information about vaccination status was collected by using the questionnaire and immunization cards were verified physically to validate information and confirm the appropriate date of vaccination. Where immunization card was not available, verification was done by examining BCG scar and interviewing the respondent during the home visit for every child. The data manager approved the quality of data and migrated data from temporary storage (ODK aggregate) to the final storage Openhds database system. Data from January 1, 2017 through April 29, 2021 were extracted. The data extraction was conducted during June 1–20, 2021.
Variables and Measurements
The Outcome Variable
Vaccination status, categorized as “not vaccinated”, “partially vaccinated” and “fully vaccinated”, as defined below in the operational definitions.
Predictor Variables
Socio-demographic variables: residence, maternal educational level, occupation, and wealth index. Obstetrics factors like age at first child birth, parity, place of delivery, antenatal care, and birth attendant. Neonatal factors: birth order and child sex were considered as predictors of child vaccination.
Operational Definition
Vaccination Status
The child who received all antigen (BCG, four dose of OPV (0–3), Pentavalent (1–3), PCV (1–3), Rota virus vaccine (2 doses) and measles vaccine (one dose) and the recommended dose categorized as “fully vaccinated”, if the child received at least one antigen they were categorized as “partially vaccinated”, and if they did not receive a single antigen they were categorized as “not vaccinated”.
Vaccination Coverage
The proportion of the eligible children (12–24 months in this case) who received recommended vaccines. According to Ethiopian EPI guideline, BCG vaccine, four doses of OPV (0–3), Pentavalent (1–3), PCV (1–3), two doses of Rota virus vaccine and one dose of measles vaccines are recommended, and the last vaccine dose (measles vaccine) is expected to be given at nine months after birth.
Vaccination Dropout Rate
In this study it is the rate difference between the first and the last dose or the rate difference between the initial vaccine and the last vaccine.
Maternal Educational Level
Maternal educational level was categorized as “literate” if attended any formal school; if not enrolled in any formal education but can read and write or read, was labeled as “can read and/or write”; if neither able to read nor write was labeled as “neither read nor write”.
Place of Residence
Individuals living in Harar City were labeled as “urban”, those living in the small town in Kersa were labeled as “semi urban” and those living in Kersa rural area were labeled as “rural”.
Wealth Index
Households were given scores based on the number and kinds of consumer goods they own, these scores are derived using principal component analysis. Wealth index are compiled by assigning the household score to each usual household member, ranking each person in the household population by her or his score and grouped individuals into three quartiles (poor, middle, and rich).
Data Management and Statistical Analysis
STATA version 16.0 software was used for data analysis. Data were cleaned, coded, and recoded before analysis. Vaccination coverage was computed for overall vaccination and each vaccine type defined by WHO.27 Percentage of vaccination coverage is number of children who received the vaccination divided by total number of 12 to 24 months children and multiplied by 100.
Descriptive analysis was presented with proportion, mean, standard deviation, median and interquartile range. The trends over years for vaccination coverage was done and presented with line graph. The statistical test for the significance of changes seen over years are presented with z and p<0.05. Multinomial logistic regression was used to find out predictors of vaccination coverage. The outcome variable was categorized in to “fully vaccinated”, “partially vaccinated”, and “not vaccinated”. In multinomial logistic regression fully vaccinated was considered as the base. Before fitting the model, chi-square assumption was checked. For each predictor variables bi-variable multinomial logistic model was fitted. In bi-variable analysis predictors with a p-value less than 0.2 were included in multivariable model. Finally, multinomial logistics regression model was fitted for level of vaccination (not vaccinated, partially vaccinated and fully vaccinated) with covariates significant in bi-variables model. The association between outcome and predictors was presented by adjusted odds ratios (AORs) with 95% confidence interval. Moreover, after fitting the model goodness of the final model was checked by using the Hosmer-Lemeshow test. The Hosmer-Lemeshow statistic indicates a good fit at p-value of 0.05 or greater.
Ethical Clearance
The HDSS obtained ethical approval from national ethical review committee and Haramaya University College of health and medical science, institutional health research ethical review committee (IHRERC). After explaining the purpose and voluntary nature of the study, written consent was obtained from each participant. For participants who cannot read and write, the data collectors were read the consent and obtain the fingerprint sign. Confidentiality of information obtained from the study participants was assured throughout the study. Personal identifiers were removed from the data. We confirm that this study complies with the Declaration of Helsinki.
Results
Socio-Demographic Characteristics of the Study Participants
From the total 14,246 children of 12 to 24 months age, 14,198 children were included in the analysis. Forty eight records were excluded from further analysis because of incompletely filled survey forms. Thirteen percent of the participants were from Harar town, and 47% were females. The median (IQR) age of mothers was 28.8 (10.4) years and the median (IQR) age at first birth was 19 (2) years. From the total caregivers, 5963 (42%) had history of antenatal care for their included child and 38% children were delivered at health facilities (Table 1).
