Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Changing Perceptions of Rural Frontline Workers and Caregivers About Management of Childhood Diarrhea and Pneumonia Despite Several Inequities: The Nigraan Plus Trial in Pakistan
Authors Rabbani F, Khan HA, Piryani S ![]() , Pradhan NA
, Pradhan NA ![]() , Shaukat N, Feroz AS, Perveen S
, Shaukat N, Feroz AS, Perveen S ![]()
Received 20 August 2021
Accepted for publication 4 November 2021
Published 2 December 2021 Volume 2021:14 Pages 3343—3355
DOI https://doi.org/10.2147/JMDH.S334844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Fauziah Rabbani,1,2 Hyder Ali Khan,2 Suneel Piryani,2 Nousheen Akber Pradhan,2 Natasha Shaukat,2 Anam Shahil Feroz,2 Shagufta Perveen2
1Office of Research and Graduate Studies, The Aga Khan University, Karachi, Sindh, Pakistan; 2Department of Community Health Sciences, The Aga Khan University, Karachi, Sindh, Pakistan
Correspondence: Fauziah Rabbani
Office of Research and Graduate Studies, The Aga Khan University, Stadium Road, P.O Box 3500, Karachi, 74800, Sindh, Pakistan
Email [email protected]
Purpose: Diarrhea and pneumonia greatly contribute to high childhood mortality in Pakistan. Frontline community health workers or the Lady Health Workers (LHWs) provide care at the doorstep of over 60% of Pakistan’s rural residents. Difficult terrain, lack of supplies, and inadequate supervision put these LHWs at an added disadvantage in the timely diagnosis and delivery of known treatment options to community caregivers (CCGs). This study aims to assess whether a supportive supervision intervention through Lady Health Supervisors (LHSs) using enhanced mentorship and written feedback cards have the potential to improve case management of childhood diarrhea and pneumonia.
Study Setting and Design: This perception-based qualitative inquiry nested within the Nigraan Plus trial included LHSs, LHWs, and CCGs as the participants. Twenty-two in-depth interviews (IDIs) and 16 focus group discussions (FGDs) were conducted before a supportive supervision intervention in 2017, and 10 FGDs were conducted in 2019 once the intervention concluded. Data were analyzed using manual content analysis.
Results: The perceived ability of LHWs and LHSs to describe the danger signs of diarrhea and pneumonia, classify dehydration and relate respiratory rate to the severity of pneumonia improved over time. Appropriate prescription of zinc in diarrhea and antibiotics in pneumonia was noted. Furthermore, CCGs’ trust in LHWs increased following the intervention, and they reported a growing inclination to contact LHWs as their first point of care. LHWs in the intervention arm were more satisfied with their job due to frequent supervisory visits and continuous feedback by LHSs.
Conclusion: Despite geographic, social, and economic inequities, supportive supervision has the potential to improve knowledge, practice, and skills of frontline health workers related to CCM of childhood diarrhea and pneumonia in disadvantaged rural communities. Additionally, the trust of CCGs in the health workers’ ability to manage such cases is also enhanced.
Keywords: community health workers, community caregivers, community case management, childhood diarrhea and pneumonia, supportive supervision, Pakistan
Plain Language Summary
Diarrhea and pneumonia are major causes of death among children under the age of five in Pakistan. Frontline community health workers or the Lady Health Workers (LHWs) provide preventive care to mothers and children at the doorstep of over 60% of Pakistan’s rural residents. Difficulty in reaching far-flung areas and lack of medical supplies impede Lady Health Supervisors (LHSs) to provide mentorship and supervision to their assigned LHWs. This study aims to assess whether supportive supervision (Nigraan Plus trial) delivered through LHSs via written feedback and improved communication with LHWs has the potential to improve community case management of diarrhea and pneumonia. LHSs, LHWs, and caregivers of children participated in 22 interviews and 16 group discussions before and 10 group discussions after the intervention (2017, 2019). The study analyzed narrative text. Perceptions of LHSs and LHWs regarding their ability to describe the danger signs and severity of these two illnesses improved over time. Knowledge enhancement regarding appropriate treatment prescription was noted. Furthermore, caregivers’ trust in LHWs increased following the intervention, and they reported a growing inclination to contact LHWs as their first point of care. LHWs in the intervention arm were more satisfied with their job due to frequent supervisory visits and continuous feedback by LHSs. Despite geographic, social, and economic difficulties, supportive supervision showed the potential to improve community case management of childhood diarrhea and pneumonia
Introduction
Pneumonia and diarrhea are responsible for around 1.5 million deaths per year in children under five globally, accounting for 23% of all deaths in this age group.1 These deaths are concentrated in South Asia and sub-Saharan Africa, particularly in Pakistan, India, Nigeria, and the Democratic Republic of Congo.2 Pakistan has a sizable burden of diarrhea and pneumonia, with 14% and 27% of children <5 experiencing an episode of these diseases, respectively, at any given point in time.3 The outcome of these episodes of illness could be improved by ensuring adequate access to existing effective interventions, including Oral Rehydration Salt (ORS), zinc supplements, and antibiotics.4 Unfortunately, 63% of sick children <5 do not receive ORS when required, and only 8% are prescribed zinc supplements. Similarly, only 46% of suspected cases of childhood pneumonia are prescribed given antibiotics.1,3 These factors adversely impact the uptake of ORS, zinc, and antibiotics, and could result in Pakistan being unable to meet the Sustainable Development Goal targets by 2030.
