Back to Journals » Clinical Interventions in Aging » Volume 19
Characteristics and Prognosis of Type 2 Myocardial Infarction Through Worsening Renal Function and NT-proBNP in Older Adults with Pneumonia
Authors Ma J, Bian S, Li A, Chen Q
Received 18 December 2023
Accepted for publication 12 March 2024
Published 28 March 2024 Volume 2024:19 Pages 589—597
DOI https://doi.org/10.2147/CIA.S438541
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Jinling Ma,* Suyan Bian, Ang Li, Qian Chen*
Department of Geriatric Cardiology, the Second Medical Center and National Clinical Research Center for Geriatric Diseases, Chinese PLA General Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinling Ma, Department of Geriatric Cardiology, the Second Medical Center and National Clinical Research Center for Geriatric Diseases, Chinese PLA General Hospital, No. 28, Fuxing Road, Haidian District, Beijing, 100853, People’s Republic of China, Email [email protected]
Background: Type 2 myocardial infarction (MI) is becoming more recognized. This study aimed to assess the factors linked to type 2 MI in older adults with pneumonia and further determine the predictive factors of 90-day adverse events (refractory heart failure, cardiogenic shock, and all-cause mortality).
Methods: A single-center retrospective analysis was conducted among older adults with pneumonia. The primary outcome was the prevalence of type 2 MI. The secondary objective was to assess the adverse events in these patients with type 2 MI within 90 days.
Results: A total of 2618 patients were included. Of these, 361 patients (13.8%) suffered from type 2 MI. Multivariable predictors of type 2 MI were chronic kidney disease (CKD), age-adjusted Charlson comorbidity index (ACCI) score, and NT-proBNP > 4165pg/mL. Moreover, the independent predictive factors of 90-day adverse events included NT-proBNP > 4165pg/mL, age, ACCI score, and CKD. The Kaplan–Meier adverse events curves revealed that the type 2 MI patients with CKD and NT-proBNP > 4165pg/mL had a higher risk than CKD or NT-proBNP > 4165pg/mL alone.
Conclusion: Type 2 MI in older pneumonia hospitalization represents a heterogeneous population. Elevated NT-proBNP level and prevalence of CKD are important predictors of type 2 MI and 90-day adverse events in type 2 MI patients.
Keywords: type 2 myocardial infarction, pneumonia, older, mortality
Introduction
Type 2 myocardial infarction (MI) is a heterogeneous group with different aetiologies and triggers, and increasingly recognized.1–3 Compared with type 1 MI patients, type 2 MIs were significantly older and had more comorbidities.4–6 Type 2 MI is caused by an imbalance between myocardial oxygen supply and demand during acute illness, such as haemodynamic instability, tachycardia, respiration failure, severe anemia, congestive heart failure, and recent surgical procedures.7–12 The pathogenesis of the disease is multifactorial; various and heterogeneous conditions can coexist and lead to a mismatch between myocardial supply and demand.13 Age-related factors may act as potential triggers and are closely linked to the diagnosis, therapy, and prognosis of type 2 MI. The occurrence of type 2 MI varies widely between 1% and 74% among all cases of MI,3,14–16 and it is high among elderly patients. Type 2 MI is frequently induced by haemodynamic instability or respiration failure.17–21 Medical triggers have association with all-cause death rate.22 The mortality after type 2 MI differs depending on the pre-existing illness, and hypoxic respiratory failure is linked with the highest death rate.23 Moreover, a significant increase in chronic kidney disease (CKD)-related mortality has been observed, and such a result is mainly due to the increase in ages 80 years or more.24
Given their high complexity and vulnerability, older adults with greater comorbidities are particularly prone to the incidence of type 2 MI. Older adults with pneumonia have a greater prevalence of multiple co-morbidities, and higher occurrence of frailty. Therefore, the aim of this study was to describe the clinical features and assess the associated factors with type 2 MI in the adults with pneumonia aged 80 years and older. Meanwhile, we determined the predictive factors of 90-day adverse events (refractory heart failure, cardiogenic shock, and all-cause death) in these patients of type 2 MI.
