Back to Journals » Clinical Ophthalmology » Volume 15
Characterization of Polybacterial versus Monobacterial Conjunctivitis Infections in Pediatric Subjects Across Multiple Studies and Microbiological Outcomes with Besifloxacin Ophthalmic Suspension 0.6%
Authors Blondeau JM, Proskin HM ![]() , Sanfilippo CM, DeCory HH
, Sanfilippo CM, DeCory HH ![]()
Received 21 September 2021
Accepted for publication 26 October 2021
Published 10 November 2021 Volume 2021:15 Pages 4419—4430
DOI https://doi.org/10.2147/OPTH.S335197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Joseph M Blondeau,1 Howard M Proskin,2 Christine M Sanfilippo,3 Heleen H DeCory3
1Clinical Microbiology, Royal University Hospital, Saskatoon, SK, Canada; 2Howard M. Proskin & Associates, Rochester, NY, USA; 3Pharmaceutical Medical Affairs, Bausch + Lomb, Rochester, NY, USA
Correspondence: Heleen H DeCory
Pharmaceutical Medical Affairs, 1400 North Goodman Street, Rochester, NY, 14609, USA
Tel +1 585 338-8161
Email [email protected]
Introduction: The choice of empiric therapy for bacterial conjunctivitis should be guided by an awareness of typical causative pathogen distributions. Bacterial conjunctivitis can be polybacterial, although pediatric-specific data are lacking.
Methods: This was a post-hoc analysis of data in pediatric subjects (1– 17 years) from five bacterial conjunctivitis trials evaluating besifloxacin ophthalmic solution 0.6%.
Results: Of the 730 pediatric subjects with culture-confirmed conjunctivitis, nearly one-fourth (23.6%) had polybacterial infections and three-fourths (76.4%) had monobacterial infections at baseline. In both polybacterial and monobacterial infections, the most prevalent organisms were Haemophilus influenzae, Streptococcus pneumoniae, Staphylococcus aureus, and Streptococcus mitis/S. mitis group. In polybacterial versus monobacterial infections, S. mitis/S. mitis group (8.7% vs 4.3%; P=0.032) and Moraxella catarrhalis (4.7% vs 0.5%; P< 0.001) were identified more frequently, whereas S. pneumoniae (14.0% vs 28.1%; P< 0.001) was identified less frequently, as the dominant infecting species. MICs for individual species were similar for tested antibiotics regardless of polybacterial or monobacterial infection, except Staphylococcus epidermidis for which fluoroquinolone MICs were ≥ 3 dilutions higher for isolates of this species sourced from polybacterial compared to monobacterial infections. Treatment with besifloxacin resulted in microbial eradication in 79.1% of polybacterial and 92.3% of monobacterial infections (P≤ 0.005 vs vehicle).
Discussion: One in four pediatric bacterial conjunctivitis infections is polybacterial, highlighting the need for a broad-spectrum antibiotic when choosing empiric therapy.
Keywords: pediatric, conjunctivitis, polybacterial, besifloxacin, minimum inhibitory concentration
Introduction
Infectious conjunctivitis is common, particularly in infants and school children,1 with bacterial pathogens identified in approximately 50–80% of acute cases in children.2–4 While conjunctivitis is generally self-limiting, topical antibacterial treatment can shorten the duration of symptoms, may lessen contagion, and allows for a faster return to school or day care.1,2,5 Cultures are rarely obtained in routine cases of conjunctivitis, and treatment choice is typically empiric. Thus, awareness of causative pathogen distributions is important to guide therapy decisions.
Choosing appropriate empiric therapy can be complicated by the fact that many ocular infections involve more than one bacterial species (polybacterial infections). Studies in patients with keratitis or endophthalmitis have found that anywhere from 2% to 62% of cases may be polybacterial or due to combinations of bacteria and other microbes, such as viruses or yeast (polymicrobial).6–17 To date, few studies have characterized polybacterial infections in patients with conjunctivitis, and very little data exist with regard to pediatric cases specifically.
Besifloxacin ophthalmic suspension 0.6% (Besivance®; Bausch + Lomb, a division of Bausch Health US, LLC; Bridgewater, NJ) is a chlorofluoroquinolone antibiotic approved in 2009 by the Food and Drug Administration for the treatment of bacterial conjunctivitis. Using pooled microbiological data from three besifloxacin clinical trials in patients of any age with bacterial conjunctivitis, we recently reported that about one in five had a polybacterial infection.18 Previous studies have reported mixed bacterial growth in 20.0%19 (bacterial conjunctivitis patients aged 1–85 in India), 47.8%20 (infants with bacterial conjunctivitis resistant to empirical therapy in Egypt), and 66.8%21 (children with infective conjunctivitis in the United Kingdom) of cases.
In the current analysis, we used pooled data extracted from five besifloxacin conjunctivitis studies to evaluate polybacterial versus monobacterial baseline characteristics of conjunctivitis in pediatric subjects. Established species-specific prespecified threshold criteria were applied to the identified and enumerated bacterial species to distinguish ocular pathogenic bacteria from commensal (ie, normal) microflora. We also compared minimal inhibitory concentration (MIC) data for various fluoroquinolones and azithromycin against pediatric conjunctivitis isolates and determined microbial eradication outcomes with besifloxacin treatment.
Methods
This was a post hoc analysis of microbiological data from pediatric (ages 1–17) subjects in five previous besifloxacin clinical trials, including three pivotal clinical trials evaluating the efficacy of besifloxacin 0.6% three times daily (TID) compared to either vehicle or active control (moxifloxacin) for conjunctivitis (ClinicalTrials.gov identifiers: NCT00347932,22 NCT00348348,23 NCT0062290824), one study evaluating besifloxacin 0.6% twice daily (BID) for conjunctivitis versus vehicle (NCT00972777),25 and one study comparing the safety of besifloxacin 0.6% TID versus vehicle (NCT01175590).26 As this was a post hoc analysis, there was no need for an informed consent process. All studies were conducted in accordance with Good Clinical Practices, the International Conference on Harmonization guidelines, the Declaration of Helsinki, and the Health Insurance Portability and Accountability Act guidelines and were approved by the Institutional Review Board of each study center or by Schulman Associates Institutional Review Board, Inc. (Cincinnati, OH) or Western Institutional Review Board Incorporated (Olympia, WA) when a local review board was not available. Advarra Institutional Review Board (Columbia, MD) reviewed the study concept retrospectively and determined that this analysis meets the criteria for exemption from IRB oversight under 45 CFR 46.101(b)(4).
