Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Characterizing Acute Pulmonary Embolism After Off-Pump Coronary Artery Bypass Surgery Using a Predictive XGBoost Model
Authors Zhang M ![]() , Sheng H, Liu J, Zhang W, Chang C, Ma Y, Yu Q, Li Y, Peng H
, Sheng H, Liu J, Zhang W, Chang C, Ma Y, Yu Q, Li Y, Peng H
Received 29 March 2026
Accepted for publication 3 July 2026
Published 9 July 2026 Volume 2026:19 612850
DOI https://doi.org/10.2147/JMDH.S612850
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Mingna Zhang,1 Hongmei Sheng,1 Jiayu Liu,1 Wei Zhang,1 Chao Chang,2 Yanhe Ma,3 Qihong Yu,1 Yi Li,1 Haiying Peng1
1Department of Respiratory and Critical Care Medicine, Tianjin Chest Hospital, Tianjin, 300222, People’s Republic of China; 2Department of Cardiac Surgery, Tianjin Chest Hospital, Tianjin, 300222, People’s Republic of China; 3Department of Imaging, Tianjin Chest Hospital, Tianjin, 300222, People’s Republic of China
Correspondence: Haiying Peng, Department of Respiratory and Critical Care Medicine, Tianjin Chest Hospital, Tianjin, 300222, People’s Republic of China, Email [email protected]
Objective: This study aims to characterize the occurrence of acute pulmonary embolism (APE) after off-pump coronary artery bypass grafting surgery (OPCABG) and develop a predictive model for APE to mitigate adverse events and improve patient prognosis.
Methods: We reviewed the clinical records of 15,259 patients who underwent OPCABG at Tianjin Chest Hospital from May 2015 to May 2025. APE was identified in 228 patients (1.49%), and 458 non-APE controls were included after matching gender and age at an approximate 1:2 ratio. We conducted statistical analyses to characterize the clinical features of APE patients and used LASSO and XGBoost algorithms to build a predictive model for APE. SHAP method evaluated influential prognostic features.
Results: After OPCABG, 49.1% of patients with APE experienced hypoxia and 33.3% had shortness of breath, while 28.5% were asymptomatic. APE was most frequently located in the right superior lobar pulmonary artery (58.8%). Bilateral pulmonary embolism occurred in 29.8% of patients, with 6.14% exhibiting bilateral pulmo-aortic involvement (central PE). APE patients demonstrated a higher prevalence of post-operative elevated D-dimer, deep vein thrombosis, pleural effusion, anemia, and hypoalbuminemia. Using LASSO regression, 36 pre- and post-operative variables were selected for model development. The XGBoost model achieved 91.3% sensitivity (95% CI: 82.5%– 98.2%) and 94.6% specificity (95% CI: 89.1%– 98.9%) in validation dataset, yielding a superior AUC of 97.6%. The SHAP analysis highlighted the contribution of postoperative D-dimer, deep vein thrombosis, the start time of low molecular weight heparin, and preoperative uric acid. While the model demonstrated satisfactory performance in our single-center validation cohort, further external validation in a multicenter setting is essential prior to its broader clinical implementation.
Conclusion: Despite adequate antiplatelet and anticoagulant therapy in clinical practice, APE occurred in 1– 2% of patients. We developed a robust predictive model for APE following OPCABG to identify at-risk patients, optimize outcomes, and ultimately reduce the associated economic burden.
Keywords: acute pulmonary embolism, off-pump coronary artery bypass surgery, ICU anticoagulant therapy, machine learning, XGBoost, risk prediction
Introduction
Acute pulmonary embolism (APE) is a critical and potentially life-threatening complication following various surgical procedures, particularly cardiac surgery. The median incidence of symptomatic and fatal APE post-surgery is 0.6% (range: 0.3–2.9%) and 0.3% (range: 0.08–1.7%), respectively.1 APE independently predicts mortality in cardiac surgical patients.2
Coronary artery bypass grafting (CABG) can be performed via two primary approaches—off‑pump and on‑pump—depending on the use of cardiopulmonary bypass. Off-pump coronary artery bypass grafting (OPCABG) is the standard treatment for left main artery and three-vessel coronary artery disease, offering advantages over conventional on‑pump approach, including myocardial preservation, reduced oxidative stress, and lower renal dysfunction rates.3,4 However, by avoiding contact activation and consumption of platelets induced by cardiopulmonary bypass, OPCABG preserves platelet function and maintains relatively low fibrinolytic activity, leading to a “hypercoagulable‑hypofibrinolytic” state that may predispose patients to graft occlusion and thromboembolic events.5 A routine imaging screening study revealed a significantly higher incidence of APE in the OPCABG group compared with the on-pump group, with an 8% absolute increase.6 Patient age, operative technique, and length of ICU stay were identified as independent predictors of APE. The reported incidence of APE following OPCABG ranges from 0.37% to 6.2%.2,7–9 Fatal APE accounts for approximately 11–20% of unexplained deaths after cardiac surgery, with at least 50% of these cases remaining undiagnosed prior to death.10,11 APE results in longer hospital stays and higher costs.12 Routine anticoagulation and antiplatelet therapy during the perioperative period effectively prevent vascular restenosis and venous thromboembolism, reducing the risk of APE by approximately 50%.1 Therefore, early identification of postoperative APE signs and timely intervention are crucial for improving patient outcomes.
The clinical symptoms and signs of APE are often non-specific.13,14 APE can present as difficulty breathing, chest pain, hemoptysis, or fainting, but many patients remain asymptomatic. Central APE may cause acute and severe dyspnea, while small peripheral APE symptoms can be mild and transient, easily overlooked due to postoperative cardiac pain, dyspnea, and other manifestations of OPCABG. This complicates early detection and diagnosis. Machine learning, a significant branch of artificial intelligence, learns from extensive datasets to predict outcomes for new samples. Its rapid development has the potential to transform clinical practices.15 Machine-learning prediction models improve early risk screening, diagnosis, and prognosis for malignant tumors and estimate the likelihood of cardiovascular disease. They also enhance diagnosis and screening across other medical specialties, including ophthalmology.16–19 Recent investigations have concentrated on predicting postoperative APE or venous thromboembolism following cardiac surgery. A machine learning-based model has been shown to effectively predict venous thromboembolism after cardiac surgery, with both preoperative and postoperative factors contributing substantially to predictive performance.20 Shen et al introduced a generative multi-task representation learning framework, termed surgVAE, which incorporated deep vein thrombosis (DVT)/APE as one of six key postoperative complications.21 Separately, Yu et al developed a nomogram specifically for hypoxia after OPCABG.22 Collectively, these models have achieved robust predictive performance, with accuracy values exceeding 0.90. This study aimed to develop a risk prediction model for APE based on relevant clinical characteristics in the OPCABG population. By focusing on key clinical features of APE patients, the model will identify risk factors and enable timely intervention, ultimately improving patient outcomes and reducing personal and socio-economic burdens.
