Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Characteristics of COPD Phenotypes in Serbia
Authors Lazic Z ![]() , Stankovic I, Milenkovic B
, Stankovic I, Milenkovic B ![]() , Zvezdin B
, Zvezdin B ![]() , Hromis S
, Hromis S ![]() , Jankovic S
, Jankovic S ![]() , Cupurdija V
, Cupurdija V ![]()
Received 6 January 2021
Accepted for publication 1 March 2021
Published 16 March 2021 Volume 2021:16 Pages 643—654
DOI https://doi.org/10.2147/COPD.S300693
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
Zorica Lazic,1 Ivana Stankovic,2 Branislava Milenkovic,3 Biljana Zvezdin,4 Sanja Hromis,4 Slobodan Jankovic,5 Vojislav Cupurdija1
1Faculty of Medical Sciences, University of Kragujevac, and Clinic for Pulmonology, Clinical Centre, Kragujevac, Serbia; 2Faculty of Medicine, University of Niš, and Clinic for Lung Diseases, Clinical Centre, Niš, Serbia; 3Faculty of Medicine, University of Belgrade, and Clinic for Pulmonology, Clinical Centre of Serbia, Belgrade, Serbia; 4Faculty of Medicine, University of Novi Sad, and the Institute for Pulmonary Diseases of Vojvodina, Novi Sad, Serbia; 5Faculty of Medical Sciences, University of Kragujevac, and Clinical Pharmacology Department, Clinical Centre, Kragujevac, Serbia
Correspondence: Slobodan Jankovic
Faculty of Medical Sciences, University of Kragujevac, Svetozara Markovića Street, 69, Kragujevac, 34000, Serbia
Email [email protected]
Background: Establishing a regional/national/international registry of patients suffering from chronic obstructive pulmonary disease (COPD) is essential for both research and healthcare, because it enables collection of comprehensive real-life data from a large number of individuals.
Objective: The aim of this study was to describe characteristics of COPD patients from the Serbian patient registry, and to investigate actual differences of those characteristics among the COPD phenotypes.
Methods: The Serbian registry of patients with COPD was established in 2018 at University of Kragujevac, Faculty of Medical Sciences, based on an online platform. Entry in the Registry was allowed for patients who were diagnosed with COPD according to the following criteria: symptoms of dyspnea, chronic cough or sputum production, history of risk factors for COPD and any degree of persistent airflow limitation diagnosed at spirometry.
Results: In the Serbian COPD registry B and D GOLD group were dominant, while among the COPD phenotypes, the most prevalent were non-exacerbators (49.4%) and then frequent exacerbators without chronic bronchitis (29.6%). The frequent exacerbator with chronic bronchitis phenotype was associated with low levels of bronchopulmonary function and absolute predominance of GOLD D group. Anxiety, depression, insomnia, hypertension and chronic heart failure were the most prevalent in the frequent exacerbator with chronic bronchitis phenotype; patients with this phenotype were also treated more frequently than other patients with a triple combination of the most effective inhaled anti-obstructive drugs: long-acting muscarinic antagonists, long-acting beta 2 agonists and corticosteroids.
Conclusion: In conclusion, the data from the Serbian registry are in line with those from other national registries, showing that frequent exacerbators with chronic bronchitis have worse bronchopulmonary function, more severe signs and symptoms, and more comorbidities (especially anxiety and depression) than other phenotypes. Other studies also confirmed worse quality of life and worse prognosis of the AE-CB phenotype, stressing importance of both preventive and appropriate therapeutic measures against chronic bronchitis.
Keywords: chronic obstructive pulmonary disease, patient registry, phenotypes
Introduction
True effectiveness of various types of treatments or performance of a diagnostic test remain hidden until studies are performed in real-life settings, i.e., in large samples that are representative of the target population.1 In this sense establishing regional/national/international registries of patients suffering from the same disease is of great help, because it enables collection of comprehensive real-life data from a large number of individuals.2 Although chronic obstructive pulmonary disease (COPD) is one of the most common chronic non-contagious diseases, and places a substantial burden on society, its patient registries are not readily available. Some of the COPD patient registries are part of a wider collection of patient data, as in Denmark, which then may lack some specific, yet important variables that characterize severity or prognosis of COPD.3 The others are strictly national, making transferability of the results to other populations questionable, especially when there are also racial differences among the nations.4 Registries formed for the purpose of an epidemiological study or project are with limited duration and size,5 and access to the raw data is usually restricted to uninvolved researchers. There is a clear need to have a national or regional COPD patient registry in every country, in order to promote and enhance clinical research of this disease, and that is why the Serbian COPD patient registry was established.
Although there are different opinions among experts about the number and characteristics of COPD phenotypes,6 almost all agree about the four main phenotypes. Non-exacerbators (NON-AE) are patients with one or no exacerbations during the last year, and frequent exacerbators without chronic bronchitis (AE NON-CB) are those who had two or more exacerbations per year; if the latter patients also suffer from chronic bronchitis, they are re-classified to frequent exacerbators with chronic bronchitis phenotype (AE-CB). Asthma–COPD overlap syndrome (ACOS) includes patients diagnosed with asthma before their 40th birthday or having a positive bronchodilator test in the last year with proofs of allergy and/or atopy. The importance of COPD phenotypes was recognized only recently. Knowing the phenotype of a patient with COPD helps to predict the evolution of his/her disease, and makes the right choice of treatment for that patient more probable.7 There are studies and expert opinions that insist on phenotype-guided therapy, underlining the importance of determining the phenotype of each patient as early in the course of the disease as possible.8
The aim of this study was to describe characteristics of COPD patients from the Serbian patient registry, and to investigate actual differences of those characteristics among the COPD phenotypes.