Detailed study methodologies (including ethics compliance and governance) and results for the five source studies have been published previously.22–26 In all studies, eligible subjects were ≥1 year of age with a diagnosis of bacterial conjunctivitis characterized by grade 1 (ie, mild) or greater purulent conjunctival discharge and bulbar conjunctival injection in at least one eye. The study eye was the eye with the highest combined score of conjunctival discharge and/or bulbar conjunctival injection at baseline, or the right eye if both eyes had equal scores. Duration of therapy and timing of follow-up visits varied among studies. In the three TID dosing studies, treatment was for five days with follow-up visits on day 4 [±1]24 or day 5 [±1]22,23 and again at day 8 or 9;22–24 in the BID study, treatment was for 3 days with follow-up at day 4 or 5 and at day 7 [±1];25 and in the TID safety study treatment was for seven days with follow-up assessments on day 8 or 9 and day 11 or 12.26
In all studies, separate microbiological and viral samples were obtained from the cul-de-sac of infected eyes (study eye and fellow eye [non-study eye], if applicable) at baseline and at each study visit, prior to instillation of study medication. Samples were shipped (in 20% glycerol for bacteria and M4RT viral transport media for viruses) to a central laboratory (Covance Central Laboratory Services, Inc. [Indianapolis, IN]) for quantitative and qualitative analysis using methods previously described.27 Briefly, serial dilutions of microbiological samples were plated on both bacteriologic and yeast media, and the resulting colonies at 2–5 days were quantified and speciated by appropriate biochemical and/or molecular identification methods. Similarly, viral cultures were inoculated onto appropriate cell lines, which were observed daily for 2–3 weeks for cytopathic effect; immunofluorescent reagents were used to identify adenovirus and herpes simplex virus. To avoid the attribution of the infection to commensal microflora, bacterial species identified at baseline were deemed causative if the colony count equaled or exceeded species-specific prespecified threshold criteria. These criteria are based on the Cagle list as modified by Liebowitz (Supplemental Table A),28,29 in which isolates are speciated and categorized according to threshold levels of colony-forming units (CFU)/mL; non-commensal isolates are assigned to lower threshold groups, while commensal ocular species are assigned to higher threshold groups. Application of these criteria reduced the likelihood of reporting artificially high culture-positive rates due to recovery of low numbers of transient organisms or organisms that normally colonize the eye but are not involved in acute infectious processes. In all studies, MICs were determined for besifloxacin and comparator antibacterial agents, including other fluoroquinolones, for all bacterial isolates that met or exceeded threshold using broth microdilution procedures recommended by the Clinical and Laboratory Standards Institute.30–32 Briefly, isolates (~5 × 105 CFU/mL) were grown in appropriate testing media in 96-well microtiter panels containing titrated antibiotic concentrations and were incubated for 16–24 hours. The MIC, defined as the lowest concentration of an antimicrobial agent that prevents visible growth of a microorganism, was determined for each isolate by comparing growth in control wells (no antibiotics) to growth in wells that contained varying antibiotic concentrations.30–32
For this post hoc analysis, microbiological data were extracted from the five source studies for pediatric (ages 1–17 years) subjects with confirmed bacterial conjunctivitis. Each subject was categorized as having monobacterial conjunctivitis (one bacterial species in the study eye at or above the prespecified threshold criteria) or polybacterial conjunctivitis (>1 bacterial species in the study eye at or above prespecified threshold criteria). To evaluate the relative contribution of each bacterial species in subjects with polybacterial infections, the fold-increase in colony count (CFU/mL) over the prespecified threshold (CFU/mL) was used to rank order the contribution of each causative bacterial species (Supplemental Table A).
Microbial eradication was evaluated on the modified intent-to-treat population, which included all randomized subjects from whom baseline cultures indicated bacteria levels at or above threshold for any accepted ocular bacterial pathogen (ie, culture-positive subjects with their assigned treatment). For each subject, eradication results for aggregates of species (Gram-positive, Gram-negative) were based on findings for the baseline-designated study eye, as defined above. However, for each subject, eradication results for individual bacterial species were based on findings for the eye (study or fellow/nonstudy) in which the species was isolated, since both eyes could contribute microbiological samples to the analysis if both eyes had signs and symptoms of bacterial conjunctivitis and the fellow/nonstudy eye had different pathogenic organism(s) than in the study eye, which met the prespecified threshold criteria.
Statistical Methods
A two-way analysis of variance with fixed effects of infection type (monobacterial or polybacterial) and clinical study was used to assess differences in age between subjects presenting with monobacterial versus polybacterial conjunctivitis. Differences in gender and viral coinfection were analyzed using Cochran-Mantel-Haenszel tests stratified by clinical study. Fisher’s exact tests were used to compare differences in prevalence of dominant infecting species.
Microbial eradication percentages were compared for besifloxacin versus vehicle and moxifloxacin versus vehicle at day 4 and day 8 for polybacterial and monobacterial infections using chi-squared tests. One study26 did not have day 4 data; thus, the day 4 analysis included only four studies. Missing data were treated as failures.
For all statistical tests of hypothesis, the level of significance was α=0.05.
Results
Study Population and Pathogen Distribution at Baseline
A total of 3379 subjects were randomized and treated across the five source studies. Of these, 1616 (47.8%) subjects had culture-confirmed bacterial conjunctivitis. Of the culture-confirmed cases, 730 (45.2%) were between the ages of 1 and 17 years and comprised the population for the current analysis. Subject distribution is outlined in Figure 1. A majority of pediatric culture-confirmed cases (76.4%) had one bacterial species at or exceeding the prespecified threshold criteria at baseline (monobacterial conjunctivitis). The remainder (23.6%) had more than one bacterial species meeting threshold criteria (polybacterial conjunctivitis).
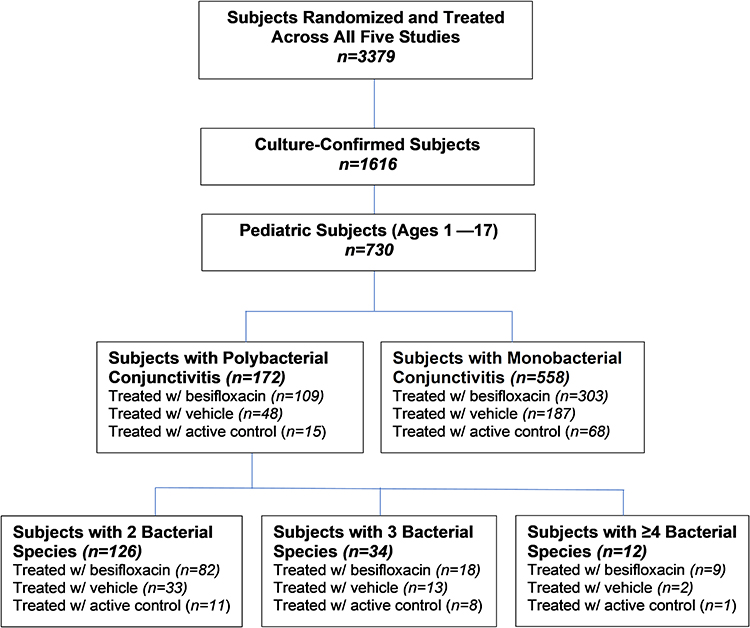 |
Figure 1 Distribution of subjects. |
A total of 67 different bacterial species were identified at or above threshold criteria. Among the polybacterial infections, 58 different species were identified; 32 different species were identified in monobacterial infections. Some isolates were identified only at the genus or group level. A complete listing of bacterial species prevalence for polybacterial and monobacterial infections is provided in Supplemental Table B. Species most commonly isolated from subjects in both polybacterial and monobacterial infections included H. influenzae (47.7% and 48.4%, respectively), S. aureus (36.0% and 9.0%), S. mitis group (36.0% and 3.8%), and S. pneumoniae (18.6% and 28.1%). Organisms identified at a frequency ≥2% in polybacterial infections only included: Moraxella catarrhalis, Dolosigranulum pigrum, S. mitis, Aerococcus viridans, Streptococcus oralis, Corynebacterium pseudodiphtheriticum, Moraxella nonliquefaciens, Streptococcus pyogenes, Rothia mucilaginosa, Streptococcus species, Corynebacterium macginleyi, Staphylococcus capitis, and Staphylococcus caprae.