Frontline Community Health Workers (CHWs) play a unique role in reducing the burden of childhood diarrhea and pneumonia. They improve the community’s access to healthcare by delivering services at their doorstep.4 When CHWs are adequately equipped and trained in the community case management (CCM) for diarrhea and pneumonia, they can effectively classify and treat sick children.5,6 Furthermore, they have a critical role in improving community caregivers’ (CCGs’), knowledge and practice in managing sick children. CCGs seeking treatment for their sick child from a CHW do not have to travel as far or wait as long and pay significantly less compared to facility-based care.7–9
In Pakistan, the Lady Health Worker (LHW) Programme was launched in 1994 to deliver maternal and child health services, including CCM for diarrhea and pneumonia.10 Inadequate knowledge and skills of LHWs, as well as poor supervision, have resulted in the LHW Programme failing to achieve the anticipated level of impact.10,11 Indeed, the Fourth External Evaluation of the National Programme for Family Planning and Primary Health Care (FENP) found that over three-fifths of sampled LHWs did not receive feedback from their Lady Health Supervisors (LHSs), and 41% of supervisors had not visited their health workers in the field in over three months.11
These LHWs serve over 60% of Pakistan’s rural communities.10 Several studies on Pakistan’s LHW Programme, and international CHWs have sought to explore how gender inequities in decision-making, poverty, and illiteracy adversely impact supervision and service delivery. One study in Badin District, Sindh, found that major challenges to the functioning of LHSs include a lack of transportation and supplies.12 This deficiency is further exacerbated by the difficulty and spread out of terrain, as well as too much importance of husband and family approval to work.12,13 Studies in lower-middle-income country (LMIC) settings indicate that factors associated with the inequitable distribution of healthcare may predispose disadvantaged rural communities to poor health outcomes adversely affecting health-seeking behavior. These include distance to health services,14 difficulties in transportation,15 caregiver access to household finances and decision-making,16 perceived quality of available health providers, availability and comprehension of health information, and perceived severity of illness.4
Despite these structural health system barriers, there is much that can be done to bring about improvements in CCM of childhood diarrhea and pneumonia in the interim. A paradigm shift of supervisory techniques has resulted in an emphasis on building a supportive link between the Supervisor and CHW. Supportive supervision substitutes the traditional inspection or control approach, focusing on trust, two-way communication, and teamwork. There is a strong emphasis on the Supervisor and CHW to engage in problem-solving, cross-learning, and skill sharing.17–21 Studies have found that training along with ongoing supportive supervision enhances CHWs skills related to CCM and subsequently improves CCG’s knowledge of signs, symptoms, and treatment of diarrhea and pneumonia.22,23
This qualitative inquiry, embedded within these existing inequities, aims to assess what changes occur in perceptions of CHWs and CCGs regarding the CCM of childhood diarrhea and pneumonia following a supportive supervision intervention.
Materials and Methods
Setting and Intervention
Project Nigraan Plus was a randomized cluster trial (RCT) conducted in the district of Mirpur Khas (MPK), in Sindh Pakistan. Exploratory qualitative assessments were conducted at baseline and endline (pre- and post-intervention) in 2017 and 2019, respectively. Such types of assessment allow for an in-depth exploration of participants’ knowledge, experiences, perceptions, and also fill in gaps that cannot be explored through quantitative surveys.24,25
District MPK is located on the south-eastern edge of the province of Sindh in Pakistan. The district covers an area of 2925 square kilometers, yet only has 716 kilometers of good-quality roads indicating poor quality road access.26 The district lies at a distance of 220 KM from the provincial capital Karachi and has a total population of 1,505,876, out of which 72% is rural.27 The sex ratio of the district is 108 males per 100 females, higher than the national average of 106 males/100 females, possibly due to an underrepresentation of women in national surveys, and a higher maternal mortality rate. These inequities are further reflected in the district’s literacy rates (for the population of 10 years and above), as 61% of the district’s men, and 27% of women are “literate”.26,28 Health coverage gaps are reduced by the district’s 983 functional LHWs that cover 62% of the district’s population. These LHWs are supervised by 39 LHSs.29 The child and infant mortality rates in MPK are 116 and 91 per thousand live births, respectively.30 The agriculture sector contributes to over 46% of the district’s income, resulting in three economic strata: landlords, small farmers, and haris (sharecroppers). Eighty percent of the haris belong to the Hindu minority group. Compared to the provincial average monthly household income of PKR 14,819, an average hari family earns around PKR 2000 per month and has poor access to healthcare facilities.26
Thirty-two LHSs were randomized, with 16 allocated to intervention and control groups. Of the 25–30 LHWs working under each LHS, five were randomly selected to take part in the study, coming to a total of 80 LHWs in each group. All 32 LHSs enrolled in Nigraan Plus trial received two days of refresher training on CCM for diarrhea and pneumonia based on the existing LHW Programme curriculum. Intervention arm LHSs received special training to improve their CCM of diarrhea and pneumonia and to enhance their supervisory mentorship skills. LHWs in this arm received written feedback during routine visits to the home of sick children between February 2018 and February 2019. Usual standard of care continued in the control arm.
The baseline qualitative assessment included 22 in-depth interviews (IDIs) and 16 focus group discussions (FGDs), and 10 FGDs were conducted at endline. These involved a total of 214 randomly selected CHWs (LHWs and LHSs) and CCGs in face-to-face interviews. The details are depicted in Figure 1. Randomly selected respondents were included in each IDI and FGD. LHS and LHW participants were recruited by the research team, and LHWs helped recruit CCG participants from their catchment areas. FGDs and IDIs were conducted up to the point of saturation.
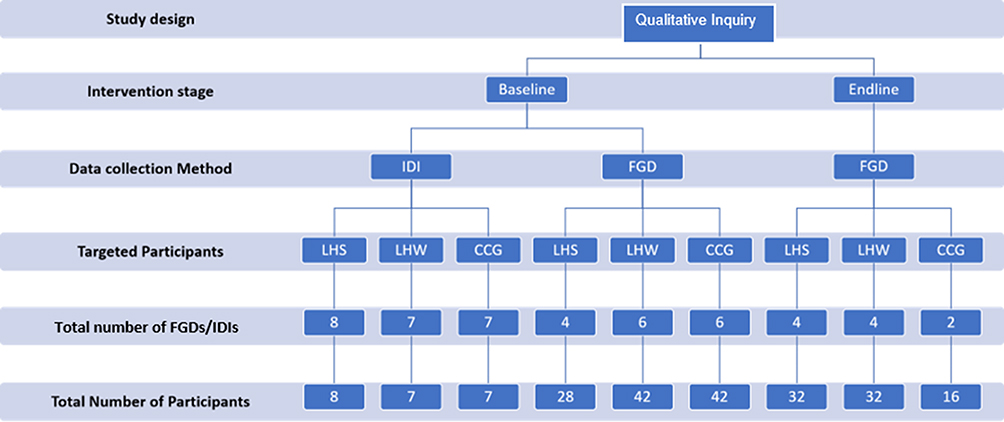 |
Figure 1 Flow chart of the methods used in the study. Abbreviations: IDI, in-depth interview; FGD, focus group discussion; CCG, community caregiver; LHS, lady health supervisor; LHW, lady health worker. |
Data Collection and Analysis
A semi-structured interview guide (Table 1) was developed for data collection through FGDs and IDIs. The guide was composed in English, translated into Urdu and Sindhi (the national and local language respectively), and back-translated into English. One FGD and one IDI were piloted during the baseline. Baseline FGDs and IDIs were conducted by SP1 (female, Senior Instructor, MSc, and MBBS), and Endline FGDs were conducted by coauthors HAK (male, Senior Research Coordinator, M.Bioeth and MBBS) and SP2 (male, Research Specialist, MPhil, MPH, MBBS), and nobody else was present besides the participants and researchers. These moderators have experience with qualitative research methods including the conduct of FGDs and IDI interviews and have a history of working in a rural setup. A relationship of trust was established with participants prior to the commencement of the qualitative inquiry through community liaising, informal talks, and by introducing the objectives of the study. Further, study participants were aware that the researchers were from a university and were doing this research as part of a project to better understand CHW and CCG perceptions regarding CCM of children <5 years who get sick with diarrhea and pneumonia.