Materials and Methods
Patients
We reviewed the records of 15,259 patients who underwent OPCABG at Tianjin Chest Hospital from May 2015 to May 2025, identifying 228 patients diagnosed with APE based on the 2026 criteria from the American Heart Association (AHA) and the American College of Cardiology (ACC).14 Using an individual matching approach, we enrolled 458 non-APE patients who underwent OPCABG during the same period at a 1:2 ratio. Matching criteria included: (1) the same hospitalization surgical episode (within ±5 working days of the index surgery date of the case group), to ensure consistency in diagnostic protocols, surgical techniques, and postoperative care; (2) exact gender matching; and (3) an age-matching tolerance of ±3 years. Exclusion criteria were as follows: (a) presence of valvular disease or infective endocarditis; (b) prior pulmonary embolism diagnosis with current anticoagulant use; (c) undergoing combined valve surgery, lobectomy, arterial replacement, or other surgical procedures; (d) unexplained sudden death within 48 hours post-surgery; (e) incomplete medical records with missing key variables, including preoperative comorbidities, surgery-related parameters, postoperative laboratory results, treatment regimens, and outcome data. The workflow is presented in Figure 1.
 |
Figure 1 Workflow diagram of the study. |
This retrospective study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Tianjin Chest Hospital (2026LW-020). As a retrospective study, it was based on patients’ medical histories and routine clinical data, without interfering with diagnosis, treatment, or patient rights, and without adding additional risks. Therefore, the requirement for informed consent was waived. Patient data will be used solely for scientific research under strict confidentiality, and consent was obtained during hospitalization.
Clinical Characteristics
Pre-operation records: We recorded gender, age, length of hospitalization, and underlying conditions. Laboratory tests included complete blood counts, biochemistry, coagulation profiles, high-sensitivity troponin, NT-ProBNP, and arterial blood gas analysis, along with cardiac ultrasound evaluations of cardiac function.
Intraoperative records: We documented surgery duration, anesthesia time, blood loss and transfusion details, vessel collection sites, and the number of bypass grafts.
Postoperative monitoring: We monitored invasive and non-invasive ventilator times, as well as ventilation duration following secondary intubation. We recorded the initiation and adjustment times for low molecular weight heparin and antiplatelet medications, including their dosages, and the duration of ICU stay. Laboratory tests and cardiac ultrasound examinations mirrored preoperative assessments. We performed lower limb vascular ultrasounds to detect the presence and location of deep vein thrombosis. Specialist radiologists conducted multi-slice spiral CT scans to evaluate vascular blood flow post-coronary artery bypass grafting and to identify the presence, location, and timing of pulmonary embolism. We also documented any postoperative complications.
Variable Selection
Least absolute shrinkage and selection operator (LASSO) regression was used for variable selection in a Cox proportional hazards model. First, the relevant variables were selected based on the univariate Cox regression results with a p-value threshold of 0.05. The selected variables were then processed, with categorical variables converted into dummy variables. The LASSO regression model was fitted using the cv.glmnet() function, which performed cross-validation to determine the optimal regularization parameter (lambda). The minimum lambda value was identified, and the final Lasso model was fitted using glmnet().
Predictive Model
A predictive model is intended for use in the early postoperative period (within 24–48 hours after surgery) to stratify OPCABG patients according to their risk of developing APE. The model can provide a dynamic risk assessment that guides clinicians in escalating monitoring, adjusting prophylactic anticoagulation, or pursuing earlier radiographic screening for high-risk patients. The strongest predictors—both preoperative and early postoperative variables—can therefore warrant heightened clinical attention.
We divided 686 participants into 80% training-test and 20% validation datasets, randomly selecting APE and non-APE patients. The training-test dataset included 548 patients (182 APE including 49 asymptomatic cases and 366 non-APE), which we split into 10 folds for training and testing, using an 8:2 ratio and rotating the folds 10 times. The validation dataset comprised 138 patients (46 APE including 16 asymptomatic cases and 92 non-APE).
The XGBoost model for binary classification with package version 1.6.0 was built in R v4.1.2. The model was configured with the binary: logistic objective and logloss as the evaluation metric. The learning rate (eta) was set to 0.1, with a maximum tree depth (max_depth) of 6 and a minimum child weight (min_child_weight) of 1. For regularization, the subsample rate (subsample) and column sampling rate (colsample_bytree) were both set to 0.8, while gamma was set to 0. The model was designed to balance positive and negative sample weights using scale_pos_weight of 1, and Nthread was set to 4 for parallel processing. Early stopping was applied after 20 rounds without improvement, with the best number of iterations determined as 97 through cross-validation.
Post-Hoc Explanation
SHapley Additive exPlanations (SHAP) was used to interpret the output of machine-learning models, particularly for feature importance. SHAP values provide a way to explain the impact of each feature on the model’s predictions, offering a detailed breakdown of how each feature influences the output. The SHAP values are calculated based on cooperative game theory and give a fair allocation of contribution to each feature by considering all possible interactions. This method helps to improve the interpretability of models by quantifying the contribution of each feature to the model’s predictions.
Statistical Analysis
We analyzed 69 continuous variables and 29 categorical variables. For continuous variables, we used independent-sample t-tests or Mann–Whitney U-tests. Categorical variables were analyzed with chi-square or Fisher’s exact tests. The odds ratio (OR) and 95% confidence interval (CI) were calculated for categorical features exhibiting significant differences between APE and non-APE. A p-value of less than 0.05 was considered statistically significant. All analyses were conducted using SPSS version 19.0 (IBM Corp, Armonk, NY).
Results
Clinical Features of APE
The incidence of post-operative APE among our OPCABG patients is 1.49% (228/15,259). The mortality rate was 0.81% (124/15,259) in OPCAB cases, compared to 3.5% (8/228) among APE patients. APE typically occurs an average of 9.16 ± 5.29 days after the surgery. Common symptoms include hypoxia (49.1%, 112/228), chest tightness (33.3%, 76/228), fatigue (13.2%, 30/228), hemoptysis (1.3%, 3/228), and asymptomatic cases (28.5%, 65/228). Imaging findings reveal that 6.14% (14/228) involve the main pulmonary artery, 29.8% (68/228) involve bilateral pulmonary arteries, and 42.1% (96/228) involve multi-lobular pulmonary arteries. The right lung’s upper lobe and/or segmental pulmonary artery are the most affected site (58.8%, 134/228), with 32.8% (75/228) involving only one segmental pulmonary artery, primarily in asymptomatic patients.
Among APE patients, 32.9% (75/228) also had DVT, with the most frequent cases being left lower limb DVT (23.2%, 53/228) and bilateral lower limb DVT (11.4%, 26/228). Additionally, 10.9% (25/228) had calf intermuscular vein thrombosis.