Methods
Study Population
A retrospective observational analysis was performed among patients who were aged 80 years and older admitted with pneumonia consecutively to Chinese PLA General Hospital from December 2016 to December 2022. The patients underwent N-terminal B-type natriuretic peptide (NT-proBNP) measurement on the basis of medical indication in 24 hours of admission. Demographic and clinical information were obtained from relevant electronic clinical files. The age-adjusted Charlson comorbidity index (ACCI) score was calculated for assessment of co-morbidity severity. ACCI is a validated method for the prediction of mortality risk on the basis of co-morbidities.25 The study was approved by research ethics committees of Chinese PLA General Hospital, and informed consent was waived due to its retrospective design (No. S2021–096-01).
Measurement of Plasma NT-proBNP
The measurement of NT-proBNP was through electrochemiluminescence immunoassay using the Dimension Vista 500 Intelligent Laboratory System (Siemens Healthcare Diagnostics, Deerfield, Illinois, USA).
Diagnosis of Type 2 MI
According to the Fourth Universal Definition of MI, the definition of type 2 MI was the occurrence of myocardial necrosis assessed by elevated cTnI, resulting from the imbalance between oxygen supply and demand of myocardium.2 Two cardiologists conducted a thorough review of all medical records and made a final determination of type 2 MI. A third cardiologist were responsible for discrepancies in diagnosis. Patients during dialysis due to end-stage kidney failure were excluded from the analysis. Additionally, the patients who had Takotsubo cardiomyopathy, type 3, 4, or 5 MI, or insufficient data available electronically were also excluded.
Clinical Outcomes
The primary outcome of the research was the incidence of type 2 MI in older adults with pneumonia. The secondary outcome was the 90-day adverse events (refractory heart failure, cardiogenic shock, and all-cause death) in these type 2 MI patients after initial presentation. The data of follow-up were collected through medical files or telephone interviews.
Statistical Analysis
Distributed normally continuous data were presented as the mean ± standard deviation, while the percentages and frequencies were used to present the categorical variables. χ2 tests were employed to compare categorical variables. In the univariate analysis these variables with P < 0.05 were included in the multivariate analysis. Multivariable logistic regression was performed to determine the independent risk factors after adjusting for confounding variables. Moreover, logistic regression was employed for prediction of adverse events (refractory heart failure, cardiogenic shock, and all-cause death) within 90 days. The findings were expressed as adjusted odds ratios (OR) and 95% confidence interval (CI). Adverse event curves were assessed using the Kaplan–Meier method and the differences in event rates among groups were compared through the Log rank test. We analyzed all data through SPSS 20 (IBM SPSS Statistics, Armonk, New York, USA). Statistical significance was defined as P < 0.05.
Results
Baseline Characteristics
We included a total of 2618 patients with pneumonia as a primary diagnosis. Of these, 361 patients (13.8%) had type 2 MI. The average age of the total cohort was 88.14 ± 5.66 years. Table 1 shows the patient demographics and characteristics.
 |
Table 1 Baseline Characteristics of Pneumonia Patients with and without Type 2 MI |
Factors Linked to the Occurrence of Pneumonia with Type 2 MI
Compared with pneumonia patients who did not have type 2 MI, those with type 2 MI exhibited a greater prevalence of CKD, NT-proBNP > 4165pg/mL, and higher ACCI scores (Table 1). Moreover, patients diagnosed with type 2 MI had a greater tendency to develop congestive heart failure NYHA III/IV. Stepwise multivariate logistic regression showed that CKD (OR 7.354 [3.604–15.005] P < 0.001), ACCI score (OR 1.093 [1.030–1.160] P = 0.003), and NT-proBNP > 4165pg/mL (OR 12.277 [7.778–19.379] P < 0.001) were independent predictors for type 2 MI after adjustments for confounding factors (Table 2) (Figure 1).
