Back to Journals » Orthopedic Research and Reviews » Volume 17
Changing Utilization of Primary Anatomic and Reverse Shoulder Arthroplasty in a Single High-Volume Institution: A Retrospective Cohort Study
Authors Wu SJ, Hernandez KL, Armond DN, McCulloch PC ![]()
Received 8 February 2025
Accepted for publication 2 July 2025
Published 3 September 2025 Volume 2025:17 Pages 421—426
DOI https://doi.org/10.2147/ORR.S515073
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Samuel J Wu, Karen L Hernandez, David N Armond, Patrick C McCulloch
Department of Orthopedics and Sports Medicine, Houston Methodist Hospital, Houston, TX, USA
Correspondence: Patrick C McCulloch, Houston Methodist Hospital, Department of Orthopedics and Sports Medicine, 6445 Main Street, Suite 2500, Houston, TX, 77030, USA, Email [email protected]
Objective: The incidence of total shoulder arthroplasty (TSA) in the United States continues to climb as an aging yet active population increases demand for the procedure. Due to promising clinical results out of Europe, improvement in prosthesis design, and wider acceptance of reverse total shoulder arthroplasty (rTSA), this study was designed to evaluate how rTSA and anatomical TSA (aTSA) utilization, patient selection, and length of stay have changed at a single institution.
Methods: This was a retrospective cohort study of patients from one hospital system between 2017 and 2023. Inclusion criteria included primary TSA cases using CPT codes. Exclusion criteria included hemiarthroplasty, revision arthroplasty, non-arthroplasty procedures. Primary arthroplasty procedures were separated into reverse or anatomic cohorts for analysis. Independent sample t-tests were used to compare continuous data between the first and last year of cohort data and to compare parameters between procedure types. Chi-square analysis was used for frequency-based data comparisons. Type-I error was set at α=0.05 for all analyses.
Results: From all 2774 shoulder arthroplasty cases identified, 2604 TSA cases were included in the final statistical analyses, 2114 of which were rTSA and 490 anatomic TSA. Comparison of arthroplasties in 2017 and 2023 revealed, rTSA increased from 115 surgery cases to 549, or 77.18% to 82.81% over the study period (p < 0.001). Anatomic TSA increased in total surgery cases from 29 to 111, (p = 0.655) and thus signifies an overall decrease in anatomic surgery utilization from 19.46% to 16.74%. Data showed an increase in average patient age for rTSA and decreased procedure time and length of stay for both groups.
Conclusion: rTSA utilization has surpassed and continues to increase relative to anatomic TSA. Peri-operative management of shoulder replacement has become more efficient with significantly decreased procedure time and decreased total hospital length of stay after primary TSA.
Keywords: total shoulder arthroplasty, reverse TSA, anatomic TSA, utilization of total shoulder arthroplasty
Introduction
The incidence of shoulder arthroplasty in the United States continues to climb as an aging yet active population increases demand for the procedure. As prior studies have noted, due to promising clinical results out of Europe, improvement in prosthesis design and wider acceptance of the procedure, the usage of total shoulder arthroplasty saw a significant increase in 2004, coinciding with the FDA approval of the reverse total shoulder arthroplasty (rTSA).1 While approved for use in the treatment of elderly, low-demand rotator cuff arthropathy, off-label indications of rTSA have expanded to include primary osteoarthritis, revision shoulder arthroplasty, proximal humerus fracture, proximal humerus tumor, fixed glenohumeral dislocation and irreparable rotator cuff tears.2
Many factors have contributed to the increased popularity of rTSA. Modern rTSA designs have continued to improve with less scapular notching and decreased rates of neurologic injury. Increased exposure during training and broader acceptance of the procedure have led to improvements in technique with prior studies reporting a learning curve of 25 cases leading to decreased operative time, improved patient reported outcome and fewer complications.3 The profile of complications has also changed; prosthetic joint infections having overtaken instability as the most common complication, suggesting improvements in surgical technique.4
In prior utilization studies drawing from the Nationwide Inpatient Sample, the reverse total shoulder arthroplasty had accounted for up to 32.6% of all arthroplasties performed in 2011 and only appears to be gaining more traction.5 The most common indications for rTSA reported were osteoarthritis, rotator cuff tear and proximal humerus fracture. The average rTSA patient was likely to be older than 75 years, female and with more medical comorbidities compared with anatomic TSA (aTSA) or hemiarthroplasty. In-hospital complications including acute respiratory distress, post-hemorrhagic anemia, post-operative hypotension and pulmonary embolism were also more commonly reported in rTSA. In a 10-year period (2005–2015) evaluating rTSA utilization at a single institution, Chalmers et al reported decreased surgical time and in-hospital stay as a correlate to clinical improvement. They also noted that rTSA became the more commonly performed TSA at the end of their observation period and projected the gap would further widen between reverse and anatomic total shoulder arthroplasty.6
The purpose of this study was to evaluate how utilization of primary anatomic and reverse total shoulder arthroplasty have changed and to describe the indications, patient selection, and complication profile system-wide between 2017 and 2023. We hypothesize that rTSA utilization will compose an increased proportion of all shoulder arthroplasty cases performed and be performed in an older patient cohort as well as decreased complication rate.