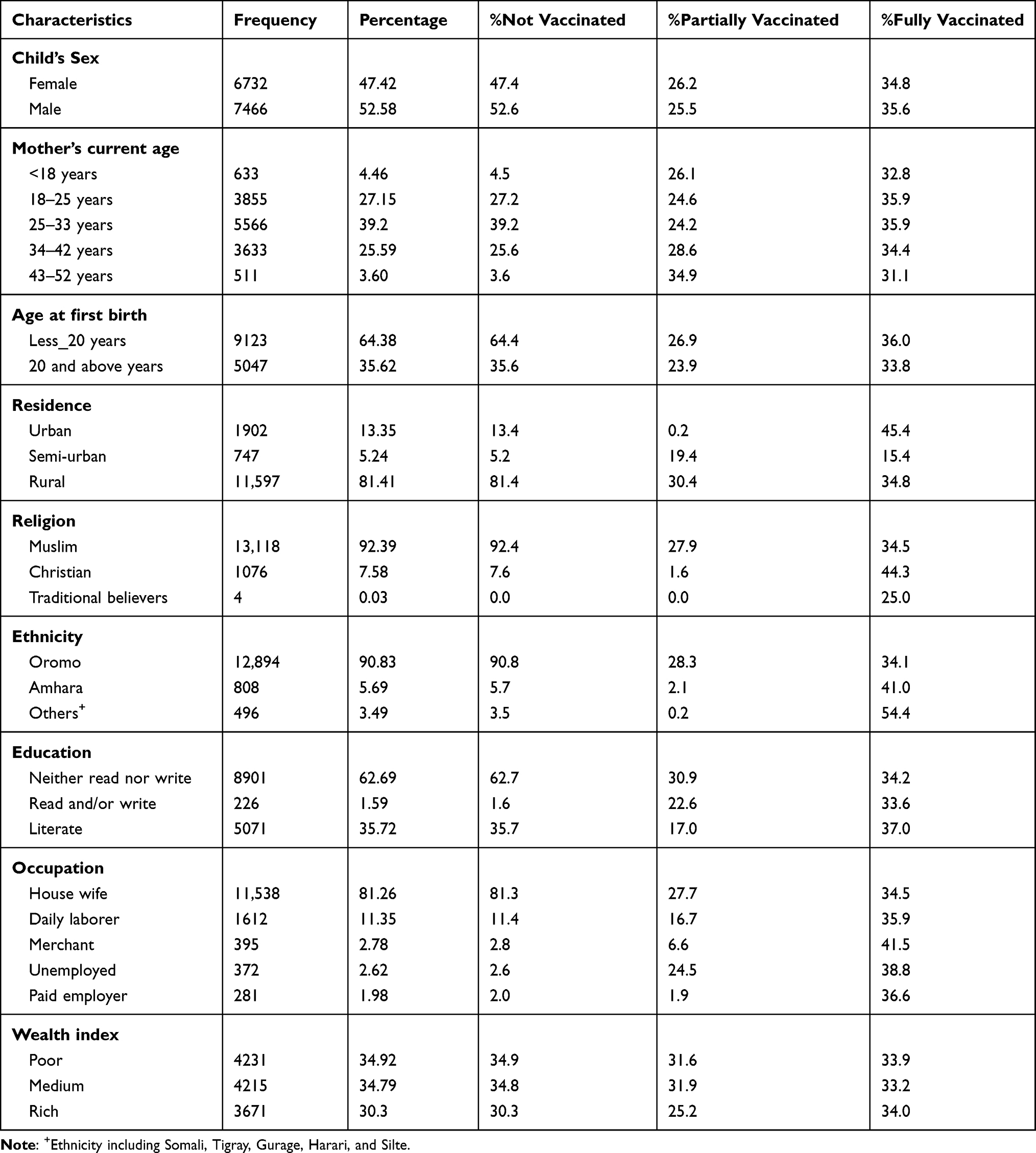 |
Table 1 Socio-Demographic Characteristics of the Caregivers and Children in Kersa HDSS from 2017 to 2021 (n=14,198) |
Vaccination Coverage
From a total of 14,198 children for whom vaccination cards, BCG scar or verbal vaccination history was assessed, 25.8% had not received any vaccine at all. The lowest vaccine coverage was recorded for measles (64.9%) while the highest coverage was for both OPV1 and Penta1 (71.8%). The full and partial vaccination coverage was 39% and 35.2%, respectively. The highest full coverage was recorded in 2021 (44.6%) and the lowest coverage was recorded in 2019 (32%). On the other hand, the partial vaccination coverage was highest in 2019 (42%); highest proportion of children were not vaccinated in 2020 (39.6%) (Table 2).