Figure 2 illustrates the rank order of dominant, secondary, tertiary, and quaternary species at baseline in polybacterial infections. There were four main dominant species (dominant in ≥10 infections): H. influenzae, S. pneumoniae, S. aureus, S. mitis/S. mitis group, and among polybacterial infections with these dominant organisms, there were 29 different secondary coinfecting organisms, the most common being S. aureus (23.3%) and S. mitis/S. mitis group (24.4%). A large proportion of polybacterial infections were due to combinations of Gram-negative and Gram-positive organisms.
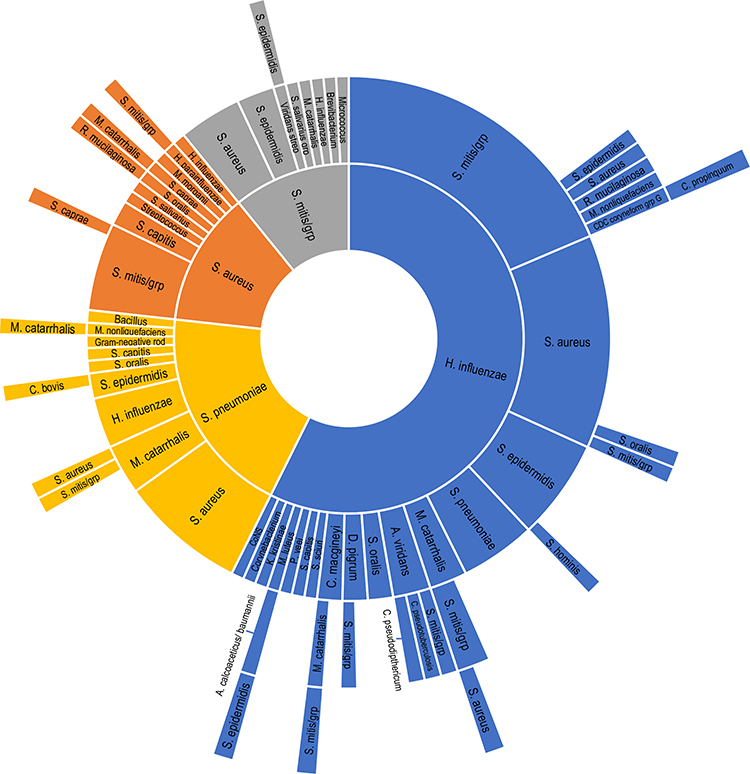 |
Figure 2 Dominant, secondary, tertiary, and quaternary infecting species at baseline in polybacterial conjunctivitis infections. Dominant bacterial species are shown in the inner ring, whereas secondary, tertiary, and quaternary infecting bacterial species are shown by rank order moving outwards by ring. Only those polybacterial infections in which the same dominant species was identified in more than 10 infections are presented. |
Table 1 summarizes patient demographics and dominant infecting species in pediatric patients with polybacterial and monobacterial conjunctivitis infections. The mean age of subjects with polybacterial infections was slightly younger compared to that of subjects with monobacterial infections (5.0 vs 6.2 years; P=0.007). Viral coinfection was more common among polybacterial vs monobacterial infections (5.2% vs 1.6%; P<0.007). No yeasts were identified in study eyes at baseline. S. pneumoniae was a causative or dominant infecting species in significantly fewer polybacterial vs monobacterial infections (14.0% vs 28.1%; P<0.001), while the opposite was true for S. mitis/S. mitis group (8.7% vs 4.3%; P=0.032) and M. catarrhalis (4.7% vs 0.5%; P<0.001), which were more frequently dominant in polybacterial infections.
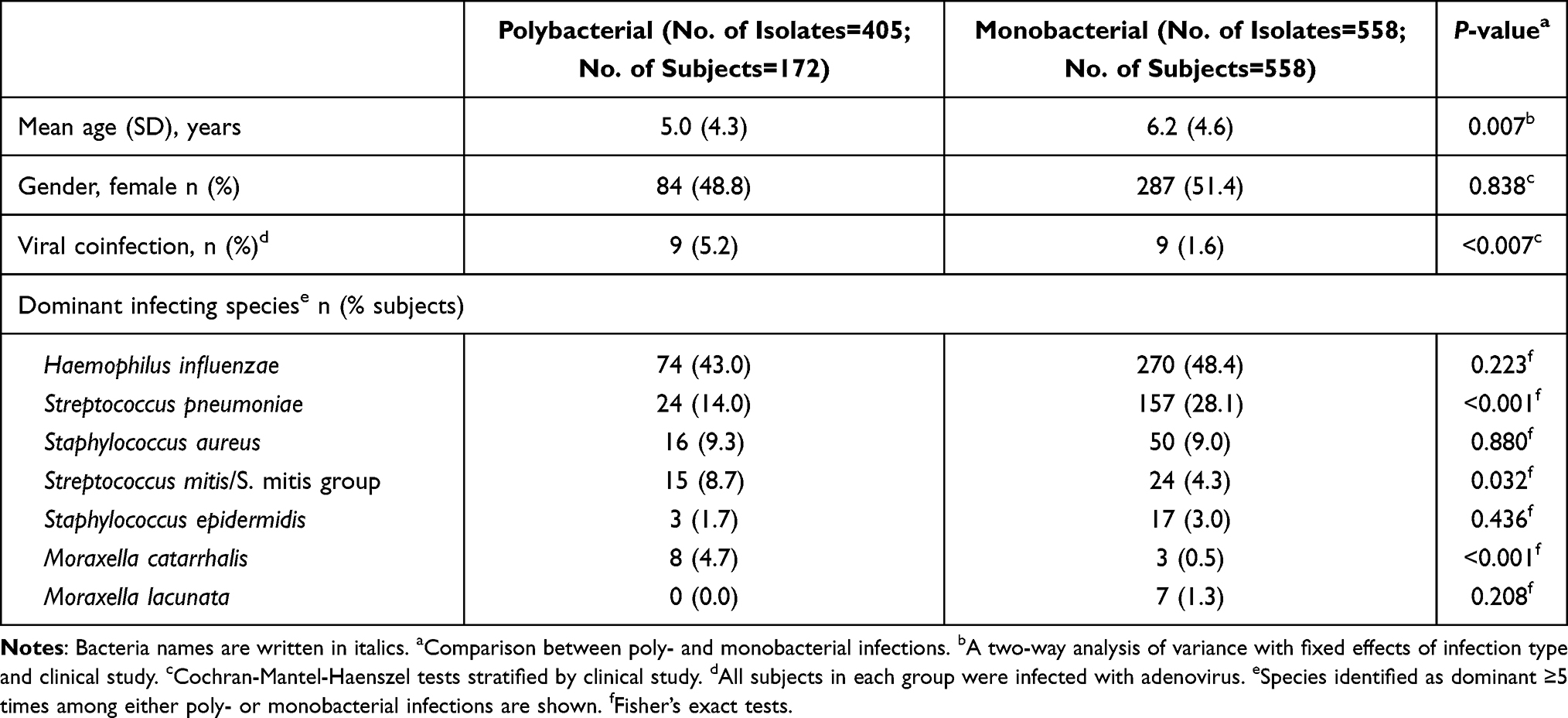 |
Table 1 Pediatric Subject Demographics in Poly- and Monobacterial Conjunctivitis Infections |
Antibiotic Minimum Inhibitory Concentrations
Table 2 displays MIC ranges and MIC90 values for besifloxacin and comparator antibiotics for all isolates, Gram-positive/Gram-negative isolates, and for individual bacterial species with ≥10 isolates at or above threshold at baseline. For all isolates combined in the polybacterial (n=405) and monobacterial (n=558) infection groups, respectively, the MIC90s were 0.25/0.125 for besifloxacin, 0.25/0.125 for moxifloxacin, 0.5/0.5 for gatifloxacin, 1/1 for levofloxacin, 2/1 for ciprofloxacin, and >8/8 for azithromycin. The MIC90s for all fluoroquinolones tested were relatively lower for Gram-negative versus Gram-positive isolates, but overall were not different whether sourced from monobacterial or polybacterial infections. The one exception was S. epidermidis for which MIC90 values for all fluoroquinolones tested were ≥3 dilutions higher for isolates of this species sourced from polybacterial versus those of this species from monobacterial infections.
