Back to Journals » Clinical Ophthalmology » Volume 19
Characteristics of Normal Tension Glaucoma Referrals at a Tertiary Care Center and Factors Associated with Unilateral versus Bilateral Disease
Authors Yazdanie F, Sims JR ![]() , Ying S
, Ying S ![]() , Misra P, Shah M, Panarelli JF
, Misra P, Shah M, Panarelli JF
Received 8 August 2024
Accepted for publication 3 March 2025
Published 31 March 2025 Volume 2025:19 Pages 1175—1182
DOI https://doi.org/10.2147/OPTH.S490512
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Fahd Yazdanie,1 Jeffrey R Sims,1 Stephanie Ying,2 Poonam Misra,3 Manjool Shah,1,4 Joseph F Panarelli1
1Department of Ophthalmology, NYU Langone Health, New York, NY, USA; 2Department of Ophthalmology, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 3Department of Ophthalmology, Manhattan Eye, Ear & Throat Hospital, Northwell Health, New York, NY, USA; 4Department of Ophthalmology and Visual Sciences, University of Michigan Kellogg Eye Center, Ann Arbor, MI, USA
Correspondence: Joseph F Panarelli, Department of Ophthalmology, NYU Langone Health, 222 E. 41st St, 4th Floor, New York, NY, 10017, USA, Tel +1 347-302-4326, Email [email protected]
Purpose: To determine the characteristics of normal tension glaucoma referrals at a tertiary care center and risk factors associated with unilateral versus bilateral disease.
Patients and Methods: Medical records were reviewed of patients who were referred to a single glaucoma provider at a tertiary care center and were given a presumptive diagnosis of normal tension glaucoma (NTG) between the years 2018 and 2021. Data collected included demographics, medical and family history, ophthalmic history, ophthalmic examination findings, neuro-ophthalmology referrals, and magnetic resonance imaging (MRI) results.
Results: A total of 98 patients were included in this study. The majority of patients (82%) had bilateral disease at initial presentation. Most patients (65%) had a history of systemic disease, including hypertension (32%), cardiovascular disease (19%), diabetes (12%), obstructive sleep apnea (10%), or orthostatic hypotension (4%). Conditions associated with vascular dysregulation were identified in 24% of patients. Sixty six percent of patients had a family history of glaucoma, while nearly half (49%) were myopic. Of patients with unilateral disease, 39% had workup or consideration of other neuro-ophthalmic diagnoses compared to 13% of patients with bilateral disease (P = 0.01).
Conclusion: Patients referred for NTG commonly present with disc changes in both eyes. Clinicians should assess for the presence of systemic diseases associated with vascular dysregulation, myopia, and a family history of glaucoma. Patients with unilateral disease consistent with NTG may benefit from additional workup including neuroimaging or a neuro-ophthalmic evaluation.
Keywords: normal tension glaucoma, intraocular pressure, optic neuropathy, myopia, masquerading
Introduction
Normal tension glaucoma (NTG), also known as low-tension glaucoma (LTG), is a glaucomatous optic neuropathy characterized by progressive optic nerve damage associated with visual field loss with intraocular pressure (IOP) that is 21 mm Hg or less. Globally, NTG is a significant disease entity. In Japanese populations in particular, NTG has been reported to constitute the majority of open-angle glaucoma cases, with prevalence rates ranging from 52 to 92%.1 Furthermore, it is estimated that 50% of patients in the world with undiagnosed glaucoma have IOP below 21 mm Hg.2 It is theorized that NTG may be associated with vascular dysregulation leading to ocular hypoperfusion and subsequent damage to the retinal ganglion cells.3 While studies show a correlation between NTG and underlying systemic diseases such as systemic hypotension, migraines, Raynaud’s phenomenon, and sleep apnea,4 NTG has been difficult to conceptualize, given a lack of understanding of the precise etiology of NTG and the lack of elevated intraocular pressure (IOP). It can be difficult to distinguish NTG from other disease entities, particularly nonprogressive optic neuropathies, vascular injuries, compressive lesions of the optic nerve and chiasm, and ischemic optic neuropathies.5,6 Myopia can also masquerade as NTG given the tilted appearance of the disc and thinning of the nerve fiber layer.
