Back to Journals » Clinical Ophthalmology » Volume 17
Characteristics, Etiological Factors, and Visual Outcomes of Pediatric Open Globe Injuries in Central Saudi Arabia: A 22-Year Retrospective Study
Authors Al Ghadeer H ![]() , Khandekar R
, Khandekar R ![]()
Received 8 August 2023
Accepted for publication 25 September 2023
Published 4 October 2023 Volume 2023:17 Pages 2909—2917
DOI https://doi.org/10.2147/OPTH.S430394
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Huda Al Ghadeer,1 Rajiv Khandekar2,3
1Emergency Department, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 2Research Department, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 3Department of Ophthalmology and Vision Sciences, Faculty of Medicine, University of British Columbia, Vancouver, BC, Canada
Correspondence: Huda Al Ghadeer, Emergency Department, King Khaled Eye Specialist Hospital, PO Box 7191, Riyadh, 11462, Saudi Arabia, Tel +966 1 4821234 ext. 2500, Email [email protected]
Purpose: To discuss the characteristics, etiological factors, and visual outcomes of open globe injuries (OGIs) in children at a tertiary eye hospital in Riyadh, Central Saudi Arabia.
Methods: This was a hospital-based cohort study conducted in 2021. Children aged ≤ 16 years with OGI based on the Birmingham Eye Trauma Terminology classification were included. The age, gender, type, cause of OGI, and vision were recorded, as well as uncorrected and best corrected visual acuity (UCVA and BCVA, respectively). There was a change in the UCVA and BCVA one year after management. BCVA following management was linked to a variety of factors.
Results: There were 664 eyes with OGI. [median age 5.1, 461 (69.6%) boys]. UCVA at presentation was < 20/400 in 525 (79%) of eyes with OGI. Injuries were mainly due to metallic objects in 195 (29.4%), glass in 102 (15.4%), and fireworks in 62 (9.4%). The Change in visual impairment grade in UCVA and BCVA after management compared to the initial presentation was significant (p < 0.001). Improvement of two lines of BCVA was noted in 345 (52%), no change in (<± 2 lines) 299 (45%) and deteriorated in 10 (1.5%).
Conclusion: OGI was identified as a leading cause of unilateral blindness. Children with OGIs who receive standard treatment have better outcomes. Many children could not achieve normal, functional vision despite the intervention of skilled care providers.
Keywords: child, injuries, ocular, pediatrics, trauma
Introduction
Eye injuries in children are a serious concern for caregivers and parents. Although most of them are preventable or avoidable,1,2 accidental injuries frequently result in patients being taken to the emergency departments of general hospitals and subsequently referred to eye hospitals.
Initial evaluation, first assistance, and adequate counseling are vital; thus, proper training of emergency care providers is needed.3
Children often cannot record their visual and ocular health upon presentation due to their young age and hospital phobia. Therefore, issues related to visual prognostic indicators are of interest to eye care professionals.4 Several ocular trauma score systems have been proposed, tested, and found effective in predicting visual prognosis for adults and children.5–7 However, it is generally accepted that the visual prognosis for children with (OGIs) is worse than that for children with closed globe injuries.8
The reported prevalence of OGI in the United States is 2–3.8/100,000. The etiology of injuries, the time between trauma and admission to the eye emergency unit, and the extent of injuries resulting in OGIs are recognized predictors of vision following management.9 The causes of OGI vary based on age, gender, and geographical location. A research of the epidemiology and management outcome of OGI is encouraged to develop an evidence-based protocol for its management and the counseling of parents of children with OGI.10,11
Our facility is an eye care center in the Middle East with various subspecialty units of ophthalmology and subspecialty ophthalmologists. Children with ocular injuries are transferred directly to the emergency unit or referred there. Subspecialty units subsequently provide treatment. We discuss the characteristics, etiological factors, and visual outcomes of children with OGIs at central Saudi Arabia.
Methods
Our institution’s Research Ethics Committee approved this study project. All participants’ parents/guardians were given an informed consent with permission to publish. Furthermore, the tenets of the Helsinki Declaration were faithfully adhered to at all stages. Children aged ≤16 years with OGI based on the Birmingham Eye Trauma Terminology classification12,13 and were brought to the hospital’s emergency unit for the first time from 1998 to 2019 were included in this hospital-based, one-armed cohort analysis. The review was held in 2021.