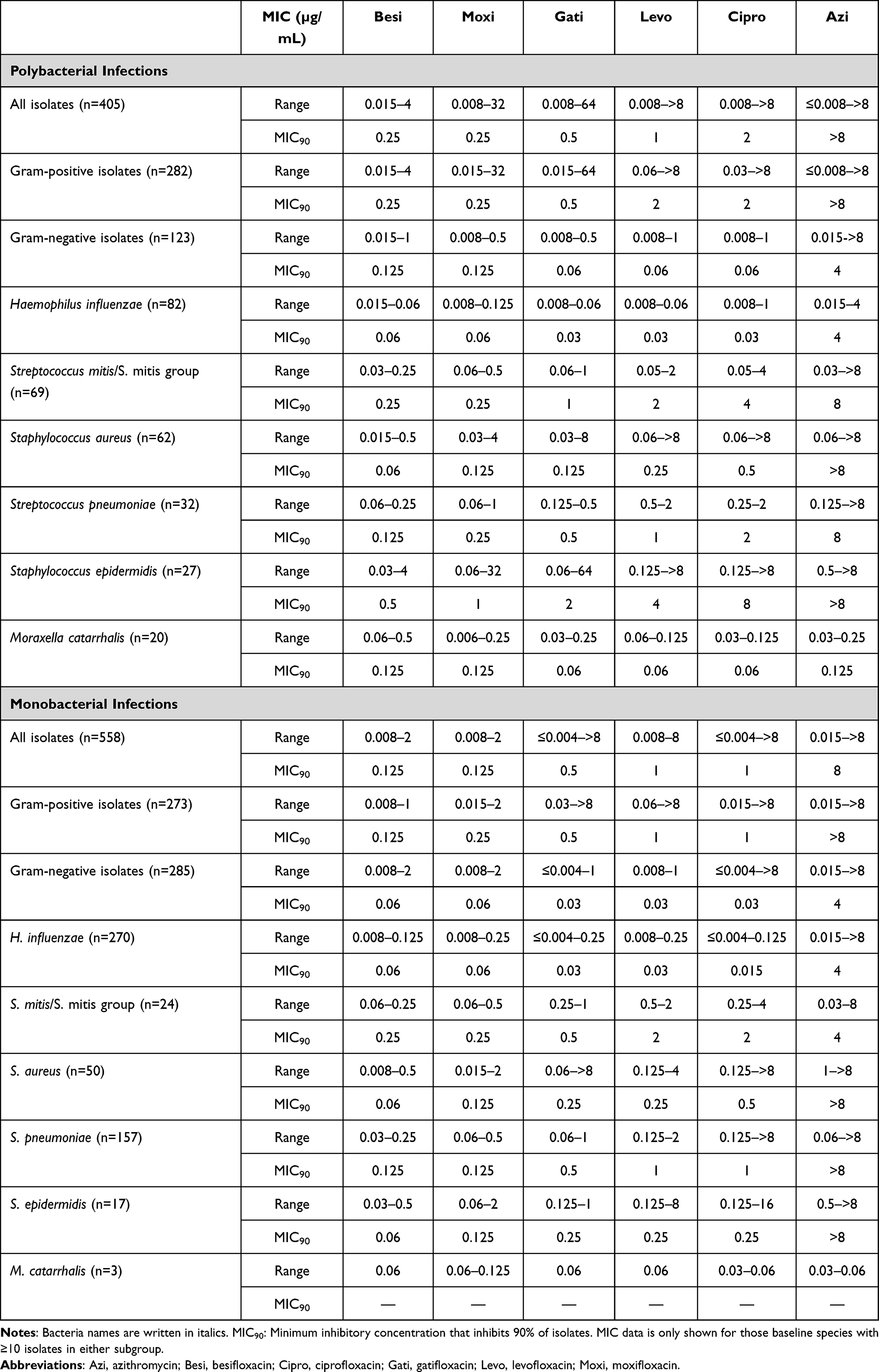 |
Table 2 Minimum Inhibitory Concentrations (MICs) of Besifloxacin and Comparator Antibacterial Agents for Baseline Isolates from Poly- and Monobacterial Conjunctivitis Infections in Pediatric Subjects |
Microbial Eradication Rates
For all pediatric subjects, microbial eradication rates on days 4 and 8 were significantly higher with besifloxacin vs vehicle for both polybacterial ([day 4] 79.1% vs 53.7%, P=0.005; [day 8] 71.6% vs 52.1%, P=0.018) and monobacterial ([day 4] 92.3% vs 60.9%, P<0.001; [day 8] 87.8% vs 69.5%, P<0.001) infections. Likewise, microbial eradication rates were significantly higher with moxifloxacin vs vehicle for both polybacterial ([day 4] 93.3% vs 53.7%, P=0.006; [day 8] 93.3% vs 52.1%, P=0.004) and monobacterial ([day 4] 88.2% vs 60.9%, P<0.001; [day 8] 82.4% vs 69.5%, P=0.041) infections.
Findings were similar for a subset of subjects aged 1 to 5 years for both polybacterial and monobacterial infections. Both fluoroquinolones were associated with significantly higher eradication percentages versus vehicle at both study visits, with the one exception being that besifloxacin was not significantly different from vehicle on day 8 among polybacterial infections (67.1% vs 50.0%; P=0.096). Among subjects who were 1 year of age, both subjects with poly- and monobacterial conjunctivitis infections showed significantly higher microbial eradication rates with besifloxacin vs vehicle, but only on day 4 of treatment ([polymicrobial] 86.7% vs 44.4%, P=0.028; [monobacterial] 81.8% vs 50.0%, P=0.021). In this age group, there were no significant differences between moxifloxacin and vehicle at either timepoint.
