Back to Journals » ClinicoEconomics and Outcomes Research » Volume 13
Changes in the Penetration Rate of Biosimilar Infliximab Within Japan Using a Japanese Claims Database
Authors Matsumoto T ![]() , Tsuchiya T, Hirano T, Laurent T, Matsunaga K, Takata J
, Tsuchiya T, Hirano T, Laurent T, Matsunaga K, Takata J
Received 24 November 2020
Accepted for publication 7 February 2021
Published 25 February 2021 Volume 2021:13 Pages 145—153
DOI https://doi.org/10.2147/CEOR.S293698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Samer Hamidi
Tsugumi Matsumoto,1,2 Takanori Tsuchiya,3 Takahiro Hirano,4 Thomas Laurent,4 Kazuhisa Matsunaga,1 Jiro Takata1
1Faculty of Pharmaceutical Sciences, Fukuoka University, Fukuoka, Japan; 2Inflammation and Immunology Therapeutic Area Medical Affairs, Pfizer Japan Inc., Tokyo, Japan; 3Patient Impact Analysis, Outcome & Evidence, Corporate Affairs Health and Values, Pfizer Japan Inc., Tokyo, Japan; 4Clinical Study Support Inc., Nagoya, Japan
Correspondence: Jiro Takata
Faculty of Pharmaceutical Sciences, Fukuoka University, 8-19-1, Nanakuma, Jonan-Ku, Fukuoka, 814-0180, Japan
Tel +81 92-871-6631
Fax +81 92-871-663
Email [email protected]
Purpose: Infliximab, which was approved in 2002, had its first biosimilar launched in 2014 across Japan. However, the penetration rate of this biosimilar remains unclear given the limited data regarding its current clinical use throughout Japan. This study was conducted to describe the current clinical characteristics of patients receiving infliximab and the penetration rate of the reference infliximab and/or biosimilar infliximab using a Japanese administrative claims database.
Patients and Methods: This retrospective, descriptive study utilized the Japan Medical Data Vision database, a nationwide hospital-based database. Data on patients receiving infliximab recorded from April 2008 to March 2019 were extracted from the database. Patient characteristics of the reference and biosimilar infliximab groups and penetration rates according to fiscal year, target diseases diagnosis, and subsidy for intractable diseases were examined.
Results: A total of 9735 patients were extracted for analysis, among whom 92% (n=8950) and 8% (n=785) received only reference infliximab and its biosimilar, respectively. Both groups exhibited similar clinical characteristics. The biosimilar penetration rate increased from 0.8% in 2014 to 22.5% in 2018, with overall penetration rates throughout the period according to diagnosis (with or without subsidy) being 14.4% (with, 4.1%; without, 16.4%), 4.7% (with, 3.7%; without, 10.6%), 5.7% (with, 4.5%; without, 13.5%), and 7.5% (with, 4.4%; without, 8.2%) for rheumatoid arthritis, Crohn’s disease, ulcerative colitis, and psoriasis, respectively.
Conclusion: Biosimilar infliximab is prescribed for patients with similar characteristics to reference infliximab. Despite the increasing penetration rates according to target disease, they remain much lower among patients receiving subsidy for intractable disease than among those who do not.
Keywords: intractable disease, biologics, TNF-α, rheumatoid arthritis, inflammatory bowel disease
Introduction
As therapeutic agents, biologic medications bring about tremendous benefits for serious life-threatening and chronic diseases.1 In Japan, several biologic medications have been approved since insulin was first approved as a biologic medication in 1985.2 While biologic medications offer considerable therapeutic benefits, they have increased medical expenditure. Drug prices of recently approved drugs, including biologics, anti-cancer drugs, and anti-hepatitis C drugs, are especially high.3,4 The Japanese national health-care system is currently facing difficulties due to population aging and the introduction of new high-cost drugs, which may jeopardize its integrity. As such, expanding the usage of biosimilars has been anticipated to be a solution for reducing national health-care costs, given that they are priced approximately 30% cheaper than their reference products within the Japanese national health insurance drug price system.5 A number of biosimilars have been approved as highly similar to their reference products, following studies required to show that they have no clinically significant differences in safety, purity, or potency (safety and effectiveness) compared with the reference product.6,7 Considering that only biosimilar products that meet rigorous standards are approved by regulatory authorities,8 physicians and patients should have no concern regarding their use. However, the truth of the matter is that some physicians lack the confidence to prescribe biosimilars, while patients receive insufficient explanations regarding biosimilars from physicians.9 As of November 15, 2019, the Japanese Pharmaceuticals and Medical Devices Agency (PMDA) has approved 21 biosimilar marketing authorizations of 11 reference biologic products.10 Since 2018, the Japanese Ministry of Health, Labour and Welfare (MHLW) has issued policies leading to awareness regarding biosimilars.11 However, previous research suggests that biosimilars had insufficient penetration rates within Japan. Discrepancies in penetration rates have been observed among four biosimilar products (insulin glargine, filgrastim, infliximab, and rituximab), which have been available in Japan within the period from 2012 to 2018. Among them, in the second half of 2018, biosimilar filgrastim had the highest penetration rate at 80% and biosimilar infliximab had the lowest rate at 5.3%.12
Infliximab is a chimeric monoclonal antibody against tumor necrosis factor alpha (TNF-α) used for treatment of rheumatoid arthritis (RA), Crohn’s disease (CD), ulcerative colitis (UC), psoriasis (Ps), Behçet’s disease with uveitis, ankylosing spondylitis, neuro-Behçet’s disease, and Kawasaki disease.13 The first biosimilar of infliximab was approved by the PMDA in 2014 for RA, CD, and UC.10 However, 5 years after its approval, the biosimilar has yet to overtake reference infliximab treatment. One possible reason is that Japan has a robust health-care system that includes a high-cost medical expense benefit program (Eligibility Certificate for Ceiling-Amount Application) and a medical care subsidy system for intractable diseases. The high-cost medical expense benefit system pays off any amount exceeding a fixed monthly limit to prevent excessive financial burden on the patient.14,15 The intractable disease system, formerly called the specific diseases program, has two major components: a research grant for intractable diseases and a medical cost subsidy for intractable diseases. Patients covered by the subsidy scheme receive waivers for all or some co-payments for medical bills to eliminate the financial barrier to health services, thereby encouraging a larger number of patients with intractable diseases to register in the research program.16 Among the indications for biosimilar infliximab, CD, UC, and some Ps are included in target diseases of the intractable system.17 The subsidy systems are believed to reduce motivation for using biosimilars, given that patients’ medical expenditure would remain the same regardless of biosimilar use. However, not enough data have been available to examine current circumstances surrounding the clinical use of biosimilar infliximab within Japan, including patient characteristics, penetration rate of biosimilars according to department, and the relationship between biosimilar penetration rate and subsidy for intractable diseases.