To calculate the sample size for this study, we considered that the best corrected visual acuity (BCVA) in eyes with OGIs was present in 39% of children after treatment.14 To achieve a 95% confidence interval and 5% acceptable error margin in a hypothesis testing study with a clustering effect of 1.5%, we need to review at least 549 children. We expanded the sample size by 20% to compensate for the data loss. This study’s final sample size requirement was 659 children with OGI. Open epi software was used to determine the sample size for this study.15
The demographic data comprised gender, affected eye, and presenting age. The agent causing the child’s ocular injury was recorded. A full ocular examination was performed on all patients at presentation and subsequent follow-up visits. The vision was assessed with the best correction wherever feasible. At six meters, the BCVA was measured using a Snellen chart with a Lea Symbol or a tumbling E chart. If the largest optotype could not be read, finger counting, hand motion, and light perception from all cardinal directions were examined. The pupillary reflex and adnexal inspection were performed with a well-focused torchlight. The anterior segment was examined using a slit lamp biomicroscope (Topcon Corp., Japan). For uncooperative children, ophthalmic loupes with a light source (Keeler, USA) were used. Indirect ophthalmoscopy was used to examine the posterior segment (Heine, Germany). B-scan ultrasound was conducted when necessary and when posterior segment examination was impossible. To prevent additional exacerbation in cases of suspected penetrating damage, manipulation, and examinations were restricted. Computed tomography examinations were requested for suspected intraocular foreign bodies and orbital injuries, including probable bone fractures. In children with penetrating or perforating wounds, an emergency assessment was done under general anesthesia, and if needed, surgical exploration and primary closure of the open globe were done. Under general anesthesia, intraocular surgery or intravitreal medication administration was performed on hospitalized patients. Intravenous antibiotics were delivered. As directed by the emergency department, a tetanus immunization was administered. Surgical intervention was performed within 24 hours of presentation. All patients with non-ophthalmic severe injuries were treated concurrently at different general hospitals. The final BCVA, ocular state, and diagnosis were included in the follow-up data. Poor visual outcome was defined as BCVA 20/200, and unilateral blindness was defined as BCVA 20/400 in the affected eye. The World Health Organization’s visual impairment grades were employed in this study.16
If the difference between uncorrected visual acuity (UCVA) and BCVA at the final follow-up and the presentation was more than two lines, we categorized it as an improvement. If it was <± 2 lines, we considered it stable; if it was <2 lines, we graded that as deterioration. The eyes with No Light Perception (NLP) were graded separately. Data were collected using an Excel spreadsheet (Microsoft Office 2010; Redmond, WA, USA). Univariate analysis was performed using Statistical Package for Social Studies (SPSS 25) (IBM Corp., Armonk, NY, USA). The median and interquartile range (IQR) was reported for quantitative variables. Qualitative variables were presented as frequencies and percentage proportions. The visual impairment grades of ≥ 20/200, < 20/200, and NLP were associated with different demographic and ocular status at presentation. Chi square value, degree of freedom, and two-sided p values were estimated. P value < 0.05 was considered statistically significant.
