Back to Journals » Clinical Ophthalmology » Volume 20
Chemical and Thermal Ocular Burns in Children: A Retrospective Single-Center Study of Etiology, Clinical Characteristics, and Outcomes
Authors Toruńska E ![]() , Engelgardt P, Szwajkowska M, Krzyżanowski MT
, Engelgardt P, Szwajkowska M, Krzyżanowski MT
Received 1 April 2026
Accepted for publication 26 May 2026
Published 25 June 2026 Volume 2026:20 613824
DOI https://doi.org/10.2147/OPTH.S613824
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Ewa Toruńska,1 Piotr Engelgardt,1 Maria Szwajkowska,2 Maciej Tomasz Krzyżanowski1
1Department of Pathomorphology and Forensic Medicine, Faculty of Medicine, University of Warmia and Mazury in Olsztyn, Olsztyn, Poland; 2Department of Head and Neck Surgery in the Field of Ophthalmology of the Regional Specialized Children’s Hospital in Olsztyn, Olsztyn, Poland
Correspondence: Ewa Toruńska, Department of Pathomorphology and Forensic Medicine, Faculty of Medicine, University of Warmia and Mazury in Olsztyn, al. Warszawska 30, Olsztyn, 10-082, Poland, Email [email protected]
Background: Ocular burns represent an ophthalmic emergency that can result in extensive damage and long-term visual impairment. The objective of this study was to compare the characteristics of chemical and thermal ocular burns in children.
Methods: The retrospective review of medical records from 2016– 2023 was conducted in the Regional Specialized Children’s Hospital in Olsztyn, Poland. The study included patients up to 18 years old admitted to the hospital with ocular burns. The cases were divided based on burn type – chemical/thermal. The visual impairment was divided according to the ICD-10. A detailed comparative analysis of injuries by burn type was then performed.
Results: Ocular burns occurred most frequently in children under 5 years old and over 15 years old. Most cases involved chemical burns (17 cases – 70.83%), with predominance of alkalis (8 cases – 47.06%). Cigarettes were the most common cause of thermal burns. The most severe cases, in which visual acuity was assessed as moderate and severe, involved thermal burns in children aged 15– 18 years. The conjunctival irrigation was not performed in most cases including visual impairment.
Conclusion: More severe visual impairment was observed in selected cases of thermal burns, while documentation of early irrigation was often absent among children with decreased visual acuity. The interpretation is limited by the small sample size, retrospective design, and incomplete follow-up data.
Keywords: ocular burn, chemical burns, thermal burns, visual impairment, children
Introduction
Ocular burns are a diverse group of ocular injuries, especially in pediatric populations, often resulting from children’s creativity and their immaturity.1 Young children are mostly unaware of the potential danger and eagerly reach for previously unknown items found in home cabinets. While injuries in children typically occur in the home environment, adult injuries most commonly occur in the workplace.2 Burns most often result in damage to the ocular protective apparatus and anterior segment. Reflexive eyelid closure, Bell’s sign, and turning the head away from the source of injury can limit tissue damage.3 Most studies indicate that ocular burns occur more frequently in males, both in the pediatric and adult populations.2,4,5 Among the causes of eye burns, we can generally distinguish chemical, thermal, and biological burns.6 The most common are chemical burns, which can be divided into those caused by alkaline and acidic substances. The characteristics of these injuries are determined by their chemical properties.4 Among the youngest children, ocular burns are most commonly caused by alkaline agents – household chemicals, detergents, liquid laundry packets (LLP), or chuna (calcium hydroxide).5–7 Overall, alkalis penetrate deeper than acids because of the liquefactive necrosis. Although strong acids may penetrate and damage deep tissue like alkali, the corneal epithelium protects against weaker acids, causing coagulation necrosis.8 Among alkali chemicals, ammonia has the fastest penetration rate, causes the most severe ocular burns, and thus is commonly used in assault.9 After severe ocular burns, restoration of the cornea may never occur. While the regeneration process usually begins minutes after small injuries, a few hours after larger damage, and up to 6 weeks if the basement membrane is destroyed.8 Although the entire limbus is damaged in severe burns, limbal stem cells survive and then undergo gradual attrition, but their initial survival allows the healing process. It is worth mentioning that the retina is not destroyed directly by chemical agents. Inflammation limited to the anterior segment tissues causes pro-inflammatory cytokines to be released, which diffuse to the posterior segment, destroying the retina.3
However, regardless of the chemical structure, prolonged contact of these substances with the ocular surface affects the severity of eye damage. Therefore, recognition and prompt intervention by eye irrigation might successfully reduce long-term complications and provide better visual outcomes.5 Nevertheless, published studies suggest that pediatric patients experience worse final visual outcomes following ocular burns compared with adults, primarily as a result of delayed examination and the requirement for irrigation under general anesthesia.7
In contrast to chemical injuries, thermal ocular burns are most often described as a part of facial burns or life-threatening injuries rather than direct eye injury.10 According to the literature data, thermal injuries constitute 17% of all eye burns in children.7 Most commonly these injuries are caused by fireworks, flames and hot liquids.6 As with chemical burns, the time of exposure to the causative agent in thermal injury affects the extent of the damage. Moreover, in the case of hot liquids, their chemical properties also determine the nature of the injury. Greases and oils are more adhesive than water-based fluids and therefore destroy deeper tissues. In addition, thermal factors affect the skin itself, which means that closing the eyelid may not provide sufficient protection for the eyeball.8
Furthermore, the literature describes burns resulting from physical factors – sometimes classified as thermal. (electrical, microwave, ultraviolet radiation) and biological factors. Biological factors most often refer to animals, plants and insects. Whereas UV radiation (tanning and antibacterial lamps, solar radiation reflected from water or snow) damages the corneal surface, resulting in superficial punctate keratitis. The onset of pain and decrease visual acuity occur after few hours and the long-term prognosis is excellent.6,8
Most available pediatric studies focus primarily on chemical ocular burns, whereas direct comparisons between chemical and thermal mechanisms remain limited. In addition, evidence regarding initial management and visual outcomes in children is heterogeneous, partly because of variable documentation and follow-up. Therefore, the aim of this study is to compare the characteristics of chemical and thermal ocular burns in children in the years 2016–2023 in Poland.
