Back to Journals » Cancer Management and Research » Volume 12
Characteristics and Management of TP53-Mutated Diffuse Large B-Cell Lymphoma Patients
Authors Qin Y, Jiang S ![]() , Liu P, Yang J, Yang S
, Liu P, Yang J, Yang S ![]() , He X, Zhou S, Gui L, Lin J, Du X, Yi Y, Sun Y, Shi Y
, He X, Zhou S, Gui L, Lin J, Du X, Yi Y, Sun Y, Shi Y ![]()
Received 27 June 2020
Accepted for publication 8 September 2020
Published 10 November 2020 Volume 2020:12 Pages 11515—11522
DOI https://doi.org/10.2147/CMAR.S269624
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Yan Qin,1,* Shiyu Jiang,1,* Peng Liu,1 Jianliang Yang,1 Sheng Yang,1 Xiaohui He,1 Shengyu Zhou,1 Lin Gui,1 Jing Lin,2 Xinhua Du,3 Yuting Yi,3 Yan Sun,1 Yuankai Shi1
1Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing Key Laboratory of Clinical Study on Anticancer Molecular Targeted Drugs, Beijing, People’s Republic of China; 2Burning Rock Biotech, Guangzhou, Mainland China; 3Geneplus Beijing, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuankai Shi
Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing Key Laboratory of Clinical Study on Anticancer Molecular Targeted Drugs, 17 Panjiayuan Nanli, Chaoyang District, Beijing 100021, People’s Republic of China
Tel +86 10 8778-8293
Fax +86 10 8777-8781
Email [email protected]
Background/Aim: TP53 mutation is recognized as a negative prognostic factor for patients with diffuse large B-cell lymphoma (DLBCL). Here, we present the characteristics of TP53mut DLBCL patients following investigation of the effect of a treatment approach on survival of TP53mut DLBCL patients.
Methods: A total of 44 DLBCL patients with TP53mut and treated with an R-CHOP regimen were included for analysis. Patients who failed to achieve a complete response (CR) to initial treatment or relapsed in the first 6 months after initial CR were deemed to have primary refractory disease.
Results: Among 44 patients harboring TP53 mutations who underwent upfront R-CHOP or R-CHOP–like treatment, 21 (47.7%) had limited-stage and 23 (52.3%) presented advanced-stage disease. Apart from the seven patients receiving upfront surgical resection, 37 had measurable disease under the R-CHOP regimen, with 59.1% (n=26) developing primary refractory disease. Seven limited-stage patients after early complete resection and one with residue resection remained event-free at median follow-up of 37 months. Multivariate analysis revealed that elevated baseline lactate dehydrogenase (LDH), extranodal involvement (two or more), Ann Arbor stage, and locoregional treatment (surgery or radiation therapy) were independent indicators for progression-free survival (PFS). After adjustment for baseline LDH and extranodal involvement, adding locoregional treatment including surgery and radiation to the R-CHOP regimen significantly improved PFS (p=0.008) and overall survival (p=0.017) in limited-stage TP53mut DLBCL patients compared to R-CHOP–only treatment.
Conclusion: This study presents the characteristics of TP53-mutated DLBCL and implies a potential benefit of locoregional treatment in limited-stage DLBCL patients with TP53 mutations.
Keywords: diffuse large B-cell lymphoma, TP53, surgery, survival, clinical benefit
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common lymphoid malignancy in non-Hodgkin’s lymphoma (NHL). Up to 50% of DLBCL patients can be cured with rituximab plus cyclophosphamide, hydroxydaunorubicin, Oncovin (vincristine) and prednisone (R-CHOP) chemotherapy, considered the standard first-line treatment,1–3 while the rest develop refraction or relapse and usually have poor prognosis. According to the literature, relapsed or refractoryDLBCL can be defined as nonachievement of complete response (CR), lacking response, or partial response in <6 months.4–7 Compared to other DLBCL patients, refractory patients have median overall survival (OS) <12 months with R-CHOP treatment.8–10 Therefore, identifying new clinical procedures to benefit DLBCL patients at higher risk of developing primary refraction under R-CHOP regimens is of great urgency.