Methods
This was a retrospective cohort study of total shoulder arthroplasty patients at a single institution. Internal Institutional Review Board (IRB) approval was required and received prior to study start. The study adhered to the principles of the Declaration of Helsinki. A request for a waiver of consent was granted, as the research was minimal risk and could not practicably be carried out without using such a method. Data confidentiality was maintained with password protection and file encryption. Inclusion criteria include primary aTSA and rTSA performed in the Houston Methodist Hospital System between 2017 and 2023. This cohort was identified with proprietary software by the health data science and analytics team using CPT codes for shoulder arthroplasty as a filter. Exclusion criteria were hemiarthroplasty, revision arthroplasty, non-arthroplasty procedures. Non-arthroplasty procedures performed at the same time as primary arthroplasty were included. Of note, system-wide data prior to 2016 was not available due to the EMR merge at our institution. Data from years 2016 and 2024 were excluded due to incomplete per annum data. Notably, there is no separate CPT code for primary anatomic versus primary reverse total shoulder arthroplasty. The extracted charts were then individually verified by an orthopedic surgeon in fellowship training to determine whether primary aTSA or rTSA procedure was performed through pre-operative medical records operative report and immediate post-surgical radiographs. Primary arthroplasty patients were separated into reverse and anatomic cohorts for analysis. Demographic data including age, sex, BMI, ASA score, length of procedure and hospital stay were compared between 2017 and 2023.
Independent sample t-tests were used to compare continuous data between first and last year of cohort data. The same test was used to compare parameters between procedure types. Next, Chi-square analysis was used for frequency-based data comparisons. Type-I error was set at α=0.05 for all analyses.
Results
A total of 2774 primary arthroplasty cases were identified, 170 patients were excluded based off inclusion and exclusion criteria. 2604 primary shoulder arthroplasties were included in the final statistical analyses, 2114 of which were reverse TSA and 490 anatomic TSA (Figure 1).
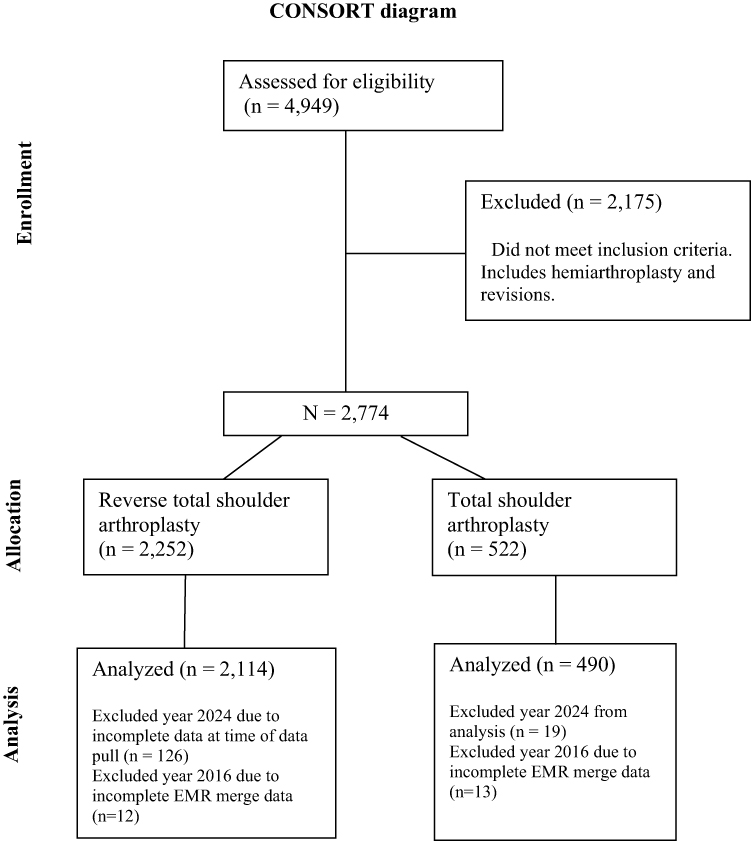 |
Figure 1 Consort diagram. Abbreviation: EMR, Electronic Medical Records. |
Both anatomic and reverse total shoulder utilization increased during the study period (Figure 2). Primary TSA utilization, both aTSA and rTSA, increased from 144 total cases to 660, or a 4.58 fold increased from 2017 to 2023. From the start of the study date (2017), rTSA had already overtaken aTSA as the more commonly performed primary shoulder arthroplasty procedure. This trend continued to increase year over year as hypothesized. As a proportion of all primary TSA performed, primary reverse TSA significantly increased from 77.18% to 82.81% (P < 0.001) over the study period, whereas primary anatomic TSA decreased from 19.46% to 16.74% (Table 1).