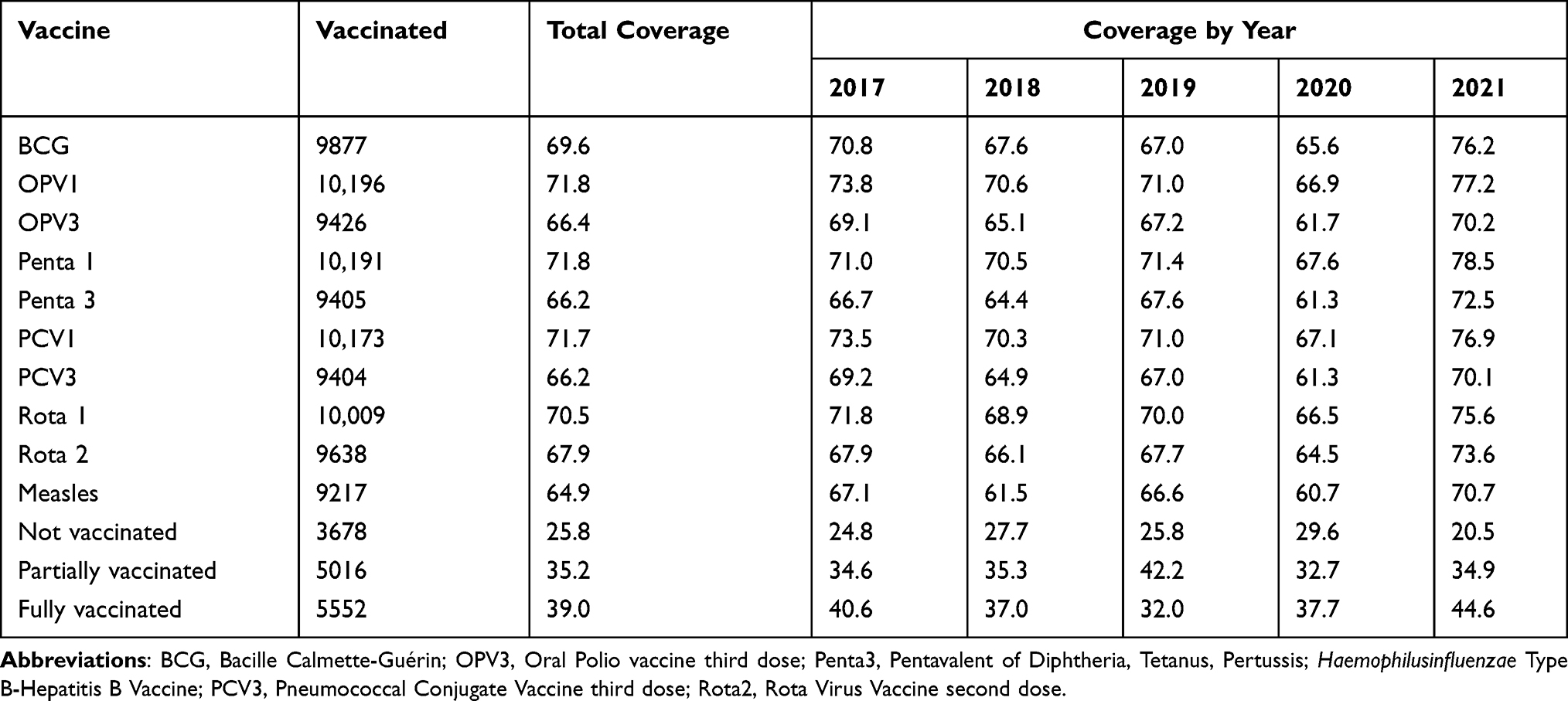 |
Table 2 Vaccination Coverage by Vaccine Type and Year of Survey (2017–2021) |
The trend of full vaccination coverage showed increment from 2017 to 2021 (z =3.7, p-value < 0.001) as that of partial vaccination drops (Figure 1A). Trend of full vaccination for each vaccine type also increased over time, with sharp increase of Rota vaccine coverage from 87% to 92%. The trend of measles vaccination was fluctuating; as decreased in 2018 and 2020 and increased to peak of 71% in 2021 (Figure 1B).
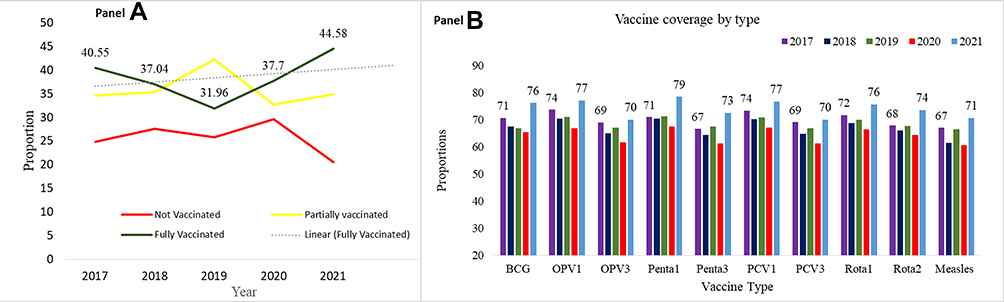 |
Figure 1 Trend of vaccination coverage among children from Kersa HDSS from 2017 to 2021. (A) Trend of status of vaccination (none, partially or fully), (B) Trend of each vaccination type. Abbreviations: BCG, Bacille Calmette-Guérin; OPV3, Oral Polio vaccine third dose; Penta3, Pentavalent of Diphtheria, Tetanus, Pertussis, Haemophilusinfluenzae type B-Hepatitis B Vaccine; PCV3, Pneumococcal Conjugate Vaccine third dose; Rota2, Rota Virus Vaccine second dose. |
Vaccine Dropout Rate
The dropout rates for specific vaccines ranged from 7.5% for OPV and 33.9% for Rota vaccine. Vaccine dropout was higher among women with multiple births (49.4%) than primiparas (18.9%). Vaccine dropout was also higher among children from rural (80.5%) than children from urban (17.1%) and semi-urban (2.3%). Similarly, children from women who cannot read and write (61%) have higher dropout than children from literate women (37.5%). Comparing the perinatal services, women who have antenatal care (44.6% for ANC Vs 55.4% for no ANC) and delivered at health institution (41.4% for institution vs 58.6% for home) have about 11% and 17% lower dropout respectively.
Predictors of Vaccination Status
Compared to fully vaccinated, being partially vaccinated and not vaccinated was significantly associated with maternal age, residence, maternal educational level and occupation, wealth index, antenatal care, institutional delivery, birth order and parity.
Current age of mother related to the increased odds of being partially vaccinated and not vaccinated. Compared to child from younger mother, being from caregivers whose age was 18–25 yrs. (AOR: 1.44; 95% CI: 1.11, 1.85), 25–33 yrs. (AOR: 1.60; 95% CI: 1.21, 2.12), and 34–42 yrs. (AOR: 1.65; 95% CI: 1.21, 2.25) increases the odds of partially vaccinated by 44%, 60%, and 65% respectively. Similarly, being from caregivers whose age was 25–33 yrs. (AOR:1.50; 95% CI: 1.12, 2.00), 34–42 yrs. (AOR:1.75; 95% CI: 1.27, 2.41) and 43–52 yrs. (AOR:2.04; 95% CI: 1.35, 3.07) increases the odds of not vaccinated by 1.5, 1.75, and 2 times respectively; compared to 15–18 yrs. old mother.