TP53 mutation occurs in 20%–25% of DLBCL patients, and has been identified as one of the most frequently mutated genes in both germinal center Bcell (GCB) and activated B-cell subtypes in DLBCL patients.11–14 TP53 mutation is associated with p53 overexpression, where the protein plays an important role in cell death, DNA repair, transcription, metabolism, apoptosis, and autophagy.12 Dysfunction of p53 is observed in many malignant tumors.15–19 In DLBCL, TP53 mutation has been identified as an unfavorable prognostic factor for patients under a CHOP or R-CHOP treatment regimen.12,20–25 In a study of 102 DLBCL patients, the CR rate was significantly higher in patients missing TP53mut.25 The prognostic impact of TP53mut was further investigated in a study with 506 de novo DLBCL patients, and the results showed TP53mut was an independent predictor of OS and progression-free survival (PFS) in patients treated with an R-CHOP regimen.23 The prognostic impact of TP53mut was further confirmed in the RICOVER 60 trial, suggesting the use of TP53mut for prognostication and treatment stratification.24
In lymphomas other than DLBCL, TP53 mutation has been identified as an independent prognostic indicator of OS under current standard care in young patients with mantle-cell lymphoma.26 It has also been confirmed that TP53mut is correlated with low response rate to immunochemotherapy in chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL) patients,27,28 and ibrutinib is a preferred treatment approach for CLL/SLL patients with TP53 mutation.29,30 Despite reports about the prognostic impact of TP53 mutation in DLBCL patients, no clinical procedures are available to seek better patient outcomes.31 Here, we conducted an analysis of 44 TP53mut DLBCL patients treated with R-CHOP to identify clinical features and explore the potential benefit of different treatment approaches.
Methods
Patients and Samples
A series of 214 patients diagnosed with DLBCL according to the World Health Organization classification of tumors of hematopoietic and lymphoid tissue (2008)32 were enrolled retrospectively between January 2013 and December 2018 at the Cancer Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College, and Suzhou Municipal Hospital. Inclusion criteria were pathologically confirmed DLBCL, treatment with R-CHOP or R-CHOP–like regimen, validated for DNA extraction, HIV-negative. Driven by the purpose of identifying genetic high-risk subtypes, most patients in that series presented with advanced-stage and high-risk disease according to the revised international prognostic index (R-IPI; part of the study has been published).25 Retrospectively selected from that cohort, patients harboring TP53 mutations were enrolled in the present study. Clinical data were collected and analyzed: sex, age, Ann Arbor stage, Eastern Cooperative Oncology Group performance status, extranodal involvement, B symptoms, lactate dehydrogenase (LDH), bulky disease, R-IPI, first-line treatment, salvage treatment, response to treatment, and survival. GCB and non-GCB were determined by immunohistochemistry (IHC) using anti-CD10, MUM1, and BCL6 antibodies (Fuzhou Maixin Biotech). IHC staining for p53 expression was performed using MX008 mAb (MXB Biotechnologies). Response was assessed according to International Working Group criteria. The study was approved by the Institutional Review Board of National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences, and Peking Union Medical College (NCC2018JJJ-004), and was performed in accordance with the ethical standards of the institutional committee and the Declaration of Helsinki.
Genomic DNA Extraction and TP53 Sequencing
Formalin-fixed, paraffin-embedded (FFPE) tissue samples were collected from the enrolled patients. Genomic DNA was extracted using the QIAamp DNA FFPE tissue kit (Qiagen). DNA concentrations were measured using Qubit dsDNA assay (Life Technologies). We then performed DNA fragmentation with an M220 focused ultrasonicator (Covaris, Woburn, MA, USA), followed by end repair, phosphorylation, and adaptor ligation. Fragments of 200–400 bp were selected by AMPure beads (Agencourt AMPure XP kit; Beckman Coulter, Brea, CA, USA). Subsequently, hybridization with capture-probe baits, hybrid selection with magnetic beads, and PCR amplification were performed. Two capture probes were chosen: one with 413 genes frequently mutated in DLBCL patients, and the other consisting of 112 genes common to lymphoma and hematologic malignancies. There were in total 100 genes overlapping between these two panels, and TP53 was one of them. A high-sensitivity DNA assay was implemented in order to ensure sufficient DNA yield. Indexed samples were sequenced using a NextSeq 500 sequencer (Illumina, Hayward, CA, USA) with pair-end reads.
After removal of terminal adaptor sequences and low-quality data, reads were mapped to the reference human genome (hg19) and aligned using a Burrows–Wheeler 0.7.10 (Broad Institute). Local alignment optimization, variant calling, and annotation were performed using GATK 3.2 and MuTect (both from Broad Institute, Cambridge, MA, USA) and VarScan (Genome Institute, Washington University, USA). Loci with a depth <100 were filtered out by the VarScan filter pipeline. At least five supporting reads were required for insertions/deletions, and eight for single-number variations in tissue samples. The average sequencing depth for all targeted regions was 1,402×. Selected exons of TP53 in two panels were analyzed. In accordance with the Exome Aggregation Consortium, 1000 Genomes Project, ESP6500SI-V2, and dbSNP databases, variants with frequency >0.1% were categorized as single-nucleotide polymorphisms and excluded from further analysis. The remaining variants were annotated with ANNOVAR and SnpEff v3.6 software. TopHat2 (Center for Computational Biology, Johns Hopkins University and Genome Sciences Department, University of Washington, USA) and Factera 1.4.3 were utilized for DNA translocation analysis.