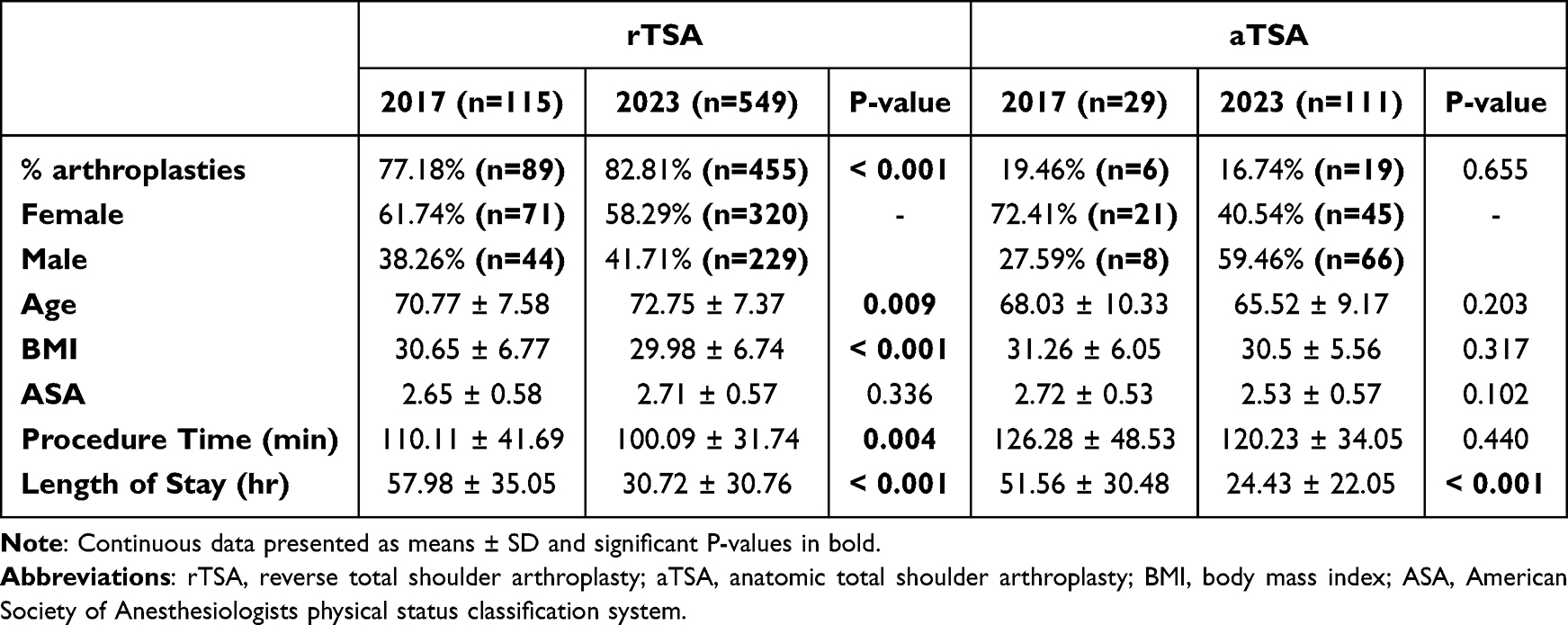 |
Table 1 Demographic Data from 2017 and 2023 |
 |
Figure 2 Incidence of rTSA (black triangles) and anatomic TSA (grey dots) by year as shown by proportion and frequency annually from 2017 to 2023. |
The average age of patients indicated for reverse TSA significantly increased from 70.77 to 72.75 years (P = 0.009). While anatomic TSA age showed a non-significant decreased from 68.03 to 65.52 years (P = 0.203). Other demographic data showed a significant decrease in procedure time for reverse TSA (110.11min to 100.09min, P = 0.004), while anatomic TSA procedure time did not have significant changes. Length of stay significantly decreased in both groups, 57.98 to 30.72 hours in reverse TSA (P < 0.001), and 51.56 to 24.43 hours in anatomic TSA (P < 0.001) (Table 1).