Methods
The Patients
The Serbian registry of patients with COPD (further: the Registry) was established in 2016 at University of Kragujevac, Faculty of Medical Sciences, based on an online platform. The Registry was open for patients from Serbia, provided that pulmonologists who treat them enter the data. The structure, variables and format of the Registry were decided by a steering committee composed of five pulmonologists. Entry in the Registry was allowed for patients who were diagnosed with COPD according to the following criteria: symptoms of dyspnea, chronic cough or sputum production, history of risk factors for COPD (particularly tobacco smoking, biomass smoke exposure, and exposure at workplace to dust, noxious fumes and vapors)9 and any degree of persistent airflow limitation diagnosed at spirometry10 that is “usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases”.6
The patients were recruited in tertiary or secondary care facilities, then given written information about the Registry and their data entered to the Registry one day later, only after signing the informed consent form. Structure and procedures of the Registry were approved by the Ethics Committee of University Clinical Center Kragujevac, and by Ethics Committees of other hospitals whose pulmonologists entered data about their patients to the Registry. This study was conducted in accordance with the Declaration of Helsinki.
The patients from the Registry were included in this study if diagnosed with COPD regardless of other comorbidities. The exclusion criteria were incomplete or irregular data that were out of possible clinical or demographic range.
The Study Variables
Values of the following variables were collected in the Registry: signs and symptoms of the COPD, existence of allergy, habits (smoking, drinking coffee or alcohol), the number of moderate (an episode of antibiotic and/or systemic corticosteroid treatment) and severe (an episode of antibiotic and/or systemic corticosteroid treatment + hospitalization) COPD exacerbations, co-morbidities including calculation of the Charlson’s score,11 forced expiratory volume in the 1st second (FEV1) after a bronchodilator, forced vital capacity (FVC) after a bronchodilator, inhaled medication used currently for more than a month, concomitant medication taken for more than a month, the COPD Assessment Test (CAT),12 the Modified Medical Research Council Dyspnea Scale (mMRC),13 classification of a patient to A-D Global Initiative for Chronic Obstructive Lung Disease (GOLD) risk category through matching number of exacerbations with either CAT or mMRC, or a combination of the two (using the worst obtained values if the assessments were repeated), and classification of a patient to one of the COPD phenotypes (non-exacerbators [NON-AE], frequent exacerbators without chronic bronchitis [AE NON-CB], frequent exacerbators with chronic bronchitis [AE-CB] and asthma–COPD overlap syndrome [ACOS]) according to the Spanish Guidelines for Management of Chronic Obstructive Pulmonary Disease (GesEPOC) 2017.14,15 The NON-AE phenotype includes patients who had a maximum of one acute exacerbation during the last year, regardless of severity of the exacerbation; AE NON-CB patients experienced two or more severe or moderate exacerbations during the last year, and AE-CB patients should satisfy the same criterion plus having chronic cough every day for 3 months or more per year, for the two last years, with production of sputum. The ACOS patients should have a diagnosis of asthma established before the 40th birthday or a positive bronchodilator test in the last year with proofs of allergy and/or atopy.
The Study Design
The current study was of retrospective, cross-sectional design, including all patients entered in the Registry after at least one visit, from July 1, 2016 to October 1, 2020. Patients were excluded if the data followed up in this study were incomplete or irregular. A flowchart of the study is shown in Figure 1. The primary outcome of this study was to calculate the prevalence of patients with certain COPD phenotypes and GOLD group within the Serbian registry. The secondary outcome of the study was comparison of the COPD phenotypes in terms of relevant patient characteristics.
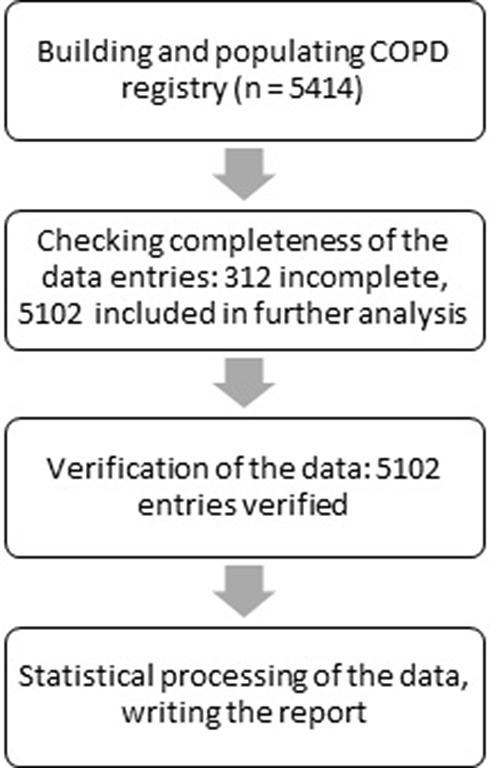 |
Figure 1 The study flowchart. |
Statistics
Values of continuous variables were described by a mean, standard deviation and range, while frequencies and percentages were used for describing categorical variables. Normality of the data distribution within continuous variables was tested by Kolmogorov–Smirnov test; if there was normality, the groups were compared by one-way analysis of variance, else Kruskal–Wallis non-parametric analysis of variance was used. Categorical variables were compared among the groups by Chi-square test, or where the assumptions were not met, by Fisher’s exact test with the Freeman-Halton extension. Maximum acceptable probability of null hypothesis was set to 0.05. The calculations were made using SPSS, version 18 (IBM Corporation, Armonk, NY, USA).