Compared to urban children, the chance of partially immunized among rural children was increased by 39% (AOR: 1.39; 95% CI: 1.15, 1.67). The odds of totally not immunized for rural children also increased by more than five times (AOR: 5.72; 95% CI: 4.82, 7.63). Contrary to the rural, being from semi-urban decreases the chance of partially vaccinated (AOR: 0.26; 95% CI: 0.20, 0.34) and totally not vaccinated (AOR: 0.47; 95% CI: 0.36, 0.62).
Being born to uneducated mother increased the odds of not vaccinated by 20% (AOR: 1.20; 95CI: 1.06, 1.37) compared to children born to educated caregivers. On the other hand, mother’s education did not significantly associate with partial vaccination status of children. Being born to unemployed mother increased the odds of partially vaccinated (AOR: 1.49; 95% CI: 1.25, 1.76) and not vaccinated (AOR: 1.44; 95% CI: 1.21, 1.73) compared to children born to housewife. Children whose caregivers are daily laborer also have 65% (1.65 (1.03, 2.64) higher chance of partially vaccinated.
Wealth index was significantly associated with vaccination status. Children from rich family had 14% (AOR: 0.86; 95% CI: 0.75, 0.99) lower chance of not vaccinated that of children from poor family. Once vaccination is initiated, the children from wealthy (rich) family (AOR: 1.22; 95% CI: 1.07, 1.38) have higher chance of dropping vaccination compared to children from poor family.
The odds of not vaccinated among children from multipara (AOR: 0.76; 95% CI: 0.64, 0.91) and grand multipara (AOR: 0.76; 95% CI: 0.58, 0.99) caregivers was decreased by 24% compared to children from caregivers give birth for first time. Children whose caregivers did not receive antenatal care had 67% higher odds of not vaccinated (AOR: 1.67; 95% CI: 1.50, 1.87) and 33% higher odds of partially vaccinated (AOR: 1.33; 95% CI: 1.20, 1.48). Children delivered at health facility have 17% (AOR: 0.83; 95% CI: 0.73, 0.94) less chance of not vaccinated compared to those who delivered at home. To the opposite of this, the odds of partial vaccination for children delivered at health facility were increased by 12% (AOR: 1.12; 95% CI: 1.01, 1.26). As the birth order of the child increased by one, the odds of partially vaccinated was increased by 4% (AOR: 1.04; 95% CI: 1.01, 1.09) Table 3.
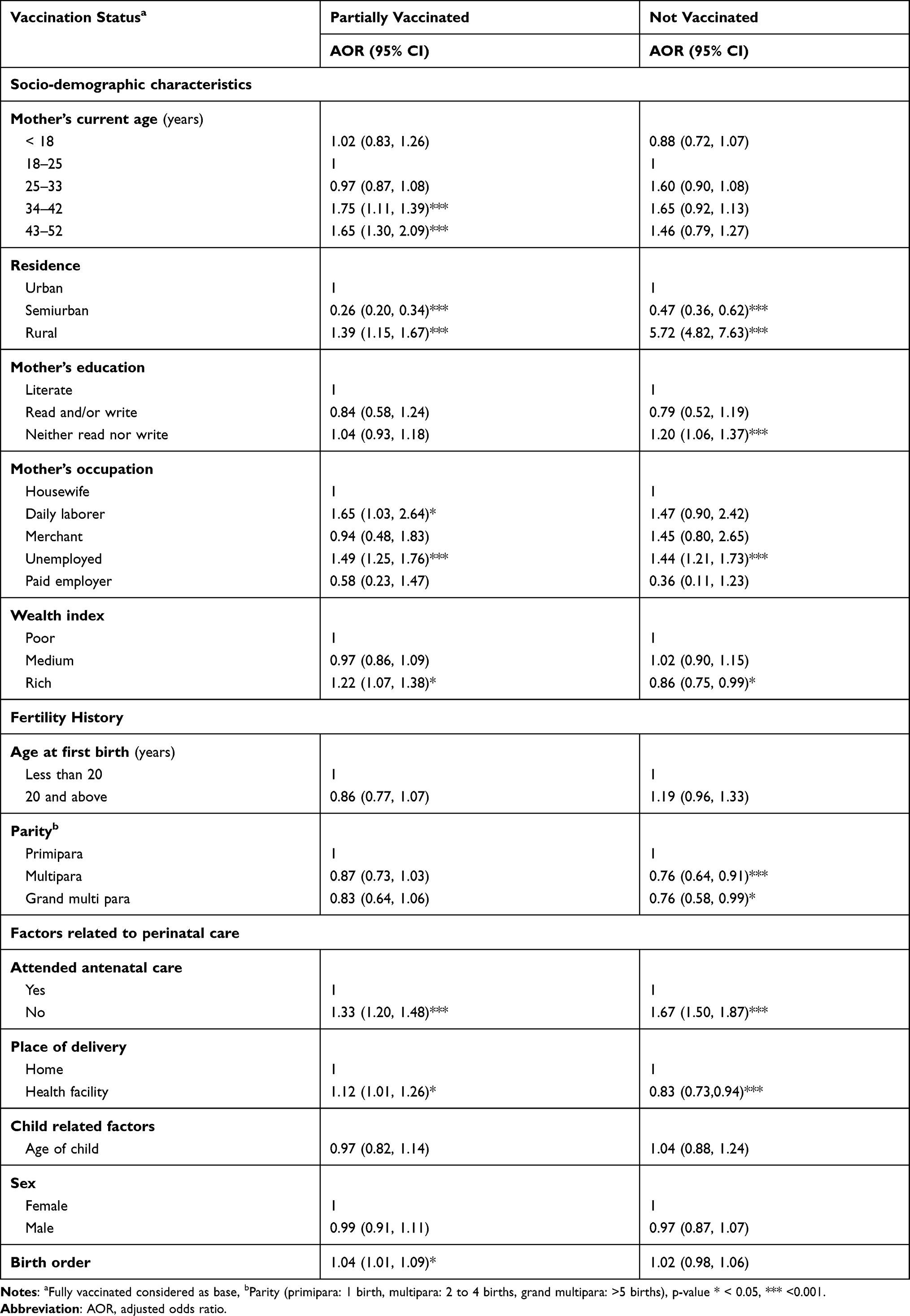 |
Table 3 Multivariable Multinomial Logistic Regression for Vaccination Status Among Children of 12 to 30 Months of Age from 2017 to 2021 |
Discussion
In this study only 39% of children were fully vaccinated. This finding has a great implication on surviving and thriving of children, combating infectious and preventable disease, and future development and productivities. Our finding is far behind the national goal of reaching 95% by 2020. With this momentum, Ethiopia strived to make sure healthy lives and promote welfare for its citizens (SDG3), and to reduce neonatal and child mortality rate.28–31 Hence, the current national intervention strategies need to be sought again and tailored to bring results.