Discussion
Demand for shoulder arthroplasty continues to increase. This is in part due to the growing role for reverse total shoulder arthroplasty for a multitude of shoulder pathologies, now with significant overlap between indications. In patients with glenohumeral arthritis without evidence of cuff tear, reverse total shoulder has become a preferred alternative procedure to the anatomic total shoulder. Prior studies have shown similar clinical and radiographic outcomes between the two procedures with a significantly higher rate of complications in the aTSA group compared with rTSA.7 Our results show an increased utilization of primary total shoulder arthroplasty over the 7-year period with over 4 in 5 new shoulder replacements in the last year being rTSA. These results are in agreeance with previously published studies.5,6 With the increasing number of reverse and total shoulder replacements overall and expanding indications for shoulder replacement, we might expect to see more complications and revision procedures as it is used in more complex clinical scenarios.
One of the advantages of rTSA over anatomic or hemiarthroplasty is less reliance on an intact rotator cuff to flex and abduct the arm, as in cases of rotator cuff tear arthropathy. Expanding indications for reverse now include complex 3- or 4-part proximal humerus fractures due to less reliance on tuberosity healing and has proven to be an excellent treatment option in both primary and revision fracture settings.8 As such, many surgeons are possibly using the reverse total shoulder rather than anatomic shoulder replacements to obtain more reliable clinical outcomes for patients.
Advantages may also be present in the design of the rTSA prosthesis which has undergone improvements from its inception. The second-generation prosthesis includes a hemispherical glenoid component and increased inclination of the humeral neck shaft. While improved, scapular notching remained a concern for implant failure.9 Modern rTSA designs have continued to increase the inclination of the shaft and decrease scapular notching and improve bony impingement.10 Biomechanically, rTSA alters the center of shoulder rotation to allow the deltoid to work in a modified form, creating tension and a longer lever for mechanical advantage in abduction. Together the improvements in prosthesis design have generated desirable effects that might contribute to this emerging trend of utilization.
Over the 7-year period at our institution, patient profiles for anatomic total shoulder arthroplasty were younger, had fewer co-morbidities using ASA score as a measure of baseline health and male. We interpreted these results as surgeons using stricter indications for the anatomic shoulder replacement in younger, healthier males. Even more telling, by the time our institution had switched to EPIC EMR in 2017, the reverse shoulders had already supplanted anatomic shoulders as the more common primary total shoulder.
Shoulder arthroplasty continues to be a high-demand procedure. While utilization of reverse total shoulder has outpaced anatomic total shoulders, incidence of both procedures has increased annually at our institution. Primary total shoulder replacement at our institution saw a 4.58-fold or 358% increase system-wide over the last 7 years. With increased use and familiarity with shoulder replacement procedures, our study suggests more efficient patient care and improved surgical technique with statistically significant decrease in operative time and hospital length of stay. While most patients in our study were admitted overnight in the hospital, as we have seen in the total knee and hip replacement population, the drive towards outpatient procedure have driven subsequent efficiency and cost-saving measures. Other studies examining same-day total shoulder arthroplasty in the United Kingdom have shown no change in readmission rate or early functional differences, but with a significant cost benefit.11
Our study has notable limitations. The retrospective, chart review nature is subject to selection bias. All surgeons performing shoulder arthroplasty system-wide were included in this analysis with varying experience in practice. This presents possible confounders including exposure to reverse and anatomic shoulder replacements that may not capture surgeon indications but rather reflect familiarity with a procedure. Patients who underwent shoulder replacement in our study reflects a subset of patients indicated for and offered surgical treatment for shoulder pathology. Our study would not capture patients who qualified for a total shoulder but either elected to not have surgery or went outside of our system. There was no direct comparison of anatomic and reverse shoulder cohorts or randomization of patients into separate groups. However, this may not be feasible or ethically sound given expected outperformance of reverse shoulders compared with anatomic.