NTG can present asymmetrically, with studies suggesting a similar prevalence of unilateral visual field loss between NTG and high-tension glaucoma patients.7 Other studies postulate, however, that NTG may be more dependent on systemic rather than ocular factors and is, therefore, usually more symmetric compared to diagnoses such as primary open angle glaucoma (POAG).8 Nonetheless, over the course of time, NTG patients with unilateral visual field (VF) loss may eventually develop VF loss in the other eye,7 but a general consensus has not yet been reached on whether treatment of the fellow eye in patients with unilateral NTG is necessary and, if necessary, when to initiate treatment.9
Improved understanding of the clinical profile and characteristics of patients with NTG can help to further elucidate the ambiguity of NTG as a clinical entity. In this retrospective study, we aim to understand and analyze the characteristics of patients given a presumptive diagnosis of NTG at a tertiary care center and identify factors associated with unilateral versus bilateral disease.
Materials and Methods
The medical records of patients presenting with possible normal tension glaucoma or low-tension glaucoma during their first visit with a single glaucoma specialist from 2018 to 2021 at New York University (NYU) Langone Health were reviewed retrospectively. Patients were identified via diagnosis codes in the electronic medical record system. All patients included were over 18 years of age and had a maximum IOP of 21 mm Hg or less.
Data was collected including demographics, medical and surgical history, family history, ophthalmic history, ophthalmic examination findings, neuro-ophthalmology referrals, and MRI results. This study adhered to the tenets of the Declaration of Helsinki and was approved by and conducted under the policies of the NYU Institutional Review Board. This retrospective chart review was exempt from the requirement for individual patient informed consent, per the Institutional Review Board, given inclusion in this retrospective chart review without intervention presented no more than minimal risk of harm. Patient confidentiality was maintained in accordance with NYU standards for protected health information and data protection, including deidentification of patient information.
Statistical Analyses
Statistical analyses were performed through IBM SPSS Statistics Version 29.0.0.0 for Macintosh (IBM Corp, Armonk, NY). A P value ≤ 0.05 was considered statistically significant. All categorical variables were compared using a Fisher’s Exact test or chi-square analysis. A univariate logistic regression model was used to compare factors in patients who presented with unilateral versus bilateral NTG.
Results
Patient Demographics and Baseline Characteristics
Ninety-eight patients who were referred and given an initial diagnosis of NTG by a single glaucoma specialist from 2018 to 2021 were included in the study. Demographics and baseline characteristics are reported in Table 1. Two-thirds of the patients were female (66 patients, 67%), with an overall mean age of 70.4 years. Almost half of the patients were White (47 patients, 48%) and 20% were Asian. Over 80% of patients presented with bilateral disease, with 8% presenting with disc changes in the right eye alone and 10% in the left eye alone. Twenty-nine percent of patients were on an oral beta-blocker. Sixty-five percent of patients had a history of systemic disease, with the most prevalent diseases being hypertension (32%), cardiovascular disease (19%), diabetes mellitus (12%), and obstructive sleep apnea (10%). Twenty four percent of patients had conditions associated with vascular dysregulation (i.e. orthostatic hypotension (4%), Raynaud’s phenomenon, migraine, etc). Almost half of the patients were myopic, with 28% presenting with “low” myopia (≥1.00 and < 6.00 diopters of myopia) and 21% presenting with “high” myopia (≥6.00 diopters of myopia).