The vaccination coverage was lower than the 2019 national coverage (43% for fully vaccination and 59% for partial vaccination).24 This finding is supported with findings from EDHS 2016 reports 38.3%,32 Ambo (36.9%),33 and Jigjiga (36.6%).34 Conversely, this finding is lower than the findings reported by study conducted in central Ethiopia (75.6%).35 The coverage varies across regions of the country as indicated in two different pooled analyses in 2020. Nour et al 2020 reported that the pooled immunization coverage of 28 articles was 47%9 and Eshete et al 2020 reported higher (58.9%) pooled coverage from the analysis of 30 studies.36 The difference of magnitude might be due to difference in geographical difference,37–40 and distribution of health facilities.41 Another reason of difference might be study period; most of the former studies were limited to one year or less time. On the other hand our study included a large number of children over the period of five-year surveillance. The larger the target group included the more dropout and not vaccinated children could be included.42,43
Similarly our report is lower than the findings reported from other sub-Saharan countries like Mozambique (71.8%),44 and Tanzania (71.1%).45 These variations might be due to the discrepancies in study periods and designs. Another reason for the observed discrepancy might be variations in access to vaccination services and public awareness about child vaccination.
This study revealed that children from rural areas had more chance of partially vaccinated or not vaccinated at all. This finding is in support of studies conducted in Ethiopia using national data,46 Mecha district of northwest Ethiopia,47 Jigjiga,34 and in Ghana.48 Different barriers could hinder the rural women to utilize maternal and child healthcare service. The major reason could be low service accessibility which hinders full vaccination of children.35 In eastern Ethiopia where the rural health coverage is low, receiving quality and affordable health care is difficult for caregivers. Women from rural area should go far and pay extra cost to vaccinate their children than the urban women did. This in turn might result in higher dropout and low vaccination uptake.
Children from uneducated caregivers were more likely to be non-vaccinated. The role of mother’s education as determinants of vaccination utilization has also been stated by other studies.49–51 Adedokun et al 2020 and Khanam et al, 2020 discussed that education has positive impact on healthcare seeking of the caregivers by empowering them on decision making regardless of their social, family and child factors.52,53 Hence the association might be justified by the fact that educated parents have more understanding of the importance of childhood vaccination and child health than uneducated parents.
The odds of partially vaccinated and not vaccinated at all were higher among children whose caregivers were unemployed. Similarly, other studies conducted in Uganda54 and Nepal also supported the findings.55 This might be justified by the low income of the unemployed which in turn determines their health service access and utilization. In spite of the free of charge provision of vaccination in government health facilities in Ethiopia, there are non-direct costs, such as transport cost. Similarly, children whose mother’s job is daily laborer are more prone to partial vaccination. This could be explained by inability to be absent from work as a result of the much time spent for travel to and time spent in the health facility.56
Being from rich family decreases the odds of not vaccinated but increases the odds of dropout. The finding related to not being vaccinated is in line with previous reports.9,51,53,56–58 This might be the result of persistent health disparities that exist between poor and rich households. Women from the poor family probability has less empowerment to give decision, inability to pay costs and spend more time to earn the means of livelihood.13,41,53
Not utilizing maternal health service was negatively associated with vaccination uptake of the children included in this study. The chance of partially immunized or not immunized was higher among children whose mother had no antenatal care and did not access institutional delivery. The result was in line with previous reports.13,59,60 Maternal and child health care are interrelated. The more women adhere to maternal and child care, the more women know benefit, understand the appointment and improved communication with care providers.61,62 These help women to increase their child’s vaccination compliance.