Comparison of APE and Non-APE Patients
We matched APE patients (n = 228) and non-APE patients (n = 458) by age (66.4 ± 7.4 years vs 65.3 ± 7.4 years) and gender (female: 33.8% vs 34.9%). The risk of APE after OPCABG significantly increases in patients with acute myocardial infarction, old myocardial infarction, old cerebral infarction, sleep apnea hypopnea syndrome, underlying basic lung diseases, and hyperlipidemia (all ORs > 1, P < 0.05) (Table 1).
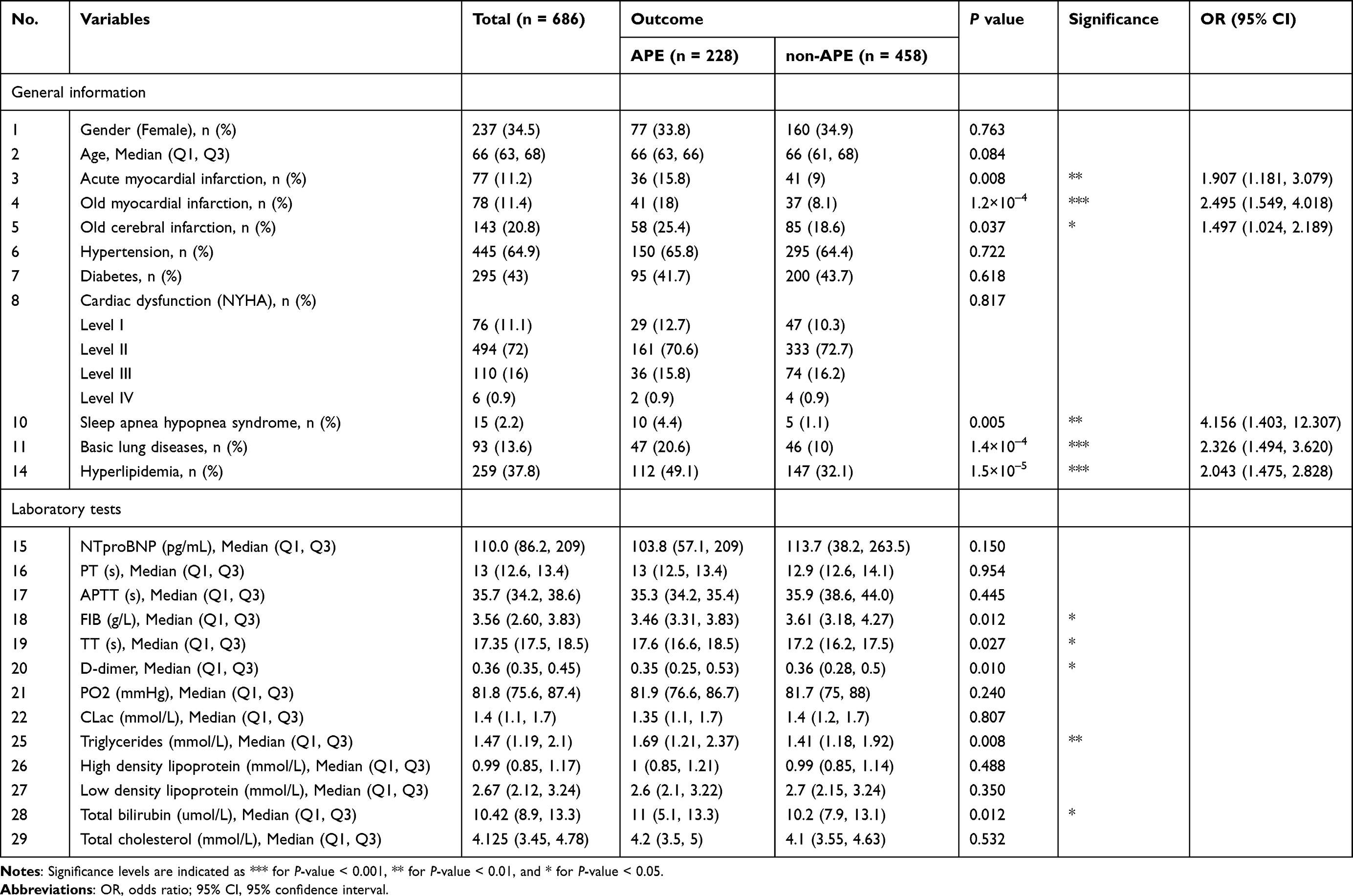 |
Table 1 Underlying Diseases, Preoperative Laboratory Tests, and Their Relationship to Acute Pulmonary Embolism (APE) |
Post-operatively, complications of pleural effusion (OR: 3.659), anemia (OR: 4.397), and hypoalbuminemia (OR: 3.766) significantly increased the risk of APE. Our study also revealed a clinical delay in the initial administration of postoperative low molecular weight heparin administration in the APE group. The mean time to administration was 18.05 ± 9.94 hours, compared to 14.34 ± 2.44 hours in the non-APE group. The proportion of patients receiving dual antibody therapy was also significantly lower in the APE group. Laboratory tests showed significant differences in PT, APTT, FIB, and D-Dimer levels (Table 2). Abnormal or persistently elevated early postoperative D-dimer levels, especially when coupled with APE-related conditions such as pleural effusion, anemia, and hypoalbuminemia, warrant prompt further imaging evaluation to rule out or confirm APE. Furthermore, the later initiation of low-molecular-weight heparin in the APE group underscores timely postoperative anticoagulation as an important modifiable intervention.