Patients and Methods
Study Design and Data Source
This retrospective, descriptive study utilized the Medical Data Vision Inc., Ltd. (MDV Inc.) database, a nationwide hospital-based database that contains health claims data, administrative data, and Diagnosis Procedure Combination (DPC) data from more than 420 Japanese acute hospitals (covering 24% of DPC hospitals). DPC is a novel medical reimbursement system introduced in 2003 only for hospital inpatients.18 Within the DPC system, detailed data, such as medical treatment, procedures, diagnosis, department, and intractable disease status, are uniformly formatted on a daily basis according to diagnosis.19 In DPC hospitals, although outpatient care is not covered by the DPC system, it is included in a fee-for-service payment system; therefore, the MDV database captures both inpatient and outpatient data. As of June 2020, the MDV database contained anonymized patient identifier, age, gender, diagnosis, medical procedures, prescriptions, inpatient/outpatient status, intractable disease designation status, total medical cost, and laboratory data of nearly 33 million cumulative patients. Many research articles have utilized the MDV database to describe a wide range of outcomes, such as treatment patterns, prevalence, and adherence.20–30
Data Extraction
Data collected from April 1, 2008 were used as patient background information, whereas data collected between April 1, 2013 and March 31, 2019 were used for analysis. The quality of the data within the database has been regularly assessed by MDV Inc.
Definition of Target Disease Diagnosis
Target disease diagnoses were identified based on the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD10). Accordingly, RA (M05, M06), CD (K50), UC (K51), and Ps (L40) were defined as target disease diagnoses given that they had been approved by the MHLW as indications for biosimilar infliximab during the data extraction period.
Study Population
Patients prescribed infliximab (reference infliximab and/or its biosimilar) after April 1, 2013 were included as the study population. However, records regarding biosimilars were available only after November 2014 when the first biosimilar of infliximab had been launched in Japan. Patients without target disease diagnosis records or with records of infliximab use before target disease diagnosis were excluded. The sex and age of those with two or more target disease diagnosis records were determined based on the first target diagnosis record. On the other hand, data regarding the number of target disease diagnoses and biosimilar penetration rates according to diagnosis or department were included in each analysis set of target disease diagnosis. Patients who satisfied the inclusion criteria were divided into two groups: the reference infliximab group and the infliximab biosimilar group. Those who had at least one record of biosimilar infliximab during the study period were included in the biosimilar group.
Statistical Analysis
Statistical analyses were conducted using Statistical Analysis System Version 9.4 (SAS Institute Inc., Cary, NC, USA). All study variables were descriptively examined. No statistical tests were performed given that the current study aimed to describe only the current situation of biosimilar infliximab and was not intended to compare among target populations or target disease diagnoses.
The following patient characteristics were examined: sex, age, subsidy for intractable diseases, multiple target diseases, comorbidity diseases [Interstitial pneumonia (J84), chronic obstructive pulmonary disease (J44), diabetes (E10, E20), and hypertension (I15)], and hospitalization in the reference and biosimilar groups. Subsidies for intractable diseases were identified through receipt names/codes, which indicated intractable disease outpatient guidance management fees (113002910) or intractable disease patients, and other hospitalization care add-on fees (190101770) after the diagnosis date of the target disease. Patients with multiple target diseases were identified as those with two or more target disease diagnoses prior to the first infliximab treatment. Any disease diagnosed after patients received their first infliximab treatment was not considered as a target disease. Biosimilar penetration rate was calculated based on the number of patients who met the inclusion criteria and described per target disease diagnosis, subsidy for intractable disease, and fiscal year (FY) from April to March based on the first infliximab treatment date. Changes in penetration rates per department were described for each target disease, while the top three departments with the highest number of infliximab records in 2018 (reference and/or biosimilar) were determined.