Results
There were 664 eyes of 662 children with OGI. The presentation profile of these cohorts is shown in Table 1. Two-thirds of the participants were males. Almost half of them were <5 years old. In 5-year old children with OGI, the male-to-female ratio was 1.75:1; between 5 and 10 years old, it was 2.8:1, and above ten years old, it was 4.5:1. Two children were diagnosed with bilateral OGI. Fifty-four children (8.1%) had NLP, and the vision of 25 children could not be tested at the time of presentation. There were 193/664 =29% eyes with cataract and 75/664 = 11.3% with retinal detachment at presentation. Three-fourths of injured eyes had severe vision impairment (SVI). A total of 195 (29.4%) of the injuries were caused by metallic objects, 102 (15.4%) by glass, and 62 (9.4%) by fireworks. (Figure 1) demonstrates the causative agents of OGI in children. In 27% of the eyes, full thickness laceration (Figure 2) and penetrating, and perforating injuries were seen (Figure 3). Surgical intervention was necessary in 23 eyes with endophthalmitis and 34 eyes with vitreous hemorrhage at the last follow-up. Additionally, one eye was found to have glaucoma, which was effectively controlled medically. The grades of visual acuity based on the UCVA and BCVA in eyes with OGI were compared at the final follow-up and presentation Table 2. The variation in visual impairment grades at the last follow-up varied significantly from that seen at the presentation of globe injury. The number of eyes having NLP increased from 8.1% to 17.6% after treatment. The number of eyes with functional vision ≥20/60 increased from 11% to 41%. Nearly half of the eyes treated with OGI showed at least a two-line