Statistical Analysis
PFS in this study was defined as time from therapy start to documented disease progression, relapse, or death. OS referred to the interval between the date of initial treatment and date of death or last follow-up. Patients who failed to achieve CR to initial treatment or relapsed in the first 6 months after initial CR were deemed to have primary refractory disease. Fisher’s exact and χ2 tests were conducted to assess associations between TP53 and clinical characteristics. OS and PFS were calculated using the Kaplan–Meier method, and log-rank tests were used to compare time-to-event curves between groups. Prognostic indicators were evaluated by Cox proportional-hazard regression. P<0.05 was set as the threshold for significance. All these analyses were conducted with R version 3.0.2 (http://www.R-project.org) and SPSS 22.0.
Results
TP53 Variants and p53 Expression
TP53 mutations were found in tumor samples from 47 of 214 (22%) patients. All detected genomic mutations are listed in Supplemental Table S1. In total, 54 mutations were found in TP53mut patients, of which 41 (87.2%) had a single TP53 mutation, five (10.6%) presented two mutations, and one had three mutations. Alterations were most commonly observed in exon 5 (n=20, 42.6%), followed by exon 6 (n=11, 23.4%), exon 7 (n=11, 23.4%), and exon 8 (n=6, 12.8%). Overall, 41 (87.2%) patients had mutations located in the DNA-binding domain (DBD) of TP53. We were only able to perform IHC staining of p53 in 18 patients with available tissue samples. Based on the cutoff rate of 10%, 16 were determined positive. Twelve patients with p53 overexpression were identified by a cutoff of 50%. For case 11 and case 45, both were negative with p53 and detected with R196 stop gained and A248 frameshift.
Clinical and Pathological Characteristics in TP53-Mutated DLBCL
Among 44 patients harboring TP53 alterations who underwent upfront R-CHOP or R-CHOP–like treatment, 21 (47.7%) were men and 23 (52.3%) women. Median age at diagnosis was 56 (range 18–82) years, and 28 (63.6%) were aged <60 years. Determined by Hans algorithm, 27.3% (12 of 44) were categorized as GCB and 68.2% (30 of 44) non-GCB. Subtype classification for two patients was missing, due to insufficient tissue samples. Among TP53mut