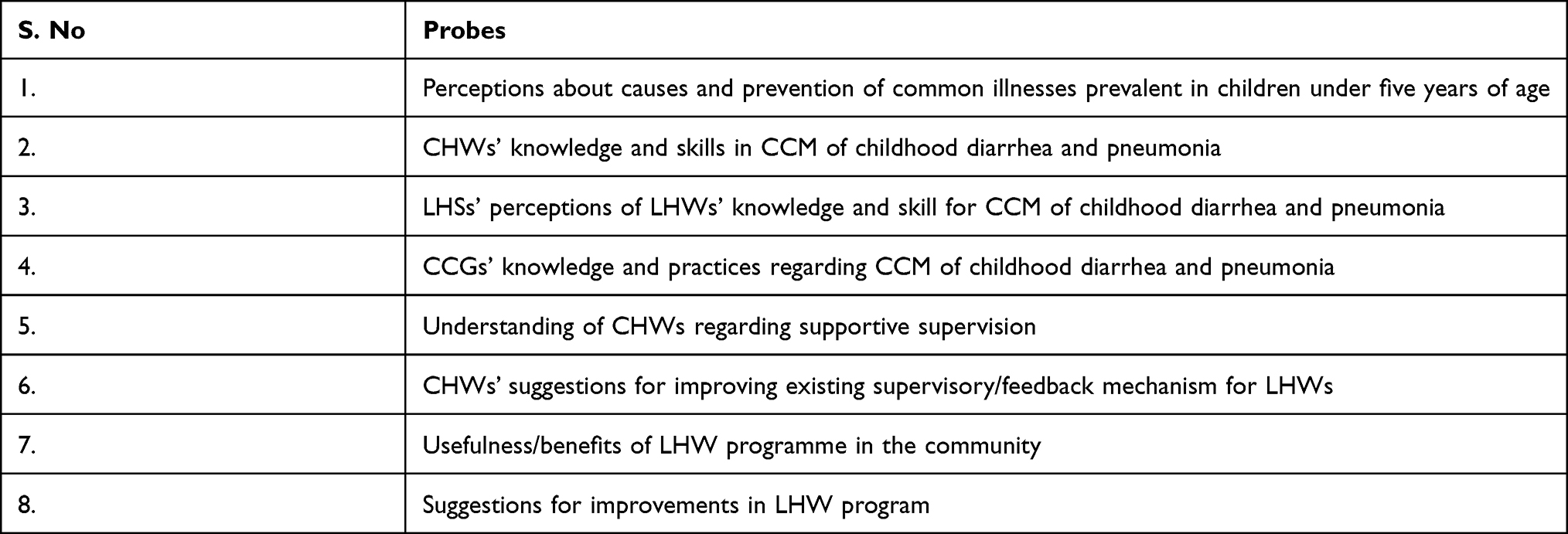 |
Table 1 Sample Probes from Focus Group Discussions and In-Depth Interviews |
FGDs and IDIs with CHWs were held at the District LHW Programme Office in MPK, while those with CCGs were conducted at a nearby health center. All FGDs and IDIs were audio-recorded with participants’ consent, and field notes were made during the interviews. The average time duration of FGD and IDI was approximately one hour.
All interviews were transcribed in English. Manual content analysis was conducted on all interview and FGD transcripts, and codes were organized into either emergent or predetermined categories by the three moderators. Commonalities and differences across the data were identified and clustered around thematic sections. Verbatim quotes have been added to complement the themes. The source of these quotes has been identified within the parenthesis next to the quote. This includes information on the timing of assessment (B: baseline/ E: endline), type (IDI/ FGD) with a unique identifier, the participant (LHS/LHW/CCG), and the arm of study from where data was collected (Intervention/Control).
Although participants were not shown transcripts of the research, a dissemination seminar was held at project conclusion, and findings shared with various stakeholders, including community representatives. Data were collected and analysis was compliant with COREQ guidelines.
Ethics
The ethical approval was obtained from the Aga Khan University (AKU) Ethical Review Committee in accordance with the Declaration of Helsinki. The main study protocol was registered with the Australian New Zealand Clinical Trial Registry (ACTRN12617000309381), and its results are reported elsewhere.31 This study is nested within a larger trial and follows the principles of a qualitative inquiry. Written consent was obtained from all respondents participating in focus group discussions and interviews. Participants were informed about the purpose of the study, and their informed consent included publication of anonymized responses.
Results
The mean age of the participating LHSs was 40.3 years. A majority of them had completed at least 12 years of schooling, and several had completed a Bachelor’s degree. Similarly, the mean age of participating LHWs was 36 years, and most reported their education level as 10th grade, which is the minimum pre-requisite educational level required for recruitment in the LHW Programme. CHWs had been working for the LHW-P for 7 −24 years. Further, the mean age of the CCGs who voluntarily participated was 32 years, and most had between one and three children under the age of five years.
Four themes emerging from this study include insights about childhood illness, knowledge and skills of CHWs regarding CCM of diarrhea and pneumonia, knowledge and practices of CCGs in the case management of these illnesses, and CHWs’ perspectives on supportive supervision (Figure 2).
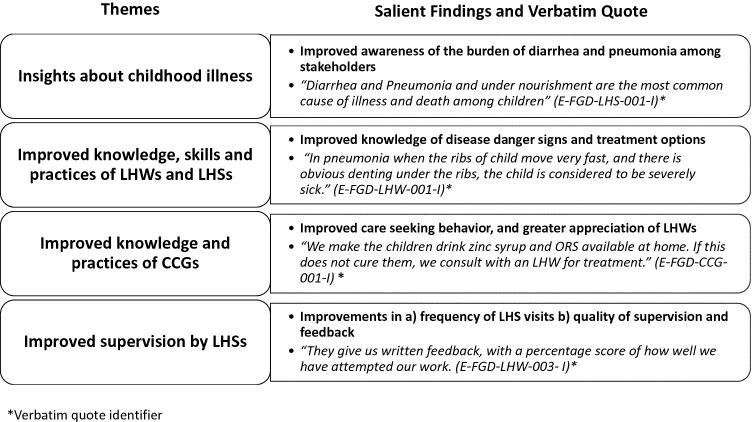 |
Figure 2 Themes and salient findings identified from qualitative interviews. *Verbatim quote identifier. |
Insights About Childhood Illness
CHW and CCG participants in the pre- and post-intervention interviews correctly perceived that diarrhea and pneumonia significantly contributed to health issues. Further, they recognized that these diseases result in several deaths among children <5 years in their community. In probing the causes of these illnesses, most CHW and CCG participants discussed how unsanitary environmental conditions and unhygienic caregiver practices are major reasons contributing to disease.