improvement in vision. The remaining patients had stable vision. The vision was not noted or deteriorated in <5% of the eyes. The BCVA following treatment of OGI was categorized as vision ≥ 20/200, SVI, and NLP. Vision at presentation in eyes with OGI was significantly related to visual outcome after surgery. Age at presentation was negatively correlated with the change in visual acuity at the last follow-up. (Pearson coefficient −0.21, P<0.001). The gender of the child with OGI was not associated with a change in visual acuity at the last follow-up (P = 0.274). The duration of follow-up was negatively correlated with the change in visual acuity. (Wilcoxon Z = −13.8, P <0.001). The type of injury was associated with the change in visual acuity at the last follow-up. (chi square = 16, df =2, P <0.001).
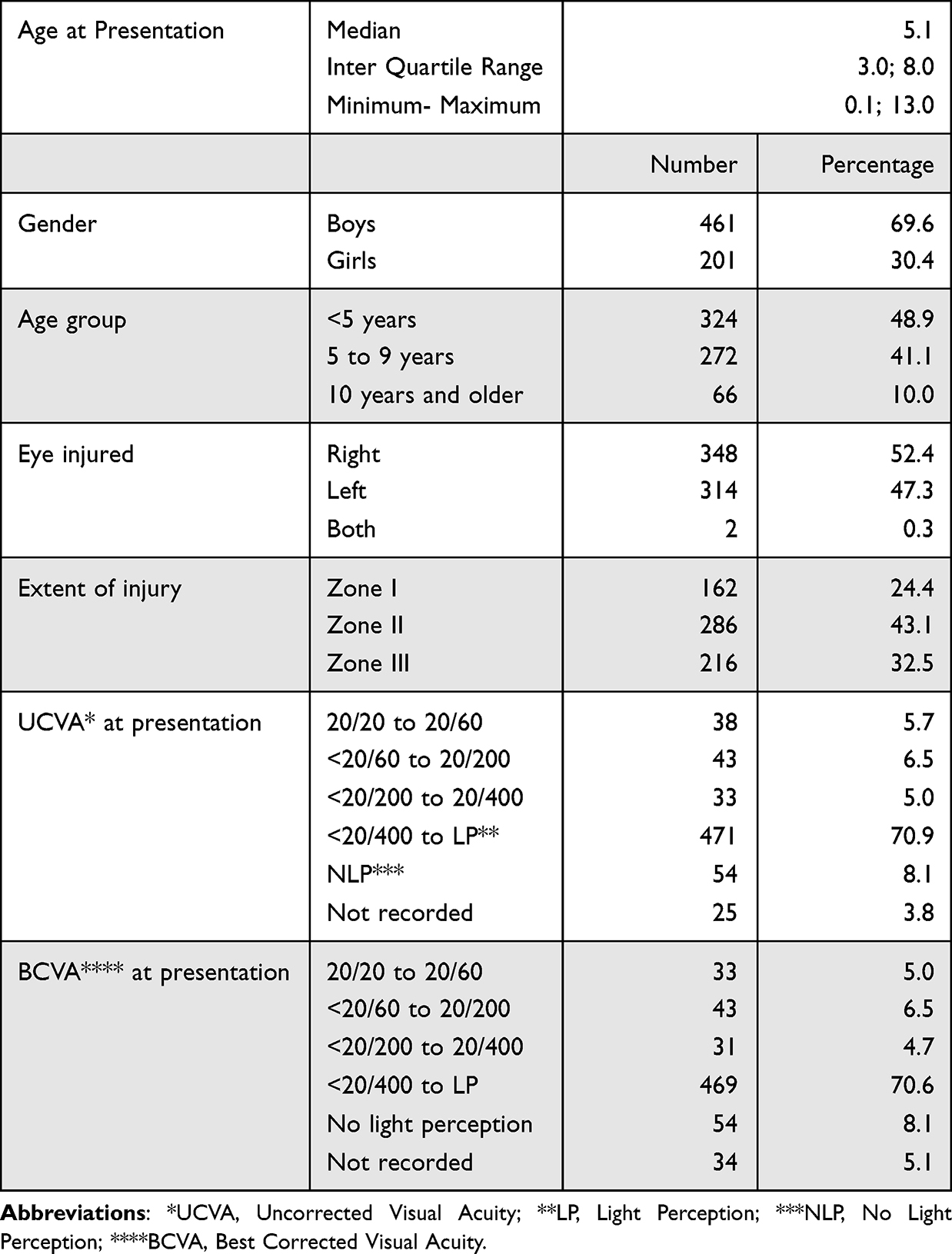 |
Table 1 Profile of Children with Open Globe Injuries in a Tertiary Eye Hospital of Central Saudi Arabia (N =664) |
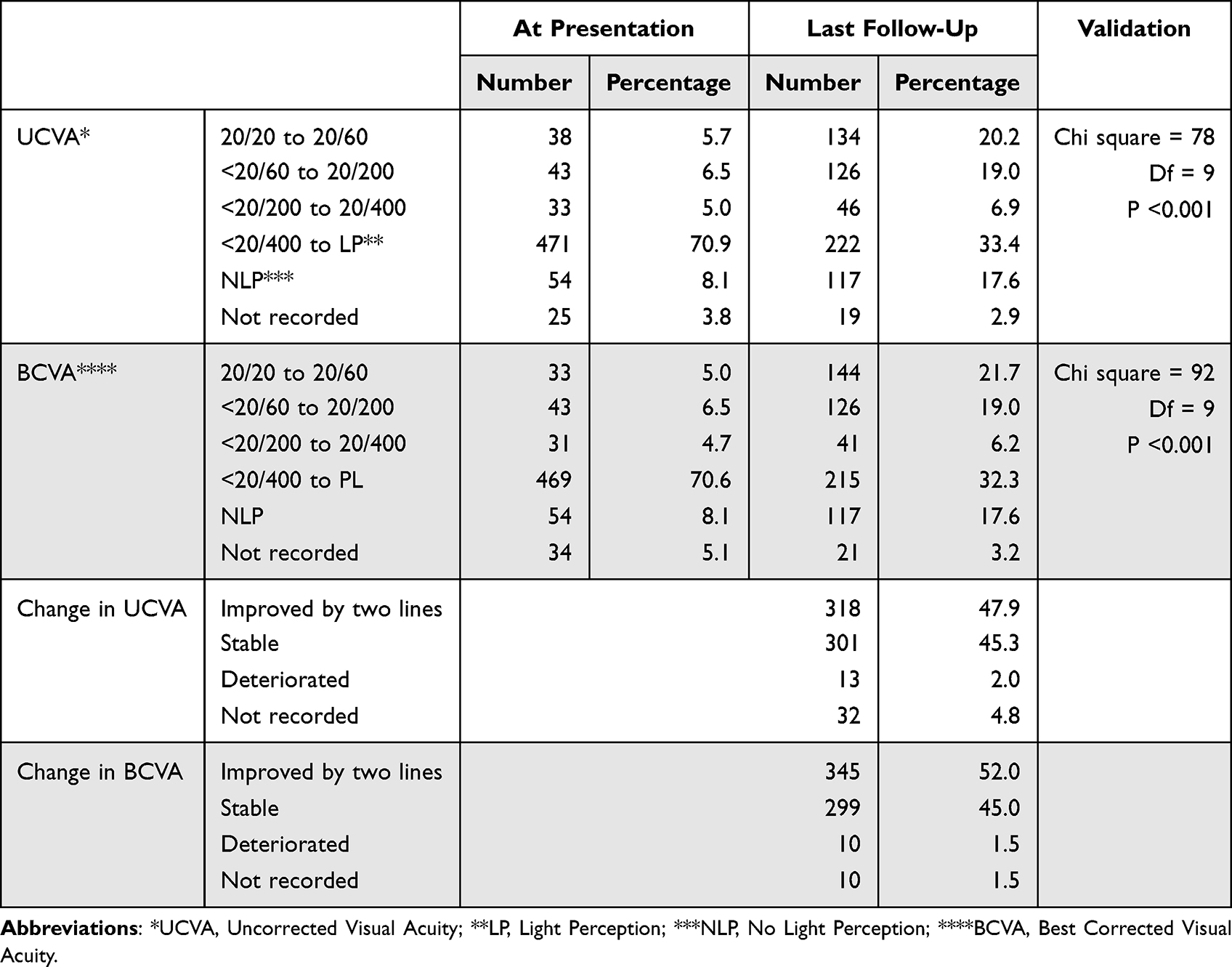 |
Table 2 Vision at the Presentation and After Management in Eyes of Saudi Children with Open Globe Injuries (OGI) |
 |
Figure 1 Causative agent of injury in children with open globe injuries (OGI) in a tertiary eye hospital of central Saudi Arabia. |
 |
Figure 2 Slitlamp photograph showing (A). Eye with open globe injury. (B) Following repair of globe injury. |
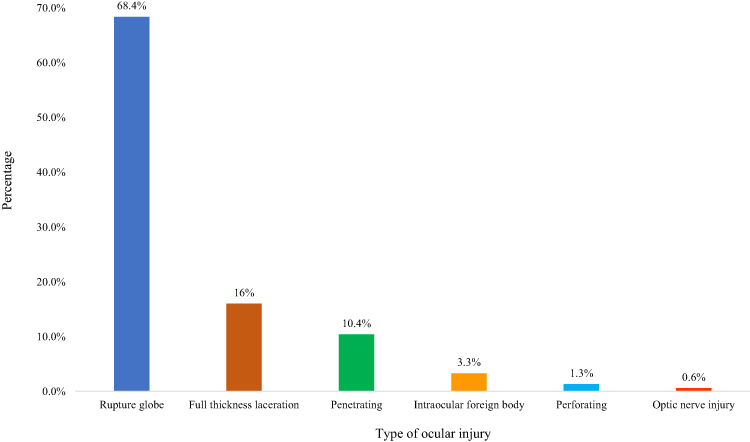 |
Figure 3 Types of ocular injury in children with open globe injuries (OGI) in a tertiary eye hospital of central Saudi Arabia (N = 664) eye. |
Discussion