Results
There were 5414 patients entered in the COPD registry on October 1, 2020; 312 entries were with irregular or with missing data, and the remaining 5102 patients were eligible for further analysis. The data were entered from 21 Serbian cities in total, but 96.7% of the patients were entered from only 9 cities. In total 69 physicians entered the patients in the Registry, and the average number of entries per physician was 74.6 ± 130.9 (range 1–499). Key demographic and clinical data are shown in Table 1.
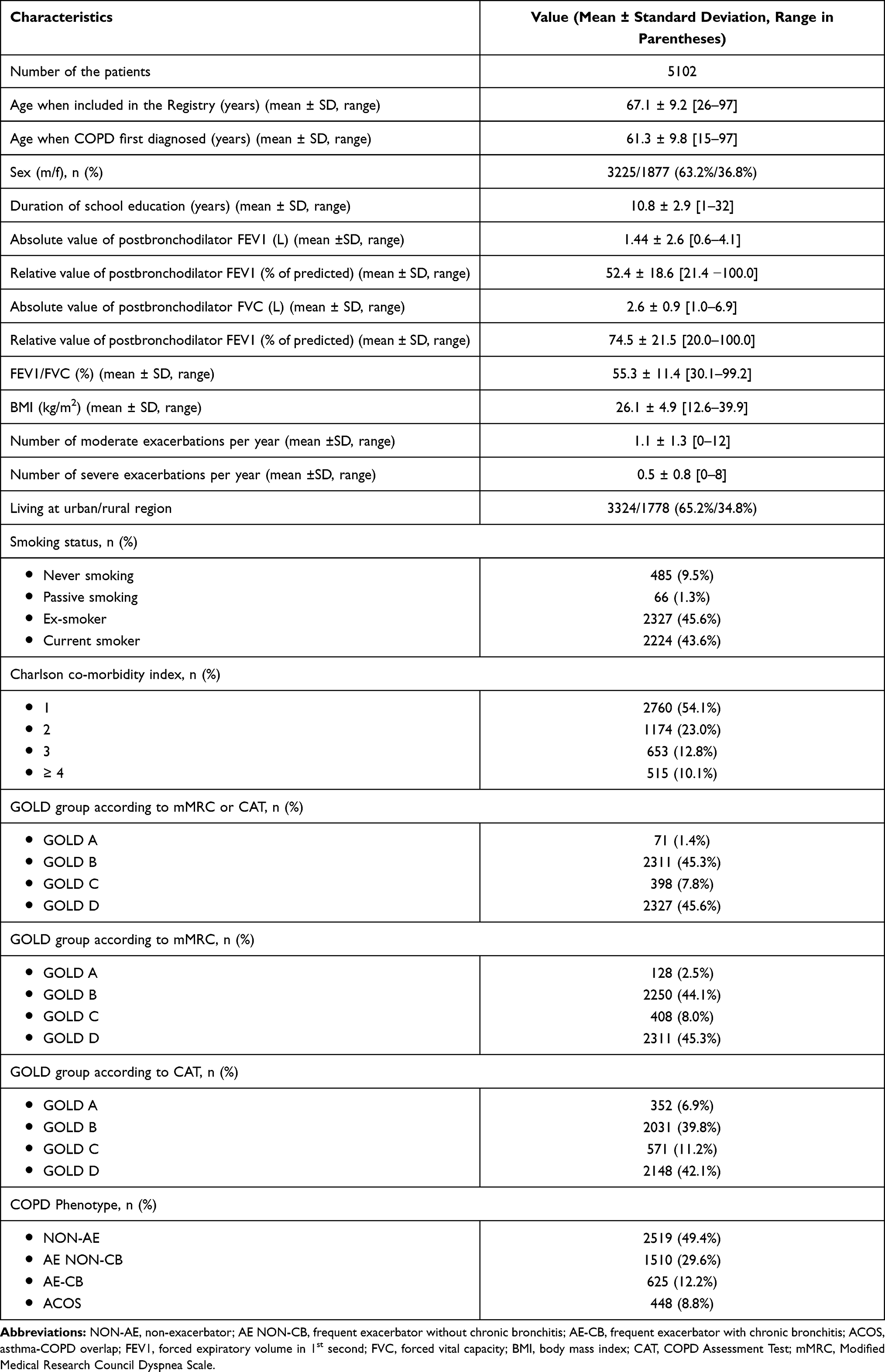 |
Table 1 Demographic and Clinical Characteristics of Patients from the Serbian COPD Registry |
Characteristics of the patients with COPD differ significantly according to the phenotype: non-exacerbator (NON-AE), frequent exacerbator without chronic bronchitis (AE NON-CB), frequent exacerbator with chronic bronchitis (AE-CB) and asthma-COPD overlap (ACOS). In Table 2 both influence of the COPD phenotype on severity of the disease and demographic characteristics of each of the phenotypes are shown.