Materials and Methods
Study Design and Data Collection
This study is a continuation of authors’ previous research on pediatric ocular injuries.11 The retrospective review of medical records was conducted in the Department of Head and Neck Surgery in the field of ophthalmology of the Regional Specialized Children’s Hospital in Olsztyn, Poland. The study included patients up to 18 years old, admitted in the years 2016–2023 to the Emergency Department (ED) with ocular burns (T26.0-T26.9 according to ICD-10). The data analyzed were selected based on a prior review of the available literature. This information was then coded in an Excel spreadsheet to de-identify patients. Burn severity was determined based on documented ophthalmological findings at the time of presentation. Because documentation was retrospective and not standardized across cases, some variables, including irrigation details and monitoring results, were incomplete. Missing or undocumented information was coded as unknown and not imputed. We extracted information about the gender, age of patients, diagnosed decrease in visual acuity and presenting symptoms, the need for hospitalization, the cause of the burn, the place of the event, the time interval between the burn and admission to the hospital, as well as whether ocular irrigation was performed and whether a follow-up visit was needed and what treatment was applied. Early irrigation was defined pragmatically as any caregiver-reported irrigation performed before hospital presentation. The exact timing, duration, and type of fluid were usually not documented; therefore, irrigation data should be interpreted cautiously. Patients with facial and body burns who had eyelid burns but no ophthalmologic complications were excluded from this analysis. These patients were seen in the emergency and surgical departments. Patients were divided into 4 age groups: 1–4, 5–9, 10–14, 15–18. The method of measuring visual acuity depended on the child’s age. In the youngest, preverbal children, visual acuity was assessed based on the ability to fixate on a toy and follow it. Older children, but those with anxiety or preverbal, were assessed using the LEA 3-meter test. In other children, visual acuity was assessed using Snellen charts (with pictures, numbers, and letters). In Poland, results are reported using the decimal system. Visual acuity loss was divided according to ICD-10 – WHO into categories: 0 (mild or no visual impairment; ≥0.3), 1 (moderate visual impairment; ≥0.1), 2 (severe visual impairment; ≥0.05), 3 (blindness; ≥0.02), 4 (blindness; light perception), 5 (blindness; no light perception). Burn-causing factors were divided into chemical and thermal. Then, a comparative analysis of chemical and thermal burns was performed.
To objectively assess the severity and prognosis of acute ocular burns we used the Roper-Hall classification and Dua classification,12 which classify the severity of burn effects based on corneal haze (Roper-Hall classification), limbal ischemia (both scales), and conjunctival irritation (Dua classification). The assessment according to both classifications was performed retrospectively by the authors based on information available in the medical records. Both classifications are summarized in Tables 1 and 2.
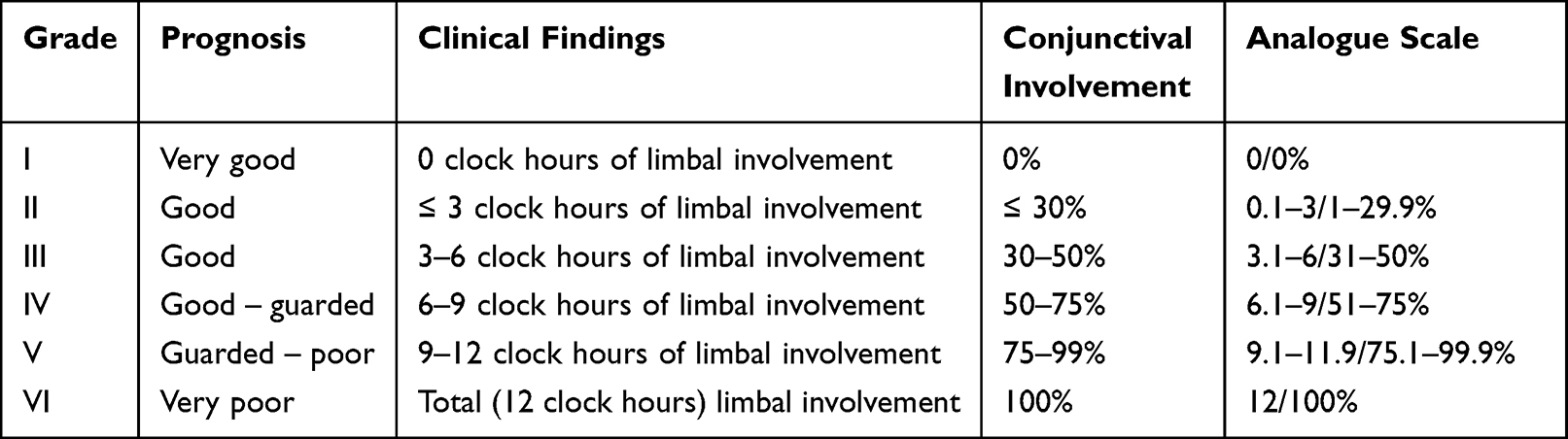 |
Table 1 Dua Classification |
 |
Table 2 Roper-Hall Classification |
Data Analysis
Data analysis, calculations and graphs were performed in Excel spreadsheet and statistical package R 4.4.1. Descriptive statistics used standard deviation (SD) and interquartile range (IQR). Due to the small size of the group, detailed statistical analysis was not performed.
Ethics
The authors declare that the study was conducted in accordance with applicable ethical guidelines and local regulations. Owing to the retrospective nature of the study, informed consent to participate was not required. All patient data were anonymized prior to analysis, and confidentiality of patient information was maintained throughout the study. The study protocol was approved by the Local Bioethics Committee of the University of Warmia and Mazury in Olsztyn (Decision No. 39/2024) on December 5, 2024. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Results
Demographics
Based on the analysis of medical records of the Emergency Department (ED), 24 (4.40%) cases of eye burns in children were detected in the years 2016–2023, while the number of all admissions for eye injuries amounted to 546 cases in this period (Figure 1).