This large cohort of children with OGI exhibited SVI in this group, even though normal functional vision could be restored in 4 of 10 eyes despite routine treatment. Vision at the presentation is essential for documentation because it permits the prediction of the final visual outcomes of eyes with OGI. Those with OGI involving the cornea and corneoscleral junction had superior visual results, while penetrating injuries and OGIs affecting the posterior portion of the eyeball result in poor visual results. A study by Alali et al17 reviewed 63 cases of open globe injuries in Tabuk City, Saudi Arabia. Nearly half of the cases were children <18 years of age. More males were affected by OGI. The change in BCVA grades before and at last follow-up after surgery was not statistically significant. Final visual acuity was associated with age, while other characteristics such as type and ocular tissue damage had no effect on visual outcomes.17 A small sample of children with OGI in this study17 should be noted before comparing the outcome of the present study.
Nearly half of the children with OGI were <5 years old, while only 10% were >10 years old. In contrast, Liu et al18 observed that the mean age of children with OGI in a Chinese region was 11.6 years. In Canada, Bunting et al19 found that 45% of children with OGI were <5 years old. Consequently, there is a wide range of vulnerable age groups among children with OGI.
The percentage of males with OGI was greater than that of girls, which is similarly noted in Canada and the United States.19,20 In our research, the ratio of males to females changed among three age groups of children. It was remarkably high among children aged ≥10. Ilhan et al21 also observed a similar gender ratio variation in OGI. More outdoor activities among older boys might explain this higher risk of OGI.