Maternal health care utilization was associated with vaccination status of the children included in this study. The chance of being partially vaccinated or not vaccinated was higher among children whose mother had no antenatal care and did not access institutional delivery. The result was in line with previous reports.13,59,60 Child and maternal healthcare are interrelated. The more women adhere to maternal and child care, the more women know benefit, understand the appointment and improved communication with care providers.61,62
Our study, however, showed opposite relationship between institutional delivery and partial vaccination. Previous studies reported the opposite.13,57,59,60,63–65 Institutional deliveries advantage for further maternal and childcare is not questionable. However, the inability of caregivers to transition from delivery services and to later continue with care provided for their children is a major concern in sub-Saharan Africa.62 Hence bad experience from the previous care might discourage them to come again for vaccination. This might be a possible reason of negative association between partial vaccination and institutional delivery. As a result, compassionate care to have a good connections with women by identifying their needs, increasing understanding of each woman’s needs and desiring is essential during the childbirth.66
The Strengths and Limitations of the Study
The study included a large sample which were prospectively collected over the period of five years. Nevertheless, in this study partially vaccinated included a child who has received a single antigen or who has missed a single antigen, thus, there is substantial difference between children with a single antigen versus children missing a single. Therefore, in interpreting the findings of this study one should take into account the mentioned limitations.
Conclusions
The overall vaccination status in the study area is not geared to break the chain of communicable diseases to attain SDGs goal 3. The complex interaction of socio-demographic characteristics, reproductive health, and maternity care were found to be associated factors for partially vaccinated and not vaccinated. Hence, improving women’s education and employment status may help in increasing the vaccination coverage. In addition, increasing access to and encouraging utilization of maternal healthcare services like antenatal care and institutional delivery could help improve vaccination coverage. Moreover, devising strategies that increase the vaccination coverage of the rural residents by increasing vaccination centers at their vicinity and convenience may be emphasized.
Data Sharing Statement
The datasets used in this study can be available from Kersa Demographic and Health Surveillance System (http://www.indepth-network.org/member-centres/kersa-0) upon reasonable request.
Acknowledgments
Authors are thankful to Haramaya University for the opportunity to conduct the study. We are grateful to data collectors for their commitment and study participants for their participation in this study.
Author Contributions
All authors contributed to conception, study design, data analysis, drafting or revising the article, gave final approval of the version to be published, agreed to the submitted to this journal, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. CDC. Global immunization strategies framework 2011–2015; 2015. Available from: https://www.cdc.gov/globalhealth/immunization/docs/gid-strat-framewk.pdf.
2. Wiysonge CS, Uthman OA, Ndumbe PM, Hussey GD. A bibliometric analysis of childhood immunization research productivity in Africa since the onset of the expanded program on immunization in 1974. BMC Med. 2013;11(1):1–10. doi:10.1186/1741-7015-11-66
3. Okwo-Bele J-M, Cherian T. The expanded programme on immunization: a lasting legacy of smallpox eradication. Vaccine. 2011;29:D74–D79. doi:10.1016/j.vaccine.2012.01.080
4. World Health Organization. Immunization agenda 2030: a global strategy to leave no one behind; 2019. Available from: https://www.who.int/teams/immunization-vaccines-and-biologicals/strategies/ia2030.
5. World Health Organization. Vaccines & diseases. Geneva; 2019. Available from: https://www.who.int/teams/immunization-vaccines-and-biologicals/diseases.
6. World Health Organization. Immunization coverage; 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage.
7. UN. The sustainable development goals report 2019; 2019. Available from: https://unstats.un.org/sdgs/report/2019/The-Sustainable-Development-Goals-Report-2019.pdf.
8. Costa JC, Weber AM, Darmstadt GL, Abdalla S, Victora CG. Religious affiliation and immunization coverage in 15 countries in Sub-Saharan Africa. Vaccine. 2020;38(5):1160–1169. doi:10.1016/j.vaccine.2019.11.024
9. Nour TY, Farah AM, Ali OM, Abate KH. Immunization coverage in Ethiopia among 12–23 month old children: systematic review and meta-analysis. BMC Public Health. 2020;20(1134):1–12.
10. Health EMo. Expanded Program on Immunization (EPI); 2020.
11. CSA I. Ethiopia Demographic and Health Survey. Rockville, Maryland, USA; 2011.
12. CSA I. Ethiopia Demographic and Health Survey. Rockville, Maryland, USA; 2016.
13. Shibre G, Zegeye B, Idriss-Wheeler D, Yaya S. Inequalities in measles immunization coverage in Ethiopia: a cross-sectional analysis of demographic and health surveys 2000–2016. BMC Infect Dis. 2020;20(1):1–12. doi:10.1186/s12879-020-05201-5
14. Bobo FT, Hayen A. Decomposition of socioeconomic inequalities in child vaccination in Ethiopia: results from the 2011 and 2016 demographic and health surveys. BMJ Open. 2020;10(10):e039617. doi:10.1136/bmjopen-2020-039617
15. Faye CM, Wehrmeister FC, Melesse DY, et al. Large and persistent subnational inequalities in reproductive, maternal, newborn and child health intervention coverage in sub-Saharan Africa. BMJ Global Health. 2020;5(1):e002232. doi:10.1136/bmjgh-2019-002232
16. Restrepo-Méndez MC, Barros AJ, Wong KL, et al. Inequalities in full immunization coverage: trends in low- and middle-income countries. Bull World Health Organ. 2016;94(11):794. doi:10.2471/BLT.15.162172
17. Koku Sisay T, Malede Mequanent S. Full immunization coverage and its associated factors among children aged 12–23 months in Ethiopia: further analysis from the 2016 Ethiopia demographic and health survey. BMC Public Health. 2019;19(1019):1–7.