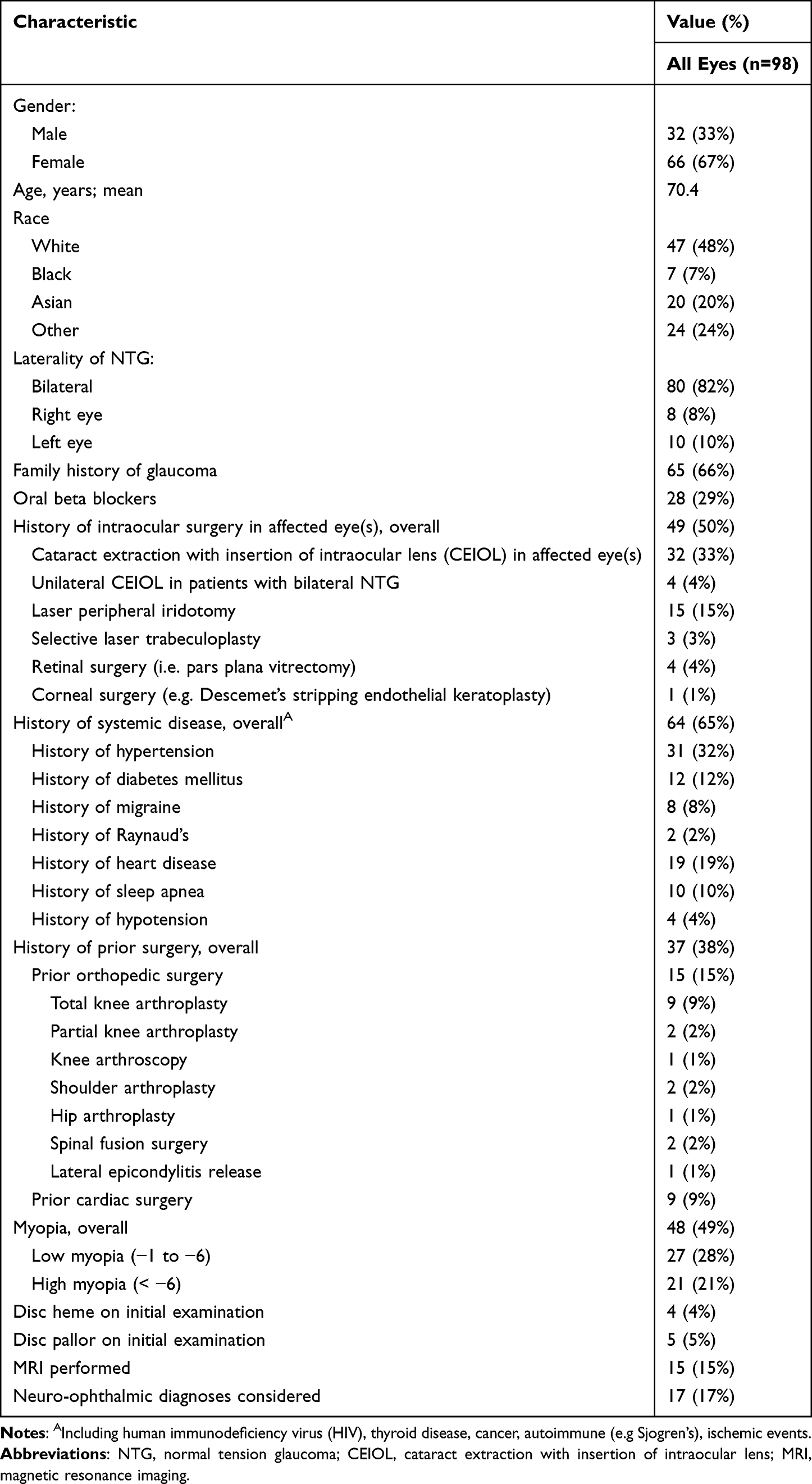 |
Table 1 Demographics and Baseline Characteristics of Patients of All Patients Given the Initial Diagnosis of Normal Tension Glaucoma (NTG) |
Overall, 17/98 (17%) patients had either a history of or consideration of neuro-ophthalmic diagnoses in the corresponding eye(s), with 15 total patients having MRI performed either before or after their initial visit with the glaucoma specialist.