Bilateral OGI was uncommon, with only a 0.3% bilateral OGI rate, which was 2.2% in a Chinese study.18 In our research, the percentage of patients with unilateral OGI with right eyes was greater than those with left eyes. In contrast, 68% of the eyes with OGI in Nigerian children22 were left-sided. It is difficult to explain the logic and inference of one eye’s preponderance over another in OGI. Perhaps a person’s reflex to avoid damage is determined by which side of the brain is dominant. Among the underlying causes, metallic items caused one-third of OGI. In a research from Turkey, OGI caused by metal accounts for 50% in children.21 In our study, children’s wooden items were the cause of OGI. In the research by Ilham et al,21 wooden items accounted for one-fourth of the causes of OGI.
Only 1.5% of our cohort experienced OGI due to road traffic accidents (RTA). In an investigation conducted in the USA,20 RTA was responsible for 9% of OGIs in children. RTA has caused 4.7% of all deaths in Saudi Arabia and has climbed to 27.4/100,000 population.23 The low incidence of OGI may be attributable to a high death rate or the fact that these children have sustained significant brain injuries due to RTA and are receiving priority care at pediatric critical care units in regular hospitals.
In our research, more than two-thirds of OGI had ruptured globes. Our study reveals that the majority of injuries occur in zone II. Lesniak et al20 found that 49% of zone I injuries, 29% of zone II injuries, and 21% of zone III injuries made up the total OGIs in children. The visual result of zone I injuries is superior to those of other zones.20,24 The presenting visual acuity in our study indicated that <10% of eyes with OGI did not have visual impairment (SVI), which indicates the degree of vision impairment caused by such injuries in children prior to the initiation of treatment. It might also be attributed to late presentation, which causes corneal edema, lenticular abnormalities that affect vision, and macular edema.11 In our research, about 8% of eyes with OGI presented with NLP. In Nigeria, where children’s access to prompt eye care is limited, as many as 25.6% of children with OGI lost vision.22 The number of eyes with NLP increased from 8% to 17.6% in the last follow-up after treatment. This indicates that a guarded prognosis should be stated at the time of presentation, even if the affected eye with OGI retains residual vision. Following initial globe closure, several patients may have had endophthalmitis, retinal detachment, or phthisis bulbi. The attending surgeon may have elected to enucleate or eviscerate the eye to prevent sympathetic ophthalmia in the other eye, treat a painful blind eye, or commence orbit socket rebuilding for cosmetic reasons.25–29
In our study, we found that one in five eyes had normal functional vision, and a comparable proportion had mild visual impairment to SVI after treatment of the eye with OGI. More than one-third of treated eyes may result in unsatisfactory vision rehabilitation. A review of OGI among Canadian children19 revealed a similar percentage of visually impaired and blind individuals.
A study in Turkey found that 54% of eyes with OGI gained vision better than 0.5 following treatment of OGI in children.30 The small sample size and a high number of eyes with zone I damage in this series30 may account for the high proportion of patients with normal functional vision. Better vision at the presentation was a predictor of good visual recovery following treatment of OGI.6,9,19,31–33
These criteria should be included in emergency department staff training. Parents should be provided with a guarded prognosis if their children have poor prognostic indicators.
Our study has a few limitations. As this was a retrospective evaluation of paper and electronic health records, information on injuries were incomplete. Therefore, we could not investigate the seasonal variation in OGI or the influence of injury location on OGI outcomes.
Conclusion
OGI was identified as a leading cause of unilateral blindness. Many children could not achieve normal, functional vision despite the intervention of skilled care providers with sub-specializations and conventional treatment. One out of every six children required eyeball removal and orbital reconstructive therapy. The gender of the child with OGI was not associated with a change in visual acuity at the last follow-up; nevertheless, the type of injury was associated with the change in visual acuity at the last follow-up. Proper documenting of risk variables and predictors, such as visual acuity at presentation, type of injury, causative agent, and eye zone, enable the care practitioner to anticipate visual outcomes after conventional therapy of OGI in children.