Ethics Approval
This study utilized a subject-level, electronic, health-related database released and maintained by MDV Inc. that protected the identity of individuals. MDV Inc. is permitted to use such anonymized data under a data transfer contract with its client health insurers. The current study complies with the “Ethical Guidelines for Epidemiological Research” established by the Japanese government.31
Results
A total of 13,302 patients with infliximab records (reference and/or its biosimilar) were identified in the MDV database from April 2008 to March 2019, among whom 10,597 started infliximab treatment after April 1, 2013. Meanwhile, 772 patients without target disease diagnosis records and 90 patients with infliximab records before the target disease diagnosis record were excluded. Overall, data from 9735 patients included in the study population were extracted (Figure 1). A total of 8950 (91.9%) and 785 (8.1%) patients were categorized into the reference and biosimilar groups, respectively. Among those in the biosimilar group, 490 patients had only a biosimilar record, 274 had switched from reference to biosimilar infliximab, and 21 had switched from biosimilar to reference infliximab. The numbers (proportion) of patients according to target disease diagnosis were 3073 (31.6%), 3797 (39.0%), 3023 (31.1%), and 735 (7.6%) for RA, CD, UC, and Ps, respectively. Patient characteristics of the reference and biosimilar groups are detailed in Table 1. Biosimilar penetration rates according to FY were 0.8%, 5.2%, 8.0%, 11.8%, and 22.5% in 2014, 2015, 2016, 2017, and 2018, respectively. All biosimilar infliximab penetration rates according to target disease diagnosis gradually increased from 2014 to 2018 (Figure 2). Biosimilar penetration rates throughout the whole study period according to diagnosis (with or without