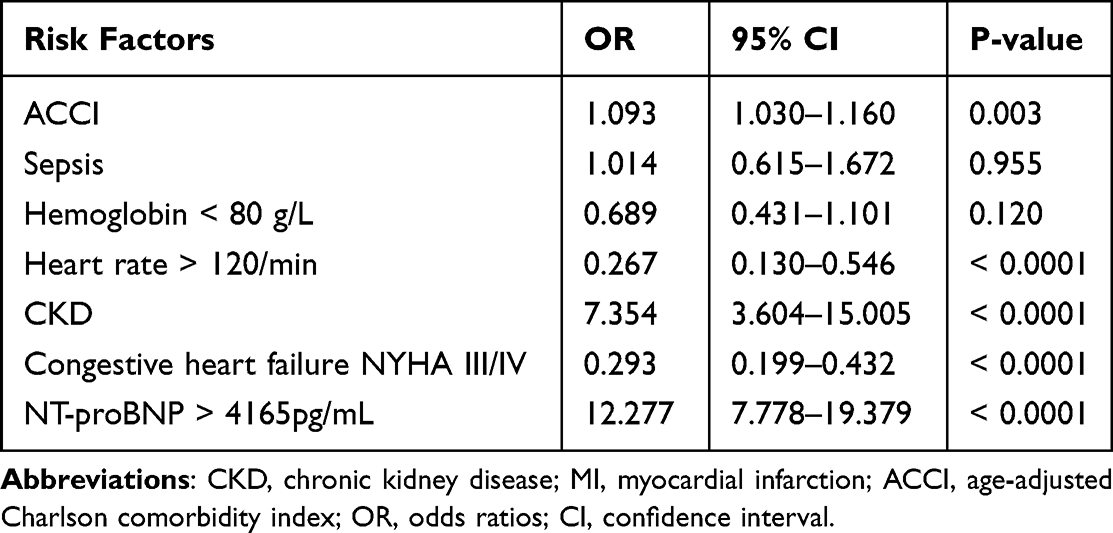 |
Table 2 Multivariate Logistic Regression Analysis of Risk Factors of Type 2 MI in Older Adults with Pneumonia |
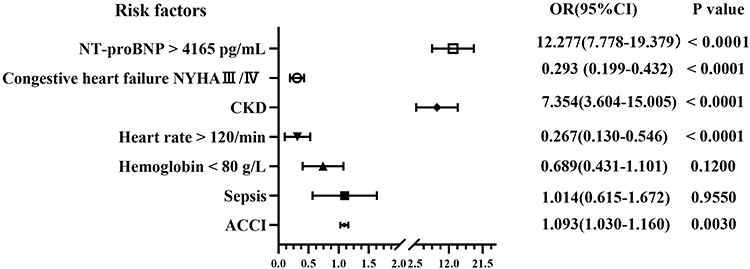 |
Figure 1 Associations of risk factors with type 2 MI in older adults with pneumonia. Abbreviations: CKD, chronic kidney disease; ACCI, age-adjusted Charlson comorbidity index. |
Factors Associated with Adverse Events (Refractory Heart Failure, Cardiogenic Shock, and All-Cause Death) of Type 2 MI Within 90 Days
Table 3 presented the clinical features of the type 2 MI patients during the 90-day follow-up. Compared with the patients without adverse events, those who experienced adverse events were older and had increased incidence of congestive heart failure NYHA III/IV, NT-proBNP > 4165pg/mL, as well as CKD. Furthermore, higher 90-day adverse events were significantly associated with higher ACCI score (Table 3).
 |
Table 3 Characteristics of Type 2 MI Based on the Occurrence of 90-Day Adverse Events (Refractory Heart Failure, Cardiogenic Shock, and All-Cause Death) |
In type 2 MI pneumonia patients, multivariable logistic regression after adjustment further showed that independent predictors of 90-day adverse events included NT-proBNP > 4165pg/mL (OR 31.53 [12.575–79.043] P < 0.0001), age (OR 1.30[1.211–1.406] P < 0.0001), ACCI score (OR 1.28 [1.111–1.469] P = 0.0006), and CKD (OR 10.06 [4.482–22.602] P < 0.0001) (Table 4) (Figure 2).