Neuro-Ophthalmic Evaluation in NTG Patients
Of the 17 patients who had either a history of or consideration of neuro-ophthalmic diagnoses in the corresponding eye(s) (Table 2), 6 patients were diagnosed with potential compressive optic neuropathy (35%), 2 with potential anterior ischemic optic neuropathy (12%), 1 with potential optic neuritis (6%), and 8 were given a diagnosis of unspecified non-glaucomatous optic neuropathy (47%).
 |
Table 2 Outline of Neuro-Ophthalmic Evaluation Reported in the NTG Patient Cohort |
Of the patients with potential compressive optic neuropathy, 1 had a pituitary adenoma, 1 had a posterior orbital hemangioma, 1 had buccal mucosa and tonsillar squamous cell carcinoma, and 1 had an optic nerve sheath meningioma. One patient was found to have a congenitally small optic chiasm of unclear significance on MRI.
Factors Associated with Unilateral versus Bilateral NTG
Eighteen of the 98 patients presented with unilateral NTG. Among these patients, univariate logistic regressions (Table 3) identified history of diabetes mellitus (Odds Ratio [OR] = 4.01; P = 0.03), and history of prior orthopedic or heart surgery (OR = 3.26; P = 0.03) as predisposing factors associated with unilateral as opposed to bilateral NTG. No other variables included were statistically significant in the univariate analyses.
 |
Table 3 Predisposing Factors Associated with Unilateral Normal Tension Glaucoma |
Additional factors related to the clinical course of the NTG patient cohort were also analyzed in relation to unilateral versus bilateral presentation. These factors are outlined in Table 4. A significantly lower percentage of patients with unilateral presentations were on glaucoma treatment prior to referral compared to patients with bilateral presentations (44% vs 70%, P = 0.03). In addition, a significantly higher percentage of unilateral NTG patients had a history or consideration of an alternative neuro-ophthalmic diagnosis, including those outlined in Table 3 (39% vs 13%, P = 0.01) compared to bilateral NTG patients.
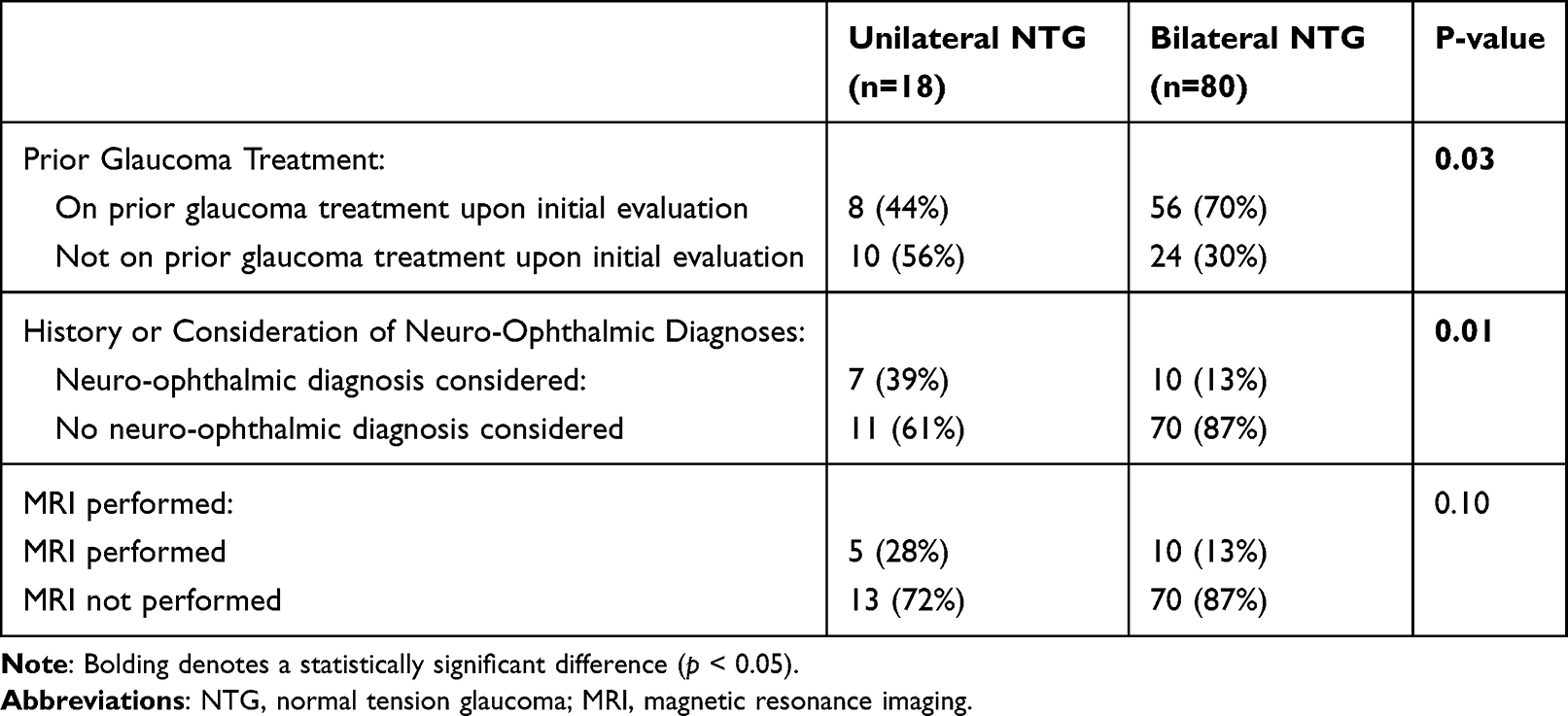 |
Table 4 Additional Factors in the Clinical Course Associated with Unilateral versus Bilateral NTG Patients |
Discussion