Table 3 presents data on microbial eradication by Gram-positive, Gram-negative, and most common organisms associated with poly- and monobacterial conjunctivitis infections in the four vehicle-controlled studies. On both days 4 and 8, the rates of microbial eradication among both poly- and monobacterial infections were numerically higher in besifloxacin-treated eyes than in vehicle-treated eyes; the only exception was for S. epidermidis infections at day 4, but that may be reflective of sample size. On day 8, eradication rates exceeding 73% among polybacterial and 83% among monobacterial infections were achieved with besifloxacin treatment for the most prevalent organisms (S. aureus, S. epidermidis, H. influenzae, S. pneumoniae).
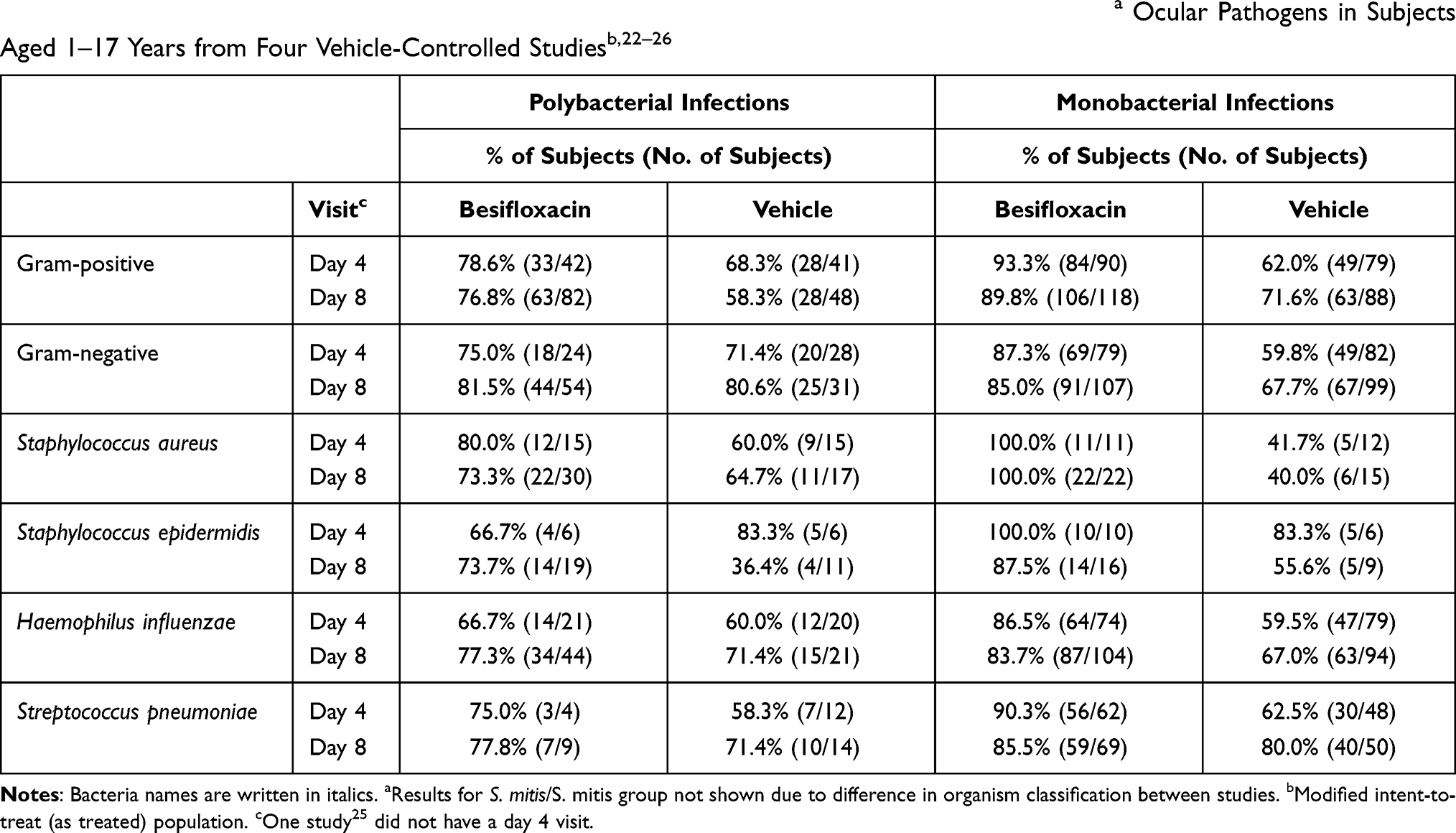 |
Table 3 Efficacy of Treatment (Subjects with Microbial Eradication) as a Function of Most Prevalenta Ocular Pathogens in Subjects Aged 1–17 Years from Four Vehicle-Controlled Studiesb,22–26 |
Discussion
This is the first known characterization of bacterial pathogen distribution and corresponding in vitro antibiotic susceptibilities for bacterial organisms isolated from monobacterial and polybacterial conjunctivitis in pediatric subjects. Pooled data extracted from five clinical studies provided a robust sample of 558 monobacterial infections/isolates and 172 polybacterial infections (405 isolates). In order to prevent inaccurately ascribing pathogen status to commensal bacteria, prespecified species threshold criteria were used to classify organisms as causative pathogens. About one in four pediatric conjunctivitis cases involve more than one bacterial species, which appears higher than that previously reported based on non-age specific data.18,19 Further, one in five pediatric subjects had three or more bacterial species identified.
The most commonly isolated bacterial species from these pediatric-sourced infections was H. influenzae, which was not only present in about half of both monobacterial (48.4%) and polybacterial (47.7%) infections but was also the most common dominant infecting species in polybacterial infections (43.0%). These findings differed somewhat from those of our previous study of conjunctivitis-sourced isolates from subjects of any age, in which H. influenzae was less prevalent overall (28.8% of polybacterial infections; 33.3% of monobacterial infections) and dominant in 25.4% of polybacterial infections,18 but consistent with the current understanding of the greater role of H. influenzae in pediatric conjunctivitis. In the current analysis, S. pneumoniae was also common, being the second most frequent causative/dominant organism from both monobacterial and polybacterial infections. S. mitis/S. mitis group, S. aureus, and S. epidermidis were more frequently isolated from polybacterial versus monobacterial infections, findings that are generally consistent with our prior non-pediatric-specific data,18 with the exception that the prevalence of S. mitis group species among polybacterial infections was higher in the current pediatric dataset (36.0% vs 13.6%).18
Viral coinfection was significantly more prevalent among polybacterial as compared to monobacterial pediatric conjunctivitis infections (5.2% vs 1.6%), although the actual number of such cases was relatively small. Other significant differences included the finding of S. pneumoniae being the dominant or causative infecting species in half as many polybacterial versus monobacterial infections (14.0% vs 28.1%), whereas S. mitis/S. mitis group and M. catarrhalis were the dominant or causative species in a greater percentage of polybacterial infections (8.7% vs 4.3% and 4.7% vs 0.5%, respectively). While S. mitis and other S. mitis group species have generally been characterized as benign commensal flora within the oral cavity, they have been reported to harbor virulence genes that confer resistance against host immune defenses33 and to exchange antibiotic resistance genes with other bacteria.34 Thus, our data suggest that S. mitis/S. mitis group may also be pathogenic in the eye. Similarly, the greater importance of M. catarrhalis in polybacterial infections is consistent with nasopharyngeal studies that suggest M. catarrhalis may promote a favorable environment for stable polymicrobial biofilms.35,36
Our findings indicate that polybacterial conjunctivitis with combinations of both Gram-positive and Gram-negative organisms is not uncommon among pediatric patients. Given the growing recognition of polybacterial infections in general,37–39 it follows that broad-spectrum coverage is an important characteristic when choosing antibiotic therapy for bacterial conjunctivitis. Further, bacterial resistance continues to be a concern among ocular pathogens.19,40–44 As a class, fluoroquinolones are widely used for bacterial conjunctivitis.45 Besifloxacin, the latest agent in this class, is a broad-spectrum chlorofluoroquinolone with potent bactericidal activity including activity against several drug-resistant pathogens.27,44,46–49 The besifloxacin molecule inhibits both bacterial DNA gyrase and topoisomerase IV in a balanced manner, thereby making it less likely for bacterial resistance to develop as compared to older-generation fluoroquinolones which preferentially target one of these enzymes.50,51 In the current analysis besifloxacin MIC90s ranged from 0.06–0.5 µg/mL and were the lowest or among the lowest MIC90s of all antibiotics tested, and were low both against Gram-positive and Gram-negative isolates.