There is no cleanliness, there is contaminated drinking water. There is such water available which is not proper to drink … This is the cause of (diarrheal) disease (E-FGD-LHS-001-I)
CHWs believed that several members of their communities do not boil water prior to drinking. Further, they described poor handwashing practices among families, such as children not washing their hands after playing, and mothers forgetting to do so before cooking or feeding their child. They believed that these poor practices were due to a lack of awareness among CCGs. Even after a year of the supportive supervision intervention, CHWs mentioned how counseling caregivers to boil water and indulge in handwashing practices is difficult.
Water is unclean, and people do not boil it before drinking. We try to counsel them, but they do not understand that (diarrheal) disease spreads through dirty water. (E-FGD-LHW-001-I)
When the child goes to the washroom, and the mother washes the child herself, she does not wash her hands properly. We tell them the proper way to wash their hands. And if they use that method in a proper way, then they can avoid these illnesses. (E-FGD-LHW-003-I)
LHWs go and teach people about hygienic practices, such as when to wash hands and how to boil drinking water. It is difficult to bring about a behavioral change in the public. (E-FGD-LHS-002-C)
Contrary to CHWs’ perceptions, CCGs were familiar with major preventive strategies for childhood illnesses, naming hand washing, breastfeeding, boiling drinking water, and avoiding outside food. They reported practicing these hygienic measures and advising their children accordingly.
We teach the children that washing hands will keep them safe from a lot of diseases. (E-FGD-CCG-002-C)
During the endline FGDs, one CHW remained optimistic in her community’s hygiene practices. She mentioned that household cleanliness has started to improve, and caregivers are more mindful of LHW counseling.
My field is clean and nice. They do as I say. They themselves are very concerned. Everyone keeps their homes clean there. (E-FGD-LHW-003-I)
Community Case Management of Diarrhea and Pneumonia: Knowledge, Skills, and Practices of CHWs
CHWs’ knowledge of the general danger signs in a sick child had improved by the endline assessment. This was evident, as several CHWs were able to correctly specify most of the danger signs of diarrhea. They listed danger signs in sick children, such as fits and convulsion, blood in stool, vomiting, unconsciousness, lethargy, and an inability to drink water or mother’s milk. As one intervention arm LHW pointed out:
Some children get a high fever, and they start getting fits. Some become lethargic, and can’t get up or open their eyes due to weakness. They also may have blood coming in their stool. Such children need to be admitted to hospital. (E-FGD-LHW-001-I)
Similarly, CHWs’ knowledge of danger signs for pneumonia improved by the end of the study. They listed fast breathing, chest indrawing, and child being unable to drink water or breast milk as danger signs of pneumonia. During the endline interviews, an LHW in the intervention arm said:
in pneumonia when the ribs of a child move very fast, and there is obvious denting under the ribs, the child is considered to be severely sick. Yet, there are many who do not take their children to the hospital in such a situation. (E-FGD-LHW-001-I)
Most baseline interview participants lacked a sound knowledge of the correct classification system for dehydration. This was improved by the endline assessment, as several participants were better able to classify the severity of dehydration.
We categorize patients as A, B, C based on the severity of their condition. If the child’s skin returns to its place slowly after being pinched, their eyes are very dry, and they’re unconscious, then we place them in Category A. We need to refer such a child to a healthcare facility. (E-FGD-LHW-001-I)
Likewise, although CHWs had a general awareness of the clinical manifestations of pneumonia at the baseline assessment, they were found to be unable to correctly classify the disease severity. While mentioning the cut-offs for breathing rates, most CHWs interviewed prior to the intervention could not specify the age-specific variation to establish diagnosis. This improved by the end of the intervention, as more CHWs were able to detail the age-specific cut-offs for respiratory rates.
Similarly, there were improvements in CHWs’ awareness of symptoms. Further, they also knew when to refer sick children to a hospital setting. During baseline interviews, several participants inaccurately reported that the referral criteria for diarrhea is the persistence of loose stools alone. Most were unsure of the circumstances when a child with pneumonia required hospitalization. By the end of the study period, many CHWs demonstrated a strong understanding of referral criteria for diarrhea and pneumonia. Most of them correctly mentioned that pneumonia patients with breathing difficulties, high-grade fever, chest indrawing, and unconsciousness are indications for referral.
Most LHSs and LHWs correctly perceived ORS as an ideal treatment for diarrhea. The awareness of CHWs in the intervention arm regarding the role of zinc improved as a result of the intervention. One LHW mentioned:
With the use of zinc, the motions which a child does frequently become less frequent. (E-FGD-LHS-001-I)
If we see a child with diarrhea, we assess dehydration by pinching their skin to see if there is normal elasticity. We recommend zinc syrup and ORS to the child’s family. Even if loose motions subside, the zinc syrup should be given to complete the full course (for ten days). (E-FGD-LHW-003-I)
There was a mixed opinion regarding the use of antibiotics in treating diarrhea. Some CHWs interviewed during the baseline held the opinion that antibiotics can only be prescribed by a physician, and it is beyond their scope to recommend them to patients. Several believe that antibiotics are unnecessary in managing children with diarrhea, as dehydration and loss of minerals are the major causes of morbidity and mortality with this illness. Similar opinions were reported by CHWs during endline interviews.
And if we do find such a child who has even little loose motions, then we guide them to give the child ORS and Zinc Syrup for ten days. And this will make your child improve and his immunity will increase, and the child will not become weak. (E-FGD-LHW-003-I)
Awareness of the treatment options for pneumonia improved over the course of Nigraan Plus. During the baseline interviews, a few CHWs mentioned that they were not taught about the treatment of pneumonia. As with the treatment of diarrhea, some felt that they were not allowed to recommend antibiotics. However, by the end of the study period, several CHWs were more confident in managing pneumonia cases. They also mentioned that they are sometimes provided with antibiotics (Amoxicillin or Cotrimoxazole) to dispense in their catchment areas.
We give antibiotics twice a day for five days and we give according to age. And after giving one dose we refer them to physician. (E-FGD-LHS-001-I)
CHWs mentioned several challenges to effective case management within the community, such as unavailability of medication. They described how these deficiencies reduce their credibility among the community they serve.