Normal tension glaucoma can present in a number of ways and tends to be a diagnosis of exclusion. Patients may have varying degrees of disc damage and visual field loss. Classic findings on examination include deep, focal notching of the disc or a shallow, saucerous appearing cup. It has been found to be more common in female than male individuals, as was also the case in our study.10 Systemic diseases that are associated with vascular dysregulation or vasospasm are thought to play a role in the pathophysiology of this disease, with disorders including Raynaud’s phenomenon and migraine having a stronger association with NTG than POAG.11 One study found that headache with or without migraine features was reported by 86% of NTG patients, compared to 68% of POAG patients.12 In the Collaborative Normal Tension Glaucoma Study, migraine and Raynaud’s phenomenon were found in 15.63% and 3.75% of NTG patients, respectively.10 Vascular dysregulation is the inability of tissue to maintain a stable blood supply despite changes in perfusion pressure. Ongoing poor ocular perfusion in the setting of potentially weaker lamina cribrosa structures is thought to cause ischemia to the optic nerve causing progressive damage despite normal IOP.13,14 As a result, nocturnal hypotension, which can be physiologic or caused by systemic antihypertensives, may contribute to disease progression.15 In our cohort of patients, 24/98 (24%) had diagnoses associated with vascular dysregulation including migraine, Raynaud’s disease, hypotension, or obstructive sleep apnea. In our practice, all patients who present for evaluation of NTG are routinely asked about these conditions, as well as treatment modalities for hypertension. Though IOP remains the only proven modifiable risk factor, treatment or modification of treatment of these underlying conditions may help in preventing further visual field loss.
While IOP-independent risk factors such as vascular dysregulation are considered to play a key role in the pathophysiology of NTG, some forms of NTG may simply be a subset under the POAG umbrella. This is supported by the idea that the main modifiable risk factor in NTG is still IOP reduction.16,17 In our population, a significant portion of patients (41%) had neither myopia nor any symptoms of vascular dysregulation. We suspect that certain patients with NTG are predisposed to optic nerve damage at lower IOP due to other risk factors. Interestingly, a substantial portion of our population (66%) in this study had a family history of glaucoma. There might be a genetic predisposition that accounts for this finding, with studies showing certain genes associated with NTG, but more evidence is needed to support this theory.18 In the end, the answer is still not clear and further research into the pathogenesis of NTG is needed.