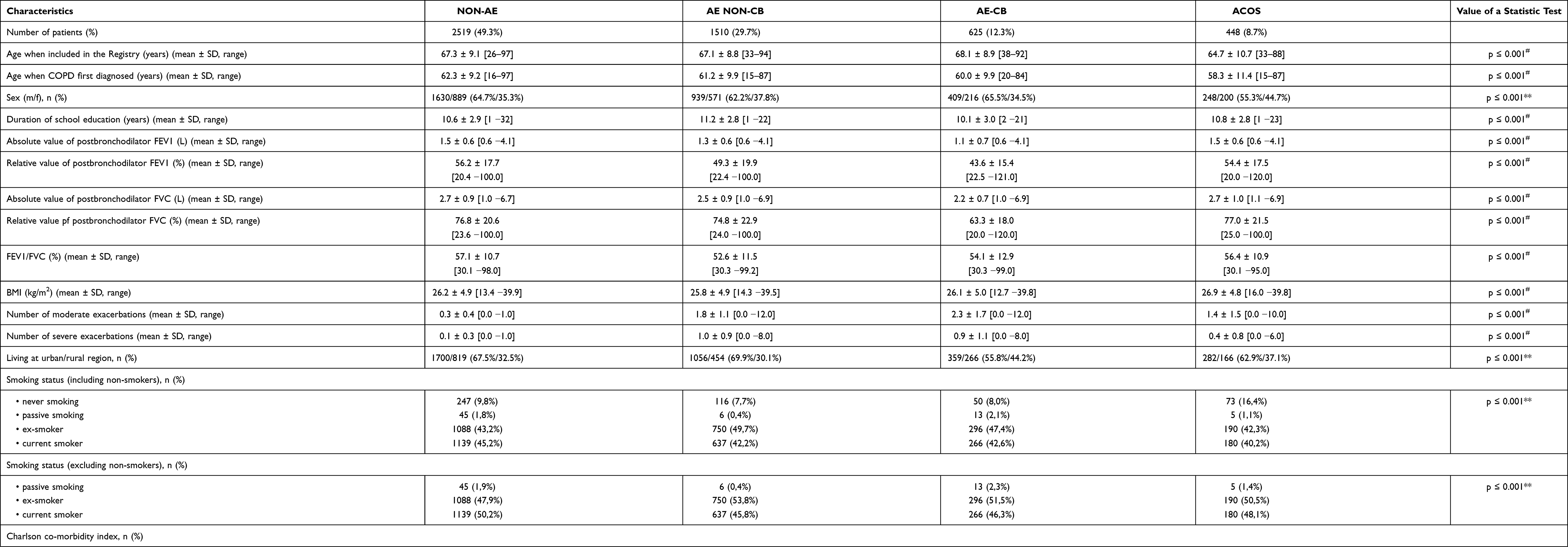 |
Table 2 Characteristics of COPD Patients According to Phenotype |
Post hoc analysis (by a series of Mann–Whitney tests) showed that the ACOS phenotype differed significantly from all other phenotypes in regard to the age at inclusion to the Registry (p ≤ 0.001), while the age at the first diagnosis of COPD was lower in ACOS phenotype when compared with NON-AE and AE NON-CB (p ≤ 0.001), and in AE-CB and AE NON-CB, when compared with NON-AE (p ≤ 0.004).
According to the post hoc comparison of phenotypes in regard to proportion of males and females (z-test comparison of proportions), the ACOS group has proportionally fewer males than females when compared with the AE-CB and the NON-AE groups (p ≤ 0.5). The AE NON-CB phenotype was associated with a significantly lower BMI in comparison with ACOS and NON-AE phenotypes (p = 0.000 and p = 0.020, respectively).
The patients with AE NON-CB phenotype had more years of education than the patients with NON-AE and AE-CB phenotypes (p ≤ 0.031), while the patients with AE-CB phenotype had fewer years of education than the patients with AE NON-CB and ACOS phenotypes (p ≤ 0.004).
In regard to the absolute and relative values of postbronchodilator FEV1, all phenotypes differed among each other significantly (p ≤ 0.001), except NON-AE and ACOS between themselves (p = 0.242 and p = 0.257, respectively). However, when the phenotypes were compared among themselves by post hoc tests in regard to the absolute values of postbronchodilator FVC, the differences were significant after all comparisons (p ≤ 0.001), except when ACOS group was compared with NON-AE (p = 0.626) and AE NON-CB (p = 0.355) groups. Post-hoc pairwise comparisons of relative values of postbronchodilator FVC showed a similar pattern, but the differences were not significant only when ACOS and NON-AE groups were compared (p = 0.999). Finally, multiple pairwise comparisons of the FEV1/FVC ratio among the phenotypes showed that it was significantly higher in ACOS and NON-AE groups than in AE-CB and AE NON-CB groups (p ≤ 0.002), while the differences between ACOS and NON-AE, and between AE-CB and AE NON-CB, were not significant (p = 1.000 and p = 0.516, respectively).
Post-hoc comparisons of frequency of moderate and severe exacerbations between the phenotypes showed that all groups differed significantly among themselves in values of both parameters (p ≤ 0.001 in all comparisons).
When non-smokers are included in the analysis (see Table 2), post hoc comparison of phenotypes in regard to proportion of smoking status categories (z-test comparison of proportions) showed that the ACOS group differed significantly from each of the other 3 groups (p ≤ 0.5) in proportion of non-smokers. AE NON-CB phenotype differed significantly (p ≤ 0.5) from ACOS and NON-AE in proportion of ex-smokers, and both AE-CB and NON-AE phenotypes had more passive smokers than AE NON-CB (p ≤ 0.5). When non-smokers are excluded from the analysis (see Table 2), post hoc comparison of phenotypes in regard to proportion of smoking status categories (z-test comparison of proportions) again showed that AE NON-CB phenotype differed significantly (p ≤ 0.5) from NON-AE in proportion of ex-smokers, and both AE-CB and NON-AE phenotypes had more passive smokers than AE NON-CB (p ≤ 0.5).