patients, 21 (47.7%) had limited stage and 23 (52.3%) advanced stage. Overall, 30 patients had extranodal involvement and four had extranodal involvement of two or more. The other 14 patients had nodular involvement only. IHC-based coexpression of Myc and BCL2 was positive in ten (26.3%) of 38 patients with cutoff values of ≥40% and ≥50%, respectively. Based on the R-IPI, eight (19%), 21 (50%), and 13 (31%) patients were classified as very good, good, and poor, respectively. Clinical features of TP53mut DLBCL patients are detailed in Table 1.
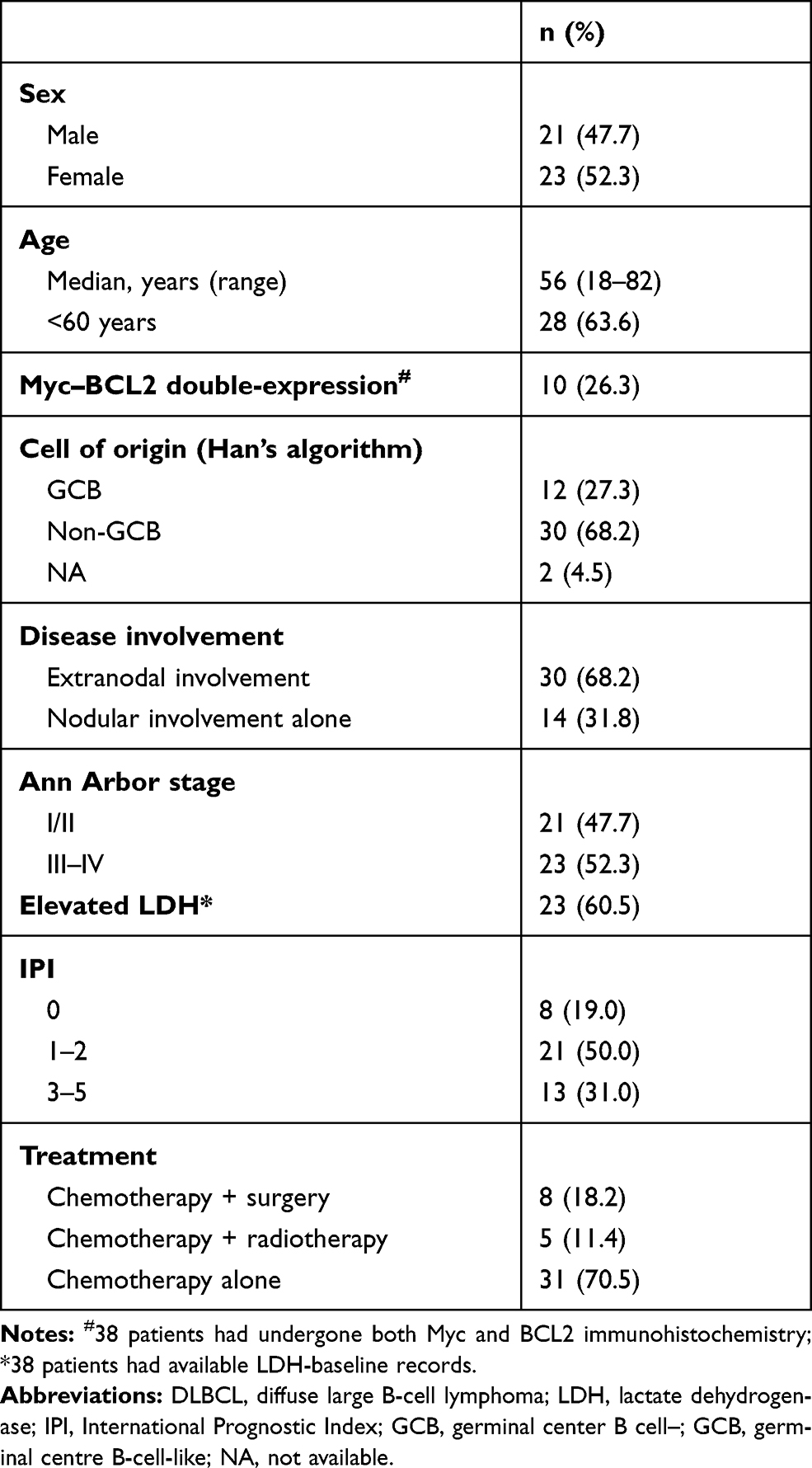 |
Table 1 Clinical Features of 44 Patients with TP53-mutated DLBCL |
Treatment Response and Survival Analysis of TP53-Mutated DLBCL Patients
For patients with limited-stage disease (n=21), 13 (61.9%) received locoregional treatment (five [22.7%] radiotherapy and eight [36.4%] surgical resection) in a front-line setting. Seven (33.3%) patients (four primary intestinal DLBCL, two primary Waldeyer’s ring DLBCL, and one primary testicular DLBCL) had complete resection before receiving immunochemotherapy. One patient with primary intestinal DLBCL had residual disease resection after six cycles of R-CHOP (Figure 1). All patients with complete resection stayed event-free till the last follow-up date, with a median follow-up of 37 months.
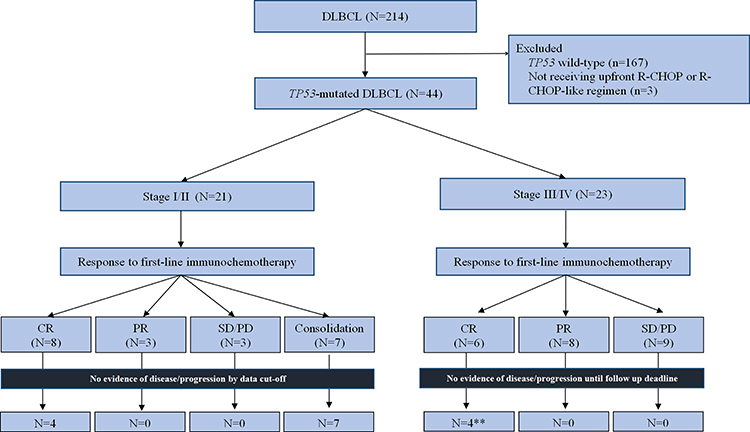 |
Figure 1 Patient disposition and response to frontline treatment and survival status in 44 DLBCL patients with TP53 mutation. |
Apart from the seven patients that received upfront surgical resection, 37 had measurable disease on R-CHOP, with 25 (67.6%) responsive to initial R-CHOP treatment (14 [37.8%] CR, 11 [29.7%] partial response). A total of 12 (32.4%) patients developed refraction to R-CHOP treatment (Figure 1). Among the 44 patients treated with R-CHOP, 59.1% (n=26) developed primary refraction, with 22 (50.0%) failing to achieve CR to initial treatment and four (9.1%) relapsing in the first 6 months after initial CR. Noticeably, among these primary refractory patients, a 51-year old woman had a most aggressive disease course and succumbed to disease progression in the second month following diagnosis. It is worth mentioning that she had a concurrent CDKN2A frameshift in addition to the TP53 mutation.