 |
Table 4 Multivariate Logistic Regression Analysis of Predictive Factors of 90-Day Adverse Events (Refractory Heart Failure, Cardiogenic Shock, and All-Cause Death) in Older Pneumonia Patients with Type 2 MI |
 |
Figure 2 Associations of risk factors with 90-day adverse events in older pneumonia patients of type 2 MI. Abbreviations: CKD, chronic kidney disease; ACCI, age-adjusted Charlson comorbidity index. |
The Kaplan–Meier Adverse Events (Refractory Heart Failure, Cardiogenic Shock, and All-Cause Death) Curves
The Kaplan–Meier adverse events curves revealed that the type 2 MI patients, who had CKD along with NT-proBNP > 4165pg/mL were at higher risk than CKD or NT-proBNP > 4165pg/mL alone (Log rank test, P = 0.0012) (Figure 3). Moreover, the Kaplan–Meier adverse events curves demonstrated that the type 2 MI patients with both CKD and NT-proBNP > 8330pg/mL (4165×2) had a considerably higher occurrence of adverse events than CKD and NT-proBNP > 4165pg/mL (Log rank test, P = 0.0082) (Figure 4).
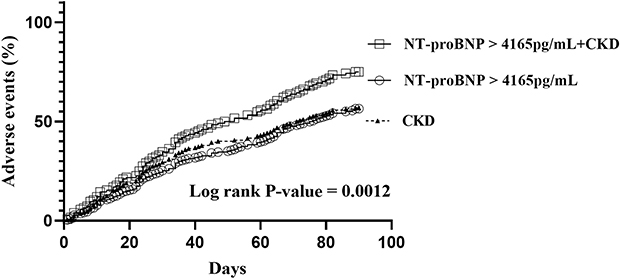 |
Figure 3 Kaplan–Meier 90-day adverse events (refractory heart failure, cardiogenic shock, and all-cause death) curves according to NT-proBNP level and CKD. Abbreviation: CKD, chronic kidney disease. |
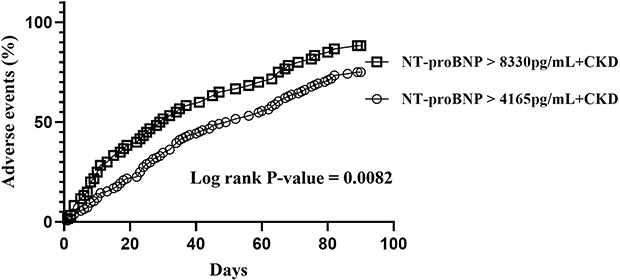 |
Figure 4 Kaplan–Meier 90-day adverse events (refractory heart failure, cardiogenic shock, and all-cause death) curves according to NT-proBNP level and CKD. Abbreviation: CKD, chronic kidney disease. |
Discussion
In this real-world study, we demonstrated that older pneumonia patients with type 2 MI represented a heterogeneous population with underlying co-morbidities compared with pneumonia patients without type 2 MI. High ACCI score and NT-proBNP > 4165pg/mL were important predictors of type 2 MI in pneumonia patients, and also patients with a history of CKD had a higher likelihood of developing the condition. These results are in line with the findings of previous research, which showed that the most common etiologies among comorbidities associated with type 2 MI comprised inflammation and CKD.6,9,18,20,23 In addition, in pneumonia patients with type 2 MI, NT-proBNP > 4165pg/mL, age, and CKD were independent predictors of 90-day adverse events. We identified 4165pg/ mL as the optimal value for NT-proBNP, which was based on our experience and another study.26 Importantly, the combined use of CKD and NT-proBNP improved the identification of 90-day adverse events. It would be more effective to assess both at the same time. Moreover, the presence of CKD and NT-proBNP > 8330pg/mL (4165×2) were significantly more likely to have adverse events than CKD and NT-proBNP > 4165pg/mL.