18. Atnafu A, Andargie G, Yitayal M, et al. Prevalence and determinants of incomplete or not at all vaccination among children aged 12–36 months in Dabat and Gondar districts, northwest of Ethiopia: findings from the primary health care project. BMJ Open. 2020;10(12):e041163. doi:10.1136/bmjopen-2020-041163
19. Tefera Alemu M, Muluken Azage Y, Kebadnew Mulatu M. Age-appropriate vaccination coverage and its associated factors for pentavalent 1–3 and measles vaccine doses, in northeast Ethiopia: a community-based cross-sectional study. PLoS One. 2019;14(8):e0218470. doi:10.1371/journal.pone.0218470
20. Yaya S, Bishwajit G, Uthman OA, Amouzou A, Leone T. Why some women fail to give birth at health facilities: a comparative study between Ethiopia and Nigeria. PLoS One. 2018;13(5):e0196896. doi:10.1371/journal.pone.0196896
21. Kifle MM, Kesete HF, Gaim HT, Angosom GS, Araya MB. Health facility or home delivery? Factors influencing the choice of delivery place among mothers living in rural communities of Eritrea. J Health Popul Nutr. 2018;37(1):1–15. doi:10.1186/s41043-018-0153-1
22. Health EFMo. Health Sector Transformation Plan (2015/16–2019/20); 2015.
23. Health EMo. Key Immunization Performance, 2011. EFY; 2019.
24. EPHI C, ICF. Ethiopia Mini Demographic and Health Survey 2019: Key Indicators. Rockville, Maryland, USA; 2019.
25. Assefa N, Lakew Y, Belay B, et al. Neonatal mortality and causes of death in Kersa Health and Demographic Surveillance System (Kersa HDSS), Ethiopia, 2008–2013. Matern Health Neonatol Perinatol. 2016;2:7. doi:10.1186/s40748-016-0035-8
26. Assefa N, Oljira L, Baraki N, et al. HDSS profile: the Kersa Health and Demographic Surveillance System. Int J Epidemiol. 2016;45(1):94–101. doi:10.1093/ije/dyv284
27. WHO. The EPI coverage survey; 2015. Available from: https://www.who.int/immunization/documents/MLM_module7.pdf.
28. FMOH. Comprehensive Multi- Comprehensive Multi-Year Plan 2016–2020; 2015.
29. WHO. IMMUNIZATION AGENDA 2030: A Global Strategy to Leave No One Behind; 2020.
30. FMOH. National Strategy for Newborn and Child Survival in Ethiopia (2015/16–2019/20); 2015.
31. FMOH. Health Sector Transformation Plan II (HSTP II) 2020/21–2024/25; 2021.
32. Tamirat KS, Sisay MM. Full immunization coverage and its associated factors among children aged 12–23 months in Ethiopia: further analysis from the 2016 Ethiopia demographic and health survey. BMC Public Health. 2019;19(1):1–7. doi:10.1186/s12889-019-7356-2
33. Etana B, Deressa W. Factors associated with complete immunization coverage in children aged 12–23 months in Ambo Woreda, Central Ethiopia. BMC Public Health. 2012;12(1):1–9. doi:10.1186/1471-2458-12-566
34. Mohamud AN, Feleke A, Worku W, Kifle M, Sharma HR. Immunization coverage of 12–23 months old children and associated factors in Jigjiga District, Somali National Regional State, Ethiopia. BMC Public Health. 2014;14(1):1–9. doi:10.1186/1471-2458-14-865
35. Mekonnen AG, Bayleyegn AD, Ayele ET. Immunization coverage of 12–23 months old children and its associated factors in Minjar-shenkora district, Ethiopia: a community-based study. BMC Pediatr. 2019;19(198):1–8
36. Eshete A, Shewasinad S, Hailemeskel S. Immunization coverage and its determinant factors among children aged 12–23 months in Ethiopia: a systematic review, and meta- analysis of cross-sectional studies. BMC Pediatr. 2020;20(1):283. doi:10.1186/s12887-020-02163-0
37. Ikilezi G, Augusto OJ, Sbarra A, Sherr K, Dieleman JL, Lim SS. Determinants of geographical inequalities for DTP3 vaccine coverage in sub-Saharan Africa. Vaccine. 2020;38(18):3447–3454. doi:10.1016/j.vaccine.2020.03.005
38. Melaku MS, Nigatu AM, Mewosha WZ. Spatial distribution of incomplete immunization among under-five children in Ethiopia: evidence from 2005, 2011, and 2016 Ethiopian demographic and health survey data. BMC Public Health. 2020;20(1):1362. doi:10.1186/s12889-020-09461-3
39. Prada JM, Metcalf CJE, Takahashi S, Lessler J, Tatem AJ, Ferrari M. Demographics, epidemiology and the impact of vaccination campaigns in a measles-free world - can elimination be maintained? Vaccine. 2017;35(11):1488–1493. doi:10.1016/j.vaccine.2017.02.008
40. Uthman OA, Sambala EZ, Adamu AA, et al. Does it really matter where you live? A multilevel analysis of factors associated with missed opportunities for vaccination in sub-Saharan Africa. Hum Vaccin Immunother. 2018;14(10):2397–2404. doi:10.1080/21645515.2018.1504524
41. Tola HH, Gamtesa DF. High inequality and slow services improvement in newborn and child health interventions in Ethiopia. Pediatric Health Med Ther. 2020;11:513–523. doi:10.2147/PHMT.S286652