Since the majority of the registered patients with COPD were of old age, it was expected that rate of comorbidities will be high. Although Charlson’s comorbidity index was not significantly different across the COPD phenotypes (Chi-square = 40.956, df = 9; p = 0.144) (see Table 2), certain specific diseases were non-uniformly distributed. Table 3 presents phenotype-specific rates of the most frequent comorbidities among the registered patients. Table 4 shows COPD phenotype-specific inhalation therapy prescribed to the patients from the Serbian COPD registry.
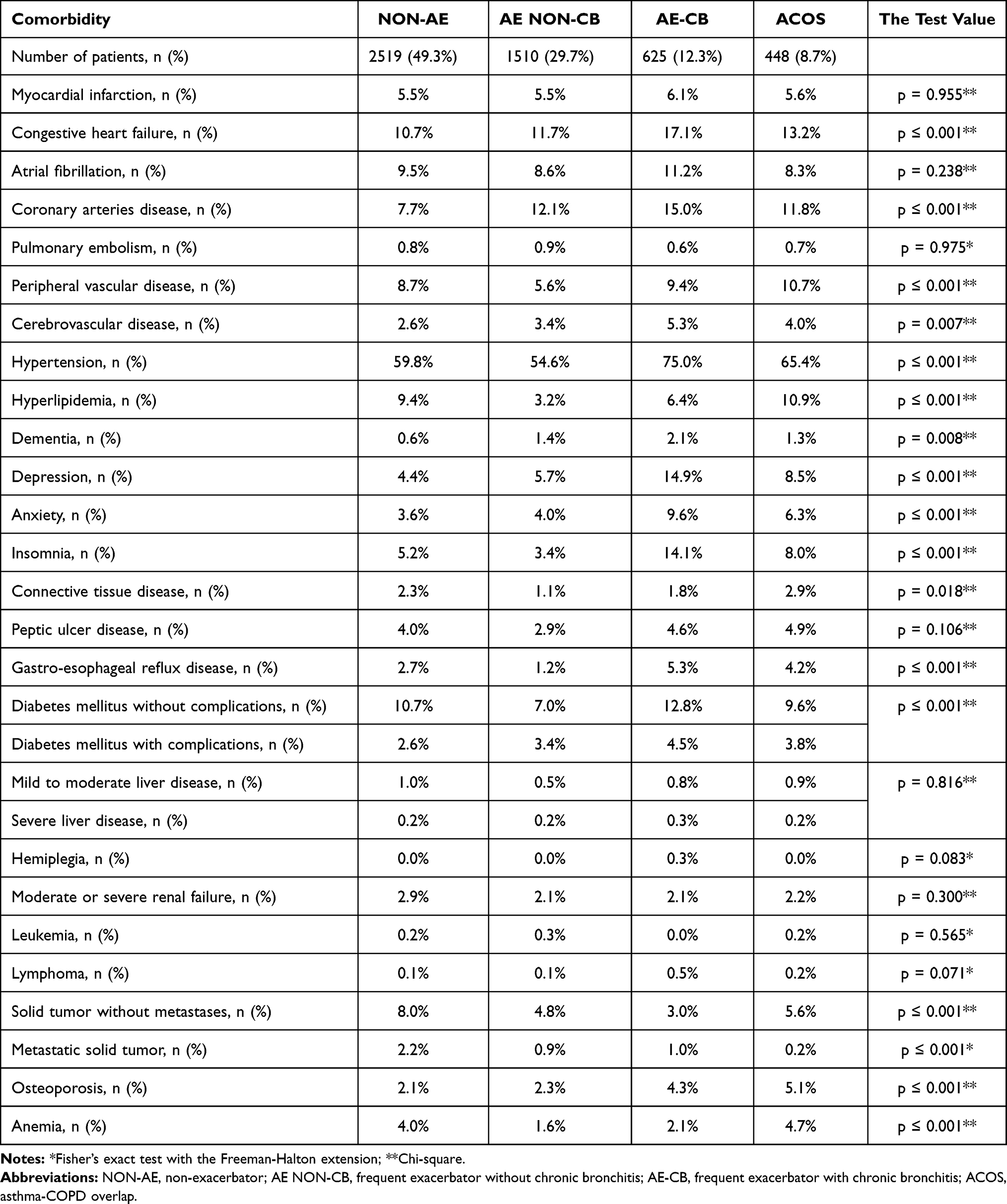 |
Table 3 COPD Phenotype-Specific Rates of the Most Frequent Comorbidities Occurring Among Patients from the Serbian COPD Registry |
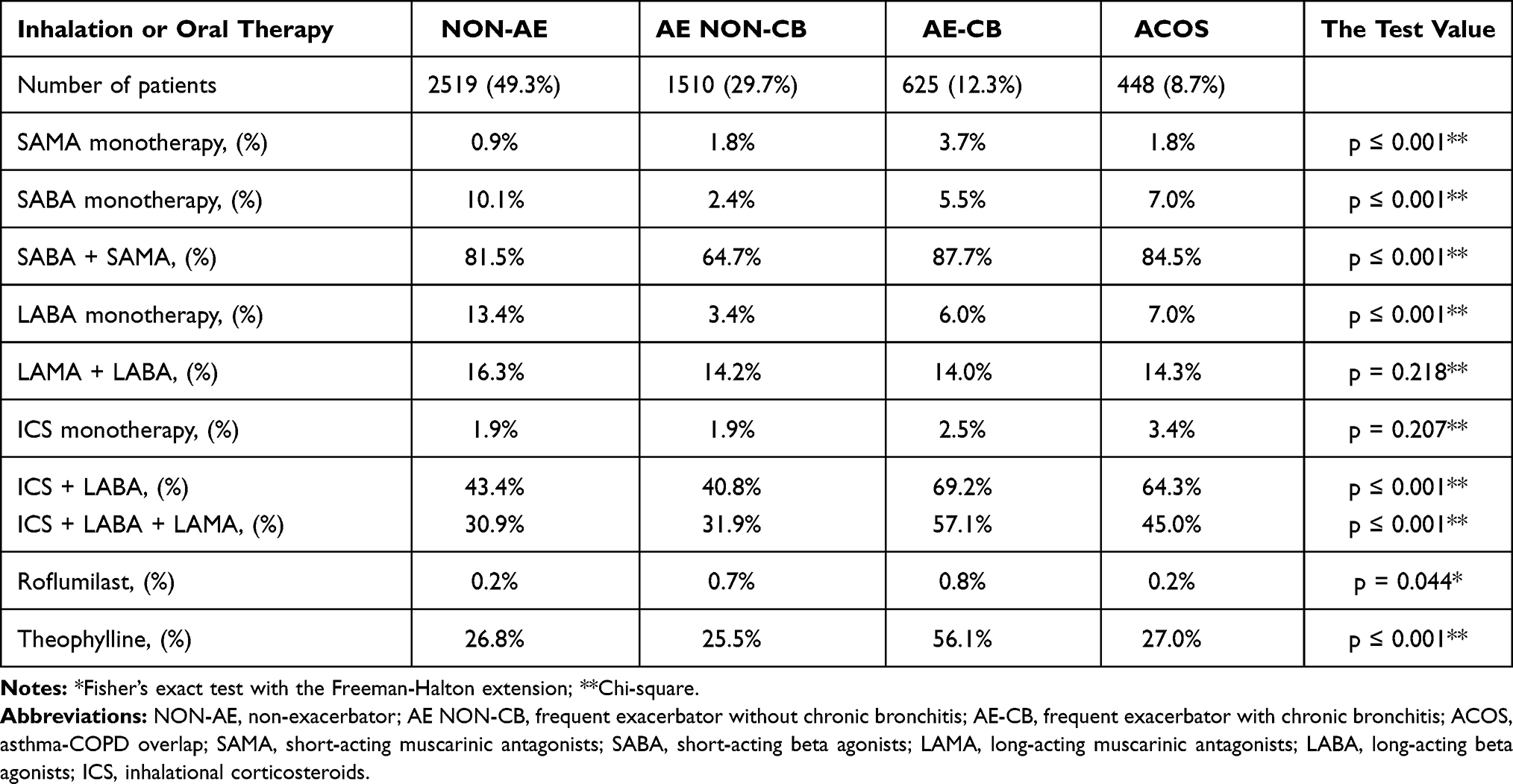 |
Table 4 COPD Phenotype-Specific Inhalation and Oral Therapy Prescribed to Patients from the Serbian COPD Registry |
Discussion
In the Serbian COPD registry B and D GOLD class were dominant, while among the COPD phenotypes, the most prevalent were non-exacerbators and then frequent exacerbators without chronic bronchitis. The frequent exacerbator with chronic bronchitis phenotype was associated with low levels of bronchopulmonary function and absolute predominance of GOLD D class. Although total Charlson’s score of comorbidities did not differ among the phenotypes, anxiety, depression, insomnia, hypertension and chronic heart failure were the most prevalent in the frequent exacerbator with chronic bronchitis phenotype; patients with this phenotype were also treated more frequently than other patients with a triple combination of the most effective inhaled anti-obstructive drugs: long-acting muscarinic antagonists, long-acting beta 2 agonists and corticosteroids.
While non-exacerbators are the most prevalent among COPD patients in the majority of registries,16 there are regional differences in the extent of this predominance,17 as well as in prevalence of frequent exacerbators with and without chronic bronchitis. Asthma-COPD overlap phenotype is the least prevalent in Serbian and other registries, too.15 Rate of active smokers could be a factor that influences distribution of COPD phenotypes, as observed in Spain, where AE-CB phenotype was more prevalent than AE NON-CB, and in both phenotypes frequency