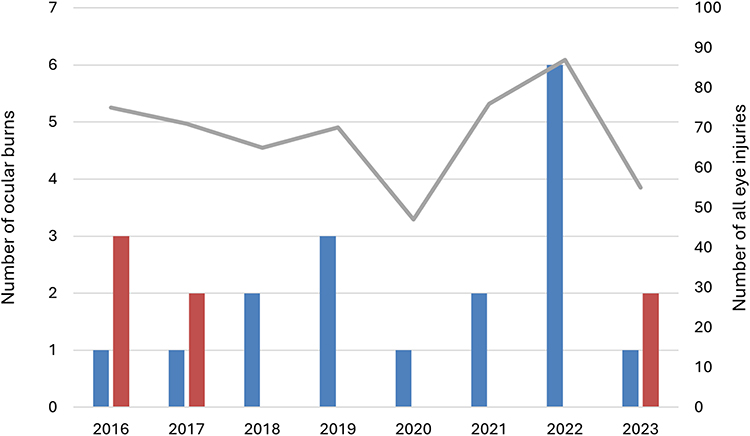 |
Figure 1 The annual number of chemical and thermal ocular burns in relation to the total number of eye injuries in children admitted to the Regional Specialized Children’s Hospital in Olsztyn, Poland. Blue – Chemical ocular burns. Red – Thermal ocular burns. Grey – All eye injuries. |
Only a slight overrepresentation of boys was observed – 13 cases (54.17%), and the trend regarding gender was visible in both thermal and chemical burns. The median age was 9.5 (IQR: 15–4), while the highest number of patients was observed in the youngest and oldest age groups (Table 3). In the case of thermal burns, patients were only from these age groups (1–4 and 15–18 years), (Figure 2).
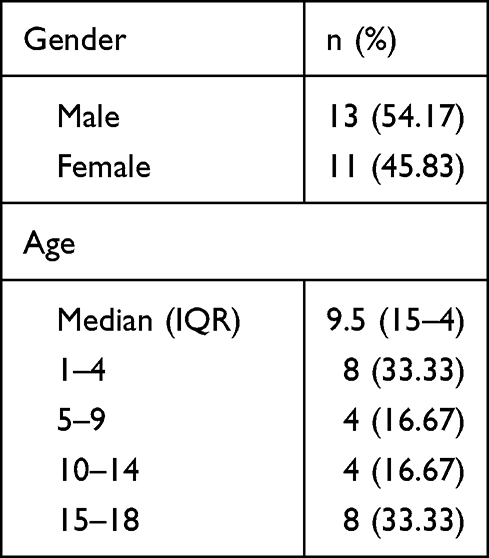 |
Table 3 Demographic Data |
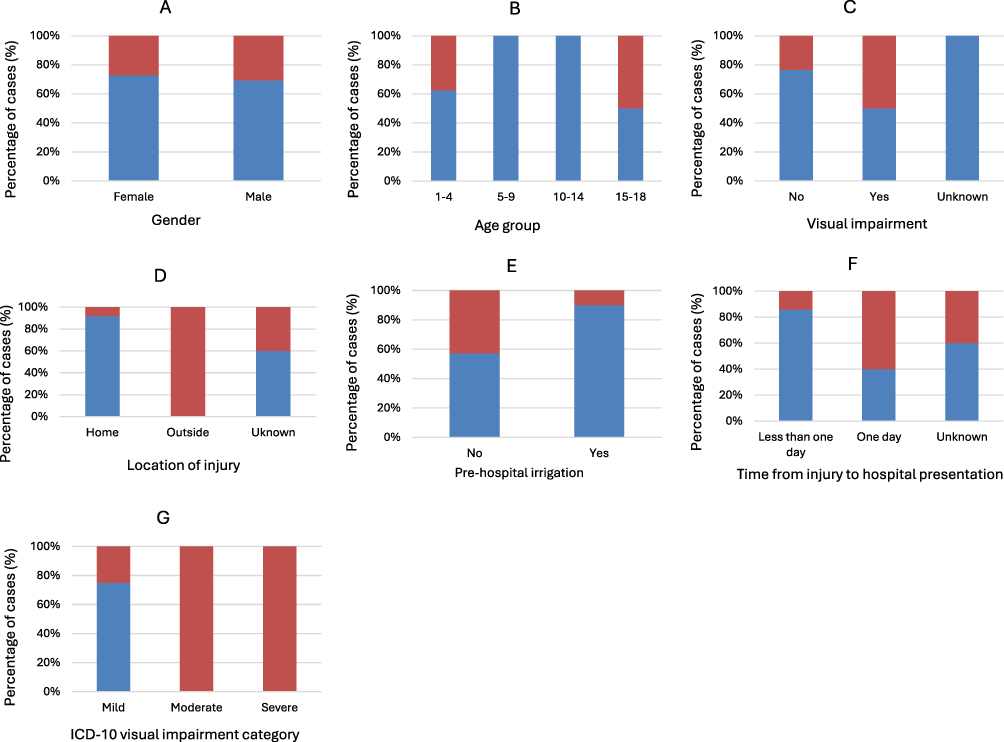 |
Figure 2 Comparison of the characteristics of the chemical ocular burns and thermal ocular burns in relation to the gender (A), age groups (B), visual impairment (C), location of injury (D), pre-hospital irrigation (E), time from injury to hospital presentation (F) and ICD-10 visual impairment category (G). Blue – Chemical ocular burns. Red – Thermal ocular burns. |
In half of the cases, the burn occurred at home, while, due to the short interview, in 10 cases, there was no information about the place of the incident. Most often, in 58.33% of cases, children were taken to the emergency room (ER) on the same day. However, these were predominantly cases of chemical burns, as caregivers reported children with thermal burns to the hospital on the day of the incident in only two cases, and on the following day in three cases. In 5 (20.83%) cases of all burns, no information about the time of the accident was found, however the analysis of symptoms allows us to assume that the incident occurred shortly before reporting to the hospital (Figure 2).
Causative Agents
In 17 cases (70.83%), the cause of the injury was chemical burns. Most often caused by alkaline substances (47.06%). In four patients, it was a liquid laundry packet, in three household detergents, and in one case lime. Among the injuries caused by acidic substances, in one case, there was an assault with pepper spray. As revealed by the data obtained from the interviews, this was the only non-accidental injury in this study. In the ophthalmological examination immediately after the assault, a decrease in vision of 0.5 in both eyes was described, but there is no information about a follow-up visit in this case. From the remaining chemical substances, 5 cases of burns with glue were distinguished. It emerged from the interview that all thermal burns were accidental. Of the 7 thermal burns, unintentional cigarette burns dominated. In this study, UV-related injury was included in the thermal/physical injury category because physical ocular burns, including ultraviolet radiation, are frequently grouped with thermal mechanisms in emergency medicine classifications. Data indicate that LLPs are most frequently used by young children (ages 1–4), while glue is most frequently used by older children. Cigarette burns occurred primarily among teenagers (ages 15–18). A detailed characteristic of the causes of burns is presented in Table 4 and Figures 3.