When they go in the field and they do not have any medicines, the ladies say that the LHW has used up the medicine. And it is a very embarrassing situation. (E-FGD-LHS-001-I)
LHWs’ practice of initial and follow-up home visits was also probed. LHSs generally perceived that LHWs were the first point of contact with health services. Most supervisors specified that LHWs pay at least monthly visits to their catchment area, and a few mentioned that visits take place when the child is seriously sick. Participants in interviews during the endline assessment also mentioned that they conduct additional visits when caretakers inform them of their child being unwell.
We follow up with our patient 2 to 3 times, and the LHS follows up once or twice. (E-FGD-LHW-001-I)
LHWs follow up with the patient within 24 hours of the initial visit, and then again within three days. (E-FGD-LHS-001-I)
By the end of the intervention period, LHWs mentioned that they exchange telephone numbers with caregivers, and follow-up with their patients telephonically too.
Mothers of sick children call us via telephone for help now. (E-FGD-LHW-001-I)
LHSs’ perception of LHW performance improved following the intervention. They perceived enhancements in LHW’s knowledge and skills in managing diarrhea and pneumonia, as well as in their counseling skills. Some LHSs said:
I have a total of 25 LHW’s, five of whom were selected for the Intervention. Now there is an obvious difference. Those selected are doing better work and have more knowledge. They are doing the categorization of illness properly. They are explaining and referring too. They are doing good work. (E-FGD-LHS-001-I)
We are not saying that LHWs have no knowledge. Since you have started this project, LHWs have started to use the knowledge they had more accurately (E-FGD-LHS-001-I)
CCM of Diarrhea and Pneumonia: Knowledge and Practices of CCGs
By the end of the intervention, most CCGs were able to recognize several important danger signs associated with poor disease prognosis, even if not all of them. “Weakness”, “vomiting” and “high fever” were commonly cited by CCGs as danger signs. Many other signs of sickness, such as abdominal pain, increased frequency of stools, fast breathing, congested chest was also reported. Interviews with CCGs revealed a perception that LHWs have not educated mothers about the danger signs in children. CCGs correctly mentioned that loose skin and unconsciousness are signs of dehydration. However, a few of the CCGs’ misperceptions about what frequency of loose stool episodes constitutes diarrhea did not improve over the course of the study.
If they are doing it thrice it’s not diarrhea, but if the frequency is around 15 again and again when you give them food then it is diarrhea (B-FGD-CCG-007-C)
Yes, like stomach gets wrinkles and checking for dehydration is done by pinching the skin. (if the child is dehydrated), we need to take them to the hospital (E-FGD-CCG-001-I)
It was noted that CCGs were generally more aware of the signs of pneumonia by the end of the study, and considered breathing difficulty as a major sign. One mother said that an LHW had taught her to look at the depression over her child’s ribs. Some also mentioned cough and fever as associated signs of pneumonia.
CCGs were familiar with the role of ORS in managing children with diarrhea. They mentioned that ORS could be made either from sachets, or could be prepared at home using salt and sugar. By the endline assessment, more CCGs were aware of the importance of zinc supplements as a result of the intervention.
We make a whole jug of ORS, by pouring 4 glasses of water in it and then adding a sachet of ORS. We give small quantities of that water to the (sick) child frequently. (E-FGD-CCG-001-I)
We make the children drink zinc syrup and ORS available at home. If this does not cure them, we consult with an LHW for treatment. (E-FGD-CCG-001-I)
Participants of both baseline and endline interviews recognized the importance of family elders, such as mothers-in-law, as important sources of health information. CCGs discuss how they require permission from their husbands or in-laws prior to seeking healthcare for their children. This highlights an inequitable share of household decision-making and the potential delay in seeking healthcare.
(Our) parents have told us about turgor and dehydration for diarrhea and movement of ribs for pneumonia … And if it’s not settled, then one should consult a doctor. (B-FGD-CCG-006-C)
When we have any problem, then we go and consult with our mother-in-law first, as to what needs to be done …. Then after that, we decide to go to the hospital or if the LHW visits, we ask her opinion as to what needs to be done (E-FGD-CCG-001-I)
CCGs interviewed prior to the intervention were found to prefer seeking care from doctors (either from private or public sector). Some stated that this was due to dissatisfaction with the frequency of LHW visits, a lack of trust in LHWs’ and a preference for curative services.
Over the course of the study, it was found that CCG perceptions regarding LHWs had improved. Half of the CCGs interviewed during the baseline expressed their dissatisfaction with LHWs visits. One mother perceived that it had been a year since her LHW had come to visit. Similarly, a group of participants complained about the infrequency of LHW visits, especially if their children were sick. A few mentioned that they only come for vaccination campaigns, or only when called by CCGs. While expressing grievances about LHWs absence, one CCG said;
Why doesn’t she (LHW) come to us …. She is not available when our children are ill, we have to take our child to a hospital for medication, if she can’t do the job, she should quit. (B-FGD-CCG-005-C)
CCG perceptions regarding preference in seeking care from LHWs have significantly improved by the endline FGDs, with many stating that they consult them first for medical care.
Initially, when our children got sick, we resorted to home remedies. Now, LHWs have made our lives easier. They provide us medicines on our doorsteps. They guide us well. We follow what they say. (E-FGD-CCG-001-I)
These perceptions were corroborated by CHWs, who reported improved interactions with the community following the Nigraan Plus intervention.
They (CCGs) used to have less trust in us, but they know and trust us a lot more since the beginning of the intervention. They ask us to come and check their sick children, and they wait for us to come and visit. (E-FGD-LHW-001-I)
Some CHWs at the endline assessment also observed that that CCGs prefer to seek care from private clinics over government hospitals and LHW.
Majority of the parents prefer to visit private hospitals. In government hospitals, the treatment is subpar, and our referrals are not getting due importance. Parents prefer visiting practitioners who have a private practice in evening. They give injections and medicines. (E-FGD-LHS-002-C)
Perspectives About Supervisors and Supportive Supervision
Although most of the participating CHWs were unaware of the term supportive supervision, a few were able to describe some corresponding characteristics following completion of intervention. LHSs considered supervision as “good and mutual support for each other and working in a friendly environment”. Supportive supervision for a few of the LHSs was “lending support to LHWs”. Some of the LHSs described it as, “receiving support from authorities and NGOs”;
Where she has problems, she gets guidance to solve problems and difficulties, she is supported. (E-FGD-LHS-003-I)
The frequency of LHS visits improved in the intervention group by the end of the Nigraan Plus trial. During the baseline assessments, LHSs reported that they visited their community infrequently. By the post-intervention period, many LHSs stated that they conduct 1–2 community visits/LHW in a month, as per program mandate. LHS participants from endline FGDs acknowledged that they perform up to six home visits per month and that the frequency depends upon case severity and distance.