MIC90s for each tested species and antibiotic were generally similar (within 1-fold dilution) for each, whether sourced from a monobacterial or polybacterial infection. The one exception was S. epidermidis for which MIC90s for all tested antibiotics were 3- to 5-fold higher among organisms sourced from polybacterial versus monobacterial infections, indicating lower in vitro potency. While research specific to the ocular surface is lacking, a growing body of data suggests the possibility of complex and synergistic interactions between different bacterial pathogens, or even between pathogens and commensal bacteria, that may contribute to the development of polymicrobial infections and possibly enhance organism virulence.52–56 While S. epidermidis is rarely a dominant species in polybacterial infections, it is possible that the presence of more highly resistant S. epidermidis strains creates an environment favorable for polybacterial infections, although additional studies are needed to confirm this. Further, S. epidermidis organisms sourced from conjunctivitis are frequently capable of forming biofilms,57–61 which may help confer such higher antibacterial resistance and enhance pathogen virulence.57,58
Bacterial eradication findings for the overall pediatric population in the current analysis were similar to our recent analysis based on non-age specific data from a subset of the same studies.18 Besifloxacin and moxifloxacin each demonstrated significantly greater bacterial eradication rates compared to vehicle in both monobacterial and polybacterial infections in the overall dataset, and, with one exception, in the subset of subjects between 1 year and 5 years of age at both follow-up timepoints evaluated (days 4 and 8); whereas only besifloxacin demonstrated significantly greater eradication rates vs vehicle in the subset of 1-year-old subjects, and only at day 4. However, the moxifloxacin 1-year-old subgroup was small.
This post hoc analysis was subject to several limitations. Although the total dataset was sizable, there were only few isolates for some specific species. With regard to rank-ordering infecting species for polybacterial infections, it is not known whether application of fold-differences in CFU/mL over the prespecified threshold criteria is an appropriate methodology. In vitro MIC data are of limited value for predicting susceptibility or resistance in ocular infections. Finally, although microbial eradication rates were provided to demonstrate the efficacy of besifloxacin, the resolution of clinical signs was not addressed.
Conclusions
This analysis of microbiological data from besifloxacin clinical trials revealed that the majority of conjunctivitis infections in pediatric subjects were characterized by the presence of H. influenzae, S. pneumoniae, S. aureus, and other Gram-positive organisms. Polybacterial infections were identified in approximately one-fourth of subjects, many of which exhibited combinations of Gram-positive and Gram-negative organisms. Differences in pathogen distribution included a greater preponderance of S. mitis/S. mitis group and M. catarrhalis and a lower preponderance of S. pneumoniae as dominant infecting species in polybacterial versus monobacterial infections. These findings highlight the importance of broad-spectrum coverage when choosing empiric therapy. In this pediatric cohort, besifloxacin therapy produced bacterial eradication in a large percentage of cases as early as day 4 of treatment, both in children with monobacterial and with polybacterial infections.
Acknowledgments
Medical writing assistance was provided by Churchill Communications (Maplewood, NJ), funded by Bausch + Lomb (a division of Bausch Health, LLC). Statistical analysis was conducted by H. Proskin, funded by Bausch + Lomb. Portions of this paper were presented at the American Academy of Pediatrics Virtual 2020 National Conference & Exhibition as a poster presentation with interim findings. The poster’s abstract was published in Pediatrics March 2021, 147 (3 MeetingAbstract) 296: https://doi.org/10.1542/peds.147.3_MeetingAbstract.296.
Author Contributions
JM Blondeau and HH DeCory contributed to the interpretation of the data, HM Proskin contributed to the analysis of the data, and CM Sanfilippo contributed to the analysis and interpretation of the data. JM Blondeau contributed to the study conception, HH DeCory contributed to the study design, and HM Proskin and CM Sanfilippo contributed to both the study design and conception. All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval for the version to be published; and agreed to be accountable for all aspects of the work.
Funding
The original studies included in this pooled analysis were funded by Bausch & Lomb Incorporated and involved the marketed product Besivance® (besifloxacin ophthalmic suspension, 0.6%).
Disclosure
HH DeCory & CM Sanfilippo are employees of Bausch Health US, LLC. Statistical analysis was conducted by HM Proskin, funded by Bausch Health US, LLC. JM Blondeau has received independent research grants from Bausch Health US, LLC. The authors report no other conflicts of interest in this work.
References
1. Hovding G. Acute bacterial conjunctivitis. Acta Ophthalmol. 2008;86:5–17. doi:10.1111/j.1600-0420.2007.01006.x
2. Block SL, Hedrick J, Tyler R, et al. Increasing bacterial resistance in pediatric acute conjunctivitis (1997–1998). Antimicrob Agents Chemother. 2000;44:1650–1654. doi:10.1128/AAC.44.6.1650-1654.2000
3. Buznach N, Dagan R, Greenberg D. Clinical and bacterial characteristics of acute bacterial conjunctivitis in children in the antibiotic resistance era. Pediatr Infect Dis J. 2005;24:823–828. doi:10.1097/01.inf.0000178066.24569.98
4. Weiss A, Brinser JH, Nazar-Stewart V. Acute conjunctivitis in childhood. J Pediatr. 1993;122(1):10–14. doi:10.1016/S0022-3476(05)83479-1
5. Azari AA, Barney NP. Conjunctivitis: a systematic review of diagnosis and treatment. JAMA. 2013;310(16):1721–1729. doi:10.1001/jama.2013.280318
6. Kunimoto DY, Das T, Sharma S, et al.; Endophthalmitis Research Group. Microbiologic spectrum and susceptibility of isolates: part I. Postoperative endophthalmitis. Am J Ophthalmol. 1999;128(2):240–242. doi:10.1016/S0002-9394(99)00112-9
7. Kunimoto DY, Das T, Sharma S, et al.; Endophthalmitis Research Group. Microbiologic spectrum and susceptibility of isolates: part II. Posttraumatic endophthalmitis. Am J Ophthalmol. 1999;128(2):242–244. doi:10.1016/S0002-9394(99)00113-0
8. Bourcier T, Thomas F, Borderie V, Chaumeil C, Laroche L. Bacterial keratitis: predisposing factors, clinical and microbiological review of 300 cases. Br J Ophthalmol. 2003;87(7):834–838. doi:10.1136/bjo.87.7.834
9. Lim NC, Lim DK, Ray M. Polymicrobial versus monomicrobial keratitis: a retrospective comparative study. Eye Contact Lens. 2013;39(5):348–354. doi:10.1097/ICL.0b013e3182a3024e
10. Hooi SH, Hooi ST. Culture-proven bacterial keratitis in a Malaysian general hospital. Med J Malaysia. 2005;60(5):614–623.