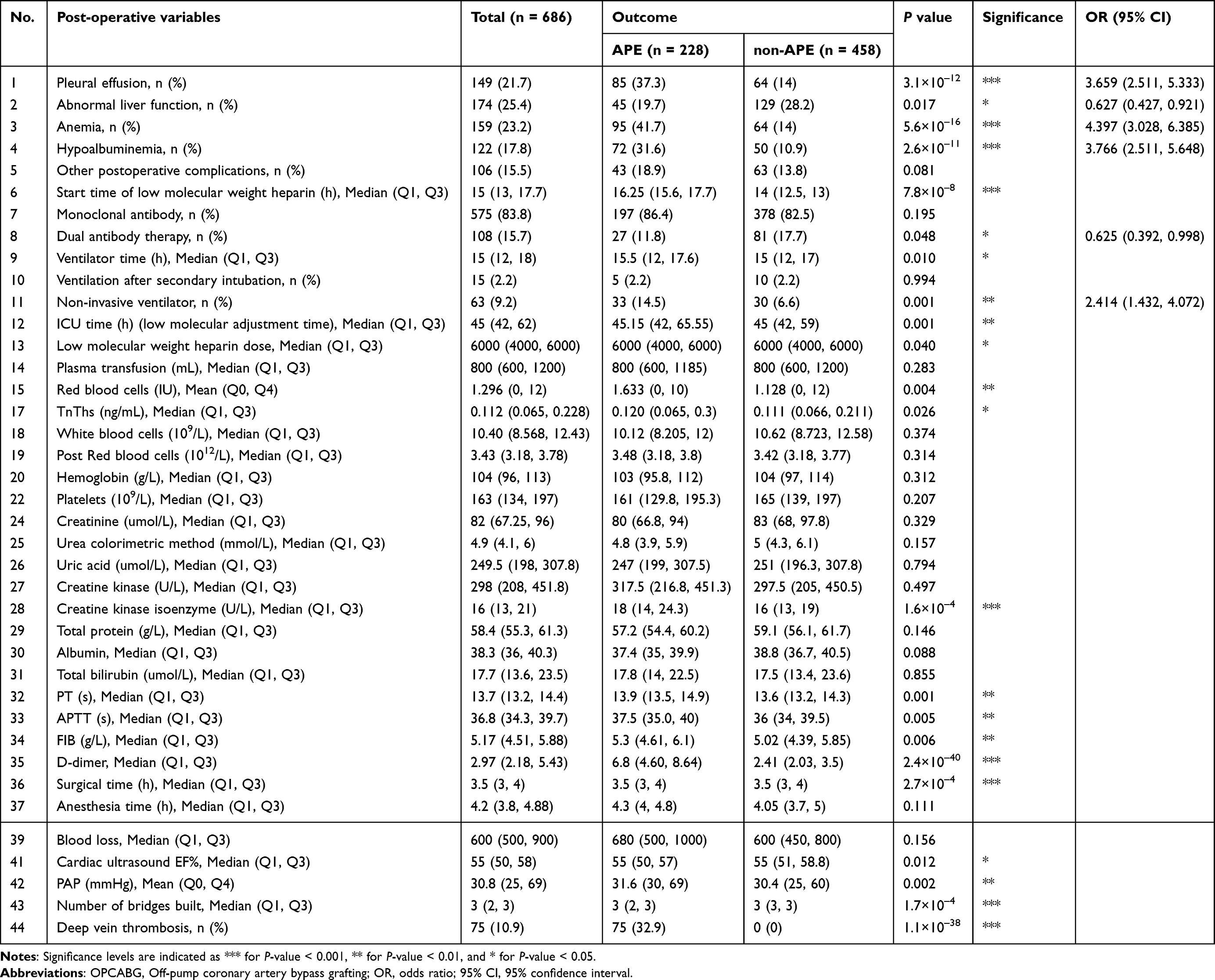 |
Table 2 Statistics of OPCABG Post-Operative Variables for Acute Pulmonary Embolism (APE) |
APE Predictive Model
LASSO regression identified an optimal set of 36 features. The minimum binomial deviance indicated that this combination of variables and their coefficients most accurately predicted APE (Figure 2 and Table 3). Post-operative deep vein thrombosis (LASSO coefficient: 4.367), D-dimer (0.755), pleural effusion (0.588), hypoalbuminemia (0.544), and pre-operative underlying lung diseases (0.239) emerged as key features, demonstrating high regression coefficients among the 36 variables.
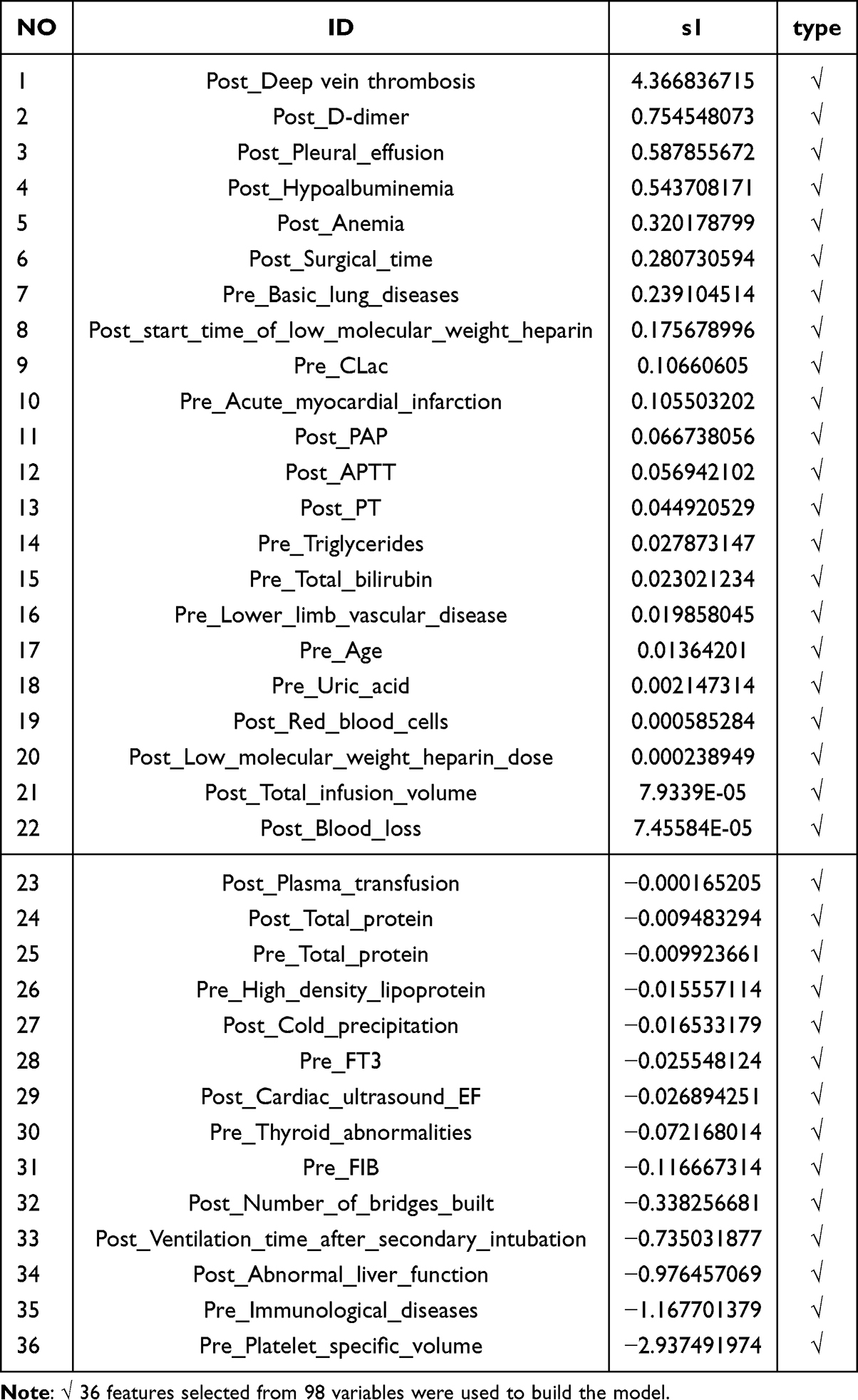 |
Table 3 Lasso Regression Coefficients for 36 Selected Features (Post- and Pre-Operative) |
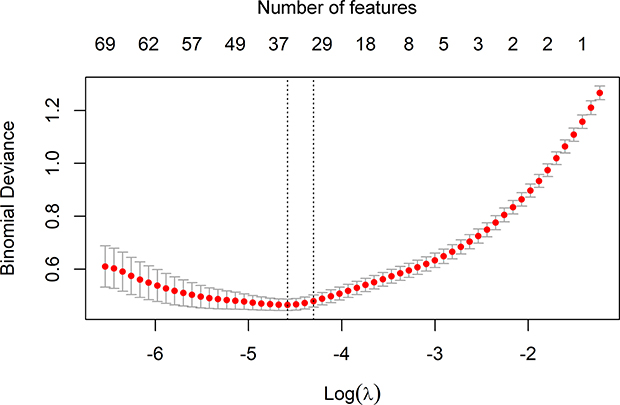 |
Figure 2 Feature selection via Lasso regression: 36 out of 98 variables were identified as optimal predictors for APE in OPCABG patients. The two vertical dotted lines indicate the λ values selected by the minimum criteria (left) and the one-standard-error (1-SE) criteria (right). |
To predict APE likelihood after OPCABG, we utilized a XGBoost machine-learning classifier and developed a risk prediction model based on 36 selected clinical features. In the 10-fold cross-validation, the model achieved an accuracy of 93.5% (95% CI: 0.891, 0.971), an AUC of 97.6% (95% CI: 0.954, 0.998), and