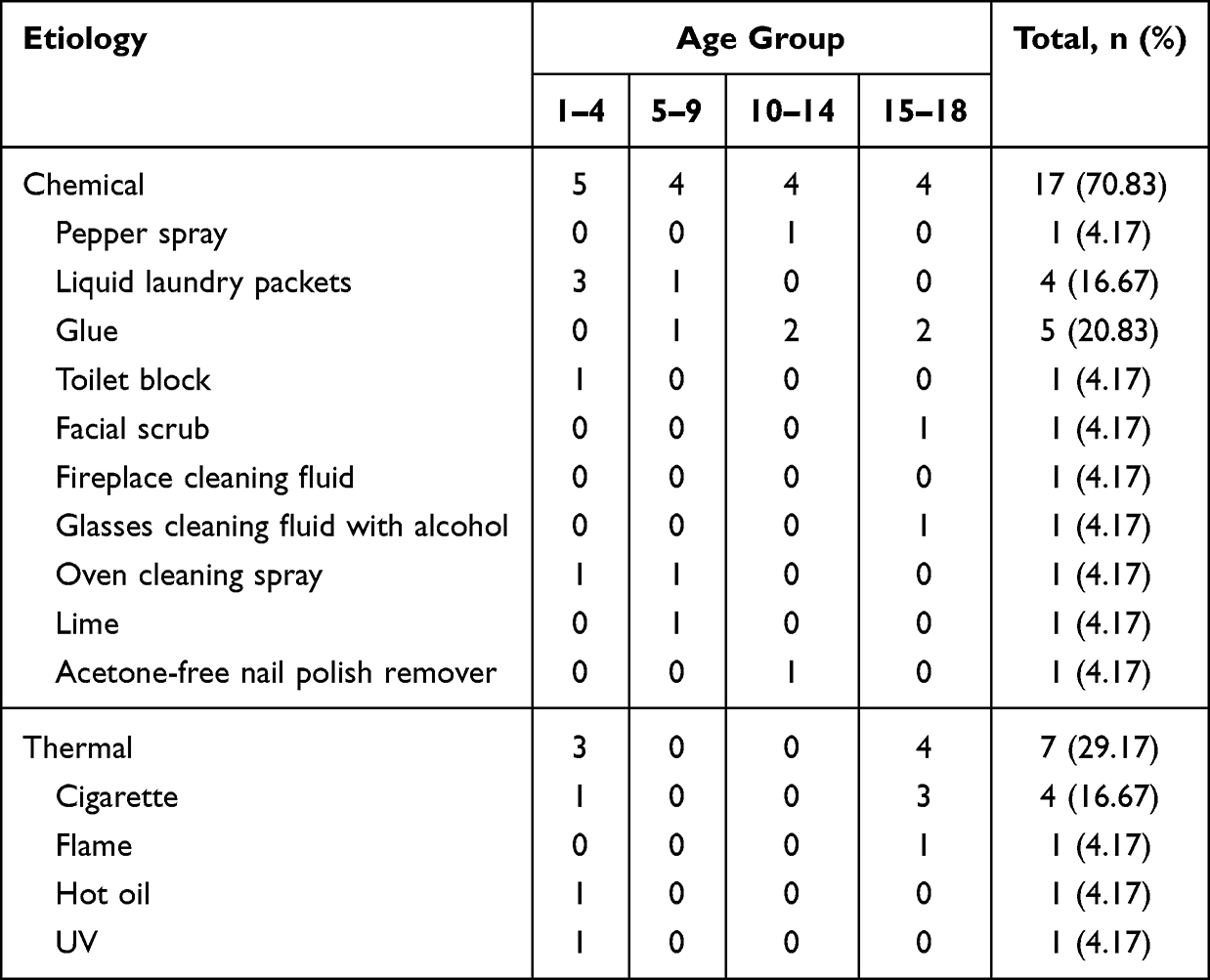 |
Table 4 Summary of Burn Etiology and Age of the Child (n=24) |
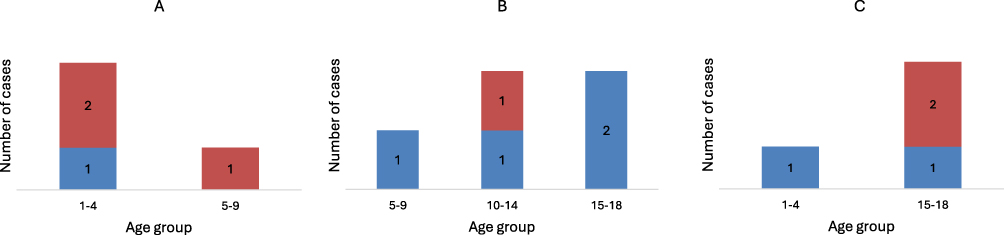 |
Figure 3 Number of cases of ocular burns caused by liquid laundry packets (A), glue (B), cigarette (C), depending on gender and age groups. Blue – Chemical ocular burns. Red – Thermal ocular burns. |
Clinical Findings and Grading of Severity
Slightly more injuries concerned the left eyeball – 11 cases (45.83%). In 9 (37.5%) cases, the right eyeball was affected, and in 4 (16.67%) both eyeballs. The most common finding on ophthalmological examination was corneal erosion, observed in 11 cases, and eye irritation/conjunctival redness, noted in 19 cases. On the other hand, a foreign body was found and removed in 3 children – glue in 2 cases, and a grain of sand in one case. The detailed list of symptoms presented in Table 5 refers to all the symptoms observed, which in some cases occurred together, so their total exceeds the number of cases.