11. Stefan C, Nenciu A. Post-traumatic bacterial keratitis—a microbiological prospective clinical study. Oftalmologia. 2006;50(3):118–122.
12. Preechawat P, Ratananikom U, Lerdvitayasakul R, Kunavisarut S. Contact lens-related microbial keratitis. J Med Assoc Thai. 2007;90(4):737–743.
13. Termote K, Joe AW, Butler AL, et al. Epidemiology of bacterial corneal ulcers at tertiary centres in Vancouver, B.C. Can J Ophthalmol. 2018;53(4):330–336. doi:10.1016/j.jcjo.2017.11.001
14. Sowmya P, Madhavan HN. Diagnostic utility of polymerase chain reaction on intraocular specimens to establish the etiology of infectious endophthalmitis. Eur J Ophthalmol. 2009;19(5):812–817. doi:10.1177/112067210901900520
15. Pijl BJ, Theelen T, Tilanus MA, Rentenaar R, Crama N. Acute endophthalmitis after cataract surgery: 250 consecutive cases treated at a tertiary referral center in the Netherlands. Am J Ophthalmol. 2010;149(3):
16. Bhattacharjee H, Bhattacharjee K, Gogoi K, Singh M, Singla BG, Yadav A. Microbial profile of the vitreous aspirates in culture proven exogenous endophthalmitis: a 10-year retrospective study. Indian J Med Microbiol. 2016;34(2):153–158. doi:10.4103/0255-0857.180280
17. Wong T, Ormonde S, Gamble C, McGhee CNJ. Severe infective keratitis leading to hospital admission in New Zealand. Br J Ophthalmol. 2003;87(9):1103–1108. doi:10.1136/bjo.87.9.1103
18. DeCory HH, Sanfilippo CM, Proskin HM, Blondeau JM. Characterization of baseline polybacterial versus monobacterial infections in three randomized controlled bacterial conjunctivitis trials and microbial outcomes with besifloxacin ophthalmic suspension 0.6%. PLoS One. 2020;15(8):e0237603. doi:10.1371/journal.pone.0237603
19. Bhattacharyya A, Sarma P, Sarma B, et al. Bacteriological pattern and their correlation with complications in culture positive cases of acute bacterial conjunctivitis in a tertiary care hospital of upper Assam: a cross sectional study. Medicine (Baltimore). 2020;99(7):e18570. doi:10.1097/MD.0000000000018570
20. Hashish AA, Elbakary MA, Allam WA. Resistant infantile bacterial conjunctivitis in Egypt: a microbiology study. J Pediatr Ophthalmol Strabismus. 2018;55(2):135–139. doi:10.3928/01913913-20170718-01
21. Rose PW, Harnden A, Brueggemann AB, et al. Chloramphenicol treatment for acute infective conjunctivitis in children in primary care: a randomised double-blind placebo-controlled trial. Lancet. 2005;366(9479):37–43. doi:10.1016/S0140-6736(05)66709-8
22. Tepedino ME, Heller WH, Usner DW, et al. Phase III efficacy and safety study of besifloxacin ophthalmic suspension 0.6% in the treatment of bacterial conjunctivitis. Curr Med Res Opin. 2009;25(5):1159–1169. doi:10.1185/03007990902837919
23. McDonald MB, Protzko EE, Brunner LS, et al. Efficacy and safety of besifloxacin ophthalmic suspension 0.6% compared with moxifloxacin ophthalmic solution 0.5% for treating bacterial conjunctivitis. Ophthalmology. 2009;116(9):1615–1623.e1. doi:10.1016/j.ophtha.2009.05.014
24. Karpecki P, Depaolis M, Hunter JA, et al. Besifloxacin ophthalmic suspension 0.6% in patients with bacterial conjunctivitis: a multicenter, prospective, randomized, double-masked, vehicle-controlled, 5-day efficacy and safety study. Clin Ther. 2009;31(3):514–526. doi:10.1016/j.clinthera.2009.03.010
25. DeLeon J, Silverstein BE, Allaire C, et al. Besifloxacin ophthalmic suspension 0.6% administered twice daily for 3 days in the treatment of bacterial conjunctivitis in adults and children. Clin Drug Investig. 2012;32(5):303–317. doi:10.2165/11632470-000000000-00000
26. Malhotra R, Ackerman S, Gearinger LS, Morris TW, Allaire C. The safety of besifloxacin ophthalmic suspension 0.6% used three times daily for 7 days in the treatment of bacterial conjunctivitis. Drugs R D. 2013;13(4):243–252. doi:10.1007/s40268-013-0029-1
27. Haas W, Gearinger LS, Usner DW, Decory HH, Morris TW. Integrated analysis of three bacterial conjunctivitis trials of besifloxacin ophthalmic suspension, 0.6%: etiology of bacterial conjunctivitis and antibacterial susceptibility profile. Clin Ophthalmol. 2011;5:1369–1379. doi:10.2147/OPTH.S23519
28. Cagle G, Davis S, Rosenthal A, Smith J. Topical tobramycin and gentamicin sulfate in the treatment of ocular infections: multicenter study. Curr Eye Res. 1981;1(9):523–534. doi:10.3109/02713688109069178
29. Leibowitz HM. Antibacterial effectiveness of ciprofloxacin 0.3% ophthalmic solution in the treatment of bacterial conjunctivitis. Am J Ophthalmol. 1991;112(Suppl4):29S–33S.
30. Clinical and Laboratory Standards Institute. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically; Approved standards.
31. Clinical and Laboratory Standards Institute. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically; Approved standards.
32. Clinical and Laboratory Standards Institute. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically; Approved standard.