an F1 score of 90.3% (95% CI: 0.831, 0.958) in the validation group. The negative predictive value (NPV) was 95.6% (95% CI: 0.909, 0.990), and the positive predictive value (PPV) was 89.4% (95% CI: 0.793, 0.978). The model demonstrated a sensitivity of 91.3% (95% CI: 0.825, 0.982) and a specificity of 94.6% (95% CI: 0.891, 0.989) (Figure 3). The optimal model successfully identified 42 cases of APE (true positive) and 87 non-APE cases (true negative) in the validation set, achieving an AUC of 97.6% (Figure 4A and B).
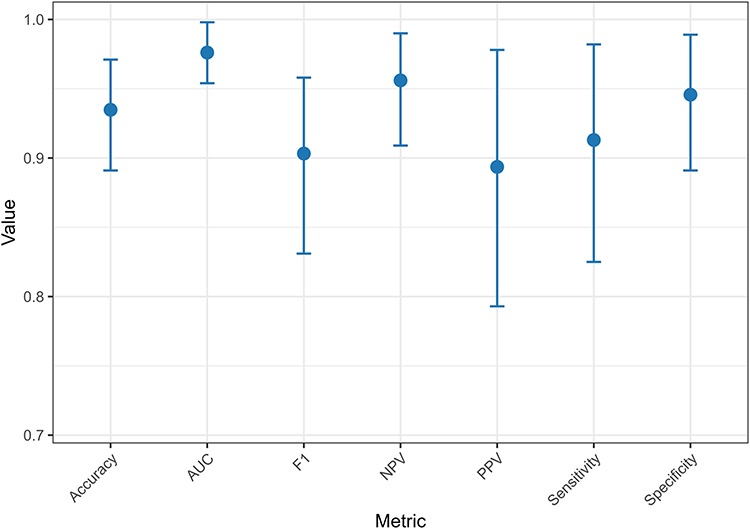 |
Figure 3 Performance of the acute pulmonary embolism predictive model using 36 features. The model achieves convergent and stable performance with respect to key evaluation metrics: accuracy, area under the curve (AUC), F1 score, negative predictive value (NPV), positive predictive value (PPV), sensitivity, and specificity. |
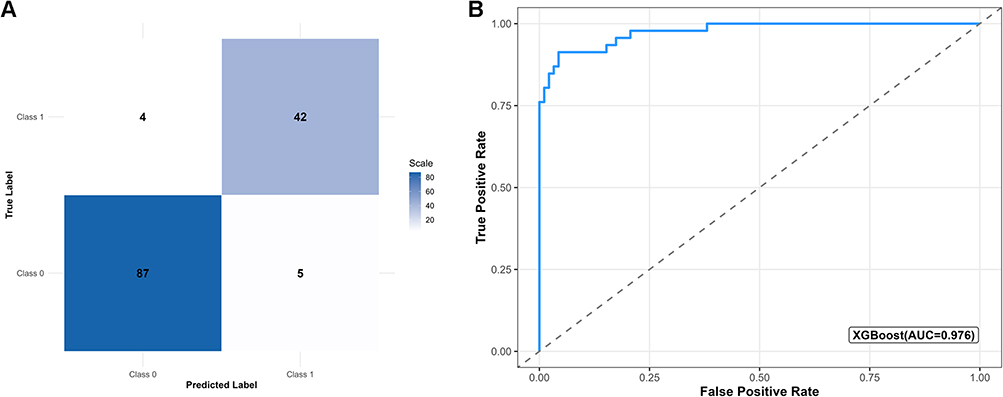 |
Figure 4 (A) Confusion matrix and (B) ROC-AUC of the best-performing XGBoost model for 138 validation patients. The best model successfully predicted 42 APEs and 87 non-APEs in the validation set, achieving an AUC of 97.6%. |
A post-hoc SHAP analysis identified post-operative D-dimer, DVT, start time of low molecular weight heparin, as well as pre-operative uric acid, FIB, triglycerides, etc, as key predictors contributing to the model’s predictive capability (Figure 5).