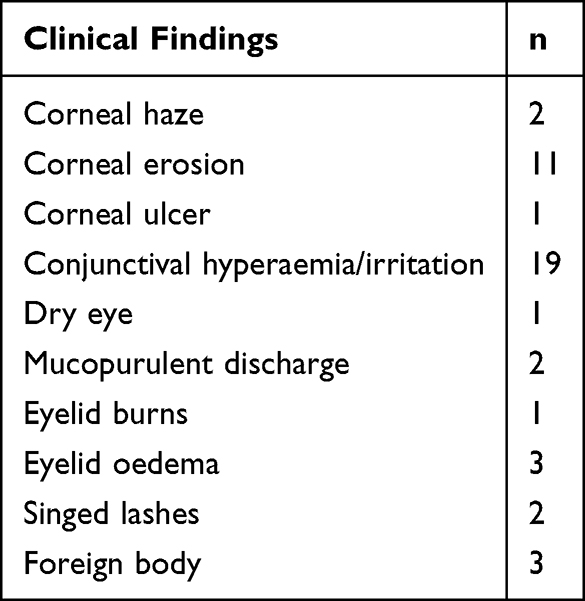 |
Table 5 Results of Ophthalmological Examination After Ocular Burns |
In 6 (25%) cases, visual impairment occurred (visual acuity in the examination: 0.1; 0.4; 0.4; <0.1; 0.8; 0.5), while in one case, it was not possible to examine a child due to significant pain. Four patients experienced a decrease in visual acuity of degree 0 according to the ICD-10 classification, ie a decrease in vision equal to or less than 0.3. One case referred to an injury in the mechanism of thermal burn – igniting with cigarette embers; while the remaining cases were in the mechanism of chemical burn (glue, nail polish remover without acetone, pepper spray). In individual cases, visual acuity was assessed as grade 1 (moderate – visual impairment: 0.1–0.3) and 2 (severe – visual impairment: 0.05–0.1). In both cases, these injuries were caused by thermal burns. The moderate burn occurred after being ignited by a cigarette burn, and the severe burn was caused by a flame, after a cool box had been thrown into the fire and exploded. Moreover, all cases of thermal burns associated with decreased vision occurred in children aged 15–18 years. Among all cases in which visual impairment occurred, only after a burn in contact with nail polish remover, early ocular irrigation was performed. In the remaining cases, there was no such information (Table 6 and Figure 2). The remaining children (70.83%) had normal visual acuity.
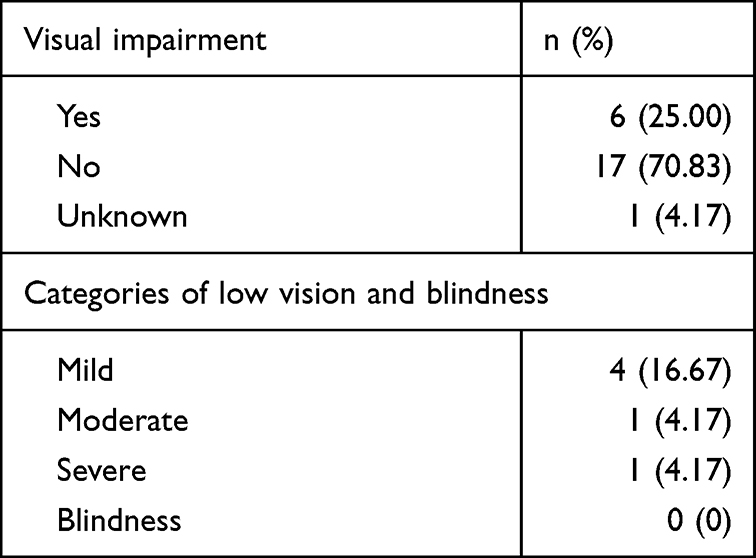 |
Table 6 The Number of Children with Visual Impairment According to the ICD-10 Codes |
The severity of ocular burns was assessed according to the Roper-Hall classification and Dua classification. Among chemical burns assessed using the Roper-Hall scale, only one case was classified as grade IV (5.88%), two as grade III (11.76%), and the remaining cases were grades I and II with a good prognosis. According to the Dua scale, three cases (17.65%) were classified as grade III, and the remaining cases were classified as lower grades. Among the thermal burns, one patient (14.29%) was classified as grade IV using the Roper-Hall scale, three as grade III (42.86%), and the remaining patients (42.86%) were classified as grades I and II. According to the Dua scale, four patients (57.14%) were classified as grade III.
Management
In 10 (41.67%) cases, caregivers declared early ocular irrigation after a burn, without additional explanation, how much time they spent on it, or what substance they used. However, only in one case irrigation was performed after a thermal burn (Figure 2). Of all 6 cases in which a decrease in vision was diagnosed, in 5 there was no information about early irrigation, but the result was not statistically significant. Detailed data regarding the above information are presented in Table 7.
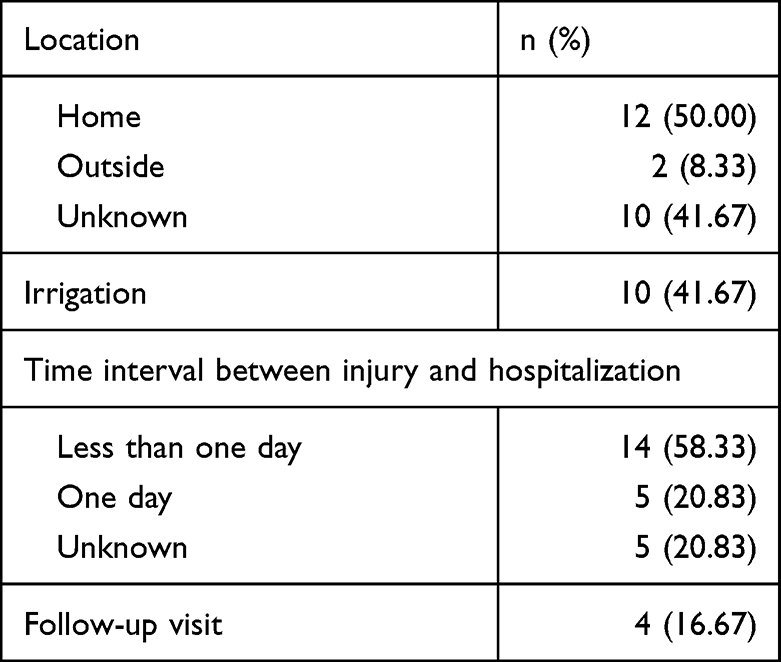 |
Table 7 Details of Injury Location, Irrigation, Time Between Injury and Hospitalization, and Follow-Up Visit |
A follow-up visit after the injury took place in only 4 cases, of which three children suffered chemical burns. A 2-year-old child required admission for a developing corneal ulcer secondary to a chemical burn caused by a LLP, associated with poor hygiene and noncompliance with medical recommendations. One case of follow-up visit involved a thermal burn, which was a consequence of an explosion after throwing a cool box into a fire. Visual acuity on admission was <0.1 in the right eye and 0.5 in the left eye (severe). During a follow-up visit performed 4 days after the injury, partial improvement in vision was observed, assessed at 0.3 in the right eye and 1.0 in the left eye. Further check-ups were recommended for the patient at the district clinic. In one case, despite the lack of visual impairment in the examination immediately after the injury, there was a deterioration in vision (0.33) observed during a follow-up visit two days after the burn. However, no information was found about the next check-up in the case of this patient. It should be noted that each patient received information about the need to report to an ophthalmological clinic in the event of a deterioration in their health, but it was not possible to check whether such a visit took place in a clinic other than the place where this examination was conducted.