It is not mandatory to visit in certain times; we can visit whenever we feel the need (B-IDI-LHS-007-C)
When the case is severe, we do visit once with the LHW and then we visit again on another time, if we can’t manage to go, then we enquire from them through phone whether they had gone to see or not. (E-FGD-LHS-001-I)
Usually we visit two times, but since the Intervention started, we go with them three or even four times, in some cases even more. (E-FGD-LHS-003-I)
LHWs’ perception of LHS supervision improved over the course of the intervention. LHWs interviewed during the study’s baseline reported that only a few supervisors visit 2–3 times in a month as per directive from LHW-P, and most do not actively go to the community. This improved by the end of the intervention. Many LHWs at endline assessment stated that LHSs pay one or two visits per month routinely, and a few of them mentioned more than two visits especially if LHWs require supervisor’s help.
LHSs don’t come and visit, which makes LHW’s work tougher (B-IDI-LHW-002-I)
They go with us whenever we ask. Like when we tell them that there is a child you need to visit, then the LHS accompanies us. (E-FGD-LHW-001-I)
While exploring the experience of CCGs in seeking care from LHWs, many pre-intervention interviewees felt that they have not seen a supervisor for a long time. A few CCGs shared that supervisors usually pay visits during Polio immunization rounds and health education sessions only.
Supervisor don’t commonly come, LHW comes once a month (B-IDI-CCG-002-C)
Some LHWs expressed their disappointment with feedback mechanisms, perceiving that they were not appreciated for their hard work.
If you perform your task well, there is no appreciation or increment in our salary. If you don’t do your work properly then also nobody praises you. (B-IDI-LHW-002-I)
This response was improved by the endline assessment, with many LHWs stating that they are getting the feedback from their supervisors monthly on regular basis. Some of them mentioned that they are getting feedback in both verbal and written form. Some of the LHWs reported that they are getting feedback individually and few mentioned in groups too.
They give us paper in which we write down and apart from that the supervisor tells us verbally what we have done well. (E-FGD-LHW-003- I)
CHWs and CCGs mentioned several challenges to effective supervision, such as unavailability of transport, poor planning and scheduling of supervisory visits, and a lack of supervisory checklists. LHSs also mentioned how the lack of transport facilities and fuel allowances impaired their ability to conduct supervisory visits.
Our (supervisory visit) plans are not properly developed, and LHWs are unaware when their supervisor will visit. So, she (an LHW) does not have a chance to check or correct her records prior to these visits (B-IDI-LHS-002- I)
Discussion
This study highlights several geographic, social, and economic inequities which act as barriers to optimal CCM for childhood diarrhea and pneumonia. The four themes illustrate how supportive supervision intervention (as in Nigraan Plus trial) has started to bring about positive improvements despite these inequities.
Positive changes were noted in LHWs’ and LHS’ ability to describe the danger signs of diarrhea and pneumonia, refer critical patients and treat these diseases. Since the intervention ensured regular CHW household visits, CCGs’ trust in LHWs’ capability to treat sick children was enhanced.
Although CHWs and CCGs were aware of the burden and causes of diarrhea and pneumonia in their community, they reported that preventive practices (such as hand hygiene and boiling water before use) remained poor among caregivers. Despite these suboptimal practices, some CHWs in the intervention arm remained optimistic, reporting that their community was becoming more receptive towards their counseling for preventive measures following the intervention. Indeed, previous studies show that interventions focusing on counseling children’s mothers improve preventive practices.32 Time may, however, be required for any effect to be measurable.33
Following one year of the Nigraan Plus execution, CHWs in the intervention arm were more familiar with the danger signs of childhood diarrhea and pneumonia. Further, they were better able to classify the severity of diarrhea and pneumonia. These findings are well supported, as other studies have found that continuous mentorship and supportive supervision lead to improvements in CHWs’ knowledge and skills for CCM of diarrhea and pneumonia in Africa and India.13,15,23 Further, in an earlier trial in Pakistan, following supportive supervision intervention, LHWs took more accurate histories for assessing danger signs of pneumonia and diarrhea, and in classifying the severity of these diseases.34
Prior to the intervention, CHWs perceived that they were not trained in the treatment of pneumonia, and could not recall the correct antibiotics to prescribe. By the end of the intervention, more CHWs were able to identify the correct antibiotic and appropriate dosages for cases of pneumonia. This is similar to a study from South Sudan, which found that a supportive supervision intervention significantly improved CHWs’ utilization rates of ORS, zinc, and antibiotics for diarrhea and respiratory infections.33
Several CHWs could recall the referral criteria for diarrhea and pneumonia following the intervention. This could be attributed to improved knowledge of the clinical manifestations and danger signs for these diseases. In a similar trial in an adjacent district, significant improvements in LHWs’ ability to appropriately refer patients to a hospital facility for cases of childhood diarrhea and pneumonia was noted.34 Stronger referral systems ultimately reduce the burden of care on secondary and tertiary healthcare facilities and minimize costs.30
The study also found similar improvements in CCGs’ (mothers) knowledge and practices in managing diarrhea and pneumonia over time. This is evident through their ability to recognize danger signs and treat their sick children. This is in line with the findings of an earlier, similar trial in rural Sindh, which reported an increase in the CCGs’ knowledge of the signs and symptoms of diarrhea and pneumonia following a supportive supervision intervention.35,36 CCGs’ knowledge of illnesses is important, as there is a direct relationship between mothers’ ability to correctly identify illness and seek care for their sick children. There is evidence from sub-Saharan Africa to support that caregiver interpretation of the severity of an illness predicts their decision to seek medical care promptly.37
CCGs interviewed during the baseline discussed their preference towards seeking care from private practitioners. This is not surprising given the poor quality of health care in the public health care system in Pakistan generally and in disadvantaged rural areas specifically. This is also consistent with other studies, which found that 78% of households in Sindh use private healthcare facilities for their medical needs.38 This is unfortunate, as over two-thirds of the total health expenditure in Sindh is out of pocket, with poorer households spending a higher proportion of income on health expenses.38 Healthcare from private health facilities can be up to six times more expensive than seeking care from LHWs.39,40 It was heartening, therefore, that CCGs interviewed following the Nigraan Plus intervention reported that LHWs were increasingly becoming their first point of contact with the healthcare system. They had a greater trust in LHWs’ skills in managing sick children and perceived improvement in the frequency of health workers’ household visits. This finding is consistent with the study conducted in Nigeria, which showed that CHWs undergoing training and ongoing support and supervision resulted in caregivers seeking them to manage their sick children.23
The baseline assessments of this study indicate that there were infrequent supervisory visits. However, towards the conclusion of Nigraan plus trial in 2019, CHWs reported that the frequency of supervisory visits and quality of feedback had improved. CHW participants of 2019 interviews noted that verbal group feedback had changed to an individual written one, which LHWs perceived to be more productive. Prior studies have shown that giving CHWs access to feedback about their work can lead to performance improvements. This was supported by an earlier trial, which found that LHWs provided structured supervisory feedback that improved their CCM of diarrhea and pneumonia.34 One study conducted in Mali reported that showing written personalized performance feedback to CHWs during face-to-face meetings with their supervisors led to improvements in health worker performance.41 Another suggests that a mix of group and individual feedback sessions, accompanied by supervisory checklists, has the potential to yield a strong impact on CHW motivation and performance.33
Despite these improvements, this study also highlights various inequities that constrain CHWS to perform optimally. CHWs were overburdened, poorly supplied with medicines, and were not provided with transportation facilities or an allowance to reach out to the far-flung homes of sick children. In addition to unhygienic behavioral practices of rural inhabitants, the influence of the traditional family system in seeking timely care, coupled with poor sanitation also impedes control of these two major childhood illnesses. Irregularities in the supervision of LHWs were also noted. These irregularities could be a consequence of budgeting difficulties, with previous studies noting how bridge grants are often used to fund the LHW Programme.13 This economic constraint is not unique to the LHW Programme. Indeed, studies on CHWs have found that lay workers function more productively when they have a manageable workload, a reasonable geographic distance to cover, adequate supplies and equipment, a supportive supervisor, and community acceptance.12,42,43
This study had some limitations, and the findings should be viewed with caution. It is only based on the perceptions of those who participated in the FGDs and IDIs. Hence, respondent and selection bias cannot be ruled out. Moreover, the actual impact of intervention on CCM of childhood diarrhea and pneumonia can only be ascertained through quantitative assessment of CHWs’ and CCGs’ knowledge and skills.