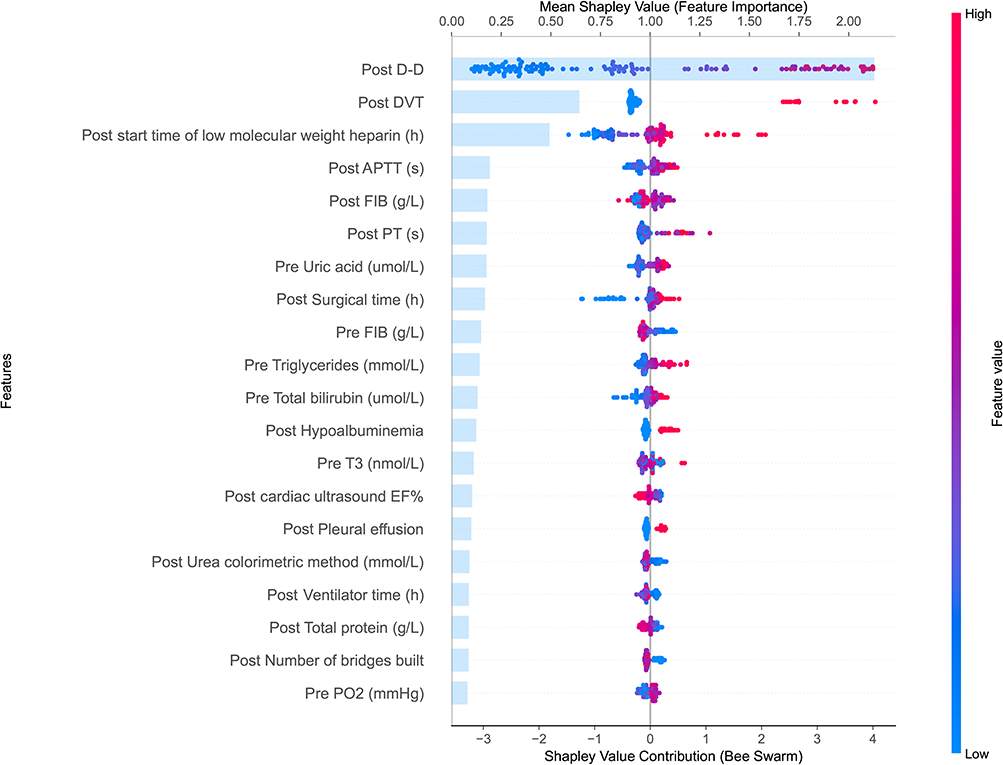 |
Figure 5 SHAP base importance (bar), contribution (bee swarm), and feature values (color) of top 20 features on XGBoost model output. |
Discussion
We reviewed clinical data on APE patients after OPCABG and found that the most common symptoms are hypoxia, chest tightness, and shortness of breath. These non-specific symptoms often overlap with post-operative chest discomfort, shortness of breath, tachycardia, and other complications. Approximately 30% of APE patients are asymptomatic, which aligns with the pulmonary artery involvement patterns seen in computed tomography pulmonary angiography. Notably, 32.8% of patients had involvement in only one lung segment, and those with limited pulmonary artery involvement are frequently asymptomatic. The upper and lower lobes/segments of the right lung are more prone to involvement, likely due to the right pulmonary artery’s larger blood flow share, which may affect intraoperative hemodynamics.
APE is a serious and potentially fatal peri-operative complication, particularly in cardiac surgery patients. Despite routine anticoagulation and monoclonal antibody/dual antiplatelet therapy, APE incidence remains notable Khoury et al noted that APE significantly increases mortality and serves as an independent predictor of death.2 DVT and APE represent different stages of venous thromboembolism (VTE). Over the past decade in the United States, the incidence of APE among patients undergoing cardiac surgery nationwide was 0.38%, and 24.3% of these APE patients were also diagnosed with DVT. OPCABG is the most common cardiac surgery, raising concerns about post-operative APE. Among our OPCABG patients over the past decade, the incidence of APE was 1.49%, with 32.9% presenting a concurrent DVT. Our findings indicate that many APE patients lack DVT, suggesting a possible “susceptibility” among those who do. Historically, most APE cases were believed to originate from thrombi in the lower extremities, and nearly 30% of DVT patients develop symptomatic pulmonary embolism. Our study confirms a strong correlation between postoperative APE and the occurrence of DVT, and further reveals that the development of lower extremity DVT is closely related to the side of the conduit harvested. Accordingly, routine lower extremity vascular ultrasound monitoring in high-risk patients serves not only as a diagnostic measure for detecting DVT but also as a direct strategy for preventing APE.
APE patients after OPCABG more frequently presented with comorbid conditions, including acute/old myocardial infarction, old cerebral infarction, underlying lung disease, and sleep apnea hypopnea syndrome. In those with prior cardiovascular or cerebrovascular disease, widespread endothelial dysfunction secondary to systemic atherosclerosis, combined with perioperative adjustments in antiplatelet therapy, may contribute to a transient prothrombotic state. Patients with underlying lung disease or sleep apnea hypopnea syndrome often experience acute or chronic hypoxemia, which can upregulate hypoxia-inducible factor-1α and promote procoagulant factor expression. Yu et al further identified a preoperative arterial partial pressure of oxygen ≤ 78.9 mmHg as an independent risk factor for APE after OPCABG.22 Postoperatively, complications such as ventilation/perfusion mismatch and atelectasis may exacerbate pulmonary circulatory stasis, thereby increasing thrombotic risk.
D-dimer, a biomarker of plasmin-mediated endogenous fibrinolysis, is widely used in the diagnosis of thrombotic events such as DVT and PE. Previous studies have shown that D-dimer levels increase significantly from baseline following OPCABG and remain elevated for at least 30 days postoperatively.23 However, abnormally elevated postoperative D-dimer levels warrant careful consideration of APE. Our study found that D-dimer levels were significantly higher in OPCABG patients who developed APE compared to those who did not. Furthermore, D-dimer levels were correlated with the occurrence of APE, and SHAP analysis confirmed that abnormal elevation of D-dimer serve as a superior predictor of APE. Therefore, when postoperative patients present with symptoms such as chest tightness and hypoxemia along with abnormally elevated D-dimer levels, a high suspicion for APE should be maintained, and lower extremity venous ultrasound as well as computed tomography pulmonary angiography should be promptly performed.
The incidence of pleural effusion after coronary artery bypass grafting is reported at 62.4%.24 Postoperative pleural effusion can compress healthy lung tissue, leading to compressive atelectasis and reduced gas exchange, which directly causes hypoxia. Moreover, pleural effusion that necessitates secondary drainage during recovery is linked to significantly worse outcomes, including higher mortality rates, longer hospital stays, and increased complications.25 Despite this, few studies have examined the relationship between postoperative pleural effusion and APE. We propose for the first time that postoperative pleural effusion is associated with APE.
Serum albumin has various physiological functions that can help reduce thrombosis.26,27 Hypoalbuminemia disrupts these functions, raising the risk of thrombosis.28 Studies have shown that low serum albumin is a moderate marker of increased VTE risk, with low levels linked to a higher risk of VTE across different populations.29–31 Hoskin et al found that hypoalbuminemia is an independent predictor of mortality after APE and can enhance patient risk stratification in prediction models.32 Our study is the first to identify an association between postoperative hypoalbuminemia and APE after OPCABG, showing that low serum albumin levels indicate hypercoagulability and can predict APE occurrence post-surgery.
Can et al noted that hemoglobin concentrations in emergency APE patients were significantly lower than in controls, suggesting low hemoglobin levels may be a risk factor for pulmonary embolism.33 Anemia increases mortality risk in APE patients and serves as an independent predictor of all-cause mortality.34 However, another case-control study found no correlation between anemia and pulmonary embolism.35 We observed a significantly higher incidence of postoperative anemia in the APE group compared to the non-APE group, though postoperative hemoglobin concentrations did not differ significantly. Our model analysis suggests that anemia following coronary artery bypass surgery is a predictive factor for APE.