With median follow-up of 15.5 months, median PFS and OS were 9 (95% CI 4.9–13.1) months and 46 (95% CI 11.2–80.8) months in the 44 R-CHOP–treated patients harboring TP53 mutations (Figure 2A and B). On univariate analysis, LDH (elevated vs normal, 6.5 vs not reached [NR] months p=0.001), disease stage (limited vs advanced, NR vs 6.2 months; p=0.005) and extranodal involvement (0-1 vs ≥2, 12.5 vs 6.0 months; p=0.017) were correlated with PFS. However, no survival difference was observed between different TP53 subtypes (DBD vs non-DBD, 8 months vs NA; p=0.389) and no factor was identified to be significantly correlated with OS.
 |
Figure 2 (A) Progression-free survival and (B) overall survival of TP53-mutated DLBCL treated with R-CHOP regimen. Locoregional treatment was associated with (C) progression-free survival and (D) overall survival. |
Locoregional Treatment in Limited-Stage Patients
We further analyzed the impact of locoregional treatment in the limited-stage subset (n=21), and found locoregional treatment was correlated with PFS (yes vs no, NR vs 6 months; p<0.001) and OS (yes vs no, NR vs 18 months; p=0.008). After adjustment for baseline LDH and extranodal involvement, adding locoregional treatment to immunochemotherpy was associated with longer PFS (HR 0.092, 95% CI 0.016–0.543; p=0.008) and OS (HR 0.032, 95% CI 0.002–0.535; p=0.017).
Discussion
We analyzed clinical features of TP53mut DLBCL patients and found a high occurrence of primary refraction. Although surgical resection is not recommended as the standard of care for DLBCL patients, this study demonstrates an improved outcome for TP53mut patients with locoregional intervention involving surgery and radiotherapy. We were able to identify 22% of DLBCL patients harboring TP53 mutations, similar to previous studies.11,12,33 Additionally, 89% of TP53 mutations were located in exons 5–8 in DBD and showed no statistically significant difference for DBD versus non-DBD mutations in relationship to poor prognosis, as previously reported.23, 34,35 Both TP53 mutation and accumulation of wild-type p53 led to readings of IHC-determined overexpression. A cutoff >50% was used for stratification of DLBCL patients.23 Among 18 TP53mut patients in our study, 16 had p53 overexpression and 12 were over the cutoff of 50%. Two TP53mut patients were p53 IHC-negative, which may relate to the spot of mutation (one frameshift and one stop gain). They both progressed in the first month of R-CHOP treatment.
TP53 mutation was associated with unfavorable response to standard treatment and resulted in short survival for many solid tumors and hematologic malignancies.36–38 Abundant evidence shows the function of TP53 mutations is varied depending on the cell type, differentiation state, stress conditions, and tissue microenvironment.39 In this study, 59.1% (n=26) of TP53mut DLBCL patients developed primary refractory disease, much higher than general population,40–42 indicating TP53 mutations correlated with unfavorable response to R-CHOP. Promoting cell-cycle arrest and apoptosis are two major functions of p53, while the absence of p53 can promote accumulation and permit survival of aneuploid cells. In CLL, evidence suggests TP53 mutations are associated with resistance to alkylator- and nucleoside-analogue treatment, resulting in a chemotherapy-resistant phenotype. Actually, in TP53mut CLL, the poor response to conventional chemotherapy has facilitated the development of targeted therapies, such as ibrutinib, optimizing clinical practice for this population.
Efforts in exploring optimal treatment have also been made in TP53mut DLBCL. Of the TP53mut DLBCL patients in the RICOVER-60 trial, eight cycles of CHOP or R-CHOP failed to improve patient outcome over six cycles.24 The present study focused on the impact of locoregional treatment, including radiotherapy and surgical intervention, in patients with limited-stage DLBCL. Although surgical resection is not recommended as a routine approach in DLBCL treatment, benefits of surgical resection have been reported in primary gastrointestinal DLBCL.43 Here, we are the first to report the impact of locoregional treatment in patients with TP53mut DLBCL, a molecular subgroup carrying unfavorable prognosis. We identified the possible clinical benefit of adding a locoregional procedure in limited-stage TP53mut DLBCL patients, and propose that a combination of systemic and locoregional measures could contribute to overcoming the chemotherapy-resistant phenotype of TP53mut DLBCL.
This study’s retrospective nature, limited sample size, and lack of incorporation of other prognostic indicators44–47 may have introduced bias, and thus the results should be interpreted with caution. Nevertheless, considering the curability of DLBCL, the frequency of TP53 mutations in DLBCL, and the proportion of primary refraction, we believe our findings could provide some hints for optimizing treatment for TP53mut DLBCL. Further studies are warranted to prospectively explore individualized treatment for this population with poor prognosis. In summary, we conclude that primary refractory disease is common in DLBCL patients with TP53 mutations receiving R-CHOP treatment. A combination of locoregional treatment and R-CHOP chemotherapy could provide additional clinical benefit to limited-stage DLBCL patients with TP53 mutations.