Numerous studies show a strong correlation between myopia and glaucoma. In our study population, nearly half of the patients were myopic 48/98 (49%). Additionally, 21/98 (21%) had high myopia with a spherical equivalence of at least 6 diopters of myopia. This correlation is still not well understood since patients with myopia who are treated for glaucoma may have IOP within normal range and may not display progression in their visual field defects.19 One theory suggests that patients with myopia who are also treated for glaucoma may have greater fluctuations in their IOP causing progressive nerve damage.20 However, it is also plausible that myopia may masquerade as glaucoma, especially when myopic patients lack the risk factor of elevated IOP. The myopic fundus may cause changes in the appearance of the nerve as well as nerve fiber layer thinning and visual field defects that could be interpreted as glaucoma. It is possible these changes may be attributed to myopia alone, and normative databases for nerve fiber layer thickness may be inaccurate for myopic patients.19,21 However, without evidence of progressive optic neuropathy, a true diagnosis of glaucoma is difficult to establish.
Glaucoma is generally believed to be a bilateral disease process, although it can be asymmetric. Our study results revealed 80/98 (82%) of patients had bilateral eye involvement, suggesting that NTG also follows a similar pattern to traditional glaucoma. Our patients with unilateral NTG had a statistically significant greater probability of undergoing neuro-ophthalmic work up (39%) compared to bilateral NTG (13%). Of the seventeen patients undergoing neuro-ophthalmic workup, 9/17 (53%) had an identifiable non-glaucomatous cause of optic nerve damage, with 6 of these patients having possible compressive optic neuropathy. As expected, significantly more patients with unilateral NTG received an MRI study (28%) compared to bilateral NTG (13%). This underscores the importance of assessing for alternate causes of optic nerve damage in patients with normal IOP and unilateral disease since the diagnosis may not be consistent with glaucoma. Normal tension glaucoma should be a diagnosis of exclusion in the face of certain pre-existing factors, especially unilateral disease. The pursuit of further workup and imaging could also potentially detect signs of life-threatening intracranial or systemic disease, and the ophthalmologist may be the first to diagnose it.
Our cohort of patients with unilateral disease were more likely than those with bilateral disease to have a prior history of orthopedic or cardiac surgery (P = 0.03). We hypothesize that major surgeries with prolonged anesthesia time, especially orthopedic or cardiac surgeries, can be associated with significant blood pressure fluctuations or even prolonged hypotension. This could result in nonperfusion to the optic nerve via a mechanism that is similar to hypovolemic shock, another suggested mechanism for the development of NTG.22 Patients who experience an isolated injury to the nerve associated with blood pressure fluctuations from major surgery may have asymmetric involvement of one eye, which may not progress further to involve the other eye.
Glaucoma specialists have varying practice patterns when managing NTG. Our patients were managed by a single glaucoma provider at a tertiary care center. Given the different mechanisms that could be involved in the pathophysiology of NTG, it is important to obtain adequate testing and stratify the risk factors associated with each patient. All patients may benefit from baseline testing such as visual fields and optical coherence tomography with serial imaging to determine which patients are at highest risk of progression. Approximately 64% of involved eyes in this study had confirmed visual field defects at the time of presentation, ranging from enlarged blind spots to arcuate defects to central field loss. Such findings can be crucial in guiding monitoring intervals, choice among management options, and potential diagnostic workup for findings that are less suggestive of glaucomatous disease. For example, visual field defects that do not respect the horizontal meridian can be highly suggestive of intracranial etiologies that require potentially life-saving evaluation.