Previous studies indicate that patients undergoing OPCABG may enter a pre-thrombotic state as early as the first postoperative day, lasting up to 30 days.5 To prevent thromboembolism, immediate VTE prophylaxis and antiplatelet therapy are essential. Ho et al strongly recommend starting these medications in patients without active bleeding right after cardiac surgery.1 Our study found that the APE group had a lower proportion of patients initiating dual antiplatelet therapy compared to the non-APE group. The predictive model suggests that postoperative dual antiplatelet use may help prevent APE. Our findings indicate that low molecular weight heparin initiation occurred later and at lower doses in APE patients compared to non-APE patients. This delay appears clinically associated with greater postoperative blood loss and higher bleeding risk in the APE group. Therefore, early low molecular weight heparin administration may help prevent APE when bleeding risk is adequately controlled.
Preoperative hyperuricemia emerged as a novel predictor in our model. Multiple studies have also reported that elevated serum uric acid levels are closely associated with the occurrence and recurrence of pulmonary embolism, suggesting that hyperuricemia may serve as a potential risk factor for pulmonary embolism.36–38 Recent studies have further revealed that elevated uric acid levels induce phosphatidylserine exposure and granule release, thereby enhancing the procoagulant activity of red blood cells and vascular endothelial cells, ultimately promoting thrombosis.39,40
Limitations
This single-center retrospective study relies on data from one hospital. The model’s generalizability to other populations or centers with different practice patterns, patient characteristics, and perioperative protocols remains uncertain; external validation in multicenter cohorts is necessary before clinical implementation. We collected clinical data from all APE patients but selected only 1:2 control patients, which may introduce bias. Only a subset of clinically suspicious OPCABG patients underwent multi-slice spiral CT angiography or venous Doppler ultrasonography, with relatively small overall sample sizes potentially compromising model stability and introducing selection bias. This retrospective design inevitably missed some APE cases, particularly among postoperative fatalities without CTA confirmation, precluding accurate assessment of true APE incidence and mortality rates. Additionally, we cannot conduct long-term prognosis follow-ups. To address these limitations, we plan to conduct a prospective study to improve and enhance the diagnostic and predictive performance of the model through comprehensive data collection and prognostic follow-up.
Conclusion
Despite adequate antiplatelet and anticoagulant therapy in clinical practice, APE occurred in 1–2% of patients. In patients presenting with symptoms such as shortness of breath and hypoxemia after OPCABG, along with preoperative hyperuricemia and postoperative abnormally elevated D-dimer, deep vein thrombosis, pleural effusion, or anemia, a high suspicion of pulmonary embolism should be maintained, and computed tomography pulmonary angiography should be promptly performed to confirm the diagnosis and initiate timely treatment. We developed a robust predictive model for APE following OPCABG to identify high-risk patients, optimize treatment outcomes, reduce unnecessary imaging examinations, and ultimately alleviate the associated economic burden. Nevertheless, given that the model was developed and validated within a single-center cohort, external validation in diverse multi-center settings is warranted before its routine clinical application.
Acknowledgments
The authors acknowledge the help of colleagues in cardiac surgery and radiology.
Funding
This study was funded by Tianjin Key Medical Discipline Construction Project (Grant No: TJYXZDXK-3-032C).
Disclosure
The authors declare no competing interests in this work.
References
1. Ho KM, Bham E, Pavey W. Incidence of venous thromboembolism and benefits and risks of thromboprophylaxis after cardiac surgery: a systematic review and meta-analysis. J Am Heart Assoc. 2015;4(10):e002652. doi:10.1161/JAHA.115.002652
2. Khoury H, Lyons R, Sanaiha Y, et al. Deep venous thrombosis and pulmonary embolism in cardiac surgical patients. Ann Thorac Surg. 2020;109(6):1804–15. doi:10.1016/j.athoracsur.2019.09.055
3. Penttila HJ, Lepojärvi MVK, Kiviluoma KT, et al. Myocardial preservation during coronary surgery with and without cardiopulmonary bypass. Ann Thorac Surg. 2001;71(2):565–571. doi:10.1016/S0003-4975(00)02002-6
4. Gerritsen WB, van Boven WJ, Driessen AH, Haas FJ, Aarts LP. Off-pump versus on-pump coronary artery bypass grafting: oxidative stress and renal function. Eur J Cardiothorac Surg. 2001;20(5):923–929. doi:10.1016/S1010-7940(01)00941-1
5. Vallely MP, Bannon PG, Bayfield MS, et al. Quantitative and temporal differences in coagulation, fibrinolysis and platelet activation after on-pump and off-pump coronary artery bypass surgery. Heart Lung Circ. 2009;18(2):123–130. doi:10.1016/j.hlc.2008.08.012
6. Lee CK, Kim YM, Shim DJ, et al. The detection of pulmonary embolisms after a coronary artery bypass graft surgery by the use of 64-slice multidetector CT. Int J Cardiovasc Imag. 2011;27(5):639–645. doi:10.1007/s10554-011-9868-4
7. Du W, Zhao X, Nunno A, et al. Risk factors for venous thromboembolism in individuals undergoing coronary artery bypass grafting. J Vasc Surg Venous Lymphat Disord. 2020;8(4):551–557. doi:10.1016/j.jvsv.2019.06.022
8. Beck KS, Cho EK, Moon MH, et al. Incidental pulmonary embolism after coronary artery bypass surgery: long-term clinical follow-up. AJR Am J Roentgenol. 2018;210(1):52–57. doi:10.2214/AJR.17.18186
9. Zhou J, Cao X, Du Y, et al. Risk factors for acute pulmonary embolism in patients with off-pump coronary artery bypass grafting: implications for nursing. J Int Med Res. 2020;48(11):300060520971445. doi:10.1177/0300060520971445
10. Zehr KJ, Liddicoat JR, Salazar JD, et al. The autopsy: still important in cardiac surgery. Ann Thorac Surg. 1997;64(2):380–383. doi:10.1016/S0003-4975(97)00551-1