of active smokers was between 50 and 60%.18 In the Serbian registry frequency of active smokers was lower (42–45% per phenotype), and consequently AE-CB phenotype was less prevalent than AE NON-CB. It is not surprising that smoking is associated with a higher rate of AE-CB phenotype, since it directly contributes to development of chronic bronchitis.19,20 Organization and efficiency of a healthcare system on a national level also may affect prevalence of certain phenotypes; if the patients are frequently misdiagnosed and inadequately treated, the most prevalent phenotype will be AE-CB, as in Russia (37.3%).21 Whether other factors, such as air pollution or genetic variations, contribute to geographic differences in distribution of COPD phenotypes remains to be established in future studies.
Frequent exacerbators with chronic bronchitis have worse bronchopulmonary function, more severe signs and symptoms, more comorbidities (especially hypertension, heart failure, coronary disease, anxiety and depression), worse quality of life22 and worse prognosis (higher death rate) than other phenotypes, as confirmed by data from the Serbian and other registries.23 Almost all patients with AE-CB phenotype in our Registry were in the GOLD D group; previous studies showed that the GOLD D was associated with 2.7 times higher risk of death than the GOLD A group.24 It is of prime importance to prevent development of chronic bronchitis in frequent exacerbators through elimination of risk factors, and to treat obstruction adequately (whether a patient has chronic bronchitis or not), which will lead to decrease in frequency of exacerbation. It was known already that COPD may contribute to development of cardiovascular diseases, so our observation was not accidental. Progression of COPD leads to pulmonary hypertension, consequent right ventricular hypertrophy, and myocardial ischemia.25 However, the link between COPD and cardiovascular disorders is much more complex, as recently recognized; COPD significantly increases risk of sudden cardiac death, and is a risk factor for 12 different cardiovascular conditions.26 There is a clear need for research that will explore this link, and create the basis for planning new therapeutic strategies for patients with COPD and cardiovascular disorders.