The main limitation of our study is the sample size of patients as well as the retrospective nature of the analysis. Our patients were recruited based on searching the charts for the billing code of NTG. It is very possible that some patients with NTG were labeled as POAG or even as glaucoma suspects, thus not truly representing the total number of referrals for this condition. A prospective evaluation would clearly be of greater utility.
Conclusion
This study demonstrates that patients referred for NTG often have bilateral disease and common risk factors including vascular dysregulation, family history of glaucoma, and myopia. Vascular dysregulation may be involved in the pathogenesis of NTG, leading to progressive optic nerve damage from ischemia. Some forms of NTG may be a subtype of POAG, especially in patients with a strong family history of glaucoma and those lacking vascular risk factors. Myopia can also be associated with NTG, which could potentially predispose patients to develop glaucoma, but could also cause nonprogressive changes in the optic nerve that may be masquerading as glaucoma. Patients with unilateral disease may have alternate pathology that explains optic nerve damage, including neuro-ophthalmic causes and possible prior ischemic damage from prolonged surgery. A prospective study would be useful to determine which characteristics in NTG are most associated with progression.
Abbreviations
IOP, intraocular pressure; LTG, low tension glaucoma; MRI, magnetic resonance imaging; NTG, normal tension glaucoma; OR, odds ratio; POAG, primary open angle glaucoma; SLT, selective laser trabeculoplasty; VF, visual field.
Funding
Department of Ophthalmology, NYU Langone Health, New York, NY. Supported by an unrestricted grant from Research to Prevent Blindness.
Disclosure
The following authors report no financial disclosures or other conflicts of interest: Fahd Yazdanie, Stephanie Ying, Jeffrey Sims, and Poonam Misra. Joseph Panarelli reports financial relationships as a consultant or speaker with: AbbVie, Aerie Pharma, Alcon, Avisi Technologies, CorNeat, Glaukos, New World Medical, Santen, Nova Eye Medical, Ocular Therapeutics, Ellios, AOI Ophthalmics, and Zeiss. Manjool Shah reports financial relationships as a consultant with: Glaukos, AbbVie, ONL Therapeutics, Bausch and Lomb, and Alcon. Manjool Shah reports personal fees from AbbVie, personal fees from Alcon, personal fees from Glaukos, personal fees from Onl therapeutics, personal fees from Bausch and Lomb, outside the submitted work.
References
1. Cho HK, Kee C. Population-based glaucoma prevalence studies in Asians. Surv Ophthalmol. 2014;59(4):434–447. doi:10.1016/j.survophthal.2013.09.003
2. Shields MB. Normal-tension glaucoma: is it different from primary open-angle glaucoma? Curr Opin Ophthalmol. 2008;19(2):85–88. doi:10.1097/ICU.0b013e3282f3919b
3. Killer HE, Pircher A. Normal tension glaucoma: review of current understanding and mechanisms of the pathogenesis. Eye (Lond). 2018;32(5):924–930. doi:10.1038/s41433-018-0042-2
4. Fan N, Tan J, Liu X. Is “normal tension glaucoma” glaucoma? Med Hypotheses. 2019;133:109405. doi:10.1016/j.mehy.2019.109405
5. Ahmed II, Feldman F, Kucharczyk W, Trope GE. Neuroradiologic screening in normal-pressure glaucoma: study results and literature review. J Glaucoma. 2002;11(4):279–286. doi:10.1097/00061198-200208000-00002