11. Rastan AJ, Gummert JF, Lachmann N, et al. Significant value of autopsy for quality management in cardiac surgery. J Thorac Cardiovasc Surg. 2005;129(6):1292–1300. doi:10.1016/j.jtcvs.2004.12.018
12. Wisniewski AM, El Moheb M, Polavarapu N, et al. Venous thromboembolism after coronary artery bypass increases health care costs: a propensity score-matched analysis. Ann Thorac Surg. 2025;120(6):1165–1173. doi:10.1016/j.athoracsur.2025.08.012
13. Pollack CV, Schreiber D, Goldhaber SZ, et al. Clinical characteristics, management, and outcomes of patients diagnosed with acute pulmonary embolism in the emergency department: initial report of EMPEROR (Multicenter emergency medicine pulmonary embolism in the real world registry). J Am Coll Cardiol. 2011;57(6):700–706. doi:10.1016/j.jacc.2010.05.071
14. Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European respiratory society (ERS). Eur Heart J. 2020;41(4):543–603. doi:10.1093/eurheartj/ehz405
15. Sidey-Gibbons JAM, Sidey-Gibbons CJ. Machine learning in medicine: a practical introduction. BMC Med Res Methodol. 2019;19(1):64. doi:10.1186/s12874-019-0681-4
16. Choudhury A. Predicting cancer using supervised machine learning: mesothelioma. Technol Health Care. 2021;29(1):45–58. doi:10.3233/THC-202237
17. Qiu B, Chen H, Zhang E, et al. A machine learning prediction model for cancer risk in patients with type 2 diabetes based on clinical tests. Technol Health Care. 2024;32(3):1431–1443. doi:10.3233/THC-230385
18. Guo Y, Xia C, Zhong Y, et al. Machine learning-enhanced echocardiography for screening coronary artery disease. Biomed Eng Online. 2023;22(1):44. doi:10.1186/s12938-023-01106-x
19. Balyen L, Peto T. Promising artificial intelligence-machine learning-deep learning algorithms in ophthalmology. Asia Pac J Ophthalmol. 2019;8(3):264–272. doi:10.22608/APO.2018479
20. Abbasi A, Li C, Dekle M, et al. Interpretable machine learning-based predictive modeling of patient outcomes following cardiac surgery. J Thorac Cardiovasc Surg. 2025;169(1):114–123e28. doi:10.1016/j.jtcvs.2023.11.034
21. Shen J, Xue B, Kannampallil T, et al. A novel generative multi-task representation learning approach for predicting postoperative complications in cardiac surgery patients. J Am Med Inform Assoc. 2025;32(3):459–469. doi:10.1093/jamia/ocae316
22. Yu HY, Bai Y-P, Song X-C, et al. Factors associated with acute pulmonary embolism in patients with hypoxia after off-pump coronary artery bypass grafting: a case-control study. J Multidiscip Healthc. 2024;17:573–583. doi:10.2147/JMDH.S447534
23. Parolari A, Mussoni L, Frigerio M, et al. Increased prothrombotic state lasting as long as one month after on-pump and off-pump coronary surgery. J Thorac Cardiovasc Surg. 2005;130(2):303–308. doi:10.1016/j.jtcvs.2004.11.002
24. Light RW, Rogers JT, Moyers JP, et al. Prevalence and clinical course of pleural effusions at 30 days after coronary artery and cardiac surgery. Am J Respir Crit Care Med. 2002;166(12 Pt 1):1567–1571. doi:10.1164/rccm.200203-184OC
25. Schiefenhovel F, Poncette A-S, Boyle EM, et al. Pleural effusions are associated with adverse outcomes after cardiac surgery: a propensity-matched analysis. J Cardiothorac Surg. 2022;17(1):298. doi:10.1186/s13019-022-02050-y
26. Fanali G, Di Masi A, Trezza V, et al. Human serum albumin: from bench to bedside. Mol Aspects Med. 2012;33(3):209–290. doi:10.1016/j.mam.2011.12.002
27. Caraceni P, Domenicali M, Tovoli A, et al. Clinical indications for the albumin use: still a controversial issue. Eur J Intern Med. 2013;24(8):721–728. doi:10.1016/j.ejim.2013.05.015
28. Sun Y, Deng J, Ding Y, et al. Serum albumin, genetic susceptibility, and risk of venous thromboembolism. Res Pract Thromb Haemost. 2024;8(5):102509. doi:10.1016/j.rpth.2024.102509
29. Kunutsor SK, Seidu S, Katechia DT, et al. Inverse association between serum albumin and future risk of venous thromboembolism: interrelationship with high sensitivity C-reactive protein. Ann Med. 2018;50(3):240–248. doi:10.1080/07853890.2018.1441537
30. Gyamlani G, Molnar MZ, Lu JL, et al. Association of serum albumin level and venous thromboembolic events in a large cohort of patients with nephrotic syndrome. Nephrol Dial Transplant. 2017;32(1):157–164. doi:10.1093/ndt/gfw227
31. Liu Z, Mi J. Serum albumin and circulating metabolites and risk of venous thromboembolism: a two-sample mendelian randomization study. Front Nutr. 2021;8:712600. doi:10.3389/fnut.2021.712600
32. Hoskin S, Chow V, Kritharides L, et al. Incidence and impact of hypoalbuminaemia on outcomes following acute pulmonary embolism. Heart Lung Circ. 2020;29(2):280–287. doi:10.1016/j.hlc.2019.01.007
33. Cağdas C, Hakan T, Reyan U. Investigation of relationship between blood hemoglobin level and acute pulmonary embolism in emergency setting. Int Med J. 2013;20(5):584–586.
34. Jimenez D, Escobar C, Martí D, et al. Association of anaemia and mortality in patients with acute pulmonary embolism. Thromb Haemost. 2009;102(1):153–158. doi:10.1160/TH09-01-0003
35. Harringa JB, Bracken RL, Nagle SK, et al. Anemia is not a risk factor for developing pulmonary embolism. Am J Emerg Med. 2017;35(1):146–149. doi:10.1016/j.ajem.2016.09.068
36. Weng H, Li H, Zhang Z, et al. Association between uric acid and risk of venous thromboembolism in East Asian populations: a cohort and Mendelian randomization study. Lancet Reg Health West Pac. 2023;39:100848. doi:10.1016/j.lanwpc.2023.100848
37. Li L, McCormick N, Sayre EC, et al. Trends of venous thromboembolism risk before and after diagnosis of gout: a general population-based study. Rheumatology. 2020;59(5):1099–1107. doi:10.1093/rheumatology/kez398
38. De Lucchi L, Nardin C, Sponchiado A, et al. Serum uric acid levels and the risk of recurrent venous thromboembolism. J Thromb Haemost. 2021;19(1):194–201. doi:10.1111/jth.15139
39. Yan M, Xu M, Li Z, et al. TMEM16F mediated phosphatidylserine exposure and microparticle release on erythrocyte contribute to hypercoagulable state in hyperuricemia. Blood Cells Mol Dis. 2022;96:102666. doi:10.1016/j.bcmd.2022.102666
40. Yu H, Wang Z, Li Z, et al. Hyperuricemia enhances procoagulant activity of vascular endothelial cells through TMEM16F regulated phosphatidylserine exposure and microparticle release. FASEB J. 2021;35(9):e21808. doi:10.1096/fj.202100426R
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.