Code Availability
Not available.
Abbreviations
DLBCL, diffuse large B-cell lymphoma; CR, complete response; R-CHOP, rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone; PFS, progression-free survival; OS, overall survival; CLL, chronic lymphocytic leukemia; NHL, non-Hodgkin’s lymphoma; GCB, germinal centre Bcell; LDH, lactate dehydrogenase; R-IPI, revised International Prognostic Index; IHC, immunohistochemistry; FFPE, formalin-fixed, paraffin-embedded; DBD, DNA-binding domain.
Data-Sharing Statement
The data set used and/or analyzed during the current study is available from the corresponding author on reasonable request.
Ethical Approval
All patients provided written informed consent. The protocol was approved by the institutional review boards of the National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College (NCC2018JJJ-004).
Consent to Participate
Consent to publish has been obtained from the participants to report individual patient data.
Acknowledgments
We thank all the patients and their families who were involved in this study, the clinical study and Weirui Chai, PhD, MS Law for providing writing and editorial assistance for the manuscript.
Funding
This study was supported by the National Key Technology Support Program (2014BAI09B12), Chinese Academy of Medical Sciences (CAMS) Innovation Fund for Medical Sciences (CIFMS) (2016-I2M-1-001), and Beijing–Tianjin–Hebei Cooperation Program for basic research (H2018206591).
Disclosure
XHD and YTY are employees of Geneplus Beijing. JL is an employee of Burning Rock Biotech. The aforementioned authors report no other potential conflicts of interest in this work. All other authors declare no conflicts of interest.
References
1. Coiffier B, Thieblemont C, Van Den Neste E, et al. Long-term outcome of patients in the LNH-98.5 trial, the first randomized study comparing rituximab-CHOP to standard CHOP chemotherapy in DLBCL patients: a study by the Groupe d’Etudes des Lymphomes de l’Adulte. Blood. 2010;116(12):2040–2045. doi:10.1182/blood-2010-03-276246
2. Friedberg JW. Relapsed/refractory diffuse large B-cell lymphoma. Hematology Am Soc Hematol Educ Program. 2011;2011:498–505. doi:10.1182/asheducation-2011.1.498
3. Pfreundschuh M, Kuhnt E, Trumper L, et al. CHOP-like chemotherapy with or without rituximab in young patients with good-prognosis diffuse large-B-cell lymphoma: 6-year results of an open-label randomised study of the MabThera International Trial (MInT) Group. Lancet Oncol. 2011;12(11):1013–1022. doi:10.1016/S1470-2045(11)70235-2
4. Gisselbrecht C, Glass B, Mounier N, et al. Salvage regimens with autologous transplantation for relapsed large B-cell lymphoma in the rituximab era. J Clin Oncol. 2010;28(27):4184–4190.
5. Cheson BD, Bartlett NL, Vose JM, et al. A Phase II study of the survivin suppressant YM155 in patients with refractory diffuse large B-cell lymphoma. Cancer. 2012;118(12):3128–3134. doi:10.1002/cncr.26510
6. Jerkeman M, Leppa S, Kvaloy S, Holte H. ICE (ifosfamide, carboplatin, etoposide) as second-line chemotherapy in relapsed or primary progressive aggressive lymphoma–the Nordic Lymphoma Group experience. Eur J Haematol. 2004;73(3):179–182. doi:10.1111/j.1600-0609.2004.00294.x
7. Kahl BS, Bailey HH, Smith EP, et al. Phase II study of weekly low-dose paclitaxel for relapsed and refractory non-Hodgkin’s lymphoma: a Wisconsin Oncology Network Study. Cancer Invest. 2005;23(1):13–18. doi:10.1081/CNV-46484
8. Hitz F, Connors JM, Gascoyne RD, et al. Outcome of patients with primary refractory diffuse large B cell lymphoma after R-CHOP treatment. Ann Hematol. 2015;94(11):1839–1843. doi:10.1007/s00277-015-2467-z
9. Sarkozy C, Coiffier B. Primary refractory diffuse large B cell lymphoma in the rituximab era. Curr Opin Oncol. 2015;27(5):377–383. doi:10.1097/CCO.0000000000000209
10. Vardhana SA, Sauter CS, Matasar MJ, et al. Outcomes of primary refractory diffuse large B-cell lymphoma (DLBCL) treated with salvage chemotherapy and intention to transplant in the rituximab era. Br J Haematol. 2017;176(4):591–599. doi:10.1111/bjh.14453
11. Lohr JG, Stojanov P, Lawrence MS, et al. Discovery and prioritization of somatic mutations in diffuse large B-cell lymphoma (DLBCL) by whole-exome sequencing. Proc Natl Acad Sci U S A. 2012;109(10):3879–3884. doi:10.1073/pnas.1121343109