To date, the epidemiological information of type 2 MI has shown that there is considerable variation. Type 2 MI is triggered by numerous heterogeneous conditions.2 In the elderly, the influence of aging, comorbidities, and their mutual interactions during acute illness led to an increased risk of the myocardial supply/demand mismatch. The incidence of type 2 MI is reliant on the population, comorbidities, definition, adjudication method, chosen cardiac biomarkers, and cut-off values employed for the diagnosis.3,27,28 Patients of type 2 MI are at higher risk of adjusted all-cause death.9,29–32 Recognition of the triggers of type 2 MI is essential for its prevention. The causes of the mismatch between oxygen supply and demand that leads to type 2 MI may be multifactorial, particularly in patients characterized by complex illnesses or multiple underlying diseases. These diseases tend to cluster in cohorts with increasing age. In addition, medical indicators have association with all-cause mortality.22 Assessing risk factors for 90-day adverse events play an important role in older type 2 MI individuals. The mortality after type 2 MI is significantly linked to the triggering factor for the mismatch of supply/demand.8 The explanation of cause-specific mortality analyses could be that this depends on various clinical patterns, intertwining acute and chronic illnesses, rather than individual predisposing factors. Thus, these factors possess the ability to cause a mismatch between demand and supply, resulting in type 2 MI. And the prognosis is associated with provoking factors. CKD overlapped with several conditions, including infection, respiratory failure, and displayed a significant correlation with reduced cardiac troponin clearance.23 The existence and the degree of CKD implied an unfavorable risk pattern, and it became increasingly linked with more co-morbidities.33 NT-proBNP plays a vital role in assessing the risk level of patients suffering from heart failure.34 The change of NT-proBNP was associated significant decrease in eGFR, which may be in part due to decreased clearance of NT-proBNP with worsening kidney function and in part related to increased myocardial stress in the setting of kidney disease.35 Elevated NT-proBNP levels specific to CKD were linked to higher risk of adverse events. In CKD patients, elevation of NT-proBNP was independently linked with higher risks of cardiovascular and all-cause mortality.36 Both serum creatinine and NT-proBNP could offer direction for individuals with heart failure.37 The long-term mortality risk of patients admitted for heart failure was affected by their renal function at admission and the early alterations of NT-proBNP levels.38
These present findings highlight the important predictors of type 2 MI, which may help physicians to differentiate patients presenting with type 2 MI. This outcome seems to diverge from other studies and could potentially be attributed to variations of coexisting medical conditions and age. Identifying a correlation between clinical features, underlying factor and prognosis can provide a valuable tool in assessing risk stratification. In addition, this study may guide practitioners in determining who could benefit from NT-proBNP target for early intensive intervention. Treating the underlying factors of type 2 MI is advised, along with implementing individualized care.39–41 This predictive analysis for 90-day adverse events can help in the risk stratification of patients with type 2 MI given that these groups are characterized by age, high prevalence of comorbidities, CKD and elevated levels of NT-proBNP. These findings emphasize elevation NT-proBNP specific to CKD could be identified to guide their use in this population. Further studies are needed to more effectively investigate the underlying factors and triggers that contribute to type 2 MI in real-life situations. Risk stratification and optimal therapeutic strategies should be tailored for the triggers of type 2 MI.
There were several limitations in the present study. First, this research was a retrospective analysis without uniform intervals for the collection of biomarkers. Furthermore, the interpretation on the possible precipitating factors of type 2 MI may be incomplete, and the frequency of type 2 MI can be underestimated. Second, the enrolment of patients was limited to older adults with pneumonia. Therefore, extrapolation to the whole population of type 2 MI patients was difficult. Several of these patients might have been hospitalized for another reason, and their features and death rates may vary. Third, despite multivariable adjustment, the database did not contain data on confounding variables, including echocardiographic outcomes and medications. It is likely that treatments were not standardized and the strategies and outcomes were different. Fourth, given that the patients receiving chronic hemodialysis were excluded, these findings cannot be extrapolated to patients with end-stage renal disease requiring dialysis. Fifth, participants of the study were derived from limited sources of population, which limited the generalizability to other groups. Therefore, the rates of occurrence cannot be compared directly to those previously documented. Sixth, the absence of coronary angiography or functional cardiac imaging is a disadvantage. Consequently, the prevalence of type 1 MI might be underestimated significantly. Possibly, several type 2 MIs were unrecognized type 1 MIs. Seventh, although these diagnoses were according to the Fourth Universal Definition of Myocardial Infarction with central adjudication by experienced cardiologists, misclassification and selection bias might have still occurred. This problem appears to be more prevalent among elderly individuals due to the frequent occurrence of non-typical clinical manifestations of MI. Finally, the 90-day follow-up period was relatively short. Therefore, it was not possible to determine the effect of type 2 MI on long-term results. Nonetheless, the study conducted a detailed analysis of a real-world group of older adults with pneumonia who developed type 2 MI. Multi-center prospective studies with sophisticated evaluations should be conducted to further confirm and address these limitations.