Abbreviations
OGI, Open Global Injury; UCVA, Uncorrected Visual Acuity; BCVA, Best Corrected Visual Acuity; NLP, No Light Perception; SPSS, Statistical Package for Social Sciences; SVI, Severe Visual Impairment; RTA, Road Traffic Accident.
Ethical Statement
This study was authorized by the King Khaled Eye Specialist Hospital’s local ethical board and followed the Helsinki Declaration’s tenets. All participants’ parents/guardians have provided written informed consent for their children to participate in this study.
Acknowledgments
The abstract of this paper was presented at the ARVO 2023 Annual Meeting as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Investigative Ophthalmology & Visual Science June 2023, Vol.64.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This manuscript received no funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Quartantri ND. Demography of Ocular Trauma in Pediatrics Patient, A Systematic Review. Int J Health Sci. 2022;1(5):538–545. doi:10.54543/kesans.v1i5.56
2. Miller KE. Pediatric ocular trauma: an update. Curr Ophthalmol Rep. 2017;5(2):107–113. doi:10.1007/s40135-017-0130-7
3. Lucio R, Nelson TL. Effective practices in the treatment of trauma in children and adolescents: from guidelines to organizational practices. J Evidence Infor Social Work. 2016;13(5):469–478. doi:10.1080/23761407.2016.1166839
4. Gupta B, Sian I, Agrawal R. Ophthalmic trauma: risk and management update. Expert Rev Ophthalmol. 2014;9(4):315–329. doi:10.1586/17469899.2014.931808
5. Hoskin AK, Watson SL, Mackey DA, et al. Eye injury registries–A systematic review. Injury. 2019;50(11):1839–1846. doi:10.1016/j.injury.2019.07.019
6. Schörkhuber MM, Wackernagel W, Riedl R, et al. Ocular trauma scores in paediatric open globe injuries. Br J Ophthalmol. 2014;98(5):664–668. doi:10.1136/bjophthalmol-2013-304469
7. Abbott J, Shah P. The epidemiology and etiology of pediatric ocular trauma. Surv Ophthalmol. 2013;58(5):476–485. doi:10.1016/j.survophthal.2012.10.007
8. Kadappu S, Silveira S, Martin F. Aetiology and outcome of open and closed globe eye injuries in children. Clin Experiment Ophthalmol. 2013;41(5):427–434. doi:10.1111/ceo.12034
9. Li X, Zarbin MA, Bhagat N. Pediatric open globe injury: a review of the literature. J Emerg Trauma Shock. 2015;8(4):216–223. doi:10.4103/0974-2700.166663
10. Zhou Y, DiSclafani M, Jeang L, et al. Open globe injuries: review of evaluation, management, and surgical pearls. Clin Ophthalmol. 2022;16:2545. doi:10.2147/OPTH.S372011
11. Placide J, Ip CS, Le BH, et al. An Update on the Management of traumatic pediatric Open Globe Repair: prognostication and Complication Management. Int Ophthalmol Clin. 2022;62(1):203–218. doi:10.1097/IIO.0000000000000399
12. Kuhn F, Morris R, Witherspoon CD. Birmingham Eye Trauma Terminology (BETT): terminology and classification of mechanical eye injuries. Ophthalmol Clin North Am. 2002;15(2):139–143. doi:10.1016/S0896-1549(02)00004-4
13. Dursun Ö, Özer Ö, Vatansever M, et al. Comparison of two scoring systems in pediatric open globe injuries. J Craniofacial Surgery. 2022;33(2):e105–107. doi:10.1097/SCS.0000000000007935
14. Man CYW, Steel D. Visual outcome after open globe injury: a comparison of two prognostic models—the ocular trauma score and the classification and regression tree. Eye. 2010;24(1):84–89. doi:10.1038/eye.2009.16
15. Dean AG, Sullivan KM, Soe MM. OpenEpi: open Source Epidemiologic Statistics for Public Health, Version. Available from: www.OpenEpi.com.
16. World Health Organization. International Statistical Classification of Diseases and Related Health Problems: Tenth Revision. Geneva; 1992.