Phenotyping of patients with COPD is important not only for determination of prognosis, but also for making an optimal choice of therapy, since not all drugs for COPD are effective in every phenotype. The AE NON-CB phenotype responds best to long-acting bronchodilators (LABA), and sometimes to inhaled corticosteroids (ICS), while the AE-CB phenotype requires a regular combination of LABA and ICS.27 While roflumilast is active in patients with AE-CB phenotype, it is not the case in patients with AE NON-CB phenotype. Patients from the Serbian Registry having AE-CB phenotype were treated the most frequently with the recommended combination of LABA and ICS; however, more than two-thirds of them were also prescribed a long-acting muscarinic agonist (LAMA), possibly reflecting severity of the disease (98% of patients of this phenotype were in GOLD D group). On the other hand, there is obvious undertreatment with roflumilast, which could be explained by the relatively recent introduction of this drug to the Serbian market, and the very stringent criteria for reimbursement imposed by the Health insurance fund in Serbia (only in patients with more than two exacerbations per year). Since in our study the NON-AE phenotype was accompanied by mostly less severe GOLD B group of patients, the ACOS phenotype was divided into GOLD B and GOLD D patients, and AE NON-CB and AE-CB phenotypes were mostly GOLD D patients, one could expect that monotherapy should have been prescribed more to patients with NON-AE and ACOS phenotypes (the GOLD guidelines advise LABA or LAMA monotherapy at least initially in GOLD B and GOLD C patients, while only GOLD D should start with combination involving ICS28). Although this was the case, the percentage of patients with monotherapy with LABA was below 15%, and LAMA monotherapy was not used at all. It is also apparent from Table 4 that combinations involving ICS and triple combinations (LAMA+LABA+ICS) were overprescribed. In general, more potent therapy was used than absolutely necessary according to the guidelines, raising questions of induction of tolerance and increased risk of adverse effects.
It is also interesting that in Serbia LAMA monotherapy for COPD was not used at all, although according to current GOLD guidelines it should be the first choice in GOLD C and GOLD D with less burden of symptoms. Inappropriate prescribing to patients with COPD is not a rare phenomenon: a recent study by Palmiotti and associates in Italy showed that between 40 and 50% of patients (depending on the GOLD group) were using inappropriate inhalation therapy, against the GOLD guidelines; however, in this study LAMA monotherapy was used in 17.9% of all patients.28 Although methods involving external control of prescribing to COPD patients may give certain improvements in quality of prescribing,29 this problem will not be solved in the future if we do not understand the motives of the prescribers for making inappropriate decisions. Unfortunately, qualitative studies that may answer this question are rare (there are none in the field of COPD), therefore this is an area where at least part of future investigations of COPD should go.
The Serbian Registry has certain limitations that should be overcome through future development. There is imbalance in the number of patients entered in the Registry from various cities in Serbia; more than 96% of patients were registered from only 9 cities, while the remaining 12 cities contributed only 4% of patients. This imbalance introduces a certain degree of geographic bias in the Registry, making the results of this analysis potentially non-representative. Other limitations are the number of patients with incomplete data (5.7%), and significant gender imbalance in favor of male patients. This could be mitigated through regular monitoring visits of the sites where the patients are entered to the Registry, and by imputation of missing data using measures of central tendency. Furthermore, apart from initial education for all potential participants, we did not have means to control quality of data collection at individual centers (spirometry quality, data accuracy, data completeness, definition of comorbidities, etc.). The Registry should be improved in the future through training of physicians who enter the data and by increasing the number of collaborating physicians from the cities where recruitment of patients was minimal up to now. However, the Serbian Registry of COPD patients is an important element of care for this large and sensitive patient population. It is not just useful for research purposes, but can help with shaping national and local treatment guidelines, as well as with evaluating quality of care and designing corrective measures.
In conclusion, the data from the Serbian Registry are in line with those from other national registries, showing that frequent exacerbators with chronic bronchitis have worse bronchopulmonary function, more severe signs and symptoms, and more comorbidities (especially anxiety and depression) than other phenotypes. Other studies also confirmed worse quality of life and worse prognosis (higher death rate) of the AE-CB phenotype, stressing importance of both preventive and appropriate therapeutic measures against chronic bronchitis in patients with COPD.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Heffler E, Paoletti G, Giorgis V, et al. Real-life studies of biologics used in asthma patients: key differences and similarities to trials. Expert Rev Clin Immunol. 2019;15(9):951–958. doi:10.1080/1744666X.2019.1653758
2. Bakken IJ, Ariansen AMS, Knudsen GP, Johansen KI, Vollset SE. The norwegian patient registry and the norwegian registry for primary health care: research potential of two nationwide health-care registries. Scand J Public Health. 2020;48(1):49–55. doi:10.1177/1403494819859737
3. Sessa M, Mascolo A, Mortensen RN, et al. Relationship between heart failure, concurrent chronic obstructive pulmonary disease and beta-blocker use: a Danish nationwide cohort study. Eur J Heart Fail. 2018;20(3):548–556. doi:10.1002/ejhf.1045
4. Kobayashi S, Hanagama M, Ishida M, et al. Clinical characteristics and outcomes in Japanese patients with COPD according to the 2017 GOLD classification: the Ishinomaki COPD Network Registry. Int J Chron Obstruct Pulmon Dis. 2018;13:3947–3955. doi:10.2147/COPD.S182905
5. Müllerova H, Maselli DJ, Locantore N, et al. Hospitalized exacerbations of COPD: risk factors and outcomes in the ECLIPSE cohort. Chest. 2015;147(4):999–1007. doi:10.1378/chest.14-0655