Conclusions
Type 2 MI in older adults with pneumonia hospitalization represents a heterogeneous population with a great burden of comorbidities. Elevated NT-proBNP levels and prevalence of CKD are important independent predictors of type 2 MI and 90-day adverse events in type 2 MI patients. The combination of CKD and elevated NT-proBNP levels is more predictive than either elevated NT-proBNP levels or CKD alone.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki. It was approved by research ethics committees of Chinese PLA General Hospital, and informed consent was waived due to its retrospective design (No. S2021–096-01). Patient data were kept confidential in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Smer A, Squires RW, Aboeata A, et al. Type 2 myocardial infarction: current concepts and our experience with cardiac rehabilitation. J Cardiopulm Rehabil Prev. 2021;41(3):147–152. doi:10.1097/HCR.0000000000000550
2. Nestelberger T, Boeddinghaus J, Badertscher P, et al. Effect of definition on incidence and prognosis of type 2 myocardial infarction. J Am Coll Cardiol. 2017;70(13):1558–1568. doi:10.1016/j.jacc.2017.07.774
3. Sandoval Y, Jaffe AS. Type 2 myocardial infarction: JACC review topic of the week. J Am Coll Cardiol. 2019;73(14):1846–1860. doi:10.1016/j.jacc.2019.02.018
4. Singh A, Gupta A, DeFilippis EM, et al. Cardiovascular mortality after type 1 and type 2 myocardial infarction in young adults. J Am Coll Cardiol. 2020;75(9):1003–1013. doi:10.1016/j.jacc.2019.12.052
5. Chapman AR, Shah ASV, Lee KK, et al. Long-term outcomes in patients with type 2 myocardial infarction and myocardial injury. Circulation. 2018;137(12):1236–1245. doi:10.1161/CIRCULATIONAHA.117.031806
6. McCarthy CP, Kolte D, Kennedy KF, et al. Patient characteristics and clinical outcomes of type 1 versus type 2 myocardial infarction. J Am Coll Cardiol. 2021;77(7):848–857. doi:10.1016/j.jacc.2020.12.034
7. Wereski R, Kimenai DM, Bularga A, et al. Risk factors for type 1 and type 2 myocardial infarction. Eur Heart J. 2022;43(2):127–135. doi:10.1093/eurheartj/ehab581
8. Raphael CE, Roger VL, Sandoval Y, et al. Incidence, trends, and outcomes of type 2 myocardial infarction in a community cohort. Circulation. 2020;141(6):454–463. doi:10.1161/CIRCULATIONAHA.119.043100
9. Tripathi B, Tan BE, Sharma P, et al. Characteristics and outcomes of patients admitted with type 2 myocardial infarction. Am J Cardiol. 2021;157:33–41. doi:10.1016/j.amjcard.2021.07.013
10. Neumann JT, Weimann J, Sörensen NA, et al. A biomarker model to distinguish types of myocardial infarction and injury. J Am Coll Cardiol. 2021;78(8):781–790. doi:10.1016/j.jacc.2021.06.027
11. McCarthy CP, Vaduganathan M, Singh A, et al. Type 2 myocardial infarction and the hospital readmission reduction program. J Am Coll Cardiol. 2018;72(10):1166–1170. doi:10.1016/j.jacc.2018.06.055
12. Nestelberger T, Boeddinghaus J, Lopez-Ayala P, et al. Cardiovascular biomarkers in the early discrimination of type 2 myocardial infarction. JAMA Cardiol. 2021;6(7):771–780. doi:10.1001/jamacardio.2021.0669
13. Putot A, Jeanmichel M, Chague F, et al. Type 2 myocardial infarction: a geriatric population-based model of pathogenesis. Aging Dis. 2020;11(1):108–117. doi:10.14336/AD.2019.0405
14. Gaggin HK, Liu Y, Lyass A, et al. Incident type 2 myocardial infarction in a cohort of patients undergoing coronary or peripheral arterial angiography. Circulation. 2017;135(2):116–127. doi:10.1161/CIRCULATIONAHA.116.023052
15. Hung J, Roos A, Kadesjö E, et al. Performance of the GRACE 2.0 score in patients with type 1 and type 2 myocardial infarction. Eur Heart J. 2021;42(26):2552–2561. doi:10.1093/eurheartj/ehaa375