One child required hospital admission for ongoing treatment. In all other cases, patients were instructed to continue treatment at home. In 22 cases, healing and moisturizing drugs (including dexpanthenol, hyaluronic acid, trehalose) were used. In 19 cases – antibiotics or chemotherapeutics, in 5 cases – glucocorticosteroids, in 2 cases tropicamide, and once nonsteroidal anti-inflammatory drugs in the form of eye drops. Most often, combined preparations were used or the simultaneous use of several of the above drugs was recommended. The hospitalized child received more intensive local treatment and intravenous antibiotic therapy.
Discussion
Our data show that ocular burns occur most frequently in the youngest and oldest age groups. Alkalis, including LLPs, were most often responsible for chemical burns, while cigarettes were the most common cause of thermal burns. The most severe cases, in which visual acuity was assessed as moderate and severe, involved thermal burns. In less than half of the cases, caregivers reported irrigation, but this occurred in only one case of thermal burn. Due to the small size of the group, detailed statistical analysis was not performed.
The mechanism of eye injury in children is strongly influenced by age, while regional, social, and cultural contexts further modulate the nature and circumstances of these injuries.11 Depending on the literature, ocular burns constitute between 2.3% and 4% of all eye injuries in children.13,14 These data are consistent with our findings, in which ocular burns accounted for 4.40% of all eye injuries. Although few publications compare chemical and thermal burns, available data indicate that chemical burns account for approximately 57% of cases (Alkali: 45%; Acid: 12%), while thermal burns represent about 17% (with the remaining cases comprising other types of burns).7 Our study demonstrates a similar trend, showing a predominance of chemical burns, albeit with a different distribution: chemical burns constituted 70.83% of cases, whereas thermal burns accounted for 29.17%. According to the data, burns occur most frequently in the youngest age group between 1 and 5 years.5,15,16 Although Ahmmed et al concluded that young working men are the most exposed group to chemical eye injuries, they also highlighted children under five years old as another high-risk group.4 In our study, the majority of incidents occurred in the home setting, which is consistent with findings reported in the literature.17,18
In contrast to the other authors,2,5,18 we observed just a minimal predominance of males. Furthermore, the most numerous were the youngest (1–4 years old) and the oldest (15–18 years old) group of patients. While, according to the literature, ocular burns occur the most frequently in the youngest children.4,5 Usually, burns are caused by chemicals, mostly alkali,2,4,7 which was also observed in our study. Moreover, Haring et al observed differences in the chemical burn (alkali vs acidic) depending on age. Alkaline burns were more common in children under 3 years old than in adults.19 Interestingly, Ahmmed et al noted that the causative agents of ocular burns are similar in children and patients over 60 years old, which might result from less exposure to occupational injuries.4
LLPs are responsible for 23.53% of all chemical ocular burns among our patients. Other studies indicate that LLPs are a common cause of ocular burns in children; for example, they accounted for 67% of cases in the study by Breazzano et al20 Reynolds et al, using data from the National Poison Data System, reported 73942 cases of accidental LLPs exposure in children younger than 6 years between 2012 and 2018.21 The number of ocular burns increased after laundry detergent pods were introduced to the shop.20 According to the literature, the amount of admissions to the poison center caused by LLPs is 5 times greater than traditional laundry detergents. LLPs are associated with serious medical outcomes more frequently than traditional detergents, which may be attributable to their higher chemical concentrations.11,21 Moreover, some authors indicate that ocular damage after LLPs burn might predispose to future corneal diseases.20 There is a belief that LLPs’ color, size, and consistency make children eagerly reach for them. Nevertheless, previous studies have shown that the aforementioned characteristics of the pods have no significant role in children’s attention.22
Another type of causative substance is glue, which, depending on the purpose, has a different chemical structure conditioning different effects on human tissues. Glue mostly causes inflammation and stuck to the eyelashes and eyelids.17 We observed 5 cases of ocular burns caused by glue. All of these children used cyanoacrylate glues, which are characterized by very fast action. In one of these cases, we noted a decrease in visual acuity of 0.4 (mild). Ocular burns caused by glue occur frequently among children, especially in the absence of adult supervision. Commonly results in conjunctival congestion, corneal abrasion, or sticking to the eyelashes and eyelids.8,17 The chemical structure of cyanoacrylate causes bonding only dry surfaces. Hence, out of the severe inflammation, chemical conjunctivitis, and keratitis, glue undergoes rapid polymerization on dry eyelid margins, causing sticking these surfaces.17 In only one case, we found information about immediate ocular irrigation. Whereas, ocular irrigation is the most important step in first aid after glue burns, delaying glue condensation, chemical tarsorrhaphy, and thus ocular injury.