6. Vestbo J. COPD: definition and phenotypes. Clin Chest Med. 2014;35(1):1–6. doi:10.1016/j.ccm.2013.10.010
7. Guerreiro I, Soccal PM. COPD and phenotypes. Rev Med Suisse. 2019;15(671):2082–2086.
8. Siafakas N, Corlateanu A, Fouka E. Phenotyping Before Starting Treatment in COPD? COPD. 2017;14(3):367–374. doi:10.1080/15412555.2017.1303041
9. López-Campos JL, Tan W, Soriano JB. Global burden of COPD. Respirol Carlton Vic. 2016;21(1):14–23. doi:10.1111/resp.12660
10. Lange P, Halpin DM, O’Donnell DE, MacNee W. Diagnosis, assessment, and phenotyping of COPD: beyond FEV1. Int J Chron Obstruct Pulmon Dis. 2016;11(Spec Iss):3–12. doi:10.2147/COPD.S85976
11. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
12. Jones PW, Harding G, Berry P, Wiklund I, Chen W-H, Kline Leidy N. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
13. Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest. 1988;93(3):580–586. doi:10.1378/chest.93.3.580
14. Miravitlles M, Soler-Cataluña JJ, Calle M, et al. Spanish Guidelines for Management of Chronic Obstructive Pulmonary Disease (GesEPOC) 2017. pharmacological treatment of stable phase. Arch Bronconeumol. 2017;53(6):324–335. doi:10.1016/j.arbres.2017.03.018
15. Koblizek V, Milenkovic B, Barczyk A, et al. Phenotypes of COPD patients with a smoking history in Central and Eastern Europe: the POPE Study. Eur Respir J. 2017;49(5):1601446. doi:10.1183/13993003.01446-2016
16. Reiger G, Zwick R, Lamprecht B, Kähler C, Burghuber OC, Valipour A. Phenotypes of COPD in an Austrian population: national data from the POPE study. Wien Klin Wochenschr. 2018;130(11–12):382–389. doi:10.1007/s00508-018-1347-7
17. Alcázar-Navarrete B, Trigueros JA, Riesco JA, Campuzano A, Pérez J. Geographic variations of the prevalence and distribution of COPD phenotypes in Spain: “the ESPIRAL-ES study.”. Int J Chron Obstruct Pulmon Dis. 2018;13:1115–1124. doi:10.2147/COPD.S158031
18. Riesco JA, Alcázar B, Trigueros JA, Campuzano A, Pérez J, Lorenzo JL. Active smoking and COPD phenotype: distribution and impact on prognostic factors. Int J Chron Obstruct Pulmon Dis. 2017;12:1989–1999. doi:10.2147/COPD.S135344
19. Mejza F, Nastałek P, Mastalerz-Migas A, Doniec Z, Skucha W. Coexistence of chronic bronchitis in chronic obstructive lung disease. Adv Exp Med Biol. 2018;1114:1–9.
20. Duffy SP, Criner GJ. Chronic obstructive pulmonary disease: evaluation and management. Med Clin North Am. 2019;103(3):453–461. doi:10.1016/j.mcna.2018.12.005
21. Arkhipov V, Arkhipova D, Miravitlles M, Lazarev A, Stukalina E. Characteristics of COPD patients according to GOLD classification and clinical phenotypes in the Russian Federation: the SUPPORT trial. Int J Chron Obstruct Pulmon Dis. 2017;12:3255–3262. doi:10.2147/COPD.S142997
22. Chai C-S, Liam C-K, Pang Y-K, et al. Clinical phenotypes of COPD and health-related quality of life: a cross-sectional study. Int J Chron Obstruct Pulmon Dis. 2019;14:565–573. doi:10.2147/COPD.S196109
23. Kania A, Krenke R, Kuziemski K, et al. Distribution and characteristics of COPD phenotypes – results from the Polish sub-cohort of the POPE study. Int J Chron Obstruct Pulmon Dis. 2018;13:1613–1621. doi:10.2147/COPD.S154716
24. Raherison C, Girodet P-O. Epidemiology of COPD. Eur Respir Rev off J Eur Respir Soc. 2009;18(114):213–221. doi:10.1183/09059180.00003609
25. André S, Conde B, Fragoso E, et al. COPD and Cardiovascular Disease. Pulmonology. 2019;25(3):168–176. doi:10.1016/j.pulmoe.2018.09.006
26. Leitao Filho FS, Sin DD. COPD and cardiovascular diseases: now is the time for action! Thorax. 2018;73(9):799–800. doi:10.1136/thoraxjnl-2018-211553
27. Zhou A, Zhou Z, Zhao Y, Chen P. The recent advances of phenotypes in acute exacerbations of COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:1009–1018. doi:10.2147/COPD.S128604
28. Palmiotti GA, Lacedonia D, Liotino V, et al. Adherence to GOLD guidelines in real-life COPD management in the Puglia region of Italy. Int J Chron Obstruct Pulmon Dis. 2018;13:2455–2462. doi:10.2147/COPD.S157779
29. Brown KE, Johnson KJ, DeRonne BM, Parenti CM, Rice KL. Order set to improve the care of patients hospitalized for an exacerbation of chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2016;13(6):811–815. doi:10.1513/AnnalsATS.201507-466OC
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.