6. Kim JA, Lee EJ, Kim TW, Yang HK, Hwang JM. Comparison of optic nerve head microvasculature between normal-tension glaucoma and nonarteritic anterior ischemic optic neuropathy. Invest Ophthalmol Vis Sci. 2021;62(10):15. doi:10.1167/iovs.62.10.15
7. Poinoosawmy D, Fontana L, Wu JX, Bunce CV, Hitchings RA. Frequency of asymmetric visual field defects in normal-tension and high-tension glaucoma. Ophthalmology. 1998;105(6):988–991. doi:10.1016/S0161-6420(98)96049-3
8. Kosior-Jarecka E, Wrobel-Dudzinska D, Pietura R, et al. Results of neuroimaging in patients with atypical normal-tension glaucoma. Biomed Res Int. 2020;2020(1):9093206. doi:10.1155/2020/9093206
9. Cho HK, Suh W, Kee C. Visual and structural prognosis of the untreated fellow eyes of unilateral normal tension glaucoma patients. Graefes Arch Clin Exp Ophthalmol. 2015;253(9):1547–1555. doi:10.1007/s00417-015-3081-4
10. Drance S, Anderson DR, Schulzer M, Collaborate Normal-Tension Glaucoma Study Group. Risk factors for progression of visual field abnormalities in normal-tension glaucoma. Am J Ophthalmol. 2001;131(6):699–708. doi:10.1016/S0002-9394(01)00964-3
11. Mallick J, Devi L, Malik P, Mallick J. Update on Normal Tension Glaucoma. J Ophthalmic Vis Res. 2016;11(2):204–208. doi:10.4103/2008-322X.183914
12. Phelps CD, Corbett JJ. Migraine and low-tension glaucoma. A case-control study. Invest Ophthalmol Vis Sci. 1985;26(8):1105–1108.
13. Flammer J, Mozaffarieh M. What is the present pathogenetic concept of glaucomatous optic neuropathy? Surv Ophthalmol. 2007;52(Suppl 2):S162–173. doi:10.1016/j.survophthal.2007.08.012
14. Muthu Krishnan V, Datta Gulnar P, Vasudev Anand R, Vijayakumar C, Balasubramaniyan G. Ocular and Systemic Risk Factors and Correlation with Glaucomatous Damage in Normal Tension Glaucoma. Cureus. 2018;10(5):e2638. doi:10.7759/cureus.2638
15. Charlson ME, de Moraes CG, Link A, et al. Nocturnal systemic hypotension increases the risk of glaucoma progression. Ophthalmology. 2014;121(10):2004–2012. doi:10.1016/j.ophtha.2014.04.016
16. Song BJ, Caprioli J. New directions in the treatment of normal tension glaucoma. Indian J Ophthalmol. 2014;62(5):529–537. doi:10.4103/0301-4738.133481
17. Costagliola C, Agnifili L, Mastropasqua L, Di Costanzo A. Low-Tension Glaucoma: an Oxymoron in Ophthalmology. Prev Chronic Dis. 2019;16:E10. doi:10.5888/pcd16.180534
18. Wiggs JL, Pasquale LR. Genetics of glaucoma. Hum Mol Genet. 2017;26(R1):R21–R27. doi:10.1093/hmg/ddx184
19. Chang RT, Singh K. Myopia and glaucoma: diagnostic and therapeutic challenges. Curr Opin Ophthalmol. 2013;24(2):96–101. doi:10.1097/ICU.0b013e32835cef31
20. Yang Y, Li Z, Wang N, et al. Intraocular pressure fluctuation in patients with primary open-angle glaucoma combined with high myopia. J Glaucoma. 2014;23(1):19–22. doi:10.1097/IJG.0b013e31825afc9d
21. Rauscher FM, Sekhon N, Feuer WJ, Budenz DL. Myopia affects retinal nerve fiber layer measurements as determined by optical coherence tomography. J Glaucoma. 2009;18(7):501–505. doi:10.1097/IJG.0b013e318193c2be
22. Kosior-Jarecka E, Lukasik U, Wrobel-Dudzinska D, et al. Risk Factors for Normal and High-Tension Glaucoma in Poland in Connection with Polymorphisms of the Endothelial Nitric Oxide Synthase Gene. PLoS One. 2016;11(1):e0147540. doi:10.1371/journal.pone.0147540
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Considerations for Glaucoma Evaluation and Management in Refractive Surgery Candidates
Seresirikachorn K, Zhu AY, Chang TC
Clinical Ophthalmology 2025, 19:4941-4950
Published Date: 30 December 2025