12. Xu-Monette ZY, Medeiros LJ, Li Y, et al. Dysfunction of the TP53 tumor suppressor gene in lymphoid malignancies. Blood. 2012;119(16):3668–3683. doi:10.1182/blood-2011-11-366062
13. Chapuy B, Stewart C, Dunford AJ, et al. Molecular subtypes of diffuse large B cell lymphoma are associated with distinct pathogenic mechanisms and outcomes. Nat Med. 2018;24(5):679–690. doi:10.1038/s41591-018-0016-8
14. Schmitz R, Wright GW, Huang DW, et al. Genetics and pathogenesis of diffuse large B-cell lymphoma. N Engl J Med. 2018;378(15):1396–1407. doi:10.1056/NEJMoa1801445
15. Ganly I, Soutar DS, Brown R, Kaye SB. p53 alterations in recurrent squamous cell cancer of the head and neck refractory to radiotherapy. Br J Cancer. 2000;82(2):392–398. doi:10.1054/bjoc.1999.0932
16. Kelsey KT, Hirao T, Schned A, et al. A population-based study of immunohistochemical detection of p53 alteration in bladder cancer. Br J Cancer. 2004;90(8):1572–1576. doi:10.1038/sj.bjc.6601748
17. Feldser DM, Kostova KK, Winslow MM, et al. Stage-specific sensitivity to p53 restoration during lung cancer progression. Nature. 2010;468(7323):572–575. doi:10.1038/nature09535
18. Scata KA, El-Deiry WS. p53, BRCA1 and breast Cancer chemoresistance. Adv Exp Med Biol. 2007;608:70–86.
19. Nishikura K, Watanabe H, Iwafuchi M, Fujiwara T, Kojima K, Ajioka Y. Carcinogenesis of gastric endocrine cell carcinoma: analysis of histopathology and p53 gene alteration. Gastric Cancer. 2003;6(4):203–209. doi:10.1007/s10120-003-0249-0
20. Pasqualucci L, Trifonov V, Fabbri G, et al. Analysis of the coding genome of diffuse large B-cell lymphoma. Nat Genet. 2011;43(9):830–837. doi:10.1038/ng.892
21. Ichikawa A, Hotta T, Takagi N, et al. Mutations of p53 gene and their relation to disease progression in B-cell lymphoma. Blood. 1992;79(10):2701–2707. doi:10.1182/blood.V79.10.2701.bloodjournal79102701
22. Ichikawa A, Kinoshita T, Watanabe T, et al. Mutations of the p53 gene as a prognostic factor in aggressive B-cell lymphoma. N Engl J Med. 1997;337(8):529–534. doi:10.1056/NEJM199708213370804
23. Xu-Monette ZY, Wu L, Visco C, et al. Mutational profile and prognostic significance of TP53 in diffuse large B-cell lymphoma patients treated with R-CHOP: report from an International DLBCL Rituximab-CHOP Consortium Program Study. Blood. 2012;120(19):3986–3996. doi:10.1182/blood-2012-05-433334
24. Zenz T, Kreuz M, Fuge M, et al. TP53 mutation and survival in aggressive B cell lymphoma. Int J Cancer. 2017;141(7):1381–1388. doi:10.1002/ijc.30838
25. Jiang S, Qin Y, Jiang H, et al. Molecular profiling of Chinese R-CHOP treated DLBCL patients: identifying a high-risk subgroup. Int J Cancer. 2020;147(9):2611–2620. doi:10.1002/ijc.33049
26. Eskelund CW, Dahl C, Hansen JW, et al. TP53 mutations identify younger mantle cell lymphoma patients who do not benefit from intensive chemoimmunotherapy. Blood. 2017;130(17):1903–1910. doi:10.1182/blood-2017-04-779736
27. Rossi D, Cerri M, Deambrogi C, et al. The prognostic value of TP53 mutations in chronic lymphocytic leukemia is independent of Del17p13: implications for overall survival and chemorefractoriness. Clin Cancer Res. 2009;15(3):995–1004. doi:10.1158/1078-0432.CCR-08-1630
28. Zenz T, Eichhorst B, Busch R, et al. TP53 mutation and survival in chronic lymphocytic leukemia. J Clin Oncol. 2010;28(29):4473–4479. doi:10.1200/JCO.2009.27.8762
29. Farooqui MZ, Valdez J, Martyr S, et al. Ibrutinib for previously untreated and relapsed or refractory chronic lymphocytic leukaemia with TP53 aberrations: a Phase 2, single-arm trial. Lancet Oncol. 2015;16(2):169–176. doi:10.1016/S1470-2045(14)71182-9
30. Ahn IE, Farooqui MZH, Tian X, et al. Depth and durability of response to ibrutinib in CLL: 5-year follow-up of a phase 2 study. Blood. 2018;131(21):2357–2366. doi:10.1182/blood-2017-12-820910
31. Hainaut P, Pfeifer GP. Somatic TP53 mutations in the era of genome sequencing. Cold Spring Harb Perspect Med. 2016;6(11):a026179. doi:10.1101/cshperspect.a026179
32. Sabattini E, Bacci F, Sagramoso C, Pileri SA. WHO classification of tumours of haematopoietic and lymphoid tissues in 2008: an overview. Pathologica. 2010;102(3):83–87.