subsidy) were 14.4% (with, 4.1%; without, 16.4%) for RA, 4.7% (with, 3.7%; without, 10.6%) for CD, 5.7% (with, 4.5%; without, 13.5%) for UC, and 7.5% (with, 4.4%; without, 8.2%) for Ps (Table 2). The rheumatology department had the largest number of patients prescribed infliximab (reference and/or biosimilar) for RA in 2018, followed by internal medicine and orthopedic surgery. For both CD and UC, the gastroenterology department had the largest number of patients prescribed infliximab, followed by internal medicine and gastrointestinal surgery. For Ps, the dermatology department had the largest number of patients prescribed infliximab, followed by internal medicine and rheumatology. The number of patients receiving biosimilar infliximab and biosimilar penetration rates according to diagnosis and department increased annually in all departments (Supplementary Figure 1).
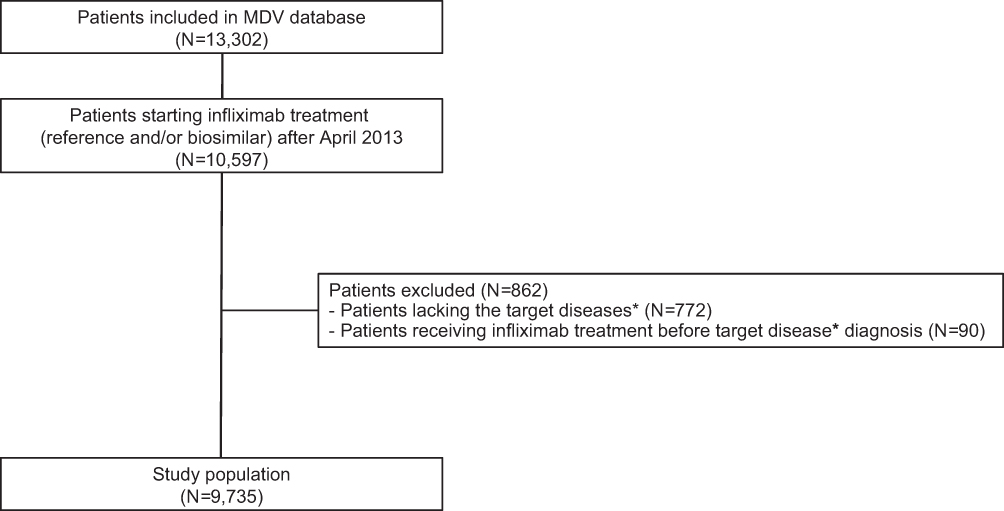 |
Figure 1 Patient flow chart. *Target diseases: RA (ICD10 Code: M05, M06), UC (ICD10 Code: K51), CD (ICD10 Code: K50), and Ps (ICD10 Code: L40). Abbreviations: MDV, Medical Data Vision; RA, rheumatoid arthritis; CD, Crohn’s disease; UC, ulcerative colitis; Ps, psoriasis; ICD, International Classification of Diseases; N, number of patients. |
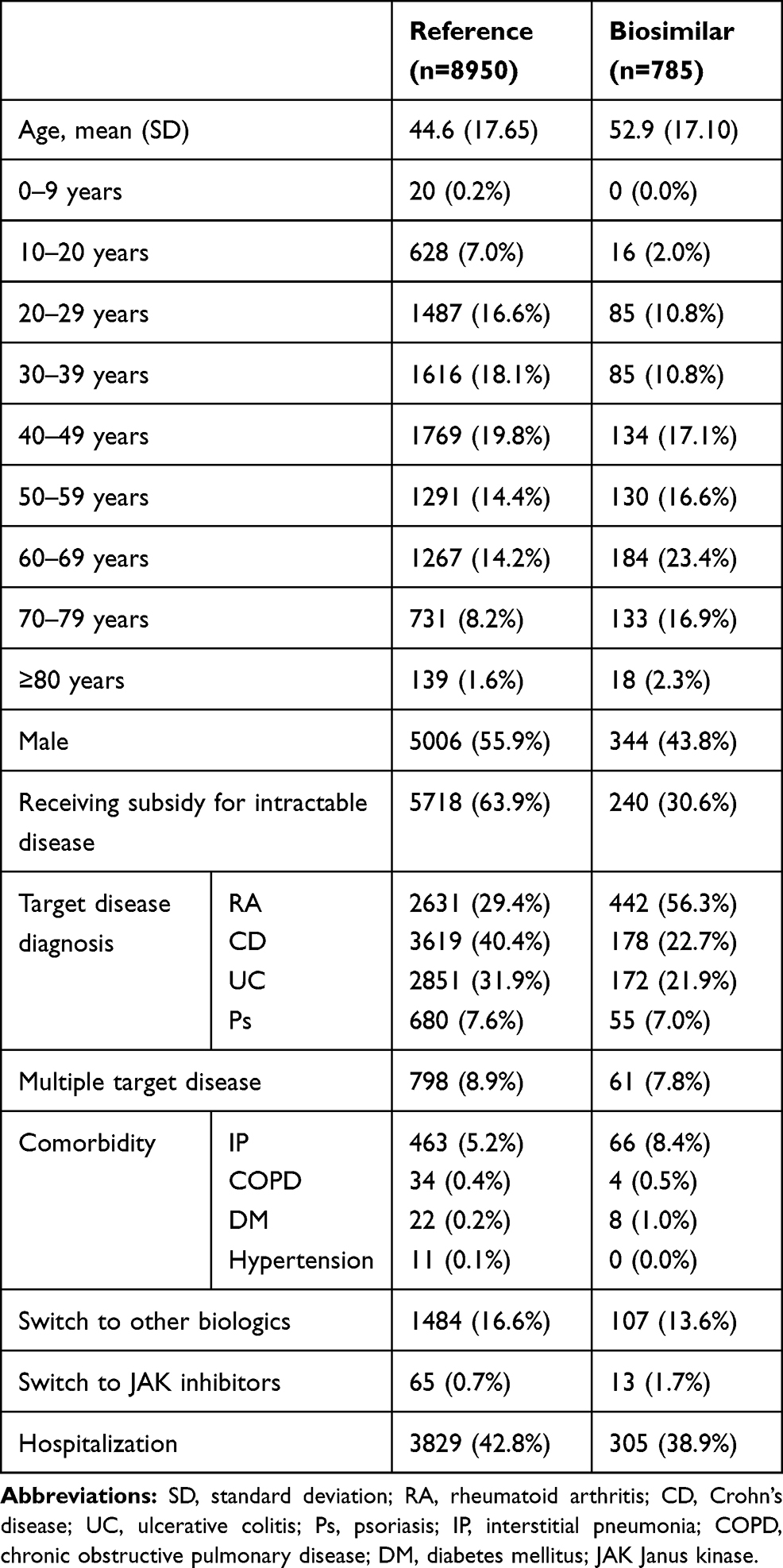 |
Table 1 Patient Characteristics |
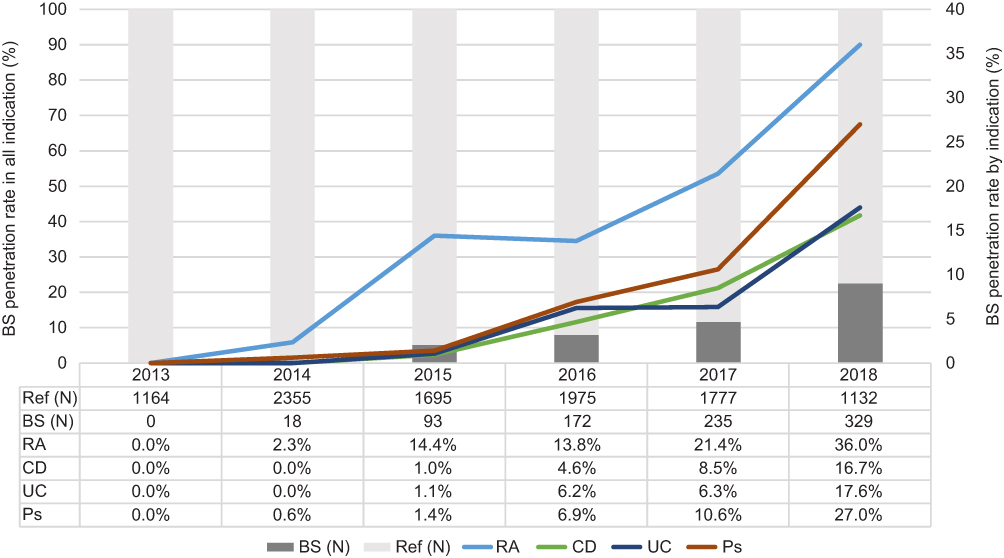 |
Figure 2 The penetration rate of biosimilar infliximab by fiscal year. Abbreviations: Ref, reference product; BS, biosimilar; N, number of patients; RA, rheumatoid arthritis; CD, Crohn’s disease; UC, ulcerative colitis; Ps, psoriasis. |
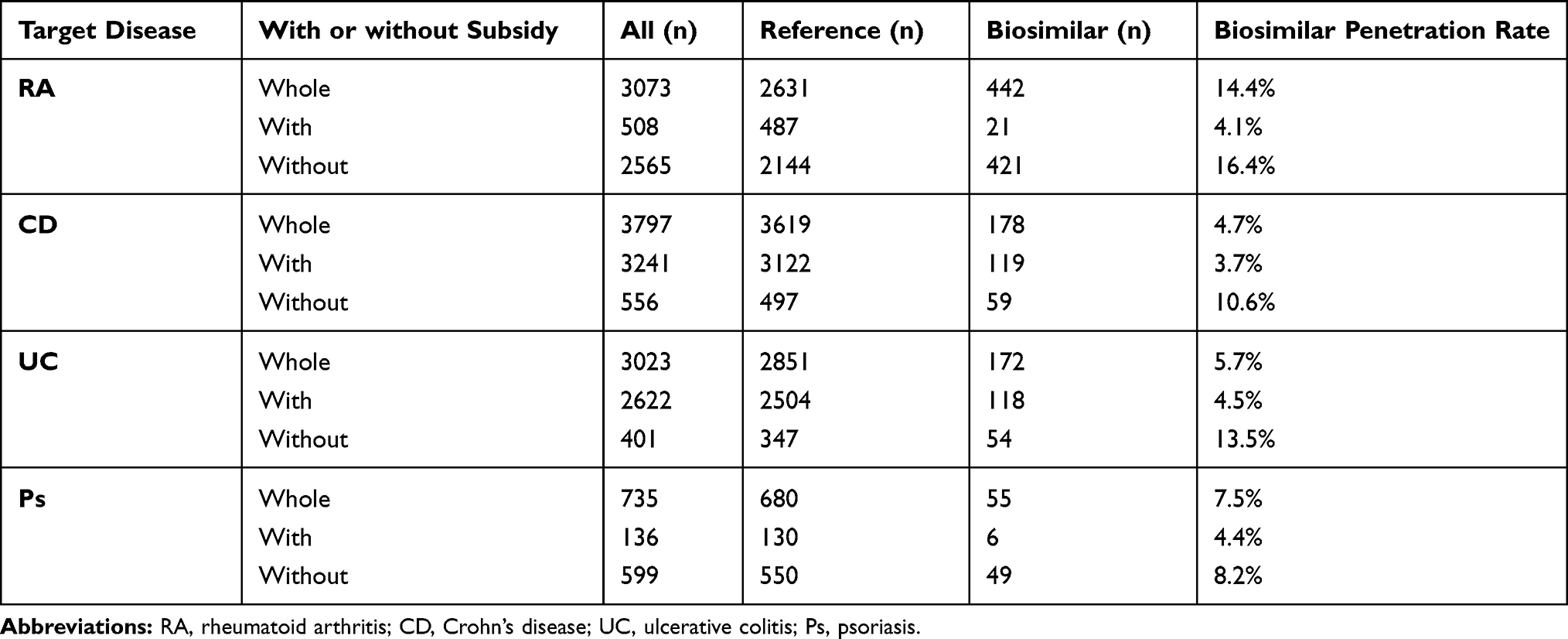 |
Table 2 Number of Patients Receiving the Reference Infliximab or Its Biosimilar for Target Disease Diagnosis (Whole, with or without Subsidy for Intractable Disease) Throughout the Study Period from 2014 to 2018 |