Direct thermal ocular burns are a rare medical finding, but they are generally responsible for the most severe ocular injury. The diagnosis of thermal ocular burns is frequently delayed because they are usually associated with life-threatening injuries.6 Although the literature currently reports cases of eye burns caused mainly by e-cigarettes, some studies also highlight non-accidental eye burns associated with traditional cigarettes,23 as well as entirely accidental injuries resulting from inattention on the part of both children and their parents.24 We found 7 cases of thermal burns, mostly caused by traditional cigarettes. Only in one case, parents declared prompt ocular irrigation. In this exploratory study thermal burns were overrepresented among the more severe presentations. Although eye irrigation was not performed in most severe cases, causality cannot be inferred due to the small sample size, retrospective study design, and incomplete follow-up. Furthermore, decreased vision in cases of thermal burns was observed exclusively in patients aged 15–18 years. However, the results were not statistically significant. According to the literature, first aid after thermal ocular burns involves eye irrigation for 15 minutes. Despite the scientific discussion about differences between specialized irrigation fluids, authors agree, that irrigation should never be delayed by lack of an appropriate solution, as tap water can be used for irrigation.25,26
Although the treatment of chemical and thermal ocular burns is similar, we can distinguish the different main goals of the therapy of these injuries. While after the thermal burns, irrigation helps to cool the eyeball, one of the goals of treating the chemical burns is to restore the physiologic pH of the eye.8,26 While tap water is recommended in first aid at home, it is not the most suitable liquid. According to the research, buffering solutions bind the alkalis and acids and therefore should be used to reduce the pH level.9 Contrary to thermal burns, irrigation after chemical exposure should be continued until the pH neutralizes; thus, some authors recommend irrigation with at least 1 L of fluid for at least 30 minutes. Topical anesthesia is often controversial because eye drops can increase chemical penetration into the anterior chamber. On the other hand, anesthesia reduces discomfort and provides more successful irrigation. Hence, some researchers recommend immediate irrigation and then using anesthetic to continue intensive flushing. It is recommended to check pH after 30 minutes, because especially alkaline solutions can dissolve slowly, increasing pH, so further flushing might be required.8,9 In our study, 41.67% of children had eye irrigation. Unfortunately, we have no accurate information regarding the method, time, or type of solution used for irrigation. Literature indicates that many patients who did not receive immediate irrigation had severe eye injuries.5 The analysis of our study shows that out of 6 patients in whom we found a decrease in visual acuity, in 5 of them, there was no information about immediate eye irrigation. In addition, the long time between injury and hospitalization contributes to the severity of the damage and worse visual or anatomical outcomes.2,5 However, Al-Ghadeer et al noted that the risk of severe visual impairment one year after treatment was not significantly different between patients who received first aid and those who did not.18 Other studies indicate that children, particularly younger ones, may develop amblyopia following ocular injury as a result of reduced or absent visual stimulation of the affected eye.1 The severity of damage after ocular burns is different depending on studies. Al-Ghadeer et al reported that 27% of children had grade IV in the Roper-Hall classification and 13% of them had grade III. What is more, the risk of blindness in eyes with grades III and IV was significantly higher than those with grades I and II.18 In the other study, 70.1% of patients had grades III and IV in ocular chemical injury.5 Whereas Kate et al reported, that 67% of children had grade I and 16% grade IV.7 In our study only one case of chemical burns was classified as grade IV (5.8%) and two as grade III (11.7%) according to the Roper-Hall classification. Among the thermal burns, one patient (14.2%) was classified as grade IV and three as grade III (42.9%). We noted that one of our patients, a 2-year-old girl, required admission for a developing corneal ulcer secondary to a chemical burn caused by a LLP, associated with poor hygiene and noncompliance with medical recommendations. However, in no case was there a need for surgical treatment. In contrast to our results, previous studies have described the need for surgical treatment in patients with ocular burns, such as limbal stem cell transplantation, amniotic membrane transplantation, and symblepharon release.7,17
This study has several limitations. The small sample size limited the ability to conduct statistical analyses in many cases. The vast majority of patients did not return for follow-up visits, making it impossible to assess long-term treatment outcomes. This observation may reflect the large geographic size of the province in which our hospital operates, leading to the treatment of many pediatric patients in emergency departments of other district hospitals. Additionally, the study period overlapped with the COVID-19 pandemic and lockdowns, during which interpersonal contact was restricted. Data were collected retrospectively, which limits access to much potentially relevant information. Furthermore, interviews conducted in the Emergency Department typically include only a brief description of the patient’s condition, aimed at prompt diagnosis and initiation of treatment. This level of information proved insufficient for a reliable comparison with results reported in the literature. Furthermore, the retrospective nature of the study may have contributed to heterogeneity in documenting the circumstances of the injury. The possibility of data entry errors, which could have led to the inadvertent exclusion of some patients from the analysis, should also be considered.
Conclusion
This retrospective, single-center study presents a descriptive comparison of chemical and thermal ocular burns in children. Chemical burns were more common, whereas thermal burns were overrepresented among the more severe cases in this cohort. In most cases, documentation of prehospital irrigation was missing, resulting in decreased visual acuity, although causality cannot be inferred due to the small sample size, retrospective study design, and incomplete follow-up period. Nevertheless these findings highlight the need for public education on first aid for ocular burns, particularly prompt ocular irrigation and early medical assessment. However larger prospective studies are needed to determine their impact on long-term visual outcomes.
Abbreviations
LLP, liquid laundry packets; ED, Emergency Department; ER, Emergency room.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The authors declare that the study complies with the ethical guidelines and applicable local law. The study was designed as a retrospective. Therefore, consent to participate was not required. This study was approved by the local Bioethics Committee of the University of Warmia and Mazury in Olsztyn – Decision No. 39/2024 – on December 5, 2024. The present study was conducted following the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funded by the Minister of Science under “the Regional Initiative of Excellence Program”.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Kański JJ, Turno-Kręcicka A, Barć A. Choroby oczu u dzieci. Górnicki Wydawnictwo Medyczne; 2002.