Conclusion
In conclusion, this study does give an early indication that supportive supervision delivered by LHSs to LHWs has the potential to produce positive perceptions, ultimately leading to gains in CCM of childhood diarrhea and pneumonia. However, social, geographic, and economic inequities should be factored in while scaling up such interventions.
Data Sharing Statement
Data can be made available on request. If you wish to request for the data, please email the corresponding author, Dr. Fauziah Rabbani, at [email protected]
Ethics Approval
Ethics approval was acquired from the Aga Khan University Ethics Review Committee in accordance with the Declaration of Helsinki
Acknowledgments
The authors would like to thank Dr. Zulfiqar Bhutta, Principal Investigator, Umeed-e-Nau Project, Center of Excillence, Woman and Child Health, AKU,for funding this study. The authors appreciate the hard work and convey their thanks to the project field staff (Raheel Roshan, Ayaz Ansari, Imran) and the entire team of data collectors. The authors would also like to thank the Department of Health (DOH), the Government of Sindh, and the Provincial and District LHW program officials for demonstrating their support for the study and allowing them to work with The Lady Health Supervisors and the Workers. Most of all, we would like to thank the LHWs and LHSs of the MPK district for their tireless efforts.
Funding
The research was funded by the Bill and Melinda Gates Foundation under the Umeed e Nau Project. The funders did not influence results in any way.
Disclosure
Dr Fauziah Rabbani, Dr Hyder Ali Khan, Dr Suneel Piryani, and Dr Shagufta Perveen report grants from Bill and Melinda Gates Foundation, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. United Nations Inter-agency Group for Child Mortality Estimation (UN IGME). Levels & Trends in Child Mortality: Report 2019, Estimates Developed by the United Nations Inter-Agency Group for Child Mortality Estimation. United Nations Children’s Fund; 2019.
2. UNICEF. One is Too Many: Ending Child Deaths from Pneumonia and Diarrhea. UNICEF; 2016.
3. National Institute of Population Studies P. Pakistan Demographic and Health Survey 2017–18. Islamabad, Pakistan: NIPS/Pakistan and ICF; 2019.
4. Bhutta ZA, Das JK, Walker N, et al. Interventions to address deaths from childhood pneumonia and diarrhea equitably: what works and at what cost? Lancet. 2013;381(9875):1417–1429. doi:10.1016/S0140-6736(13)60648-0
5. Gilroy K, Winch P. Management of sick children by community health workers. Intervention models and programme examples; 2006.
6. Hadi A. Diagnosis of pneumonia by community health volunteers: experience of BRAC, Bangladesh. Trop Doct. 2001;31(2):75–77. doi:10.1177/004947550103100206
7. Soremekun S, Kasteng F, Lingam R, et al. Variation in the quality and out-of-pocket cost of treatment for childhood malaria, diarrhea, and pneumonia: community and facility based care in rural Uganda. PLoS One. 2018;13(11):e0200543. doi:10.1371/journal.pone.0200543
8. Shaw JD, Gupta N, Delery JE. Alternative conceptualizations of the relationship between voluntary turnover and organizational performance. Acad Manage J. 2005;48(1):50–68. doi:10.5465/amj.2005.15993112
9. Daviaud E, Besada D, Leon N, et al. Costs of implementing integrated community case management (iCCM) in six African countries: implications for sustainability. J Glob Health. 2017;7(1). doi:10.7189/jogh.07.010403.
10. Hafeez A, Mohamud BK, Shiekh MR, Shah SAI, Jooma R. Lady health workers programme in Pakistan: challenges, achievements and the way forward. J Pak Med Assoc. 2011;61(3):210.
11. Oxford Policy Management. Lady Health Worker Programme: External Evaluation of the National Programme for Family Planning and Primary Health Care. Quantitative Survey Report. Oxford Policy Management; 2009.
12. Rabbani F, Shipton L, Aftab W, Sangrasi K, Perveen S, Zahidie A. Inspiring health worker motivation with supportive supervision: a survey of lady health supervisor motivating factors in rural Pakistan. BMC Health Serv Res. 2016;16(1):397. doi:10.1186/s12913-016-1641-x
13. Rabbani F, Perveen S, Abbas IN, et al. Policy makers perceptions regarding performance of the lady health worker programme: is there a know-do gap? Findings from the NIGRAAN project. Pak J Public Health. 2016;5(4):30.