42. Hajian-Tilaki K. Sample size estimation in epidemiologic studies. Caspian J Intern Med. 2011;2(4):289–298.
43. Hee SW, Willis A, Tudur Smith C, et al. Does the low prevalence affect the sample size of interventional clinical trials of rare diseases? An analysis of data from the aggregate analysis of clinicaltrials.gov. Orphanet J Rare Dis. 2017;12(1):44. doi:10.1186/s13023-017-0597-1
44. Jani JV, De Schacht C, Jani IV, Bjune G. Risk factors for incomplete vaccination and missed opportunity for immunization in rural Mozambique. BMC Public Health. 2008;8(1):1–7. doi:10.1186/1471-2458-8-161
45. Chambongo PE, Nguku P, Wasswa P, Semali I. Community vaccine perceptions and its role on vaccination uptake among children aged 12–23 months in the Ileje District, Tanzania: a cross section study. Pan Afr Med J. 2016;23(1). doi:10.11604/pamj.2016.23.162.8925
46. Debie A, Lakew AM. Factors associated with the access and continuum of vaccination services among children aged 12–23 months in the emerging regions of Ethiopia: evidence from the 2016 Ethiopian demography and health survey. Ital J Pediatr. 2020;46(28). doi:10.1186/s13052-020-0793-9
47. Debie A, Taye B. Assessment of fully vaccination coverage and associated factors among children aged 12–23 months in Mecha District, north West Ethiopia: a cross-sectional study. Sci J Public Health. 2014;2(4):342–348. doi:10.11648/j.sjph.20140204.26
48. Budu E, Darteh EKM, Ahinkorah BO, Seidu -A-A, Dickson KS. Trend and determinants of complete vaccination coverage among children aged 12–23 months in Ghana: analysis of data from the 1998 to 2014 Ghana demographic and health surveys. PLoS One. 2020;15(10):e0239754. doi:10.1371/journal.pone.0239754
49. Fenta SM, Biresaw HB, Fentaw KD, Gebremichael SG. Determinants of full childhood immunization among children aged 12–23 months in sub-Saharan Africa: a multilevel analysis using demographic and health survey data. Trop Med Health. 2021;49(29). doi:10.1186/s41182-021-00319-x
50. Mukungwa T. Factors associated with full immunization coverage amongst children aged 12–23 months in Zimbabwe. Afr Pop Stud. 2015;29(2). doi:10.11564/29-2-745
51. Girmay A, Dadi AF. Full immunization coverage and associated factors among children aged 12–23 months in a hard-to-reach areas of Ethiopia. Int J Pediatr. 2019;2019:1924941. doi:10.1155/2019/1924941
52. Adedokun ST, Yaya S. Factors influencing mothers’ health care seeking behaviour for their children: evidence from 31 countries in sub-Saharan Africa. BMC Health Serv Res. 2020;20(1):842. doi:10.1186/s12913-020-05683-8
53. Khanam M, Hasan E. Inequalities in health care utilization for common illnesses among under five children in Bangladesh. BMC Pediatr. 2020;20(1):192. doi:10.1186/s12887-020-02109-6
54. Bbaale E. Factors influencing childhood immunization in Uganda. J Health Popul Nutr. 2013;31(1):118. doi:10.3329/jhpn.v31i1.14756
55. Bhandari P, Shrestha SS, Ghimire DJ. Sociocultural and geographical disparities in child immunization in Nepal. Asia Pac Popul J. 2007;22(1):43–64. doi:10.18356/1e441780-en
56. Obanewa OA, Newell ML. The role of place of residency in childhood immunisation coverage in Nigeria: analysis of data from three DHS rounds 2003–2013. BMC Public Health. 2020;20(1):123. doi:10.1186/s12889-020-8170-6
57. Grout L, Conan N, Juan Giner A, et al. Local discrepancies in measles vaccination opportunities: results of population-based surveys in Sub-Saharan Africa. BMC Public Health. 2014;14:193. doi:10.1186/1471-2458-14-193
58. Murtaza F, Mustafa T, Awan R. Child health inequalities and its dimensions in Pakistan. J Family Community Med. 2015;22(3):169–174. doi:10.4103/2230-8229.163036
59. Budu E, Seidu AA, Agbaglo E, et al. Maternal healthcare utilization and full immunization coverage among 12–23 months children in Benin: a cross sectional study using population-based data. Arch Public Health. 2021;79(1):34. doi:10.1186/s13690-021-00554-y
60. Deressa AT, Desta MS, Belihu TM. Vaccination status and associated factors among street children 9–24 months old in Sidama Region, Ethiopia. Ann Glob Health. 2020;86(1):4. doi:10.5334/aogh.2650
61. WHO. The maternal, newborn, and child health continuum of care: opportunities for Africa’s Newborns; 2020. Available from: https://www.who.int/pmnch/media/publications/aonsectionII.pdf.
62. Owili PO, Muga MA, Chou Y-J, Hsu Y-HE, Huang N, Chien L-Y. Associations in the continuum of care for maternal, newborn and child health: a population-based study of 12 sub-Saharan Africa countries. BMC Public Health. 2016;16(1):414. doi:10.1186/s12889-016-3075-0
63. Adedire EB, Ajayi I, Fawole OI, et al. Immunisation coverage and its determinants among children aged 12–23 months in Atakumosa-west district, Osun State Nigeria: a cross-sectional study. BMC Public Health. 2016;16(1):1–8. doi:10.1186/s12889-016-3531-x
64. Asnake M, Lamessa D, Ayantu K, Zemedu A. Determinants of incomplete childhood vaccination among children aged 12–23 months in Gambela region, southwest Ethiopia: a case control study. Ethiop J Health Sci. 2021;31(1):63–72.
65. Geweniger A, Abbas KM. Childhood vaccination coverage and equity impact in Ethiopia by socioeconomic, geographic, maternal, and child characteristics. Vaccine. 2020;38(20):3627–3638. doi:10.1016/j.vaccine.2020.03.040
66. Krausé SS, Minnie CS, Coetzee SK. The characteristics of compassionate care during childbirth according to midwives: a qualitative descriptive inquiry. BMC Pregnancy Childbirth. 2020;20(1):304. doi:10.1186/s12884-020-03001-y
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.