2. Korkmaz I, Palamar M, Egrilmez S, Yagci A, Barut Selver O. Ten years of pediatric ocular chemical burn experience in a tertiary eye care center in Turkey. Eye Contact Lens. 2022;48(4):175–12. PubMed PMID: 35296629. doi:10.1097/ICL.0000000000000858
3. Dua HS, Shu D, Ting J, Al A, Dalia S. Chemical eye injury: pathophysiology, assessment and management. Eye. 2020;34:2001–2019. doi:10.1038/s41433-020-1026-6
4. Ahmmed AA, Ting DSJ, Figueiredo FC. Epidemiology, economic and humanistic burdens of Ocular Surface Chemical Injury: a narrative review. Ocul Surf. 2021;20:199–211. PubMed PMID: 33647471. doi:10.1016/j.jtos.2021.02.006
5. Vajpayee RB, Shekhar H, Sharma N, Jhanji V. Demographic and clinical profile of ocular chemical injuries in the pediatric age group. Ophthalmology. 2014;121(1):377–380. PubMed PMID: 23948464. doi:10.1016/j.ophtha.2013.06.044
6. Ratnapalan S, Das L. Causes of eye burns in children. Pediatr Emerg Care. 2011;27(2):151–156. PubMed PMID: 21293228. doi:10.1097/PEC.0b013e318209f08c
7. Kate A, Sharma S, Yathish S, et al. Demographic profile and clinical characteristics of patients presenting with acute ocular burns. Indian J Ophthalmol. 2023;17(1):1. PubMed PMID: 10071898. doi:10.4103/ijo.IJO
8. Spector J, Fernandez WG. Chemical, thermal, and biological ocular exposures. Emerg Med Clin North Am. 2008;26(1):125–136. doi:10.1016/j.emc.2007.11.002
9. Bizrah M, Yusuf A, Ahmad S. An update on chemical eye burns. Eye. 2019;1362–1377. doi:10.1038/s41433-019-0456-5
10. Bouchard CS, Morno K, Perkins J, McDonnell JF, Dicken R. Ocular complications of thermal injury: a 3-year retrospective. J Trauma - Injury Infect Crit Care. 2001;50(1):79–82. PubMed PMID: 11231674. doi:10.1097/00005373-200101000-00014
11. Toruńska E, Engelgardt P, Szwajkowska M, Krzyżanowski M. Epidemiology of pediatric ocular injuries in Poland: cross-sectional study. BMC Ophthalmol. 2025;25:698. doi:10.1186/s12886-025-04529-3
12. Gupta N, Kalaivani M, Tandon R. Comparison of prognostic value of Roper Hall and Dua classification systems in acute ocular burns. Br J Ophthalmol. 2011;95(2):194–198. PubMed PMID: 20805137. doi:10.1136/bjo.2009.173724
13. Matsa E, Shi J, Wheeler KK, McCarthy T, McGregor ML, Leonard JC. Trends in us emergency department visits for pediatric acute ocular injury. JAMA Ophthalmol. 2018;136(8):895–903. PubMed PMID: 29879287. doi:10.1001/jamaophthalmol.2018.2062
14. Ferguson RA, Justin M, Mbchb S, Mckelvie J. New Zealand childhood ocular trauma study: analysis of 75 601 cases of ocular injury from 2007 to 2016. Clin Experiment Ophthalmol. 2019;47:718–725. doi:10.1111/ceo.13489
15. Patel PS, Uppuluri A, Zarbin MA, Bhagat N. Epidemiologic trends in pediatric ocular injury in the USA from 2010 to 2019. Graefes Arch Clin Exp Ophthalmol. 2022;260(4):1387–1394. PubMed PMID: 34536117. doi:10.1007/s00417-021-05368-w
16. Mancebo JG, García-Loygorri CF, Romero AI, López PV, García AR. Ocular trauma in the pediatric emergency departments, characteristics and risk factors of immediate sequelae. Anales de Pediatría. 2021;94(3):161–172. doi:10.1016/j.anpede.2020.07.008
17. Malepati N, Sharma S, Kate A, Basu S, Shanbhag SS. Original Article Clinical profile and management of ocular superglue injuries: case series and review of literature. Indian J Ophthalmol. 2024;72(2):587–591. doi:10.4103/IJO.IJO
18. Al-Ghadeer H, Al Amry M, Aldihan KA, Alobaidan OS, Alqahtani GMS, Khandekar R. Demographic, clinical profile and management outcomes of ocular chemical injuries in Saudi children. Clin Ophthalmol. 2022;16:3247–3255. doi:10.2147/OPTH.S379081
19. Haring RS, Sheffield ID, Channa R, Canner JK, Schneider EB. Epidemiologic trends of chemical ocular burns in the United States. JAMA Ophthalmol. 2016;134(10):1119–1124. PubMed PMID: 27490908. doi:10.1001/jamaophthalmol.2016.2645
20. Breazzano MP, Day HR, Tanaka S, Tran U. Prospective analysis of pediatric ocular chemical burns: laundry detergent pods. J AAPOS. 2018;22(6):426–428. PubMed PMID: 30342182. doi:10.1016/j.jaapos.2018.07.349
21. Reynolds KM, Burnham RI, Delva-Clark H, Green JL, Dart RC. Impact of product safety changes on accidental exposures to liquid laundry packets in children. Clin Toxicol. 2021;59(5):392–399. PubMed PMID: 32960108. doi:10.1080/15563650.2020.1817478
22. Richmond A, Schwebel DC, Morgan CH, et al. The exploration of size and toddler interaction with liquid laundry detergent capsules. PLoS One. 2020;15:1–13. PubMed PMID: 33378406. doi:10.1371/journal.pone.0244481
23. Grałek M, Moll A, Niwald A. Non-accidental injury of vision organ in children. Klinika Oczna. 2021;123(3):103–107. doi:10.5114/ko.2021.110003
24. Man CB, Shah AK, James NK. Smoking still harms those around you: a cigarette burn to a child’s eye. J Plast Reconstruct Aesthetic Surg. 2010;63(3):e296–7. PubMed PMID: 19748841. doi:10.1016/j.bjps.2009.07.035
25. Berry J, Ashley J, Jeffery S. Ophthalmological evaluation of facial burns in a regional burns centre. Burns. 2020;46(4):970–973. PubMed PMID: 31771901. doi:10.1016/j.burns.2019.10.025
26. Schrage NF, Struck HG, Gerard M. Empfehlungen zur Akutbehandlung von Verätzungen und Verbrennungen der Augen und Lider. Ophthalmologe. 2011;108(10):916–920. PubMed PMID: 22037724. doi:10.1007/s00347-010-2252-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.