14. Ferrer BE, Webster J, Bruce J, et al. Integrated community case management and community-based health planning and services: a cross sectional study on the effectiveness of the national implementation for the treatment of malaria, diarrhea and pneumonia. Malar J. 2016;15(1):340. doi:10.1186/s12936-016-1380-9
15. Lungu EA, Biesma R, Chirwa M, Darker C. Healthcare seeking practices and barriers to accessing under-five child health services in urban slums in Malawi: a qualitative study. BMC Health Serv Res. 2016;16(1):410. doi:10.1186/s12913-016-1678-x
16. Dougherty L, Gilroy K, Olayemi A, et al. Understanding factors influencing care seeking for sick children in Ebonyi and Kogi States, Nigeria. BMC Public Health. 2020;20(1):1–11. doi:10.1186/s12889-020-08536-5
17. Bailey C, Blake C, Schriver M, Cubaka VK, Thomas T, Martin Hilber A. A systematic review of supportive supervision as a strategy to improve primary healthcare services in Sub‐Saharan Africa. Int J Gynecol Obstet. 2016;132(1):117–125. doi:10.1016/j.ijgo.2015.10.004
18. Marquez L, Kean L. Making supervision supportive and sustainable: new approaches to old problems. MAQ Paper No. 4. Supplement to Population Reports, Volume XXX, Issue 4; 2011.
19. Bradley S, Kamwendo F, Masanja H, et al. District health managers’ perceptions of supervision in Malawi and Tanzania. Hum Resour Health. 2013;11(1):43. doi:10.1186/1478-4491-11-43
20. Hill Z, Dumbaugh M, Benton L, et al. Supervising community health workers in low-income countries–a review of impact and implementation issues. Glob Health Action. 2014;7(1):24085.
21. Kok MC, Vallières F, Tulloch O, et al. Does supportive supervision enhance community health worker motivation? A mixed-methods study in four African countries. Health Policy Plan. 2018;33(9):988–998. doi:10.1093/heapol/czy082
22. Shiroya-Wandabwa M, Kabue M, Kasungami D, et al. Coaching community health volunteers in integrated community case management improves the care of sick children under-5: experience from Bondo, Kenya. Int J Integr Care. 2018;18(4). doi:10.5334/ijic.3971.
23. Oresanya O, Counihan H, Nndaliman I, et al. Effect of community-based intervention on improving access to treatment for sick under-five children in hard-to-reach communities in Niger State, Nigeria. J Glob Health. 2019;9(1). doi:10.7189/jogh.09.010803.
24. Kitzinger J. Qualitative research: introducing focus groups. BMJ. 1995;311(7000):299–302. doi:10.1136/bmj.311.7000.299
25. Berg B. Qualitative Research Methods for the Social Sciences.
26. Pakistan emergency situation analysis - District Mirpurkhas, Sindh.pdf. Available from: https://reliefweb.int/sites/reliefweb.int/files/resources/PESA-District-Mirpurkhas-Sindh.pdf.
27. Pakistan Bureau of Statistics. Block wise provisional summary results of 6th population & housing census-2017. Pakistan Bureau of Statistics; 2018. Available from: http://www.pbs.gov.pk/content/block-wise-provisional-summary-results-6th-population-housing-census-2017-january–03–2018.
28. Pakistan Bureau of Statistics. Mirpur Khas district at a glance; 2013. Available from: http://www.pbs.gov.pk/content/district-glance-mirpur-khas.
29. UNDP Pakistan & Government of Sindh. Report on the Status of Millennium Development Goals Sindh. UNDP Pakistan & Government of Sindh; 2012.
30. Sindh Bureau of Statistics & UNICEF. Sindh Multiple Indicator Cluster Survey 2014, Final Report. Sindh Bureau of Statistics and UNICEF; 2015.
31. Aftab W, Piryani S, Rabbani F. Does supportive supervision intervention improve community health worker knowledge and practices for community management of childhood diarrhea and pneumonia? Lessons for scale-up from Nigraan and Nigraan Plus trials in Pakistan. Hum Resour Health. 2021;19(1):
32. Sunanda G, Ramaiah D, Sadiq MMJ, Narayana G. Impact of structured educational program on maternal knowledge, attitude, and practice toward diarrhea management in children< 5 years age in Anantapur district. CHRISMED J Health Res. 2017;4(3):186.
33. Rosales A, Hedrick J, Amet KK, et al. Maintaining knowledge and technical skills among illiterate frontline community health workers (HHPs) delivering Integrated Community Case Management (ICCM) in South Sudan [Online]. Washington DC: CCMCentral by USAID/MCHIP; 2014.
34. Aftab W, Rabbani F, Sangrasi K, Perveen S, Zahidie A, Qazi SA. Improving community health worker performance through supportive supervision: a randomised controlled implementation trial in Pakistan. Acta Paediatr. 2018;107:63–71. doi:10.1111/apa.14282
35. Sangrasi K, Rabbani F, Aftab W, et al. Caregivers knowledge, practices about childhood diarrhea and pneumonia and their perceptions of lady health worker program; findings from NIGRAAN implementation research project. J Community Med Health Educ. 2016;6(5):1.
36. Aftab W, Shipton L, Rabbani F, et al. Exploring health care seeking knowledge, perceptions and practices for childhood diarrhea and pneumonia and their context in a rural Pakistani community. BMC Health Serv Res. 2018;18(1):44. doi:10.1186/s12913-018-2845-z
37. Noordam AC, Sharkey AB, Hinssen P, Dinant G, Cals JW. Association between caregivers’ knowledge and care seeking behaviour for children with symptoms of pneumonia in six sub-Saharan African Countries. BMC Health Serv Res. 2017;17(1):107. doi:10.1186/s12913-017-2060-3
38. Zaidi S. Sindh Health Sector Strategy 2012 – 2020; 2012:126.
39. Sadruddin S, Ibad Ul Haque Khan AB, Khan A, Ahmad I, Qazi SA. Effect of community mobilization on appropriate care seeking for pneumonia in Haripur, Pakistan. J Glob Health. 2015;5(1). doi:10.7189/jogh.05.010405
40. Sadruddin S, Shehzad S, Bari A, Khan A, Khan A, Qazi S. Household costs for treatment of severe pneumonia in Pakistan. Am J Trop Med Hyg. 2012;87(5_Suppl):137–143. doi:10.4269/ajtmh.2012.12-0242
41. Whidden C, Kayentao K, Liu JX, et al. Improving community health worker performance by using a personalised feedback dashboard for supervision: a randomised controlled trial. J Glob Health. 2018;8(2). doi:10.7189/jogh.08.020418.
42. Jaskiewicz W, Tulenko K. Increasing community health worker productivity and effectiveness: a review of the influence of the work environment. Hum Resour Health. 2012;10(1):38. doi:10.1186/1478-4491-10-38
43. Ludwick T, Turyakira E, Kyomuhangi T, Manalili K, Robinson S, Brenner JL. Supportive supervision and constructive relationships with healthcare workers support CHW performance: use of a qualitative framework to evaluate CHW programming in Uganda. Hum Resour Health. 2018;16(1):11. doi:10.1186/s12960-018-0272-1
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.