33. Rasmussen LH, Højholt K, Dargis R, et al. In silico assessment of virulence factors in strains of Streptococcus oralis and Streptococcus mitis isolated from patients with Infective Endocarditis. J Med Microbiol. 2017;66(9):1316–1323. doi:10.1099/jmm.0.000573
34. Mitchell J. Streptococcus mitis: walking the line between commensalism and pathogenesis. Mol Oral Microbiol. 2011;26(2):89–98. doi:10.1111/j.2041-1014.2010.00601.x
35. Bair KL, Campagnari AA. Moraxella catarrhalis promotes stable polymicrobial biofilms with the major otopathogens. Front Microbiol. 2020;10:3006. doi:10.3389/fmicb.2019.03006
36. Perez AC, Pang B, King LB, et al. Residence of Streptococcus pneumoniae and Moraxella catarrhalis within polymicrobial biofilm promotes antibiotic resistance and bacterial persistence in vivo. Pathog Dis. 2014;70(3):280–288. doi:10.1111/2049-632X.12129
37. Short FL, Murdoch SL, Ryan RP. Polybacterial human disease: the ills of social networking. Trends Microbiol. 2014;22(9):508–516. doi:10.1016/j.tim.2014.05.007
38. Brogden KA, Guthmiller JM, Taylor CE. Human polymicrobial infections. Lancet. 2005;365:253–255. doi:10.1016/S0140-6736(05)70155-0
39. Griffiths EC, Pedersen AB, Fenton A, Petchey OL. The nature and consequences of coinfection in humans. J Infect. 2011;63(3):200–206. doi:10.1016/j.jinf.2011.06.005
40. Silvester A, Neal T, Czanner G, Briggs M, Harding S, Kaye S. Adult bacterial conjunctivitis: resistance patterns over 12 years in patients attending a large primary eye care centre in the UK. BMJ Open Ophthalmol. 2016;1(1):e000006. doi:10.1136/bmjophth-2016-000006
41. Shrestha SP, Khadka J, Pokhrel AK, Sathian B. Acute bacterial conjunctivitis—antibiotic susceptibility and resistance to commercially available topical antibiotics in Nepal. Nepal J Ophthalmol. 2016;8(15):23–35. doi:10.3126/nepjoph.v8i1.16153
42. Asbell PA, DeCory HH. Antibiotic resistance among bacterial conjunctival pathogens collected in the Antibiotic Resistance Monitoring in Ocular Microorganisms (ARMOR) surveillance study. PLoS One. 2018;13(10):e0205814. doi:10.1371/journal.pone.0205814
43. Alter SJ, Sanfilippo CM, Asbell PA, DeCory HH. Antibiotic resistance among pediatric-sourced ocular pathogens: 8-year findings from the Antibiotic Resistance Monitoring in Ocular Microorganisms (ARMOR) surveillance study. Pediatr Infect Dis J. 2019;38:138–145. doi:10.1097/INF.0000000000002206
44. Asbell PA, Sanfilippo CM, Sahm DF, DeCory HH. Trends in antibiotic resistance among ocular microorganisms in the United States from 2009 to 2018. JAMA Ophthalmol. 2020;138(5):1–12. doi:10.1001/jamaophthalmol.2020.0155
45. Research and Markets. Global conjunctivitis drugs market 2018–2024. Available from: https://www.researchandmarkets.com/research/xx9d9p/global?w=5.
46. Haas W, Pillar CM, Zurenko GE, Lee JC, Brunner LS, Morris TW. Besifloxacin, a novel fluoroquinolone, has broad-spectrum in vitro activity against aerobic and anaerobic bacteria. Antimicrob Agents Chemother. 2009;53(8):3552–3560. doi:10.1128/AAC.00418-09
47. Haas W, Pillar CM, Hesje CK, Sanfilippo CM, Morris TW. Bactericidal activity of besifloxacin against staphylococci, Streptococcus pneumoniae and Haemophilus influenzae. J Antimicrob Chemother. 2010;65(7):1441–1447. doi:10.1093/jac/dkq127
48. Haas W, Sanfilippo CM, Hesje CK, Morris TW. Contribution of the R8 substituent to the in vitro antibacterial potency of besifloxacin and comparator ophthalmic fluoroquinolones. Clin Ophthalmol. 2013;7:821–830. doi:10.2147/OPTH.S44085
49. Miller D, Chang JS, Flynn HW, Alfonso EC. Comparative in vitro susceptibility of besifloxacin and seven comparators against ciprofloxacin- and methicillin-susceptible/nonsusceptible staphylococci. J Ocul Pharmacol Ther. 2013;29(3):339–344. doi:10.1089/jop.2012.0081
50. Cambau E, Matrat S, Pan XS, et al. Target specificity of the new fluoroquinolone besifloxacin in Streptococcus pneumoniae, Staphylococcus aureus and Escherichia coli. J Antimicrob Chemother. 2009;63(3):443–450. doi:10.1093/jac/dkn528
51. Mah FS, Sanfilippo CM. Besifloxacin: efficacy and safety in treatment and prevention of ocular bacterial infections. Ophthalmol Ther. 2016;5:1–20. doi:10.1007/s40123-016-0046-6
52. Murray JL, Connell JL, Stacy A, Turner KH, Whiteley M. Mechanisms of synergy in polymicrobial infections. J Microbiol. 2014;52(3):188–199. doi:10.1007/s12275-014-4067-3
53. Hendricks KJ, Burd TA, Anglen JO, Simpson AW, Christensen GD, Gainor BJ. Synergy between Staphylococcus aureus and Pseudomonas aeruginosa in a rat model of complex orthopaedic wounds. J Bone Joint Surg Am. 2001;83(6):855–861. doi:10.2106/00004623-200106000-00006
54. Bousbia S, Raoult D, La Scola B. Pneumonia pathogen detection and microbial interactions in polymicrobial episodes. Future Microbiol. 2013;8(5):633–660. doi:10.2217/fmb.13.26
55. Shak JR, Vidal JE, Klugman KP. Influence of bacterial interactions on pneumococcal colonization of the nasopharynx. Trends Microbiol. 2013;21(3):129–135. doi:10.1016/j.tim.2012.11.005
56. Nguyen AT, Oglesby-Sherrouse AG. Interactions between Pseudomonas aeruginosa and Staphylococcus aureus during co-cultivations and polymicrobial infections. Appl Microbiol Biotechnol. 2016;100(14):6141–6148. doi:10.1007/s00253-016-7596-3
57. Catalanotti P, Lanza M, Del Prete A, et al. Staphylococcus epidermidis and S. aureus in acute bacterial conjunctivitis in soft contact lens wearers. New Microbiol. 2005;28(4):345–454.
58. Murugan K, Usha M, Malathi P, Al-Sohaibani AS, Chandrasekaran M. Biofilm forming multi drug resistant Staphylococcus spp. among patients with conjunctivitis. Pol J Microbiol. 2010;59(4):233–239. doi:10.33073/pjm-2010-036
59. Flores-Páez LA, Zenteno JC, Alcántar-Curiel MD, et al. Molecular and phenotypic characterization of Staphylococcus epidermidis isolates from healthy conjunctiva and a comparative analysis with isolates from ocular infection. PLoS One. 2015;10(8):e0135964. doi:10.1371/journal.pone.0135964
60. Fariña N, Samudio M, Carpinelli L, Nentwich MM, de Kaspar HM. Methicillin resistance and biofilm production of Staphylococcus epidermidis isolates from infectious and normal flora conjunctiva. Int Ophthalmol. 2017;37(4):819–825. doi:10.1007/s10792-016-0339-8
61. Elkhashab THT, Adel LA, Nour MS, Mahran M, Elkaffas M. Association of intercellular adhesion gene A with biofilm formation in staphylococci isolates from patients with conjunctivitis. J Lab Physicians. 2018;10(3):309–315. doi:10.4103/JLP.JLP_122_17
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.