16. McCarthy CP, Vaduganathan M, Januzzi JL. Type 2 myocardial infarction-diagnosis, prognosis, and treatment. JAMA. 2018;320(5):433–434. doi:10.1001/jama.2018.7125
17. McCarthy CP. Type 2 myocardial infarction and value-based programs: cutting the supply in the absence of demand. Am J Med. 2019;132(10):1117–1118. doi:10.1016/j.amjmed.2019.02.037
18. Thygesen K, Jaffe AS. The gloomy long-term prognosis of patients with type 2 myocardial infarction or myocardial injury. J Am Coll Cardiol. 2020;75(9):1014–1016. doi:10.1016/j.jacc.2020.01.004
19. Oblavatckii DV, Boldueva SA, Soloveva MV, et al. The frequency of type 2 myocardial infarction in the structure of hospital mortality according to 7-years data of a state university clinic. Kardiologiia. 2020;60(6):896. doi:10.18087/cardio.2020.6.n896
20. Rasla S, Thabet R. The prognostic yield of type 2 myocardial infarction. J Am Coll Cardiol. 2020;76(3):353. doi:10.1016/j.jacc.2020.03.089
21. McCarthy CP, Murphy S, Cohen JA, et al. Sex differences in patient characteristics, treatment strategies, and outcomes for type 2 myocardial infarction. J Am Coll Cardiol. 2019;73(24):3230–3232. doi:10.1016/j.jacc.2019.04.016
22. Hoang TH, Lazarev PV, Maiskov VV, et al. Concordance and prognostic relevance of angiographic and clinical definitions of myocardial infarction type. J Cardiovasc Pharmacol Ther. 2021;26(5):463–472. doi:10.1177/10742484211005929
23. Mohamed MO, Contractor T, Abramov D, et al. Sex-based differences in prevalence and outcomes of common acute conditions associated with type 2 myocardial infarction. Am J Cardiol. 2021;147:8–15. doi:10.1016/j.amjcard.2021.02.011
24. Navarra S, Solini A, Baroni MG, et al. A long-term nationwide study on chronic kidney disease-related mortality in Italy: trends and associated comorbidity. J Nephrol. 2022;35(2):505–515. doi:10.1007/s40620-021-01132-9
25. Zhang XM, Wu XJ, Cao J, et al. Effect of the age-adjusted Charlson comorbidity index on all-cause mortality and readmission in older surgical patients: a national multicenter, prospective cohort study. Front Med. 2022;9:896451. doi:10.3389/fmed.2022.896451
26. Adamo M, Pagnesi M, Mebazaa A, et al. NT-proBNP and high-intensity care for acute heart failure: the STRONG-HF trial. Eur Heart J. 2023;44(31):2947–2962. doi:10.1093/eurheartj/ehad335
27. Shah ASV, Sandoval Y, Noaman A, et al. Patient selection for high sensitivity cardiac troponin testing and diagnosis of myocardial infarction: prospective cohort study. BMJ. 2017;359:j4788. doi:10.1136/bmj.j4788
28. DeFilippis AP, Chapman AR, Mills NL, et al. Assessment and treatment of patients with type 2 myocardial infarction and acute nonischemic myocardial injury. Circulation. 2019;140(20):1661–1678. doi:10.1161/CIRCULATIONAHA.119.040631
29. Kimenai DM, Lindahl B, Chapman AR, et al. Sex differences in investigations and outcomes among patients with type 2 myocardial infarction. Heart. 2021;107(18):1480–1486. doi:10.1136/heartjnl-2021-319118
30. McCarthy CP, Murphy S, Rehman S, et al. Home-time after discharge among patients with type 2 myocardial infarction. J Am Heart Assoc. 2020;9(10):e015978. doi:10.1161/JAHA.119.015978
31. Lambrakis K, French JK, Scott IA, et al. The appropriateness of coronary investigation in myocardial injury and type 2 myocardial infarction (ACT-2): a randomized trial design. Am Heart J. 2019;208:11–20. doi:10.1016/j.ahj.2018.09.016