We did not include hemiarthroplasty procedures in our analysis as the surgical indications have less overlap with those of reverse total shoulders, although the number of hemiarthroplasties performed system-wide at our institution is already far out-numbered by the total shoulder procedures and unlikely to change our data to any significant degree. Lastly, this study did not measure outcomes or complications in anatomic or reverse shoulder arthroplasty cohorts. With increased utilization of primary total shoulder replacements, there will be an associated increase in complications and revisions. Further studies exploring long-term outcome data in these cohorts will be important to develop and refine practices in managing these shoulder pathologies.
Conclusion
Based on our findings, reverse total shoulder arthroplasty utilization has increased and surpassed anatomic total shoulder replacements. Peri-operative management of shoulder replacement has become more efficient with decreased procedure time of reverse TSA and total hospital length of stay after primary TSA procedures. While indications in this cohort of patients included tumor, irreparable cuff tears and fracture, further work is needed to examine how primary TSA utilization patterns have changed for these other complex shoulder problems and investigate long-term outcome data following use of shoulder replacement for these pathologies.
Disclosure
Dr Patrick McCulloch reports Consultancy from Arthrex, Inc., Stock Options from Orthobullets.com, outside the submitted work. The authors report no conflicts of interest in this work.
References
1. Kim SH, Wise BL, Zhang Y, Szabo RM. Increasing incidence of shoulder arthroplasty in the United States. J Bone Joint Surg Am. 2011;93L:2249–2254.
2. Kuhn JE, Weber SC, St Pierre P, et al. Off-label use of reverse total shoulder arthroplasty: the American academy of orthopedic surgeons shoulder and elbow registry. Semin Arthroplasty. 2023;33:261–269.
3. Avendano JP, Sudah SY, Gencarelli P, et al. The learning curve for anatomic and reverse total shoulder arthroplasty: a systematic review. JSES Rev Reports Techniques. 2023;3:150–159.
4. Kim SC, Kim IS, Jang MC, Yoo JC. Complications of reverse shoulder arthroplasty: a concise review. Clin Shoulder Elb. 2021;24:42–52.
5. Schairer WW, Nwachukwu BU, Lyman S, Craig EV, Gulotta LV. National utilization of reverse total shoulder arthroplasty in the United States. J Shoulder Elbow Surg. 2015;24:91–97.
6. Chalmers PN, Salazar DH, Romeo AA, Keener JD, Yamaguchi K, Chamberlain AM. Comparative utilization of reverse and anatomic total shoulder arthoplasty: a comprehensive analysis of a high-volume center. J Am Acad Orthop Surg. 2018;26:e504–e510.
7. Friedman RJ, Schoch BS, Eichinger JK, et al. Comparison of reverse and anatomic total shoulder arthroplasty in patients with an intact rotator cuff and no previous surgery. JAAOS. 2022;30(19):941–948.
8. Dezfuli B, King JJ, Farmer KW, Struk AM, Wright TW. Outcomes of reverse total shoulder arthroplasty as primary versus revision procedure for proximal humerus fractures. J Shoulder Elbow Surg. 2016;25(7):1133–1137. doi:10.1016/j.jse.2015.12.002
9. Grassi FA, Murena L, Valli F, Alberio R. Six-year experience with the Delta III reverse shoulder prosthesis. J Orthop Surg. 2009;17(2):151–156. PMID: 19721141. doi:10.1177/230949900901700205
10. Werner BS, Chaoui J, Walch G. The influence of humeral neck shaft angle and glenoid lateralization on range of motion in reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2017;26(10):1726–1731. PMID: 28528016. doi:10.1016/j.jse.2017.03.032
11. Borakati A, Ali A, Nagaraj C, Gadikoppula S, Kurer M. Day case vs inpatient total shoulder arthroplasty: a retrospective cohort study and cost-effectiveness analysis. World J Orthop. 2020;11(4):213–221.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.