17. Alali N, ALBalawi HB, Albazei A, et al. Epidemiological characteristics and outcome of open globe injuries in Tabuk City, Kingdom of Saudi Arabia: retrospective cohort study. Ophthalmol Therapy. 2022;11(2):759–769. doi:10.1007/s40123-022-00475-1
18. Liu X, Liu Z, Liu Y, et al. Determination of visual prognosis in children with open globe injuries. Eye. 2014;28(7):852–856. doi:10.1038/eye.2014.108
19. Bunting H, Stephens D, Mireskandari K. Prediction of visual outcomes after open globe injury in children: a 17-year Canadian experience. J Am Assoc Pediatric Ophthalmol Strabismus. 2013;17(1):43–48. doi:10.1016/j.jaapos.2012.10.012
20. Lesniak SP, Bauza A, Son JH, et al. Twelve-year review of pediatric traumatic open globe injuries in an urban US population. J Pediatr Ophthalmol Strabismus. 2012;49(2):73–79. doi:10.3928/01913913-20110712-02
21. Ilhan HD, Bilgin AB, Cetinkaya A, et al. Epidemiological and clinical features of paediatric open globe injuries in southwestern Turkey. Int J Ophthalmol. 2013;6(6):855–860. doi:10.3980/j.issn.2222-3959.2013.06.20
22. Ojabo CO, Malu KN, Adeniyi OS. Open globe injuries in Nigerian children: epidemiological characteristics, etiological factors, and visual outcome. Middle East Afr J Ophthalmol. 2015;22(1):69–73. doi:10.4103/0974-9233.148352
23. Ahmed S, Mahmood M, Rizvi SA, et al. Frequency and nature of road traffic injuries: data of more than 10,000 patients from Ha’il, Saudi Arabia. Cureus. 2019;11(1):667.
24. Yildiz M, Kıvanç SA, Akova-Budak B, et al. An important cause of blindness in children: open globe injuries. J Ophthalmol. 2016;2016:1–5. doi:10.1155/2016/7173515
25. Arevalo JF, Garcia RA, Al-Dhibi HA, et al. Update on sympathetic ophthalmia. Middle East Afr J Ophthalmol. 2012;19(1):13–21. doi:10.4103/0974-9233.92111
26. Ojuok E, Uppuluri A, Langer PD, et al. Predictive factors of enucleation after open globe injuries. Graefe’s Arch Clin Exp Ophthalmol. 2021;259(1):247–255. doi:10.1007/s00417-020-04794-6
27. Dave TV, Das AV, Mohapatra S, et al. Demography, Clinical Settings and Outcomes in Evisceration with Implant: an Electronic Medical Records Driven Analytics of 2071 Cases. Semin Ophthalmol. 2022;1–8.
28. Savar A, Andreoli MT, Kloek CE, et al. Enucleation for open globe injury. Am J Ophthalmol. 2009;147(4):595–600. doi:10.1016/j.ajo.2008.10.017
29. Uppuluri S, Uppuluri A, Langer PD, et al. Enucleation in pediatric open globe injuries: demographics and risk factors. Graefe’s Arch Clin Exp Ophthalmol. 2022;260(9):3115–3122. doi:10.1007/s00417-022-05618-5
30. Çetin EN, Saraç G, Kaşıkçı A, et al. Epidemiologic and clinical features of open-globe injuries in childhood. Available from: http://acikerisim.pau.edu.tr:8080/xmlui/handle/11499/8623.
31. Madhusudhan AP, Evelyn-Tai LM, Zamri N, et al. Open globe injury in Hospital Universiti Sains Malaysia - A 10-year review. Int J Ophthalmol. 2014;7(3):486–490. doi:10.3980/j.issn.2222-3959.2014.03.18
32. Park SJ, Son BJ. The Relationship between Visual Outcome and Ocular Trauma Score after Open Globe Injuries in Children. J Korean Ophthalmol Society. 2018;59(11):1062–1070. doi:10.3341/jkos.2018.59.11.1062
33. AlGhadeer H, Khandekar R. Clinical Profile, Etiology, and Management Outcomes of Pediatric Ocular Trauma in Saudi Arabia. Pediatr Emerg Care. 2022;38(10):e1626–e1630. doi:10.1097/PEC.0000000000002581
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.