32. Arora S, Strassle PD, Qamar A, et al. Impact of type 2 myocardial infarction (MI) on hospital-level MI outcomes: implications for quality and public reporting. J Am Heart Assoc. 2018;7(7):e008661. doi:10.1161/JAHA.118.008661
33. De Luca L, Cappadona F, Temporelli PL, et al. Impact of eGFR rate on 1-year all-cause mortality in patients with stable coronary artery disease. Eur J Intern Med. 2022;101:98–105. doi:10.1016/j.ejim.2022.04.021
34. Núñez J, de la Espriella R, Rossignol P, et al. Congestion in heart failure: a circulating biomarker-based perspective. A review from the Biomarkers Working Group of the Heart Failure Association, European Society of Cardiology. Eur J Heart Fail. 2022;24(10):1751–1766. doi:10.1002/ejhf.2664
35. Jia X, Al Rifai M, Hoogeveen R, et al. Association of long-term change in N-Terminal Pro-B-Type natriuretic peptide with incident heart failure and death. JAMA Cardiol. 2023;8(3):222–230. doi:10.1001/jamacardio.2022.5309
36. Wang K, Zelnick LR, Anderson A, et al. Cardiac biomarkers and risk of mortality in CKD (the CRIC Study). Kidney Int Rep. 2020;5(11):2002–2012. doi:10.1016/j.ekir.2020.08.028
37. McCallum W, Tighiouart H, Kiernan MS, et al. Relation of kidney function decline and NT-proBNP with risk of mortality and readmission in acute decompensated heart failure. Am J Med. 2020;133(1):115–122.e2. doi:10.1016/j.amjmed.2019.05.047
38. Lorenzo M, Núñez G, Fuertes-Kenneally L, et al. The modifying role of admission renal function and decongestion. Eur J Intern Med. 2023;115:96–103.
39. Ariss RW, Minhas AMK, Nazir S, et al. Outcomes and resource utilization of atrial fibrillation hospitalizations with type 2 myocardial infarction. Am J Cardiol. 2021;152:27–33. doi:10.1016/j.amjcard.2021.04.036
40. Richter D, Guasti L, Koehler F, et al. Late phase of COVID-19 pandemic in general cardiology. A position paper of the ESC council for cardiology practice. ESC Heart Fail. 2021;8(5):3483–3494. doi:10.1002/ehf2.13466
41. Raphael CE, Roger VL, Sandoval Y, et al. Causes of death after type 2 myocardial infarction and myocardial injury. J Am Coll Cardiol. 2021;78(4):415–416. doi:10.1016/j.jacc.2021.05.026
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Characteristics of Elderly Hip Fracture Patients in Jordan: A Multicenter Epidemiological Study
Dawod MS, Alisi MS, Saber YO, Abdel-Hay QA, Al-Aktam BM, Alfaouri Y, Alfraihat LB, Albadaineh AA, Abuqudiri AZ, Odeh RM, Altamimi AAR, Alrawashdeh MA, Alebbini MM, Abu-Dhaim OA, Al-Omari AA, Alaqrabawi I, Alswerki MN, Abuawad A, Al Nawaiseh MR, Hammad Y, Al-Ajlouni J
International Journal of General Medicine 2022, 15:6591-6598
Published Date: 13 August 2022
Platelet-to-White Blood Cell Ratio as a Predictor of Mortality in Patients with Severe COVID-19 Pneumonia: A Retrospective Cohort Study
Thungthienthong M, Vattanavanit V
Infection and Drug Resistance 2023, 16:445-455
Published Date: 24 January 2023
A Prediction Scoring Model for the Effect of Withdrawal or Addition of Inhaled Corticosteroids in Patients with Chronic Obstructive Pulmonary Disease
Lee JH, Kim S, Oh YM
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:113-127
Published Date: 15 February 2023
Hospital Burden of Chronic Obstructive Pulmonary Disease in Hong Kong – The Trend from 2006 to 2014
Chan HS, Ko FWS, Chan JWM, Choo KL, So LKY, Lam DCL, Sin KM, Wong WY, Cheng YL, Wong MML
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:507-519
Published Date: 6 April 2023
Respiratory Infection Triggering Severe Acute Exacerbations of Chronic Obstructive Pulmonary Disease
Abi Abdallah G, Diop S, Jamme M, Legriel S, Ferré A
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:555-565
Published Date: 27 February 2024