Discussion
This is the first study to describe whether patients with RA, CD, UC, and Ps received infliximab and/or its biosimilars and whether or not they received subsidy for intractable diseases. Reference infliximab (Remicade®), which was launched in Japan in 2002, has been widely used for inflammatory diseases such as RA, CD, and UC. Its first biosimilar (infliximab BS1, Nippon Kayaku, Celltrion) was approved by the PMDA in 2014, while the second (infliximab BS2, Nichiiko, Yakuhan Pharma) and third (infliximab BS3, Pfizer) biosimilars were approved in 2017 and 2018, respectively. Given that the extracted data were from April 2013 to March 2019, the database employed here mainly contained data for BS1 and BS2.10 It is unlikely that there are differences in disease entry or demographics of disease between BS1 and BS2 since patients in Japan have the right to choose any medical institution, regardless of disease sensitivity or severity, and the price of these biosimilars is the same, based on a price policy listed on the national health insurance program.
Patient background, characteristics, comorbidity, and hospitalizations were similar between the reference and biosimilar groups, except for rate of subsidy for intractable disease. Although the biosimilar group was older (mean, 52.9 years) than the reference group (mean, 44.6 years), this was partly because biosimilars were rarely used for patients under 20 years of age (Table 1). In the biosimilar group, 62.4% of the patients (490 of 785) had only biosimilar records, while 34.9% (274 of 785) had records of switching from reference infliximab. This indicates that biosimilar infliximab was more often prescribed for patients who started infliximab treatment than for those who had already been prescribed the reference product.