33. Voropaeva EN, Pospelova TI, Voevoda MI, Maksimov VN, Orlov YL, Seregina OB. Clinical aspects of TP53 gene inactivation in diffuse large B-cell lymphoma. BMC Med Genomics. 2019;12(Suppl S2):35. doi:10.1186/s12920-019-0484-9
34. Karube K, Enjuanes A, Dlouhy I, et al. Integrating genomic alterations in diffuse large B-cell lymphoma identifies new relevant pathways and potential therapeutic targets. Leukemia. 2018;32(3):675–684. doi:10.1038/leu.2017.251
35. Young KH, Weisenburger DD, Dave BJ, et al. Mutations in the DNA-binding codons of TP53, which are associated with decreased expression of TRAILreceptor-2, predict for poor survival in diffuse large B-cell lymphoma. Blood. 2007;110(13):4396–4405. doi:10.1182/blood-2007-02-072082
36. Tahara T, Shibata T, Okamoto Y, et al. Mutation spectrum of TP53 gene predicts clinicopathological features and survival of gastric cancer. Oncotarget. 2016;7(27):42252–42260. doi:10.18632/oncotarget.9770
37. Ungerleider NA, Rao SG, Shahbandi A, et al. Breast cancer survival predicted by TP53 mutation status differs markedly depending on treatment. Breast Cancer Res. 2018;20(1):115. doi:10.1186/s13058-018-1044-5
38. Nelson HH, Wilkojmen M, Marsit CJ, Kelsey KT. TP53 mutation, allelism and survival in non-small cell lung cancer. Carcinogenesis. 2005;26(10):1770–1773. doi:10.1093/carcin/bgi125
39. Kastenhuber ER, Lowe SW. Putting p53 in Context. Cell. 2017;170(6):1062–1078. doi:10.1016/j.cell.2017.08.028
40. Pfreundschuh M, Trumper L, Osterborg A, et al. CHOP-like chemotherapy plus rituximab versus CHOP-like chemotherapy alone in young patients with good-prognosis diffuse large-B-cell lymphoma: a randomised controlled trial by the MabThera International Trial (MInT) Group. Lancet Oncol. 2006;7(5):379–391. doi:10.1016/S1470-2045(06)70664-7
41. Pfreundschuh M, Schubert J, Ziepert M, et al. Six versus eight cycles of bi-weekly CHOP-14 with or without rituximab in elderly patients with aggressive CD20+ B-cell lymphomas: a randomised controlled trial (RICOVER-60). Lancet Oncol. 2008;9(2):105–116. doi:10.1016/S1470-2045(08)70002-0
42. Cunningham D, Hawkes EA, Jack A, et al. Rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisolone in patients with newly diagnosed diffuse large B-cell non-Hodgkin lymphoma: a Phase 3 comparison of dose intensification with 14-day versus 21-day cycles. Lancet. 2013;381(9880):1817–1826. doi:10.1016/S0140-6736(13)60313-X
43. Kim SJ, Kang HJ, Kim JS, et al. Comparison of treatment strategies for patients with intestinal diffuse large B-cell lymphoma: surgical resection followed by chemotherapy versus chemotherapy alone. Blood. 2011;117(6):1958–1965. doi:10.1182/blood-2010-06-288480
44. Găman M-A, Papoi A, Găman A. Pathophysiological mechanisms involved in the development of anemia in patients with non-Hodgkin’s lymphoma. Haematologica. 2017;102:845.
45. Ennishi D, Mottok A, Ben-Neriah S, et al. Genetic profiling of MYC and BCL2 in diffuse large B-cell lymphoma determines cell-of-origin-specific clinical impact. Blood. 2017;129(20):2760–2770. doi:10.1182/blood-2016-11-747022
46. Abdulla M, Hollander P, Pandzic T, et al. Cell-of-origin determined by both gene expression profiling and immunohistochemistry is the strongest predictor of survival in patients with diffuse large B-cell lymphoma. Am J Hematol. 2020;95(1):57–67. doi:10.1002/ajh.25666
47. Gaman MA, Epingeac ME, Gaman AM. The evaluation of oxidative stress and high-density lipoprotein cholesterol levels in diffuse large B-cell lymphoma. Rev Chim. 2019;70(3):977–980. doi:10.37358/RC.19.3.7043
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.