Infliximab was prescribed mostly for patients with CD (39.0%), followed by RA (31.6%), UC (31.1%), and Ps (7.6%) during the study period. Biosimilar infliximab penetration rates increased annually from 0.8% in 2014 to 22.5% in 2018, a trend observed for all indications (Figure 2). The penetration rate determined herein was comparable to that presented in previous reports from the European Union, which showed a total market penetration rate of 24% in 2017.32 In particular, penetration rates greatly increased during 2017 and 2018. One reason for this could be the clear statement in the Japanese government-approved policy document of the Council, published on June 9, 2017. While this policy enhanced supporting measures for the research and development of biopharmaceuticals and biosimilar pharmaceuticals, it disclosed the effective amount of optimization of medical costs and value share of biosimilar pharmaceuticals, and aimed to double the number of biosimilar pharmaceuticals (number of ingredients basis) by the end of the financial year 2020.33 Taking these measures into account, the medical associations and pharmaceutical companies have definitely made an effort to promote biosimilars. However, there is a considerable discrepancy when comparing the volume-based market share of infliximab biosimilar with that of other counties. According to previous research, the market share of infliximab biosimilars reached approximately 89% in the UK, followed by France (48%), and Korea (35%), whereas it was only 6% in Japan, based on the values for quarter one of 2018.34 Previous studies have shown an obvious discrepancy among the penetration rates of four biosimilar products in Japan, namely insulin glargine, filgrastim, infliximab, and rituximab, among which the biosimilar of filgrastim had the highest penetration rate of 80%, whereas the biosimilar of infliximab had the lowest penetration rate of 5.3%.12 This discrepancy may be due to differences between products in aspects such as the number of indications and prescriber expertise. Although filgrastim is prescribed mainly by hematologists for hematic cancer in the short term, infliximab is prescribed not only by rheumatologists for RA but also by gastroenterologists for UC and CD over the long term. This means greater effort is needed for physicians to gain understanding and experience in the use of infliximab biosimilar than for filgrastim biosimilar, without incentives, as well as for patients to accept a switch to the biosimilar version. Moreover, intractable disease systems may affect the motivation to use biosimilars. Filgrastim is prescribed mainly to patients with non-intractable diseases, whereas infliximab is prescribed mainly to those with intractable disease, such as CD, UC, or Ps. The current study also explored the relationship between biosimilar penetration rate and subsidy for intractable diseases. As expected, patients receiving subsidy for intractable diseases had much lower biosimilar penetration rates than those who did not, regardless of indication (Table 2). Although UC, CD, and some Ps have been designated as intractable disease, RA is not. The current findings could suggest that biosimilar infliximab penetration rates were highest in rheumatology departments. The intractable designation is an excellent system that reduces patient costs for the treatment of intractable diseases. Accordingly, those patients recognized as having a designated intractable disease need not pay over the cap on the total amount due each month. Through this system, patients with designated intractable diseases may focus on their treatment without considering treatment costs—part of a health-care system the Japanese government takes pride in globally. This system, however, causes patients to lack motivation for using biosimilars17,35,36 given that the use of biosimilars instead of reference biologics does not decrease patient costs. Had treatment costs become cheaper, the use of biosimilars would certainly have increased due to the potential savings with no loss in benefits. Thus, the generous Japanese health-care system could be one of the barriers toward expanding biosimilar use.
In spite of RA not covered by the intractable disease subsidy some treated RA patients were in receipt of subsidy. It anticipated that these particular patients had other comorbid diseases, such as rheumatoid vasculitis, which attracted an intractable disease subsidy. Not all patients with UC or CD received subsidies for intractable disease, perhaps because they failed to satisfy the disease severity criteria for designated intractable diseases. Some patients may also receive a medical expense subsidy other than that for intractable diseases.
The rheumatology departments of Japanese hospitals had the highest biosimilar penetration rates in 2018 among all indications and departments (59.0%). However, the number of patients receiving biosimilars has remained stable since 2015 (Supplementary Figure 1A). Therefore, an apparent increase in penetration rate rather than biosimilar use can be inferred. This result is reasonable considering the current RA treatment situation, where there is less opportunity for infliximab treatment given the number of new classes of available drugs, such as additional biologic disease-modifying antirheumatic drugs, TNF inhibitors, sarilumab (an anti-interleukin-6 receptor antibody that targets the same molecule as tocilizumab), and tofacitinib and baricitinib (Janus kinase inhibitors).37
Penetration rates for CD and UC had an increasing tendency across each department in Japanese hospitals, with the timing of the increase being slightly later than that for RA (Supplementary Figures 1B and C). The same tendency was observed for Ps in dermatology departments (Supplementary Figure 1D). As mentioned earlier, obtaining direct benefits from using biosimilar infliximab remains difficult given that CD and UC have been designated as intractable diseases. However, the significance of using biosimilars lies with not only reducing the burden on patients but also contributing toward a sustainable health-care system impervious to time.9 To control health-care expenditure, especially in Europe, there are strict policies on the use of high-cost drugs, based on Health Technology Assessment. On the other hand, in Japan, although drug prices are listed on the national health insurance program, there is no limit to the use of high-cost drugs, regardless of disease history or severity. In the current situation, controlling the increase in medical expenditures throughout Japan, with an aging population, remains an urgent concern. The Japanese government consistently established policies that pushed biosimilar use in Japan from 2017 to 2019,33,38,39 while educational seminars for health-care professionals and patients by the MHLW started in 2018.11 In 2020, the national price of reference infliximab per 100-mg vial was 75,009 Japanese Yen (JPY) and biosimilar infliximab was 43,229 JPY. Therefore, by using the biosimilar, the Japanese government could potentially save 30,384 JPY per vial.40 MHLW reported that the total number of infliximab reference and biosimilar was approximately 962,000 vials per year in financial year 2016.41 If biosimilar infliximab penetration increases to the same extent as biosimilar filgrastim, to 80%, the saving is estimated to be approximately 24,457 million JPY per year. With the promotion of biosimilars in mind, members of the pharmaceutical industry established the Japan Biosimilar Association in 2016 to create a biosimilar-friendly environment for both the development and appropriate usage of biosimilars in Japan. The association provides educational opportunities and materials for health-care professionals and patients. We believe that these activities would be effective in increasing the penetration rate of biosimilar infliximab. Therefore, continuously promoting the appropriate use of biosimilars while understanding the significance of these activities is important. We believe that our findings could help the government and associations to establish new policies.
Limitations of the Study
The present study has several limitations worth noting. First, using claims data may affect the validity and reproducibility of our research results. Although the MDV database covers approximately 24% of all DPC hospitals in Japan, our results might not show the current national situation of biosimilar infliximab. However, we believe that the current findings represent at least the current status of DPC hospitals, given that infliximab is an intravenous product prescribed in almost all DPC hospitals. Moreover, the use of biosimilar infliximab in DPC hospitals could be one key factor that determines the introduction timeline and penetration of each biosimilar in Japan.8 Therefore, our results may be helpful in understanding the current situation of biosimilars in Japan. Second, this study identified patients based on both the diagnostic code present in the claims data and prescription records of infliximab. In actual clinical practice, some coding may not be accurately recorded, some cases may have been misdiagnosed, or several professionals may have different coding patterns. Thus, the possibility of including misclassified patients cannot be ruled out. Despite the aforementioned limitations, the MDV database remains useful and provides the best data to investigate actual conditions of the patients receiving infliximab, including its biosimilars.
Conclusion
The present study described the current situation of biosimilar infliximab according to diagnosis in Japan using a claims database. Accordingly, the reference and biosimilar groups showed similar patient characteristics. Moreover, the overall penetration rate of biosimilar infliximab has been gradually increasing since its indication in 2014, with rates reaching 22.5% by 2018. Patients receiving subsidy for intractable diseases had much lower biosimilar penetration rates than those who did not, across all target disease diagnosis. Rheumatology, gastroenterology, and internal medicine are the primary departments that prescribe biosimilar infliximab.
Disclosure
Tsugumi Matsumoto and Takanori Tsuchiya are employees of Pfizer Japan Inc. and hold stocks in the same company. Takahiro Hirano and Thomas Laurent are affiliated with Clinical Study Support Inc. All other authors of this manuscript declare that they have no conflicts of interest.
References
1. Walsh G. Biopharmaceutical benchmarks 2010. Nat Biotechnol. 2010;28(9):917–924. doi:10.1038/nbt0910-917
2. National Institute of Health Sciences, 2019. List of approved biologics 2020. (In Japanese). Available from: http://www.nihs.go.jp/dbcb/approved_biologicals.html.
3. Konstantinidou S, Papaspiliou A, Kokkotou E. Current and future roles of biosimilars in oncology practice. Oncol Lett. 2020;19(1):45–51. doi:10.3892/ol.2019.11105
4. Rabaan AA, Al-Ahmed SH, Bazzi AM, et al. Overview of hepatitis C infection, molecular biology, and new treatment. J Infect Public Health. 2020;13(5):773–783. doi:10.1016/j.jiph.2019.11.015
5. Ministry of Health, Labour and Welfare, Japan. Update of drug pricing system in Japan 2018. Available from: https://www.mhlw.go.jp/content/11123000/000335166.pdf.
6. Kang HN, Thorpe R, Knezevic I. The regulatory landscape of biosimilars: WHO efforts and progress made from 2009 to 2019. Biologicals. 2020;65:1–9. doi:10.1016/j.biologicals.2020.02.005
7. Kuribayashi R, Sawanobori K. Current Japanese regulatory systems for generics and biosimilars. J Pharm Sci. 2018;107(3):785–787. doi:10.1016/j.xphs.2017.10.040
8. Rathore AS, Bhargava A. Biosimilars in developed economies: overview, status, and regulatory considerations. Regul Toxicol Pharmacol. 2020;110:104525. doi:10.1016/j.yrtph.2019.104525
9. Yonezawa A, Matsubara K. Current issues and future perspectives of biosimilar in cancer therapy. (In Japanese). Jpn J Cancer Chemother. 2020;47(3):397–401.
10. Generics and Biosimilars Initiative. Biosimilars approved in Japan. Available from: http://gabionline.net/Biosimilars/General/Biosimilars-approved-in-Japan.
11. Ministry of Health, Labour and Welfare, Japan. What’s new 2018. Available from: https://www.mhlw.go.jp/english/new-info/2018.html.
12. Goto Y, Tsuchiya T, Tanabe K. Investigation on the current status surrounding biologics and the impact of biosimilars on drug cost using real world data. (In Japanese). Jpn J Med Pharm Sci. 2019;76(2):193–207.
13. Melsheimer R, Geldhof A, Apaolaza I, Schaible T. Remicade® (infliximab): 20 years of contributions to science and medicine. Biologics. 2019;13:139–178. doi:10.2147/BTT.S207246
14. Ministry of Health, Labour and Welfare, Japan. An outline of the Japanese medical system. Available from: https://www.mhlw.go.jp/bunya/iryouhoken/iryouhoken01/dl/01_eng.pdf.
15. Ministry of Health, Labour and Welfare, Japan. High-cost medical expense benefit (eligibility certificate for ceiling-amount application) or KOGAKU RYOYOHI SEIDO (GENDOGAKU TEKIYO NINTEISHO) 2018. Available from: https://www.mhlw.go.jp/seisakunitsuite/bunya/kenkou_iryou/iryou/kokusai/setsumeisiryo/dl/en09.pdf.
16. Nakatani H, Kondo T. Characteristics of a medical care program for specific diseases in Japan in an era of changing cost-sharing. Health Policy (New York). 2003;64(3):377–389. doi:10.1016/S0168-8510(02)00199-9
17. Ministry of Health, Labour and Welfare, Japan. Intractable disease measures. Available from: https://www.mhlw.go.jp/english/wp/wp-hw5/dl/23010223e.pdf.
18. Ministry of Health, Labour and Welfare, Japan. Summary of diagnosis procedure combination system and its basic concept. (In Japanese). Available from: https://www.mhlw.go.jp/stf/shingi/2r985200000105vx-att/2r98520000010612.pdf.
19. Hamada H, Sekimoto M, Imanaka Y. Effects of the per diem prospective payment system with DRG-like grouping system (DPC/PDPS) on resource usage and healthcare quality in Japan. Health Policy (New York). 2012;107(2–3):194–201. doi:10.1016/j.healthpol.2012.01.002
20. Oh A, Kisanuki K, Nishigaki N, Shimasaki Y, Sakaguchi K, Morimoto T. Comparison of persistence and adherence between DPP-4 inhibitor administration frequencies in patients with type 2 diabetes mellitus in Japan: a claims-based cohort study. Curr Med Res Opin. 2020;36(3):387–395. doi:10.1080/03007995.2019.1699519
21. Winburn I, Ishii T, Sumikawa T, Togo K, Yasunaga H. Estimating the prevalence of transthyretin amyloid cardiomyopathy in a large in-hospital database in Japan. Cardiol Ther. 2019;8(2):297–316. doi:10.1007/s40119-019-0142-5
22. Wake M, Oh A, Onishi Y, Guelfucci F, Shimasaki Y, Teramoto T. Adherence and persistence to hyperlipidemia medications in patients with atherosclerotic cardiovascular disease and those with diabetes mellitus based on administrative claims data in Japan. Atherosclerosis. 2019;282:19–28. doi:10.1016/j.atherosclerosis.2018.12.026
23. Sakata Y, Matsuoka T, Ohashi S, Koga T, Toyoda T, Ishii M. Use of a healthcare claims database for post-marketing safety assessments of eribulin in Japan: a comparative assessment with a prospective post-marketing surveillance study. Drugs Real World Outcomes. 2019;6(1):27–35. doi:10.1007/s40801-019-0150-8
24. Nishimura R, Kato H, Kisanuki K, et al. Comparison of persistence and adherence between fixed-dose combinations and two-pill combinations in Japanese patients with type 2 diabetes. Curr Med Res Opin. 2019;35(5):869–878. doi:10.1080/03007995.2018.1551192
25. Nishimura R, Kato H, Kisanuki K, et al. Treatment patterns, persistence and adherence rates in patients with type 2 diabetes mellitus in Japan: a claims-based cohort study. BMJ Open. 2019;9(3):e025806. doi:10.1136/bmjopen-2018-025806
26. Wake M, Onishi Y, Guelfucci F, et al. Treatment patterns in hyperlipidaemia patients based on administrative claim databases in Japan. Atherosclerosis. 2018;272:145–152. doi:10.1016/j.atherosclerosis.2018.03.023
27. Matsui A, Morimoto M, Suzuki H, Laurent T, Fujimoto Y, Inagaki Y. Recent trends in the practice of procedural sedation under local anesthesia for catheter ablation, gastrointestinal endoscopy, and endoscopic surgery in Japan: a retrospective database study in clinical practice from 2012 to 2015. Drugs Real World Outcomes. 2018;5(3):137–147. doi:10.1007/s40801-018-0136-y
28. Imai K, Petigara T, Kohn MA, et al. Risk of pneumococcal diseases in adults with underlying medical conditions: a retrospective, cohort study using two Japanese healthcare databases. BMJ Open. 2018;8(3):e018553. doi:10.1136/bmjopen-2017-018553
29. Teramoto T, Uno K, Miyoshi I, et al. Low-density lipoprotein cholesterol levels and lipid-modifying therapy prescription patterns in the real world: an analysis of more than 33,000 high cardiovascular risk patients in Japan. Atherosclerosis. 2016;251:248–254. doi:10.1016/j.atherosclerosis.2016.07.001
30. Chang CH, Sakaguchi M, Dolin P. Epidemiology of lactic acidosis in type 2 diabetes patients with metformin in Japan. Pharmacoepidemiol Drug Saf. 2016;25(10):1196–1203. doi:10.1002/pds.4030
31. Ministry of Education, Culture, Sports, Science and Technology, Ministry of Health, Labour and Welfare. Ethical guidelines for epidemiological research. Available from: http://www.niph.go.jp/wadai/ekigakurinri/guidelines.pdf.
32. IQVIA. IQVIA report 2018: the impact of biosimilar competition in Europe. Available from: https://ec.europa.eu/docsroom/documents/31642.
33. Cabinet Office, Government of Japan. Basic policy on economic and fiscal management and reform 2017. Available from: https://www5.cao.go.jp/keizai-shimon/kaigi/cabinet/2017/2017_basicpolicies_en.pdf.
34. Kim Y, Kwon HY, Godman B, Moorkens E, Simoens S, Bae S. Uptake of biosimilar infliximab in the UK, France, Japan, and Korea: budget savings or market expansion across countries? Front Pharmacol. 2020;11:970. doi:10.3389/fphar.2020.00970
35. Japan Interactable Diseases Information Center. Information on medical expenses subsidy system for patients with designated intractable disease. (In Japanese). Available from: https://www.nanbyou.or.jp/entry/5460.
36. Okabayashi S, Kobayashi T, Hibi T. Inflammatory bowel disease in Japan - is it similar to or different from Westerns? J Anus Rectum Colon. 2020;4(1):1–13. doi:10.23922/jarc.2019-003
37. Smolen JS, Landewé RBM, Bijlsma JWJ, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79(6):685–699. doi:10.1136/annrheumdis-2019-216655
38. Cabinet Office, Government of Japan. Basic policy on economic and fiscal management and reform 2018. Available from: https://www5.cao.go.jp/keizai-shimon/kaigi/cabinet/2018/2018_basicpolicies_en.pdf.
39. Cabinet Office, Government of Japan. Basic policy on economic and fiscal management and reform 2019. Available from: https://www5.cao.go.jp/keizai-shimon/kaigi/cabinet/2019/2019_basicpolicies_en.pdf.
40. Ministry of Health, Labour and Welfare, Japan. National health insurance drug price standard list for injection. (In Japanese). Available from: tp 20201211-01_02.pdf (mhlw.go.jp).
41. Ministry of Health, Labour and Welfare, Japan. 424th central social insurance medical council document 1–1 (54). (In Japanese). Available from: 000522373.pdf (mhlw.go.jp).
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.